








1 Department of Pharmaceutics, Manipal College of Pharmaceutical Sciences, Manipal Academy of Higher Education, 576104 Manipal, Karnataka, India
2 Department of Pharmaceutical Quality Assurance, Manipal College of Pharmaceutical Sciences, Manipal Academy of Higher Education, 576104 Manipal, Karnataka, India
3 Department of Pharmaceutics, R. C. Patel Institute of Pharmaceutical Education and Research, 425405 Shirpur, Maharashtra, India
4 PSIT-Pranveer Singh Institute of Technology (Pharmacy), 209305 Kanpur, Uttar Pradesh, India
5 Faculty of Pharmacy, Sankalchand Patel University, 384315 Visnagar, Gujurat, India
Abstract
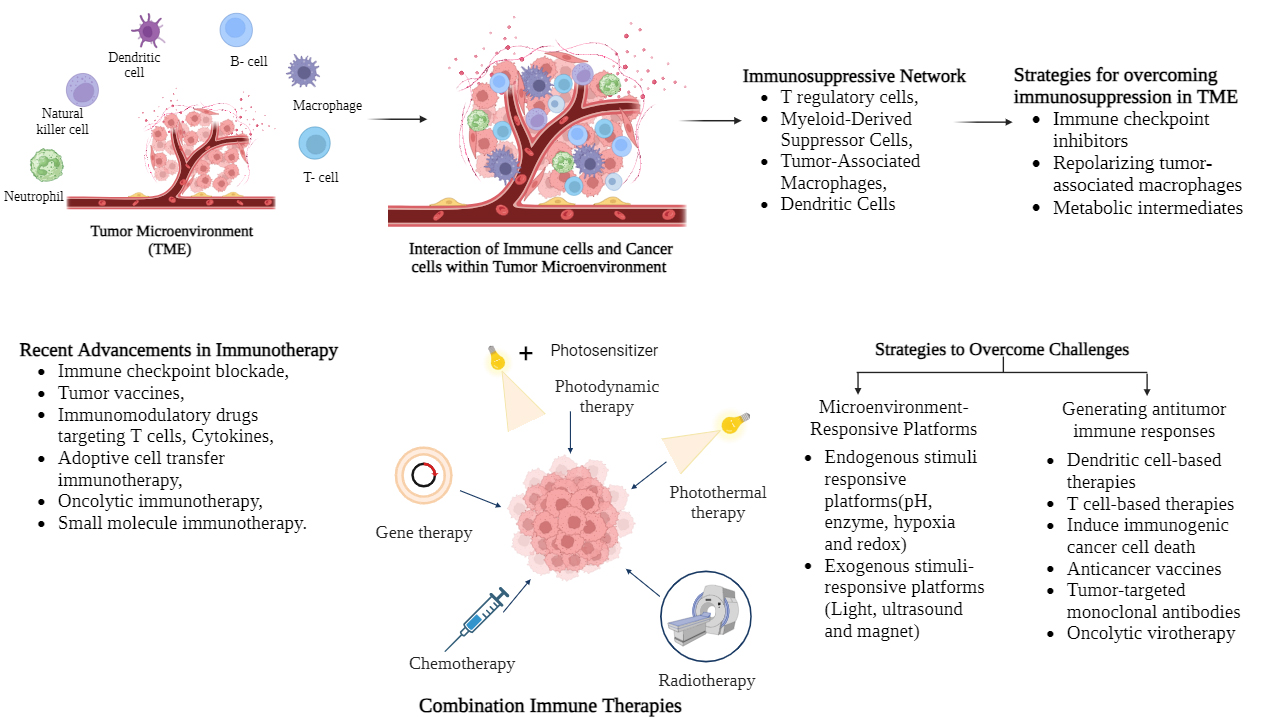
The immune system and cancer cells interact intricately during the growth of tumors, and the dynamic interplay between immune activation and suppression greatly influences the cancer outcome. Natural killer cells (NK), cytotoxic T lymphocytes (CTLs) and Dendritic cells (DC), employ diverse mechanisms, to combat cancer. However, the challenges posed by factors such as chronic inflammation and the immunosuppressive tumor microenvironment (TME) often hinder immune cells' ability to detect and eliminate tumors accurately. Immunotherapy offers a promising approach, reprogramming the immune system to target and eliminating cancer cells while minimizing side effects, enhancing immune memory, and lowering the risk of metastasis and relapse compared to traditional treatments like radiation and surgery. Nanotechnology presents a potential solution by enabling safer, more efficient drug delivery through nanoparticles. These nanoengineered drugs can be tailored for controlled activation and release. Improving TME characters holds potential for enhancing personalized immunotherapy and addressing T cell availability issues within tumor sites, particularly when combined with existing therapies. This review discusses TMEs and the strategies to overcome immunosuppression in TME, and various immune cell-based strategies to improve antitumor response. It also focuses on the strategies for constructing microenvironment responsive nanoplatforms based upon the factors present at higher levels in TME like acidic pH, hypoxia facilitated by poor oxygen supply, higher expression of certain enzymes, and other factors such light, ultrasound and magnetic field. Combination immune therapies combined with immunotherapy include photodynamic therapy, photothermal therapy, chemotherapy, gene therapy and radiotherapy, revealing a high level of anticancer activity in comparison to a single therapy, enhancing immunogenicity, promoting therapeutic efficacy, and lowering metastasis. In conclusion, cancer immunotherapy is a potential technique to combat cancer cells and boost the immune system, hindering their growth and recurrence. In order to prevent cancer, it helps the immune system target cancer cells selectively and strengthens its long-term memory. Clinical trials are extending the application of immunotherapy and identifying strategies to improve the immune system tumor-fighting capabilities. Immunotherapy has enormous promise and gives hope for more successful cancer treatment.
Graphical Abstract
Keywords
- immunotherapy
- cancer
- nanomedicines
- personalized medicines
- stimuli-responsive platforms
- vaccines
Development of tumor arises from the intricate interplay between immune cells
and cancer cells, involving a complex balance of immune activation and
suppression. Immune cells like natural killer cells (NK), cytotoxic T lymphocytes
(CTLs), and dendritic cells (DC) destroy cancer cells by different mechanisms
like granzyme and perforin secretion, recruiting T lymphocytes to the tumor
microenvironment (TME) by producing chemokine like chemokine (CXC motif) ligand
and secretion of cytokines like interferon (IFN)-
TME is an important factor responsible for the anticancer activity and could cause resistance to immunotherapy. Tumors overcome immune response by a mechanism called as cancer immunoediting, promoting tumor growth in the TME. Overcoming this limitation of suppressive TME is important to deliver drugs and restoring T cell treatment. Hence reprogramming and modulating the immunosuppressive TME is crucial for improving the efficacy of cancer immunotherapy [7]. Nanotechnology indicates a potential breakthrough in the drug design for overcoming the immunosuppression. Nanoparticles can be easily absorbed by the cells, hence could result in a low EC50 value because of the improved cell internalization which shows that the nanoengineered drugs are safer and efficient. The molecules could be engineered to release the drug slowly or can be activated at a particular circumstance. Also, the toxicity is reduced by maintaining the drugs at effective dose level at the targeted site [1]. The variation of the parameters in TME is promising generally in combination with the current approaches as the nanoengineered immune niches not just aid in enabling personalized immunotherapy but also help in addressing the disadvantages of existing strategies linked to T cell availability at the tumor site [7].
In this review, the strategies for improving immunotherapy efficacy by using approaches like antitumor immunotherapy and various immune cell-based strategies to improve antitumor response have been discussed. The review also takes into account the strategies for constructing microenvironment responsive nanoplatforms based upon the factors present at higher levels in TME like acidic pH, hypoxia facilitated by poor oxygen supply, higher expression of certain enzymes, and other factors like light, ultrasound and magnetic field and synergism of immunotherapy with other therapies like radiotherapy, phototherapy, gene therapy, and chemotherapy showing high antitumor efficiency compared to the single treatment helping promote immunogenicity, improving therapeutic efficacy and reducing the metastasis.
Existence of inflammatory cells in tumor tissue poses an important challenge in oncology. The inflammatory cells were seen first in human cancer. More efforts are put to understand the purpose of these inflammatory cells in cancer. It has been found that the adaptive and innate immune response results in tumorigenesis by selection of violent clones leading to the increased immunosuppression and activating cancer cell proliferation. In the starting stage of cancer formation, the CD8+ T cells and cytotoxic NK identify and eradicate the immunogenic tumor cells. This elimination phase only screens the proliferation of less immunogenic tumor cell variants and invisible for the detection by the immune system. While the neoplastic tumor tissue grows into a clinical detectable tumor, the various of inflammatory cells decide the tumor fate. Increased amounts of tumor infiltrated T cells is linked with a better cancer prediction whereas higher macrophage infiltration correlates with worse prognosis [8]. Herein, the essential aspects of immune cells associated with cancer with the focus from starting to colonization of tumors would be discussed.
T lymphocytes are extensively studied cell types in the tumors and are second
most important cells found in the human tumors. CD8+ T exert their effect on
priming and upon activation by the antigen-presenting cells (APCs), these cells
get differentiated into CTLs and exhibit antitumoral activity via
exocytosis of the granzyme and perforin-containing granules exerting antitumoral
activity whereas cytotoxic CD8+ T cell reinforced by CD4+ T helper
(Th1) cells by producing Tumor necrosis factor alpha (TNF-
In a process involving T cells, the cancer cells which express immunogenic antigens would be identified and destroyed in the initial tumor development stage. The less immunogenic tumor cells resist T cells and are not killed. This process is called as cancer immune editing. These survived cells adopt an immune resistant phenotype. This results in the resistance to the local cytotoxic response from the NK cells, T cells, tumor associated macrophages (TAMs) and tumor associated neutrophils (TANs). As tumor starts growing, the TME evolves, and new antigens are formed and the immune system capacity to prepare many T cells increases directing them to the tumor modifying the efficiency of tumor suppression. Cancer cells and TME suppress anticancer activity by involving recruiting regulatory CD4+ T cells (Tregs) and immune checkpoints as the immune system prevents cancer growth. Tregs exist in higher amounts in the TME, and its function is to suppress the anticancer activity. Tregs inhibit T cell stimulation and anticancer immune response in lung and breast cancer [8, 9]. Tregs have a main role in the advancement of breast tumor by suppressing the anticancer activity by various mechanisms [8].
The immunotherapy utilizes the antigen specific T cell attack for fighting against tumor. The key problem is recognizing the phenomenon by which tumor cells undergo changes to avoid attack by T cells. Furthermore, understanding the heterogeneity of the tumors will help in developing better immunotherapies for cancer.
B cells possess both negative and positive roles in the immunity against cancer [9]. There are reports on the efficiency of B cells increasing the T cell functionality in the mouse models in squamous carcinogenesis [10]. Presence of CD20+ B cells in cervical carcinoma [11], gastric cancer [12], breast [13], lung cancer [14], prostate cancer [15] is linked with better prognosis. Importance of B cells in cancer therapy poorly known to date. Reports have indicated that B cells support and promote tumor growth. Ammirante & co-workers (2010) [16] demonstrated that B cells, employed by chemokine C-X-C motif ligand 13 (CXCL13), facilitate the prostate cancer development by producing lymphotoxin. de Visser et al. (2005) [10] showed that the tumor progression was found to be decreased when the mature B cells were absent. The adoptive transfer of B cells was found to increase angiogenesis, chronic inflammation and tumor growth. Though lymphotoxin could aid in tumorigenesis, the cytokine produced by B cells can aid in the tertiary lymphoid organs (TLOs). The number of TLOs correlates with the advantageous results in human and mouse models. Occurrence of B cells in TLOs has helped in the prognosis leading to the longer survival in cancer [17]. B cells possess ability to make cytokines, chemokines and also recruiting the immune cells to the TLOs, secondary lymphoid organs (SLOs) and other important effector sites [17].
The portion of B cells inducing immunosuppression are known as regulatory B
cells. Immunogenic chemotherapy in human and mouse prostate cancer need B cell
subtype removal, IL, plasmocytes expressing IgA, and Programmed Death-Ligand 1
(PD-L1) the presence of which is dependent on the TGF-
The role of DCs is to attack the antigens found in configuration of peptide
major histocompatibility complex (MHC) and presenting those antigens to the T
cells [9]. Stimulation of immune cells facilitates inflammation and disturbs
tissue homeostasis and also is linked with the cancer development. Main mechanism
is controlled by myeloid-derived IL-6, that stimulates the transcription factors
namely, nuclear factor-
NK cells display a very fast cytolytic activity to the infected cells. These
cells possess stimulatory and inhibitory receptors onto their surface and are
used in immune surveillance and recognize peptides presented on the MHC
molecules. These NK cells help not only in destroying the cancer cells by
releasing cytolytic granules but also release cytokines and chemokines
stimulating the immune response [8, 9, 19, 20]. Main characteristic of NK cells
is their inhibition by the receptors binding to MHC Class I and because of this
reason NK cells destroy tumor cells lacking MHC-I. In normal cells, the receptors
binding to the MHC-I molecules possess an inhibitory effect on the NK cell
function [9]. Also NK cells could negatively affect anticancer responses by
modulation of T and DC cells [9]. Glasner & group (2018) [21] showed a new way
by which NK cells modulate immune response. A study reported that the NK
cytotoxic receptor activation in mouse and NKp46 in human leads to enhanced
production of IFN-
The TAMs possess a main function in the cancer associated inflammation.
Macrophages play a vital role in every step starting from the early phase to the
metastatic cancer progression stage to the resistant to therapy stage. According
to the clinical and pre-clinical data, TAMs are linked with the poor prognosis
and reduced survival of cancer patients. Macrophages on activation are known as
pro-inflammatory (M1 type) facilitated by IFN-
Neutrophils comprise approximately 50–70% of the leukocytes and display
primary defense against any infection. In the TME, the key phenomena facilitate
polarization of neutrophils in the different subpopulations viz. N1
(antitumorigenic), N2 (protumorigenic), and TANs [9]. TANs are thought to be
associated with the inflammation during the start and progression of cancer. In a
study reported by Chang & co-workers (2014) [27] in a lung adenocarcinoma model
in mouse, IL-17 responsive TANs were found to encourage cancer growth. Neutrophil
elastase is an enzyme secreted at the inflammation site which encourages
angiogenesis, tumor invasion and proliferation [28, 29]. Recent reports have
showed that the neutrophils display a key function in the awakening of dormant
cells and tumor metastasis growth [30]. TGF-
The TME refers to the unique milieu arising due to interactions among the tumor and host as the tumor progresses resulting in the cellular and molecular crosstalk of events within the surrounding tissue. The TME promotes the tumor proliferation and survival while protecting it against the host immune system. Apart from the tumor cells, it constitutes stromal cells, immune system cells (viz. DC, B cells, T cells), myeloid-derived suppressors cells (MDSCs), TAMs, cancer-associated fibroblasts (CAFs), lymphatics, extracellular matrix (ECM), and tumor vasculature [34, 35]. The ECM (a physical scaffold for the cells of the TME) actively promotes metastasis, as the movement of a cell in and out of the TME depends on its adhesion to the ECM [36]. Transitions in the TME take place due to a combination of biomechanical and biochemical changes of the ECM [37]. A complicated network of cytokines, growth factors, and chemokines are present in the TME. It is an extremely heterogenic and functional environment owing to a complex interaction among its constituents and the host immune system.
Pathological interactions between immune components within the TME and cancer cells gives rise to an immunosuppressive network because of which attack by the host immune cells are shielded and tumor growth is promoted (Fig. 1). The complex network formed by immune cells (T regulatory cells, MDSCs, TAMs, DC) in the TME helps to escape the cancer cells to immune surveillance [38]. The immunosuppressive mechanisms of cancer cells are manifold which avoids immune recognition and reduces or disables effector T cells by mimicking important signalling pathways to gain immune tolerance, altering antigen presenting machinery, secreting immunosuppressive cytokines and inhibitory factors, to name a few [39]. Extrinsic and intrinsic factors, such as an increase in MDSCs and T regulatory cells or antigen loss tumor variants selection, both favour immune surveillance escape. The interaction of immunosuppressive cells (T regulatory cells, MDSCs, TAMs) with effector T cells is critical in understanding the mechanism of immunosuppression [40]. Sub-population of T regulatory cells builds up in the tumor tissues and hinder antitumor responses in cancer patients although they can control immune homeostasis in peripheral tissues [41].
 Fig. 1.
Fig. 1.
Immunosuppression mechanisms in tumor microenvironment.
TGF-
Tumor progression is promoted by an enrichment of immunosuppressive cells in “cold tumors” referring to non-T cell inflamed tumors. Whereas tumor regression can occur in “hot tumors” which are T cell-inflamed in which the epitopes of tumor cells can be identified by tumor infiltrating T cells [42, 43]. High expression of the CAF membrane protein FAPa in epithelial tumors might reduce hypoxic necrosis as demonstrated in vitro which could relate to tumor growth control in vivo, thus throwing light on the importance of these cells as immunosuppressors in the TME [44]. The abnormal metabolism of tumor cells along with microenvironmental factors like hypoxia, acidic conditions, and high interstitial fluid pressure accelerates survival of the tumor. High interstitial fluid pressure prevents immune cells recruitment in the tumor site [45]. Hypoxia promotes vascularization, the activation of several signalling pathways, and the expression of pro-angiogenic factors, which leads to metastasis and tumor aggressiveness [46]. The development of immunosuppressive cells is promoted in tumor’s low pH which also inhibits T cell infiltration and activation of TAMs [47].
Immune checkpoints are the immune system’s inhibitory pathways, which protects tissues from damage while fighting pathogens, provide tolerance to self-antigens and maintain homeostasis. To prevent autoimmunity, T cell activation or effector functions need to be downregulated. A lot of research indicates that evasion of the immune system by tumors occur through engagement of immune checkpoints [48]. Therefore, agents that modulate immune checkpoints are of specific interest in immunotherapy.
The first immune checkpoint receptor targeted is CTLA-4. CTLA-4 is responsible for reducing the amplitude of T cell activation by opposing cluster of differentiation 28 (CD28) co-stimulatory signal. CD80 (or B7.1) and CD86 (or B7.2) are the two common ligands shared by CTLA-4 and CD28, with CTLA-4 having a higher affinity of ligand binding, thus outcompeting CD28 which ultimately leads to reducing the T cell response.
CTLA-4 knockout in mice lead to immune hyperactivation and is lethal, thus demonstrating its critical role in controlling T cell activation. Antibodies that will bind to CTLA4 and block its immunosuppressive signal, as a result in T cell activation (tumor antigen activated T cells) and proliferation, which leads to cytokine production and cytotoxicity [48]. The Food and Drug Administration (FDA) approved anti-CTLA4 therapy for advanced melanoma patients in 2010, making it the first agent to show a benefit in patient survival [49]. In the year 2000, pre-clinical findings led to the start of clinical testing of fully humanised CTLA4 antibodies ipilimumab and tremelimumab. After much careful testing and evaluation, the FDA approved ipilimumab for advanced melanoma treatment in 2010 [49]. Several Phase II trials are currently underway for tremelimumab, for example, in combination with durvalumab for bladder cancer and pediatric cancer and tremelimumab alone in patients who have previously received programmed cell death-1 (PD-1) blockade [50, 51, 52].
PD-1 is another immune checkpoint receptor which is known to show immunotherapeutic effects. It is like CTLA-4, regulates the balance of T cell activation and immune tolerance. PD-1 is also present on NK cells and B cells along with T cells [53, 54]. Another difference between these two receptors lies in their regulatory impact on T cell function. Specifically, PD-1 suppresses the activity within peripheral tissues, while CTLA-4 exerts its inhibitory effects within lymphatic tissues [48]. PD-1 can be exploited by tumors causing CTLs and NK cells anergic and non-cytotoxic. PD-L1, one of its ligand, has been found to be upregulated in melanoma, lung, ovarian and several other solid tumors. Compared to the CTLA-4 knockout mice, knocking out the pdl, pdl1 and pdl2 genes results in a milder phenotype [48]. PD-1/PD-L1 blocking agents under clinical trials are nivolumab [BMS-936558], lambrolizumab [MK-3475], MPDL3280A, pidilizumab [CT-011], avelumab [MSB0010718C], MEDI4736 and the anti-PD-1 fusion protein, AMP-224 [55, 56, 57, 58, 59, 60, 61].
The transmembrane protein receptor lymphocyte activation gene 3 (LAG3) is present on T regulatory cells, CD4 and CD8+ T cells, NK cells, B cells, and plasmacytoid DC [62]. When activated, it acts as an immune checkpoint receptor, suppressing immune cell activity. It attaches to the MHC Class II complex on APCs and is thought to bind to Galectin-3 to influence effector T cell responses [63, 64]. The blocking of LAG3 is expected to improve the cytotoxicity of T cells. The pharmacological LAG3 blocking agents currently under clinical trials are IMP321, BMS-986016, MK-4280 and LAG525 [65, 66, 67, 68].
A member of the T cell immunoglobulin and mucin-domain-containing (TIM) gene family, the transmembrane protein TIM-3 is found on Th1 cells, DC, CD8+ T cells and monocytes. Galectin-9, Ceacam1, High Mobility Group Box 1 (HMGB1) and phosphatidylserine are known to bind to TIM-3 [69]. T cell anergy is caused by the interaction of TIM-3 to its ligands. Combined checkpoint inhibitor therapy of TIM-3 with PD-1 along with focal radiation showed survival improvement in in murine gliomas [70]. Phase I clinical trials of monoclonal antibodies against TIM-3 are underway: TRS-022 alone or in conjuction with anti-PD-1 (Clinical Trial ID: NCT02817633) [71] and Sym023 (Clinical Trial ID: NCT03489343) [72].
V-domain immunoglobulin suppressor of T cell activation (VISTA), like PD-1 and CTLA-4 from the B7 family of T cell coreceptors, is a checkpoint inhibitor and suppressor of T cells. It is found on neutrophils, macrophages, and T cells [73]. VISTA and its ligand V-Set and immunoglobulin domain containing 3 (VSIG-3) have shown T cell inhibition when tested in vitro [74]. Studies in mice have also shown the response of VISTA against tumors [75]. CA-170, an antagonist of VISTA/PD-1 recently completed Patients diagnosed with solid tumors or lymphoma are being enrolled in a phase I clinical trial (Clinical Trial ID: NCT02812875) [76].
The IDO pathway is another regulator in the TME, which is often exploited by tumor cells. T cell activity requires tryptophan which is broken down by IDO to control damage from excessive activation of the immune system. Therefore, IDO inhibitors are another option to boost T cell response [77].
Nanoparticles hold promise for delivering immunotherapeutic agents in cancer treatment, aiming to enhance efficacy and safety through nanoengineering [78]. However, challenges in clinical translation arise due to the complexity of formulating and modifying nanoparticles, leading to difficulties in reproducibly manufacturing clinical-grade products at a scale [78, 79]. The key factors impacting translation include safety, biocompatibility, specificity, stability, manufacturing scalability and regulatory approval. Barriers to clinical translation include suboptimal targeting efficiency, safety concerns, scalability limitations, and in sufficiently representative tumor models [80]. Enhancing nanoparticles safety and biodistribution is crucial for clinical utility, with toxicity concerns posing significant obstacles during pre-clinical development [80]. Optimized nanoparticle characteristics are essential to prevent unintended nanoparticle accumulation in clinical trials [81]. Factors like size, charge and stability profoundly influence nanoparticle distribution and safety, with modifications such as ligand attachment and polymer alteration impacting nanoparticle safety [82]. Biocompatible lipids like low-density lipoprotein and high-density lipoprotein show promise in clinical trials for drug delivery, with adjustments in lipid ratios improving stability and preventing burst release [83]. Synthetic biomaterials are explored due to challenges in obtaining natural lipids. Incorporating polymers enhances nanoparticles stability and reduces toxicity in animal models [84, 85]. Strategies to improve nanoparticles distribution within tumors are evolving, considering TME’s complexity [80]. Lowering nanoparticle dosage through enhanced delivery systems and potent drug cargos reduce toxicity risks, with targeted delivery improving efficacy and reducing side effects [86, 87]. Balancing potency with favorable biodistribution is essential. Overall, optimizing nanoparticles characteristics and delivery methods holds promise for safer and more effective clinical translation. Further, efficient and scalable nanoparticle production is vital for clinical translation. Strategies like the microfluidics, two-vial system, flash nano-precipitation (FNP) and quality by design (QbD) enables scalable nanoparticle manufacturing [80]. The two-vial system, validated in a phase I clinical trials, allows bedside mixing while preserving nanoparticle activity [88]. Microfluidics and FNP offer precise control, promising automated mass production [89, 90]. While these methods have been successful in formulating functional nanoparticles, however, scalability for large hydrophilic molecules remains challenging [91, 92]. Considering scalability early in nanoplatform development is crucial to prevent inefficiencies. QbD principles aid in understanding formulation effects on nanoparticles properties, facilitating models for improving scalability [80].
Polarization of functions occur in macrophages as diverse environmental signals
result in the activation of a wide variety of intracellular transcriptional
networks in them. The classically simulated M1 macrophages are initiated by
Granulocyte macrophage colony-stimulating factor (GM-CSF), IFN-
Macrophages express Toll-like receptors (TLRs), when activated, they cause M1 polarization. TLR agonists were studied in mice for their capacity to reprogram TAMs and cause an antitumor effect. 3M-052, a TLR7/8 agonist, increased the systemic antitumor effect upon local delivery by repolarization to M1 TAMs which have a nitric oxide-producing property and could eradicate metastatic melanoma [95]. A TLR8 agonist, motolimod was used in standard combination treatment with chemotherapy/cetuximab in a randomized clinical trial to investigate the effect on squamous cell carcinoma of head and neck (SCCHN) patients. Overall survival of patients was not improved, although, a subset of the patients (those with human papilloma virus (HPV) disease and injection site reactions) showed improved outcomes relating to overall and progression-free survival [96].
The use of CD40 agonists is another strategy to for TAM repolarization to
pro-inflammatory phenotype. CD40 is highly expressed on macrophages, and it
causes delivery of pro-inflammatory cytokines and CD80/CD86 expression to support
T cell functions [93]. Depletion of TAMs in pancreatic ductal adenocarcinoma
patients by administration of anti-CSF-1R could increase endogenous T cells
within the tumor but showed poor longevity. When TAMs were reprogrammed with
agonist anti-CD40, both the accumulation and the persistence of the engineered T
cells were increased. However, this strategy failed to maintain cytokine
production of the engineered T cells [97]. Synergistic effect of CSF-1R
inhibitors and anti-CD40 mAbs enhanced therapeutic outcome in a melanoma mouse
model. The M2 state in tumors which were secreting MMP9, and CCL17/22 was
converted into an inflammatory population of TAMs secreting TNF-
CCL2 is a chemokine that recruits monocytes from bone marrow to peripheral blood, which they subsequently migrate to the tumor site and differentiate into TAMs. Targeting CCR2 with an inhibitor (PF-04136309) in conjunction with chemotherapy was found to be risk-free in individuals diagnosed with pancreatic ductal adenocarcinoma [99]. Dual targeting using CSF-1/CSF-1R inhibition and CD40 agonism to overcome the suppressive myeloid population in the TME showed enhanced antitumor effect [100]. Inhibition of CSF-1R was also found to block the growth and progression of glioblastoma (GBM) not through depletion of TAMs but through their “re-education” or repolarization [101].
A novel strategy of chemoimmunotherapy based on selective targeting to simultaneously target tumor cells and TAMs were developed by Wang & group (2019) [102]. Core-shell nanoparticle structure containing sorafenib and IMD-0354 as the agent for TAM repolarization were prepared as a co-delivery system that could provide separated cell targeting and robust anticancer activity [102]. TAM repolarization by modulation through innate defence regulators, was studied using RP-182 which induces a conformational switch in CD206, a mannose receptor on M2 macrophages. Due to the switch, the M2 macrophages converted to M1 type and showed improved adaptive and innate immune responses because of increase in endocytosis and apoptosis. Therefore, RP-182 was able to shift the immunosuppressive cells to a phagocytosing phenotype [103]. Receptor-interacting serine/threonine protein kinase (RIP-1) is upregulated in TAMs in the case of pancreatic ductal adenocarcinoma and targeting these TAMs using a selective inhibitor of RIP-1 could reprogramme them through STAT-1 towards an immunogenic phenotype. RIP-1 inhibition resulted in high production of cytotoxic T cells and T helper cells of Th1/Th17 mixed phenotype which is distinctly immunogenic. This study showed tumor immunity in both organotypic human models and mice of pancreatic ductal adenocarcinoma [104].
Iron has the ability to repolarize macrophages associated with tumors from tumor-promoting M2 to antitumor M1 type. Polydopamine iron chelate nanoparticles were designed for TAM repolarization which could also act as a photothermal therapy (PTT) agent. The repolarized TAMs could apprehend and present tumor-associated antigens (TAAs) (released after PTT) to T cells thus eliciting an antitumor response. The immunosuppressive TME could be reversed due to the antigen presentation and increased infiltration of T cells [13]. Iron based metal organic frameworks with macrophage targeting peptide loaded with diclofenac were developed to efficiently target M2 macrophages and repolarize them to M1 type. Additionally, the role of diclofenac was to maintain the retention of iron through activation of hepcidin/ferroportin pathway. By overcoming the immunosuppression and activation of CD8+ T cells, effective remodelling of the TME with long term memory could be achieved [105]. The macrophage activating function of iron oxide nanoparticles depended on the structure of the nanoparticles as studied by Gu & group (2019) [106]. They found out that magnetite iron oxide nanoparticles are more potent than hematite iron oxide nanoparticles at macrophage polarization and tumor inhibition. The M1 polarization occurred through the IFN regulatory factor 5 (IRF5) pathway and arginase-1 expression was inhibited by magnetite to impair M2 functions. This pathway favoured activation of CTL and antitumor activity. Superparamagnetic iron oxide nanoparticles (SPIONs) coated with hyaluronic acid (HA) were developed as a reprogramming nanoparticle-assisted strategy. The HA coating facilitated better internalization of the nanoparticles by the macrophages resulting in inflammatory and apoptotic effects and re-educating macrophages to M1 type. This cell reprogramming approach proved to be efficient in antitumor activity and could drive forward cell-typed therapeutics in the future [107].
Combination of ferroptosis and TAM repolarization for cancer therapy was developed with gold nanocages. Loading of doxorubicin (DOX) and L-buthionine sulfoximine increased reactive oxygen species (ROS) accumulation and glutathione (GSH) consumption, thus inducing ferroptosis. Gold nanocages are known to have good photothermal properties under near-infrared (NIR) radiation. Collectively, accumulation of ROS and photothermal effect could reprogramme TAMs and effective tumor ablation was achieved [108]. Gold nanorods encapsulating paclitaxel and modified with albumin were synthesized as a combination of photothermal and chemotherapy. Effective antitumor activity was achieved with PTT displaying the ability to modulate TAMs and thus overcoming immunosuppression of the TME. The suppression was dose-dependent, and an illumination time of 3 minutes showed the best effect [109].
The Ru-based nanoparticles were designed as multifunctional vehicle which could release drugs at tumor site in response to inflammatory microenvironment and caused vigorous tumor elimination in a dual mode: by repolarizing TAMs and by inducing hyperthermia and production of ROS. Sotuletinib being one of the drugs acts as a CSF-1R signal inhibitor thus causing the repolarization of TAMs into M1 type. This study combines repolarization strategy with traditional PTT to produce a better anticancer goal [110]. Encapsulation of nanoparticles with cell membranes is a promising approach in bioinspiring nanotechnology to improve circulation time and hemocompatibility. Combining this with PTT, 2D MoSe2nanosheets were developed as a biomimetic antitumor delivery system with enhanced biocompatibility and elevated photothermal conversion efficiency. The photothermal effect of the nanosheets caused reprogramming of TAMs thus showing effective immunotherapy [111].
Antigen presenting cells are activated by extracellular ATP through purinergic
receptors [112]. Immune suppression is produced during ATP enzymatic degradation
when the byproducts AMP and adenosine are bound to adenosine A2a receptors [113].
Thus, to overcome immunosuppression, inactivation of the enzymes [114, 115] that
degrade ATP and adenosine A2a receptors are a potential option [116, 117].
Indoleamine 2,3-dioxygenase-1 (IDO1) is another target in immunotherapy for
overcoming immunosuppression. IDO1 is a metabolic enzyme that catalyzes the
conversion of tryptophan to kynurenine, and it is abundant in tumor cells. This
causes low levels of tryptophan and accumulation of kynurenine which results in
reduction of T cell activity, cytotoxicity of on effector T cells and distinction
into T regulatory cells [118]. Inhibitors and blockers of IDO1 like
methyltryptophan shows antitumor activity in preclinical studies [119]. Other
amino acid targets include glutamine and arginine. The hypoglycaemic profile,
lactate profile and fatty acid metabolism of the TME can be targeted to achieve
antitumor activity. There are also studies on using the nutrient and oxygen
sensing pathways as targets [120]. Exhaustion of lactic acid is another approach
towards metabolic therapy in cancer. An MnO2 system camouflaged with red
blood cell membrane and incorporated with lactate oxidase and a glycolysis
inhibitor was developed for metabolic therapy in conjunction with immune
checkpoint therapy as a synergistic strategy. The red blood cell membrane
rendered long circulation and subsequent accumulation of the nanosystem in the
tumor. The low pH of the TME and endogenous H2O2 causes release of
lactate oxidase from the MnO2 system which oxidizes lactic acid and consumes
it up. The glycolysis inhibitor depleted the source of lactic acid and blocked
ATP as well. These effects together resulted in converting the immunosuppressive
TME to an immunocompetent one as macrophages were activated via TLR and
NF-
Extensive research through pre-clinical studies and clinical trials have led to
a vast exploration of immunotherapy against cancer. However, in the overall
population and clinical setting, the response rates towards immunotherapy are
quite low for majority of patients. Resistance to immune therapy can be
conceptualized as primary, adaptive, and acquired. Some patients fail to show any
response from the treatment, which is termed as primary resistance, while some
stop responding after an initial period of benefit which is termed as acquired
resistance. In the case of adaptive resistance, the immune system recognises the
cancer, but the immune attack is not successful because the cancer can protect
itself by adapting to the immune attack. Immune therapy was unsuccessful in
several common types of cancers and variance in response has been observed in
distinct tumors of the same patient as well. The resistance mechanisms and immune
responses of patients are very dynamic and depends on many factors related to
treatment interventions. Intrinsic mechanisms for resistance to immunotherapy
include lack of tumor antigens and deficiency in T cell recognition, alterations
in signalling pathways (Mitogen-Activated Protein Kinase (MAPK), Wingless-related
integration site (WNT), IFN-
Immunotherapy stands at the cutting edge of cancer treatment, representing a groundbreaking approach that makes use of the body’s immune system to combat cancer. While traditional therapies like surgery, chemotherapy, and radiation have been cornerstones in cancer management, some tumors develop resistance mechanisms, making them less susceptible to these conventional treatments [123]. Nanotherapeutics, though promising, have shown limited efficacy in significantly impacting patient survival compared to established therapies. However, immunotherapy has emerged as a game-changer, demonstrating remarkable success in managing advanced-stage cancers [124]. This innovative therapeutic strategy employs several tactics, including DC-based therapy, T cell-based therapies like chimeric antigen receptors (CARs) T cell therapy, immunogenic cancer cell death induction, anticancer vaccines, monoclonal antibodies, bi-specific antibodies, and oncolytic virotherapy (OV). These strategies aim to bolster the immune system’s capacity to recognize and selectively target cancer cells, potentially leading to their elimination [125].
Immunotherapy’s underlying principle revolves around activating the immune response of the body to specifically detect and eliminate cancer cells while sparing healthy tissues. Its targeted specificity holds significant promise, given its potential not only for the elimination of cancer cells but also for potentially preventing tumor recurrence [126]. An ideal immunotherapeutic agent should possess specific characteristics: the ability to precisely target cancer cells, robust effectiveness in eliminating tumor cells, and durability in maintaining its efficacy over time [127]. By harnessing the body’s natural anti-cancer defences, immunotherapy offers hope in overcoming the limitations associated with conventional cancer treatments, hinting at a future where more effective and precisely targeted therapies can be offered to cancer patients, potentially transforming the field of cancer care. Ongoing research and advancements in immunotherapeutic strategies continue to pave the way for more tailored and impactful cancer treatments across various types of cancer [128].
Immunotherapy’s success lies in its ability to the immune system towards the recognition and eradication of cancer cells while sparing healthy tissues. Although research has advanced understanding and application, the immune system’s complexities persist, evidenced by certain immunosuppressive drugs, like rapamycin and rapalogs, showing utility in cancer therapy and prevention [129]. Thus, a careful approach to manipulating compounds within the immune system remains crucial for effective cancer treatment and prevention.
The DCs play a pivotal role in regulating and coordinating immune responses within the body [130]. As professional APCs, they possess a distinctive capability to initiate, sustain, and modulate T cell responses, thereby bridging a link between the adaptive and innate components of the immune system. This orchestration is vital in combating tumor cells, where the immune system’s innate response serves as the initial defence, followed by the adaptive response [131].
One of the critical functions of DCs is to serve as a link between these immune responses by introducing antigens to T cells, triggering cell activation, and augmenting immune reactions [123]. DCs hold paramount importance in stimulating antitumor immunity by recognizing various entities like microbes and tumor cells, aided by specialized receptors on their surfaces. DCs effectively internalize antigens after recognition via efficient phagocytic and endocytic mechanisms. Subsequently, they process these captured antigens to facilitate both class I and II presentation. This process triggers an upsurge in DCs’ ability to present these antigens to T cells, amplifying the immune response [132].
The maturation of DCs is stimulated by tumor-derived molecules, including high mobility-group box 1 proteins and heat shock proteins. Along with proinflammatory cytokines generated by immune cells within the TME. Additionally, the maturation is influenced by proinflammatory cytokines released by immune cells within the TME. Mature DCs migrates from the tumor site to SLOs, where they instigate the activation of tumor-reactive CD8+ CTLs and CD4+ T cells. The CD8+ CTLs play an essential role in recognizing and eradicating tumor cells presenting peptides derived from TAAs in conjunction with human leukocyte antigen (HLA) class I molecules [133]. Simultaneously, CD4+ T cells aid in enhancing the capacity of DCs to generate CTLs through interactions like CD40-CD40 ligand and provide support for the maintenance and development of these CTLs through cytokine secretion, such as IL-2 [134].
The use of antigen-pulsed DCs, which are prepared by in vitro loading of specific antigens onto DCs, represents a potential method for evoking immune responses in cancer patients and also in individuals suffering from a variety of clinical diseases [135, 136]. The process involves the expectation that DCs will identify, uptake, internalize, and process antigens in vitro, and subsequently, these antigen-loaded DCs might migrate directly to lymphoid tissues, activating lymphocytes and triggering TAAs-specific immunity [137].
Immature DCs demonstrate particular efficiency in capturing tumor-derived material in peripheral tissues. They internalize these antigens, undergo processing, and upon migrating to T cell-rich zones in secondary lymphoid tissues such as lymph nodes, they undergo maturation and express co-stimulatory molecules. Besides their exceptional capability to elicit and stimulate T cell responses, DCs significantly enhance natural killer cells immunomodulatory and cytotoxic potential, which contribute significantly to eradicating tumor cells. Additionally, DCs have the ability to directly mediate cytotoxicity against tumor cells, demonstrating their multi-faceted antitumor effects [138].
The preparation of DCs is primarily achieved by isolating them from peripheral
blood mononuclear cells (PBMCs), with monocyte-derived DCs (moDCs) being more
commonly employed, given the restricted availability of CD34+ precursors
[139]. These cells are initially created as immature DCs using granulocyte
macrophage colony-stimulating factor (GM-CSF), IL-4, or IFN-
Recent advances in DC-based immunotherapy involve employing neoantigens for loading DCs aiming to elicit more robust immune responses and the development of rapid, standardized, and automated production of DC vaccines comprising natural DC subsets. These advancements hold promise in improving the quality of DC vaccines and enabling multicentre trials. Combining DC vaccination with other therapeutic approaches such as monoclonal antibodies against chemotherapy, immune checkpoints, cytokine-induced killer cells (CIK), radiotherapy, or nanoparticles shows potential in further enhancing anticancer immunity. However, the optimal combination treatment regimen requires further investigation and refinement through comprehensive research in this domain [141].
Numerous clinical trials are currently exploring the therapeutic potential of DC vaccination in various cancer types, signalling a significant advancement in cancer treatment strategies. These trials represent a diverse array of cancer types and investigate the safety and effectiveness of DC vaccination either as a standalone therapeutic approach or in combination with ICIs, aiming to augment anti-tumor immune responses. For example, a Phase III trial (NCT04855275) focuses on advanced melanoma, assessing the synergistic effects of an autologous DC vaccine combined with PD-L1 blockade across multiple sites in the United States and Europe. Simultaneously, a Phase II trial (NCT03918174) is evaluating DC vaccination in tandem with nivolumab for advanced non-small cell lung cancer (NSCLC) in various locations in the US and Canada. In a parallel effort, a Phase II trial (NCT04940393) investigates the combination of DC vaccination with pembrolizumab for metastatic CRC, involving multiple sites across the US and Australia. Additionally, a Phase I/II trial (NCT04656486) targets pancreatic cancer antigens with DC-based vaccines in the United States, while a Phase I/IIa trial (NCT03541087) explores DC vaccination in advanced SCCHN patients.
The phase I study (NCT01730118) explored a Human Epidermal Growth Factor Receptor 2 (HER2)-targeting DC vaccine in metastatic cancer and high-risk bladder cancer expressing HER2. It had two parts: one for bladder cancer progression after standard treatment or no conclusive evidence of disease, and another for cancer progression after anti-HER2 therapy. The vaccine, generated from autologous monocytes transduced with AdHER2, was administered in five doses. Among 33 patients across different dose levels, 33.3% showed clinical benefit, including one complete response, one partial response, and five stable diseases. No cardiac toxicity was observed, and adverse events were mainly injection-site reactions. After three doses, 23.1% displayed an antibody response, and 90.9% exhibited anti-HER2 responses in lymphocytes, with multifunctional immune responses in 72.7%. The AdHER2 DC vaccine showed promising preliminary clinical benefit and immunogenicity, indicating potential for further combined therapeutic applications [142].
Adoptive T cell therapy represents a groundbreaking approach in cancer treatment by leveraging a patient’s immune cells to target and eliminate cancer [143]. TILs are first derived from the patient’s tumor tissue. These TILs, harbouring potential antitumor activity, are then cultured and developed ex vivo before subsequent reintroduction into the patient as portrayed in Fig. 2A. Despite showing promise in some cases, TIL therapy presents logistical challenges due to the difficulty in isolating and expanding sufficient TILs for effective treatment, along with the need for substantial resources and time.
 Fig. 2.
Fig. 2.
Adoptive T-cell therapy for cancer treatment. (A) Approaches for the adoptive transfer of a patient’s own T cells for cancer therapy. (B) T-cell receptors and Chimeric antigen receptors engineered to target cancer cells. MHC, major histocompatibility complex; TCR, T-cell receptor; CAR, chimeric antigen receptors.
Researchers have turned to genetic engineering to create more effective cancer-targeting T cells to overcome these limitations. This involves modifying a patient’s T cells outside the body to express specific receptors capable of identifying and attacking cancer cells. Two primary types of receptors used in adoptive T cell therapy are CARs and T cell receptors (TCRs) depicted in Fig. 2B.
TCRs are genetically engineered to detect unique cancer epitopes presented on the tumor cell surface by major MHC molecules. This personalized approach aims to create TCRs tailored to a patient’s specific cancer type, enhancing specificity in targeting tumor cells while mitigating damage to healthy tissues.
On the other hand, Chimeric antigen receptor (CAR) T therapy implies modifying T cells to express CARs that combine an antibody’s extracellular domain’s antigen-recognition capability with T cell signalling domains. This configuration allows CAR-T cells to recognize cancer-specific antigens independently of MHC molecules, broadening the range of tumor targets [144, 145, 146, 147].
Despite the potential of TILs and genetically modified T cells, there are challenges. TIL therapy’s personalized nature limits its scalability and efficiency due to the complex and costly process of isolating and growing these cells. Additionally, the administration of high-dose IL-2 alongside adoptive transfer may lead to severe side effects.
Genetically modified TCRs have shown promise against certain cancers, yet they may also cause off-target effects, damaging healthy tissues expressing the targeted antigen. CAR-T therapies, targeting antigens like CD19, have gained approval for certain types of leukemia and lymphoma, demonstrating remarkable efficacy, but they can be linked to adverse effects like cytokine release syndrome (CRS) and neurotoxicity [35, 48].
Continued research aims to improve the effectiveness and safety of adoptive T cell therapy. Scientists explore strategies like synthetic sensors and switches to control T cell activity more precisely and are also investigating genome editing and cellular engineering techniques to optimize the therapeutic potential of these T cells that have been genetically modified. Advancements in this field may lead to more efficient and safe cancer treatments in the future.
The overactivation of antigen-specific T cells, while a vital part of the immune response, can sometimes lead to serious side effects, including CRS and damage to healthy tissues. The immune system employs a variety of inhibitory mechanisms to regulate T cell activity.
Inhibitory receptors like CTLA-4 and PD-1, along with PD-L1, play vital roles in controlling T cell activation. Additionally, regulatory T cells (Tregs) expressing CD4, CD25, and forkhead box protein 3 gene (FOXP3), also IL-2-mediated activation-induced cell death (AICD), contribute to immune regulation [148].
CTLA-4 and PD-1/PD-L1 checkpoint blockade function at various phases of the immune response and exert distinct effects on T cells. CTLA-4 acts at initial stage, affecting T cells in lymphoid organs, whereas PD-1/PD-L1 modulation occurs in peripheral tissues during later immune responses. PD-1 blockage revives dormant T cells to reinstate their anticancer activity, while inactivation of CTLA-4 leads to the stimulation and proliferation of new T cell clones and diminishes the suppressive action of Tregs [149].
When comparing PD-1/PD-L1 and CTLA-4 blockades, PD-1/PD-L1 inhibition has a more targeted effect on antitumor T cells. Continuous exposure to antigens enhances the therapeutic effectiveness of PD-1/PD-L1 blockade with reduced toxicity. Several FDA-approved medications, such as Pembrolizumab (Keytruda®), Nivolumab (Opdivio®), Cemiplimab (Libtayo®), Avelumab (Bavencio®), Atezolizumab (Tecentriq®), and Durvalumab (Imfinzi®), target PD-1 or PD-L1, and are utilized in the treatment of various cancers including Hodgkin’s lymphoma [35].
These immunotherapies that target PD-1 or PD-L1 have revolutionized cancer treatment by releasing the immune system’s ability to fight cancer. They have shown remarkable efficacy in certain cancers, offering durable responses and improved survival rates for many patients, while their selective action on specific T cell subsets minimizes adverse effects compared to traditional chemotherapy. However, further research continues to refine these therapies to optimize their efficacy and mitigate potential adverse effects.
Recent trials using increased lymphodepletion before infusing autologous TIL achieved impressive response rates of 49% to 72%. Persistence of infused cells, their characteristics, and the removal of suppressor cells before treatment contribute to its success. ACT’s (Adoptive cell therapy’s) bility to generate durable responses across various sites signifies its potential. Ongoing efforts focus on refining ACT by modifying lymphocyte genetics, altering cell functions, and exploring vaccines to stimulate transferred cells [150].
The ELIANA trial, using Tisagenlecleucel in paediatric and young adult individuals diagnosed with CD19+ relapsed or refractory B-cell acute lymphoblastic leukemia (ALL), yielded impressive results, with an overall remission rate of 81% at three months. Moreover, the survival probability at six months reached a notable 73%. Meanwhile, the ZUMA-1 trial, involving patients with primary mediastinal B-cell lymphoma (PMBCL), diffuse large B-cell lymphoma (DLBCL), or transformed follicular lymphoma (TFL), demonstrated encouraging outcomes, showing an 82% overall remission rate. However, the 18-month survival rate was observed to be 52% [151, 152].
Notably, the FDA’s approval of Axicabtagene Ciloleucel for treating various lymphomas in adults and Tisagenlecleucel for refractory or relapsed ALL in young patients, along with certain cases of DLBCL in adults, marked significant milestones in CAR T-cell therapy for hematological malignancies.
The discussion around CAR T-cell therapy for solid tumors highlighted substantial challenges. While specific trials were not detailed, the obstacles in this realm are multifaceted. They encompass difficulties in selecting appropriate Tumor-associated antigens (TAAS) crucial for effective therapy, inadequacies in T cell infiltration into tumors, and the hostile nature of TMEs. Furthermore, issues related to T cell self-regulation add complexity to this therapeutic approach [132].
Moreover, the presence of toxicities associated with CAR T-cell therapy further underscores its complexity. These include on-target off-tumor effects such as CRS, anaphylaxis, and neurotoxicity. These complexities and limitations pose significant hurdles to extending CAR T-cell therapy successfully to the treatment of solid tumors.
Apoptosis, once viewed as a non-inflammatory process, is now known to potentially evoke an immune response under specific conditions, termed immunogenic cell death (ICD). This phenomenon occurs when cells undergoing apoptosis release specific substances, including ATP, HMGB1, and calreticulin, which signal the immune system to detect and eliminate preapoptotic tumor cells [153, 154]. Recent research has revealed that certain chemotherapeutic agents and oncolytic viruses (OVs) induce ICD by releasing immunomodulatory molecules that activate immune cells, leading to a robust adaptive immune response against cancer cells.
Various cellular processes, such as components associated with the endoplasmic reticulum (ER) stress, DNA damage response, and apoptosis pathways, contribute to the immunogenicity of tumor cells. These processes trigger the release of danger signals and enhance immune activation, crucial for activating effective antitumor immune responses. Despite the historical belief that apoptotic cell death was immune-tolerant, it’s now understood that apoptotic cells produce molecules which are known as damage-associated molecular patterns (DAMPs), which possess potential anticancer properties by stimulating immune recognition.
It is crucial to comprehend the process of ICD in relation, to cancer immunotherapy. Different inducers of ICD have been categorized into type I and II based on their mechanisms of inducing apoptotic cell death and ER stress. Type I inducers include chemotherapeutic agents, specific antibodies and inhibitors while type II inducers consist of photodynamic treatments and certain viruses. These inducers hold promise in modulating tumor cell responses and triggering immune reactions against cancer, paving the way for Oxaliplatin is a chemotherapy drug that falls under the platinum compounds class and is used to treat variety of cancers, including CRC. Its unique mechanism of action includes the induction of ICD, which is a sort of PD that activates the immune system. This process may be beneficial in the treatment of cancer as it helps to eliminate cancer cells effectively. Several innovative therapeutic approaches have been developed using oxaliplatin in cancer treatment [155].
A recent study has shown that oxaliplatin triggers a process called ICD in CRC cells. This process involves the exposure of calreticulin (CRT), a protein involved in calcium regulation and ER stress response, to the extracellular environment. CRT then moves to the surface of cancer cells, initiating a signal cascade to DCs, immune cells tasked with capturing and presenting antigens to T cells. Additionally, oxaliplatin leads to the liberation of high-mobility group box 1 (HMGB1), a protein that binds to TLRs on DCs and macrophages (immune cells that phagocytose and process antigens). These events enhance DCs and macrophages’ ability to present antigens, thereby stimulating T cell activation and cytotoxicity against cancer cells [156].
The study found that oxaliplatin-induced ICD was more effective than cisplatin-induced ICD in CRC cells. Both drugs were equally efficient in releasing HMGB1. However, only oxaliplatin induced pre-apoptotic CRT exposure while cisplatin did not. Research also demonstrated that CRT exposure by oxaliplatin-treated CRC cells induced an antitumor immune response in vivo, and this response was reduced by knocking down CRT or HMGB1 expression or function. Moreover, they found that patients with advanced CRC who received oxaliplatin-based chemotherapy had a higher frequency of TLR4 loss-of-function allele than the general population, which was associated with reduced progression-free survival [156].
Vaccination is a cornerstone in disease prevention, with two main types: preventive and therapeutic. Preventive vaccines work by generating specific antibodies and long-term memory B cells to stop the spread of infections. Therapeutic vaccines, on the other hand, aim to target and eliminate the underlying cause of a disease, such as virally infected cells or cancer cells, to treat the condition. Their effectiveness often hinges on antigen-specific CD8+ T cells, which produce CTLs responsible for identifying and destroying affected cells [157].
Various strategies exist in the domain of anticancer vaccination as depicted in Fig. 3. These strategies aim to leverage the immune system’s capability to identify and eliminate malignant cells while promoting long-term immunity [48, 125, 158]. They include:
• Whole Cell or Tumor Lysate Vaccines: These vaccines use irradiated
tumor cell lines combined with immunostimulatory cytokines. While showing
promise, their efficacy can vary. Various cytokines such as GM-CSF,
IFN- • DNA-Based Vaccines: These vaccines use plasmid DNA to induce
antigen-specific cellular and humoral immunity. They have the advantage of
delivering multiple antigens in a single immunization, activating various forms
of immunity [161]. Neoepitope-based cancer vaccines show promise in igniting
tumor-specific immune responses but face challenges due to cost and time
constraints. Research using DNA-based neoepitope vaccines demonstrated protection
against colon tumor-26 (CT26) tumors and a robust CD4+ and CD8+ T-cell
response targeting mutated epitopes. Administering multiple neoepitopes in a
single plasmid proved more effective than subgroup plasmids. While therapeutic
DNA vaccination post-tumor inoculation didn’t show significant effects, combining
anti-PD-1 ( • Peptide-Based Vaccines: These vaccines utilize peptides derived from
specific antigens presented by MHC molecules on cell surfaces. They are easy to
produce, administer, and monitor but they are limited to specific HLA alleles.
The first successful clinical response to peptide-based immunotherapy utilized
peptides obtained from the melanoma-associated antigen (MAGE-3), showcasing the
potential for tumor regression with this approach. Peptide-based vaccines offer
various advantages, including easy and cost-effSSective production in clinical
settings, simple patient administration, non-toxic nature, and the ability to
monitor antigen-specific anti-tumor immune responses. However, a significant
limitation is that peptides are specific to certain HLA alleles, narrowing the
scope of effectiveness. Ideal candidates for peptide-based anticancer vaccines
are those obtained from TAAs expressed solely on tumor cells (like HER2, Mucin 1)
able to induce a cytotoxic T cell response upon vaccination. Another concern is
“tumor escape”, wherein tumor cells can alter antigens or reduce the production
of HLA molecules and immunogenic antigens, evading immune detection (cancer
immunoediting) [163]. • Protein-Based Vaccines: These vaccines employ whole TAAs in the form of
proteins, aiming to be taken in by tissue resident DCs for immune presentation.
Adjuvants are often used to enhance immunogenicity. Such proteins are expected to
be collected by tissue-resident DC after injection, resulting in their
presentation within HLA class II and potentially class I molecules. To enhance
the immunogenicity of antigen peptide and protein-based vaccines, they are often
combined with adjuvants like incomplete Freund’s adjuvant (IFA), BCG (Bacillus
Calmette-Guérin), tetanus toxoid peptide epitopes, diphtheria toxoid, IL-12,
and GM-CSF. Additionally, they may be loaded onto DCs generated ex vivo
to boost their efficacy in eliciting immune responses [163, 164, 165]. • Heat Shock Protein (HSP) Vaccines: Heat shock proteins (HSPs) serve as
intracellular proteins that act as peptide chaperones, including examples like
gp96, HSP70, calreticulin, and HSP110. After being released from a cell, APCs can
collect these proteins and subsequently display HSP-associated peptides through
HLA class I molecules. The presence of extracellular HSPs triggers DC maturation
by providing an activating signal to these cells. HSPs can be genetically
modified to transport specific TAAs like the E7 protein from the MAGE or HPV
antigen. Alternatively, they can be isolated from a patient’s tumor specimens and
re-injected to create anticancer vaccines [166, 167]. • Viral Vector Vaccines: Several viruses, engineered to express tumor
antigens, can trigger an antigen-specific immune response. They often induce
strong immunogenicity, but the development of neutralizing antibodies and side
effects limit their use. Various viruses, such as attenuated
replication-defective poxviruses (like avipox, canarypox, and fowlpox, virus),
herpes virus, adenovirus, and Venezuelan equine encephalitis virus, can be
modified to express specific tumor antigens, triggering an immune response
targeting those antigens. Compared to other vaccination methods, using viruses
tends to generate robust immunogenicity, resulting in a significantly amplified
immune response to the antigen encoded. However, the major limitations hindering
the widespread use of viral vectors in anticancer vaccinations include the
formation of neutralizing antibodies in individuals encountering a specific virus
for the first time after vaccination and the substantial side effects associated
with virus administration [35, 36]. • Dendritic Cell -Based Vaccines: DCs, as potent APCs, bridge innate and
adaptive immunity. Vaccines using protein-pulsed, peptide-pulsed, or viral-vector
infected DCs have shown promise in several tumor types. Notably, the first
FDA-approved autologous cell vaccine, Sipuleucel-T, specifically targets males
with metastatic prostate cancer. This vaccine consists of APCs derived from
PBMCs, treated with prostatic acid phosphatase (PAP) linked to GS-CSF [158].
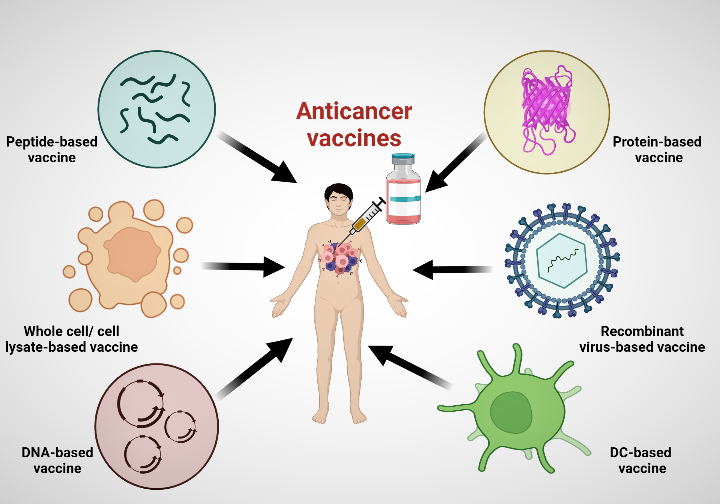 Fig. 3.
Fig. 3.
Anticancer vaccine strategies.
Despite the potential, challenges exist, such as tumor escape mechanisms, limited antigen specificity, and potential side effects associated with certain vaccine types. Ongoing research aims to overcome these hurdles, striving to develop effective and safe anticancer vaccines to improve patient outcomes.
Among the most promising realms in contemporary cancer therapy involves monoclonal antibodies (mAbs), specialized in targeting specific proteins crucial for tumor cell proliferation [168]. Belonging to the IgG class, these biological macromolecules form a burgeoning pharmaceutical pipeline and stand as a pivotal tool in cancer immunotherapy. Engineered replicas of immune system proteins, mAbs aid in eradicating cancer cells by binding specifically to surface antigens on these cells. They trigger immune responses like complement-dependent cytotoxicity (CDC), antigen-dependent cellular cytotoxicity (ADCC), and facilitate antigen cross-presentation. Moreover, they target immunomodulatory receptors such as PD-L1 and CTLA-4, thereby obstructing signal transduction via growth factor receptors (like epidermal growth factor (EGFR) family members), leading to tumor cell elimination [169, 170, 171]. However, for mAbs to be effective, they must overcome obstacles to reach target cell antigens. Intravenous (IV) delivery faces challenges due to varied antigen expression on tumor cells, evasion of the host immune system, and traversal of physical barriers like vascular endothelium, high interstitial pressure, stromal barriers, and epithelial barriers within solid tumors [172]. Monoclonal antibodies for cancer treatment can be classified into two types: naked antibodies, which aren’t combined with any drug, and conjugated monoclonal antibodies, acting as carriers for chemotherapeutic drugs, radioactive particles, or toxins [169].
Rituximab is a monoclonal antibody targeting CD20 on immune cells. Treats lymphomas, leukemias, arthritis, and autoimmune diseases by eliminating specific cells or modulating immune responses [173]. In a study involving follicular lymphoma patients responding to rituximab treatment, two groups were compared: one receiving maintenance rituximab every 3 months and the other rituximab only upon disease progression. Results showed similar disease control among the groups over a 4.5-year median follow-up, with comparable treatment failure rates at the 3-year mark (61% retreatment vs. 64% maintenance). Health-related quality of life remained consistent. The patients in maintenance group received more rituximab doses but experienced infrequent serious side effects (94% overall survival in both groups). Limitations included differences in induction therapy and the study’s design favouring responsive patients for retreatment. However, the retreatment strategy showed promise in avoiding further therapy for responsive patients after rituximab induction [174].
Another study evaluated first-line treatment using monotherapy with trastuzumab in 114 women with HER2-overexpressing metastatic breast cancer. Patients received varying doses of trastuzumab and showed an overall 26% objective response rate, with higher rates among those with HER2 3+ overexpression compared to HER2 2+ expression. Clinical benefit rates were notably higher in patients with HER2 3+ overexpression. A substantial portion of patients with positive responses or clinical benefit did not experience disease progression even after 12 months. Frequently observed treatment-related adverse events included chills, fever, asthenia, nausea, and pain. Cardiac dysfunction manifested in 2% of patients with a cardiac disease history, and subsequent to trastuzumab discontinuation, further intervention was not required. The study demonstrated that trastuzumab as a monotherapy, exhibits efficacy and favorable tolerability as a first-line treatment for metastatic breast cancer, particularly in cases of HER2 3+ overexpression as determined by immunohistochemistry or gene amplification determined by fluorescence in situ hybridization analysis [175].
Bi-specific antibodies, such as bi-specific T cell engagers (BiTEs), have
appeared as a promising avenue in cancer treatment due to their unique ability to
simultaneously bind to two different proteins, guiding the immune system to
target and attack tumors. By combining two distinct monoclonal antibodies, these
constructs facilitate the connection between cancer cells and T cells, directing
T cells to destroy cancerous cells via the CD3 and cancer antigen interaction.
Dual-affinity re-targeting (DART) represents a bi-specific antibody molecule
composed of variable heavy and light chain domains linked together, showcasing
substantial potential in preclinical and clinical studies for cancer treatment
[176, 177, 178]. Blinatumomab, the sole FDA-approved BiTE, has demonstrated
significant clinical responses in B-lineage acute lymphoblastic leukemia by
binding to CD19 on tumor cells and activating T cells via CD3. In a phase 3 trial
for relapsed/refractory acute lymphoblastic leukemia (ALL), blinatumomab, an
immunotherapy, displayed improved overall survival (OS) when compared to
chemotherapy after initial treatment cycles. The study assessed additional
blinatumomab cycles given as consolidation and maintenance therapy to patients in
remission post-induction. Among those achieving remission, 32% received
consolidation (cycles 3-5) and 13% maintenance (cycles
Bintrafusp alfa (M7824) is another investigated BiTE targeting both
TGF-
Oncolytic virotherapy (OV) is an innovative cancer treatment that employs viruses to target and destroy cancer cells while leaving healthy cells. This therapy employs modified viruses to infect and replicate specifically within tumor cells, ultimately causing their destruction. These viruses are engineered to selectively replicate within cancer cells, leading to their lysis or death, and triggering an immune response that helps in further eradicating the tumor [182].
The concept behind OV is based on the potential of certain viruses to preferentially infect and replicate in cancerous tissues due to specific mutations or alterations present only in tumor cells. Once the virus infects the cancer cell, it undergoes replication, resulting in the tumor cells destruction. This process generates antigens capable of stimulating the immune system, activating immune cells to identify and target any remaining cancer cells throughout the body. Several viruses, including adenoviruses, herpes simplex viruses (HSV), reoviruses, and vaccinia viruses, have been studied and engineered for oncolytic purposes. Advances in genetic engineering and molecular biology have enabled scientists to modify these viruses to enhance their specificity for cancer cells and to equip them with additional therapeutic genes, making them more effective in targeting tumors [183, 184, 185].
The clinical application of OV has shown promise in various types of cancers. Clinical trials investigating the safety and efficacy of OVs, both as standalone treatments and in combination with other therapies like chemotherapy or immunotherapy, have demonstrated encouraging results. Notably, the U.S. Food and Drug Administration (FDA) has approved OV for certain types of cancers, marking a significant advancement in the field of cancer treatment [186].
While OV holds immense potential, challenges remain, such as optimizing viral delivery to the tumor site, preventing premature immune clearance of the virus, and minimizing potential side effects. Additional research is being conducted to refine viral engineering, improve delivery methods, and identify optimal combinations with other cancer treatments to enhance its effectiveness [187].
Preclinical studies have shown the potential of OV, particularly with genetically engineered HSV-1 G207, in treating pediatric brain tumors. G207 is programmed to replicate only within tumor cells, leaving normal brain tissue alone. A case study evaluated the use of HSV-1 G207 in pediatric high-grade glioma, a condition known for poor survival rates and limited treatment options. The trial involved twelve children and adolescents with progressive or recurrent supratentorial brain tumors. Administered intratumorally, G207 showed an acceptable safety profile, with no severe adverse events attributed to treatment. Notably, G207 treatment led to neuropathological, radiographic, or clinical responses in most patients. Remarkably, the median overall survival (mOS) reached 12.2 months, with some patients surviving 18 months post-treatment. Equally significant was G207’s impact on TILs, significantly increasing their presence, transforming “cold” tumors into immunologically active ones. This case study suggests the potential of HSV-1 G207 in shifting the TME and improving outcomes in pediatric high-grade glioma (ClinicalTrials.gov number, NCT02457845) [188].
Talimogene laherparepvec (T-VEC) has gained approval for treating patients with recurrent melanoma. In a recent study, researchers explored the efficacy of T-VEC therapy in a cohort of 13 patients with primary cutaneous B-cell lymphoma (pCBCL). The findings were promising, with 11 patients exhibiting a positive response to T-VEC, including six complete responses. T-VEC showed notable efficacy in injected lesions, mirroring responses observed in melanoma. The study indicated that immune-mediated rejection might drive distant antitumor activity, as the virus was solely detected in injected lesions. Gene expression studies revealed rapid changes post-T-VEC treatment, indicating an increase in genes related to immune response. These results suggest T-VEC’s potential effectiveness in pCBCL, emphasizing the need for further research to define responses in non-injected lesions and understand oncolytic virus therapy better in cancer treatment [189].
In summary, OV represents a promising avenue in cancer treatment, leveraging viruses to selectively target and destroy cancer cells, while also stimulating the immune system for a comprehensive anti-tumor response. Continued research and clinical trials aim to further develop and refine this innovative therapeutic approach for improving outcomes in cancer patients.
Microenvironment-responsive nanoplatforms are a class of nanomaterials that can be designed to respond to specific signals in the TME, such as pH, temperature, and enzymatic activity. By responding to these signals, the nanoplatforms can stimulate the release therapeutic agents at the tumor site, improving targeted drug delivery and efficacy. Microenvironment-responsive nanoplatforms can be loaded with various immune modulators, immunomodulatory drugs, and chemotherapy drugs to improve the immune response against cancer cells [190]. By exploiting the unique features of the tumor environment, they hold great potential for developing more effective cancer immunotherapies. This article section describes the various endogenous and exogenous stimuli-responsive nanoplatforms explored for cancer immunotherapy.
Endogenous stimuli-responsive platforms are developed to respond the endogenous stimuli within the TME, such as hypoxia, pH, enzyme, or oxidative stress, and release therapeutic agents at the tumor site.
Solid tumors extracellular environments are known to be acidic (pH 6.5–7.0) than normal tissues (pH 7.4). This difference in pH can act as an intrinsic trigger for the release of therapeutic molecules at tumor locations, reducing drug leakage in the bloodstream or normal tissues. The pH-responsive behaviour of these nanomaterials is typically achieved by incorporating pH-sensitive chemical bonds/functional groups (hydrazone, oxime, imine, ether, and ortho ester and polyacetal/ketone) [190] or pH-responsive polymers into the structure of the nanomaterials. In cancer immunotherapy, pH-responsive nanomaterials have been used to enhance immune modulator delivery, such as adjuvants, antigens, and cytokines, to the TME. These immune modulators can activate immune cells, such as DCs and T cells, to mount an efficacious antitumor immune response. For instance, Yao et al. (2022) [191] developed CaCO3 mineralised single-atom Fe nanoparticles (SAF NPs), as a theranostic, and a pH-responsive nanosystem. The SAF NP’s active site can cause in situ production of toxic OH in TME that induces apoptosis, and its porous structure may be utilized to load and release therapeutic molecules like DOX to improve chemotherapy. The in-situ mineralization of CaCO3 and A549 membrane helped in preventing DOX leakage from NPs in blood and achieve specific targeting. Furthermore, excess calcium causes mitochondria malfunction, cytoskeleton breakdown, and stress (by oxidation), leading to calcium ions interference treatment. The developed multi-synergetic nanoplatform, could have promising application in tumor treatment [191].
Enzyme-responsive platforms are intended to react to specific enzymes present in the TME, such as matrix metalloproteinases (MMPs), hyaluronidase and cathepsins. By detecting and responding to these enzymes, the platforms can release therapeutic agents at the tumor site, leading to improved targeted drug delivery and efficacy. MMPs and cathepsins are frequently upregulated in the TME and can be exploited to trigger therapeutic agent release from nanoplatforms [192]. Hyaluronidase, on either side, can degrade the ECM and enhance drug penetration into the tumor [193]. Other enzymes that have been studied for use in enzyme-responsive platforms include proteases, esterases, and oxidases. The choice of enzyme will be determined by the specific characteristics of the TME, and the therapeutic agent being delivered.
HA, for instance, is a commonly used polysaccharide to modify the surface of NPs to achieve enzyme responsiveness. It has been shown that HA has a potent and precise ability to target CD44, a transmembrane glycoprotein that is elevated expression on a variety of tumor cells. Additionally, because HA is made up of enzyme-degradable disaccharide units, it makes a suitable material for creating NPs with a hyaluronidase-responsive platform. In this context, Zhang et al. (2016) [194] fabricated biotin-modified HA-coated mesoporous silica nanoparticles (MSNs) to develop hyaluronidase enzyme responsive nanoplatform. It was proposed that after NPs were taken up by target cells, biotin (in the cytoplasm) and HAase (in the ECM) assisted in opening the pores for regulated intracellular DOX release. The in vitro analysis revealed that the coexistence of biotin and HAase greatly facilitated the DOX release, leading to increased apoptosis of cancer cells. The in vivo results demonstrated superior antitumor effects of MSN-HA/DOX compared to the free drug. Similarly, another team [195] used HA-coated MSN for the codelivery of DOX and siRNA in an enzyme responsive manner. To enhance breast cancer targeting specificity, the NPs underwent additional functionalized with PEGA-pVEC (cell-penetrating peptide). The resulting NPs were up taken by CD44 receptor mediated endocytosis and accumulated selectively in the tumor vasculature as directed by the cell penetrating peptide (CPP). HA also acted as a protective coating to prevent the leaching of the cargo until acted upon by hyaluronidase. Once HA layer is degraded the gene responsible for drug resistance was silenced by siRNA and facilitated the apoptotic effect of DOX.
Hypoxia reduces oxygen availability, increasing patient resistance to therapy and favouring tumor development. Massive tumor cell growth separates cells from the vasculature, resulting in a lack of blood that delivers oxygen and nutrients to the surrounding environment. Hypoxic circumstances cause a molecular reaction in the cells, which involves the initiation of the hypoxia inducible factor (HIF). This is an essential transcription factor that regulates many genes that enhance tumor angiogenesis, glycolysis, other tumor survival responses, metastasis, and invasion [196]. Overexpression of HIF-1 and HIF-2 is usually linked to metastasis and poor clinical outcomes. Combining HIF-inhibitors with anti-angiogenic medications may reduce the pro-metastatic effects of antiangiogenetic-induced hypoxia while also improving the efficacy of existing antiangiogenic therapy [197]. Due to toxic energy metabolites, deprivation, acidification, and other suppressive signals, tumors and suppressive stromal thrive in these hypoxic, nutrient-depleted situations, whereas antitumor immunity fails. Reversing cancer hypoxia can increase tumor-infiltrating T cells’ survival and effector activity and re-sensitize tumors to immunotherapy [198]. Oxygen delivering nanoparticles and hypoxia-responsive nanoparticles are two complementary approaches that can be combined to improve immunotherapy efficacy in solid tumors. Oxygen delivering nanoparticles, such as perfluorocarbon-based nanocarriers, can be used to deliver oxygen to hypoxic regions within the TME, thereby reducing the hypoxic conditions and improving the efficacy of immunotherapy. Hypoxia-responsive nanoparticles, on the other hand, can selectively release their payload in response to the hypoxic conditions within the TME, thereby enhancing the delivery and activity of immune modulators or chemotherapeutic agents [199]. By combining these two approaches, oxygen delivering nanoparticles can improve the delivery of hypoxia-responsive nanoparticles and enhance their therapeutic efficacy.
For instance, a report by Zhang et al. (2022) [200] describes the development of NIR responsive nanoplatform that release oxygen on-demand (O2-PPSiI). Here, Poly(lactic-co-glycolic acid) (PLGA) served as core to co-load paclitaxel and perfluorooctyl bromide. Ultrathin-walled silica shell was used to prevent the leach of O2. Indocyanine green (ICG) served the role of photothermal converter to aid release of O2 on demand. Gd3+ complexes were used to monitor the biodistribution of the nanosystem and arginine–glycine–aspartic acid (RGD) peptide and urokinase plasminogen activator were used to impart the receptor targeting ability. The developed nanosystem could precisely target the tumors and synergistically provide PTT, chemotherapy, hypoxia mitigation and thus increased the therapeutic efficacy of the chemotherapy in suppressing the tumor metastasis and invasion. Besides, due to the Gd3+ complexes in the nanosystem, the biodistribution of the NPs could be monitored via magnetic resonance imaging (MRI) and thus quantify the NPs reaching the tumor (Fig. 4, Ref. [200]). TAMs are a type of immune cells that infiltrate the TME and can have a significant impact on the response to immunotherapy. TAMs can have both protumor and antitumor effects depending on their polarization status. In general, TAMs are polarized towards an M2-like phenotype, which is associated with protumor effects such as immune suppression, angiogenesis, and tumor growth and metastasis.
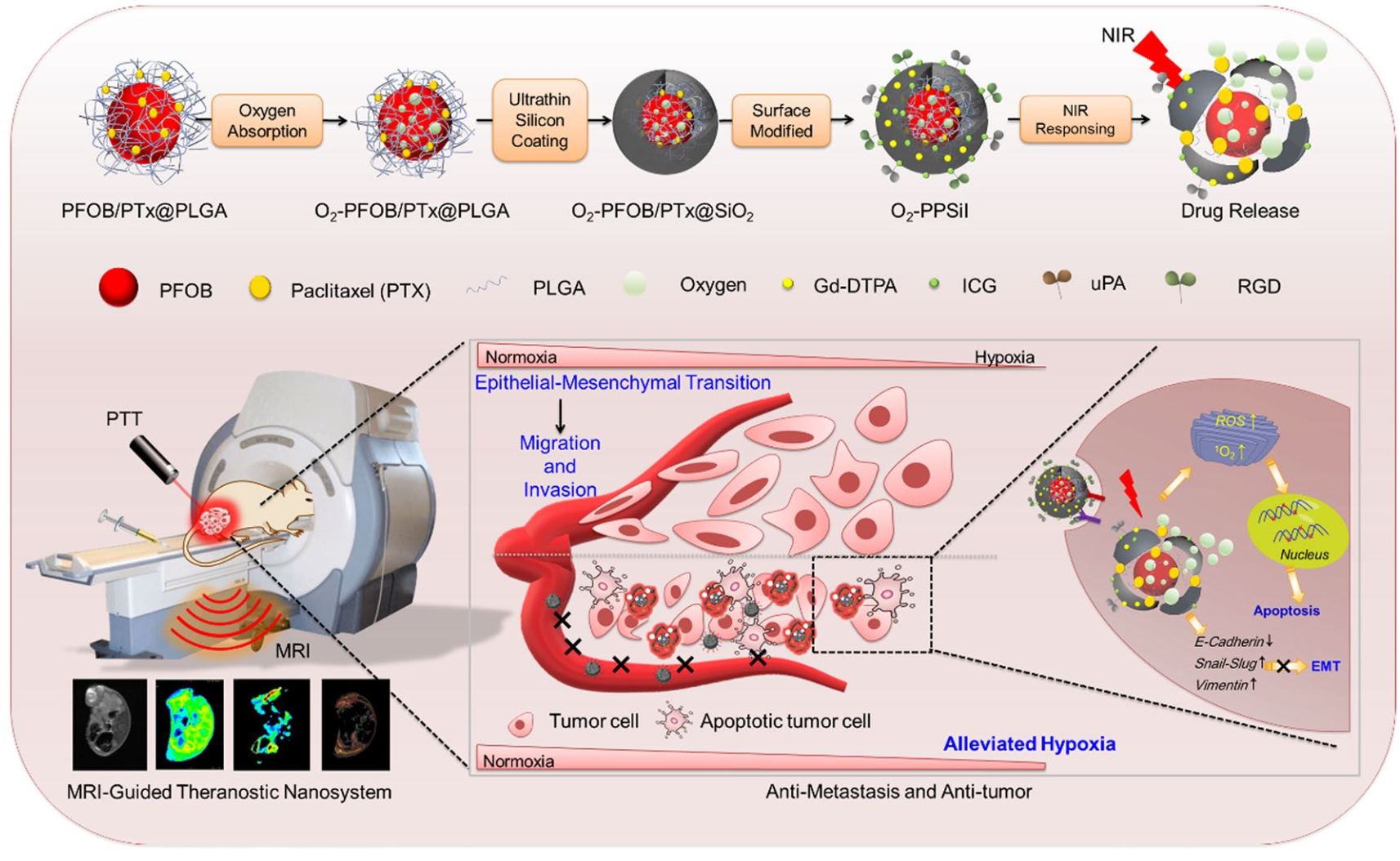 Fig. 4.
Fig. 4.
The rational design of NIR-responsive on-demand drug releasing nanomedicine system to relieve tumor hypoxia, enhance chemotherapy and inhibit tumor metastasis. [Adapted from [200], an article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution, and reproduction in any medium or format]. PFOB, perfluorooctyl bromide; PTx, paclitaxel; PLGA, poly(lactic-co-glycolic acid); SiO2, silicon dioxide; O2-PPSil, on-demand oxygen releasing nanoplatform; Gd-DTPA, gadolinium–diethylenetriamine pentaacetic acid; ICG, indocyanine green; uPA, urokinase plasminogen activator; RGD, arginine–glycine–aspartic acid; PTT, photothermal therapy.
Aiming to target the TAMs in hypoxia, another research team developed polyethylene glycol-azobenzene-poly(l-lysine) PEG-azo-PLL nanocomplex [201]. The in vivo results showed the boost in infiltration of CD8+ T cell and considerable decrease in the M2-like TAMs leading to conversion of immunosuppressive TME. The nanosystem could elicit antitumor effect in the B16F10 tumor bearing mice and prolonged the survival time of animal.
Redox-responsive nanomaterials have appeared as a promising class of drug delivery systems for cancer immunotherapy. These nanomaterials are engineered to release therapeutic agents in response to the changes in the redox state of the TME, which is characterized by high levels of reactive oxygen species (ROS) and a higher reducing environment compared to normal tissues. Their redox-responsiveness is typically achieved by incorporating redox-sensitive chemical bonds or functional groups, (such as disulphide bonds, thioether bonds, diselenide bonds, thiol groups, thioether bonds and thioketal linkages) [202], into the structure of the nanomaterials [203]. Under the reducing conditions of the TME, these bonds can be cleaved, allowing the therapeutic agents to be released. In cancer immunotherapy, redox-responsive nanomaterials have been used to enhance immune modulator delivery, such as TLR agonists and cytokines, to the TME. These immune modulators can activate immune cells, such as T cells and DCs, to locate an effective antitumor immune response. Moreover, redox-responsive nanomaterials can also be used to deliver immunomodulatory drugs, such as ICIs, to the TME. ICIs can prevent cancer cells from bypassing the immune system, resulting in an induction of antitumor immune responses.
In this context, one of the researches [204] focused on altering the hyperbranched PAA (HPAA) containing di-sulphide bond in developing fluorinated HPAA to employ as a vaccine delivery system in the treatment of antitumor immunotherapy. The nanocomposite was also modified with ovalbumin (OVA) to enhance its uptake. The redox responsiveness of the nanocomposite was evaluated using gel permeation chromatography by measuring elution time of glutathione treated and untreated HPAA. The result indicates that HPAA degraded in the presence of glutathione indicating redox responsiveness of the nanocomposite. The in vitro studies performed on the DC2.4 cells showed that internalization of HPAA/OVA was higher than free OVA which could be due to the nanocomposite’s positive charge. Further the flow cytometry data demonstrated that the order of cellular uptake in the DC2.4 cells fluorinated HPAA/OVA better as compared to HPAA/OVA better than free OVA. Further studies like splenocyte proliferation, memory T cell response and immune stimulation effects was greater in the fluorinated HPAA/OVA nanocomposite compared to the other two. In vivo tumor challenge assay performed on mouse thymoma EL4 (E.G7-OVA) cells tumor bearing mice demonstrated that the fluorinated HPAA/OVA nanocomposite not only enhanced the efficacy of immunotherapy but also prolonged the survival of tumor-induced mice (Fig. 5, Ref. [204]). Overall, it was concluded that the strategy of fluorination could be used to improvise the tumor immunotherapy while using polymer-based vectors.
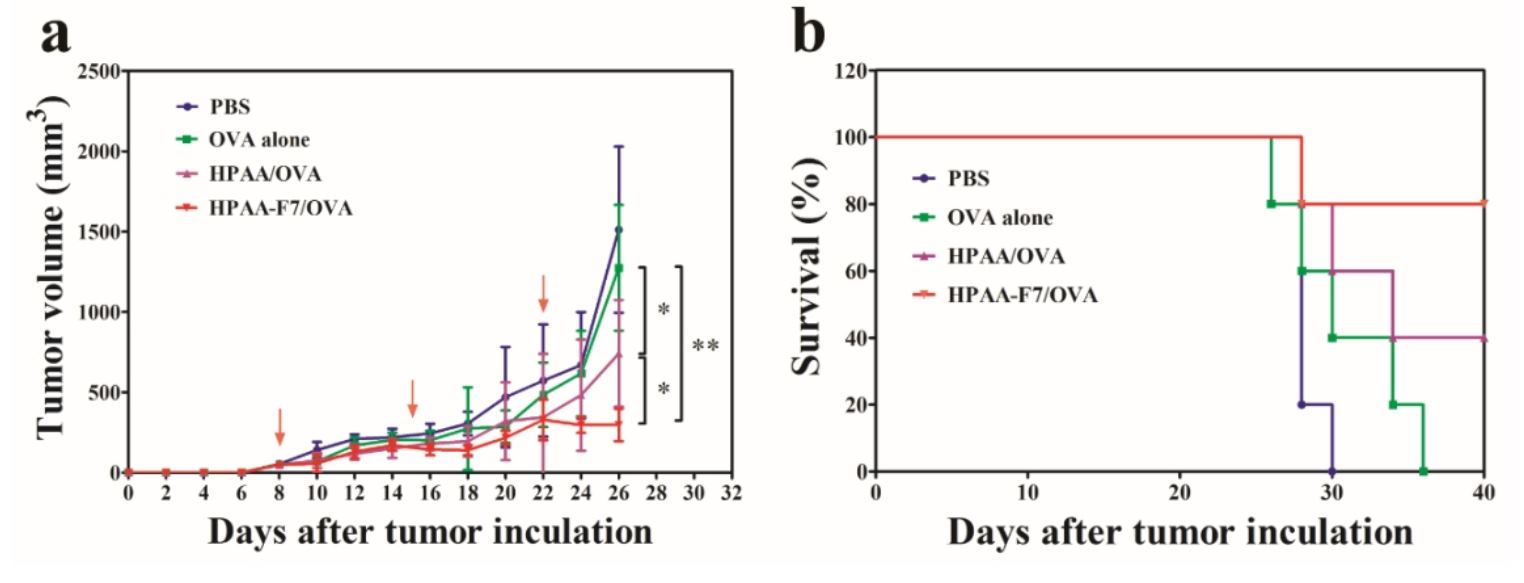 Fig. 5.
Fig. 5.
Antitumor effect induced by the subcutaneous
administration of OVA, HPAA/OVA and HPAAF7/OVA. (a) Tumor volumes and (b)
survival curves. * p
Another team [205] developed redox responsive nanohydrogel for the delivery of OVs which can kill cancer cells. The nanohydrogel was prepared by water-in-oil (W/O) emulsion method and crosslinker disulphide groups of thiolated HA. The redox responsive of the nanohydrogel was evaluated using the presence of different concentration of glutathione. The system stability in the physiological conditions was maintained for 5 days while in the reductive environment the sample degraded in 10 h. The in vitro studies demonstrated oncolytic activity against cancer cell line by inducing cell lysis. These results show the immunotherapeutic efficiency of redox responsive nanoplatforms against cancer.
Tumor immunotherapy strategies are not always tumor precise. Few of these are also found in non-malignant tissues, and the unintentional release of tumor immunotherapeutic agents into the healthy tissues might have catastrophic effects. As a result, controlled delivery of tumor immunotherapeutic drugs into the precise location is crucial for producing effective antitumor immune responses while limiting adverse effects. Stimuli-responsive systems are built to allow for the desired release of loaded chemotherapeutics in a temporally and spatially controlled way [206].
Phototherapy has attained wide attention in current years due to its spatiotemporal addressability, relative clinical efficacy, and minimum invasiveness. UV radiation of 100 to 400 nm, visible light in the range of 400 to 760 nm, and near-infrared (NIR) light of 760 to 1350 nm are all extensively used in tumor photo-immunotherapy. Furthermore, due to biological tissue absorption, the frequently employed UV and visible light possess minimal tissue penetration, limiting conventional phototherapy to superficial cancers and increasing the risk of recurrence and metastasis. NIR-light-sensitive nanoplatforms have been produced to solve the issue of phototherapy’s low light penetration depth [207]. Light is a versatile trigger among the many external stimuli since it is simple to change the place treated and the intensity of the applied treatment. O-nitrobenzyl linkages that are photocleavable have been used extensively for light-sensitive payload release. The presence of reversible transition from cis to trans configuration in albendazole and related derivative groups make them a suitable agent for NIR-mediated release [208].
Li & co-workers (2019) [209] fabricated organic semiconducting pronano-constituent (OSPC) with NIR-photosensitive immunotherapeutic activity for tumor immunotherapy. The developed system consisting of immunostimulant conjugating with a singlet oxygen cleavable linker and semiconducting polymer NP. On irradiation with NIR light, the system produced singlet oxygen as well as heat which induced the phototherapy for the tumor ablation along with the production of TAAS. Furthermore, NIR laser irradiation stimulated the singlet oxygen cleavable linker cleavage and immunostimulant release from the device to maintain the immunosuppressive tumor environment. They chose Navoximod (NLG919) as an immunostimulant due to its indoleamine 2,3-dioxygenase blockage activity. The cell viability studies on 4T1 cells showed that the treated cells had the same viability as that of control groups, which suggested the negligible toxicity of the fabricated system. The in vivo studies on a xenograft mouse tumor model showed a synergistic anticancer immune reaction associated with the immunostimulant release followed by the NIR irradiation. Blood biochemistry analysis, histological tests and body weight monitoring studies confirmed the biosafety of the developed OSPC [209].
In another study by Sato et al. (2018) [210] conjugated an NIR sensitive dye IRdye 700DX with a monoclonal antibody for a specific antigen targeting present on the tumor cell surface. Followed by the administration, the target cell attached with the conjugate was exposed to NIR irradiation. NIR laser irradiation produces a process known as axial ligand release, which results in changes in the IR-dye700DX hydrophilicity, which results in changes in antigen-antibody complex structure. This physical alteration then raises the physical strain inside the plasma membrane, causing an increased transmembrane water flow and fast and extremely selective ICD of the targeted tumor cells [210].
Wang et al. (2014) [211] found that in mice, photothermal destruction of primary tumors using single walled carbon nanotubes (SWCNTs) in conjunction with anti-CTLA-4 antibody treatment can inhibit tumor metastasis. They modified single walled carbon nanotubes (SCWNTs) with PEG via noncovalent approach, where the PEGylated SCWNT exhibited excellent stability in different physiological media. PEGylated SWCNTs with high NIR absorbance may be quickly heated up when exposed to 808-nm NIR light, allowing them to be used as an efficacious photothermal agent. PEGylated SWCNTs exhibited significant Raman scattering resonance, significant preserving of pristine structure of SWCNTs following polymer layering. It was observed that polymer coated SWCNTs could also be used for photothermal tumor killing. The developed polymer layered SWCNTs showed few ideal characteristics of a typical PTT agent such as considerable release of TAAS and enhanced maturation and generation of DCs. In addition, CTLA-4 inhibition used in SCWNT-based photothermal destruction of primary tumors will generate effective T cell infiltration while significantly lowering regulatory T cells at distant tumors [211]. Xu et al. (2021) [212] reported the fabrication of a biomimetic semiconducting polymer nanoengager (SPN) for effective NIR-II based photothermal-mediated immunotherapy. The semiconducting polymer is made up of a greatly NIR-II absorbing core layered with the 4T1 tumor cell membrane and DCs that have been prefabricated to have higher levels of damage-associated molecular patterns and factors stimulating T cell, respectively. The developed design enables for multicellular interactions among tumor cells, DC, and T cells, facilitating the DC activation and T cells for increased antitumor immune response. SPN can work as a nanovaccine after systemic delivery, successfully accumulating in both tumor and lymph nodes to activate the immune system. SPN regulates photothermal activity of NIR-II irradiation of primary tumor to eradicate the tumor and induce ICD of tumor cells to further boost DC maturing and T cell priming. Hence, SPN-mediated NIR-II photothermal-based immunotherapy may produce systemic immune activity in living mice, effectively inhibiting primary and distant cancers, preventing lung as well as liver metastasis, and generating immunological memory [212]. For the first time, Hu & colleagues (2020) [213] fabricated Cu-PPT nanoparticles from p-phenylenediamine, copper acetate, and 5,10,15,20-tetra (4-aminophenyl) porphyrin, through an oxidative coupling process, and the resulting product was employed for synergistic photodynamic therapy (PDT), photothermal therapy (PTT), and chemodynamic treatment. This developed nanosystem with cascade reactions might effectively limit tumor development and trigger immune responses [213].
Ultrasound (US) drug delivery is based on the association of acoustic wave with a biocompatible platform. The release specificity is created by concentrating the waves in the treatment zone utilising physical principles and techniques developed previously for diagnostic as well as therapeutic applications like lithotripsy and High intensity focused ultrasound (HIFU). The major problem in ultrasound-mediated treatment is the development of carrier having physiological activity and ultrasound sensitive. Carriers should have the capacity to transport big payloads and have greater accumulation within the cancer tissue. These difficulties have been solved by pioneering researchers like Tacker and Anderson [214], as well as broad and contemporary multinational partnerships such as sonodrugs [215, 216, 217]. US have recently been proven to offer great effect in tumor immunotherapy. High intensity targeted US elimination of tumors may result in in situ immunity formation as the immune cells are subjected to tumor debris and immune-stimulatory chemicals contained in tumor remnants [218, 219, 220].
Even if less US energy is utilised than is required for ablation, transient
disturbances in cell membranes can occur [221]. Sonoporation is a phenomenon that
has been studied to optimise the delivery of many medicines and other bioactive
molecules. The actual process of cell membrane sonoporation is unknown; however
morphological alterations in cell membranes have been seen. Irradiating a tissue
causes heating, which enhances the dynamic properties of lipid bilayers and
facilitates passive transport [222]. Casey & colleagues (2010) [223] delivered
GM-CSF to solid tumors via direct US-sonoporation. The administration of
plasmids containing the GM-CSF following US showed 55% survival (compared to 0%
without US) and full resistance to recurrent tumor occurrence, showing an
antitumor immune reaction. Transferring splenocytes from the treated animals to
naïve caused a total resistance to tumor challenge (100% survival),
implying that cellular mediation was responsible for the observed immune response
[223]. Other investigations have demonstrated effective plasmid DNA delivery to
prostate tumor cells in vitro [224], in vivo [225], and
IFN-
There are various studies going on the usage of microbubble (MB) and US for gene delivery. Co-injection is the most feasible approach for MB administration of bioactive compounds. MB and the bioactive ingredient are combined in solution before being administered and US administered in vivo. This method has the benefit of allowing both components to be handled totally independently until the moment of injection, and it even allows for two distinct injections of the components. Furthermore, this simplifies treatment adjustment because it is feasible to vary the relative ratio of constituents as well as replace or include one constituent without affecting the other [229]. Greenleaf et al. (1998) [230] utilized microbubble cavitation nuclei and other procedural modifications, acoustically induced transfection was improved roughly 20 times above previously reported levels, putting it on par with other techniques like lipofection in terms of effectiveness. Applications in vivo are now conceivable because to the improved efficiency and further potential improvements like DNA-Albunext complex development [230]. In another study on the use of MB to transport pDNA, SonoVue MBs were used to carry the cytokine IL-27 encoding pDNA to mouse prostate cancers. The MB and IL-27 pDNA were intravenously co-injected, and US was immediately used. All three of the tumor models that were evaluated had a significant slowing of tumor development when this therapy was administered three times with 48-hour breaks between each. Additionally, after therapy, there was a raise in the CD3+CD8+ cell infiltration in the tumor, indicating immune system activation [231].
Several studies on the use of BLs, which are lipid particles encased in gas, have been published. At high pressure, liposome dispersions are mixed with perfluoropropane (PFP) gas, and the sealed vials are sonicated to generate PFP-containing particles with diameters less than 1000 nm (usually 500–700 nm). These particles’ hypothesised structure is gas bubbles encased in a bigger liposome [232, 233]. BLs has been used to transport the immune-stimulating IL-12 to solid tumors, which resulted in considerably reduced tumor development. The impact was CD8+ T lymphocyte dependent; CD8+ T lymphocyte deficient animals had no effect [233]. In another study by Suzuki & co-workers (2009) [234], BLs were used to transport OVA to DCs. DCs were given OVA in conjunction with BLs and US.
Magnetic systems show enhanced spatiotemporal influence over the transportation, release, and dosage of immunomodulatory therapeutic agents in the body, together with decreased off-target effects and enhanced effectiveness for optimising immunotherapies. Several unique techniques of programming immune responses are made possible by magnetic systems, as opposed to substitutes for promoting drug release like light and pH. Usually, a single or many inorganic magnetic substances make up magnetic particles [235]. Since 1996, when magnetic particles were first used clinically as a negative contrast agent for MRI [236], the FDA has authorised the use of specific magnetite (Fe3O4) SPIONs for therapeutic as well as diagnostic functions [237]. Magnetic field causes magnetic nanoparticles to rapidly oscillate, which converts magnetic energy into heat energy, a process known as magnetic hyperthermia (MH) [238]. Since it was first proposed as a treatment in 1957, localised magnetic induction heating of malignant tissues has attracted a lot of interest [239]. The prime advantage of MH is that it can produce required immunomodulation without adding any drugs into that system [240]. Even though hyperthermia therapy elicits few disadvantages, it is commonly used in combination with radiotherapy or chemotherapy [241]. The foremost reason behind hyperthermia not to be used as primary treatment is the lack of information regarding desirable therapeutic parameters for human use [242]. The ultimate mechanism of MH as a stand-alone immunotherapy is based on physical changes generated by local heat rises, which improve immune cell transport and medication penetration into tumors. Hypoxia and immunosuppression in the TME are promoted by decreased blood artery density and blood flow to the tumor [241]. Furthermore, MH inside tumors has been found to improve immune cell recruitment by increasing the expression of vascular adhesion molecules such as ICAM-1 owing to enhanced IL-6 production [243]. Another research team found that iron oxide nanocubes, disrupt the ECM structure present in tumors through MH, which resulted in better medication and nanoparticle penetration [244].
Protecting therapeutic moiety and regulating drug biodistribution via noninvasive stimuli are two core aims of immunotherapy. Thermosensitive nanoplatforms are thus interesting platforms for spatiotemporal drug release control [245]. Research into the combination of these medications with MH has been sparked by the promise of checkpoint inhibitors like anti-PD and anticytotoxic T-lymphocyte-associated protein in treating metastatic malignancies. Despite the fact that checkpoint inhibitors are often less toxic than the majority of chemotherapeutics, they can nevertheless cause pro-inflammatory cytokine storms that have toxic reactions that are dose-limiting [242]. These limitations have forced more study into strategies for remotely controlling the delivery of immunomodulatory medicines [246]. Given the wide variety of medications used in MH, it is possible to apply this strategy to substances other than chemotherapy, including checkpoint inhibitors, antigens, and other vaccine constituents [247].
Combination therapy refers to methods for treating the primary and metastatic
cancer simultaneously by combining MH with more traditional treatments, such as
chemotherapy or immunotherapies. Combination treatment is commonly used to create
the abscopal effect, which is an adaptive immune reaction that can fight against
distant metastatic tumor cells [248]. Several articles that demonstrated better
cancer cell destruction when MH was coupled with TNF-
Even though the major objective of magnetic-based targeting system is better tumor localization, external fields along with implanted magnets can be utilised to enhance the immunotherapeutic efficiency. Various studies have explained novel applications of magnetic targeting platforms to improve the absorption of chemotherapeutics by immune cells, either in conjunction with passive ligand-receptor interactions or by imbuing the cells with magnetic targeting abilities [253, 254]. Grippin et al. (2019) [255] demonstrated that when an external magnetic field was introduced in vitro prior to immunisation, SPIONs housed within RNA-contained liposomes permitted three times greater transfection rate than electroporation. The efficiency improved with the concentration of SPION present inside the liposome, and this approach also resulted in the activation of DC [255].
The PTT is a potential alternative owing to its extreme low invasiveness and higher selectivity. It involves inserting the biomaterials which effectively convert the light energy (generally at near IR wavelengths) to heat inside the tumor tissue and illuminating them to enhance the tumor heating in a lethal manner [256]. As PTT depends on the long-wavelength light it does not harm the non-target tissue and irradiates the target tissue with the lesser energy [257, 258]. According to the clinical and preclinical reports, the hyperthermia in the tumor cells can improve the blood flow and can result in increased perfusion in the cancer tissue at time and temperature dependent manner. This alters the tumor permeability, oxygenation and decrease in the interstitial pressure, as well as resetting the normal physiological pH conditions. These changes could aid in the nanoparticle-based chemotherapy accumulation and distribution in the target tissue. There are proofs that have shown that the increased heat could help trigger the immune response by stimulating the immune cell activation (CD8+ T cells, NK cells and DCs) leading to the release of exosomes from the cancer cells and causing up-regulation in the inflammatory cytokine’s levels and heat shock proteins. Hyperthermia could lead to the induction of tumor cell necrosis or apoptosis releasing the antigens associated with the tumor which are occupied by the antigen Presenting cells thereby activating the immune system and inducing anticancer immune response [259, 260, 261, 262]. The recurrence of tumor after the use of single tumor targeting therapy is very high. Hence the combination of PTT and immunotherapy can lead to the inhibition of the tumor metastasis. One of the reports showed that the systemic delivery of tumor targeting PTT-based nanoagents by IVroute can result in the lower accumulation in the tumors. Hence, Chen et al. (2018) [263] investigated the potency and feasibility of intratumor administration in combination with immunotherapy without causing systemic toxicity by formulating polydopamine-coated Al2O3 nanoparticles with a higher PTT efficiency. These nanoparticles were synthesized by encapsulating Al2O3 nanoparticles with the biodegradable, non-toxic polydopamine demonstrating higher efficacy in PTT. The near IR radiation could potentially eradicate most target cancer cells, consequently inducing the release of TAAs. The combined presence of Al2O3 and cytosine-gunaine (CpG) serves as an adjuvant, eliciting a cell-mediated immune response that effectively eliminates residual cancer cells and diminishes tumor recurrence. The results indicated the usefulness of the combined PTT-immunotherapy for tumor shrinkage [263]. Zhang et al. (2019) [264] developed a gold nanoshell carrier for the photothermal gene release that target HER-2 and an immunologic adjuvant CpG sequence in the gastric cancer cells. This resulted in a multidimensional therapy including the immune, gene and PTT [264]. Chen & co-workers (2016) [265] developed a strategy for eliminating the primary tumors, impeding metastasis and stopping the tumor relapse by combining nanoparticle-based PTT with the immune checkpoint blockade (ICB) immunotherapy (Fig. 6A, Ref. [265]) wherein a photothermal agent ICG, and imiquimod (TLR7 agonist) co-encapsulated by PLGA. These multifunctional nanoparticles encapsulating NIR heaters and TLR agonists can be employed for photothermal tumor ablation thereby generating TAAs, which display vaccine-like responses which can be combined with the CTLA4 checkpoint blockade resulting in the highly efficient cancer immunotherapy (Fig. 6B) [265].
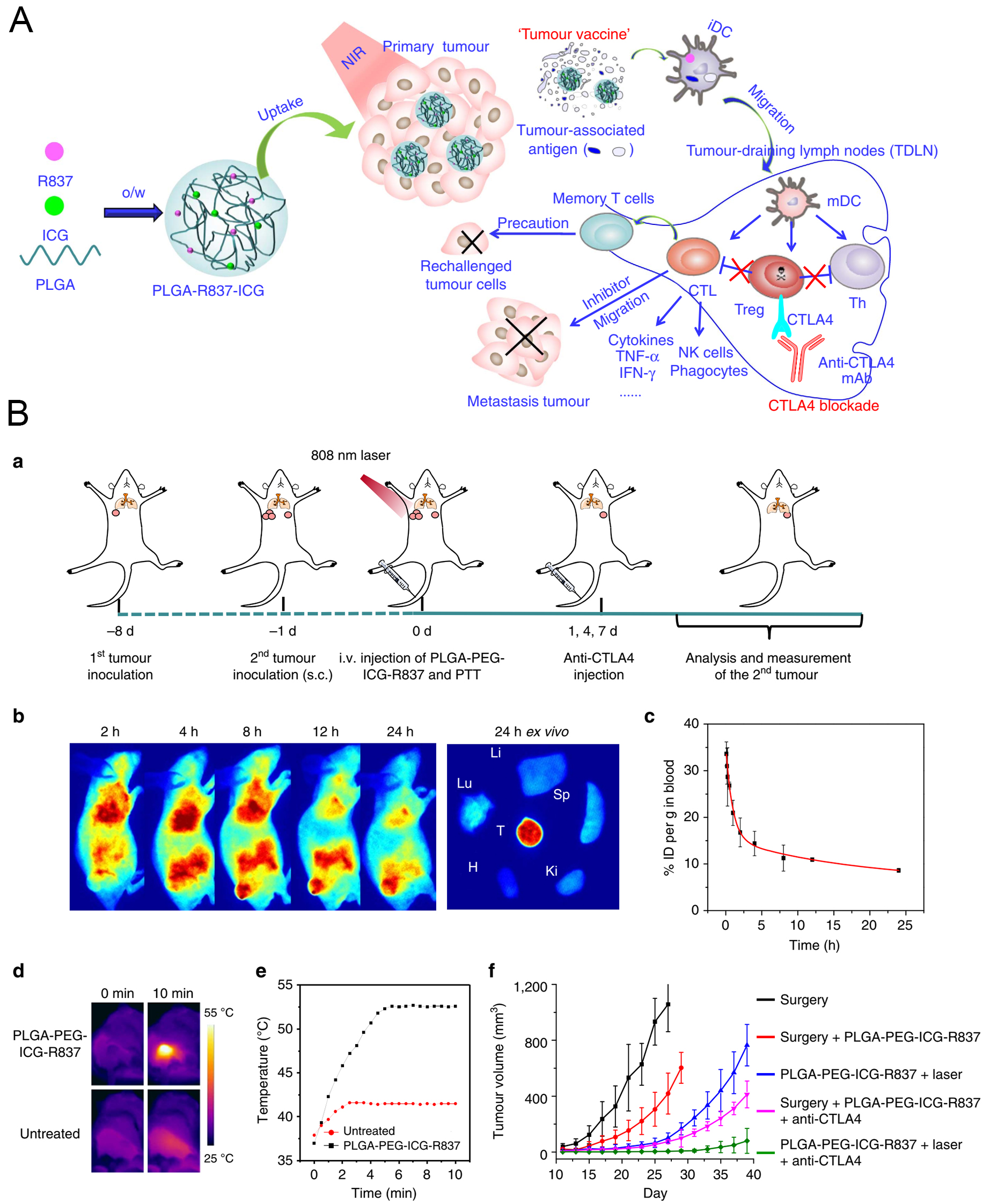 Fig. 6.
Fig. 6.
Synergistic effects of Phototherapy and Immunotherapy. (A) The
mechanism of antitumor immune responses induced by PLGA-ICG-R837-based
photothermal therapy (PTT) in combination with checkpoint-blockade. (B)
PTT-triggered immunotherapy via systemic injection of nanoparticles. (a)
Schematic illustration showing the design of animal experiments. (b) In
vivo fluorescence images of CT26-tumor-bearing mice taken at different time
points post i.v. injection of PLGA-PEG-ICG-R837. The right column shows an
ex vivo fluorescence image of major organs and tumor dissected from the
mouse 24 h post injection. Tu, Li, Sp, Ki, H and Lu stand for tumor, liver,
spleen, kidney, heart and lung, respectively. (c) Blood circulation curve of
PLGA-PEG-ICG-R837 in mice by measuring the fluorescence of indocyanine green
(ICG) in blood at different time points post i.v. injection (three mice per
group). (d) IR thermal images sof CT26-tumor-bearing mice injected with
PLGA-PEG-ICG-R837 or PBS under the 808 nm laser (0.8 Wcm-2) irradiation. (e)
The tumor temperature changes based on IR thermal imaging date in (d). (f) The
growth curves of secondary tumors in different groups of CT26-tumor-bearing mice
after various treatments to eliminate their primary tumors (six mice per group).
Data are presented as the mean
Tu et al. [266], introduced Ru1105, a self-assembled near-infrared light-activated ruthenium (II) metallacycle. Ru1105 synergistically potentiates immunomodulatory responses and reduces adverse effects in deep tumors through NIR-light excitation, ROS generation, selective tumor cell targeting, precision organelle localization and improved tumor penetration/retention capabilities. The structural and photophysical properties of Ru1105 were confirmed via UV-Vis spectroscopy and emission spectroscopy, showing suitable NIR absorption and emission properties for deep-tissue imaging and phototherapy, along with excellent stability and ROS capability. Ru1105 displayed superior cytotoxicity against various cancer cell lines (A549, HeLa, and HepG2), especially when combined with laser irradiation, attributed to ROS generation and photothermal effects. Mechanistic insights revealed Ru1105’s cellular uptake, subcellular localization, and induction of immunogenic cell death, validated through vaccination experiments in mice, activating CD8+ T cells and down-regulating Foxp3+ T cells, enhancing antitumor immune response and leading to significant tumor regression and improved survival in mice [266].
PTT could be used singally for direct eradication of the primary tumor or could be combined with the existing therapies to boost their efficacy. But the PTT-immunotherapy combination could enhance therapy for both primary as well as metastatic tumor cells at the distant sites and enhance anticancer efficacy with shorter duration.
Photodynamic therapy (PDT) is a treatment that uses light energy and a photosensitiser to eliminate cancer cells in a non-invasive manner [267]. Contrarily, immunotherapy improves the body’s immunological response to cancer cells. However, both therapies have their limitations when used separately. Combination therapies have been devised to overcome these drawbacks and increase their effectiveness in preventing cancer spread and recurrence. It has been demonstrated that combining PDT with immunotherapy improves the antitumor immune response by eradicating primary and distant cancers utilising various immunotherapeutic techniques, including immunological adjuvants, immune inhibitors, and ICB [268]. Recently, a treatment approach using a combination of therapies has shown promising results for treating cancers [269]. PDT is used to induce acute inflammation in cancer cells, attracting immune cells to the tumor site. It has the potential to cause immunogenic cell death, which releases signals of danger and pro-inflammatory cytokines as well as antigens specific to cancer. These signals cause the activation of T cells, DCs, and NK, which enhances the identification and elimination of cancer cells. Combining PDT with immunotherapy medications such as ICIs or cancer vaccines can boost the immune response [270]. PDT also changes the TME, encouraging immune cell infiltration and reversing the immunosuppressive properties of the tumor. A two-pronged attack on cancer cells is created when immunotherapy and PDT are combined, improving treatment outcomes, and raising the potential of prolonged remission [271].
A recent study looked at the possibility of immunotherapy as a beneficial treatment option when combined with PDT and chemodynamic therapy (CDT). While PDT and CDT both increase immunogenicity, their efficacy may be constrained by issues including hypoxia, low H2O2 activity, and excessive glutathione in the TME. Cu2+-Pyropheophorbide-a-Cysteine (CuPPaCC), a self-reinforcing compound that enables synergistic PDT/CDT while depleting glutathione, was created by researchers to overcome these constraints. These conjugates formed spherical nanoparticles that were then modified with hyaluronic acid (HA) forming HA modified Cu2+-Pyropheophorbide-a-Cystine conjugate (HSCuPPaCC) to facilitate tumor-specific targeting. They were encased in mesoporous silica and were found to exhibit a dual glutathione-depleting and ROS mechanism that elevated intracellular ROS levels, improved immunogenicity, effectively killed cancer cells, and boosted tumor sensitivity to checkpoint PD-L1 blocking therapy. Treatment with HSCuPPaCC in combination with anti-PD-L1 ICB therapy eliminated the primary tumor and completely suppressed the distant tumor in a CT26 mouse model. This study offers convincing support for the potential of PDT, CDT, and immunotherapy in combination as a novel therapeutic strategy for cancer treatment. The self-reinforcing conjugates showed effective tumor targeting, activation in the TME, and improved antitumor effects, underlining their potential as an effective approach for treating cancer [272].
Photo-mediated immunotherapy, which combines PTT and immunotherapy, has demonstrated potential in the treatment of cancer. However, its efficacy may be hampered by the immunosuppressive conditions found in malignancies. Fucoidan@Al(OH)3-Poly(I:C)/IR-820, a nano-adjuvant that targets tumors, was created by researchers as a solution to this problem. This nano-adjuvant can release tumor antigens and has immunomodulatory properties that assist counteract immunosuppression and boost antitumor immunity. This multifunctional nanoadjuvant has been successfully used to treat breast cancer and prevent metastasis when combined with photothermal, photodynamic, and immunotherapy. This technique provides a potentially effective means of enhancing therapeutic effects and overcoming the difficulties associated with immunosuppressive TMEs in the management of breast cancer. This tumor-targeted nanoadjuvant has considerable potential because it may simultaneously release tumor antigen and modify the immune response [273].
ICB therapy has showed potential to treat advanced and metastatic cases of hepatocellular carcinoma (HCC). However, because of low exposure to tumor antigens and the TME’s strong immunosuppressive effects many HCC patients may not respond. To combat this, the Ce6@PMTKP light-triggered nanoplatform was developed, which combines chemo-photodynamic therapy with ICB therapy to increase its efficacy. The ROS-sensitive paclitaxel polymeric prodrug (PMTKP) for chemotherapy and Ce6 for photodynamic therapy were combined to create the Ce6@PMTKP micelles (Fig. 7A, Ref. [274]), which produced good tumor accumulation and light-triggered drug release (Fig. 7B). Combination therapy utilizing Ce6@PMTKP resulted in a considerable improvement in tumor removal, triggered immunogenic cell death, accelerated DC maturation, and increased the infiltration of CTL, which reduced the immunosuppressive effects of the TME (Fig. 7C).
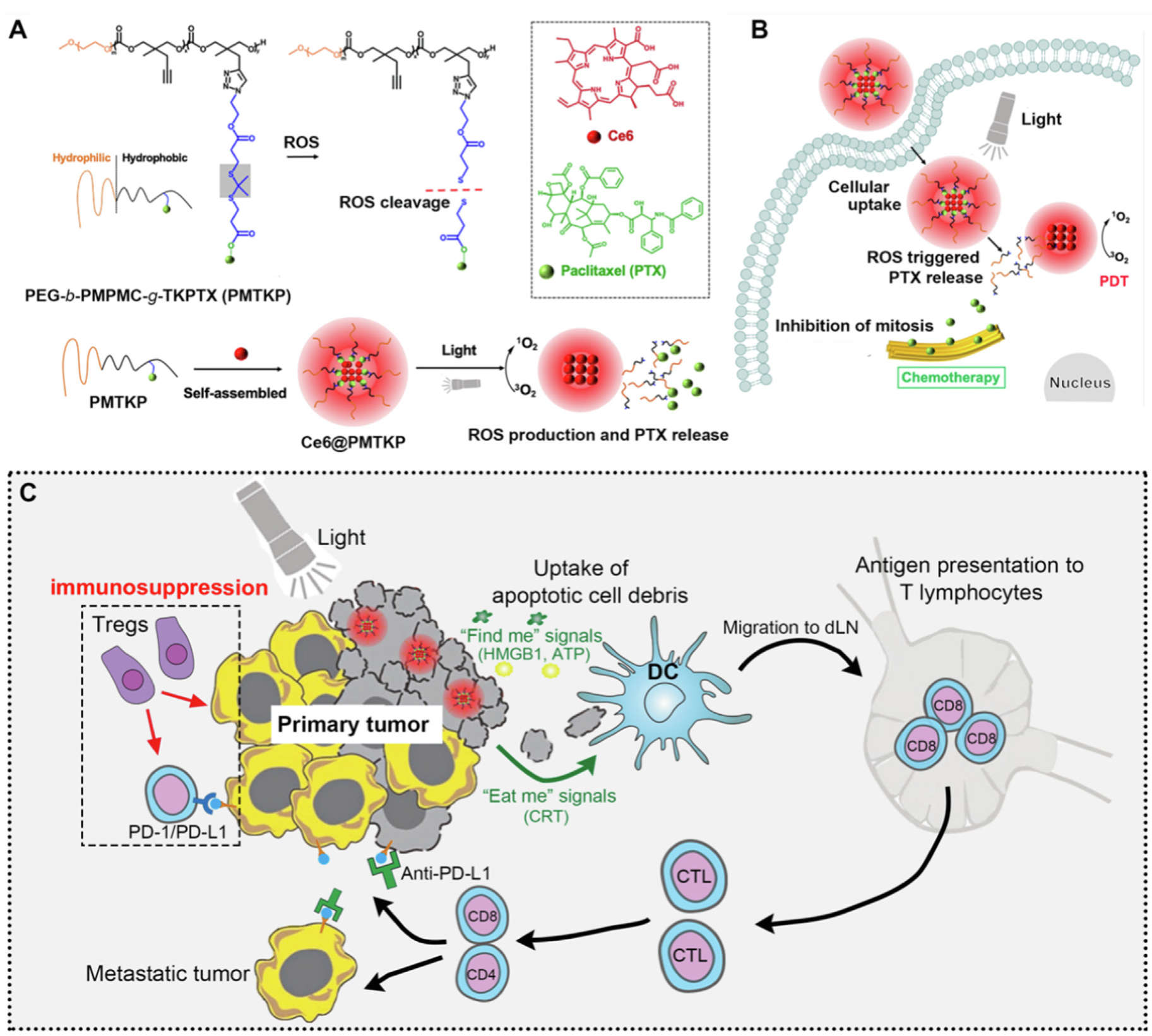 Fig. 7.
Fig. 7.
Light-triggered polymeric prodrug nano-assembly with entrapped photosensitizer for combination chemo-photodynamic therapy to potentiate checkpoint blockade cancer immunotherapy. (A) Ce6@PMTKP micelles were prepared by the self-assembly of the reactive oxygen species (ROS)-cleavable prodrug paclitaxel polymeric prodrug (PMTKP) and encapsulation of Ce6 into the core of micelles by the hydrophobic effect. (B) Under light irradiation, ROS produced by Ce6 could play the role of PDT to destroy the disulfide bond, resulting in the release of PTX for chemotherapy. (C) Synergy of chemo-photodynamic therapy by Ce6@PMTKP micelles resulted in an immunogenic cell death (ICD) effect for TAA release, DCs recruitment, maturation, migration, and cytotoxic T cells activation. Combinatorial Ce6@PMTKP treatment with anti-PD-L1 antibodies induced complete tumor regression of primary tumors and effectively inhibited distant metastatic tumors by enhancing antitumor immune responses. [Reproduced from [274], with kind permission of the copyright holder, © Elsevier]. ROS, reactive oxygen species; Ce6, chlorin e6; PTX, paclitaxel; PDT, photodynamic therapy; PMTKP, PEG-b-PMPMC-g-TKPTX; PD, programmed cell death protein; PD-L, programmed cell death ligand; Treg, regulatory T cells; HMGB1, high mobility group box 1; ATP, adenosine triphosphate; DC, dendritic cell; CD, cluster of differentiation; CRT, calreticulin; CTL, cytotoxic T lymphocytes.
The Ce6@PMTKP micelles completely regressed primary tumors when used in conjunction with anti-PD-L1 immunotherapy. They also successfully reduced distant metastatic tumors by boosting antitumor immune responses. The light-triggered nanoplatform shows promise for enhancing treatment outcomes and overcoming the difficulties associated with HCC, and this study supports the potential of combining chemo-photodynamic therapy with ICB therapy for HCC treatment [274].
William B. Coley revealed for the first time in 19th cent. that bacterial toxins may be utilized as immunotherapeutic agent to manage patients with ortho and soft tissue sarcoma. Cancer immunotherapy is revolutionizing to much greater extend. In 21st century, numerous investigations are carried out in the domain of oncology associated with immunology. Amalgamation of these therapies boosted the cancer treatment to the next level [275].
It basically targets the tumor cells through training the host human immune system such as lymphatic system. Immune therapy is known for its long-term memory for several foreign particles. The major disadvantages are this therapy is limited response rate to checkpoint blockers (CPB). Evidence suggests that only a minority of patients react to immune checkpoint blockers (CPBs) (usually 10–30% responses, conditional on the kind of cancer). Patients with cold tumors, which are characterised by a least number of immune cells or low activation of PD-L1, have a poor response to immune CPBs. In contrast, patients with hot tumors having a substantial number of tumor-passing immune cells and showing the expression of increased amounts of PD-L1 benefited from immune CPBs with durable medical results [276, 277].
Absence of antitumor immune response is a crucial factor that allows malignant cells to proliferate, disperse, and spread. PD-1, also known as CD279 and CD274, PD-L1, B7 homolog 1 (B7-H1) axis have a crucial role in the capacity of malignant cells to elude the immune system among the several immunological checkpoints identified over the last decade [278]. Blocking the link between PD-1/PD-L1 is critical for preventing cancer cells from bypassing anticancer immune responses. Currently, six monoclonal antibodies (mAbs) targeting PD-1 (Pembrolizumab, Nivolumab, Cemiplimab) [279] or PD-L1 (Avelumab, Atezolizumab, Durvalumab) [280] are used to treat certain solid tumors, and more than 15 other mAbs are in clinical development.
In the past decade, several researchers reported that chemotherapeutic agents have excellent antitumor activity, but also mentioned the resistance occurred in studies. The preclinical and human trails also explained the chemoresistance to several receptors that lead to fail of therapy. Likewise, a potent chemotherapeutic agent like doxorubicin, paclitaxel, mercaptopurine, cisplatin, hydroxyurea along with monoclonal antibodies reported for effective treatment in various carcinomas such as lung, brain, breast, and oral cancer and so on. In addition to eliminating cancer cells, they also induce systemic immune activation and immunogenic cell death [281, 282, 283].
Pancreatic ductal adenocarcinoma requires immediate development of innovative life-prolonging treatments (PDAC). Liu & colleagues (2021) [284] found that increased irinotecan administration via a mesoporous silica nanoparticle coated with lipid bilayer, commonly referred as a silicasome. ICD is characterized by the production of calreticulin and the release of HMGB1 in dying Kras-induced pancreatic cancer cells, as established by a vaccination experiment that inhibited Kras-induced pancreatic cancer (KPC) tumors development in the contralateral location. Strong antitumor immunity coexists with the enhanced irinotecan transportation through the silicasome and can be dynamically augmented by anti-PD-1 in the orthotopic paradigm. Beyond the deposition of perforin and granzyme B deposition, immunophenotyping validates the presence of calreticulin, PD-L1, HMGB1 and an autophagy marker. The silicasome induces a stronger chemo-immunotherapy response than the free or liposomal medication Onivyde. Relative to the administration of anti-PD-1 with either free irinotecan or Onivyde, the co-administration of silicasome and anti-PD-1 leads to a substantial improvement in overall survival [284]. Tarantino & colleagues (2021) [285] conducted human trails on 1496 TNBC patients and were observed. Results claimed that patients with high chances of relapse got improved pCR rates with low relapse. Platinum-based drugs such as cisplatin and carboplatin, and antibiotic agent anthracycline combination with anti-PD-L1 immunotherapeutic agents such as atezolizumab, pembrolizumab, durvalumab. Different trials were conducted with all combination of chemo- and immune-therapeutic agents with difference groups of TNBC patients of various stages (I–IV). The study claimed that use of PD-L1 agents significantly improve the risk of relapsing in TNBC patients. PD-L1 was also considered as a biomarker for disease detector in the early stages. The modification in the receptor can be easily useful in detection of stage of cancer [285]. Liu et al. (2021) [286] found that DOX and 5-carboxy-8-hydroxyquinoline (IOX1), a strong immunotherapeutic small drug, may inhibit tumors development in diverse animals. In vitro and in vivo, IOX1 reduces tumors PD-L1. It decreases multidrug resistance in cancer cells and enhances intracellular DOX accumulation, dramatically increasing DOX-induced ICD. IOX1 and DOX enhance T cell infiltration and activation while diminishing tumors immunosuppressive factors. Consequently, liposomal IOX1 and DOX eradicate several mouse cancer models, establishing enduring immunological memory against rechallenging subcutaneous (s.c.) and lung metastatic tumors. IOX1, a widely accessible antibody-free chemo-immunotherapy, treats cancer [286]. Similarly, FOLFOX, Dox and imiquimod, Docetaxel and IDO1 Inhibitor effectively used for the management of Colorectal and breast cancer [287, 288, 289, 290].
Zhu et al. [291], self-assembled the immunomodulator epigallocatechin gallate palmitate (PEGCG) and immunoadjuvant metformin (MET) into tumor-targeted micelles encapsulating doxorubicin (DOX)-loaded PEGCG-MET micelles (PMD) combined with immune checkpoint inhibitors (ICIs) for triple negative breast cancer. Therapy. PMD micelles efficiently delivered drugs with sustained release, targeting tumor cells via laminin receptors, inducing immunogenic cell death, releasing damage-associated molecular pattherns and activating DCs and T cells. Additionally, PMD micelles downregulated PD-L1 expression, enhancing antitumor immune response. In vivo, PMD micelles combined with anti-PD-1 efficiently inhibited tumor growth by activating CD8+ T cells and NK cells while reducing immunosuppressive cells, exhibiting prolonged circulation, tumor targeting and good biocompatibility, offering a promising strategy for TNBC therapy integrating chemotherapy and immunotherapy to enhance treatment efficacy [291]. Yu and colleagues [292] studied the strategy to elicit dual pyroptosis pathways using calcium sulfide-based nanoreservoirs for cancer immunotherapy. Neodymium (Nd3+)-doped calcium sulfide nanoparticles were coated with silica shell and conjugated with glucose oxidase to obtain multifunctional nanoreservoirs (CSSG). These nanoparticles demonstrated stability in biological environments stimulating TME. CSSG induced cell pyroptosis, inhibited tumor cell proliferation, triggered mitochondrial disfunction, elevated oxidative stress, and activated the NOD-like receptor thermal protein domain associated protein 3 (NLRP3) inflammasome pathway, leading to pyroptotic cell death. In vivo, CSSG exhibited potent antitumor effects, activating DCs and tumor-infiltrating T cells, stimulating immunostimulatory cytokine secretion and suppressing distant tumor growth, indicating its potential for inducing systematic antitumor responses and overcoming cancer metastasis [292].
New treatment strategies have been created in recent years for both orphan illnesses and the area of cancer. Moreover, the prognosis for certain advanced neoplastic illnesses has been significantly altered using CPBs, and the development of gene therapies has made it possible to treat conditions that were previously thought to be incurable [293]. ICIs reverse T cell fatigue, which is common in neoplastic illnesses, by blocking inhibitory receptors on the T cell membrane, thereby enhancing the antitumor immune response. Current ICIs target both the CTLA-4 and PD-1 or PD-L1 pathways, which play important roles in controlling autoimmunity. A monoclonal antibody targeting CTLA-4, such as ipilimumab, demonstrated improved overall survival in patients with metastatic melanoma who had undergone prior treatments over the past decade. Anti–PD-1 drugs (nivolumab, cemiplimab, and pembrolizumab) and anti–PD-L1 drugs (atezolizumab, avelumab and durvalumab) were utilized in a variety of solid and hematologic malignancies since 2015s. Although the use of CPBs dramatically increases patient survival in certain cancer types, such as lung cancer and melanoma, it may also produce immune-related adverse events (irAEs) owing to a lack in self-tolerance [294, 295].
The adoptive transfer of T cells modified with receptors has shown remarkable outcomes in the treatment of lymphomas and B-cell leukemias in patients. The result has inspired academic and corporate researchers to build comparable “off-the-shelf” receptors targeting common antigens on epithelial malignancies, the primary cause of cancer mortality. Use of this method to successfully treat the patients with solid tumors is unlikely to be easy. Due to the on-target identification of normal tissues, T cells engineered with receptors have the ability to induce lethal toxicity, and there is a scarcity of tumor-specific antigens that are common in tumor types [296]. Kamran et al. (2017) [297] demonstrated that myeloid mediated immunosuppression has enormous potential for improving the efficacy of gene therapy mediated immunotherapy for GBM. The data demonstrated that MDSCs comprise more than forty percent of the immune cells invading the tumors. These cells express chemicals that are essential for antigen-specific T cell suppression, including IL-4R, arginase, inducible nitric oxide synthase (iNOS), PD-L1, and CD80. Depletion of MDSCs significantly improved the thymidine kinase plus Fms-like tyrosine kinase ligand (TK/Flt3L) gene therapy-induced tumor-specific CD8+ T cell response, resulting in an improvement in median survival and the proportion of long-term survivors. In addition, adding CTLA-4 or PD-L1 immune checkpoint inhibition enhanced the effectiveness of TK/Flt3L gene therapy significantly [297]. Similarly, Chiocca and colleagues (2022) [298] reported that Veledimex (VDX)-regulatable IL-12 gene therapy induces tumor infiltration of CD8+ T cells in tumor, enhancing survival. However, it also upregulates immune checkpoint signaling, justifying a combination trial with ICIs in recurrent GBM. The results claimed that similar to IL-12 gene monotherapy, the toxicities of the combination were dose-related, predictable, and reversible when VDX and/or nivolumab dosages. Plasma pharmacokinetics of VDX indicated a dose-response association between VDX tissue penetration and IL-12 production. Serum IL-12 levels peaked in all participants around three days following surgery. The mOS for VDX 10 mg plus nivolumab was 16.9 months, whereas it was only 9.0 months for all participants [298].
Radiotherapy (RT) is an old therapy for the cancer treatment and has a
significant impact in the treatment of tumor patients. According to the
literature more than 60% of cancer patients accepted this technique [299]. The
primary mechanism by which RT works is by eradicating cancer cells when their DNA
is damaged (through apoptosis or autophagy, for example) during cell division or
in between cell divisions (like in lymphocytes) [300]. Despite with these
advantages of RT some drawbacks are also there. RT does not always eliminate the
major tumor. This is particularly the case for diseases like pancreatic cancer.
Radiotherapy can also cause a lot of toxicity to normal cells [301, 302]. To
minimize this problem there is need for a new strategy. Recent research has shown
that RT works because it causes the best immune reaction in the tissue that is
treated. Experiments showed that mice without T and B cells needed a higher
amount of radiation to get the same effect against tumors as mice with a healthy
immune system [303]. Also, early research showed that RT was less effective in
mice lacking NK, macrophages, or DC [304]. Also, it was shown that IFN-
Ukleja et al. (2021) [313] discussed about the treatment of genitourinary malignancies using immunotherapy and radiotherapy in combination. ICIs have been shown in preclinical and early clinical trials to have an additive impact with radiation treatment, increasing tumor cell death at both the local treated site and, in some instances, at remote sites via the abscopal effect. Author concluded based on previous data combination of both therapies may be solution for the problems of available treatment [313]. Lei et al. (2021) [314] discussed about the treatment of urological malignancy using combination therapy of radiotherapy and immunotherapy. It was observed that the radiation treatment and chemotherapy altogether improve the prognosis for various types of bladders tumors. Author discussed the interaction between radiation and immunotherapy for cancer was addressed, along with the impacts of radioactivity on the immune system [314]. Sezen et al. (2021) [315] addressed the difficulties that arise when planning immunotherapy clinical studies in conjunction with radiation treatment. Clinical trials begin with the formulation of a theory and establishment of primary study goals. Selecting a suitable theory that can be verified in future research and generating new questions for inquiry presents a challenge during the development of studies analysing mixtures of immunotherapy and radiation treatment (RT) [315]. De Felice et al. (2023) [316] describes the case report of NSCLC treatment using the combination of immunotherapy, radiotherapy, and denosumab.
The most widely used immunotherapy-based antitumor therapies include immune checkpoint blockade, tumor vaccines, immunomodulatory drugs targeting T cells, cytokines, adoptive cell transfer immunotherapy, oncolytic immunotherapy, small molecule immunotherapy and other therapies [168, 317, 318].
Discovery of ICIs has been considered as a significant milestone in the arena of cancer therapy. ICIs have achieved tremendous positive therapeutic outcome in the different cancers like RCC, lung cancer, melanoma and CRC [317]. The checkpoint proteins for ICIs involve PD-L1/PD-1, LAG-3, CTLA-4, T cell immunoglobulin, mucin domain 3, and glucocorticoid stimulated tumor necrosis factor receptor associated proteins. In regular conditions, these molecules are properly expressed after the proper activation of immune system regulating the immune response. The adverse immune feedback generated from the cancer cells is utilized for generating the immunosuppressive microenvironment by causing over-expression of the immune checkpoint proteins like LAG-3 and PD-L1. Reports have indicated that PD-L1 is over-expressed in tumor and increases T lymphocytes apoptosis avoiding cancer cell recognition by the CTLs. Hence, anti-PD-L1/PD-1 is utilized to restore the steps in the immune response [317]. ICIs refer to the monoclonal antibodies which act by preventing this immunosuppression by inhibiting the involvement of these checkpoint molecules strengthening the immune response [319]. By inhibiting the immunosuppressive signals, the checkpoint inhibitors can improve body’s anticancer immune response [320].
The important immune checkpoints are PD-1, PD-L1 and CTLA-4. CTLA-4 is present on activated CD4+ and CD8+ T cells [320]. Firstly, Mak showed that the lack of CTLA-4 can lead to the accumulation of T cell blasts, indicating the negative impact on immune responses. In mice, CTLA-4 knockout mice have T cells which are super-activate and proliferating indicating that this receptor plays a role in T cell response regulation. This became the basis by which Allison depicted antitumor efficacy by blocking CTLA-4 [168]. During the initial T-cell stimulation, there is a competition of CTLA-4 with costimulatory receptor CD28 for binding with the ligands B7-1 and B7-2 present on the APCs. This is followed by the facilitation of the negative regulation of the immune response, suppressing the IL-2 secretion and T cell proliferation inhibiting the immune response to cancer cells. PD-1, a transmembrane protein present on the T cells and PD-L1, which may be expressed on T cells. The interaction between of PD-1 to PD-L1 diminishes the T cell responses to the TCR activation signals. As a consequence of the attenuation of antitumor T cell responses, the anticancer efficacy of antibodies inhibiting CTLA-4 and the PD-1/PD-L1 axis is observed [320]. To date, two anti-CTLA-4 antibodies tremelimumab antibodies ipilimumab are utilized for metastatic melanoma and mesothelioma, NSCLC respectively and three anti-PD-1 antibodies like Cemiplimab for skin carcinoma, nivolumab for melanoma, bladder cancer, NSCLC, RCC, HCC, Hodgkin lymphoma, stomach and oesophagus cancer; pidilizumab for follicular lymphoma, multiple myeloma, DLBCL, and pembrolizumab used for bladder cancer, NSCLC, melanoma, SCCHN, Hodgkin lymphoma, stomach and esophageal cancer, squamous cell carcinoma of skin. Three anti-PD-1 antibodies viz. (i) avelumab utilized in Merkel carcinoma, and metastatic urothelial cell carcinoma, (ii) durvalumab for urothelial bladder cancer, and (iii) atezolizumab for NSCLC and bladder. Ipilimumab has been employed widely for treating of numerous cancers like lung cancer, prostate, and kidney cancer. 20% patients with ipilimumab survived higher than 4 years and some survived for more than 10 years [320, 321]. With Nivolumab, the response rate for the treatment was more than 80% with Hodgkin’s lymphoma. The response for the PD-L1/PD-1 blocking antibody is more than 10%. The adverse effects of ICIs like rash, diarrhoea, colitis, endocrinopathies and hepatotoxicity. Fatal side effects are occasionally observed. The application of ICIs is constrained by elevated treatment-related toxicity and diminished response rates [5].
The FDA approved ICIs are illustrated in Table 1 [322, 323].
| Drug | Target | Indications |
| Ipilimumab | cytotoxic T-lymphocyte antigen 4 (CTLA-4) | |
| Nivolumab | PD-1 | |
| Ipilimumab + nivolumab | CTLA-4 + PD-1 | |
| Pembrolizumab | Programmed Cell Death Protein 1 (PD-1) | |
| Atezolizumab | Programmed Cell Death Ligand 1 (PDL-1) | |
| Durvalumab | PDL-1 | |
| Avelumab | PDL-1 | |
| Cemiplimab | PD-1 |
In melanoma, immunotherapy by ICIs has a response rate which is not greater than 50%. Though the buildup of these antibodies in the cancer cells is restricted and the normal tissues exposed to the checkpoint blockade could result in autoimmune diseases. To date, suitable delivery strategies for improving the targeting these checkpoint blockades for reducing side effects and toxicity are rarely reported [317]. There are no reports on ICIs regarding safety in children. CTLA-4 inhibitors in the higher doses were found to be linked with a greater risk of therapy associated mortality. In patients and children undergoing therapy with anti PD-1 monoclonal antibodies neurological and endocrinological adverse reactions are seen out of which some are irreversible. The toxicity of PD-1 and PD-L1 blockade is less serious in comparison to CTLA-4, with no noteworthy rise in TRM. Mostly the side effects associated with ICIs include inflammatory conditions like pneumonitis than colitis. This is of concern in children whose organs are least matured and are susceptible to lifelong disabilities. Skin toxicities like rash, vitiligo and pruritis were seen and vitiligo was found to be common with ipilimumab [324].
Cancer vaccine takes benefit of TAAs for stimulating the immune system, specially longer lasting and robust immune response of CD8+ T cells preventing the metastasis, growth, and recurrence of cancer cells. Cancer vaccines are divided in two categories: therapeutic and preventive. Preventive cancer vaccines prevent cancer occurrence by enhancing the immune response whereas therapeutic cancer vaccines eradicate cancer cells by inducing tumor specific immune reactions. In TVI, the TAAs are presented in the body of patient for enhancing the immune response to the tumors and activating the immune responses of the patient for inhibiting the tumor growth. TVI is used to mend the primary and secondary steps in immunotherapy antitumor response loop [317]. According to the reports, HPV-16 synthetic long peptide vaccine could re-establish normal vulvar neoplasia. Several vaccines have been prepared for preventing cervical carcinoma triggered by HPV infection. Tumor vaccines have been employed for preventing virus related recurrence of tumor as their impact in virus related cancers is not satisfactory. Till now, sipuleucel-T (Provenge) based immunotherapy stands as the sole FDA approved vaccine for prostate cancer, but it is found to show limited effects [317]. This vaccine can improve the survival of the prostate cancer patients by 3 months. Many experiments have shown that the cancer vaccines have shown great clinical effect.
Since a long time, the antigens utilized in the preparation of tumor vaccines were predominantly TAAs. Though these antigens can be present on the tumor cells, they can be also expressed in the normal cells [317]. Owing to the limited specificity for the tumor and immune tolerance, the autoimmune disorders like vitiligo take place. Recently antigens specific to tumor have been identified. For the identification of neoantigens, the cancer cells and the normal cells were taken from the patients followed by the sequencing of the relevant samples by transcriptome sequencing or whole exome sequencing for identification of nonsynonymous mutations existing in cancer cells. This is followed by the utilization of MHC peptide in combination with specific prediction algorithm for screening the antigen sequence that is most immunogenic for the personalized cancer vaccine preparation. Neoantigens possess high specificity as they emerge from the random mutations in the cancer tissues but not in the normal cells [325]. In the clinical trials, neoantigen (NA) based immunotherapies have shown better antitumor efficiency. Tumor mutation burden relates to the number of gene mutations in the cancer cells and indicates high correlation with the efficiency of NA based vaccines. Hence patients with TMB could be good candidates in case of NA based vaccine therapy. Patients with lesser TMB can be treated with TAA based vaccines. Hence, selecting the proper tumor antigens individually for patients could be a significant factor that determines the cancer vaccine success [325].
The neoantigen based immunotherapy poses following limitations:
i. Universal, safe, and efficient neoantigen delivery strategies are still lacking.
ii. The neoantigen identification is individualized, requiring high throughput screening and precise prediction methods for quick identification of new tumor antigens [317].
Cytokines refer to the molecular messengers allowing the immune system cells to
connect to one another generating a robust, synchronized response for the target
antigen. Cytokines are basically proteins, glycoproteins, or polypeptides with a
molecular weight 30 KDa that transmit cell differentiation, proliferation
anti-inflammatory or inflammation signals. There has been growing interest in
exploiting the immune system for cancer eradication. The first cancer
immunotherapy to be approved was cytokine immunotherapy. Several cytokines like
IL-7, IL-12, IL-15, IL-18, IL-21, and GM-CSF have entered the clinical trials for
the advanced cancer patients. To date. FDA approved anticancer agents include
IL-2 for RCC and metastatic carcinoma and INF-
IL-2 is responsible for the activation, maturation, and viability of NK cells. Higher doses of IL-2 (HDIL-2) are responsible for anticancer activity and the low doses can enhance suppressor T cells proliferation suppressing the immune system activation and weakening the anticancer efficacy. Recently the treatments with other cytokines like IL-15 and IL-17 are in clinical trials. HDIL-2 was approved by FDA for the RCC treatment in 1992 and metastatic melanoma in 1998. GM-CSF is a cytokine that resembles IL-3, which stimulates IL-5 and myelopoiesis, the important growth factor for eosinophil by way of a common beta chain on the GM-CSF receptor. GM-CSF may induce initiation of T cells and maturation of DC for improving anticancer effect which has been utilized recently for granulocyte recovery. IFNs are utilized for promotion and maturation of macrophages, DCs, T lymphocytes and NK cells and regulates tumor blood vessel growth [317, 320, 326].
The limitations of cytokine therapy include:
i. Anticancer efficacy of cytokines therapy is limited.
ii. Cytokines display poor pharmacokinetic features and a short half-life. Hence, administration of a higher dose is needed, leading to severe vascular leakage syndrome and CRS.
iii. Higher IL-2 dose can result in capillary leak syndrome leading to hypotension, organ damage, lung edema and kidney failure resulting in fluid extravasation in the organs [317].
Adoptive cell transfer immunotherapy (ACT) is a personalized cancer treatment involving administration of immune cells with anticancer activity to the cancer patient. ACT has shown good anticancer efficiency, especially in haematological malignancies. The two main types of ACT are CARs and tumor-infiltrating lymphocyte (TIL) therapy. Both involve collection of immune cells from the patients, growing them in large amounts in the laboratory and the injection of these cells with immunologic functionality back into the patients or a new recipient host. In TIL therapy, tumor-specific T lymphocytes are isolated from the patient’s tumor followed by in vitro amplification and reactivation, and subsequently reintroduced into the patient. The use of this strategy is constrained due to its difficulty to obtain enough tumor-infiltrating T cells. In case of CAR-T cell therapy, the T lymphocytes are sourced from peripheral blood of patient and subsequently undergo in vitro transinfected with a CAR. After reinfusing in the patients, these cells exhibit the capability to selectively recognize tumor antigens, leading to the targeted destruction of cancer cells. The CAR-T cell treatment can maintain the activity for 10 years or more in vivo. Currently, CAR-T cell treatment is used for treating refractory large B-cell lymphoma and acute lymphoblastic leukemia.
i. The treatment utilizes killer T lymphocytes with large amounts of CTL entering the body and secreting cytokines like IL-6 and IFN-C in abundance leading to severe cytokine storm.
ii. B-cell leukemia and other lymphomas that lack CD19 antigens have an impact on CAR-T cell therapy [320].
Small molecule immunotherapy (SMI) is the utilization of small
molecules for regulation of related enzyme activities or the receptors in the
immune pathways for overcoming immunosuppression or for activation of antitumor
responses. Small molecules medicines possess good tissue permeability, reasonable
half-life, and good bioavailability. These small molecules include cyclooxygenase
(COX-2) inhibitors, TGF-
i. SMIs possess poor specificity compared to the antibodies.
ii. SMIs possess dose dependent toxicity.
iii. SMIs are used in combination with chemotherapy and PTT but the effect of SMIs alone is not significant [317].
The utilization of nano-platform in immunotherapy facilitates targeted delivery of bioactive components through surface modifications, thereby extending their circulation period in the bloodstream, diminishing non-specific dispersion, and augmenting selective targeting [328]. The nanoparticles possess the capacity to mediate the immune response by virtue of their inherent adjuvanticity, thereby enhancing immunogenicity [329]. Certain nanomaterials, owing to distinct physicochemical properties, possess intrinsic abilities to regulate immune responses. Further, nanoparticles act as barriers to immunotherapeutic agents against degradation and heighten their bioavailability by shielding them from enzymatic and other degradative factors [328]. Tailoring nanoparticles enables the mitigation of systemic toxicity by directing it towards specific cells or tissues, thereby reducing the dissemination of immunotherapeutic agents to non-targeted regions [330].
Oncolytic immunotherapy uses OVs. These OVs are naturally occurring viruses administered via an IV or intralesional injections for inducing cell death in the cancer cells and activating the anticancer immune response [331]. OVs can result in tumor cell lysis and adaptive and innate immune response stimulation by selective replication in the cancer cells without causing any damage to the normal cells. This makes this type of immunotherapy superior compared to other immunotherapy approaches as it combats cancer without depending on the expression of a specific antigen [320]. USFDA approved OV include T-VEC, a genetically engineered oncolytic HSV for advanced melanoma. Most of the tumors are metastatic and hence an IVinjection is an important method of drug delivery to the tumors. Avoiding early removal of OVs because of the antiviral response becomes very essential. Ideal immunotherapy needs a balance between the antiviral and antitumoral responses. Various approaches have been tried for obtaining the balance and the therapeutic effect like the depleting antibodies, genetic modification, carrier cells and polymer coating [5]. Oncolysis when used in combination with immunostimulatory cytokines can improve the effect of OV therapy. OV therapy when combined with ICIs could increase the antitumor efficacy [184]. Intra-tumoral injection is safe and is preferred as it could prevent the humoral immunity from virus removal and repeated injections in the tumors can enhance strong immune response against the tumor [332]. OVs activate the immune system to identify the cancer cells and stimulate the anticancer immunity by enhancing immunogenicity and killing the cancer cells [320].
i. Immune system tends to generate antiviral response diminishing anticancer efficiency by premature clearing the virus [320].
Cancer immunotherapy acts by strengthening the immune system preventing cancer metastasis and recurrence making immunotherapy a potential therapy for the cancer control. It aids in boosting the immune system to specifically attack the cancer cells and aiding its long-lasting memory function. Though cancer immunotherapy has achieved success in the recent years with impressive response rates, the side effects, immunosuppressive tumor environment and inefficient immune responses pose challenges to the immunotherapy. The efficacy of immunotherapy is hindered by different factors like high immunosuppression, low immune response, and various negative adverse effects. Also, some immunotherapeutic agents display poor pharmacokinetic profile and small biological half-lifes. Immunotherapy can lead to the proliferation of Tregs giving rise to the autoimmune diseases. There has been ongoing research for improving the effectiveness of cancer immunotherapy agents and searching for new immunotherapy targets for reducing the toxicity, combining the immunotherapy with the other therapies to extend its scope, stimuli-responsive platforms, and newer strategies for overcoming immunosuppression. Clinical trials in cancer immunotherapy have expanded the indications of these treatments and explored the ways to strengthen the immune system for treating tumors. Immunotherapy has immeasurable potential in research and the rapid advancement and development in the field has brought a new hope in curing the cancer.
ND: Conceptualization, Data curation, Writing—original draft. RK: Conceptualization, Data curation, Writing—original draft. SK: Data curation, Writing—original draft. SS: Data curation, Writing—original draft. PDN: Data curation, Writing—original draft. JK: Data curation, Writing—original draft. AAR: Data curation, Writing—original draft. VC: Data curation, Writing—review and editing. RR: Data curation, Writing—original draft. AG: Data curation, Writing—review and editing. CP: Data curation, Writing—review and editing. DB: Data curation, Writing—review and editing. RT: Data curation, Writing—original draft. JP: Data curation, Writing—review and editing. SMoo: Data curation, Writing—review and editing. SMut: Conceptualization, Supervision, Writing—review and editing, Project administration, Resources. All authors have contributed to editorial changes in the manuscript; read and approved the final manuscript; participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
The authors would like to express their gratitude to Manipal College of Pharmaceutical Sciences, Manipal Academy of Higher Education, Manipal, India for providing necessary facilities. The authors would like to acknowledge Biorender for providing platform for drawing figures for this manuscript.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.