


 , Alexander Shefler 1, Jacob Bejar 2, Sagi Shprits 1, Ofir Avitan 1, Sarel Halachmi 1, Ofer Nativ 1
, Alexander Shefler 1, Jacob Bejar 2, Sagi Shprits 1, Ofir Avitan 1, Sarel Halachmi 1, Ofer Nativ 11 Department of Urology, Bnai-Zion Medical Center, Haifa, Israel
2 Department of Pathology, Bnai-Zion Medical center, Haifa, Israel
†These authors contributed equally.
Abstract
Background: Prostate cancer is one of the most common cancers affecting men worldwide with an increasing incidence in most countries. The gold standard for diagnosis is Transrectal Ultrasonography-guided prostate biopsy. The quality of the biopsy is determined by parameters like the length of the biopsy core and the degree of fragmentation, affecting detection rate. SmartBx™ is a tool designed for the handling of prostate biopsy specimens and is intended for maximal tissue preservation. The aim of the current study was to evaluate the detection rate of prostate cancer using the new SmartBx™ tool. Patients and Methods: The study group had a biopsy using the SmartBx™ system and each biopsy core was applied into a cassette, which included two cores of biopsies which were then downloaded into a formalin-filled container. The control group included patients who underwent a Transrectal Ultrasonography-guided biopsy using the “standard” technique of biopsy collection. Data were collected prospectively in the study group, and retrospectively in the control group. Overall detection rate, and detection rate per core, were calculated and compared between the two groups. Results: The study included 600 patients, 300 in each group. There were no statistically significant differences between the groups regarding baseline characteristics. The average core numbers obtained per patient were 13.0 ± 2.7 and 14.1 ± 4.4 (P = 0.001) in the SmartBx™ and control groups, respectively. The use of the SmartBx™ system resulted in 21.2% better tissue preservation than in the control group. The overall detection rate as well as the detection rate per core were higher in the study group. More Gleason score 4 + 3 (Grade Group III) were detected in the study group (44.1% vs. 12.5%, P = 0.01). Conclusions: The use of the SmartBx™ system yielded more biopsy tissue for diagnosis. It increased the detection rate per core and the detection of Gleason score 4 + 3 (Grade Group III) prostate cancer.
Keywords
- Prostate cancer
- transrectal ultrasound
- SmartBX
Prostate cancer (PCa) is one of the most common cancers affecting men worldwide with an increasing incidence in most countries [1, 2]. Early diagnosis and treatment of PCa can reduce metastatic disease and mortality [3]. Major efforts have been invested to improve the detection rate of clinically significant PCa, and to eventually administer the treatment of choice [4, 5].
Transrectal ultrasound (TRUS)-guided prostate biopsy is the gold standard procedure for the pathological diagnosis of PCa [6, 7]. The quality of the biopsy is determined by parameters like the length of biopsy core and degree of fragmentation, affecting detection rate [8, 9, 10, 11]. It was also found that improved pre-embedding method by placing the biopsy core directly in cassettes may have some advantage if this is performed at the biopsy suite by the urologists [8]. This is mainly due to decreasing manipulation and damage to the biopsy specimen.
Poor biopsy quality may affect prognostic parameters like number of involved cores and extent of cancer in an individual core, which may affect treatment decision [12].
SmartBx™ (UC-Care Medical Systems, Yokneam, Israel) is a tool designed for the handling of prostate biopsy specimens and is intended for maximal tissue preservation as well as for accurate localization and orientation of the biopsy cores.
The main objective of the current study was to evaluate the impact of the SmartBx™ system on the detection rate of PCa.
SmartBx™ is a semiautomatic device which enables downloading the biopsy core from the biopsy needle while maintaining its unity and orientation (Fig. 1). The SmartBx™ cassette comprises a Nylon-based membrane which allows non-covalent binding with the biopsy tissue via hydrophobic and charge-based interactions. This binding does not result in any modifications to the tissue. The membrane carrying the biopsy cores is designed to go through the standard fixation and embedding processes.
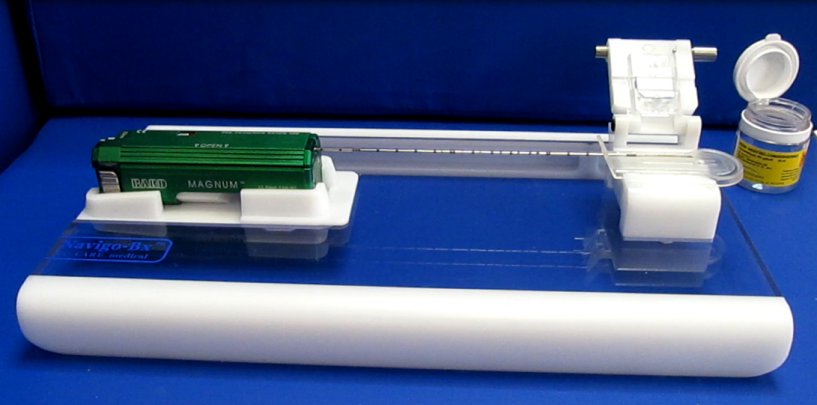 Fig. 1.
Fig. 1.The SmartBx™ needle with the gun.
The study was approved by the local ethical committee and all patients signed a written informed consent (Institutional Review Board no. BNZ-0053-11). We performed a prospective data collection for the study group which included patients with clinically suspected PCa that were referred to TRUS-guided biopsy in our hospital from 2011 to 2017. The results were compared to a control group who underwent TRUS-guided biopsy during the same years without the use of SmartBx™, and their data were collected retrospectively.
In the study group, biopsies obtained by SmartBx™ were downloaded by the urologist into a formalin-filled container, with each cassette containing two cores. In the control group, biopsy cores were downloaded by shaking the needle directly into a formalin-filled container and two floating cores were preserved in each container.
All the biopsies were performed by a single urologist and sent to the local pathology lab and managed by the same standard tissue processing, and diagnosed by the same pathologists.
The detection rate was defined as the number of patients diagnosed with PCa divided by the total number of the patients in each group. Moreover, because of variation in the total number of cores, we calculated the detection rate per core by dividing the positive cores on the total number of the cores in each group.
The initial core length was documented on the needle notch using uEye camera (Imaging Development Systems, Obersulm, Germany), and measured again on the slide. From these measurements we calculated the percentage of biopsy tissue preservation. T-test was used to compare between continuous variables, and Chi-Square was used to compare between categorical variables. Statistically significant differences were defined as p value of < 0.05. All statistical analyses were performed using the SAS system.
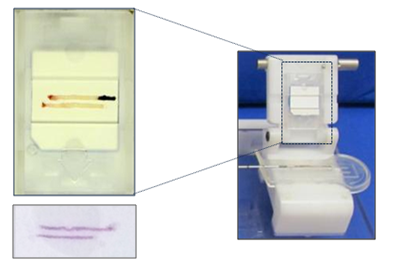 Fig. 2.
Fig. 2.Two blopsy cores. The image on the right shows the needle crib. The left image shows two cores on a cassette.
Six-hundred patients were included in the study, 300 in each group. Table 1 shows that there were no statistically significant differences in baseline characteristics between the two groups including age, PSA, digital rectal exam and prostate volume.
| SmartBx™ (n = 300) | Control (n = 300) | P value | |
|---|---|---|---|
| Mean age (years) | 65.2 ± 8.5 | 65.8 ± 7.6 | 0.35 |
| PSA (ng/mL) | 8.8 ± 10.5 | 9.0 ± 9.5 | 0.8 |
| PSA density (ng/mL2) | 0.17 ± 0.24 | 0.15 ± 0.17 | 0.23 |
| Prostate volume (cc) | 65.0 ± 36.0 | 68.8 ± 40.9 | 0.2 |
| Abnormal DRE | 45.3% | 47.3% | 0.6 |
PSA - Prostate-specific antigen. DRE - Digital rectal examination.
The average core number obtained per patient was 13.0 ± 2.7 and 14.1 ± 4.4 (P = 0.001) in the SmartBx™ and control groups, respectively. The use of SmartBx™ system resulted in 1.13 ± 4.07 mm longer tissue core (12.00 ± 2.80 mm vs. 10.87 ± 2.96 mm, P = 0.001) available for pathological evaluation compared with the standard system. This indicated a 21.2% better biopsy specimen preservation (84.5% vs. 63.3%).
The detection rate in the study group was higher than in the control group (37.7% vs. 30.3%) although statistical significance was not attained (P = 0.06). The detection rate per core was substantially higher in the SmartBx™ group compared with the control group (14.1% vs. 8.1%, P = 0.001), as shown in Table 2. The latter Table also shows the differences in the detection rates stratified by Gleason score (GS) and Grade groups (GG). It should be noted that higher rates of GS 4 + 3 (GG III) were detected in the study group (44.1% vs. 12.5%, P = 0.01).
| SmartBx™ (n = 300) | Control (n = 300) | P value | |
|---|---|---|---|
| Average core number per patient | 13.0 ± 2.7 | 14.1 ± 4.4 | 0.001 |
| Biopsy length on the slide (mm) | 12 ± 2.8 | 10.87 ± 2.96 | 0.001 |
| Percentage of biopsy preservation | 84.5% | 63.3% | 0.01 |
| Detection rate | 37.7% | 30.3% | 0.06 |
| Detection rate per core | (548/3892) 14.1% | (342/4239) 8.1% | 0.01 |
| Detection rate by GS (GG) | |||
| 6 (I) | 33.0% (n = 37) | 37.8 (n = 34) | 0.48 |
| 7 = 3 + 4 (II) | 21.4% (n = 24) | 38.9% (n = 35) | 0.01 |
| 7 = 4 + 3 (III) | 17.0% (n = 19) | 5.6% (n = 5) | 0.01 |
| 8 (IV) | 10.7% (n = 12) | 19.0% (n = 9) | 0.08 |
| 9-10 (V) | 17.9% (n = 20) | 7.8% (n = 7) | 0.04 |
GS = Gleason Score. GG = ISUP Grade Group.
Although being the gold-standard procedure for diagnosing PCa, TRUS-guided prostate biopsy has a detection rate of less than 50% [13, 14]. Every effort should be invested to maximize the detection rate, including proper processing of the specimen, which have been shown to improve its quality for proper pathological examination [15, 16].
Core length is proportionally related to better diagnosis and higher detection rate [9, 17]. Specimen observation is also related to improved pathological examination [8].
In our current study, we showed that using SmartBx™ system resulted in a 1.13 mm longer core in average, and 21.2% more biopsy tissue was preserved when compared to standard biopsy. This was eventually translated into higher detection rate per core. It should be mentioned that the overall detection rate, which was higher in the study group, did not reach statistically significance, though it was nearly attained (P = 0.06). This could be explained by the fact that the standard group had more cores than the study group.
One more interesting fact was the higher proportion of GS 4 + 3 (GG III) in the study group and the higher proportion of GS 3 + 4 (GG II) in the control group. We do not know the reason for this difference, however, it could be related to the fact that the longer and better-preserved tissue in the SmartBx™ group enabled the pathologists to detect a higher proportion of Gleason pattern 4, which differentiates between GS 3 + 4 (GG II) and 4 + 3 (GG III). This is important because of the different prognosis of these two groups, which differentiates patients between favorable and unfavorable intermediate risk PCa by NCCN tables [7].
Our study has some limitations, the main of which was the fact that there was no randomization. Moreover, data on the control group was obtained retrospectively. The number of patients in each group is relatively small, and as such could miss other statistically significant differences between the groups. However, our study strength points were the facts that all the biopsies were performed by the same surgeon and all the specimens were examined by the same pathologist. Moreover, the data on the study group were collected prospectively.
In conclusion, this study showed that the use of SmartBx™ system preserved more tissue and core-length, improved detection rate per core, and increased detection rate of GS 4 + 3 (GG III).
We would like to express my gratitude to all those who helped me during the writing of this manuscript.
The authors declare no conflict of interest.