



 , Md Sahab Uddin 13,14, Bairong Shen 15, Mohammad A. Kamal 15,16,17,18, Ghulam Md Ashraf 19,20,*
, Md Sahab Uddin 13,14, Bairong Shen 15, Mohammad A. Kamal 15,16,17,18, Ghulam Md Ashraf 19,20,* , Athanasios Alexiou 21,22,*
, Athanasios Alexiou 21,22,*1 Faculty of Medicine, University of Thessaly, 41500 Larissa, Greece
2 Novel Global Community Educational Foundation, NSW 2770 Hebersham, Australia
3 Faculty of Medicine, University of Crete, 28403 Heraklion, Greece
4 Department of Pathophysiology, Medical School, National University of Athens, 11527 Athens, Greece
5 Department of Pharmacology & Toxicology, College of Pharmacy, Jazan University, 45142 Jazan, Saudi Arabia
6 Department of Social Studies and Arts, Novel Global Community Educational Foundation, NSW 2770 Hebersham, Australia
7 Department of Business Administration, University of West Attica, 12243 Athens, Greece
8 Department of Physics and Computer Science, Wilfrid Laurier University, Waterloo, ON N2L-3C5, Canada
9 Department of Mathematics, Northern Virginia Community College, 21200 Campus Drive, Sterling, VA 20164-8699, USA
10 School of Human Sciences, College of Life and Natural Sciences, University of Derby, DE22 1GB Derby, UK
11 Department of Biotechnology, School of Engineering & Technology (SET), Sharda University, 201310 Greater Noida, Uttar Pradesh, India
12 Department of Biotechnology, School of Applied & Life Sciences (SALS), Uttaranchal University, 248007 Dehradun, India
13 Department of Pharmacy, Southeast University, 1213 Dhaka, Bangladesh
14 Pharmakon Neuroscience Research Network, 1341 Dhaka, Bangladesh
15 West China School of Nursing/Institutes for Systems Genetics, Frontiers Science Center for Disease-related Molecular Network, West China Hospital, Sichuan University, 610041 Chengdu, Sichuan, China
16 King Fahd Medical Research Center, King Abdulaziz University, 21589 Jeddah, Saudi Arabia
17 Department of Pharmacy, Faculty of Allied Health Sciences, Daffodil International University, 1341 Dhaka, Bangladesh
18 Enzymoics, Peterlee Place, NSW 2770 Hebersham, Australia
19 Pre-Clinical Research Unit, King Fahd Medical Research Center, King Abdulaziz University, 22254 Jeddah, Saudi Arabia
20 Department of Medical Laboratory Technology, Faculty of Applied Medical Sciences, King Abdulaziz University, 22254 Jeddah, Saudi Arabia
21 Department of Science and Engineering, Novel Global Community Educational Foundation, NSW 2770 Hebersham, Australia
22 AFNP Med Austria, 1030 Wien, Austria
Academic Editor: Graham Pawelec
Abstract
While frailty corresponds to a multisystem failure, geriatric assessment can recognize multiple pathophysiological lesions and age changes. Up to now, a few frailty indexes have been introduced, presenting definitions of psychological problems, dysregulations in nutritional intake, behavioral abnormalities, and daily functions, genetic, environmental, and cardiovascular comorbidities. The geriatric evaluation includes a vast range of health professionals; therefore, we describe a broad range of applications and frailty scales-biomarkers to investigate and formulate the relationship between frailty lesions, diagnosis, monitoring, and treatment. Additionally, artificial intelligence applications and computational tools are presented, targeting a more efficacy individualized geriatric management of healthy aging.
Keywords
- aging
- artificial intelligence
- bioinformatics
- brain-computer interface
- dementia
- expert systems
- frailty
- geriatrics
Fundamentally, Geriatrics has been developed to understand better and manage aging, paving the way to healthy aging. While aging is progressive and determined as unavoidable for all humans, quality of life among elderly individuals is disrupted by many diseases occurring in aging but not caused by aging per se. A condition such as dementia and other neurodegenerative disorders and metabolic syndrome, cardiovascular and musculoskeletal conditions affect most of the elderly population worldwide [1, 2]. Their implications have been conceptualized under frailty, an umbrella term encompassing the multitude of dysfunctions in human biological mechanisms that influence several organ systems and quality of life and mainly refers to genetic, physiological, behavioral alterations, neurodegeneration, and other comorbidities coexistence. Comprehensive modeling of frailty is a prerequisite to conducting frailty—oriented research [3]. Currently, two models of frailty have been reported, the phenotypic and the multidimensional model of frailty. The Cardiovascular Health Study has validated the phenotypic model and based on a pre-defined set of clinical features associated with aging and the severity of concomitant conditions. The Canadian Aging and Health study have validated the multidimensional model to predict all-causes mortality. Although both perceptions have contributed to geriatrics research, the frailty index is considered broader and more suitable for the study of populations with or tools related to dementia. Hence, the authors have focused on the multidimensional aging model in this study given numerous dementia and neurodegeneration—oriented computational tools [4]. In this context, it is established that individuals accumulate age-related disorders and conditions, subjecting them to potentially lethal internal and external stress factors. To evaluate the vulnerability of an old patient, the frailty index is commonly used. Increased frailty is linearly associated with adverse health outcomes and mortality [5, 6]. The rapid development and success of computational tools have transformed healthcare and medical practice during the past decade, with their multidisciplinary applications extending from diagnostic algorithms, risk stratification to establishing treatment strategies, aiding physicians’ and healthcare workers’ decision making, as well as providing patients personalized management and improved quality of life. In addition to refined Artificial Intelligence (AI) tools and applications, wearable devices and social assistive robotic systems have revolutionized the approach to senior services. Several recent publications in gerontology and geriatrics evaluating the use of modern technological approaches and AI in senior care indicate the need for their implication and proved efficacy in everyday clinical practice [6, 7]. Frailty development and symptoms inflection points seem to vary among the elderly population. By taking into consideration some of the latest researches on geriatric medicine and frailty [8, 9, 10, 11, 12], a few lists for frailty scale and symptoms have already been presented concerning mainly psychological, behavioral and daily functions, genetic, environmental, cardiovascular, aging, comorbidities and neurodegeneration symptoms [13, 14, 15, 16, 17]. In the following sections, we describe the corresponding theory and highlight the core components of this review study, including the necessary framework to design a Geriatrics Clinical Decision Support System and well-known computational tools for the management of frailty and individualized diagnosis and treatment in geriatric patients (Fig. 1). Frailty scales enhanced with computational tools and expert systems have a positive outcome in frail populations’ quality of life. At the same time, inherent characteristics and health determinants of these populations can affect their access to this framework. While geriatric evaluation is based on a broad range of tests and frailty scales-biomarkers, several artificial intelligence applications and computational tools may provide holistic management of geriatric patients. This is a literature review study. We have searched biomedical (Pubmed) and tech-oriented (Intech) databases with keywords (frailty, geriatrics, classifications, computational system, and computational tool) to identify computational tools applied in geriatric medicine and frailty management. Original studies reporting or assessing the impact of such tools in the aforementioned fields were prioritized for inclusion. Technical reports, protocols published in peer-reviewed journals, and reviews and assessment reports of computational tools were also eligible for this study to fully assess the contemporary computational arsenal available in geriatrics and frailty management. We excluded reviewed studies published in languages other than English and non peer-reviewed material of commercial or promotional content.
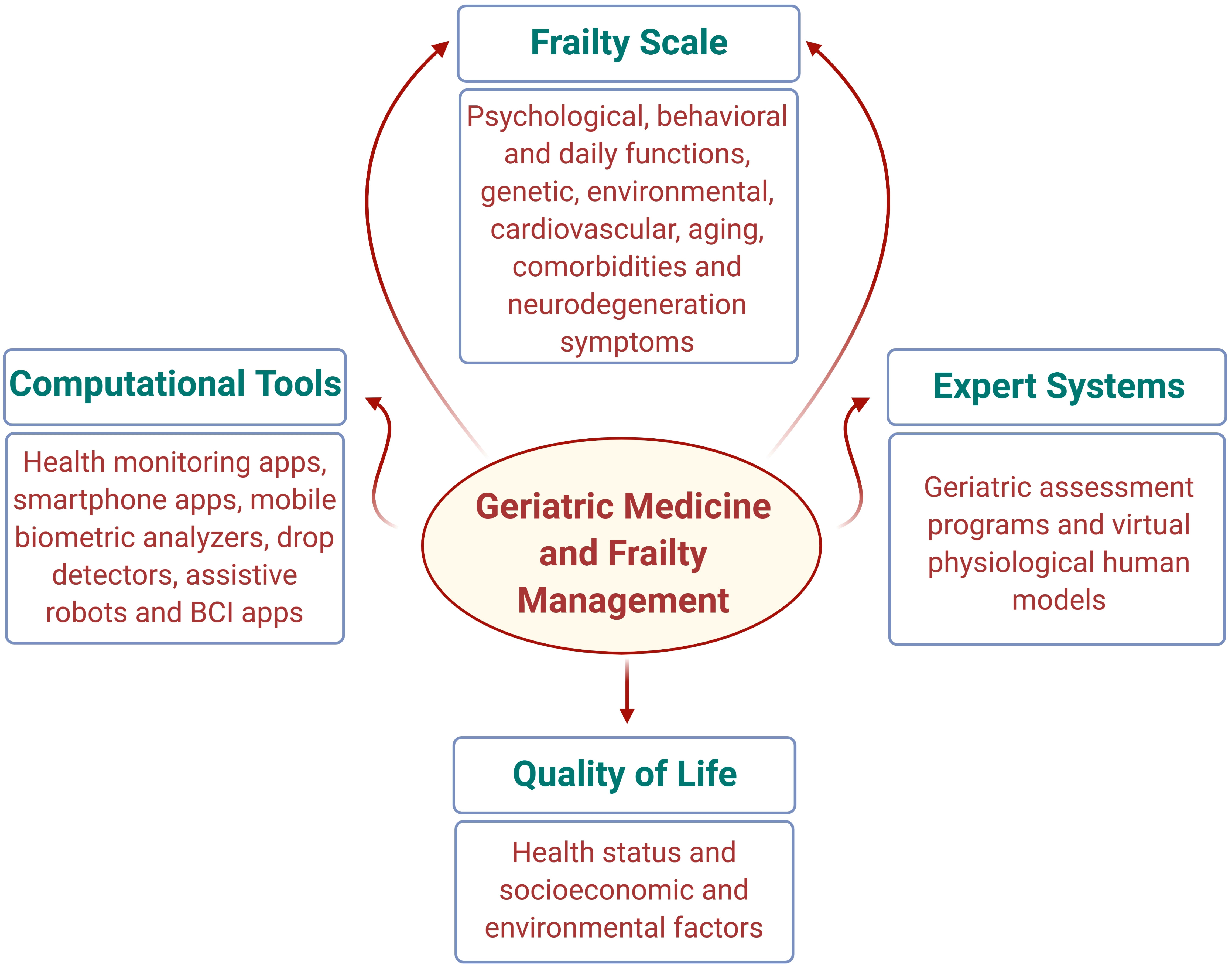 Fig. 1.
Fig. 1.Interim relationship of geriatric medicine and frailty management with quality of life, computational tools and expert systems. The proposed multidisciplinary approach in this article will be significant for researchers from different fields, including frailty indexes and scores, artificial intelligence applications, and computational tools targeting frailty diagnosis and treatment.
Fillit et al. [18] and Alexiou et al. [2] defined Geriatric
Assessment Programs (GAPs) as multidimensional diagnostic processes to identify
functional and pathophysiological problems in a frail person’s life and design a
long-term treatment. Within a rapidly increasing aging population and life
expectancy worldwide, geriatric medicine focus on functional disabilities and
other comorbidities that frail patients commonly present over 65 (Figs. 2,3, Ref. [19]).
Several screening tests are already applied involving the evaluation of
activities of daily living (ADL) and instrumental activities of daily living
(IADL) efficacy, such as Mini-Mental State Examination (MMSE), Clinical Dementia
Rating (CDR), Hachinski ischaemic Scale, Geriatric Depression Scale (GDS),
Functional Assessment Questionnaire, Neuropsychiatric Inventory Questionnaire
(NPI-Q), and Alzheimer’s Disease Assessment Scale-Cognitive (ADAS-COG) [20, 21, 22, 23, 24, 25, 26, 27, 28]
including physical, social and sexual function and cognitive health measure. The
concepts of ADL/IADL have evolved in close proximity to dementia and cognition
research. Hence, dementia-centered computational approaches consist of the bulk
of related ADL/IADL evidence [29]. On top of the above, many disorders are not
caused by aging itself and do not occur in every elderly patient like anemia,
cardiovascular diseases, cancer, stroke, diabetes mellitus, hypothyroidism,
osteoporosis, prostate disease, sexual dysfunction, vision loss, and free
radicals, and this could be a crucial problem on the efficient recognition of
frail patients. Many patients with Mild Cognitive Impairment (MCI) display the
same morphological changes as Alzheimer’s Disease (AD) patients and show no
progression of symptoms. Others eventually develop other types of dementia [2, 30]. Thus, patients with MCI are a mix of individuals that will and will not
convert to AD. As far as imaging techniques are concerned, the hippocampal volume
of medial temporal lobe atrophy as obtained by Magnetic Resonance Imaging (MRI)
and the temporoparietal/precuneus hypometabolism hypoperfusion on or
Single-Photon Emission Computed Tomography (SPECT) biomarkers of neurological
injury is considered as biomarkers with high efficacy in frail patients [2, 31].
Another biomarker of neuronal injury is tau/phosphorylated tau protein. When the
two biomarkers, amyloid beta (A
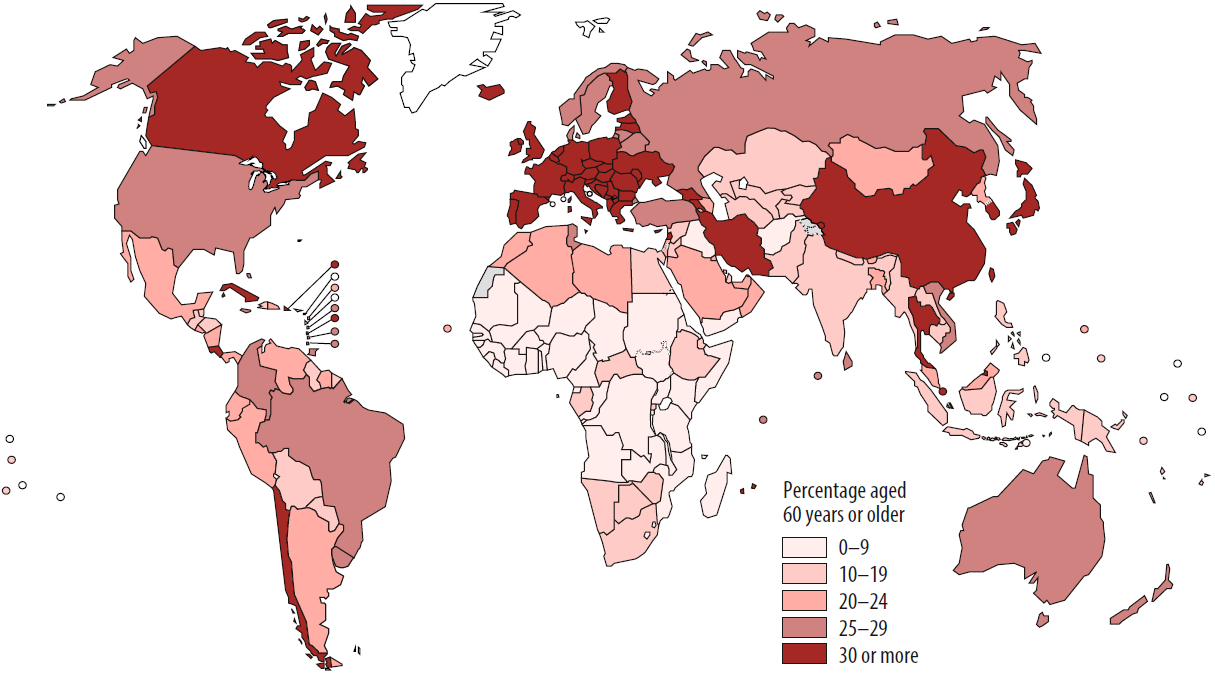
 Fig. 2.
Fig. 2.Changes in life expectancy from 1950, with projections until 2050, by WHO Region and worldwide [19].
A holistic approach to examining the geriatric population remains the wisest
strategy to timely diagnose, provide adequate treatment, improve quality of life,
and reduce morbidity and mortality rates associated with comorbidities.
Additional to all these multiple pathologies, several cellular changes and
molecular mutants can disrupt genetic integrity, leading to cancer [23, 42].
While several clinical trials for elderly medication therapies led novel
therapeutic products like cholinesterase inhibitors for AD,
• Personal demographic data
• Current living conditions
• Information related to elderly health insurance
• Physicians, medical doctors-geriatricians or/and other medical professionals involved
• Personal and family health record
• Hereditary diseases involving the family history
• Information related to physical activity, exercise program, dietary restrictions, and medication records does not require a prescription
• Current medication
• Adverse drug reactions like allergies, intolerabilities, or other side effects
• Physical examination
• Functional inquiry including ADL, IADL, or other support in daily living
• Cognitive testing & behavior
• Results of recent medical examinations-diagnostics, critical medical tests, dental history as well as vaccination history, imaging tests.
Additionally, a frailty system’s differential diagnosis must occur to the 2nd level of disease classification, regarding international standards. More details for implementing the above can be found in the Appendices (Supplementary Material). Considering the above, many studies aim at designing an integrative multiscale Virtual Physiological Human (VPH) model for the accurate evaluation of human frailty and the proposed diagnostic protocols in elderly populations. The clinical data for a VPH model should include neuropsychological test scores, molecular data, imaging, electrophysiological data, biomarkers detected from blood, patient history, and demographic data. While many tools have already been designed and developed to organize and analyze biological data [44, 45], specialized Information and Communication Technologies (ICT) components should be used for the implementation of a VPH model, such as the Web Ontology Language (WOL), the Field Modeling Language (FieldML), and the OSIRIX Open-Source software (OsiriX MD 12.x (PIXMEO SARL, Geneva, Switzerland)) for the imaging data manipulation and storage [46, 47, 48, 49, 50, 51, 52, 53, 54, 55].
As humanity seeks ways to extend life expectancy [56], the need for advanced biological engineering tools is dire. Over the last decades, mounting experience of methodological scientific documentation and experimentation, resulted in the development of interdisciplinary approaches involving genetic engineering, nanotechnology, quantum mechanics, and computer science. While biomedical evolution and synthetic biology are formulating the so-called 4th industrial revolution, it is essential to highlight the available geriatric medicine tools. Considering the exponential growth of AI funding during the last years, healthcare AI has become an essential component of the majority of these tools. These applications aim to improve treatments’ effectiveness, reduce costs, and leverage healthcare services by means of home health monitoring apps, mobile biometric analyzers, drop detectors, virtual companions, and anti-aging open data research [7, 10, 11, 12, 57]. 2019 marked a tremendous increase in healthcare AI funding. Despite the fact that a considerable decrease was noted during the last months of 2019, a positive trend towards higher funding has been observed from the beginning of 2020 onwards [58].
Several innovative tools focus on individualized monitoring and diagnosis in the elderly population based on mobile monitoring applications and wearables (Table 1, Ref. [29, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89]). Apple offers the triplet of HealthKit (Apple Inc., California, USA), ResearchKit 2.0 (Apple Inc., California, USA), and CareKit (Apple Inc., California, USA) for multitasking data processing, targeting researchers, health professionals, and patients [59]. HealthKit is the core platform for safe data storage and manipulation, and interconnection between health apps. ResearchKit offers a reliable framework for the creation surveys and gather clinical data from end-users. Finally, CareKit provides the necessary framework for personalized healthcare and continuous communication between patients and doctors. One of the well-known and widely applied applications of Apple’s ResearchKit library is the mPower 2.0 (Sage Bionetworks, Seattle, USA) [60], which is an evidence Smartphone-based study for the identification of Parkinson’s Disease (PD) severity by measuring dexterity, balance, gait, and memory, providing with very low-cost clinical data from thousands of patients in a short time [61]. Similarly, the EpiWatch (Johns Hopkins Medicine Technology Innovation Center, Baltimore, USA) is a powerful application of Apple’s ResearchKit library from the Johns Hopkins University, predicting seizure incidents using the Apple Watch [62, 63]. This app could help manage epilepsy, creating a correlation between episode history and medication, based on the heart rate accelerometer and gyroscope sensors of the Apple Watch, simultaneously informing caregivers or family members of any produced alert situation. Another very useful for frailty management Apple’s ResearchKit application is SleepHealth [64, 65] (University of California, San Diego, USA). A mHealth study based on the iPhone, iPod Touch, and Apple Watch, offers a personalized wellness tool for the evaluation of sleep habits and their potential correlation with the comorbidities of the nowadays status quo, like diabetes, heart disease, obesity, and depression.
| Release date | Tool | Functionality | Target group |
| 2014 | Apple HealthKit API (Health App) [59] | Core platform for safe data storage and manipulation, interconnection between health apps | Researchers, Healthcare professionals, Patients |
| 2015 | Apple ResearchKit API (Health App) [61, 62, 63] | Creating surveys and gathering clinical data from end-users | Researchers, Healthcare professionals, Patients |
| 2016 | Apple CareKit API (Health App) [59] | Framework for personalized healthcare and continuous communication between patients and healthcare professionals | Researchers, Healthcare professionals, Patients |
| 2015 | mPower [60, 61] | Smartphone-based study for the identification of Parkinson’s Disease (PD) severity by measuring dexterity, balance, gait, and memory | Patients with PD and specialized healthcare professionals |
| 2019 | EpiWatch (combined with the Apple Watch) [62, 63] | Prediction of seizures and management of epilepsy, Correlation between episode history, medication, vital signs, accelerometer and gyroscope sensors of the Apple Watch, Instant notification to caregivers | Patients with seizures/epilepsy, caregivers and specialized healthcare professionals |
| 2016 | SleepHealth [64, 65] | Personalized wellness wearable for the evaluation of sleep habits and their correlation with comorbidities such as diabetes, heart disease, obesity, and depression | Patients and (seemingly) healthy individuals |
| 2019 | Harvard nanoparticle-enabled smartphone system [66] | Rapid and sensitive virus detection by means of a microchip labeled with specifically designed platinum nanoprobes using a convolutional neural network. Designed for HBV, HCV and Zika virus but can be adapted to SARS-CoV-2 | Elderly, vulnerable populations, frontline workers (particularly those of advanced age) |
| 2019 | At-Home Kidney Testing from Healthy.io [67, 68] | Urine analysis at home by means of smartphone camera, referral for the Albumin to Creatinine ratio (ACR) at-home test kit, results available for doctor’s review | Patients with kidney disease and patients at risk of developing kidney disease (Diabetes mellitus, hypertension etc.) |
| 2018 | The Google IDx-Diabetic Retinopathy (DR) AI diabetic screening system [69, 70] | DeepMind convolutional neural network-based Diabetic Retinopathy detection algorithm | Patients with diabetes mellitus and known or suspected Diabetic Retinopathy |
| 2018 | EyeArt® by EYENUK [71] | Deep Learning-based deep-neural networks system for imaging classification | Patients with diabetes mellitus and known or suspected Diabetic Retinopathy, patients with age-related macular degeneration, cataract, retinopathy of prematurity, retinal vein occlusion, and glaucoma |
| 2006–2019 | Brain-Computer Interaction (BCI) neuroinformatic tools [72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82] | Electroencephalography (EEG)-based self-navigation through virtual worlds, management of depression and apathy through enhanced environmental stimulation, or application of low-pressure ultrasounds for the activation of neurons in neurodegeneration. Mechanistically, these might improve dendritic branching and synaptic density resulting in neurogenesis | Patients with neurodegeneration combined with enriched sensorimotor stimulations who can benefit from cognitive-behavioral therapy and art therapy |
| 2015 | Personal care robots (Care-O-bot®, Robot-Era®, the Zora®, the JustoCat®, PARO®) [83, 84, 85, 86, 87, 88] | Social assistive robots mainly used on a non-medical basis offering assistance autonomously on patients with reduced decision-making ability and supporting the services of professional caregivers and geriatricians | Patients with a low level of functionality—autonomy, physicians, caregivers |
| 2019 | Clinatec and the University of Grenoble, France [89] | A mind-reading exoskeleton based on two brain implants that monitor the brain’s part responsible for movement | Tetraplegic patients |
| 1950 | (Instrumental) Activities of Daily Living (IADL–ADL), Barthel Index (BI), Katz Index of Independence in Activities of Daily Living, Functional Independence Measure (FIM), Activities of Daily Living (ADL) Profile, Activities of Daily Living Questionnaire (ADLQ) [29] | Indexes measuring and assessing personal demographic data, current living conditions, health insurance features, personal and family health record including hereditary diseases, available healthcare resources, physical activity, exercise program, dietary restrictions, medication (both on prescription and over the counter medication) records, adverse drug reactions, physical and laboratory examinations, imaging tests’ findings, functional inquiry, cognitive testing & behavior, dental history, vaccination history | Patients with limited functionality (Dementia, Motor deficits, Spinal Cord Injury, Dementia, Advanced Cancer etc.) |
Within the Smartphone-based applications and point-of-care diagnostics [66, 90, 91, 92, 93], the latest nanoparticle-enabled Smartphone system (Harvard Medical School, Boston, USA) from the Harvard Medical School offers rapid and sensitive virus detection on a microchip labeled with specifically designed platinum nanoprobes using a convolutional neural network, such as HBV, HCV, and Zika virus [66]. Although these advances seem loosely connected to geriatrics, they have become relevant during the COVID-19 pandemic. Offering point-of-care diagnostics to vulnerable geriatric populations can mitigate the spread of viral infections such as COVID-19 and the seasonal flu. Repurposing such modalities for COVID-19 has been in the spotlight of ongoing research [94].
On top of these, it is worth to mention the beneficial At-Home Kidney Testing from Healthy.io (Boston, USA) [67, 68], which turns the Smartphone camera into a medical device for urine analysis at home. The application aims to streamline the diagnosis and monitoring of Chronic Kidney Disease (CKD) in few simple steps: the Albumin to Creatinine ratio (ACR) test kit is sent to patients with their consent, the patients performs the urine test and use their smartphone to analyze the results, and eventually the exported ACR diagram is sent to physicians. Additionally, platforms with strong sensitivity and high diagnostic accuracy for Diabetic Retinopathy (DR), age-related macular degeneration, cataract, retinopathy of prematurity, retinal vein occlusion, and glaucoma gradually become available. The Google DeepMind convolutional neural network-based DR-detection algorithm (AlphaBet Inc, London, UK) [69], the IDx-DR AI diabetic screening system (Digital Diagnostics, Coralville, USA) is already being used to more effectively diagnose eye diseases [70] and the EyeArt DL-based deep-neural networks system (Eyenuk Inc., Woodland Hills, USA) for imaging classification [71] are well known and highly applied in the market AI platforms for geriatric medicine (not limited). A different approach uses Brain-Computer Interaction (BCI) tools in patients with neurodegeneration combined with enriched sensorimotor stimulations offering cognitive-behavioral therapy and art therapy [72, 73]. These neuroinformatics tools provide Electroencephalography (EEG)-based self-navigation through virtual worlds [74, 75], reduce depression and apathy through enhanced environmental stimulation improving dendritic branching and synaptic density resulting in neurogenesis [76, 77, 78] or apply low-pressure ultrasounds for the activation of neurons in an effort to reduce or even reverse neurodegeneration [79, 80, 81, 82].
It is crucial to include in this review, personal care robots, which are nowadays widely used increasing the quality of life of elderly population. Such social assistive robots are usually used on a non-medical basis offering assistance autonomously on patients with reduced decision-making ability also supporting the services of professional caregivers and geriatricians [83, 84]. Even though several types of assistive robots are already launched in the market like the Care-O-bot®, the Robot-Era®, the Zora®, the JustoCat, and the PARO, for monitoring daily activities, still the acceptance within the general population can be characterized as low, depending on the patients’ age, gender, cognitive ability, education, culture and social status quo [83, 85, 86, 87, 88]. Closing this section, we present the latest presentation of an exoskeleton controlled by a brain-machine interface in tetraplegic patients. The French biomedical research center Clinatec and the University of Grenoble, France, demonstrated a mind-reading exoskeleton based on two brain implants that monitor the brain’s part responsible for movement [89].
Computational tools and particularly AI has multiple applications in medicine, specifically in acute clinical care and in the hospital setting, implementing various specialties and influencing healthcare delivery quality. Clinicians should be aware of the recent advances of AI in geriatrics. By endorsing programs and systems in their everyday clinical practice, decision-making will become more efficient and faster, providing different treatment options in individual patients. These systems will make extensive use of existing interoperability standards to address interoperability issues related to heterogeneous data sources, organize, analyze, and share vast quantities of biomedical research data, therefore clinicians will also be much more confident about their clinical decisions. While GAPs are already increasingly applied in nursing homes and individuals’ health professionals for diagnostic accuracy, the proposed study enhances the scientific community with a new and efficient Aging Cure and Care tool. However, the implementation of such computational tools in clinical practice renders a variety of challenges. First and foremost, efficacy and proved patient safety can become quite disputable. For consideration, a diagnostic AI algorithm is deemed a high-risk tool since the consequences of an instant misdiagnosis could potentially prove problematic, even lethal to patients. Moreover, the liability in case of medical errors attributed to such tools can be quite intricate, varying among regions and legislative systems [95]. Without a doubt, computational tools whose human input remains minimal appear more troublesome comparing to AI advances with more human engagement. However, the deposition of confidential personal health-related data to this kind of software can also raise significant concerns.
What is more, a considerable number of individuals fulfilling the frailty criteria lack the digital skills necessary for the shift of their care towards computational diagnostics and management. During the COVID-19 pandemic, policymakers, healthcare providers and individuals have become more receptive and knowledgeable in terms of digital health. This familiarization in the context of COVID-19 or other communicable and non-communicable diseases has already paved the way of digital literacy among the elderly [96]. Cost-effectiveness and accessibility to AI programs consist of another two limitations that need further evaluation. For future direction, extensive clinical and non-clinical trials are necessary to evaluate these significant parameters for the AI systems to be approved and widely used by healthcare professionals [97, 98, 99]. The current study’s limitations include the lack of a meta-analytic approach to assessing the reported tools’ real-life effectiveness. This can be the scope of a future study. Overall, computational tools in contemporary geriatrics and frailty management aim to improve treatments’ effectiveness, reduce costs, and increase healthcare validity, and capacitate home health monitoring apps, mobile biometric analyzers, drop detectors, virtual companions, and anti-aging open data research.
Not applicable.
Frailty classification for differential diagnosis, according to the icd10data.com American system for medical coding rules and procedures in the Supplementary Material File.
ADL, Activities Daily Living; ACR, Albumin to Creatinine Ratio; AD, Alzheimer’s
Disease; ADAS-COG, Alzheimer’s Disease Assessment Scale-Cognitive; A
Conceptualization done by BS, MAK, GMA and AA; methodology design and implementation by AK, IH, IG, GZ, NKJ and MSU; data collection and analysis by AML, CT, PC, GZ, FA and PS; All authors contributed in writing manuscript, reviewing and editing, and final approval.
Not applicable.
Not applicable.
This work was funded by the Deanship of Scientific Research (DSR), King Abdulaziz University, Jeddah, Saudi Arabia under grant no. (RG-18-130-43). The authors, therefore, acknowledge with thanks DSR technical and financial support.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/j.fbl2708232.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.