
 , Emanuela Turillazzi 2, Vittorio Fineschi 1,*
, Emanuela Turillazzi 2, Vittorio Fineschi 1,*
1 Department of Anatomical, Histological, Forensic and Orthopedic Sciences, Sapienza University of Rome, 00185 Rome, Italy
2 Department of Legal Medicine, University of Pisa, 56126 Pisa, Italy
Currently, no reliable tools exist to predict suicide risk, and the best prevention strategies focus on universal approaches and improving access to mental healthcare. A multitude of factors influences suicidal events, often stochastic, making them unpredictable, even when some clinical risk and protective factors are recognized. Studying peripheral biomarkers may be useful in bridging the gap of uncertainty.
In recent years, research has focused primarily on the study of
neuroinflammation. Black and Miller [1] conducted a meta-analysis to investigate
cytokine levels in psychiatric patients with and without suicidality compared to
healthy controls (HCs). They observed significantly elevated levels of C-reactive
protein (CRP), interleukin 10 (IL-10), IL-6, and transforming growth factor beta (TGF-
In the context of neuroinflammatory dysregulation, the levels of neurotrophins, specifically Brain-Derived Neurotrophic Factor (BDNF) and Glial Cell-Derived Neurotrophic Factor (GDNF), have been studied due to their roles in both central and peripheral neuronal plasticity. BDNF primarily interacts with the Tropomyosin receptor kinase B (Trk-b) receptor, whose expression on plasma membranes is dynamic. BDNF exists in two forms: mature BDNF and its precursor, proBDNF, which exert contrasting functions. BDNF is also implicated in serotonergic pathways, interacting with receptors like 5-HT1A and 5-HT2A, and influencing tryptophan metabolism. These neurotrophins exhibit a strong correlation among their plasma, cerebral, and cerebrospinal fluid (CSF) levels [7]. For BDNF, no significant differences were found in peripheral levels between psychiatric patients with vs. without a history of suicide attempts (SAs), regardless of the timing of the attempt (lifetime vs. recent) [8]. Evidence regarding GDNF remains limited and inconclusive. A study on an adolescent population did not find any association between serum levels of GDNF and suicidality, as well as the severity of depression [9].
Early studies on neurotransmission, particularly the serotoninergic system, produced conflicting results regarding serotonin (5-HT) metabolites and receptors (such as 5-HTR1A, 5-HTR2A, and 5-HTR2C). Similar inconsistencies were observed in studies on 5-HT receptor expression and tryptophan hydroxylase 2 (TPH2), a rate-limiting enzyme involved in the 5-HT pathways. Recently, Kouter et al. [10] identified significant DNA methylation differences in specific neuropsychiatric genes, such as HTR1A, SKA2, MAOA, and GABRA1, in the blood of male suicide victims. No differences were found in other genes like NR3C1, NRIP3, and TPH2.
In a study comparing 30 suicide subjects to 25 HCs, Liu et al. [11] found significant differences in plasma levels of TPH2, proBDNF, GDNF, and the BDNF/proBDNF ratio, but not in BDNF and Trk-b levels. Subgroup analysis showed that TPH2 and proBDNF were higher, and GDNF was lower in suicides, with no differences between suicides due to psychiatric illness (PI) vs. life events (LE), or violent vs. nonviolent SAs. The BDNF/proBDNF ratio was significantly lower only in LE suicides vs. HCs, whereas no differences were noted between PI suicides vs. HCs, or between PI vs. LE categories.
Research on circulating microRNAs (miRNAs) is emerging as a new frontier. Kosten et al. [12] found that in patients with SI, four specific miRNAs (miR-424-5p, miR-378i, miR-6724-5p, and miR-10b-5p) were down-regulated after recovery compared to non-SI patients. These miRNAs are closely associated with fundamental brain functions involving the MAPK, ErbB, AMPK, Ras, p53, and PI3K-Akt pathways. Belzeaux et al. [13] also identified miR-3688 and miR-5695 as significantly associated with worsening SI in depressed patients.
Additionally, lipids, essential for cellular membranes and signal transduction, may influence suicidality by affecting 5-HT neurotransmission through alterations in neuronal membrane components. Currently, the main evidence concerns the association between suicidal risk and low levels of total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C), as well as the expression of Apolipoprotein E, whose overexpression might be implicated in the decrease of plasma cholesterol levels [14].
Regarding lipid absorption, Ohlsson et al. [15] found significantly higher levels of intestinal fatty acid binding protein (I-FABP) in patients with recent SA (rSA) compared to patients with non-suicidal major depressive disorder and HCs. I-FABP is a cytoplasmic protein expressed by small intestine enterocytes, particularly in the jejunum and ileum regions. It serves as a sensitive biomarker for gut integrity and inflammation. In the same study, the rSA group also exhibited significantly lower levels of Zonulin, a protein involved in the permeability of tight junctions between enterocytes. Additionally, there was a notable significant correlation between I-FABP and IL-6.
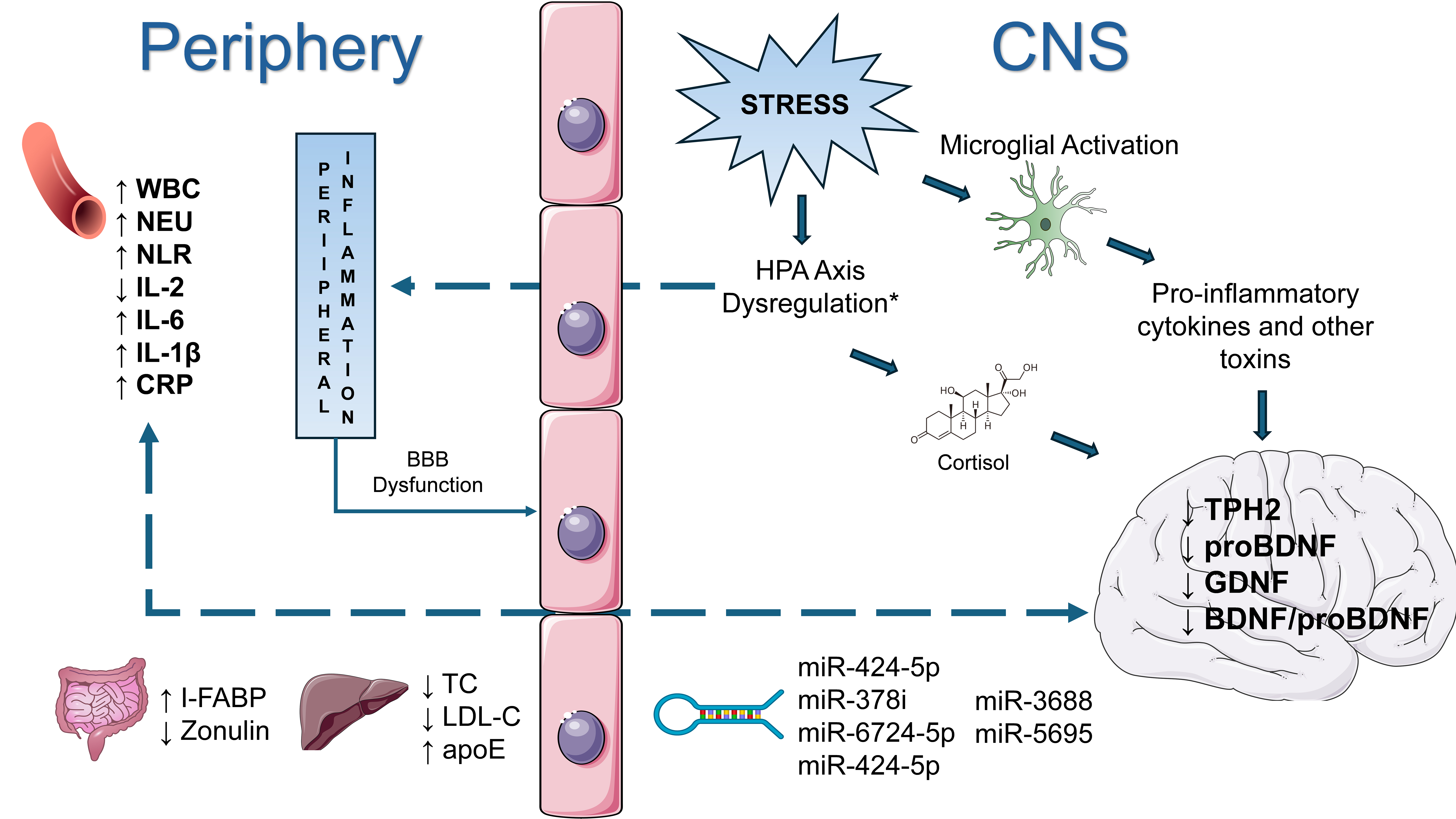
In summary, this overview highlights current biomarker research for suicide, emphasizing noninvasive measures. Stress, psychological distress, and HPA Axis dysregulation emerge as common factors in these findings, potentially linking them to suicide risk (Fig. 1).
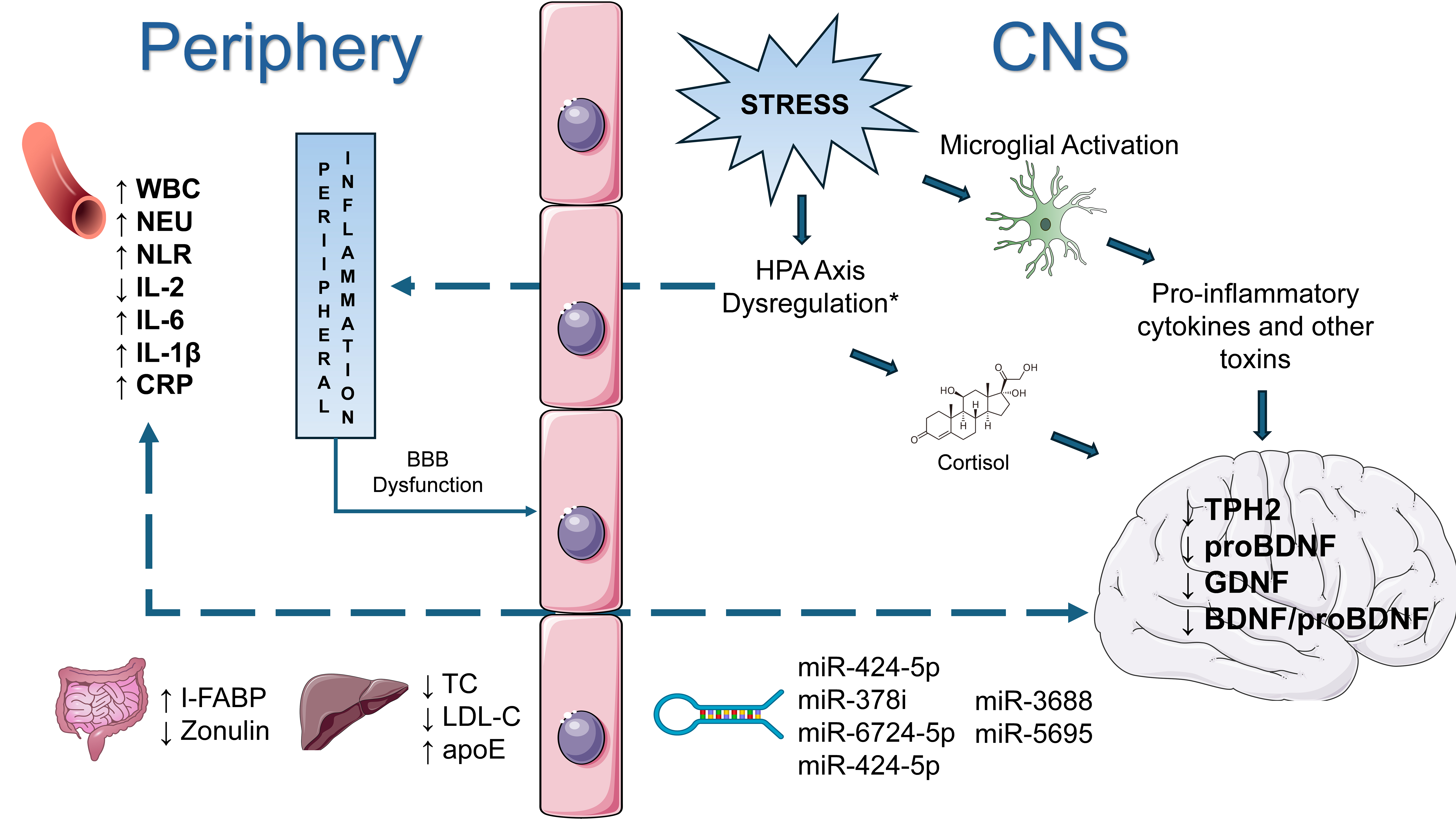 Fig. 1.
Fig. 1.
Schematic representation of the interaction between stress, the central nervous system, and the immune system, with a particular focus on relevant biomarkers in suicide. The dashed lines indicate the passage of molecules through the Blood-Brain Barrier (BBB). CNS, Central Nervous System; BBB, Blood-Brain Barrier; WBC, Increased White Blood Cell count; NEU, Neutrophils; NLR, Neutrophil-to-Lymphocyte Ratio; CRP, C-reactive Protein; HPA Axis, Hypothalamic-Pituitary-Adrenal Axis; TPH2, Tryptophan Hydroxylase 2; proBDNF, pro-Brain-Derived Neurotrophic Factor; GDNF, Glial Cell-Derived Neurotrophic Factor; BDNF, Brain-Derived Neurotrophic Factor; I-FABP, Intestinal Fatty Acid-Binding Protein; TC, Total Cholesterol; LDL-C, Low-Density Lipoprotein Cholesterol; apoE, Apolipoprotein E; IL-2, interleukin-2. *The HPA Axis has been placed in the CNS region, rather than integrated with the Periphery, merely for simplification.
Currently, no established biomarker panel provides highly sensitive and specific diagnostic indications for suicide risk. Future research should aim to develop such a panel to assist clinicians in assessing patients at high risk for suicide and forensic pathologists in distinguishing between suicidal and non-suicidal deaths. AI and machine learning will be crucial in integrating biological and clinical data to create effective risk algorithms.
During the preparation of this work the authors used ChatGpt-3.5 in order to check spell and grammar. After using this tool, the authors reviewed and edited the content as needed and takes full responsibility for the content of the publication.
DM conceived the project and drafted the manuscript; ET and VF supervised the project and critically reviewed the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Thanks to all the peer reviewers for their opinions and suggestions.
This research received no external funding.
The authors declare no conflicts of interest. Given his role as the Editorial Board Member, Prof Vittorio Fineschi had no involvement in the peer-review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Graham Pawelec.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.