



 , Anna Lehmann 1, Rafał Rutkowski 2, Katarzyna Korybalska 2, Janusz Witowski 2, Anna Surdacka 1
, Anna Lehmann 1, Rafał Rutkowski 2, Katarzyna Korybalska 2, Janusz Witowski 2, Anna Surdacka 11 Department of Conservative Dentistry and Endodontics, Poznan University of Medical Sciences, 60-812 Poznan, Poland
2 Department of Pathophysiology, Poznan University of Medical Sciences, 60-806 Poznan, Poland
Abstract
Background: Increased myeloperoxidase (MPO) levels in saliva are
thought to reflect ongoing periodontal inflammation. Less clear is whether and to
what extent salivary MPO is increased as a result of systemic inflammation.
Methods: In the present study, we aimed to determine which demographic,
anthropometric, biochemical, and dental parameters affect the level of MPO in
whole mixed saliva in healthy adults with no apparent inflammatory lesions in the
oral cavity. Thus, 113 individuals, aged 20–61 years (including 30.1% men and
23.9% smokers), were examined. Results: In the univariate analysis,
higher levels of MPO in saliva were found to be associated with age, an increased
body mass index (BMI), higher levels of cytokines tumour necrosis
factor-
Keywords
- myeloperoxidase
- saliva
- body mass index
- inflammation
- oral health
- obesity
Myeloperoxidase (MPO) is the most abundant proinflammatory enzyme stored in the
azurophilic granules of neutrophils, accounting for 5% of their dry mass. It is
also present to a lesser degree in the lysosomes of monocytes. MPO is a component
of the intracellular microbicidal system of phagocytes and part of innate
immunity [1, 2]. MPO is a heme enzyme that is released during phagocytosis, which
uses the superoxide (O
Saliva is a valuable yet complex diagnostic medium, as it is a mix of salivary gland secretions, serum transudate from gingival crevices, oral mucosa cells, and oral microorganisms [5]. Neutrophil-derived MPO constitutes a significant proportion of the total salivary peroxidase activity [6], while the number of neutrophils that migrate to the oral cavity determines the MPO activity in saliva. Due to its potentially defensive role, MPO is found to be increased in conditions associated with oxidative stress and inflammation [7, 8]. Indeed, high salivary MPO levels have been reported in patients with oral inflammation [9]. However, much less is known about the impact of systemic conditions and medication on salivary MPO. Some studies have reported that MPO could be a mediator of inflammatory processes, promoting tissue damage and contributing to the pathogenesis of diseases, such as cardiovascular disease, rheumatoid arthritis, and neurodegenerative disorders [10, 11, 12]. In this respect, Polizzi et al. [13] detected increased levels of MPO in saliva from patients with coronary artery disease. We have recently observed that, compared to healthy individuals, patients with ulcerative colitis that are not responding to combined immunosuppression treatment had significantly decreased salivary MPO levels [14], which subsequently increased when patients responded satisfactorily to biologic therapy [15]. However, changes in the salivary MPO levels from either oral or systemic factors have not currently been investigated in healthy subjects.
Thus, in the present study, we aimed to determine how oral health status and anthropometric factors affect salivary MPO levels in apparently healthy adults. Additionally, we aimed to assess whether biochemical alterations in saliva or demographic factors could be confounders in these relationships.
The study group included 113 randomly selected adult patients (aged 20–61 years, median 32 years; 30.1% men) who presented for a routine dental examination in the Department of Conservative Dentistry and Endodontics at Poznan University of Medical Sciences. All patients provided informed consent to donate saliva for research purposes and were in generally good health, although a few patients had previously received therapy for hypertension (n = 11) and hypothyroidism (n = 7). The exclusion criteria included the presence of another systemic disease (e.g., diabetes mellitus), active oral diseases (e.g., periodontal disease), acute illnesses or infections, administering of drugs or treatment affecting salivary flow, and pregnancy. Smoking was declared by 27 patients.
The examinations of the patients were performed by routine methods and included the parameters of oral hygiene (approximal plaque index: API; plaque index: PlI) and periodontal status (gingival index: GI; sulcus bleeding index: SBI; periodontal probing depth: PPD). The cleaning index was calculated as the product of self-reported brushing frequency and brushing time [16]. None of the included patients were found to have overt inflammatory lesions in the oral cavity.
All patients were measured and weighted to determine their body mass index (BMI).
Unstimulated whole mixed saliva was collected over a period of 20 minutes and
processed, as previously described in detail [17]. Salivary MPO concentrations
were measured using the DuoSet Immunoassay (R&D Systems, Bio-Techne;
Minneapolis, MN, USA). Moreover, two proinflammatory cytokines and two
antioxidants were selected as the markers to reference any changes in body weight
and oral microinflammation. The levels of interleukin-6 (IL-6) and tumour
necrosis factor-
Statistical analysis was performed using Statistica 13.3 (StatSoft, Cracow,
Poland) and GraphPad Prism 9.4.1 (GraphPad Software, San Diego, CA, USA).
Continuous data were analysed for normality using the Shapiro–Wilk test. Data
not normally distributed were analysed using non-parametric statistical tests,
which are specified in each figure legend. To assess the relationships between
MPO levels and other variables, Spearman’s correlation coefficient analysis and
logistic regression modelling, with V-fold cross-validation, were conducted. The
significance level was set at
The myeloperoxidase concentration in the saliva of the examined individuals
ranged from 3 to 720 ng/mL (median of 297 ng/mL). No differences in salivary MPO
concentrations were found between either men and women (Fig. 1A) or between
smokers and non-smokers (Fig. 1B). Therefore, all patients were grouped, and all
subsequent analyses were performed on all patients as a single group. In this
group, the median BMI was 27.5 kg/m
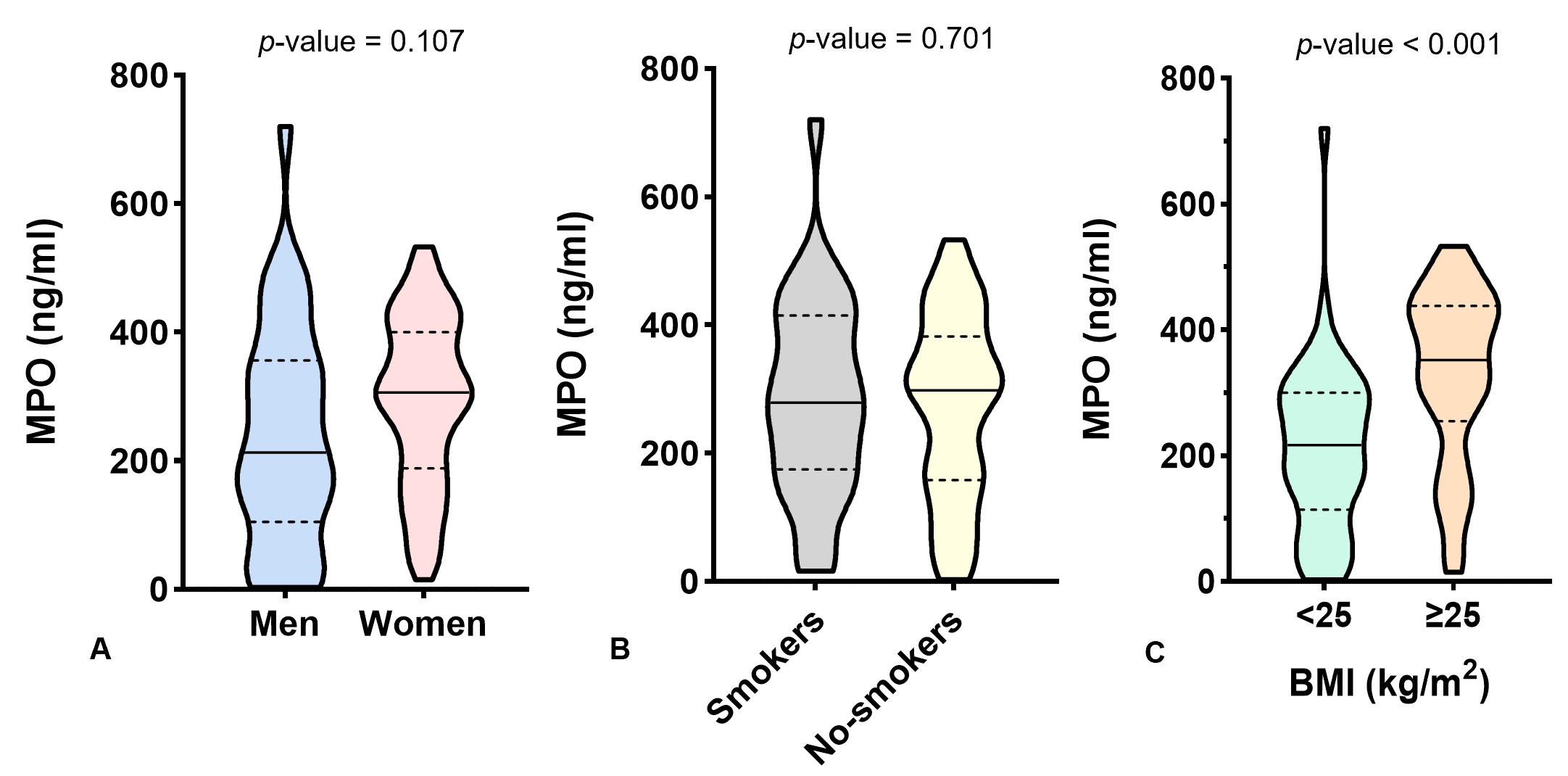 Fig. 1.
Fig. 1.Comparison of MPO concentrations between (A) men (n = 34) and women (n = 79), between (B) smokers (n = 27) and non-smokers (n = 86), and between (C) underweight/normal weight (n = 50) and overweight/obese (n = 63) patients. The data were analysed using Welch’s t-test (A,B) and the Mann–Whitney test (C) and presented as violin plots with medians and quartiles indicated. MPO, myeloperoxidase; BMI, body mass index.
| Parameters | Median | Q1–Q3 | MPO, ng/mL | ||
| R |
p-value | ||||
| Oral health | |||||
| API, % | 60.0 | 30.0–85.7 | 0.332 | 0.001* | |
| PlI | 0.45 | 0.16–0.85 | 0.344 | ||
| SBI, % | 7.7 | 0.0–19.2 | 0.215 | 0.040* | |
| GI | 0.23 | 0.00–0.75 | 0.272 | 0.009* | |
| PPD, mm | 0.90 | 0.69–1.18 | 0.149 | 0.159 | |
| Cleaning index | 6 | 4–8 | –0.163 | 0.134 | |
| Salivary antioxidants | |||||
| SOD, U/mL | 8.9 | 7.9–9.3 | 0.008 | 0.937 | |
| Uric acid, µmol/L | 182.1 | 120.7–246.9 | –0.040 | 0.675 | |
| Salivary pro-inflammatory cytokines | |||||
| IL-6, pg/mL | 3.2 | 1.0–8.0 | 0.256 | 0.008* | |
| TNF, pg/mL | 1.3 | 0.5–2.3 | 0.227 | 0.017* | |
| Salivation | |||||
| Saliva flow rate, mL/min | 0.32 | 0.25–0.50 | –0.272 | 0.005* | |
| Stimulated saliva flow rate, mL/min | 1.25 | 0.75–1.75 | –0.309 | 0.001* | |
| pH of unstimulated saliva | 7.0 | 6.7–7.2 | –0.175 | 0.078 | |
| pH of stimulated saliva | 7.4 | 7.0–7.7 | 0.006 | 0.950 | |
Q1–Q3, interquartile range; API, approximal plaque index; PlI, plaque index; SBI, sulcus bleeding index; GI, gingival index; PPD, periodontal probing depth; SOD, superoxide dismutase; IL-6, interleukin 6; TNF, tumour necrosis factor; *, significant Spearman’s correlation coefficient.
First, we observed that there was a moderate, positive correlation between
salivary MPO levels and BMI (R
As previously mentioned, clinical examinations revealed that the patients had generally good oral health, with a fairly good level of oral hygiene, and no evidence of periodontal inflammation. Nevertheless, there was a weak-to-moderate correlation between MPO levels and the parameters reflecting poorer oral hygiene (API and PlI) and gingival status (GI and SBI). Interestingly, none of the other biochemical parameters correlated significantly with any indices of oral hygiene and gingival conditions, such as MPO in saliva (data not presented).
Moreover, MPO levels correlated positively with the levels of the two
proinflammatory cytokines (IL-6 and TNF
Finally, the MPO levels showed an inverse correlation with both basal and stimulated salivation. Moreover, similar to the correlations with the dental indices, significant correlations were observed relating to saliva flow rates and MPO, although no correlations were noted for the other biochemical parameters (data not presented). Likewise, no correlation was found between MPO concentration and the pH of the saliva.
Since MPO levels significantly correlated with many potentially related parameters, logistic regression analysis was performed to clarify the nature of these relationships. Thus, the study group was divided into two subgroups according to the median MPO concentration (297 ng/mL), and all the variables were subjected to logistic regression analysis.
Table 2 shows the univariate analysis indicated that several of these variables were significant predictors of higher MPO, with BMI presenting the strongest correlation. Moreover, an increase in the levels of all predictors, except for stimulated salivation, was associated with higher salivary MPO concentrations. Furthermore, as shown in Fig. 2, many of the identified parameters showed levels of correlation, with oral hygiene and gingival indices presenting strong correlations, and moderately significant correlations between BMI and these indices. Again, the stimulated saliva flow rate presented inverse correlations.
| Parameter | Standard error | p-value | OR | –95% CI | +95% CI | ||
| Univariate logistic regression models – statistically significant predictors | |||||||
| BMI, kg/m |
0.083 | 0.024 | 1.086 | 1.036 | 1.139 | ||
| API, % | 0.014 | 0.007 | 0.039 | 1.015 | 1.001 | 1.029 | |
| PlI | 1.194 | 0.486 | 0.014 | 3.300 | 1.273 | 8.553 | |
| SBI, % | 0.025 | 0.011 | 0.025 | 1.025 | 1.003 | 1.048 | |
| GI | 1.250 | 0.547 | 0.022 | 3.492 | 1.196 | 10.197 | |
| IL-6, pg/mL | 0.058 | 0.025 | 0.018 | 1.060 | 1.010 | 1.112 | |
| Stimulated SFR, mL/min | –0.667 | 0.284 | 0.019 | 0.513 | 0.294 | 0.895 | |
| Multivariate logistic regression model – forward stepwise method | |||||||
| Intercept | –1.682 | 0.887 | 0.058 | 0.186 | 0.033 | 1.057 | |
| BMI, kg/m |
0.085 | 0.026 | 0.001 | 1.089 | 1.035 | 1.146 | |
| Stimulated SFR, mL/min | –0.555 | 0.298 | 0.062 | 0.574 | 0.320 | 1.029 | |
OR, odds ratio; CI, confidence interval; BMI, body mass index; API, approximal plaque index; PlI, plaque index; SBI, sulcus bleeding index; GI, gingival index; IL-6, interleukin 6; SFR, saliva flow rate.
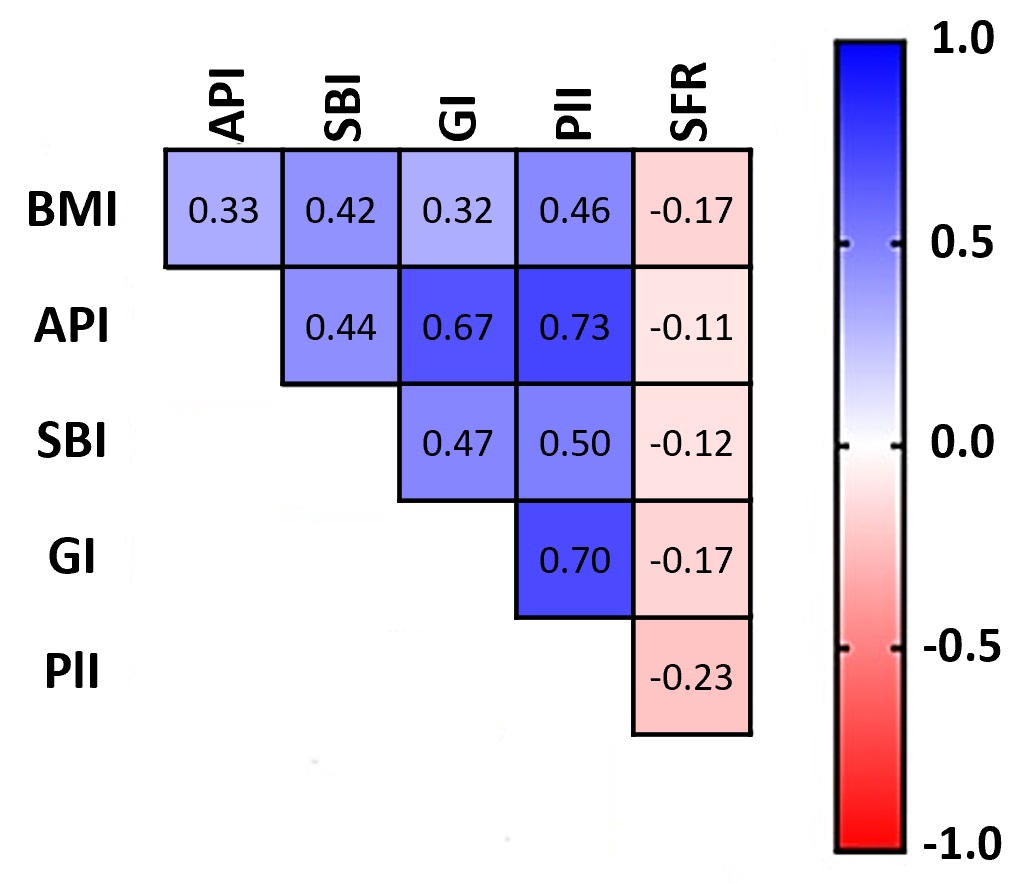 Fig. 2.
Fig. 2.Correlation matrix between the shown parameters. The numbers represent Spearman’s correlation coefficients (R). BMI, body mass index; API, approximal plaque index; PlI, plaque index; SBI, sulcus bleeding index; GI, gingival index; SFR, saliva flow rate.
Thus, next, a multivariate model of forward stepwise logistic regression was constructed. The calculated odds ratios indicated that an increased BMI and a lower stimulated saliva flow rate offered the best predictive marker values for high salivary MPO levels (Table 2).
The model was validated by the V-fold cross-validation method with the presented
receiver operating characteristic (ROC) curves. The high area under the curve
(AUC) values for the training and testing curves confirmed that the model
provided good quality data (0.744
The main observation in the present study was that the salivary MPO levels in apparently healthy adults predominantly correlate to their BMI. While this association does not imply causality, one may envisage a number of mechanisms through which an increased body mass can contribute toward an increase in saliva MPO levels.
Firstly, a higher BMI is associated with inferior gingival status, poorer oral hygiene, and increased levels of proinflammatory cytokines in the saliva. Although the impairment of oral health from the observed parameters appeared to be minimal in the population, the primary cause of these associations remains unknown; however, the resulting chronic microinflammation may lead to an increase in neutrophil migration to the oral cavity, their lysis in a hypotonic environment, and MPO release [18].
Secondly, the level of salivary MPO may be partly related to the level of systemic MPO, which has been reported to increase in accordance with obesity [19]. To the best of our knowledge, this represents the first study to clearly identify that the MPO levels found in saliva correlate to BMI in healthy subjects.
Previous studies on MPO and obesity only analysed the MPO levels found in the
blood. For example, Qaddoumi et al. [20] found that plasma MPO
concentrations were elevated in obese patients, both with and without diabetes,
compared to non-obese subjects. These MPO levels correlated clearly with both BMI
and inflammatory markers, such as CRP, TNF
Moreover, Choromańska et al. [21] found that serum MPO concentrations were significantly elevated and could be used to differentiate obese patients with metabolic syndrome from those only suffering from obesity. These findings showed that MPO activity rose in parallel with the progression of metabolic disturbances in patients with obesity. Additionally, Sparks et al. [22] observed that a twelve-week aerobic exercise intervention promoted a reduction in BMI and a decrease in plasma MPO concentration.
Only a few previous studies have measured the level of MPO in saliva, and these have been performed primarily in the context of periodontium inflammation. In a three-week experimental study by Nascimento et al. [23], the rapid development of gingival inflammation was associated with an increase in salivary MPO.
Klangprapan et al. [24] observed that compared to healthy controls, salivary MPO was significantly increased in patients with periodontitis, and to a lesser extent, in those with gingivitis. Nizam et al. [25] confirmed a close relationship between MPO levels in the saliva and periodontal indices of patients with generalised periodontitis.
Similarly, Lahdentausta et al. [26] showed that using salivary MPO concentrations could clearly distinguish patients with periodontitis from healthy subjects. Interestingly, Polizzi et al. [13] found that salivary MPO levels were higher in patients with periodontitis and coronary heart disease than in those solely with periodontitis. Based on the multivariate regression analysis, the authors concluded that plasma C-reactive protein and total cholesterol levels were the best predictors of salivary MPO levels in these patients.
Meschiari et al. [27] observed that salivary MPO activity was significantly higher in patients with periodontitis and decreased only marginally following three months of non-surgical therapy.
In contrast, Hernández et al. [28] found a significant decrease in MPO activity in the gingival crevicular fluid (GCF) after two months of treatment for chronic periodontitis. Over et al. [29] found that the highest MPO concentrations in patients with rapidly progressive periodontal disease were in the saliva and GCF. Moreover, Saloom et al. [30] observed an increase in GCF secretion during orthodontic treatment and a simultaneous increase in MPO levels, which were associated with a greater rate of tooth movements, especially in obese adolescents.
The strengths of the current study are that a cross-sectional character was performed to investigate the potential relationships between local and systemic parameters and the antioxidant status in healthy adult subjects, while such data were determined in a non-invasive manner. Despite an absence in previously justifying the sample size used, this study determined the correlations and regressions with a high testing power. However, the limitations of the study include the relatively good periodontal condition of the included patients, who reported for regular routine oral examinations; however, this fact excluded the potential confounding of poor oral conditions on systemic dependencies. Thus, in order to investigate further relationships, such as considering body mass and age as concurrent confounders, the size of the subgroups should be increased to provide these analyses with higher statistical powers.
Moreover, additional studies should be performed to consider the correlations between salivary MPO levels and oral, demographic, and anthropometric factors and how these relate to potential alterations in serum MPO levels. Currently, salivary markers are a promising branch of laboratory diagnostics and offer the possibility of determining reference ranges in the future, since these have not yet been determined and large populations are required for testing.
Salivary levels of myeloperoxidase in healthy adults with no clinically detected signs of inflammation in the oral cavity correlated predominantly with the patient’s body mass index. Additionally, a higher body mass index was also associated with reduced oral hygiene, lower gingival status, and less salivation. Therefore, these factors should be considered when interpreting increased salivary MPO concentrations.
Data are available on request from the corresponding author.
KN is responsible for conceptualisation, methodology, formal analysis, investigation and resources, writing the original draft, review and editing, visualisation. AL is responsible for investigation and resources. RR is responsible for investigation and resources. KK is responsible for conceptualisation and methodology. JW is responsible for conceptualisation, methodology, writing review and editing, visualisation and supervision. AS is responsible for conceptualisation, writing review and editing and supervision. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Bioethics Committee of Poznan University of Medical Sciences (189/14). Informed consent was obtained from all subjects involved in the study.
Not applicable.
This research received no external funding.
Given the role as Guest Editor, Kacper Nijakowski had no involvement in the peer-review of this article and has no access to information regarding its peer-review. Full responsibility for the editorial process for this article was delegated to Pier Paolo Piccaluga.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.