

 , Zi-Qiang Wang 1
, Zi-Qiang Wang 11 Colorectal Cancer Center, Department of General Surgery, West China Hospital, Sichuan University, 610041 Chengdu, Sichuan, China
Abstract
Colorectal cancer (CRC) is one of the high incident and lethal malignant tumors, and most of the patients are diagnosed at an advanced stage. The treatment of CRC mainly includes surgery, chemotherapy, radiotherapy and molecular targeted therapy. Despite these approaches have increased overall survival (OS) of CRC patients, the prognosis of advanced CRC remains poor. In recent years, remarkable breakthroughs have been made in tumor immunotherapy, especially immune checkpoint inhibitors (ICIs) therapy, bringing long-term survival benefits to tumor patients. With the increasing wealth of clinical data, ICIs have achieved significant efficacy in the treatment of high microsatellite instability/deficient mismatch repair (MSI-H/dMMR) advanced CRC, but the therapeutic effects of ICIs on microsatellite stable (MSS) advanced CRC patients is currently unsatisfactory. As increasing numbers of large clinical trials are performed globally, patients treated with ICIs therapy also have immunotherapy-related adverse events and treatment resistance. Therefore, a large number of clinical trials are still needed to evaluate the therapeutic effect and safety of ICIs therapy in advanced CRC. This article will focus on the current research status of ICIs in advanced CRC and discuss the current predicament of ICIs treatment.
Keywords
- colorectal cancer
- immunotherapy
- immune checkpoint inhibitors
- microsatellite instability
- deficient mismatch repair
Colorectal cancer (CRC) places a tremendous financial and medical burden on the world. With an estimated almost 1.9 million new cases and 935,000 deaths worldwide, CRC is the third most frequent cancer and the second leading cause of cancer death in 2020 [1]. Even worse, the incidence and mortality rates of CRC have been steadily rising in recent years, in part due to the growth in industrialization, urbanization, and the senior population [1, 2]. The advancement of tumor stage was inversely associated with the prognosis of CRC. Although recent improvements in chemotherapy, radiation, and surgery have made it possible to treat roughly 90% of CRC patients in the early stages, the 5-year survival rate of those advanced CRC patients remains poor [2, 3]. Furthermore, there is an emerging recognition that some rectal cancer patients are not sensitive to the current chemoradiotherapy. With the development of precision medicine, it has been found that rectal cancer patients with high microsatellite instability/deficient mismatch repair (MSI-H/dMMR) have minimal benefit from current 5-fluorouracil (5-FU)-based chemotherapy [4]. The heterogeneous nature of CRC presents a significant therapy problem, and, accordingly, it is necessary to develop individualized treatment for CRC.
At present, the individualized treatment of CRC includes molecular targeted drugs for targeted inhibition of epidermal growth factor (EGFR) [5], BRAF [6], and NTRK [7]. But not all CRC patients harbor these targets. As a new “target”, immune checkpoint brings new hope for the treatment of CRC. Microsatellites are non-coding DNA repeats with a length of 1–10 base pairs, and are prone to mutation during DNA replication and recombination [8]. As an increasing number of neoadjuvant therapy protocols of CRC were studied, neoadjuvant immunotherapy has become the focus of the research in recent years. CRC can be divided into MSI-H/dMMR and proficient mismatch repair (pMMR)/microsatellite stable (MSS) including microsatellite instable-low (MSI-L) and MSS, according to the microsatellite/MMR system. MSI-H is the accumulation of frameshift mutation in microsatellite repeats due to short repetitive sequence stretches called microsatellites. MMR systems combat these errors by identifying and repairing DNA damage, correcting insertions, deletions, or mismatched bases caused by wrong cycles during DNA replication [9]. MSI-H/dMMR accounts for 15% of all colorectal tumors, and tumors with MSI-H/dMMR are characterized by high immunogenicity, strong lymphocyte infiltration in tumor microenvironment and resistance to conventional 5-FU-based chemotherapy [4]. Fortunately, with the continuous progress of CRC immunotherapy research, the emergence of neoadjuvant immunotherapy brings hope to CRC patients with MSI-H/dMMR. Recently, immune checkpoint inhibitors (ICIs) therapy has shown significant efficacy and favorable safety profiles in clinical trials in CRC patients with MSI-H/dMMR [10, 11, 12, 13]. This paper will discuss the mechanism of CRC immunotherapy and focus on the current research status of immunotherapy with ICIs for CRC, analyzing its controversies and challenges. It is expected that this review will provide up-to-date information about CRC immunotherapy and direction for the development of effective treatment to CRC in the future.
Currently, in non-metastatic CRC, surgery alone or combined with adjuvant chemotherapy is considered the mainstay of treatment. However, the efficacy is unsatisfactory, and the treatment impact for CRC in an advanced stage is considerably worse. Despite extensive research and advancement in CRC treatment, drug resistance and recurrence following therapy remain the two main barriers to effective anticancer therapy for CRC [14, 15, 16]. And it has been reported that the objective response rate (ORR) of CRC patients to 5-FU therapy is only approximately 40–50% [17]. Therefore, it is vital and necessary to find new and potent control methods for CRC, and particularly for metastatic CRC.
In recent years, CRC therapeutics has entered a new era of immunotherapy with the development of gene identification and immunotherapy technology. Unlike traditional chemotherapy and targeted therapy, immunotherapy does not directly attack tumor cells, but kills tumor cells by helping direct the immune system to recognize cancer cells as “foreign cells” and attack cancer cells. The immune system mainly combines T cell receptors (TCR) on the surface of T cells with complexes of peptides with major histocompatibility complex (MHC) class I molecules expressed on the surface of other cells (including tumor cells) to distinguish foreign bodies from itself. However, the mutual binding of TCR and peptide–MHC class I complexes alone is not enough to activate the immune activity of T cells, because the activation of its activity is also tightly regulated by co-stimulatory or co-inhibitory signal molecules [18]. As a class of co-inhibitory signal molecule, immune checkpoint inhibitors (ICIs) are a hot spot in the field of tumor immunotherapy. The ICIs are crucial defense mechanism that suppress the immune system via interactions between ligand and receptor to prevent the immune system from attacking normal cells and tissues. On the other hand, cancer cells also use ICIs to avoid detection and destruction from the immune system, leading to continuous advances of cancer cells. At present, cytotoxic T lymphocyte antigen 4 (CTLA4) and programmed cell death 1 (PD-1)/PD1 ligand 1 (PD-L1) inhibitors exhibiting better anti-tumor effects in many studies have gradually become a hot research direction [19]. PD-1, a member of CD28 superfamily, is an important immunosuppressive transmembrane protein expressed on T cell surface. PD-1 mainly includes two ligands: PD-L1 (B7-H1) and PD-L2 (B7-DC). In the microenvironment of tumors, tumor cells can express PD-L1 or PD-L2, and the expression of PD-L1 is more common [20, 21]. T cells cannot destroy cancer cells when PD-1, a transmembrane protein on their surface, binds to PD-L1, which is expressed on the surface of cancer cells. And blocking the interaction of PD-1 and PD-L1 by using anti-PD-1 or anti-PD-L1 antibodies can restore the immune activity of T cells against tumor cells, providing potent antitumor efficacy [22, 23] (Fig. 1).
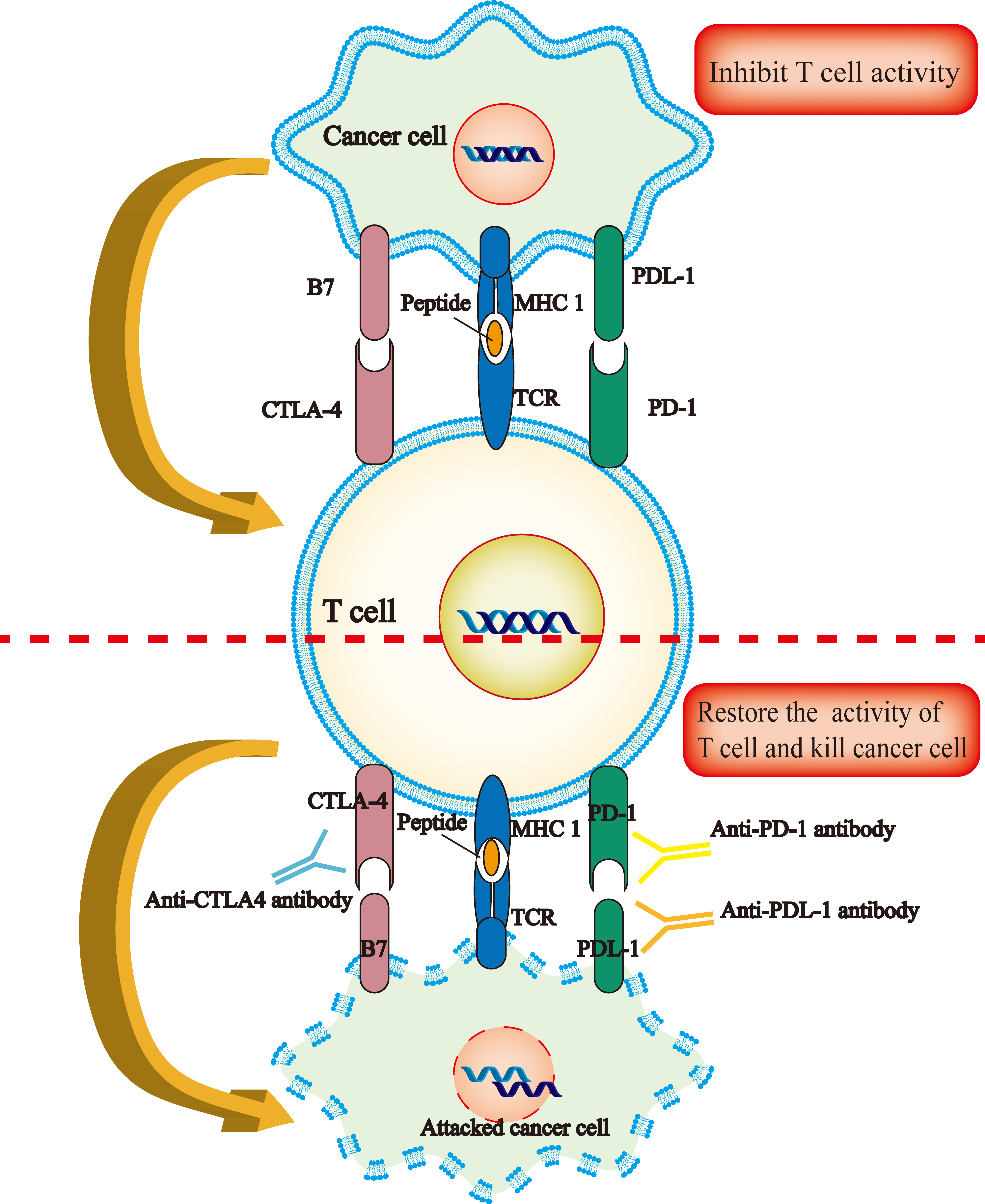 Fig. 1.
Fig. 1.Mechanism of immunotherapy checkpoint inhibitors. Cancer cells inhibit the immune activity of T cells by up-regulating the expression of inhibitory ligands B7 (CD80, CD86) and PDL-1 and binding to the receptors CTLA4 and PD-1 expressed on T cells, respectively. This process will help CRC cells evade immune-mediated killing, which in turn leads to tumor progression. ICIs, such as CTLA4 inhibitors and PD-1 or PDL-1 inhibitors, will help restore the immune-killing effect of T cells to kill tumor cells. ICIs, immune checkpoints; CTLA-4, cytotoxic T-lymphocyte-associated antigen 4; PD-1, programmed cell death receptor 1; PD-L1, programmed cell death ligand 1.
In recent years, with the development of immunotherapy, some potential novel mechanisms of immunotherapy have emerged. In 2019, Yost, Kathryn E et al. [24] published a study aimed at exploring whether PD-1 inhibitors play an anti-tumor effect by “reactivation” of tumor infiltrating T cells or by recruiting new T cells to reach the tumor region. They obtained T cells from tissue samples of 11 patients with basal cell carcinoma before and after anti-PD-1 therapy for RNA single cell sequencing and TCR sequencing. The results showed that the T cells that really play a role after anti-PD-1 therapy may not mainly rely on “resident T cells or memory T cells” but mainly come from newly recruited T cells. Another study [25] found that the effector-like T cells were not only cloned and expanded in tumors, but also in normal adjacent tissues and peripheral blood. Moreover, patients with this clonal expansion feature had the best response to PDL-1 inhibitor treatment. It may be possible to predict the clinical benefits and prognosis of immunotherapy of tumor patients by identifying amplified clones in peripheral blood in the future. In addition, PD-1 is not only expressed on T cells, but also on B cells, regulatory T cells, natural killer cells and myeloid cells. In the past, immunotherapy targeting PD-1 are thought to be due primarily to the contribution of T cells, ignoring the outstanding contributions made by other cells. In January 2020, Strauss, Laura et al. [26] found that PD-1 in myeloid cells might be more immunosuppressive effect than PD-1 in T cells, and myeloid cells may play a leading role in tumor immune escape. Mayoux, Maud et al. [27] also found that dendritic cells are one of the key targets for PD-L1 inhibitors to produce anti-tumor immune response. In addition to PD-1, PD-L1 can bind to B7.1, a key costimulatory molecule expressed by antigen presenting cells such as dendritic cells. Binding of PD-L1 to B7.1 expressed on dendritic cells cam make B7.1 unable to bind to CD28 on T cells, leading to the loss of the ability of antigen presenting cells to activate T cells. PD-L1 antibody can effectively block the mutual binding of PD-L1 and B7.1 after binding of PD-L1 antibody to PD-L1 on dendritic cells. This makes B7.1 released can be bound to CD28 of T cells, which in turn enhances the antitumor response of T cells. In summary, the specific mechanism of ICIs-induced anti-tumor responses remain elusive and needs to be further explored.
At present, it is believed that microsatellite instability (MSI) or mismatch repair (MMR), tumor mutational burden (TMB) and the number of tumor-infiltrating T-cells have been established as a predictive biomarker for response to ICIs therapy, regardless of the primary site [28, 29]. CRC can be classified into two types, MSI-H/dMMR accounting for approximately 15% of all CRCs and MSS/pMMR accounting for approximately 85% of CRCs, according to its status of MSI or MMR in a tumor [30]. And MSI-H/dMMR CRC generally has a higher TMB and increases T cell infiltration in the tumor microenvironment, thereby triggering a strong anti-tumor immune response [31, 32]. Some initial studies [33, 34] showed that ICIs had great therapeutic potential in patients with advanced refractory CRC, which was further confirmed by the results of KEYNOTE-016 study. In 2015, KEYNOTE-016 trial showed that the immune-related ORR and 20-week progression-free survival (PFS) rate of dMMR CRC patients treated with pembrolizumab (an anti-PD-1 inhibitor) were 40% (4 of 10 patients) and 78% (7 of 9 patients), respectively [35]. In 2017, pembrolizumab and nivolumab were approved by the Food and Drug Administration (FDA) for the treatment of CRC patients with MSI-H/dMMR [36]. KEYNOTE-177 study confirmed that pembrolizumab could be used as the first-line standard treatment for MSI-H/dMMR patients with significantly improved median PFS [median, 16.5 vs. 8.2 months, HR 0.59, 95% CI 0.45–0.79, p = 0.0002] and fewer treatment-related adverse events compared with chemotherapy alone or combined with a targeted agent [13]. Because of this study, National Comprehensive Cancer Network (NCCN) guidelines recommend pembrolizumab as the standard of care for first-line MSI-H/dMMR advanced CRC [37]. And according to NCCN guidelines, MSI or MMR testing is now recommended for all patients with a history of CRC [38].
MSS/pMMR CRC has a low TMB and less immune cell infiltration in the tumor microenvironment compared with MSI-H/dMMR CRC. And compared with the exciting anti-tumor effect of ICIs in MSI-H/dMMR advanced CRC, the vast majority of CRC patients with MSS/pMMR are often called a “cold tumor”, which is generally considered to be a part of CRC that is resistant to immunotherapy [18]. The situation mentioned above limits the clinical application of ICIs in CRC patients. In order to expand the portion of CRC patients who may benefit from immunotherapy, researchers are also conducting a number of clinical trials of immunotherapy in MSS/pMMR CRC patients. Fortunately, some clinical trials have shown that there is still a subset of CRC patients with MSS/pMMR who are more sensitive to immunotherapy [39, 40]. For instance, results of the NICHE study from the Netherlands showed that among the 15 pMMR patients, 4 (27%) showed pathological responses, with 3 pathological complete responses and 1 pathological partial response. Subsequent translational analysis found that CD8+ and PD-1-positive T cell infiltration was a predictor of response to immunotherapy in pMMR patients [39]. Therefore, this review will summarize the current research status of CRC immunotherapy according to the MSI/MMR status of CRC, and discuss the current problems of CRC immunotherapy and its possible solutions.
In the last decade, cancer immunotherapy is revolutionizing the treatment of CRC. Unlike conventional therapy such as chemotherapy and radiation, which directly kills cells (both normal and tumor cells), immunotherapy aims to stimulate the body’s innate and adaptive anti-tumor immune response, leaving healthy cells free from damage [41, 42]. However, not all CRCs can benefit from immunotherapy, and potential biomarkers are urgently needed to better stratify the patient populations who may benefit from immunotherapy. In this section, we will review biomarkers for the assessment of immunotherapy efficacy and the progress of immunotherapy in CRC.
To date, MMR or MSI status remains the most important molecular marker for predicting the efficacy of immunotherapy for CRC. Multiple studies have shown that MSI-H/dMMR CRC is more likely to have a favorable outcome for ICIs immunotherapy than MSS/pMMR CRC [43, 44, 45, 46, 47]. The extent of MSI and the resulting mutational burden have been confirmed to be the basis for response to PD-1 blockade immunotherapy in MSI-H/dMMR human and mouse tumors. And the degree of response to PD-1 inhibitors was particularly correlated with the accumulation of indel mutation burdens [48]. Therefore, MSI/MMR status is considered a well biomarker of CRC for response to immunotherapy. The status of MSI can be directly detected by polymerase chain reaction or indirectly detected by immunohistochemical identification of the expression of MMR proteins including MSH2, MLH1, MSH6 and PMS2 [49]. These two methods are also widely used clinically to detect the MSI status of CRC.
TMB is considered another potential predictive marker. The best predicted cut
point for TMB is generally considered to be between 37 and 41 mutations/Mb [50].
And pembrolizumab has been given FDA approval for solid tumor patients with
TMB-high (
Growing evidence shows that tumor growth and progression rely heavily on immune cells infiltrating the tumor microenvironment [59, 60, 61]. Several studies have confirmed that the type and density of immune cell infiltration in tumor are associated with loss of early metastatic invasion and prolonged survival in CRC. Therefore, analysis of tumor-infiltrating immune cells may be another biomarker for predicting the efficacy of CRC treatment [62, 63, 64]. The immunoscore was developed to calculate the density of two lymphocyte populations, cytotoxic (CD8/CD3) and memory (CD45RO) T cells in the core and invasive margin regions of tumor. Based on the density of the lymphocyte population, the immunoscore is divided into four grades, ranging from immunoscore 0 (two lymphocytes in both regions are low density) to immunoscore 4 (two lymphocytes in both regions are high density) [65, 66]. Pagès F et al. [67] conducted a multicenter study of an international consortium of 14 centers in 13 countries to evaluate the prognostic value of the immunoscore on postoperative recurrence risk in patients with TNM stage I–III colon cancer. The results of this study showed that patients with high immunoscore had a lower 5-year risk of relapse, both in the training set and in the validation set. A study including 561 stage III colon cancer specimens showed that dMMR colon cancers had an overall higher density of CD3+ and CD8+ T cells in the tumor microenvironment than pMMR tumors. Furthermore, low levels of CD3+ infiltration at the tumor invasive margin were independent risk factors for poor OS in colon cancer, both in dMMR and pMMR colon cancers [68]. With the deepening of the research on CRC immunoscore, it is even believed that for stage I–III CRC, immunoscore is better than TNM staging in predicting progression-free survival (DFS) and OS [67, 69]. In addition to predicting the prognosis of CRC, the immunoscore has been also considered to be able to predict the treatment response of multiple cancer including CRC to ICIs [70, 71, 72, 73]. Chakrabarti S et al. [74] performed an exploratory assessment of the relationship between intratumoral T cell density (CD3+ and CD8+) and response to PD-1 inhibitor therapy in dMMR metastatic CRC patients treated with a PD-1 inhibitor (pembrolizumab) after failure of standard chemotherapy. They found that the density of CD3+ and CD8+ T cells positively correlated with ORR and disease control in dMMR metastatic CRC receiving a PD-1 inhibitor. However, another study [35] found that the expression of CD8+ T cells was not closely related to tumor PFS and OS. Therefore, there is still controversy about immune cell infiltration as a predictive marker of immunotherapy, and further research is needed to evaluate the potential of immune cell infiltration as a predictive marker of immunotherapy.
In summary, at present, MSI status, tumor mutational burden, and immune cell infiltration in the tumor microenvironment may be effective predictors of CRC response to immunotherapy.
At present, multiple therapeutic strategies are available for CRC, including surgery, chemotherapy, radiotherapy and targeted therapy, etc. According to the advantages and disadvantages of various treatment modalities, as well as the type and stage of CRC, multimodality treatment combining various treatment modalities has been the consensus of CRC experts [75]. With the successful application of ICIs in the treatment of various tumors, such as melanoma and small cell lung cancer [76, 77], there is interest in its therapeutic value for treatment of CRC. For MSI-H/dMMR CRC, immunotherapy has gradually become an alternative treatment strategy for neoadjuvant therapy. In addition, clinical trials have explored from the initial single drug of immunotherapy, to the later double drugs of immunotherapy, and now to explore the treatment strategies combining multiple therapeutic modalities in a personalized manner. As mentioned above, cancer evade host’s immune responses mainly through co-inhibitory receptors on T cells (PD-1, CTLA4) that bind to their ligands (PD-L1/2 and B7, respectively) to downregulate T cell function. Therefore, ICIs targeting PD-1, PD-L1 and CTLA4 were developed to restore immunosurveillance and aid inmmune system fight cancer. Table 1 lists published or ongoing clinical trials on the use of ICIs in CRC.
| ClinicalTrials.gov Identifier | Phase | Study population | Immune checkpoint inhibitor | Primary purpose |
| NCT01876511 | II | Cohort A: MSI-H colon cancer; Cohort B: MSS colon cancer; Cohort C: other MSI-H cancers. | Pembrolizumab (a PD-1 inhibitor) | To explore the efficacy and safety of pembrolizumab in three different populations. |
| NCT02460198 | II | Cohort A: MSI-H/dMMR mCRC that had progressed through standard therapy. | Pembrolizumab (a PD-1 inhibitor) | To explore the efficacy and safety of pembrolizumab monotherapy in previously-treated mCRC. |
| Cohort B: MSI-H/dMMR mCRC that had progressed through at least one line of systemic standard of care therapy. | ||||
| NCT02563002 | III | MSI-H/dMMR mCRC treated with pembrolizumab monotherapy; | Pembrolizumab (a PD-1 inhibitor) | Compare the prognostic outcomes of pembrolizumab versus standard chemotherapy in MSI-H/dMMR stage IV CRC |
| MSI-H/dMMR mCRC treated with standard chemotherapy | ||||
| NCT02060188 | II | MSI-H/dMMR mCRC | Nivolumab (a PD-1 inhibitor) | To explore the therapeutic effect of nimoximab by itself or in combination with other anti-cancer drugs on mCRC |
| NCT-03026140 | II | MSI-H and MSS early-stage colon cancer (Group1: nivolumab + Ipilimumab; Group2: nivolumab + Ipilimumab + COX2-inhibitors) | Nivolumab (a PD-1 inhibitor) + ipilimumab (a CTLA-4 inhibitor) | To explore the therapeutic effect of nivolumab, Ipilimumab and COX2-inhibition in early colon cancer |
| NCT04730544 | II | MSI-H/dMMR CRC | Nivolumab (a PD-1 inhibitor) + ipilimumab (a CTLA-4 inhibitor) | To evaluate efficacy and safety of nivolumab + ipilimumab in CRC patients with MSI-H/dMMR |
| NCT04008030 | III | MSI-H/dMMR mCRC | Nivolumab (a PD-1 inhibitor) + ipilimumab (a CTLA-4 inhibitor) | To the clinical benefit achieved by nivolumab + ipilimumab vs. by nivolumab monotherapy in MSI-H/dMMR mCRC patients |
| NCT03638297 | II | MSI-H/dMMR or high TMB CRC | BAT1306 (a PD-1 inhibitor) | To evaluate efficacy and safety of BAT1306+ COX inhibitor in CRC patients with MSI-H/dMMR or high TMB |
| NCT02788279 | III | mCRC patients treated with at least two chemotherapy regimens. | Cobimetinib (a MEK1/2 inhibitor) + atezolizumab (a PD-L1 inhibitor) | To investigate the efficacy and safety of cobimetinib + atezolizumab and atezolizumab monotherapy vs. regorafenib in mCRC patients treated with at least two chemotherapy regimens. |
| NCT02178722 | I, II | certain cancers including MSI-H/dMMR CRC | Pembrolizumab (a PD-1 inhibitor) | To assess the safety, tolerability, and efficacy of pembrolizumab + INCB024360 in participants with certain cancers. |
| NCT02227667 | II | MSI-H advanced CRC | Durvalumab (a PD-L1 inhibitor) | To evaluate the efficacy of durvalumab in MSI-H advanced CRC |
| NCT02777710 | I | Metastatic/advanced CRC and pancreatic | Durvalumab (a PD-L1 inhibitor) | To assess the safety and efficacy of durvalumab + pexidartinib in metastatic/advanced pancreatic or CRC patients |
| NCT03435107 | II | MSI-H or POLE mutated mCRC | Durvalumab (a PD-L1 inhibitor) | To the therapeutic effect of durvalumab monotherapy in patients with previously treated, MSI-H or POLE mutated mCRC. |
| NCT02982694 | II | Chemotherapy resistant CRC with MSI-H | Atezolizumab (a PD-L1 inhibitor) | To determine the efficacy of atezolizumab + bevacizumab in chemotherapy resistant CRC patients with MSI-H |
| NCT02997228 | III | dMMR mCRC | Atezolizumab (a PD-L1 inhibitor) | To evaluate the efficacy of combination chemotherapy, bevacizumab, and/or atezolizumab in CRC with dMMR |
| NCT02912559 | III | dMMR stage III colon cancers | Atezolizumab (a PD-L1 inhibitor) | To explore the efficacy and safety of atezolizumab + FOLFOX and FOLFOX alone in stage III dMMR colon cancers |
| NCT03186326 | II | MSI-H mCRC | Avelumab (a PD-L1 inhibitor) | To evaluate the efficacy and tolerance of avelumab in the 2nd line of treatment in MSI-H mCRC patients after failure of standard 1st line chemotherapy +/– targeted therapy. |
| Clinical trial details may be accessed at https://www.clinicaltrials.gov/. mCRC, metastatic, unresectable or recurrent CRC. | ||||
Pembrolizumab, a PD-1 receptor inhibitor, was approved by the FDA in May 2017
for cancer patients with MSI-H/dMMR, regardless of tumor site [78]. This is also
the first ICIs approved by FDA for dMMR metastatic CRC. In 2015, Le DT et
al. [35] published the results of KEYNOTE-016: researchers found that various
dMMR tumors could benefit from pembrolizumab immunotherapy. The ORR of dMMR non
CRC cancer patients was 71%, while in patients with advanced CRC, the ORR of
pembrolizumab monotherapy was 40% in dMMR/MSI-H patients and 0 in pMMR patients.
All patients in dMMR/MSI-H group did not reach the median PFS and OS, while the
median PFS and OS in pMMR group were only 2.2 and 5.0 months. Although this study
showed a higher ORR rate for pembrolizumab in the treatment of cancer patients
that were not colorectal, the study found that anti-PD-1 agents could
significantly benefit patients with MSI-H/dMMR advanced metastatic CRC. Since
then, the advantage of immunotherapy in MSI-H/dMMR advanced metastatic CRC has
been found. In 2020, LeD T et al. [79] published the results from the
phase 2 study of KEYNOTE-164 which aimed at evaluating the antitumor activity of
pembrolizumab monotherapy in previously treated, metastatic, MSI-H/dMMR CRC. A
total of 124 metastatic MSI-H/dMMR CRC patients were enrolled in this phase 2
study. These included 61 patients from cohort A (participants were previously
treated with at least two lines of standard therapies, which must include
fluoropyrimidine, oxaliplatin, and irinotecan) and 63 patients from cohort B
(participants were previously treated with at least one line of systemic standard
of care therapy). The results showed that no matter in cohort A or cohort B, CRC
patients with MSI-H/dMMR receiving pembrolizumab monotherapy achieved promising
clinical outcomes (ORR: 33% and 33%; Median PFS: 2.3 months and 4.1 months;
treatment-related grade 3–4 adverse events: 16% and 13%, respectively).
Although this study was also limited by the small subgroup size, lack of a
comparator and local assessment of MSI or dMMR status, it has again confirmed
that pembrolizumab monotherapy is a safe and effective treatment option for CRC
patients with MSI-H/DMMR. Similarly, results of the final analysis of the phase 3
KEYNOTE-177 study showed that pembrolizumab monotherapy did not significantly
improve OS in metastatic CRC patients with MSI-H/dMMR compared with chemotherapy.
The researchers of KEYNOTE-177 study believed that KEYNOTE-177 study did not
achieve the prespecified
In addition to pembrolizumab monotherapy, there are also some other PD-1/PD-L1
inhibitors that have been shown to have antitumor activity against MSI-H/dMMR
CRC. Overman MJ et al. [10] conducted a multicenter phase 2 trial
(CheckMate 142) that included 74 patients with
MSI-H/dMMR metastatic CRC after
the failure of first-line treatment, aiming to evaluate the therapeutic value of
nivolumab, a PD-1 inhibitor, in these patients. The results of CheckMate 142
study showed that nivolumab monotherapy could provide long-lasting tumor control
and responses (31.1% patients achieved an investigator-assessed objective
response and 69% patients had disease control for 12 weeks or longer) with
acceptable drug-related adverse events for MSI-H/dMMR metastatic CRC. And based
on the results of the CheckMate-142 study, nivolumab was approved by FDA in
MSI-H/dMMR metastatic CRC refractory to fluoropyrimidine, oxaliplatin, and
irinotecan-based therapy [12]. Kim JH et al. [82] conducted a
multicenter phase 2 study aimed at evaluating the efficacy and safety of
avelumab, an anti-PD-L1 antibody, in metastatic or unresectable CRC with
MSI-H/dMMR or POLE mutations. The study included 33 metastatic or unresectable
CRC patients with MSI-H/dMMR or POLE mutations after failure of
After ICI monotherapy showed promising clinical results in the treatment of cancer, there has been massive interest in the clinical value of combination of ICIs in cancer patients including CRC. Early trials of the combination of PD-L1 inhibitor and CTLA-4 inhibitor in malignant melanoma showed that combination therapy of nivolumab and ipilimumab could provide higher clinical antitumor activity with acceptable safety compared with monotherapy [86]. In 2017, a meta-analysis including 7 randomized controlled trials evaluated ICI monotherapies and combination therapies in lung cancer and melanoma patients showed that adding nivolumab to ipilimumab was more beneficial for PFS and overall response rate. And sargramostim (a recombinant human granulocyte-macrophage colony-stimulating factor (GM-CSF) that activates innate immunity) plus ipilimumab was associated with better OS and safety [87]. CheckMate 142 is a multicenter, open, nonrandomized, multi cohort phase II clinical trial. It is the largest cohort study of the combination of PD-1 monoclonal antibody and CTLA-4 monoclonal antibody in the field of CRC. It aims to evaluate the efficacy and safety of nivolumab alone or nivolumab combined with ipilimumab in the treatment of dMMR/MSI-H mCRC. The study was divided into three cohorts: the C1 cohort was treated with nivolumab alone in the second- or later-line settings, the C2 cohort was treated with nivolumab combined with ipilimumab at least in the second- or later-line settings, and the C3 cohort was treated with nivolumab combined with ipilimumab in the first line settings. In June 2022, Lenz HJ et al. [88] published the results of the phase 2 study of CheckMate-142: the ORR of the three groups were 39%, 65% and 71%, respectively, and the median response duration (DOR) was not reached. However, at 48 months, the PFS rate of the three cohorts reached 36%, 54% and 51%, respectively, and the OS rate was 49%, 71% and 72%. The OS rate of the double immunotherapy was more than 70%, which proved that the double immunotherapy could bring sustainable survival benefits to these patients. And the earlier immunotherapy is likely to be more effective through a comparison of first-line therapy versus second-line (and beyond) therapy [88]. According to the results of CheckMate 142, nivolumab plus low-dose (1 mg/kg) ipilimumab was approved by FDA for the treatment of metastatic CRC patients with MSI-H/dMMR whose tumors progressed after treatment with fluoropyrimidine, oxaliplatin and irinotecan [89]. Similarly, another clinical study involving 57 previously treated metastatic CRC with MSI-H/dMMR showed that the combination of nivolumab and ipilimumab led to satisfactory disease control rates (86.0% at 12 weeks) and survival outcomes in these patients [90]. These studies show that the combination therapy of ICIs seems to be superior to the ICI monotherapy, and it is expected that there will be more clinical trials on the combination therapy of ICIs in CRC in the future to explore the efficacy and safety.
Despite significant progress in the treatment of metastatic CRC with ICIs, 5-fluorouracil (5-FU)-based regimens such as FOLFOX, FOLFIRI, combined with vascular endothelial growth factor(VEGF) or EGFR inhibitors are still the mainstream treatment strategy for metastatic CRC [75, 91, 92]. Therefore, ICIs in combination with other therapeutic strategies including chemotherapy or molecular targeted therapies for advanced CRC may become a major breakthrough in the treatment of these patients. The relevant research is currently in the clinical trial stage (such as NCT02997228 and NCT02912559; Table 1). It is expected that these studies can bring a promising new therapeutic strategy for advanced CRC.
In conclusion, the published or ongoing clinical trials related to ICIs therapy for CRC indicate that ICIs is a potential treatment strategy for advanced MSI-H/dMMR CRC, but more clinical trials are still needed to explore the safety and clinical effects of its long-term treatment.
Despite the striking efficacy of immunotherapy in the metastatic CRC population with MSI-H/dMMR, the vast majority of metastatic CRC (approximately 95%) are “cold” tumors defined as MSS/pMMR [4]. In order to allow more advanced CRC to benefit from immunotherapy, relevant clinical trials are being carried out (Table 2).
| ClinicalTrials.gov Identifier | Phase | Study population | Immune checkpoint inhibitor | Primary purpose |
| NCT03026140 | II | dMMR and pMMR early-stage colon cancers | Nivolumab (a PD-1 inhibitor) + ipilimumab (a CTLA-4 inhibitor) | To explore the efficacy and safety of nivolumab + ipilimumab in early-stage dMMR and pMMR colon cancers |
| NCT03104439 | II | MSS colorectal and pancreatic cancer | Nivolumab (a PD-1 inhibitor) + ipilimumab (a CTLA-4 inhibitor) | To test the safety and effectiveness of ICIs (nivolumab + ipilimumab) + radiation therapy as a possible treatment for MSS colorectal and pancreatic cancer |
| NCT02860546 | II | MSS mCRC | Nivolumab (a PD-1 inhibitor) | To evaluate the safety and efficacy of TAS-102 (trifluridine/tipiracil) plus nivolumab in MSS refractory mCRC. |
| NCT02948348 | Ib/II | locally advanced resectable rectal cancer with MSS | Nivolumab (a PD-1 inhibitor) | To evaluate the pathological complete remission rate of locally advanced rectal cancer with MSS treated with nivolumab |
| NCT03711058 | I/II | MSS mCRC | Nivolumab (a PD-1 inhibitor) | To evaluate the efficacy of copanlisib (PI3Kinase inhibition) and nivolumab in relapsed/refractory solid tumors with expansions in MSS CRC |
| NCT03388190 | II | MSS/pMMR mCRC | Nivolumab (a PD-1 inhibitor) | To determine the efficacy, safety, and tolerability of the sequential addition of nivolumab to standard-of-care therapy |
| NCT03406871 | Ib | MSS/pMMR mCRC | Nivolumab (a PD-1 inhibitor) | To evaluate the efficacy and safety of regorafenib plus nivolumab in MSS/pMMR mCRC |
| NCT03712943 | I | MSS/pMMR mCRC | Nivolumab (a PD-1 inhibitor) | To evaluate the efficacy and safety of regorafenib plus nivolumab in MSS/pMMR mCRC |
| NCT03374254 | I | MSS/pMMR mCRC | Pembrolizumab (an anti-PD-1 antibody) | To explore safety and efficacy of pembrolizumab + binimetinib alone or pembrolizumab + chemotherapy with or without binimetinib |
| NCT02851004 | II | MSS mCRC | Pembrolizumab (an anti-PD-1 antibody) | To exploratively evaluate the efficacy and safety of BBI608 plus pembrolizumab in MSS mCRC patients who are refractory standard chemotherapy |
| NCT04109755 | II | Localised MSS rectal cancer | Pembrolizumab (an anti-PD-1 antibody) | To investigate the clinical and biological impact of pembrolizumab plus short course radiotherapy (5 Gy, five times) in the neo-adjuvant treatment of localized MSS rectal cancer |
| NCT03626922 | Ib | Chemo-refractory MSS mCRC | Pembrolizumab (an anti-PD-1 antibody) | To evaluate the safety and preliminary anti-tumor activity of pembrolizumab in combination with pemetrexed with or without oxaliplatin in patients with chemo-refractory MSS mCRC without any further standard treatment options |
| NCT03102047 | II | MSS stage II-IV rectal cancer | Durvalumab (a PD-L1 inhibitor) | To evaluate the safety and response to the investigational drug durvalumab (MEDI4736) following chemo-radiation therapy for patients with MSS stage II to IV rectal cancer |
| NCT04108481 | I/II | MSS/pMMR mCRC | Durvalumab (a PD-L1 inhibitor) | To evaluate the feasibility and safety of Yttrium-90 radioembolization (Y90-RE) in combination with durvalumab (750 mg) in MSS/pMMR mCRC |
| Clinical trial details may be accessed at https://www.clinicaltrials.gov/. mCRC, metastatic, unresectable or recurrent CRC. | ||||
Chemotherapy, radiotherapy or molecule-targeted therapy are standard treatment for advanced CRC patients. Therefore, the clinical trial of immunotherapy combined with standard-of-care therapy for advanced MSS/pMMR CRC has also been underway, such as KEYNOTE651 study and METIMMOX study. In April 2020, Chalabi M et al. [39] published the results of the NICHE study involving 40 early-stage colon cancers patients (21 dMMR and 20 pMMR). Results of the study showed that neoadjuvant immunotherapy (nivolumab + ipilimumab) was well tolerated and no surgical delay occurred in all patients. Of the 15 pMMR patients in the NICHE study who received nivolumab + ipilimumab, 4 (27%) were observed to show a pathological response, of which 3 achieved a major pathological response. Subsequent translational analysis found that CD8+ and PD-1-positive T cell infiltration was a predictor of response to immunotherapy in pMMR patients. In November 2021, Lin Z et al. [40] published a prospective, single-arm, phase II trial designed to investigate the safety and efficacy of consolidative chemotherapy with camrelizumab (an anti-PD-1 antibody) following short-course radiotherapy and subsequent surgery in locally advanced rectal cancer patients. In this study, 27 patients received immune neoadjuvant therapy, of which 26 were pMMR patients, and all patients underwent radical surgical resection. The postoperative pCR rate was 48.1%, and among pMMR patients, the pathological complete response (pCR) rate also reached 46.1%; the main immune-related adverse reaction was reactive cutaneous capillary endothelial proliferation (grade 1–2), with an incidence of 81.5% and no grade 4/5 adverse events occurred. However, Patel MR et al. [93] conducted a multicenter, single arm, safety lead-in, phase 2 study to evaluate the efficacy and safety of nivolumab in combination with TAS-102 in patients with refractory metastatic MSS CRC. The results suggest that these patients do not derive clinical benefit from this regimen of chemotherapy plus immunotherapy, although the tolerability and feasibility of this regimen are acceptable.
Radiotherapy is considered not only to kill local tumors, but also to enhance the systemic anti-tumor immune response through a phenomenon known as the abscopal effect (the abscopal effect of radiotherapy means that in addition to the irradiated tumor lesions, the non-irradiated tumor lesions also decrease) [94, 95]. In November 2021, Parikh AR et al. [96] published results of a phase 2 trial aimed at investigating the efficacy and safety of radiotherapy combined with ICIs (nivolumab + ipilimumab) in MSS colorectal and pancreatic cancer. The results showed that the disease control rate (DCR) of CRC patients receiving this therapy strategy was 25% according to treatment intention, while in the per-protocol analysis, defined as receipt of radiation, the DCR rate of CRC was 37%. This study indicated that the addition of radiotherapy to PD-1 and CTLA4 pathway inhibition could to some extent enhance the anti-tumor activity of ICIs in refractory CRC patients with MSS. In June 2020, Corrò, C et al. [97] started a phase II study to evaluate the neoadjuvant pembrolizumab in combination with short-term radiotherapy (5 Gy, five times) in localized MSS rectal cancer. Despite the study is currently recruiting subjects, it is the first clinical trial to explore the combination of ICI and short-course radiotherapy for rectal cancer, and this study may lead to significant breakthroughs in the treatment of rectal cancer, especially in MSS rectal cancer.
Cobimetinib (a potent small molecule MEK inhibitor) can inhibit the MAP kinase
pathway, which is essential for controlling the cell cycle and influences the
immunological environment in the tumor microenvironment. In preclinical models of
CRC, cobimetinib has been shown to upregulate the expression of MHC class I and
the infiltration of effector CD8+ cells into tumors, and produce long-lasting
antitumor immunosuppressive agents when combined with a PD-L1 inhibitor [98].
However, in June 2019, Eng C et al. [99] published the results of the
IMblaze370 study, a study aimed at investigating the efficacy and safety of
cobimetinib plus atezolizumab and atezolizumab monotherapy versus regorafenib in
metastatic CRC patients with MSS/pMMR. The results of the study showed that both
ICI monotherapy and ICIs plus targeted therapy failed to improve the DFS and OS
rate of these patients. It has been reported that tumors can continuously release
various immunosuppressive factors, such as VEGF, which promote tumor growth and
immune escape [100]. Therefore, ICIs combined with small molecule drugs targeting
to inhibit VEGF may be a promising direction for future research to improve the
efficacy of ICIs in the treatment of MSS/pMMR CRC. Bevacizumab, a monoclonal
antibody which targets VEGF to block tumoral neoangiogenesis and tumor
metastasis, is mainly applied in the advanced CRC therapy. NIVACOR trial
(NCT04072198) is a prospective phase II clinical trial to explore the efficacy of
FOLFOXIRI (fluorouracil, calcium folinate, oxaliplatin and irinotecan) +
bevacizumab combined with navumab in patients with metastatic CRC [101]. On
December 14, 2021, Damato, Angela et al. [102] reported results of the
10-patient safety run-in. The results showed that the trial was well tolerated
and its toxicity was acceptable (two patients delayed taking the drug; one
patient stopped the experimental treatment; no treatment related death occurred).
Another phase II clinical trial, the AtezoTRIBE trial (NCT03721653), evaluated
whether FOLFOXIRI plus bevacizumab combined with atezumab might be an effective
treatment strategy for metastatic CRC [103]. The preliminary results of this
study showed that FOLFOXIRI + bevacizumab combined with atezumab was safe and the
median PFS was significantly improved compared with the FOLFOXIRI plus
bevacizumab group [13.1 months vs. 11.5 months, p = 0.012] in
patients with previously untreated metastatic CRC [104]. Regorafenib, a potent
inhibitor of VEGF and oncogenic kinases, is regarded as one of the standard
salvage-line treatments for refractory metastatic CRC patients [105]. A phase IB
study of regorafenib combined with nivolumab in metastatic gastric cancer and CRC
(REGONIVO study) showed that the objective tumor response rate was 36%, the
median PFS was 7.9 months and the incidence of grate
In conclusion, according to the current research, immunotherapy combined with radiotherapy, chemotherapy and (or) targeted therapy can improve the ORR of most MSS/pMMR CRC patients, but the impact on DFS and OS still warrant further validation in the subsequent follow-up.
The application of immunotherapy in CRC cannot be separable from the accurate molecular typing and disease stage of CRC. At present, molecular typing is mainly based on the status of MMR and MSI. Patients can be divided into two molecular typing: dMMR/MSI-H and pMMR/MSS. The clinical staging is related to the risk stratification of patients, which is to distinguish the risk of patients by analyzing the imaging results and pathological results of patients, combining T staging, N staging, MRF status, EMVI status or lateral lymph node status of rectal cancer and other factors. Based on accurate molecular typing and disease stage, we can provide more accurate individualized and appropriate treatment for CRC patients. For example, in the future, for dMMR/MSI-H patients, simple immunotherapy may be enough; while for pMMR/MSS patients, a certain intensity of combined treatment may be required.
The first challenge of ICIs in cancer treatment is immune-related adverse events (IRAEs). As with all the other therapeutic strategies, immunotherapies, including ICIs, also have adverse effects. While activating T cell function, ICIs may also cause a series of special adverse events due to the activation of the immune system and the induction of autoimmunity [108]. IRAEs mainly involve the dermatological, gastrointestinal, pulmonary, hepatic and endocrine organs [109]. The onset of toxicity for IRAEs usually occur within a short period of time after administration of treatment, some IRAEs sometimes can occur months or years after discontinuation of treatment with ICIs [110]. Unlike the management of adverse events of other conventional anticancer treatments, in addition to symptomatic treatment and suspension of ICIs, corticosteroids are often used as first-line treatment for IRAEs. However, corticosteroid therapy also carries potential risks and may increase the risk of overlapping toxicities [109]. And these late-onset, severe and fatal IRAEs can cause untreatable harm to patients. However, the complex molecular mechanisms of IRAEs development and progression are not yet fully understood. It is necessary to further study the molecular mechanism behind IRAEs in order to better manage and effectively prevent side effects in a timely manner.
In recent years, ICIs have shown impressive therapeutic effects in various types
of tumors. Compared with radiotherapy, chemotherapy and targeted therapy, ICIs
therapy has unique advantages. However, ICIs cannot avoid the phenomenon of drug
resistance. Both the tumor itself and the tumor microenvironment have an impact
on the treatment of ICIs, ICIs resistance mechanisms are complex, dynamic and
interconnected. The ICIs resistance mainly includes two forms of primary drug
resistance and acquired drug resistance, and ICIs resistance mechanisms includes
intrinsic and extrinsic factors [111]. For primary resistance, intrinsic factors
such as activation of Wnt/
Another challenge of ICIs in cancer treatment is that the evaluation endpoint of clinical trial needs to be further improved. Currently ORR, median OS and PFS are often used as endpoints for most anticancer drug therapy evaluations. However, most of the patients treated with ICIs are patients with advanced metastatic tumors, and the treatment goals of these patients are durable disease control and prolong survival as much as possible. Median OS allows estimates of OS in 50% of patients with an outcome event, however this does not capture the long-term benefit of ICIs because median OS does not take into account the tails of the survival curve [113]. In addition, ORR assessments did not take into account that effective ICIs therapy may experience delayed therapeutic effect (e.g., tumor regression followed by persistent tumor growth) or “pseudoprogression” (e.g., tumor regression followed by inflammatory responses leading to what appears to be tumor growth). And PFS also faces the same dilemma [114]. Therefore, immune-related response criteria [115], immune response evaluation criteria in solid tumors (iRECIST) [116] and immune-modified RECIST [117] were developed to better define and validate the evaluation endpoints of ICIs treatment in clinical trials. However, it is still necessary to continuously improve the evaluation endpoints of ICIs treatment in order to truly evaluate the anti-tumor therapeutic effect of ICIs therapy.
Immunotherapy with ICIs is now becoming a promising approach for CRC treatment, especially for advanced CRC patients with MSI-H/dMMR. Therefore, the detection of MSI/MMR status in advanced CRC patients to screen the patient populations who may potentially benefit from immunotherapy with ICIs, by polymerase chain reaction or immunohistochemistry, has become the consensus for the treatment of advanced CRC. Despite some clinical trials evaluating the clinical efficacy and safety of ICIs immunotherapy in CRC patients with MSS/pMMR have shown that these patients responded to immunotherapy and could show evidence of partial pathological response. It remains long-term follow up to confirm that these responses translate into long-term survival benefits. ICIs combined with other standard treatments including chemoradiotherapy and targeted therapy show significant clinical improvement and acceptable safety, but there is still a risk of severe immune-related adverse events. In addition, the emergence of resistance to ICIs immunotherapy and the reliability of clinical trial endpoints are still issues that cannot be ignored in the development of ICIs immunotherapy. There are still many trials exploring the clinical benefits and safety of different ICIs treatment regimens or ICIs combined with chemoradiotherapy and targeted therapy as first-line or subsequent-line treatment for patients with advanced CRC. It is expected that these trials will shed new light on the treatment of advanced CRC.
CRC, colorectal cancer; CTLA4, cytotoxic T lymphocyte antigen 4; EGFR, epidermal growth factor; FDA, Food and Drug Administration; ICIs, immune checkpoint inhibitors; MHC, major histocompatibility complex; MMR, mismatch repair; MSI, microsatellite instability; MSI-H/dMMR, high microsatellite instability/deficient mismatch repair; MSI-L, microsatellite instable-low; MSS, microsatellite stable; NCCN, National Comprehensive Cancer Network; OS, overall survival; PD-1, programmed cell death 1; PD-L1, PD1 ligand 1; PFS, progression free survival; pMMR, proficient mismatch repair; RR, remission rate; TCR, T cell receptors; TMB, tumor mutational burden; VEGF, vascular endothelial growth factor.
Literature review, data analysis, and manuscript preparation were performed by YY. WM and ZW contributed for the study conception, design, and revision. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.