



1 Aortic Institute at Yale-New Haven Hospital, New Haven, CT 06510, USA
2 Saint Peter’s University Hospital, New Brunswick, NJ 08901, USA
3 Department of Cardiovascular and Endovascular Surgery, Kazan State Medical University, 420012 Kazan, Russia
Academic Editor: Yan Topilsky
Abstract
Purpose: According to the 2020 American College of Cardiology/American
Heart Association guidelines, the aortic valve should be replaced in the setting
of severe aortic stenosis or regurgitation, independent of left ventricular
function (even for EF
Keywords
- aortic valve replacement
- ejection fraction
- heart failure
- intra-aortic balloon pump
- aortic stenosis
- aortic regurgitation
ACC/AHA Practice Guidelines recommend aortic valve replacement surgery (SAVR)
for patients with severe asymptomatic aortic regurgitation (AR) and a low left
ventricular ejection fraction (EF
Despite subsequent advancements in the medical and surgical landscape, AVR is
still likely underutilized. A recent report from 2022, for example, showed that
in over 6000 AS patients for whom it was indicated or potentially indicated, only
48% of patients had an AVR [4]. Importantly, a low EF (
The safety and efficacy of TAVR has been convincingly demonstrated. Several recent studies looking at TAVR in low-EF patients show marked improvements in mortality and in EF [7, 8, 9]. The mortality and improvements in EF may be non-inferior to patients with a preserved or milder reduction in LVEF [10, 11]. The question addressed by this study, however, is whether a low EF in and of itself poses a risk significant enough to recommend against SAVR specifically, or whether these patients may still see significant clinical benefit. For young patients with low EF, for example, a durable mechanical valve may be quite strongly preferable to a biological TAVR valve.
We present here our single-center, single-surgeon retrospective analysis of a group of 40 very low EF patients with AS and/or AR who underwent SAVR and were followed up for several months to years.
This is a retrospective cohort study from a large university medical center
(Yale Aortic Institute, Yale New Haven Hospital, New Haven, Connecticut, USA).
Using a database containing records from 2004 to 2019 of patients treated at the
Yale Aortic Institute, we searched for patients who underwent SAVR for aortic
stenosis and/or aortic regurgitation by a single surgeon (JE). 895 patients fit
these criteria. Of these, 40 patients had an ejection fraction of 35% or less,
and these made up our study population. The AHA/ACC diagnostic criteria for
severe aortic stenosis include an aortic valve maximum velocity
Detailed chart reviews were performed on these patients (both alive and dead) to extract clinical and surgical data. The patients were divided into three groups: severe AS, severe AR, or mixed aortic valve disease, i.e., both AR and AS. 18 patients were identified for whom we employed the prophylactic use of an intra-aortic balloon pump (IABP). Patients who underwent other cardiac surgical procedures simultaneously were not excluded (27/40 patients).
Kaplan-Meier survival analysis (constructed in GraphPad Prism®, GraphPad Software, San Diego, California, USA) was also undertaken. An age and gender-matched control curve was constructed by matching each patient individually and following that patient according to life table survival data from the Centers for Disease Control and Prevention for the intercensal year 2010 (the mean year of operation). A single-sample log-rank test was employed for assessing the difference between patient and matched population survivals. The comparison of the operated group against the controls was constructed up to 5 years [12]. Further statistical analysis was conducted using the R programming language.
All surgeries were performed via median sternotomy. Standard ascending aortic and dual stage venous cannulation were employed. Myocardial preservation was by a combination of systemic hypothermia, topical hypothermia with iced saline, and cold crystalloid cardioplegia given initially antegrade (except in case of severe AR) and subsequently retrograde through the coronary sinus. Cardiopulmonary bypass and cross-clamp times are recorded in the Results section. Intra-aortic balloon pump, when employed, was used prophylactically through the groin pre-bypass. The decision to use IABP was based on a gestalt of the following factors: how low the EF was; the degree of left ventricular enlargement; the overall appearance of the patient and how compromised they seemed; and the severity of the AR. IABP was used liberally in compromised patients, as it is the authors’ opinion that it provides strong perioperative cardiac support without the oxygen debt related to inotropes.
Primary endpoints for this study were changes in EF and mortality at 30 days and in the mid-term (beyond 1 year post-op). Changes in EF and LV dimensions over time were measured by echocardiography done during follow-up visits. These follow-ups were obtained regularly and at periodic intervals as post-operative visits or follow-ups in clinics. A typical follow-up consisted of clinical examination and serial echocardiography. Where direct patient follow-up was not possible, follow-up was obtained from the patient’s family physician.
The study was approved by the Human Investigation Committee of Yale University. Individual patient consent was waived for retrospective review.
Preoperative clinical data, including chest x-ray, Doppler
echocardiography, cardiac catheterization, and coronary artery anatomy, were
collected by review of the medical records of 40 eligible patients, representing
4.47% of the entire population of patients who underwent SAVR for AS and/or AR
(n = 895) by the single surgeon during the same period. All patients
underwent two dimensional and Doppler echocardiography
From 2004 to 2019, 895 patients underwent SAVR for aortic stenosis, aortic regurgitation, or mixed disease by a single surgeon at our institution. 16 patients presented with AS, 20 with AR, and 4 with a combination of AS and AR. There were 35 men and 5 women, with a mean age of 63.7 at the time of operation. SAVR was most commonly performed either in isolation or in combination with an ascending aortic aneurysm resection (13 each), with a further 7 patients receiving concomitant CABG. Amongst the patients who had concomitant CABG, 3 had vein grafts only, 3 had an arterial graft only, while 4 had a mixture of both types of graft.
The mean ejection fraction improved from 26% to 35% in the first year and up
to 46% beyond 1 year with mean follow-up of 43 months (0.1–140.7) when the most
recent scan result was considered. These results are illustrated graphically in
Fig. 1. The diagnosis sub-group with the lowest initial EF was the AS-only group
(mean 24.8%), followed by AR-only group (mean 26.2%) and then the AS+AR group
(mean 31.5%). The EF of all three subgroups improved significantly
postoperatively when the most recent follow-up EFs were considered (unpaired
two-tailed t-tests; +17.0% p
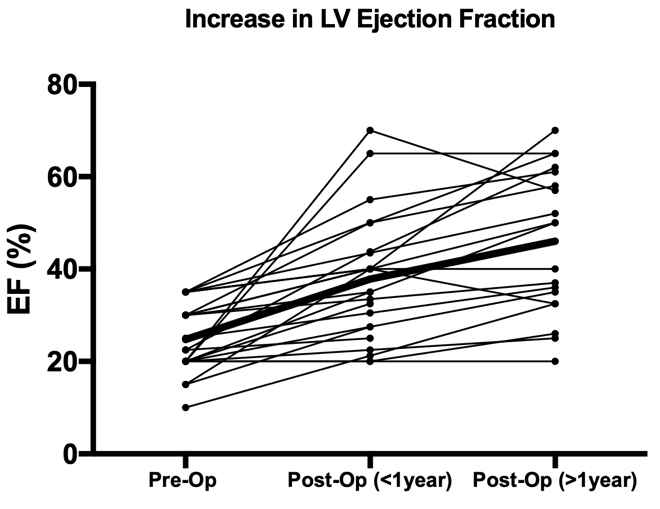 Fig. 1.
Fig. 1.Changes in EF over time following AVR. One dot represents one
patient’s reading, with lines representing changes over time for each patient.
“Post-Op (
The prevalence of common cardiovascular risk factors, further operative details,
and further echocardiogram readings for each group are listed in Table 1.
Comparisons between the groups to assess for statistically significant
differences were done using
| Variable | AR | AS | Mixed | Overall | Significance | |
| Risk factors | ||||||
| Age at Surgery | 56.9 | 70.6 | 69.5 | 63.6 | p = 0.004* | |
| Height/m | 1.78 | 1.72 | 1.82 | 1.76 | p = 0.072 | |
| Weight/kg | 92.5 | 87.5 | 100.9 | 91.4 | p = 0.389 | |
| % Diabetes | 10 | 50 | 50 | 30 | p = 0.02* | |
| % COPD | 10 | 18.75 | 0 | 12.5 | p = 0.553 | |
| % Hypertension | 70 | 68.75 | 100 | 72.5 | p = 0.429 | |
| % Dyslipidemia | 40 | 56.25 | 50 | 47.5 | p = 0.621 | |
| % Cancer | 10 | 43.75 | 25 | 25 | p = 0.067 | |
| % Smokers | 52.6 | 26.7 | 50 | 42.1 | p = 0.296 | |
| % Bicuspid aortic valve | 45 | 25 | 25 | 35 | p = 0.415 | |
| EuroScoreII | 6.3 | 10.1 | 5.8 | 7.8 | p = 0.541 | |
| Operative details | ||||||
| Cross-clamp time/min | 103 | 90 | 74 | 92 | p = 0.227 | |
| Cardiopulmonary bypass time/min | 138 | 113 | 115 | 123 | p = 0.345 | |
| % Bioprosthetic valve | 50 | 43.75 | 100 | 52.5 | p = 0.125 | |
| Echocardiogram measurements | ||||||
| LV end-diastolic diameter (EDD) | 6.5 | 5.5 | 6.1 | 6.0 | p = 0.007* | |
| LVEDD |
6.3 | 5.7 | 5.3 | 5.9 | p = 0.312 | |
| LVEDD |
5.5 | 5.2 | 4.9 | 5.3 | p = 0.466 | |
| LV end-systolic diameter (ESD) | 5.1 | 4.5 | 5.0 | 4.8 | p = 0.18 | |
| LVESD |
5.0 | 4.6 | 4.5 | 4.8 | p = 0.642 | |
| LVESD |
4.2 | 4.2 | 3.7 | 4.1 | p = 0.666 | |
| LV interventricular septum width (IVS) | 1.1 | 1.1 | 1.3 | 1.1 | p = 0.278 | |
| LVIVS |
1.1 | 1.1 | 1.2 | 1.1 | p = 0.739 | |
| LVIVS |
1.1 | 1.0 | 1.2 | 1.1 | p = 0.119 | |
| LV posterior wall thickness (PW) | 1.1 | 1.1 | 1.2 | 1.1 | p = 0.75 | |
| LVPW |
1.1 | 1.1 | 1.2 | 1.1 | p = 0.599 | |
| LVPW |
1.1 | 1.0 | 1.2 | 1.1 | p = 0.133 | |
| Values quoted are percentages or mean values. “Significance” denotes whether
the three groups (AS/AR/Mixed) are statistically different to each other based on
| ||||||
Patients in whom IABP was used had a lower initial EF than those without IABP (range 10–35, mean 23% with IABP vs. range 15–35%, mean 27.6% without IABP). This was a statistically significant difference (p = 0.014). Those who received IABP had a smaller EF increase (+12.3% vs. +19.0%), but this difference was not significant (p = 0.18).
In addition to EF, changes in LV dimensions were tracked over the same period. As shown in Table 1, in the mid-term, both LV end-diastolic diameter (LVEDD) and LV end-systolic diameter trended downwards (LVESD), while LV intraventricular septal thickness and posterior wall thickness remained relatively steady. Statistical analysis shows that only the decrease in LVEDD was significant over this period (p = 0.0046), though the decrease in LVESD over this period almost reached significance (p = 0.056). These results further demonstrate post-operative LV remodeling.
Overall morbidity and mortality were low. A total of 9 patients (22.5%) died during the follow-up period (4 AS (25%), 4 AR (20%), and 1 mixed (25%)), with a mean of 1336 days between operation and death (range 10–2889 days). The mean days till death was 834 days in the AS-only group, 1728 days in the AR-only group, and was 1778 days in the single mixed patient. Only 2 patients died from a cardiovascular cause. Five-year survival was comparable between the study group and an age- and gender-matched general population (p = 0.834), as seen in Fig. 2.
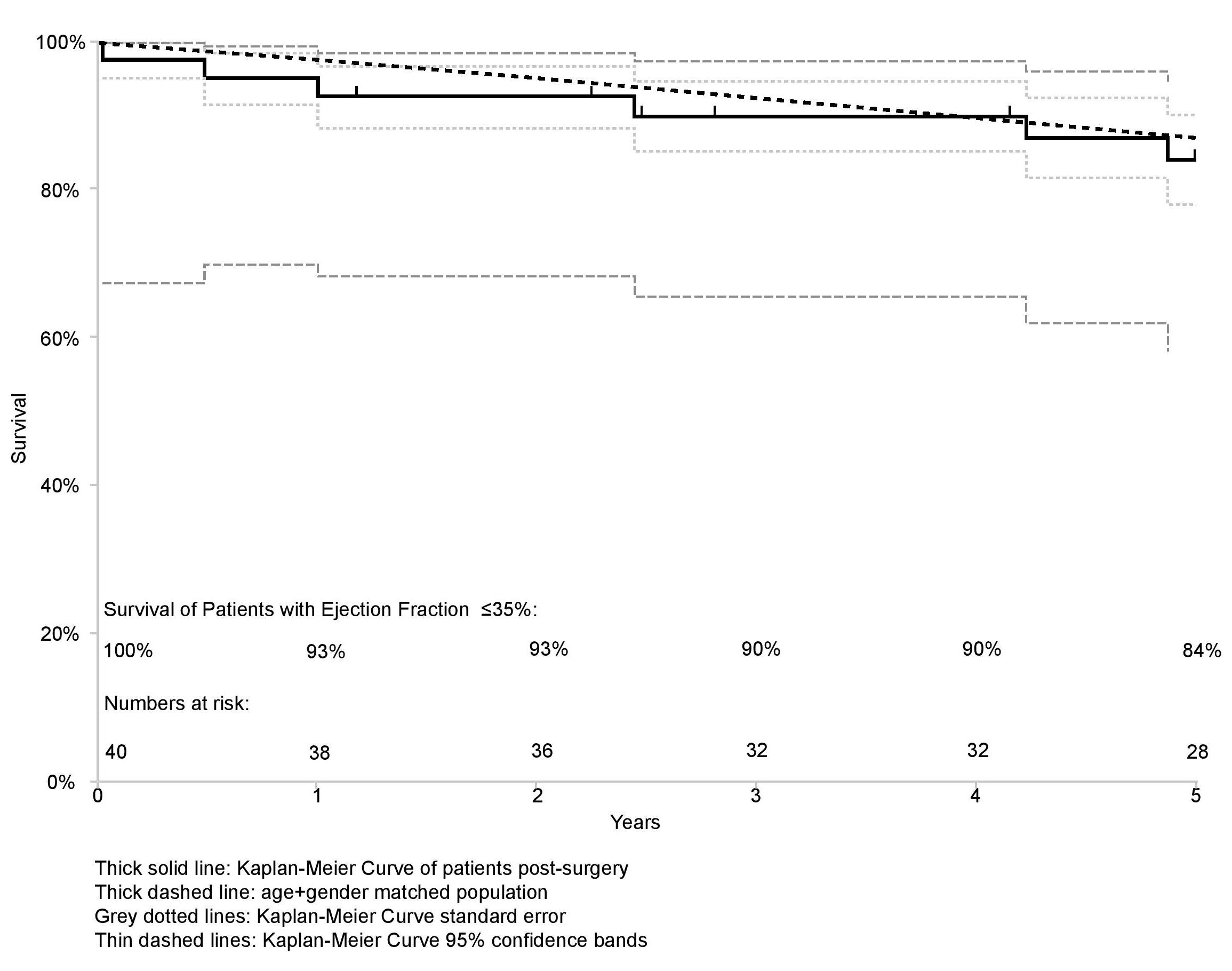 Fig. 2.
Fig. 2.Kaplan-Meier curves for the post-op and age/gender-matched control cohorts. Note, remarkably, that survival of the low-EF surgical group equals that of the normal age and gender matched population.
Only one patient, a male who was 47 at the time of the operation, died within 30 days of the operation. He had AR only and received concomitant ascending aortic aneurysm replacement. Two days after discharge, he developed chest pain, tightness, and shortness of breath, and had to be readmitted to hospital. He was found to have a large LAD thrombus, requiring single CABG to the LAD and LVAD insertion. Due to a lack of improvement from his state of cardiogenic shock, care was withdrawn in the ICU two days later, a total of 10 days post-op.
Of the pre-operative and operative variables outlined in Table 1, only older age (p = 0. 0195; OR 1.10 (1.03-1.21); mean 60.8 for alive and 73.8 for dead) and higher EuroScore II (p = 0.0375; OR 1.17 (1.04–1.41); mean 5.1 for alive and 16.8 for dead) independently predicted mid-term mortality. The change in EF also predicted mid-term mortality (+18.9% alive vs. +5.7% dead, p = 0.037), but importantly, the initial EF did not (p = 0.45).
Two of the patients who died had AVR only. The remainder had AVR + CABG (3), AVR +
aneurysm repair (3), or AVR + CABG + aneurysm repair (1). There was no
significant difference in mid-term mortality between the three choices of vessel
graft (vein, artery, or both; p = 0.91). The distribution of operation
type in the death subset was not significantly different from the distribution in
all patients taken together (
In addition to mortality, the incidence of other major cardiovascular events- post-op MI and stroke- were tracked. Post-op MI occurred in 5.1% of cases (AR: 10%, AS + Mixed: 0%) and post-op stroke occurred in 10.3% of cases (AR: 15%, AS: 6.7%, Mixed: 0%). ANOVA tests reveal there is no significant difference between the three groups for either of these two outcomes (p = 0.37 for MI, p = 0.56 for stroke).
We report our results with SAVR in patients with an impaired left ventricle, who
had AS, AR, or both. We show that early and late post-surgical outcomes are
excellent. We show that even in patients with severely impaired left ventricles,
i.e., EF
From the perspective of functional outcomes, the predictive value of smoking status is in line with many prior studies which illustrate the link between smoking and LV dysfunction, including a recent study that used UK Biobank data to show how this association persists even when controlling for other common risk factors such as hypertension and diabetes mellitus [16]. The effect may even be dose-dependent in ex-smokers [17]. The etiology of this relationship is thought to be multifactorial, involving inflammatory and oxidative damage to the vascular endothelium and subsequent ischaemic damage to the myocardium [16, 18]. There may even be damage to the myocardium directly [19, 20]. In-vitro studies using cigarette smoke extract have also shown that smoke can damage cardiac stem cells, which in turn would impair the repair of cardiac injury [21].
Reports of short-term mortality of patients who underwent SAVR for AS and/or AR
with low EF vary widely in the literature, from as low as 0% to a high of 21%.
A number of variables have been proposed to predict prognosis in patients, some
of which are different from those identified in the present study [22, 23, 24]. Kaneko
et al. [14] found that advanced age, high NYHA class, and elevated
preoperative creatinine were associated with an increased risk of mortality in
their cohort. Pereira et al. [25] showed that age and serum creatinine
level were predictors of mortality in patients who received AVR for severe AS
with low transvalvular gradient and severe left ventricular dysfunction (EF
Bach et al. [27] concluded that some patients with severe symptomatic
AS were denied access to potentially lifesaving therapy due to a perception of
prohibitive operative risk. They found that 191 (52%) patients with severe AS at
their centers did not undergo AVR, of which 33 (17%) had an EF
In addition to SAVR, other operations such as CABG have also been investigated
in the low EF population. Such studies similarly illustrate that low EF need not
preclude an operation as long-term survival is the same or better when compared
to non-operated controls. As with SAVR, an increase in EF is also commonly seen,
and this may contribute to improving any associated ventricular dysfunction. A
study from 2001, for example, followed 135 patients with an EF
Our study has several important limitations. These include its retrospective nature and the observational nature of the study design. Moreover, the small number of patients may have limited the power of the study to detect clinically important differences between groups. It also remains to be seen whether the results are generalizable.
A regurgitant or stenotic aortic valve can contribute to progressive LV dysfunction (LVD) through an increase in afterload or a volume overload. Conceptually, if a patient’s LV dysfunction were caused at least in part by their valve lesion, then it may not be prudent to dismiss the patient as a surgical candidate based primarily on their LVD, as we might expect it to improve following correction of the valve dysfunction. The data from this study suggest that this theory is borne out: the EF improved on average by 77% above the pre-operative value, while 5-year survival was rendered comparable to an age- and gender-matched population. As noted in previous work from our group, there are a few factors which cumulatively contribute to the risks of this operation: the severity of pre-op symptoms, the severity of the left ventricular systolic dysfunction, and the duration of this dysfunction [31]. Operating in a timely manner may thus prevent long-term, irreversible LV dysfunction from developing.
Our data suggest that left ventricular failure, specifically manifesting as EF
AK wrote the manuscript. JE operated on the patients. AK, TV, OA, and PC collected the data. AK and PC performed the statistical analysis. MZ, BZ, and JE supervised the project and critically reviewed the final draft.
The study was approved by the Human Investigation Committee of Yale University (Protocol Number 1609018416). Individual patient consent was waived for retrospective review.
Not applicable.
This research received no external funding.
Dr. Elefteriades is a Principal of CoolSpine, serves on the Data and Safety Monitoring Board of Terumo, and is a consultant for CryoLife.
The authors declare no conflict of interest. John A. Elefteriades is serving as one of the Editorial Board Members and Guest Editors of this journal. We declare that John A. Elefteriades had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Yan Topilsky.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.