





 , Xiujun Li 2,†, Beilei Liu 2, Bin Wu 2, Changgui Chen 1, Liqun He 1,*
, Xiujun Li 2,†, Beilei Liu 2, Bin Wu 2, Changgui Chen 1, Liqun He 1,* , Gang Wu 3,*
, Gang Wu 3,*1 Department of Pharmacy, Wuhan No.1 Hospital, 430022 Wuhan, Hubei, China
2 Department of Cardiology, Hubei Provincial Hospital of Traditional Chinese Medicine, Affiliated Hospital of Hubei University of Chinese Medicine, 431799 Wuhan, Hubei, China
3 Department of Cardiology, Hubei Key Laboratory of Cardiology, Renmin Hospital of Wuhan University, Cardiovascular Research Institute, Wuhan University, 430060 Wuhan, Hubei, China
†These authors contributed equally.
Abstract
Enhanced cardiac sympathetic activity contributes to chronic heart failure (CHF). Interventions targeting the stellate ganglion (SG) can reduce this activity, potentially slowing the progression of cardiovascular diseases. This study examined the effects and mechanisms of stellate ganglionectomy on myocardial hypertrophy and cardiac dysfunction caused by pressure overload.
A rat model of pressure overload was created using abdominal aortic constriction. Four groups were studied: the sham surgery, abdominal aortic coarctation (AB), aortic constriction plus left stellate ganglionectomy (LSG), and aortic constriction plus right stellate ganglionectomy (RSG) groups. Cardiac function was assessed via echocardiography, and myocardial hypertrophy and fibrosis were evaluated using hematoxylin-eosin staining (H&E) and Masson staining. Serum atrial natriuretic peptides (ANP) and norepinephrine (NE) levels were measured using enzyme linked immunosorbent assay (ELISA), and the levels of the molecular markers tyrosine hydroxylase (TH) and growth-associated protein-43 (GAP43) were analyzed using Western blotting and PCR. Calcium calmodulin dependent protein kinase II (CaMKII) and phosphorylated Ryanodine Receptor 2 (p-RyR2) expression were also investigated.
Stellate ganglionectomy significantly reduced myocardial hypertrophy and improved cardiac function, as indicated by decreased left ventricular posterior wall thickness (LVPWD) (p < 0.01), left ventricular end-diastolic diameter (LVEDD) and volume (p < 0.001), left ventricular end-diastolic volume (LVEDV) (p < 0.001), increased left ventricular ejection fraction (LVEF) (p < 0.001) and left ventricular fractional shortening (LVFS) (p < 0.001). Histological analysis confirmed reduced myocardial dilation. Molecular analysis revealed decreased CaMKII/RyR2 signaling (p < 0.001) and lower NE levels (p < 0.01), suggesting reduced neurohormonal stress.
Stellate ganglionectomy alleviates hypertrophy and cardiac dysfunction caused by pressure overload, likely through inhibition of the CaMKII/RyR2 pathway, underscoring its potential as a therapeutic approach.
Keywords
- stellate ganglionectomy
- cardiac hypertrophy
- CaMKII
- p-RYR2
Myocardial hypertrophy is caused by increased cardiac afterload, such as hypertension, aortic stenosis, and heart valve disease [1, 2]. Long-term excessive cardiac afterload causes irreversible cardiac hypertrophy and dysfunction, even heart failure and cardiac death [3]. The pathophysiological mechanism of myocardial hypertrophy caused by pressure overload is very complex, among which dysfunction of the autonomic nervous system, especially overactivation of the sympathetic nervous system, is an important factor [4]. Although appropriate sympathetic activation can enhance myocardial contractility, it can increase heart rate and cardiac ejection function by promoting the release of norepinephrine (NE) to improve cardiac function over a period of time; moreover, it can lead to severe myocardial hypertrophy and cardiac dysfunction, ultimately leading to heart failure [5, 6].
The stellate ganglion (SG), also known as the cervical thoracic sympathetic ganglion, is an important component of the distal sympathetic nervous system of the heart [7]. The sympathetic ganglia can innervate the ipsilateral eyelids, dilated pupils, and sweat glands while regulating the activity of the heart and blood vessels. Interventions such as resection, block, and ablation of the stellate ganglion can regulate cardiac sympathetic excitability and effectively prevent cardiovascular diseases [8]. Previous studies have shown that bilateral stellate ganglion blockade significantly reduces the burden of ventricular tachycardia or ventricular fibrillation in patients with refractory ventricular tachycardia or ventricular fibrillation [9]; moreover, it has similar therapeutic effects on ventricular arrhythmia subtypes (monomorphic and polymorphic ventricular arrhythmias) and the etiology of cardiomyopathy [10]. Another study revealed that left stellate ganglion ablation can inhibit the occurrence of ventricular arrhythmias after acute stroke by downregulating catecholamine levels in plasma and preventing macrophage activation in the myocardium [11]. Similarly, research has shown that stellate ganglion stimulation facilitates atrial fibrillation (AF) induction and aggravates electrical remodeling in the atrium and pulmonary vein. Unilateral stellate ganglionectomy reduces the incidence of atrial fibrillation by inhibiting sympathetic nerve activation [12]. However, there is no relevant research revealing the impact of stellate ganglionectomy on cardiac sympathetic nerve activation or on pressure overload-related myocardial hypertrophy and cardiac dysfunction.
As an important calcium-binding protein, calmodulin (CaM) is composed of four EF-hand calcium (Ca)-binding motifs and can regulate various cellular functions. In cardiomyocytes, CaM plays a crucial role as a regulator of ryanodine Receptor 2 (RyR2) to control the flow of Ca between intracellular stores. RyR2, a member of the homologous tetramer Ca2+ release channel family, is a Ca2+ release channel on the cardiac sarcoplasmic reticulum membrane and is expressed mainly in the myocardium [13]. Studies have demonstrated that CaM-RyR2 interactions play a key role in various heart disorders [14]. For example, Søndergaard MT et al. [15] revealed that the aberrant regulation of RyR2 is a common reason that CaM mutations cause catecholaminergic polymorphic ventricular tachycardia (CPVT) and long QT syndrome (LQTS) arrhythmias, and Lv T et al. [16] demonstrated that CaM mutations are also an underlying mechanism for CPVT.
Additionally, the impaired binding of CaM and RyR2 has been observed in various heart failure models. However, it is unclear whether stellate ganglion intervention can reduce the expression of calcium calmodulin dependent protein kinase II (CaMKII) and the phosphorylation of RyR2 in heart failure. Based on the above issues, this study provides a detailed understanding of the effects of stellate ganglionectomy on pressure overload-induced myocardial hypertrophy and its possible molecular mechanisms.
Male Sprague-Dawley rats (weighing 200–230 g, 6-week-old) were provided by the Animal Center of the People’s Hospital of Wuhan University (animal certificate number: 00270753), and they were housed at the Animal Experiment Center of Renmin Hospital of Wuhan University with a controlled room temperature and free access to food and water under a natural day/night cycle. This study strictly follows the “Guidelines for Animal Protection and Use” formulated by Wuhan University. All animal experiments were approved by the Experimental Animal Ethics Committee of the Renmin Hospital of Wuhan University (Number: 20230901B), and performed in accordance with the Guidelines for the Ethical Review of Laboratory Animal Welfare and was granted on September 4, 2023. The rats were randomly assigned to one of four experimental groups using a random number table: a sham surgery control group (Sham), an abdominal aortic coarctation group (AB), a left stellate ganglionectomy group (LSG), and a right stellate ganglionectomy group (RSG). The AB group underwent isolated abdominal aortic constriction. The LSG group consisted of rats that received a left stellate ganglionectomy combined with abdominal aortic constriction. Similarly, the RSG group included rats that underwent a right stellate ganglionectomy along with the abdominal aortic constriction. There were 5 rats in each group, a total of 20 rats. The discrepancy between the initial number of rats and those ultimately included in the statistical analysis stems from technical difficulties encountered during surgical procedures. To ensure the robust establishment of the experimental model, we supplemented the rats. During the experiment, there were no abnormal deaths of rats, and all rats survived normally until the end of the experiment. At the termination of the experiment, the rats were humanely euthanized using Carbon dioxide (CO2) inhalation (the CO2 concentration elevated by 10% to 30% of the chamber volume per minute, continuing this incremental rise until the rodents lose consciousness and ultimately reach a state of euthanized repose).
The surgical procedures were performed based on previously published methodologies [17]. Specifically, the rats were anesthetized following a standardized protocol via an intraperitoneal (IP) injection of 3% sodium pentobarbital at a dose of 50 mg/kg [18]. After skin preparation and disinfection, cut the skin, fascia, muscles, and parietal peritoneum longitudinally along the midline of the abdomen to expose the internal organs. Find the abdominal aorta, abdominal artery, and right renal artery from the abdominal vein upwards, and then passively separate the abdominal aorta between the abdominal artery and right renal artery. Place the 22-G needle parallel to the separated segment of the abdominal aorta, and ligate them. Then, carefully remove the needle to cause partial stenosis of the abdominal aorta, and restore the intestinal canal to its normal position, suturing the muscles, fascia, and skin. After surgery, 10,000 units of penicillin were administered to resist infection.
On the 2nd day after surgery, the rats gradually developed symptoms such as accelerated breathing and heartbeat, fear of cold fatigue, decreased appetite, cyanosis, and subcutaneous edema, indicating that the model was constructed successfully.
A physiological recorder was used to record the electrocardiogram of the rats after successful ligation of the abdominal aorta. Preparing and disinfecting the middle of the neck, and blunt separation of subcutaneous tissue, fascia, and muscle on one side. Find the common carotid artery next to the trachea, and separate the surrounding nerves and blood vessels using a glass dividing needle carefully to get about 2 cm common carotid artery. Cross two 7-0 sutures below the common carotid artery for backup. Before operation, inject 0.3% heparin saline injection into the catheter and pressure transducer until there are no bubbles. Then ligate the distal end of common carotid artery with sutures and clamp the proximal end with arterial clamps to temporarily block this segment of blood vessel. Use ophthalmic scissors to make a small oblique incision on the vascular wall near the ligation at the distal end. Then, insert the prepared catheter into the blood vessel along the incision, after releasing the arterial clamp, push the catheter about 1cm further towards the proximal end to see the blood pressure waveform of the artery. Finally, use the remaining suture to ligate and fix the catheter. After the animal stabilizes for about 5 minutes, data such as heart rate, blood pressure, and electrocardiogram can be recorded.
The stellate ganglionectomy was performed 30 minutes after abdominal aortic constriction surgery. The rats were fixed in a supine position and passively separated subcutaneous tissue, fascia, and muscle at the midpoint incision of the neck. The common carotid artery located at the inner edge of the sternocleidomastoid muscle and near the trachea. The superior cervical ganglia located on the dorsal side of the bifurcation of the common carotid artery. The stellate ganglion was found along the common carotid artery towards the proximal end, and it was severed 3 mm below the superior cervical ganglion. When the rat shows symptoms of Horner’s syndrome such as enophthalmos, pupil narrowing, and ptosis within 5 minutes, it indicates that the stellate ganglionectomy has been successfully completed. Due to the difficulty in survival of rats with both left and right simultaneous stellate ganglionectomy, this experiment will not study on bilateral stellate ganglionectomy.
Echocardiography was performed before and 10 weeks after SG resection for detecting cardiac function using a Mylab30CV ultrasound system (Biosound Esaote, Genoa, Italy) with a 15-MHz transducer. Surgery was performed under isoflurane anesthesia (5% for induction and 1–2% during surgery) (R500, RWD, Shenzhen, China). The ventricular interventricular septal defect (IVSD, mm), left ventricular posterior wall thickness (LVPWD, mm), left ventricular end diastolic diameter and volume (LVEDD, mm), left ventricular end diastolic volume (LVEDV, mL), left ventricular ejection fraction (LVEF, %), and left ventricular short axis shortening fraction (LVFS, %) were measured using animal cardiac ultrasound in three groups of rats. Detect at least 3 or more cardiac cycles for all parameters. The results were analyzed with the Chart 5.0 software (Applied Biosystems, Danvers, MA, USA).
Obtain heart tissue and to homogenize the tissue. Before operation, add
sufficient tissue protein extraction reagents and an appropriate amount of
protease inhibitors in advance. The thoroughly lysed tissue was centrifuged at
2000 rpm for 5 minutes, carefully collect the centrifuge supernatant as a total
protein solution. Firstly, prepare a sufficient amount of BCA working solution,
and add a certain concentration of sample and 25 µL standard samples to the
micropores respectively. Then add 200 µL BCA working solution in sequence,
mix thoroughly, and incubate at 37 °C for 30 minutes. Next, calculate the protein
concentration and calculate the total protein (each sample to be 40 µg).
Add protein loading buffer to the protein sample and soak in boiling water for 5
minutes. After preparing separation gel and concentration gel, sample loading and
electrophoresis are carried out in sequence. After electrophoresis, membrane
transfer is carried out. Rinse the PVDF film and place it in a sealing solution.
Shake the bed for 2 hours and remove it in TBST for 3 times
The expression of ANP, growth-associated protein-43 (GAP43), TH, CaMKII, PYR2 in myocardium was measured by RT-qPCR. Total RNA was isolated from ventricular samples with Tripure Extraction Reagent (orb782896, Biorbyt, Danvers, MA, USA) according to the manufacturer’s protocol. cDNA was synthesized using EntiLink™ 1st Strand cDNA Synthesis Kit (EQ003, Yeasen, Shanghai, China). Real-time fluorescent quantitative PCR was performed on the StepOne real-time PCR instrument (4376374, Thermo Fisher, Waltham, MA, USA), and each sample was made into three duplications using EnTurbo™ SYBR Green PCR SuperMix kit (EQ001, Biorbyt, Danvers, MA, USA). GAPDH was used as the internal control (Table 1), and all reactions were performed in triplicate. Relative RNA expression was calculated using the 2-ΔΔCt method [15].
| Gene | Primer sequence |
| Anp (rat) | F: 5′- CTCCGATAGATCTGCCCTCTTGAA -3′ |
| R: 5′- GTACCGGAAGCTGTTGCAGCCTA -3′ | |
| CamkII (rat) | F: 5′- TGGCATAGTTCACAGGGACC -3′ |
| R: 5′- TGCCAGCAAAACCAAACCAC -3′ | |
| RyR2 (rat) | F: 5′- GTGAAGCAGCCCAAGGGTAT -3′ |
| R: 5′- TGGACTGTTCTCCGCTGTTC -3′ | |
| Gapdh (rat) | F: 5′- CTCAGTTGCTGAGGAGTCCC -3′ |
| R: 5′- ATTCGAGAGAAGGGAGGGCT -3′ |
Note: F: Forward; R: Reverse; Anp, atrial natriuretic peptide; CamkII, calcium/calmodulin-dependent kinase II; RyR2, ryanodine receptor type 2.
The concentration of brain natriuretic peptide (BNP) and norepinephrine (NE) generated from rat serum was detected by ELISA. The BNP concentration in the rat serum (n = 3) in validation cohort was determined by the ELISA BNP Immunoassay (RAB0386-1KT, Sigma, MO, USA) according to the manufacturer’s instructions. The NE levels from rat serum (n = 3) were determined using NA/NE (Noradrenaline/Norepinephrine) ELISA Kit (E-EL-0047, Elabscience, Beijing, China) following the manufacturer’s instructions.
10 weeks after stellate ganglionectomy, rats were first anesthetized with 1.5–2% isoflurane by inhalation firstly, and then were euthanized by cervical dislocation. Take the hearts of rats for pathological examination to observe the degree of myocardial hypertrophy and ventricular remodeling. The heart was fixed in 4% paraformaldehyde buffer (P6148, Sigma, MO, USA) overnight and then transferred to 70% ethanol. Following this, the tissues were embedded in paraffin, sectioned at 30 µm and subjected to hematoxylin-eosin staining (H&E) (PH0516-100, PHYGENE, Fujian, China), Phygene Masson staining (G1340, Solarbio, Beijing, China). H&E staining was performed according to a routine standard operating procedure using a Leica Multistainer (ST5020, Leica, Vizna, Germany). Slides were dewaxed and rehydrated with successive applications of xylene, alcohol 100%, alcohol 70% and tap water. Haematoxylin (Mayer’s, Klinipath, Benelux, USA) was applied for 4 minutes followed by a 20 second differentiation in ammonia after which eosin (Eosin Y A+B, Klinipath, Benelux, USA) was applied for 20 seconds. Masson staining was used to examine the myocardial fibrosis of the heart based on the proportion of myocardial collagen fibers.
Statistical analyses were performed using GraphPad PRISM software v8.4.2
(GraphPad Software Inc, San Diego, CA, USA). As indicated, statistical analysis
was performed by calculating mean SEM. Student’s t-test was used when
only two groups were analyzed. For comparisons between multiple groups, homo
geneity variance was first tested, and the one-way ANOVA (Tukey’s multiple
comparisons test) was applied when variance was homogeneous, or non-parametric
independent sample t-test (the Mann–Whitney test) was used for
inhomogeneity. Paired Student’s t-test or one-way ANOVA was used to
analyze the quantitative Western blot as indicated in figure legends. Two-tailed
test was used for all t-tests, and p
Previous study had demonstrated that inhibiting the activity of the stellate ganglia can effectively treat chronic heart failure [8]. Based on this knowledge, we aimed to further investigate the impact of stellate ganglion activity on cardiac function. To test this hypothesis, we developed a rat model of chronic heart failure (Fig. 1A). The successful establishment of the model was confirmed by comparing the mean arterial pressure and heart rate between the rats in the sham surgery group (Sham) and abdominal aortic coarctation group (AB) (Fig. 1B,C). Next, we surgically removed the left (LSG) or right stellate ganglion (RSG) to further investigate their roles in cardiac hypertrophy and chronic heart failure. Surprisingly, we found that resection of either the left (LSG) or right stellate ganglion (RSG) significantly reduced the mean arterial pressure and heart rate in rats compared with those in the AB group (Fig. 1D,E). These findings suggest that surgical removal of the stellate ganglia can effectively alleviate the elevated mean arterial pressure and tachycardia associated with chronic heart failure.
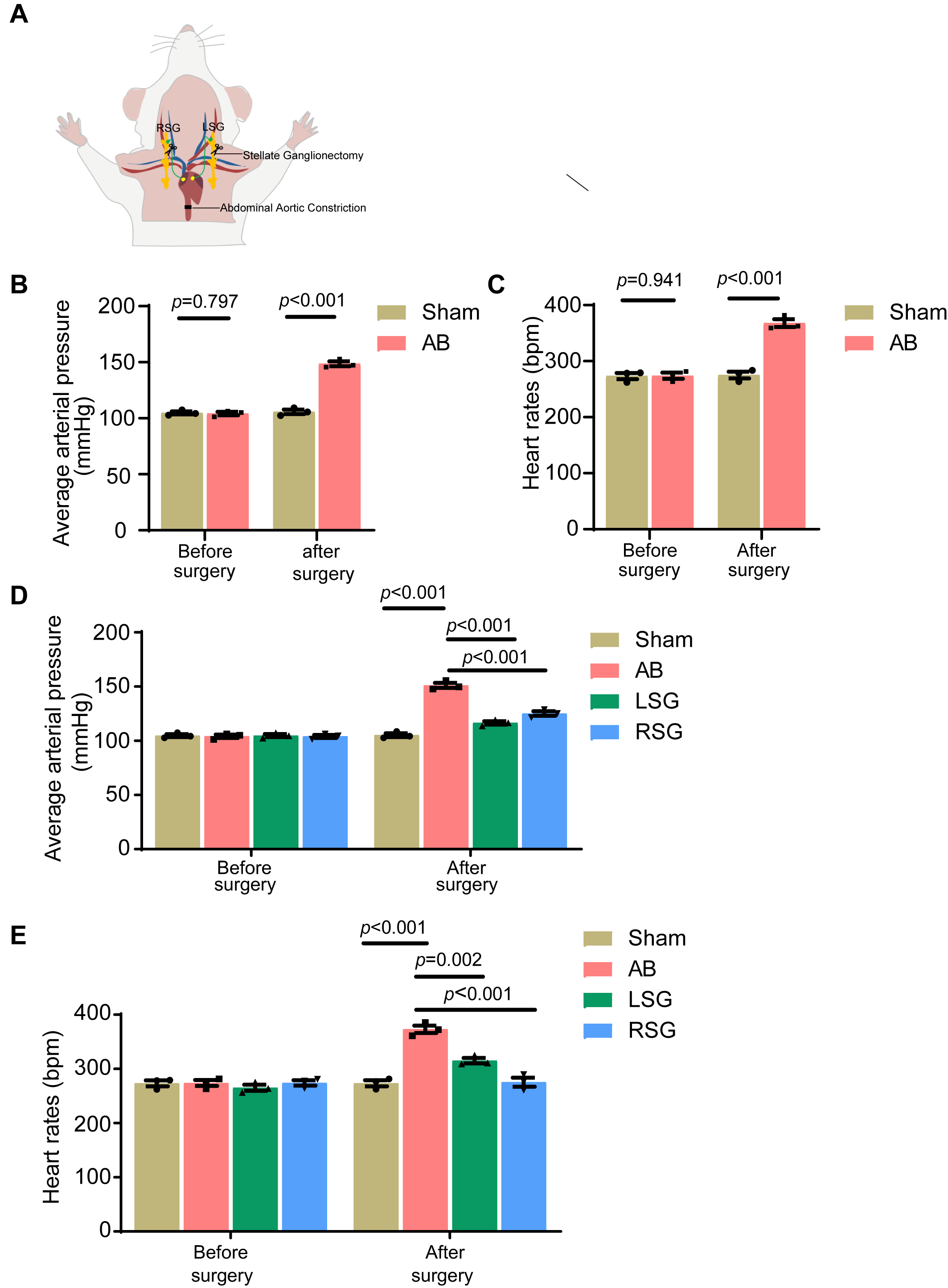 Fig. 1.
Fig. 1.
Effective alleviation of cardiac symptoms in chronic heart
failure patients through stellate ganglionectomy. (A) Schematic representation
of stellate ganglionectomy. (B) The average arterial pressure of each
group was tested before and 10 weeks after stellate ganglionectomy. (C)
Heart rates of each group were tested before and 10 weeks after stellate
ganglionectomy. (D) The average arterial pressure of each group was
tested before and 10 weeks after stellate ganglionectomy. (E) Heart rates of each
group were tested before and 10 weeks after stellate ganglionectomy. Sham, sham
surgery group; AB, abdominal aortic coarctation group; LSG, left ganglionectomy
group; RSG, right ganglionectomy group. Error bars, means
The results of our preliminary experiments demonstrated that stellate ganglionectomy significantly improved abnormal vital signs, such as the mean arterial pressure and heart rate, in rats with chronic heart failure. Chronic overload of mean arterial blood flow and elevated heart rate are known contributors to cardiac overload, leading to heart failure [19]. To investigate the therapeutic potential of stellate ganglionectomy on cardiac function in chronic heart failure patients, we conducted echocardiographic measurements. We assessed interventricular septal defect (IVSD, mm), left ventricular posterior wall thickness (LVPWD, mm), left ventricular end-diastolic diameter (LVEDD, mm), left ventricular end-diastolic volume (LVEDV, mL), left ventricular ejection fraction (LVEF, %), and left ventricular fractional shortening (LVFS, %), among other parameters, to evaluate postsurgical cardiac function across different groups of rats (Fig. 2A). Our findings indicate that stellate ganglionectomy significantly reduces the LVEDV (mL), LVPWD (mm) and LVEDD (mm) (Fig. 2B,E,F) while significantly increasing the LVFS (%) (Fig. 2C) and LVEF (%) (Fig. 2D). Notably, among the treatments considered, solely RSG exerts a significant influence on the interventricular septal diameter (IVSD) (mm) (Fig. 2G). These results suggest that stellate ganglionectomy effectively mitigates cardiac dysfunction associated with chronic heart failure.
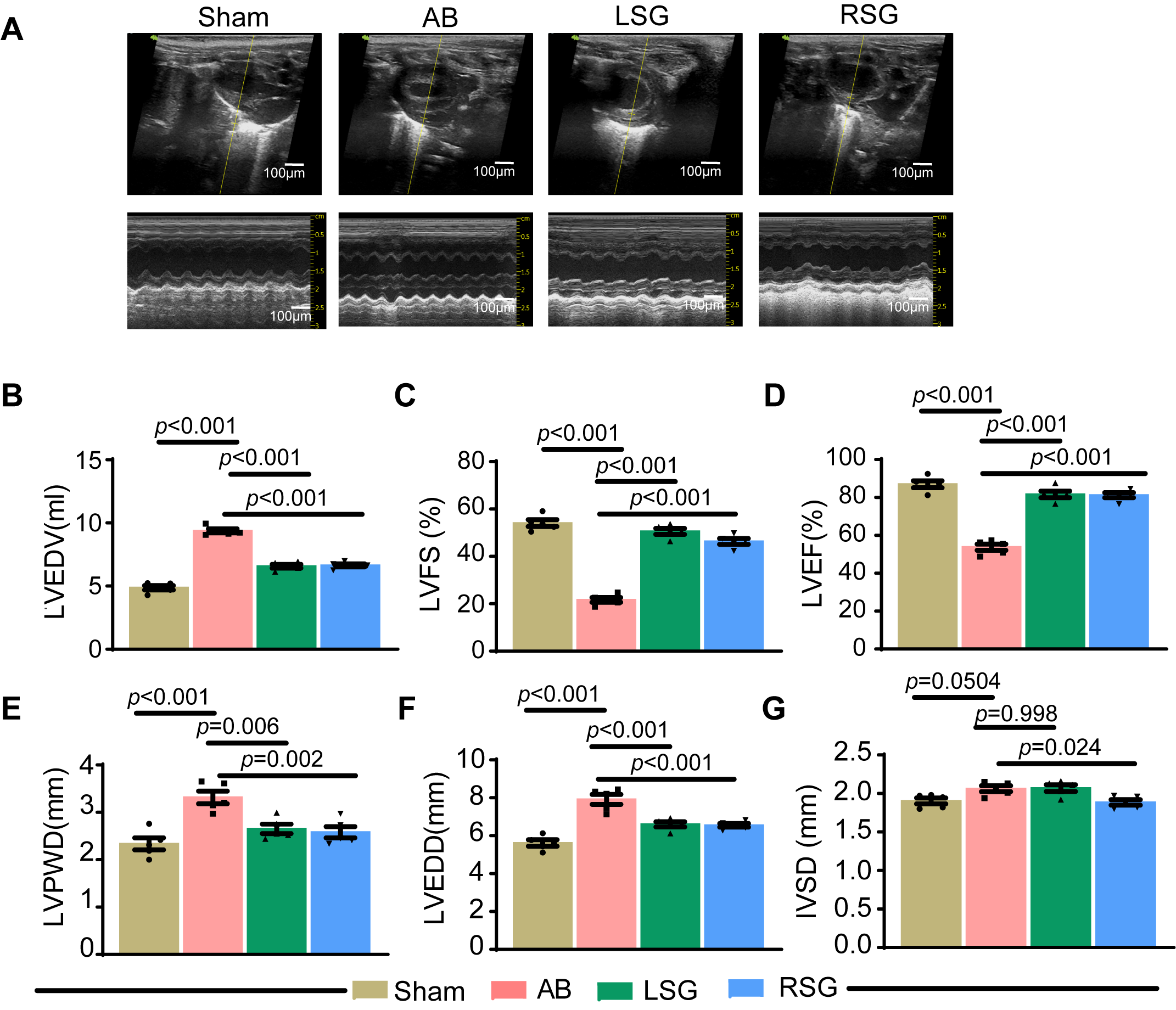 Fig. 2.
Fig. 2.
Stellate ganglionectomy significantly mitigates cardiac
dysfunction in chronic heart failure. (A) Representative images of
echocardiograms from each group. The scale bars = 100 µm. (B–G)
Statistical evaluation of echocardiography data from each group. Left ventricular
end-diastolic volume (LVEDV, mL) (B), left ventricular short-axis shortening
fraction (LVFS, %) (C), left ventricular ejection fraction (LVEF, %) (D), left
ventricular posterior wall thickness (LVPWD, mm) (E), left ventricular
end-diastolic diameter and volume (LVEDD, mm) (F), and ventricular
interventricular septal defect (IVSD, mm) (G). Sham, sham surgery group; AB,
abdominal aortic coarctation group; LSG, left ganglionectomy group; RSG, right
ganglionectomy group. Error bars, means
In addition to investigating the impact of stellate ganglionectomy on cardiac function in chronic heart failure patients, we aimed to further explore whether this procedure can be used to treat structural lesions associated with chronic heart failure. Research has indicated that sustained mean arterial pressure overload and rapid heart rate can lead to heart failure, resulting in compensatory cardiac hypertrophy and ultimately chronic heart failure [20]. Therefore, we utilized the heart-to-body weight ratio and heart size-to-calf length ratio as preliminary indicators of organic cardiac dilation. As anticipated, at 10 weeks post surgery, the rats in the AB group presented significant increases in both the heart-to-body weight ratio and heart size-to-calf length ratio compared with those in the sham group (Fig. 3A,B). Notably, stellate ganglionectomy markedly reduced these ratios (Fig. 3A,B). We further employed H&E staining and Masson staining to assess the pathological changes associated with postoperative cardiac hypertrophy. The results demonstrated that the rats in the AB group presented significant pathological dilation of myocardial fibers, whereas stellate ganglionectomy significantly ameliorated this pathological myocardial fiber dilation (Fig. 3C,D). In conclusion, inhibiting stellate ganglion activity not only effectively mitigates cardiac dysfunction caused by chronic heart failure but also fundamentally addresses the structural lesions associated with chronic heart failure.
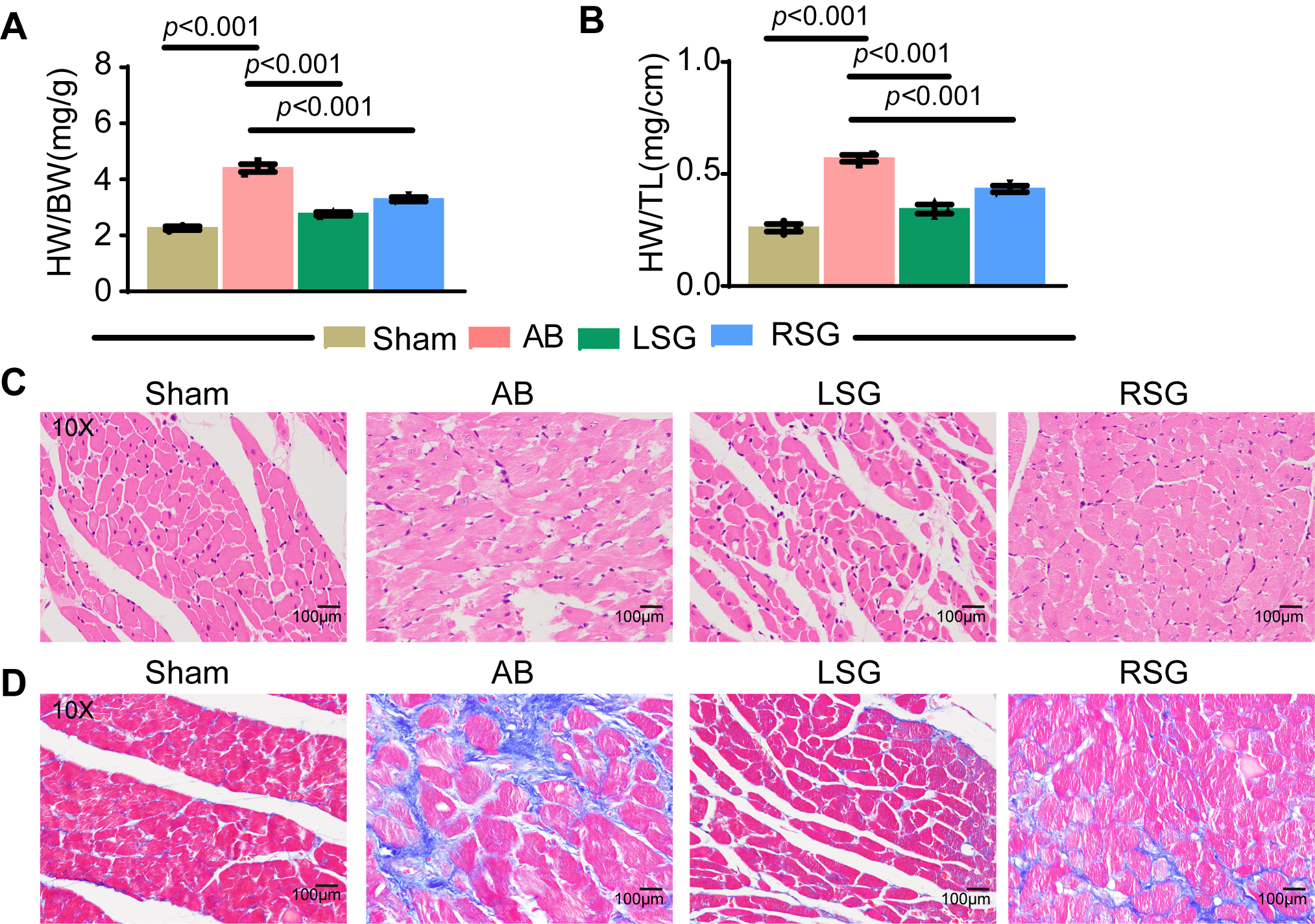 Fig. 3.
Fig. 3.
Stellate ganglionectomy reduces structural cardiac lesions and
mitigates dysfunction in chronic heart failure. (A) Statistical evaluation of
heart weight-to-body weight (HW/BW) in each group. (B) Statistical evaluation of
heart weight to tibia length (HW/TL) in each group. (C) H.&E. Analysis of
myocardial fibers in the cardiac tissues of each group. (D) Masson strain
analysis of myocardial fibers in the cardiac tissues of each group. Sham, sham
surgery group; AB, abdominal aortic coarctation group; LSG, left ganglionectomy
group; RSG, right ganglionectomy group. The scale bars = 100 µm for (C) and
(D). Error bars, means
In the early stages of heart failure, a decrease in cardiac output and blood
pressure triggers the neurohormonal system, including the
renin‒angiotensin‒aldosterone system (RAAS) and sympathetic nervous system (SNS),
as a compensatory mechanism to maintain circulatory homeostasis [21]. The
stellate ganglia, formed by the fusion of the 7th cervical and 1st thoracic
sympathetic ganglia, serve as postganglionic nerves to regulate cardiac function.
Prolonged elevation of mean arterial pressure, which leads to cardiac
dysfunction, activates the stellate ganglia to secrete neurotransmitters such as
norepinephrine, which in turn activate atrial natriuretic peptide (ANP) to
provide stress-induced cardiac protection [22]. To further investigate the
molecular mechanisms underlying stellate ganglion activity in the context of
myocardial fiber dilation and chronic heart failure, we measured the protein
expression levels of GAP43 and TH proteins, which are markers of stellate
ganglion activity, using protein immunoblotting. Our results indicated that,
compared with those in the sham group, GAP43 and TH expression levels were
significantly elevated in the AB group. Notably, these elevations were
significantly reversed following stellate ganglion resection (Fig. 4A–C).
Additionally, we quantified plasma norepinephrine levels using ELISA. Compared
with that in the sham group (215.2
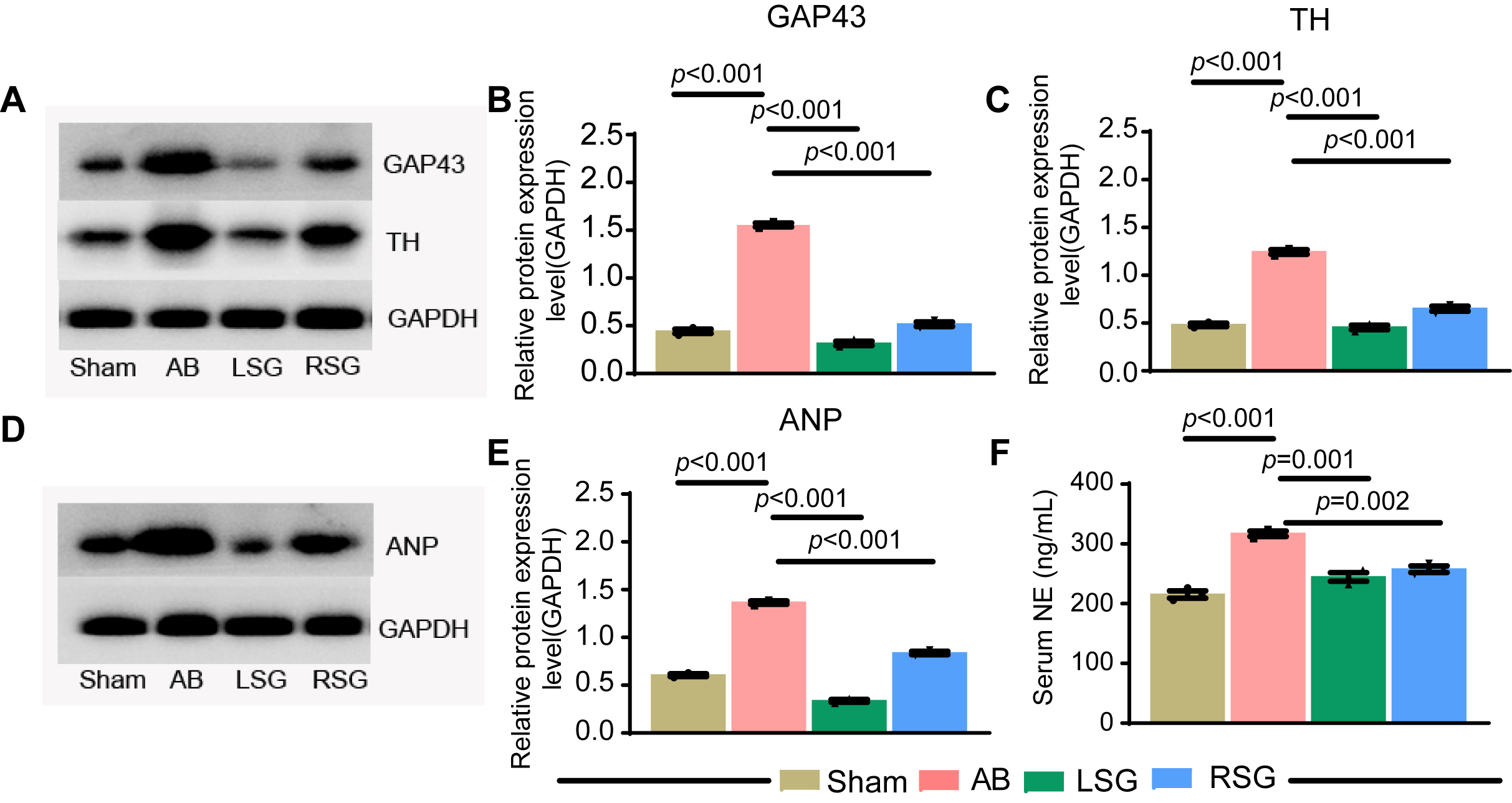 Fig. 4.
Fig. 4.
Modulation of neurohormonal activity by stellate ganglionectomy
in chronic heart failure. (A) Western blotting was used to detect the protein
expression levels of tyrosine hydroxylase (TH) and growth-associated protein-43
(GAP43) in the cardiac tissues of each group. (B) Statistical analysis
of GAP43 expression. (C) Statistical analysis of TH expression.(D) Western blotting was used to detect the protein expression levels of atrial
natriuretic peptides (ANP) in the cardiac tissues of each group. (E)
Statistical analysis of ANP expression. (F) The concentration of
norepinephrine (NE) in serum. Sham, sham surgery group; AB, abdominal
aortic coarctation group; LSG, left ganglionectomy group; RSG, right
ganglionectomy group. Error bars, mean
Calcium ions play a crucial role in cardiac excitation, with excessive diastolic calcium ion (Ca2⁺) leakage leading to arrhythmia and heart failure. Previous studies have demonstrated that calcium/calmodulin-dependent kinase II (CaMKII) enhances RyR2-mediated Ca2⁺ leakage through the phosphorylation of RyR2 at Ser2814 [23]. However, the precise mechanism by which hyperactivity of the stellate ganglia results in abnormal calcium loading in cardiomyocytes remains unclear. To address this, we assessed the expression levels of CaMKII and RyR2 in different experimental groups by immunoblotting and RT-qPCR. Our findings indicate that chronic heart failure significantly elevates in total CaMKII protein levels, but has no change in the total of RyR2 (Fig. 5A,B). Importantly, stellate ganglionectomy effectively mitigated these increases, reversing the elevated expression levels of total CaMKII protein and the RyR2 phosphorylation associated with chronic heart failure (Fig. 5C,D).
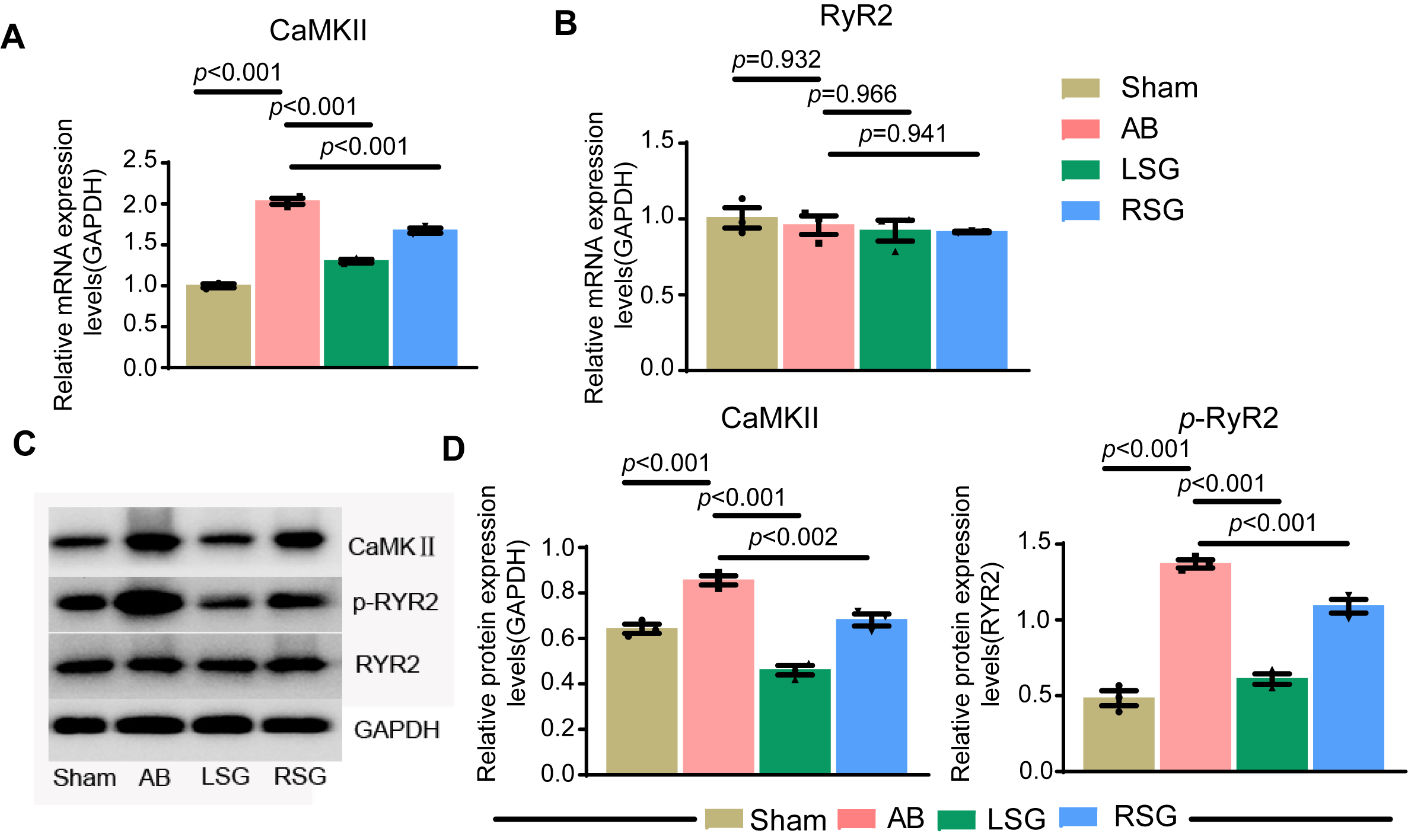 Fig. 5.
Fig. 5.
Stellate ganglionectomy reverses abnormal calcium regulation in
chronic heart failure. (A,B) RT-qPCR was used to measure the gene expression
levels of calcium/calmodulin-dependent kinase II (CaMKII) and Ryanodine Receptor
2 (RyR2) in the cardiac tissues of each group. (C) Western blotting was
used to detect the protein expression levels of CaMKII, phosphorylated RyR2 and
total RyR2 in the cardiac tissues of each group. (D) Statistical
analysis of CaMKII and phosphorylated RyR2 expression. Sham, sham
surgery group; AB, abdominal aortic coarctation group; LSG, left ganglionectomy
group; RSG, right ganglionectomy group. Error bars, mean
Our research provides initial insights into the effectiveness of stellate ganglionectomy in treating chronic heart failure. We developed a model of chronic heart failure through abdominal artery ligation, which led to elevated expression of GAP43, a marker of stellate ganglion activity [24]. These findings suggest that chronic heart failure induces a robust response from the peripheral nervous system. We then surgically removed the left or right stellate ganglion and observed significant improvements in cardiac function and structural heart conditions, such as cardiac hypertrophy. Further investigations revealed that stellate ganglionectomy reduces epinephrine secretion, which in turn diminishes the activity of the CaMKII/RyR2 signaling pathway in cardiomyocytes. This alleviation of signaling pathway activity enhances cardiac ejection function and mitigates the symptoms of chronic heart failure. Thus, our study highlights the CaMKII/RyR2 pathway, which is regulated by the stellate ganglion, as a novel target for chronic heart failure therapy, marking a significant advancement in the field.
Cardiac sympathetic overactivation is a key feature of heart failure and
primarily contributes to arrhythmias and sudden cardiac death. The stellate
ganglion, located at the fusion of the 7th cervical and 1st thoracic sympathetic
ganglia, predominantly governs the postganglionic nerves of the cardiac
sympathetic nervous system [25]; it regulates heart ejection functions through
the release of neurotransmitters such as norepinephrine and neuropeptide Y. Human
adrenoceptors are broadly categorized into alpha and beta types, with each type
further divided into subtypes:
While the current study has provided significant insights into the efficacy of stellate ganglionectomy in mitigating pressure overload-induced cardiac hypertrophy and dysfunction, several limitations warrant critical evaluation. Primarily, our experimental model was based on a rodent system, which may not fully replicate the complex pathophysiological nuances of human chronic heart failure. Therefore, future research should aim to validate these findings in more advanced animal models or, ideally, through clinical trials, to better assess the translational potential of this therapeutic intervention. Additionally, although the CRISPR-Cas9-based lineage tracking platform has proven effective in delineating cellular lineages, integrating this technology with in vivo imaging techniques could enhance real-time monitoring of cellular dynamics. This integration would provide a more comprehensive understanding of the underlying biological mechanisms, thereby enabling researchers to thoroughly examine both the immediate and long-term effects of stellate ganglionectomy on myocardial cells and their interactions within the cardiac microenvironment.
The CaMKII (calcium/calmodulin-dependent protein kinase II) and RyR2 (type 2 ryanodine receptor) signaling pathways have garnered significant attention for their roles in chronic heart failure. CaMKII is crucial in regulating calcium ion flow within cardiomyocytes, a fundamental process for myocardial contraction and relaxation. RyR2 serves as a vital calcium channel in cardiomyocytes, where its activation triggers calcium ion release from the sarcoplasmic reticulum, influencing myocardial contractility [30]. In chronic heart failure, aberrant activation of these proteins may disrupt calcium homeostasis in cardiomyocytes, potentially causing myocardial dysfunction and structural changes in the heart. Overactivation of CaMKII can hasten RyR2 opening, increasing myocardial calcium leakage and leading to hyperexcitability and arrhythmias in cardiomyocytes. Research indicates that inhibiting CaMKII activity can diminish RyR2 overactivation, helping to reestablish calcium balance in cardiomyocytes and enhance cardiac function [31]. Our experimental findings suggest that stellate ganglionectomy effectively reduces epinephrine secretion, subsequently suppressing CaMKII/RyR2 pathway activity in cardiomyocytes. Thus, therapeutic strategies targeting the CaMKII/RyR2 signaling pathway may offer promising options for treating chronic heart failure.
While this study underscores the beneficial effects of stellate ganglion resection on cardiac hypertrophy and function induced by pressure overload, several limitations merit attention. Primarily, the research was confined to rat models, limiting the direct applicability of the findings to human subjects; thus, clinical trials are essential for further validation. Additionally, the study did not examine the long-term effects of stellate ganglionectomy, leaving the sustained impact on cardiac function unclear. Potential physiological or psychological side effects resulting from the procedure have also not been thoroughly explored. Moreover, the stellate ganglion, strategically positioned at the confluence of the cervical and upper thoracic vertebrae, represents an indispensable element within the sympathetic nervous system. Although anatomically symmetrical, the left and right stellate ganglia exhibit divergent functional profiles due to their distinct innervation territories and neural connectivity patterns. Of particular significance is the greater influence exerted by the right stellate ganglion over cardiac and pulmonary functions, which can be attributed to its direct participation in the pericardial bronchial plexus—a network that assumes a critical role in modulating the tension within the heart’s and lungs’ vasculature. In contrast, while the left stellate ganglion also exerts effects on the cardiovascular system, its primary function seems to revolve around the regulation of vascular tone in the ipsilateral upper extremity. Recent studies had demonstrated that a blockade of the left stellate ganglion could markedly enhance left ventricular end-diastolic volume (LVEDV) and left ventricular end-systolic volume (LVESV) in normative subjects; however, analogous changes were not as evident when interventions targeted the right side [32]. These observations suggested that the differential physiological responses elicited by the resection or blockade of either stellate ganglion may fundamentally stem from intrinsic functional disparities between these bilateral entities. In conclusion, the significant variations in the physiological roles of the left and right stellate ganglia underscore the intricate nature of autonomic nervous system regulation. This complexity highlights the imperative need for considering lateralized differences in both clinical practice and experimental research paradigms. In addition, although we have preliminarily demonstrated through experiments that star-shaped ganglion resection can restore cardiac function by inhibiting the protein expression of the CaMKII/RyR2 signaling pathway to rebuild the myocardial cell calcium balance in a chronic heart failure model, we still need to activate the expression of CaMKII/RyR2 on the basis of star-shaped ganglion resection in the future to demonstrate the effectiveness of the above pathway in treating chronic heart failure function through salvage experiments. Future research should aim to overcome these limitations to assess the clinical viability of stellate ganglionectomy fully.
In conclusion, our investigation highlights the role of sympathetic nervous system hyperactivation in cardiac hypertrophy and dysfunction using in vivo animal experiments and probing its downstream molecular mechanisms. These findings provide new research avenues for clinical therapeutic development.
Our study revealed that stellate ganglionectomy has significant therapeutic potential in reducing myocardial hypertrophy and improving cardiac function in rats with pressure overload-induced heart conditions. This surgical intervention not only delayed the progression of heart failure but also elucidated a potential mechanism involving the inhibition of the CaMKII/RyR2 signaling pathway. These findings highlight the importance of modulating sympathetic nerve activity to treat cardiac dysfunction and suggest a promising avenue for future clinical applications in managing similar cardiac conditions in humans. Further studies are warranted to explore the long-term effects and potential clinical implementation of this procedure.
CHF, chronic heart failure; SG, stellate ganglion; AB, abdominal aortic coarctation group; LSG, left stellate ganglionectomy; RSG, right stellate ganglionectomy; RyR2, ryanodine receptor type 2; IVSD, ventricular interventricular septal defect; LVPWD, left ventricular posterior wall thickness; LVEDD, left ventricular end diastolic diameter and volume; LVEF, left ventricular ejection fraction; LVFS, left ventricular short axis shortening fraction; ANP, atrial natriuretic peptides; BNP, brain natriuretic peptide; NE, norepinephrine; LVEDV, eft ventricular end diastolic volume; TH, tyrosine hydroxylase; GAP43, growth-associated protein-43; CaMKII, Calcium Calmodulin Dependent Protein Kinase II.
All analyzed data supporting the study are included in this published article and its supplementary information files. And the raw data will be made available from the corresponding author on request.
Conceptualization: GW, HY and XJL; methodology: BL; data curation: BW; formal analysis: CGC; investigation and project administration: GW and LQH; resources: LQH; software: HY and XJL; supervision: GW; writing—original draft: HY; writing—review and editing: GW and LQH. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
All animal experiments were approved by the Experimental Animal Ethics Committee of the Renmin Hospital of Wuhan University (Number: 20230901B), and performed in accordance with the Guidelines for the Ethical Review of Laboratory Animal Welfare and was granted on September 4, 2023.
GW were supported by the Department of Cardiology, Hubei Key Laboratory of Cardiology, Renmin Hospital of Wuhan University, Cardiovascular Research Institute, Wuhan University, Wuhan, China. LQH were supported by the Department of Cardiology, Intervention Cardiology Center, Wuhan No.1 Hospital, Wuhan, Wuhan hospital of Traditional Chinese and western medicine, 430022, Wuhan, China.
This work was supported by grants from The National Natural Science Foundation of China (82270243).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.