



 , Ana Paula O. Barbosa 1,†, João Vítor E. H. Szortyka 1, Adriana T. de Lemos 2, Felipe de S. Stigger 2,*
, Ana Paula O. Barbosa 1,†, João Vítor E. H. Szortyka 1, Adriana T. de Lemos 2, Felipe de S. Stigger 2,*
1 Undergraduate Physiotherapy Program, Federal University of Health Sciences of Porto Alegre, 90050-170 Porto Alegre, Rio Grande do Sul, Brazil
2 Department of Physiotherapy, Federal University of Health Sciences of Porto Alegre, 90050-170 Porto Alegre, Rio Grande do Sul, Brazil
†These authors contributed equally.
Abstract
Functional mobility, which encompasses movements required for everyday activities, involves the ability to perform two tasks simultaneously, a concept known as dual-tasking (DT). The impact of interference between these tasks is observed by comparing the performance of a single task with that of the same task when associated with a second task, known as the dual-task effect (DTE). The decline in these functions due to aging and the associated increase in DTE might impair basic functions involving mobility, consequently increasing the risk of falls. Thus, this study aims to evaluate the DTE in functional mobility tasks across young, middle-aged, and older adults and to examine how different types of secondary tasks affect DT performance.
This laboratory-based cross-sectional observational study involved forty-four young adults (32.5 ± 6.9 years), thirty-five middle-aged adults (54.6 ± 6.3 years), and twenty-eight older adults (73.9 ± 7.0 years). DT conditions included performing three functional mobility tasks (the 3-meter Walking Test, Figure-8 Walk, and Four Square Step Test) alone and simultaneously with four different secondary tasks [Coin Transference (CTT), Stroop Color Word (SCWT), Digit Span (DST), and Semantic Verbal Fluency (SVFT) tasks]. The time taken to complete the mobility tasks was measured, while performance on secondary tasks was assessed based on the CTT rate, number of errors (SCWT and DST), and rate of recalled words (SVFT). The DTE was calculated, and patterns of dual-task cost were analyzed across all task conditions.
Decreases in functional mobility performance during dual-task performance were observed across all experimental groups. Older adults took longer to perform complex tasks involving turning and anterior/lateral/posterior displacements during dual-task conditions compared to young and middle-aged adults. The CTT and SCWT caused a high level of interference under dual-task conditions, while the SVFT and DST induced reduced impairments in functional mobility tasks. Most dual-task conditions led to “mutual interference”, where participants performed worse on both the primary and secondary tasks in the dual-task conditions.
All primary functional mobility tasks experienced interference under dual-task conditions. The relationship between dual motor and cognitive tasks may depend on the difficulty level presented to a given population. This study highlights the importance of understanding dual-task interference to develop targeted interventions for reducing fall risk, especially in older adults.
Keywords
- physical functional performance
- executive function
- motor skills
- multitasking behavior
- gait
- aged
Aging diminishes the adaptability of the body to physical and environmental stresses, thereby increasing the risk of falls [1, 2]. In fact, previous studies indicate that 30% of adults over 65 years experience one or more falls each year [3], with most of them occurring during daily mobility tasks, leading to dramatic consequences such as injury, fear, decreased mobility, and morbidity [4]. Evidence suggests a connection between cognitive functioning and fall risk [5]. As individuals age, the nervous system undergoes changes in processing visual, proprioceptive, vestibular, and cognitive information, resulting in limitations in functional mobility [2, 6]. Age-related alterations in the frontal lobe are associated with impaired executive function [7, 8]. Since executive function is responsible for planning, attention, working memory, reasoning, and problem solving, it enables individuals to perform tasks concurrently [8, 9].
Older adults are often required to perform multiple tasks simultaneously. The ability to do so is crucial for effective communication, object handling, and environmental monitoring, all of which help mitigate potential mobility risks [10], and thereby support independence [11]. This capacity to manage two distinct tasks with different goals and strategies is referred to as dual-task performance. Dual-task performance involves performing a primary task alongside a secondary task, which may be either cognitive or motor [10]. Common cognitive tasks in dual-task paradigms include the Stroop Color Word Test (SCWT), which assesses inhibitory control [12]; the Digit Span Test (DST), which engages attention and working memory [13, 14]; and the Semantic Verbal Fluency Test (SVFT), which evaluates semantic memory [15]. In contrast, manual tasks, such as transferring a coin from one pocket to another [16], involve recruitment of both motor and cognitive systems [17].
Compared to single-task conditions, where tasks are performed independently, the concurrent execution of a secondary task can reduce the performance of one or both tasks, a phenomenon known as dual-task interference [17]. Distinct theories of information processing that are not mutually exclusive explain these impairments. Capacity-sharing theory suggests that the brain is a limited-capacity parallel processor that divides resources between tasks, while bottleneck theory argues that central processes occur sequentially, handling one task at a time [18, 19, 20]. The theory of multiple resources proposes that dual-task performance is more likely to be impaired when tasks share functional resources or common structures [21, 22].
Understanding the effects of dual-task performance is clinically relevant, as it impacts not only mobility but also daily activities, independence, fall risk, and community participation [11, 17, 23, 24]. How attentional resources are allocated during dual-tasking is crucial, as it may vary with task priority and is influenced by age-related cognitive changes [25]. Previous observational cross-sectional studies on aging and dual-task performance have often used a limited number of dual-task conditions and convenience samples of young and/or older adults. Few studies have investigated age-related differences in dual-task performance in middle-aged groups [26]. Thus, including a middle-aged sample and diverse dual-task conditions that vary in nature and complexity could provide a better understanding of how aging affects daily activities involving both motor and cognitive interactions [27]. Furthermore, as dual-task gait performance might be an early indicator of accelerated brain aging or otherwise presymptomatic neurodegenerative conditions [28], studying middle-aged individuals presents a unique opportunity to identify early risk factors before the onset of more pronounced age-related decline. Hence, the present study aimed to: (a) explore the impact of multiple attention-demanding tasks on functional mobility in young, middle-aged, and older adults, comparing the magnitude of dual-task interference across these age groups; and (b) examine how the complexity and type of primary and secondary tasks influence dual-task performance, identifying patterns of interference in both tasks across age groups. We hypothesized that: (a) cognitive demand during dual-tasking will negatively affect functional mobility across all groups, with older adults experiencing the greatest dual-task interference, and (b) as the type and complexity of both primary and secondary tasks increase, dual-task interference will also intensify. The degree and nature of this interference are expected to vary according to movement pattern demands (e.g., linear and curved gait or anterior, lateral, and posterior displacements) and the specific domain of the secondary tasks (e.g., non-executive vs. executive function tasks). Furthermore, we hypothesized that patterns of dual-task interference will differ across distinct groups, with age potentially modulating the interference experienced during the simultaneous execution of tasks.
The findings of this study could have practical applications in real-world settings such as fall prevention programs and rehabilitation. By understanding how dual-task interference varies across tasks and age groups, interventions can be developed to address the specific cognitive and motor challenges faced at distinct environment walking demands and different stages of life. These insights could help inform the design of tailored strategies to improve mobility, balance, and multitasking abilities, ultimately reducing fall risk and enhancing the quality of life, particularly among older adults and those at risk of mobility decline.
This laboratory-based, cross-sectional observational study was approved by the Research Ethics Committee (CAAE number 57415416.3.0000.5345). All participants provided written informed consent in accordance with the Declaration of Helsinki prior to data collection. No incentives were provided to participate in the study.
Between June 1, 2019, and November 30, 2020, 107 participants of both sexes were recruited and categorized by age: (a) young adults (YG), aged 20–44 years; (b) middle-aged adults (MG), aged 45–64 years; and (c) older adults (EG) aged 65 years or older. Participants were recruited using the snowball sampling technique and included if they: (a) were independent in activities of daily living, (b) could walk without assistance, (c) were able to provide self-reported data, and (d) could understand and sign an informed consent form. The exclusion criteria included musculoskeletal, metabolic, or cardiac disorders, as well as visual or hearing impairments that could interfere with the experiment.
The sample size was estimated using GPower 3.1 software (Franz Faul,
Universität Kiel, Germany). A moderate effect size (ES) was adopted for
dual-task effects (DTE) in all studied tasks (dz = 0.55). Using a matched pairs
model, power (ß-1) = 0.80,
After confirming the eligibility of the participants, all participants provided informed consent in accordance with the Helsinki Declaration. Next, all participants completed a short questionnaire (age, sex, weight, height, marital status, and years of education) and medical condition (health status and self-reported number of falls within the past 60 days) as well as the International Physical Activity Questionnaire–Short Form (IPAQ-SF) and the Montreal Cognitive Assessment (MoCA). Subsequently, the participants attended a single session for data collection.
Three mobility tests were chosen as primary tasks (Fig. 1): (a) 3-meter Walk Test (3MWT) [29, 30]; (b) Figure-8 Walk Test (F8WT) [31]; and (c) Four Square Step Test (4SST) [32, 33]. These tests were chosen considering that mobility-related steps in daily activities consist of walking in different strategies, such as straight line, turning, and anterior/posterior/lateral displacements. In addition, these tests are validated and can be performed in an office setting without sophisticated technical equipment, which is ideal for widespread clinical use.
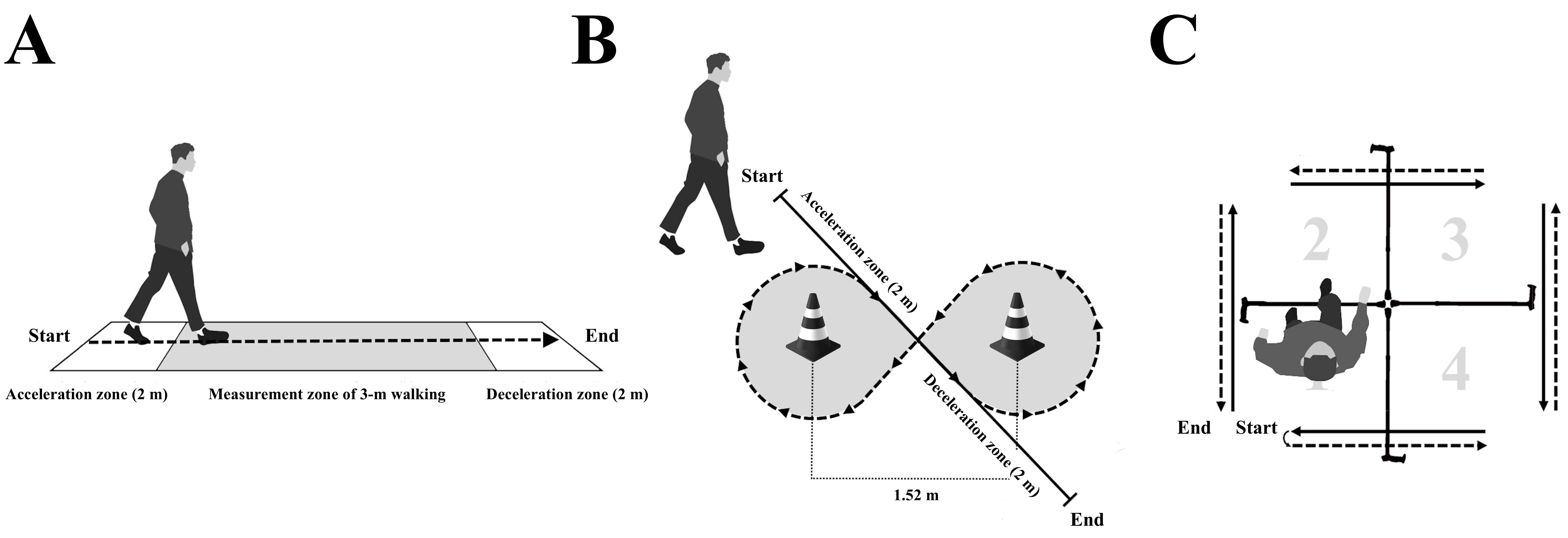 Fig. 1.
Fig. 1.
Primary mobility tasks. Visual schematic of the mobility tests procedures chosen as primary tasks illustrating: (A) 3-meter Walk Test; (B) Figure-8 Walk Test; and (C) Four Square Step Test. Arrows illustrate the direction of the walking path. Note: m, meters.
During the 3MWT, participants were required to walk on a 3 m walkway without assistance (Fig. 1A). The participants were timed from the moment their foot crossed the initial line of the measurement zone to the moment their foot crossed the final line of the measurement zone and the total course. For the F8WT, participants were instructed to walk a figure-of-8 around two cones placed 1.52 m apart and then stop upon to the final position (Fig. 1B). Participants were timed from the moment they first crossed the midpoint between the two cones until the moment they crossed it for the last time. During the 3MWT and F8WT, distances were provided at the beginning and end of the timed walkway (2 m) to allow participants to accelerate or decelerate outside the data collection area to reduce gait variability introduced during these phases. Finally, for the 4SST, participants were instructed to step forward, backward, and sideways in a predetermined sequence over four walking canes of the same width, placed in a cross configuration on the ground. The participants were instructed to start in square 1, facing square 2. Then, facing this direction, step into squares 2, 3, 4, 1, 4, 3, 2, and back to 1 (Fig. 1C). The time required to complete each sequence was recorded. During both the 3MWT and F8WT, participants were instructed to walk at their comfortable, usual pace. For the 4SST, the participants were asked to complete the specified sequence as quickly as possible without hitting the equipment. All participants executed each test once for familiarization before the data recording.
One motor task and three cognitive tasks were selected as the secondary tasks.
Coin Transference test (CTT) was chosen as the secondary motor task [16, 34]. This
task was selected considering that it mimics various tasks commonly used in the
natural context of daily life activities, such as walking while searching for
keys in a purse or manipulating objects while walking. For the CTT, participants
were instructed to transfer 10 coins of 50 cents (Brazilian currency) once at a
time, with the dominant hand, from the pocket on the nondominant side to the
pocket on the dominant side. A specific apron was made for this test with two
different sizes (50
Cognitive secondary tasks included: (a) the SCWT; (b) the DST; and (c) the SVFT. These secondary tasks were employed because they are commonly used to evaluate the presence of cognitive impairment in older adults and have previously been used to explore dual-task performance during walking. Also, SCWT involves speed processing, executive functioning, and inhibitory control [35, 36], that are particularly important when navigating complex environments such as walking on a busy street, where there are multiple potential distractions or hazards. Conversely, DST reflects the everyday attention and/or memory demands faced by older adults [14], such as remembering sequences of directions, managing phone numbers or appointments, and holding multiple pieces of information while engaging in daily tasks. In addition, the SVFT, which assesses semantic memory, requires participants to retrieve words from their mental lexicon, focus on the task, select words that meet specific criteria, and avoid repeating words-all of which clearly involve language, semantic declarative memory, storage capacity, retrieval and executive processes [37].
Prior to the SCWT, the visual and color discrimination abilities were tested. For color discrimination, participants were presented with colored rectangles (yellow, blue, black, red, and green) and were asked to identify each color. Next, for visual ability, participants were presented to a page with 44 words (color names) divided into four columns, printed in black, and instructed to read the words. During the SCWT trial, a similar page was used; however, on the trial page, the color names were painted so that colors and words did not match. Participants were instructed to say out the printed font color loud, without reading the color name, of all words on the page as fast as possible. The examiner instructed the participants to not interrupt the test if errors occurred. The number of incorrect responses was recorded. A greater number of errors suggests a worse performance [38, 39]. For the DST, participants were instructed to remember, after a brief delay, a series of digits, and repeat it in the same order. Initially, the number of digits to be repeated was individually adjusted for each participant’s forward digit span. This number was determined by the longest digit span the subject could recall after a delay equivalent to the average time to perform the primary mobility task [40]. The number of errors was recorded. Finally, for the SVFT, participants were asked to recall as many words as possible from a randomly predetermined category (e.g., animals or fruits) for 30 s. The rate of generated words per minute was calculated using a simple rule of three. A large number of words recalled per minute indicated better performance [41, 42].
Secondary CTT tasks during the single-task condition were performed in an upright position, whereas secondary SCWT, SVFT, and DST tasks were performed in a seated position. The performance of secondary tasks was individually adjusted for each functional mobility task combination to match the corresponding dual-task time [27].
The dual-task paradigm in this study involved an experimental setup in which participants first performed each primary mobility task individually, followed by a combination of each primary task with one of the selected secondary tasks in a dual-task condition. This approach allowed for the comparison of participants’ performance in the single-task and dual-task conditions. Therefore, twelve experimental combinations were: (a) 3MWT+CTT; (b) 3MWT+SCWT; (c) 3MWT+DST; (d) 3MWT+SVFT; (e) F8WT+CTT; (f) F8WT+SCWT; (g) F8WT+DST; (h) F8WT+SVFT; (i) 4SST+CTT; (j) 4SST+SCWT; (k) 4SST+DST; and (l) 4SST+SVFT. The order of the tasks for each participant was chosen randomly to avoid performance bias. No instructions were given on which task to prioritize during the dual-task condition to establish a real-life ecological situation [43].
The evaluators received proper training and a standard operating procedure was followed to ensure that the instructions were delivered to participants consistently. Primary and secondary tasks were recorded during both single- and dual-task performances. A single blinded assessor, who was unaware of the study’s objectives and hypotheses, reviewed and scored all the videos.
Primary outcome measures consisted of absolute and relative values of primary and secondary task performance. The absolute values included the time to complete functional mobility tasks (3MWT, F8WT, and 4SST [in seconds]), CTT rate, number of incorrect responses (SCWT and DST), and number of generated words per minute (SVFT) during single and dual-task performance.
DTE is a relative measure consisted of the comparison of dual- and single-task performance and was calculated for each of the primary and secondary tasks [44]. Considering that for the 3MWT, F8WT, 4SST, SCWT, and DST tasks, higher values represent worse performance, DTEs were calculated by multiplying the original formula by a negative one (–1). Thus, negative values could indicate that performance was worse in the dual-tasking (DT) condition than in the Single-task performance (ST) condition [45].
Age, years of education, height, weight, body mass index, number of falls, MoCA
scores, self-reported physical activity levels, functional mobility task
performance, and secondary task performance were presented as means and standard
deviations (SDs). Sex was expressed as the total number and percentage. Data
normality was verified using the Shapiro–Wilk test. A one-way analysis of
variance (ANOVA), followed by Bonferroni’s test, was used to compare sample
characteristics between groups. Comparisons between tasks (single, dual tasks,
and DTE) and between groups (young, middle-aged, and older adults) were performed
using a mixed ANOVA. In addition, repeated measures analysis of covariance (ANCOVA) was performed for
comparisons between tasks (single and dual tasks) with years of education as a
covariate. Adjusted p-values, using Greenhouse–Geisser values, were
examined if the assumption of sphericity was not tenable, as demonstrated by
Mauchly’s test of sphericity. Bonferroni’s post hoc analysis was performed for
significant results considering a p
The demographic characteristics and results of the physical status and cognitive
measurements of all the participants are summarized in Table 1. Twenty-eight
older adults (mean age 73.9
| Characteristics | Younger (N = 44) | Middle-aged (N = 35) | Older (N = 28) |
| Age (years), mean (SD) | 32.5 (6.9) | 54.6 (6.3)1 | 73.9 (7.0)1,2 |
| Male, n (%) | 23 (52.3) | 9 (25.7)1 | 6 (21.4)1 |
| Female, n (%) | 21 (47.7) | 26 (74.3)1 | 22 (78.6)1 |
| Education (years), mean (SD) | 18.9 (4.1) | 17.2 (5.6) | 15.0 (7.8)1 |
| Height (m), mean (SD) | 1.7 (0.1) | 1.6 (0.1)1 | 1.6 (0.0)1 |
| Weight (kg), mean (SD) | 76.7 (17.1) | 73.6 (13.0) | 74.6 (20.6) |
| BMI (kg/m2), mean (SD) | 25.5 (4.7) | 26.8 (4.2) | 27.4 (4.3) |
| Falls past 60 days, mean (SD) | 1.0 (0.1) | 1.0 (0.2) | 1.0 (0.1) |
| MoCA score (M, SD) | 27.0 (1.9) | 26.7 (1.7) | 24.8 (2.3)1,2 |
| IPAQ [(MET)-min/week], mean (SD) | 2357.1 (2586.2) | 4358.7 (4030.8) | 5810.6 (4525.4)1 |
Note: BMI, body mass index; N, sample; M, mean; SD, standard deviation; n,
number; m, meters; kg, kilogram; kg/m2, kilograms per square meter; MoCA,
Montreal Cognitive Assessment (a total score of
1 Significant difference compared to younger adults, p
2 Significant difference compared to middle-aged adults, p
Functional mobility performance under single and dual-task conditions is shown in Fig. 2 and Table 2. A mixed factorial ANOVA revealed significant differences across the five 3MWT conditions (single or dual-task) (F(3.4, 354.5) = 48.4, p = 0.000), as well as significant differences between groups (F(2, 104) = 5.8, p = 0.004) in the time to complete the task. An interaction between experimental conditions and group was also observed in the 3MWT performance (F(6.8, 354.56) = 2.0, p = 0.049). Post hoc comparisons indicated that all secondary tasks affected 3MWT performance in young and older participants. DST was the only secondary task that did not impact 3MWT performance in middle-aged adults. Furthermore, older adults took longer to complete the 3MWT compared to middle-aged adults across all dual-task conditions. Additionally, when the 3MWT was associated with the SCWT, older adults took longer to complete the mobility task compared to young participants.
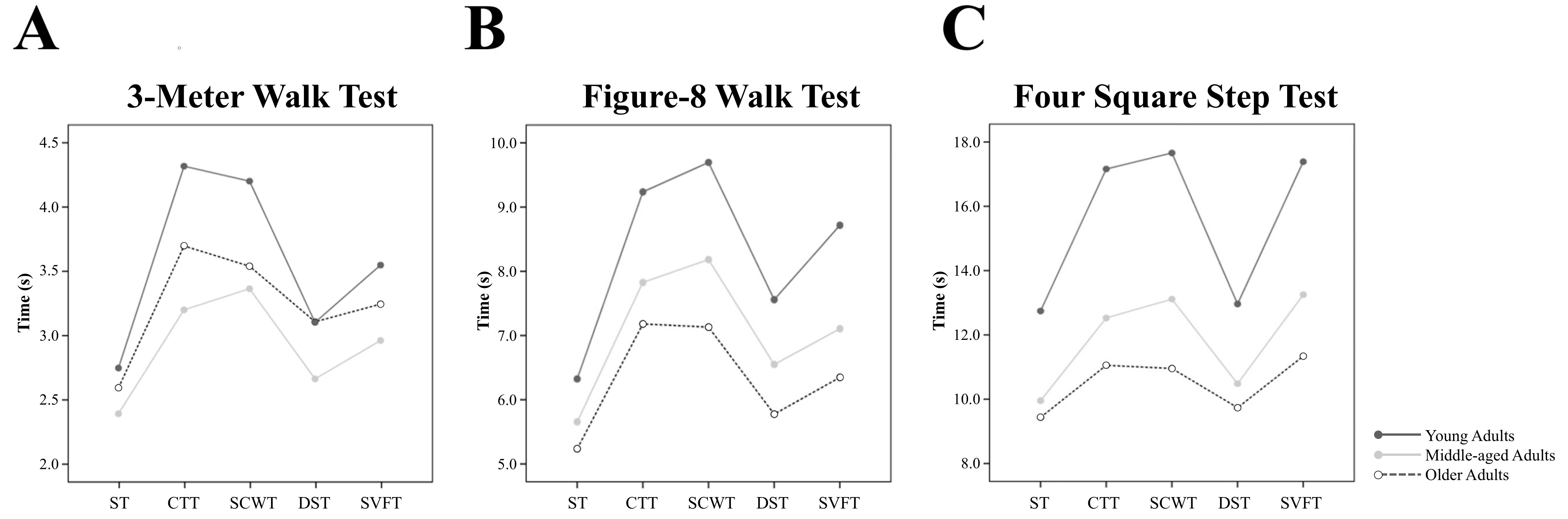 Fig. 2.
Fig. 2.
Primary mobility tasks performance on experimental single-task and dual-tasks conditions. (A) 3-meter Walk Test; (B) Figure-8 Walk Test; and (C) Four Square Step Test. Functional mobility performance of young (white circles), middle-aged (light grey circles) older (dark grey circles) adults on experimental single-task and dual-tasks conditions. Note: ST, Single-task performance; CTT, Coin transference test; SVFT, Semantic verbal fluency test; DST, Digit span test; SCWT, Stroop Color Word Test.
| Variable | Single-task performance | Dual-task performance | ||||
| Coin transference | Stroop color word | Digit span | Semantic verbal fluency | |||
| 3-Meter walk test, time (m/s), mean (SD) | ||||||
| Younger | 2.6 (0.8) | 3.7 (1.2)3 | 3.5 (1.2)3 | 3.1 (1.2)3 | 3.2 (1.2)3 | |
| Middle-aged | 2.4 (0.4) | 3.2 (0.5)3 | 3.3 (0.7)3 | 2.6 (0.5) | 2.9 (0.5)3 | |
| Older | 2.7 (0.6) | 4.3 (1.9)2,3 | 4.1 (1.0)1,2,3 | 3.1 (0.7)2,3 | 3.5 (0.9)2,3 | |
| Figure-8 walk test, time (s), mean (SD) | ||||||
| Younger | 5.2 (1.6) | 7.1 (1.7)3 | 7.1 (1.7)3 | 5.7 (1.5) | 6.3 (1.7)3 | |
| Middle-aged | 5.6 (1.0) | 7.8 (1.6)3 | 8.1 (1.5)1,3 | 6.5 (1.2)1,3 | 7.1 (1.4)3 | |
| Older | 6.3 (1.4)1 | 9.2 (2.0)1,2,3 | 9.6 (2.3)1,2,3 | 7.5 (1.5)1,2,3 | 8.7 (2.3)1,2,3 | |
| Four square step test, time (s), mean (SD) | ||||||
| Younger | 9.4 (2.8) | 11.0 (2.0)3 | 10.9 (2.1)3 | 9.7 (1.8) | 11.3 (3.0)3 | |
| Middle-aged | 9.9 (2.4) | 12.5 (3.0)3 | 13.1 (3.1)1,3 | 10.5 (1.9) | 13.2 (2.8)1,3 | |
| Older | 12.7 (2.7)1,2 | 17.1 (5.0)1,2,3 | 17.6 (4.4)1,2,3 | 12.6 (2.5)1,2 | 17.4 (4.3)1,2,3 | |
Note: Younger (n = 44); Middle-aged (n = 35); Older (n = 28); s, seconds.
1 Significant difference compared to younger adults, p
2 Significant difference compared to middle-aged adults, p
3 Significant difference compared to single-task performance, p
Mixed factorial ANOVA also revealed significant differences across the five F8WT conditions (F(3.5, 367.1) = 99.4, p = 0.000) and between groups (F(2, 104) = 17.4, p = 0.000) in the time to complete the task. A significant interaction between experimental conditions and group was also observed (F(7.0, 367.1) = 2.5, p = 0.014). Post hoc comparisons indicated that older adults took longer to complete the F8WT under single-task conditions compared to younger participants. However, no significant differences in F8WT performance were observed between young and older adults when compared to middle-aged participants. Additionally, comparisons showed that the time to complete the F8WT was differently impacted by secondary tasks across the groups. In young adults, only the DST did not affect the time to complete the F8WT. In contrast, all secondary tasks impacted the F8WT performance in older and middle-aged adults. Furthermore, older adults’ performance on the F8WT was significantly worse across all secondary tasks compared to both young and middle-aged participants.
Similarly, mixed factorial ANOVA revealed significant differences across the five 4SST conditions (F[3.5, 367.6] = 57.3, p = 0.000), between groups (F[2, 104] = 44.5, p = 0.000), and a significant interaction between experimental conditions and group (F[7.0, 367.6] = 5.1, p = 0.000) in the time to complete the task. Post hoc comparisons showed that older adults had the worst performance on the 4SST during single-task conditions compared to both young and middle-aged participants. No differences in 4SST performance during single-task were found between young and middle-aged adults. Once again, the time to complete the 4SST was differently impacted by secondary tasks across groups. While the DST did not affect the time to complete the 4SST in any group, older adults demonstrated the longest completion time. The SWCT, CTT, and SVFT affected the performance of all groups, but older adults showed the worst performance compared to both young and middle-aged adults.
Given the differences in years of education between the older and younger groups, and considering that education level has been shown to influence dual-task performance [27], we conducted a repeated measures ANCOVA with years of education as a covariate. However, years of education did not significantly affect functional mobility performance: 3MWT (F(1, 103) = 0.01, p = 0.916), F8WT (F(1, 103) = 0.04, p = 0.834), and FSST (F(1, 103) = 0.96, p = 0.329).
Finally, considering the differences in the proportion of women observed in the middle-aged and older groups compared to the young group, comparisons between tasks (single-task, dual-task, and DTE), groups (young, middle-aged, and older adults), and sex were performed using mixed factorial ANOVA. The results revealed no significant interaction between sex and dual-task conditions on the 3MWT (F[4, 404] = 0.2, p = 0.890), F8WT (F[1, 101] = 0.0, p = 0.914), or 4SST (F[1, 101] = 0.0, p = 0.968). Additionally, no significant effects were found for the interaction of sex, dual-task condition, and group on the 3MWT (F[8, 404] = 0.7, p = 0.609), F8WT (F[1, 101] = 0.0, p = 0.914), or 4SST (F[2, 101] = 0.1, p = 0.859).
DTEs on functional mobility performance are presented in Table 3. A mixed factorial ANOVA revealed a significant effect of task condition on DTEs across all mobility tasks: (a) 3MWT (F[2.7, 290.9] = 30.0, p = 0.000); (b) F8WT (F[2.4, 254.8] = 30.0, p = 0.000); and (c) 4SST (F[2.6, 276.2] = 41.5, p = 0.000). No significant differences in DTEs were observed between groups, and no interaction between experimental conditions and group was found for the 3MWT and F8WT. However, for the 4SST, a significant interaction between task condition and group on DTEs was observed (F[5.3, 276.2] = 2.7, p = 0.016). Despite this interaction, no main effect of group on the 4SST DTEs was detected (F[2, 104] = 1.0, p = 0.350). Post hoc comparisons indicated that older adults exhibited higher DTEs on the 4SST during the SCWT compared to young participants.
| Variable | Dual-task Effect | ||||
| Coin transference | Stroop color word | Digit span | Semantic verbal fluency | ||
| 3-Meter walk test, DTE (%), mean (SD) | |||||
| Younger | –47.9 (47.2)3,4 | –41.8 (45.8)3,4 | –24.9 (46.6)1,2 | –30.1 (47.5)1 | |
| Middle-aged | –36.0 (26.7)3,4 | –41.6 (27.7)3,4 | –12.7 (21.3)1,2 | –26.2 (29.2) | |
| Older | –59.8 (61.5)3,4 | –57.4 (44.0)3,4 | –16.0 (30.9)1,2,4 | –31.7 (35.8)1,2 | |
| Figure-8 walk test, DTE (%), mean (SD) | |||||
| Younger | –48.2 (59.5)3,4 | –46.7 (51.8)3,4 | –18.6 (45.3)1,2,4 | –30.5 (47.6)1,2,3 | |
| Middle-aged | –40.0 (25.5)3 | –46.1 (24.3)3,4 | –16.8 (16.6)1,2,4 | –26.7 (20.1)2,3 | |
| Older | –52.4 (59.9)3 | –57.8 (47.5)3,4 | –23.7 (36.1)1,2,4 | –42.1 (47.8)2,3 | |
| Four square step test, DTE (%), mean (SD) | |||||
| Younger | –22.9 (30.0)3 | –20.6 (22.9)3 | –7.4 (21.7)1,2,4 | –23.9 (28.6)3 | |
| Middle-aged | –28.3 (28.7)3 | –34.9 (31.1)3 | –8.3 (21.6)1,2,4 | –37.2 (33.7)3 | |
| Older | –37.6 (39.7)3 | –42.2 (37.5)3,5 | –4.1 (21.1)1,2,4 | –41.8 (44.5)3 | |
Note: Younger (n = 44); Middle-aged (n = 35); Older (n = 28); DTE, dual-task effect.
1 Significant difference compared to coin transference task, p
2 Significant difference compared to stroop color word task, p
3 Significant difference compared to digit span task, p
4 Significant difference compared to semantic verbal fluency task, p
5 Significant difference compared to younger adults, p
A repeated measures ANCOVA with years of education as a covariate was conducted to examine its effect on DTEs. The results showed no significant effect of years of education on any of the DTEs: 3MWT (F(1, 103) = 0.06, p = 0.795), F8WT (F(1, 103) = 0.01, p = 0.978), and FSST (F(1, 103) = 0.28, p = 0.592).
The performance of all secondary tasks during single- and dual-task conditions is shown in Table 4. A mixed factorial ANOVA revealed significant differences in the number of errors across the four SCWT conditions (F[2.2, 234.7] = 7.5, p = 0.000) and between groups (F[2, 104] = 17.2, p = 0.000). Additionally, a significant interaction between experimental conditions and groups was observed (F[4.5, 234.7] = 3.2, p = 0.009). Post hoc comparisons indicated that older adults made more errors during the single-task SCWT compared to both young and middle-aged participants, with no significant difference between the latter two groups. During dual-task conditions, the number of errors was not significantly impacted by mobility tasks in young or middle-aged participants. However, while older adults showed a reduction in errors during all mobility tasks, their error rate during F8WT and 4SST remained higher compared to both young and middle-aged participants. Similarly, during the 3MWT, older adults made more errors than young participants.
| Variable | Single-task performance | Dual-task performance | |||
| 3 m walking test | Figure-8 walking test | Four square step test | |||
| Stroop color word, errors (n), mean (SD) | |||||
| Younger | 0.4 (0.6) | 0.2 (0.5) | 0.3 (0.6) | 0.4 (0.5) | |
| Middle-aged | 0.9 (1.3) | 0.7 (1.0) | 0.4 (0.7) | 0.6 (0.8) | |
| Older | 2.5 (3.3)1,2 | 0.9 (1.6)1,3 | 1.3 (1.2)1,2,3 | 1.3 (1.7)1,2,3 | |
| Coin transference, transfer rate (coins/min), mean (SD) | |||||
| Younger | 18.4 (3.9) | 11.3 (10.1)3 | 14.5 (5.8)3 | 11.2 (3.9)3 | |
| Middle-aged | 18.4 (3.5) | 15.3 (11.0) | 15.8 (6.0)3 | 13.3 (4.4)3 | |
| Older | 16.2 (2.6)1,2 | 19.5 (19.7)1 | 15.4 (7.5) | 11.6 (4.0)3 | |
| Digit span, errors (n), mean (SD) | |||||
| Younger | 5.4 (1.3) | 4.7 (1.1) | 4.6 (1.2) | 5.0 (1.0) | |
| Middle-aged | 4.7 (0.9) | 4.5 (1.0) | 4.3 (0.8) | 4.5 (0.8) | |
| Older | 4.5 (1.1) | 3.9 (0.7) | 3.6 (1.1) | 4.1 (0.9) | |
| Semantic verbal fluency, generated words (n/min), mean (SD) | |||||
| Younger | 16.2 (4.3) | 8.5 (2.9) | 13.2 (3.1) | 14.8 (3.5) | |
| Middle-aged | 15.8 (3.1) | 7.9 (1.5) | 11.6 (3.4) | 14.6 (2.5) | |
| Older | 13.6 (3.4) | 7.5 (1.7) | 11.6 (3.6) | 14.6 (2.4) | |
Note: Younger (n = 44); Middle-aged (n = 35); Older (n = 28).
1 Significant difference compared to younger adults, p
2 Significant difference compared to middle-aged adults, p
3 Significant difference compared to single-task performance, p
A mixed factorial ANOVA also revealed significant differences across the four CTT conditions (F[1.5, 158.4] = 9.7, p = 0.000), as well as a significant interaction between experimental conditions and groups in the number of transferred coins per minute (F[3.0, 158.4] = 3.0, p = 0.029). Post hoc comparisons demonstrated that the mean number of coins transferred per minute was significantly lower in older adults compared to young and middle-aged participants during the single-task condition. The coin transfer rate was affected by all mobility tasks in young adults. Furthermore, CTT performance was influenced by the F8WT task in middle-aged participants and by the 4SST task in both middle-aged and older adults. Additionally, older adults performed worse on the CTT compared to young adults during the 3MWT.
Regarding the DST and SVFT, a mixed factorial ANOVA showed significant
differences in test performance (number of errors for DST and number of generated
words for SVFT) across the four conditions (DST: F[2.7, 285.0] = 21.0, p
= 0.000; SVFT: F[2.7, 281.3] = 142.7, p = 0.000), as well as between
groups (DST: F[2, 104] = 8.9, p = 0.000; SVFT: F[2, 104] = 4.0,
p = 0.032). Post hoc comparisons revealed that older adults performed
better on the DST, making significantly fewer errors than the other groups
(p
Fig. 3 presents representative operating characteristic graphs comparing DTEs on primary and secondary tasks across young, middle-aged, and older participants, based on the conceptual framework proposed by Plummer and Eskes [46]. Overall, our results suggest that when performing mobility tasks alongside secondary tasks, participants tend to exhibit one of the following patterns: (a) significant decrements in primary mobility task performance only (mobility interference), (b) decrements in both primary motor and secondary motor or cognitive performance (mutual interference), or (c) no dual-task interference.
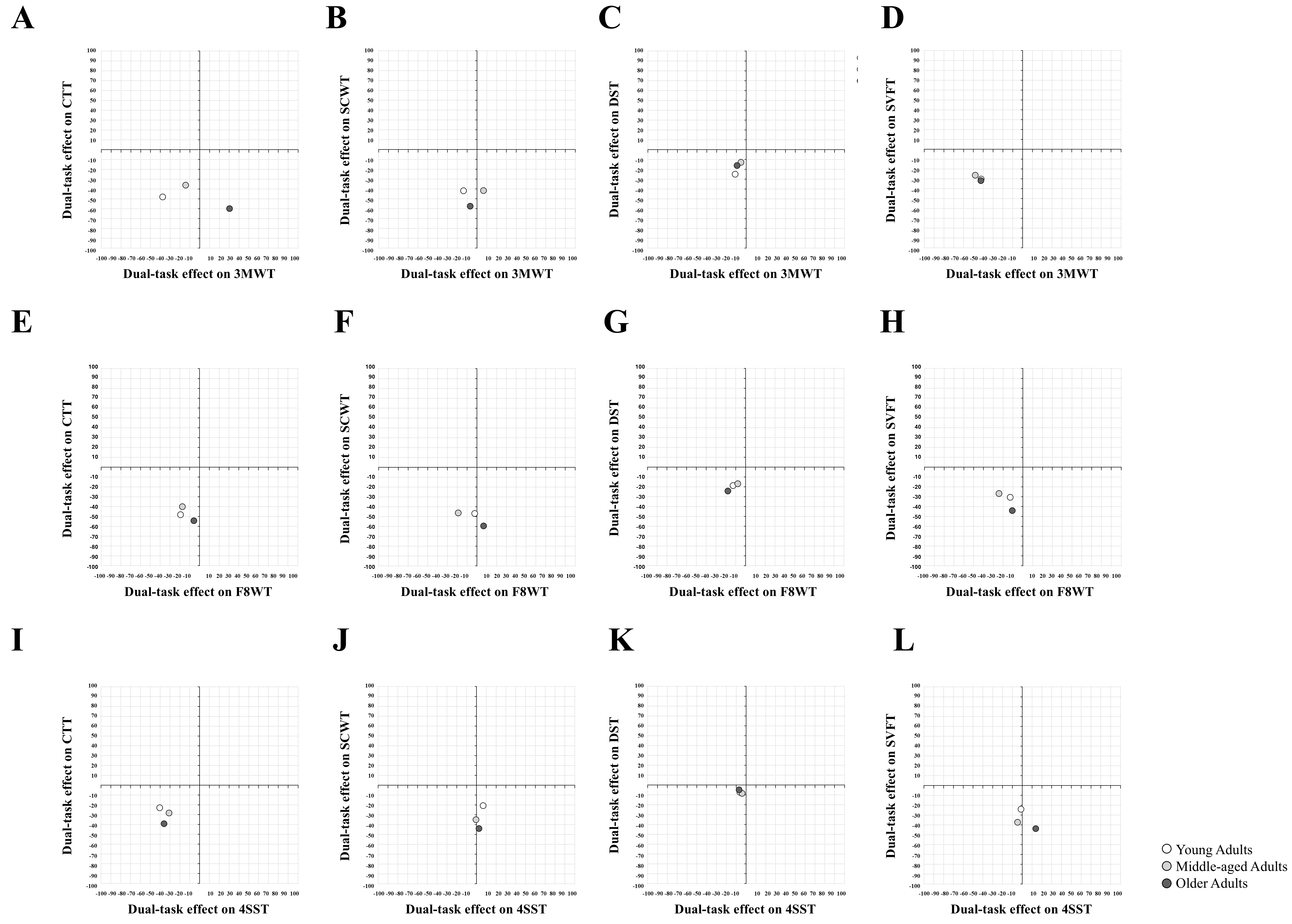 Fig. 3.
Fig. 3.
Mean patterns of dual-task interference on different gait tasks and secondary tasks among participants. (A) 3MWT+CTT; (B) 3MWT+SCWT; (C) 3MWT+DST; (D) 3MWT+SVFT; (E) F8WT+CTT; (F) F8WT+SCWT; (G) F8WT+DST; (H) F8WT+SVFT; (I) 4SST+CTT; (J) 4SST+SCWT; (K) 4SST+DST and (L) 4SST+SVFT. Representative operating characteristic graphs contrasting dual-task effects in primary and secondary tasks of young (white circles), middle-aged (light grey circles) and older (dark grey circles) participants based on the conceptual framework proposed by Plummer and Eskes [46]. Grey square represents an area within a maximum 20% of dual-task effect on primary and secondary tasks. Note: MWT, 3-meter walk test; F8WT, figure-8 walk test; 4SST, four square step test.
Secondary task priority trade-off (i.e., improvement in the secondary task performance while primary task is deteriorated) was observed only when older adults performed the 3MWT simultaneously with the CTT (Fig. 3A). During this experimental condition, both young and middle-aged participants demonstrated either mutual interference (young adults) or mobility interference (middle-aged adults). Young, middle-aged and older participants showed mobility interference when they performed 3MWT+SCWT, F8WT+SCWT, F8WT+CTT and 4SST+SVFT (Fig. 3B,E,F,L respectively). A similar mobility interference pattern was observed when older adults performed F8WT+DST (Fig. 3G), but young and middle-aged adults showed nearly no dual-task interference during the same task (Fig. 3G). Older adults also showed the same mobility interference pattern when they performed either F8WT+SVFT or 4SST+SCWT (Fig. 3H,J respectively). In contrast, while young adults shared the same patter, middle-aged adults demonstrated slight mutual interference during F8WT+SVFT (Fig. 3H). Moreover, during 4SST+SCWT middle-aged participants presented the same pattern as older participants, while young adults demonstrated no dual-task interference (Fig. 3J). No dual-task interference was mainly observed when DST was added as a secondary task. While middle-aged and older participants shared this patter during 3MWT+DTS, young and older adults shared no dual-task interference performing F8WT and DST simultaneously (Fig. 3C,G respectively). During 4SST+DST all groups also demonstrated no dual-task interference (Fig. 3K). Finally, 3MWT+SVFT or 4SST+CTT led to a mutual interference pattern for all participants independent of the group (Fig. 3D,I respectively).
This study aimed to investigate the age-related effects on dual-task performance in young, middle-aged, and older adults. To the best of our knowledge, few studies have explored the interference of different dual-task conditions during functional mobility tasks (e.g., straight-line walking, turning, and anterior/posterior/lateral displacements) to describe hierarchical patterns of secondary task performance across a three-group sample.
Our results can be summarized as follows: (a) all groups experienced declines in functional mobility performance during dual-tasking; (b) older adults took longer to complete complex tasks involving turning and anterior/lateral/posterior displacements compared to young and middle-aged adults; (c) motor tasks and the SCWT caused significant interference in functional mobility, while the DST led to only minor impairments; and (d) most dual-task conditions resulted in “mutual interference” or “mobility interference”.
Functional mobility refers to the set of movements used in common daily activities, which involve balance and gait, and is directly related to an individual’s functional capacity and age. In this study, we evaluated functional mobility through a dual-task paradigm based on different walking strategies executed independently during simple tasks and simultaneously with secondary motor (CTT) or cognitive (SCWT, DST, and SVF) tasks. Consistent with our hypothesis, we observed a significant effect of almost all experimental dual-task conditions on mobility performance across all the three age groups. Corroborating to our results, several studies provided evidence that cognitive demands during walking interferes on task performance [11, 47, 48, 49]. Interference of secondary tasks on mobility suggests that walking control is interlinked with cognitive networks and that interference may occur when simultaneous tasks compete for neural processing and/or divide attention, requiring greater postural control, balance, and environmental adjustments [50]. Additionally, a larger impact on mobility performance was observed in older adults. The increased time to perform primary functional mobility tasks while dual-tasking might be attributed to age-related changes in both the motor and cognitive systems. As individuals age, there is a natural decline in muscle strength, coordination, and balance, which affects motor performance [51]. Concurrently, cognitive functions such as attention, processing speed, and executive function also deteriorate with age [52]. These changes can make it harder for older adults to allocate cognitive resources efficiently between tasks, leading to slower and less effective performance in dual-task situations. Additionally, increased cognitive load from primary or secondary tasks can further diminish cognitive capacity, exacerbating the decline in functional mobility. For instance, walking task conditions or the nature and complexity of the concurrent cognitive task can amplify this effect [53].
Considering the relationship between the type of secondary task and mobility function, whether motor or cognitive secondary tasks have a greater impact remains controversial. As highlighted by Plummer-D’Amato et al. [54], dual-task complexity may not necessarily be determined by whether a secondary task is cognitive or motor in nature. For instance, although previous studies have shown that motor-motor dual tasks are generally associated with the lowest DTEs [16, 55], it has also been demonstrated that a concurrent motor task can have a greater impact on walking than a secondary cognitive task [56]. Expanding on this topic, our results demonstrated that both motor and cognitive tasks can result in high DTEs, with DTEs being more dependent on the complexity and cognitive demands of the secondary task rather than simply the nature of the task (motor or cognitive). Regardless of the group, the CTT and SCWT caused greater interference with mobility performance than the SVFT or DST. This difference likely stems from the distinct cognitive functions engaged by these secondary tasks. Among them, CTT may specifically require simultaneous activation of both motor and cognitive systems [17]. Although arm and hand movements are primarily controlled by motor cortical regions, they also depend on attention, visual guidance, and somatosensory feedback for proper execution [16]. Walking and concurrent secondary motor tasks might share more cognitive resources, as both require motor control. Consequently, the resulting DTE would likely be greater than that observed in a purely simple cognitive task, leading to more pronounced performance decrements in both motor tasks. On the other hand, the SCWT, a more complex task involving executive functions such as selective attention, cognitive flexibility, and inhibitory control [57], also demonstrated high DTEs. It has been previously emphasized the critical role of executive functions in gait, with deficits in these functions being associated with poorer walking performance [7]. According to the cross-talk model [58], the involvement of executive functions in both SCWT and primary mobility tasks could explain the greatest DTEs observed. In contrast, the SVFT and DST appear to be simpler than the CTT and SCWT, which may explain their lower interference with mobility during dual-tasking. While the DST primarily engages attention and working memory [59], the SVFT involves additional cognitive processes [60]. Effective SVFT performance requires participants to strategically explore the semantic store, typically by exploring semantic categories (e.g., fruits) and clustering items into subcategories (e.g., soft fruits and citrus fruits), flexibly switching between them, and still monitoring output to prevent repetitions or errors. In addition, participants were required to maintain an active state given the time constraints of the task [61]. Thus, the distinct complexity between SVFT and DST may explain the variations in DTEs in mobility observed in these tasks.
Regarding the effects of different primary mobility tasks on secondary task performance, it is important to highlight that gait requires additional cognitive control, particularly when the complexity increases [62]. The 4SST, which requires rapid movement in multiple directions and weight transfer between legs, has emerged as the most complex task, exhibiting the highest DTEs when paired with secondary cognitive tasks. Previous studies have shown that aging slows movement [33] and increases reaction times and weight transfer time between the lower limbs [63] which likely contributed to the observed performance decrements in this gait pattern. Additionally, the F8WT appears to be the second most complex task. Although it more closely resembles daily walking activities, it imposes greater demands on executive function processing than straight walking [64]. Specifically, the increased attentional demands required by these more complex gait patterns, when compared to continuous straight walking, may have led to a greater focus on gait control, thereby inducing the greatest DTEs on secondary task measures.
Another hypothesis of our study was that age could potentially modulate the interference experienced by the participants. Based on previous studies [65, 66], we expected that older adults would present higher DTEs than younger participants. However, with the exception of the simultaneous performance of 4SST and SCWT, no significant differences in DTEs were observed between older and young adults, middle-aged and young adults, or older and middle-aged adults. As previously mentioned, 4SST is a cognitively demanding motor task. It requires participants to remember a predefined sequence of steps while maintaining rhythmic cadence [33, 43], demanding substantial executive function processing. Similarly, SCWT challenges cognitive control by requiring individuals to name the ink color of a word while suppressing the automatic tendency to read the word itself [38]. In addition to inhibitory control and attention, the SCWT also involves cognitive flexibility, processing speed, working memory, and the ability to manage interference from competing information [67, 68]. Aging is associated with a decline in central processing capacity, which negatively affects key executive functions, such as planning, decision-making, and task coordination [7, 8, 69, 70]. Given that both 4SST and SCWT rely on these functions, their performance is likely influenced by aging [43, 47]. Thus, simultaneously performing these tasks may overload cognitive resources and exacerbate the effects of frontal lobe dysfunction. Successful execution of both primary and secondary tasks in this combination requires efficient allocation of attentional resources. Consequently, older adults may struggle to filter environmental distractions and distribute their already limited cognitive and attentional resources effectively during dual-tasking [71]. These findings support the assumption that decline in executive function, particularly those associated with frontal lobe aging, plays a critical role in the reduction of functional performance [72].
Finally, most dual-task conditions resulted in “mutual interference”, with performance declines in both the primary mobility task and the secondary motor or cognitive task, or “mobility interference”, where performance deteriorated exclusively in the primary mobility task. Both the “mutual interference” and “mobility interference” patterns were most commonly observed in a recent systematic review of individuals after stroke [17]. These findings suggest that cognitive resources are distributed between tasks during dual-tasking, and when attentional demands exceed capacity, they can affect each other, impairing performance in both tasks [73]. However, some of the secondary tasks in this study were not sufficiently demanding to induce significant mutual interference. The predominance of mobility interference in these conditions supports the idea that in less cognitively demanding scenarios, participants prioritize the secondary task compromising mobility [74]. It has been previously demonstrated that healthy adults tend to prioritize cognitive tasks over walking. No dual-task interference was observed when the DST was added as a secondary task. This supports the findings that memory tasks, such as recall, may result in minimal interference on dual-task performance [75].
Our results demonstrated that all primary functional mobility tasks were affected by dual-task conditions. In addition, the degree and pattern of DTE depends on the selected primary and secondary tasks (their components and/or cognitive domains). DST seems to be a cognitive task of relatively lower complexity that does not cause great DTE in walking when compared to a more complex task. In contrast, cognitive tasks that involve multiple domains of cognitive tasks and motor control present the highest level of interference. During dual-task, both mobility interference and mutual interference were the most commonly observed pattern of dual-task.
To understand their clinical impact, it is important to investigate DTEs. Thus, the selection of dual-task combinations with standardized procedures might capture specific deficits in dual-task performance. Exploring patients’ daily habits and their ecological interactions with different cognitive domains may help to identify specific dual-task combinations that are most appropriate for a tailored assessment and to design individualized, safe training programs that can be incorporated into the daily lives of older adults, promoting greater independence, safety, and social participation. Also, investigating changes during dual-task activities can be clinically important, as one of the goals of physical therapy is to minimize the effects of compensatory strategies and performance reductions, as well as their potential implications for patient mobility, such as an increased risk of falls.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
FdSS was responsible for conceptualization and designed the research study. FdSS managed and coordinated the research activity planning and execution. TRLPT and APOB conducted research process and performed data collection. ATdL and JVEHS analyzed and synthesized study data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The research protocol was approved by the Ethics Committee of Federal University of Health Sciences of Porto Alegre (Ethic Approval Number: 57415416.3.0000.5345). The study was carried out in accordance with the guidelines of the Declaration of Helsinki and all of the participants provided signed informed consent.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.