







1 Department of Ophthalmology, Cullen Eye Institute, Baylor College of Medicine, Houston, TX 77030, USA
2 Everglades Biopharma, LLC, Houston, TX 77054, USA
3 Texas Children Hospital, Baylor College of Medicine, Houston, TX 77030, USA
4 Department of Ophthalmology, The Second Hospital of Jilin University, 130041 Changchun, Jilin, China
5 Vascular Biology Institute, University of Miami Miller School of Medicine, Miami, FL 33136, USA
Academic Editors: Shikun He and Graham Pawelec
Abstract
Background: To circumvent possible systemic side effects, anti-angiogenic drugs targeting vascular endothelial growth factor (VEGF) for ocular neovascular diseases in adults are approved only for intravitreal administration. However, intravitreal injection itself can elicit injection-related adverse effects, and premature eyes of infants with retinopathy of prematurity (ROP) may be particularly susceptible to intravitreal injection. Therefore, an unmet clinical need is to develop safe systemic anti-angiogenic therapies for ROP. We recently reported that secretogranin III (Scg3) is a disease-restricted angiogenic factor and that systemic anti-Scg3 mAb alleviates ROP in animal models with minimal side effects on developing eyes and organs. The aim of this study is to investigate the safety and efficacy of a humanized anti-Scg3 antibody via systemic administration. Methods: We analyzed the safety and efficacy of a humanized anti-Scg3 antibody Fab fragment (hFab) delivered by intraperitoneal injection in oxygen-induced retinopathy (OIR) mice, a surrogate model of ROP. Results: The results showed that systemic anti-Scg3 hFab effectively alleviated pathological retinal neovascularization in OIR mice with similar efficacy to the anti-VEGF drug aflibercept. Systemic aflibercept conferred significant adverse side effects in neonatal mice, including reduced body weight, abnormalities in retinal and renal development, and retarded physiological neovascularization, whereas systemic anti-Scg3 hFab elicited no such side effects. Conclusions: The findings suggest that systemic anti-Scg3 hFab is a safe and effective therapy for OIR and support further development for ROP treatment.
Keywords
- retinopathy of prematurity
- oxygen-induced retinopathy
- secretogranin III
- Scg3
- pathological angiogenesis
- physiological angiogenesis
- targeted anti-angiogenic therapy
Retinopathy of prematurity (ROP) is a leading cause of vision loss in children, primarily affecting preterm infants born with extremely low gestational ages or birth weights [1]. The disease is characterized by pathological retinal neovascularization (RNV) that may progress toward retinal detachment, severe vision loss or even blindness. One of the unique features of ROP is the concurrent presence of physiological and pathological angiogenesis in the developing retina [2, 3]. The disease is currently treated with laser therapy or cryotherapy, both of which destroy the peripheral retina to save the central vision but do not address the underlying causes of pathological RNV [4].
The advent and approval of anti-vascular endothelial growth factor (VEGF) drugs were a major breakthrough for the treatment of proliferative ocular vascular diseases, including neovascular age-related macular degeneration (AMD) and diabetic retinopathy (DR). VEGF inhibitors, such as ranibizumab, bevacizumab and aflibercept, have also been used off-label to treat ROP [5, 6, 7]. Ranibizumab was recently approved for the therapy of ROP in the European Union following positive outcomes of the randomized, multicenter RAINBOW clinical trial [8].
However, VEGF regulates both diseased and healthy vessels and is a growth and survival factor for numerous cells, including healthy endothelial cells and neurons [9, 10]. As a result, systemic anti-VEGF therapy for cancer is known to elicit adverse side effects, including hypertension, nephrotic syndrome, thromboembolic events, bowel perforation and delayed wound healing [11, 12]. To circumvent systemic side effects, VEGF inhibitors for ocular disease therapy are all approved for intravitreal injection. However, this delivery route may also cause injection-related adverse effects, such as endophthalmitis, intraocular inflammation, rhegmatogenous retinal detachment, increased intraocular pressure and ocular hemorrhage [13]. Therefore, although systemic anti-VEGF drugs can effectively alleviate neovascular AMD, such delivery route is not approved for any ocular disease due to safety concerns [14].
We recently discovered secretogranin III (Scg3) as a disease-restricted angiogenic factor that selectively binds to and stimulates angiogenesis of diseased but not healthy vessels, whereas VEGF binds and drives angiogenesis of both diseased and healthy vessels [15]. We generated Scg3-neutralizing monoclonal antibodies (mAbs) that alleviate pathological RNV with high efficacy in oxygen-induced retinopathy (OIR) mice, a surrogate model of ROP [15, 16]. We further demonstrated that anti-Scg3 mAb injected either intravitreally or intraperitoneally (i.p.) elicits no adverse side effects, whereas the anti-VEGF drug aflibercept injected by either route adversely suppresses the normal development of retinal structure and function in neonatal mice [16]. These encouraging results provide a basis for systemic anti-Scg3 therapy.
Here we characterized the safety and efficacy of systemically delivered anti-Scg3 humanized antibody Fab fragment (hFab) in the OIR model. We found that systemic anti-Scg3 hFab effectively alleviated pathological RNV in OIR mice with minimal adverse effects on physiological angiogenesis. The results support further development of anti-Scg3 humanized antibody (hAb) for systemic ROP therapy.
C57BL/6J mice were obtained from the Jackson Laboratory. All procedures of animal studies were approved by the Institutional Animal Care and Use Committee at Baylor College of Medicine. Anti-Scg3 hFab derived from anti-Scg3 mAb was engineered by Everglades Biopharma, LLC [17, 18].
OIR mice were generated as described [15, 19]. Briefly, mice (male and female) at postnatal day 7 (P7) were exposed to 75% oxygen in a chamber for 5 days with their nursing mothers, returned to room air at P12 and analyzed at indicated time points.
OIR mice received i.p. injection of anti-Scg3 hFab, aflibercept or control hFab
at indicated doses on P14, P16 and P18. Eyes were enucleated from euthanized mice
at P19 and fixed in 4% paraformaldehyde (pH 7.4) for 45 min. Previous studies
found that pathological RNV severity at P17 and P19 has insignificant difference
[20, 21]. Therefore, we analyzed RNV at P19. Retinas were isolated, stained for
vessels with Alexa Fluor 488-conjugated isolectin B4 (AF488-IB4) (10
Healthy mice were treated with aflibercept, anti-Scg3 hFab or PBS via i.p.
injection at P1, P3 and P5. Eyes were enucleated from euthanized mice at P6.
Retinas were isolated, stained with AF488-IB4, flat-mounted and analyzed using
the SIM, as described above. Additionally, aflibercept, anti-hFab or PBS was
injected into healthy mice at P2, P4, P6, P8 and P10, and eyes were enucleated at
P12 and embedded in optimal cutting temperature compound (OCT). Cryosections in
10-
Indicated therapeutic agents were injected i.p. into healthy C57BL/6J mice at
P1, P3, P5, P7, P9 and P11. Body weight was monitored from P1 to P12. Kidneys
were isolated at P12, fixed in 4% paraformaldehyde overnight at 4 ℃ and embedded
in paraffin for H&E staining or OCT for immunostaiing. Cryosections in
10-
Mice were treated with aflibercept, anti-Scg3 hFab or PBS via i.p. injection, as described in the systemic toxicity section. At P12, kidneys were isolated, fixed in 3% glutaraldehyde, washed in 0.1 M sodium phosphate buffer (pH 7.3), re-fixed in 1% osmium tetroxide and dehydrated in a series of graded ethanol solutions to a final 100% ethanol. Eyes were infiltrated (harden) with acetone and Poly/Bed® 812 plastic resin, embedded in plastic block molds with 100% Poly/Bed 812. Sections (80–90 nm) cut on a Leica Ultracut R ultramicrotome were stained with uranyl acetate and lead citrate and analyzed using a Zeiss EM902 Transmission Electron Microscope. Images were captured using an AMT V602 digital camera.
Results are expressed as means
To investigate relative efficacies of systemic anti-angiogenic therapy for OIR,
mice were injected i.p. with anti-Scg3 hFab, aflibercept or control hFab (5
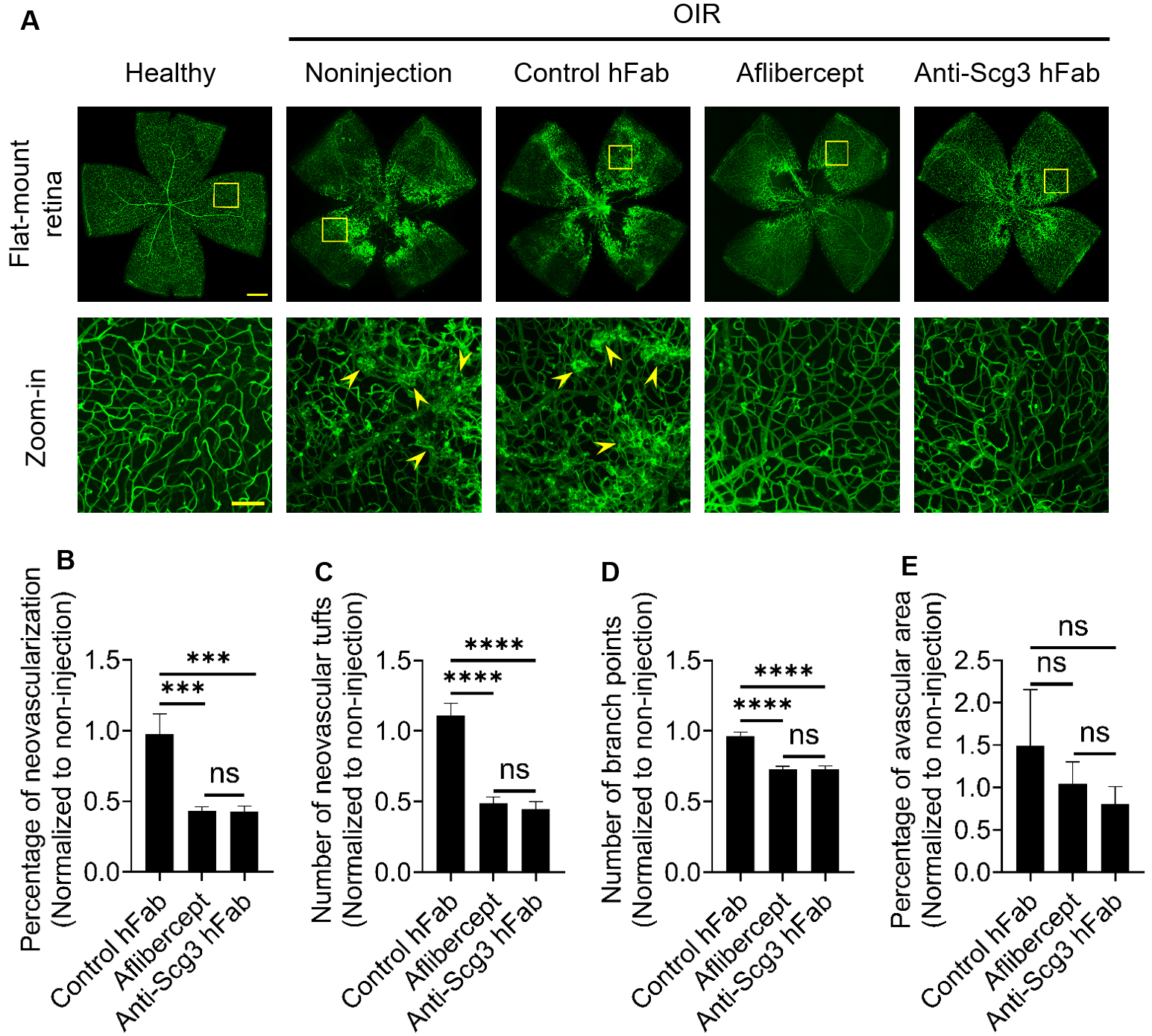 Fig. 1.
Fig. 1.Systemic therapy of OIR. Aflibercept, anti-Scg3 hFab (5
To compare the adverse effects of anti-Scg3 vs. anti-VEGF on physiological
angiogenesis of the developing retina, we injected i.p. anti-Scg3 hFab,
aflibercept (5
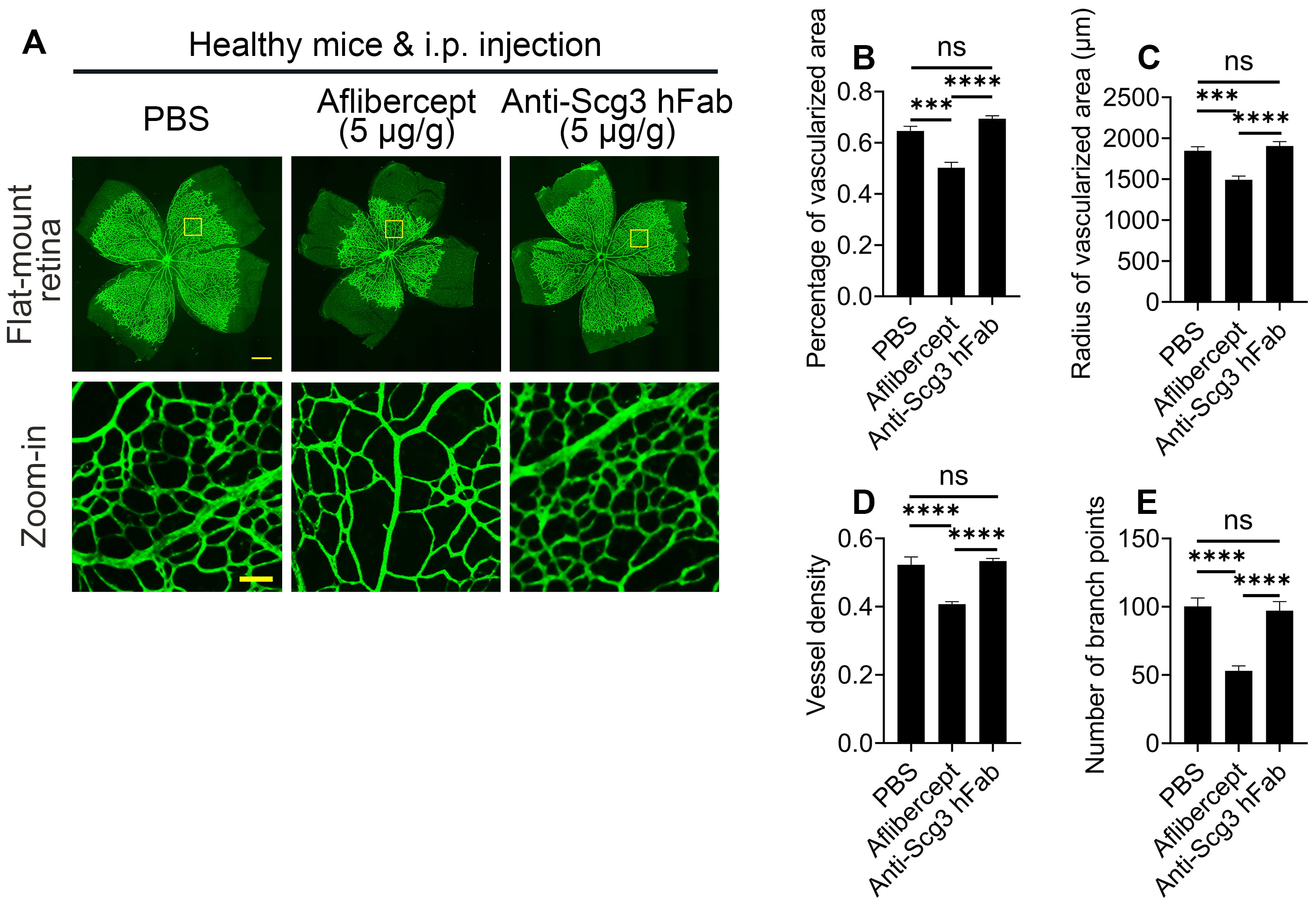 Fig. 2.
Fig. 2.Systemic aflibercept, but not anti-Scg3 hFab, suppresses
physiological retinal angiogenesis. Aflibercept, anti-Scg3 hFab (5
The retinal vasculature comprises three vascular layers, including the superficial, intermediate and deep plexuses, which are progressively and sequentially developed during P1–P12 [22]. To analyze the adverse effects of systemic anti-angiogenic therapy on the individual plexuses, we injected i.p. anti-Scg3 hFab, aflibercept, and PBS to mice at P2, P4, P6, P8 and P10. IHC analyses of retinal sections with anti-CD31 mAb at P12 indicated that systemic aflibercept significantly inhibited the development of the intermediate and deep plexuses, but not the superficial plexus (Fig. 3). By contrast, systemic anti-Scg3 hFab was without detectable adverse effects on any of the retinal vascular plexuses, consistent with the results of flat-mount retinas shown in Fig. 2.
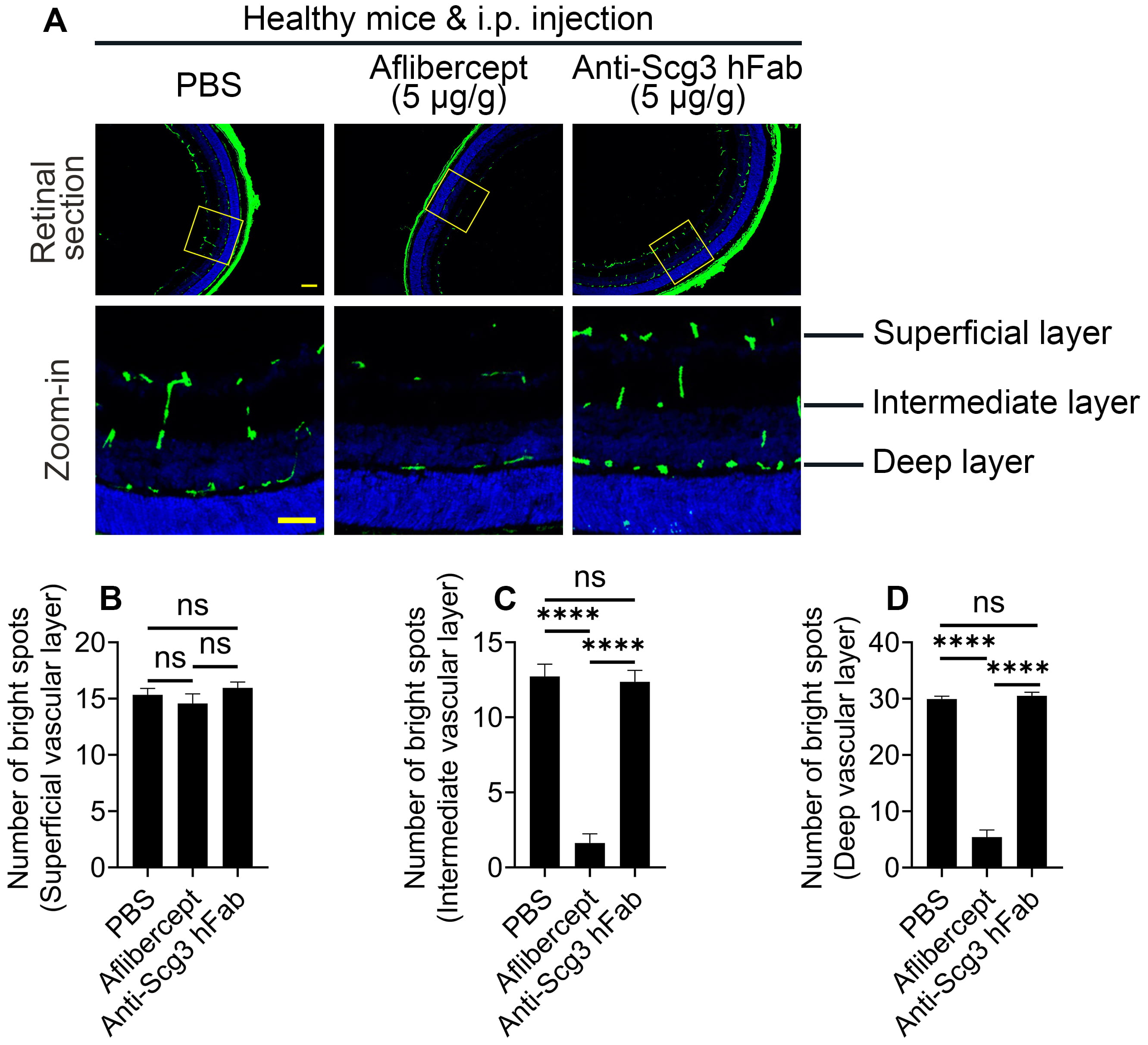 Fig. 3.
Fig. 3.Systemic aflibercept, but not anti-Scg3 hFab, inhibits
development of the intermediate and deep retinal vascular plexuses. Aflibercept,
anti-Scg3 hFab (5
The kidney is one of the most vascularized organs, and systemic bevacizumab for cancer therapy is known to cause proteinuria [12, 23]. Here, we injected i.p. aflibercept or anti-Scg3 hFab into healthy neonatal mice and compared the effects on kidney development. Histological examination revealed that aflibercept significantly reduced the number of glomeruli and increased the glomerular size (Fig. 4A, top row; Fig. 4B,C). Additionally, H&E staining detected dilation of renal tubules in aflibercept-treated mice (Fig. 4A, top panel), and quantification revealed significantly increased tubular injury score in the aflibercept group (Fig. 4D).
By IHC, we found that aflibercept significantly reduced CD31+ glomeruli and vessel density (Fig. 4A, bottom two rows; Fig. 4E,F). No adverse effects were detected in anti-Scg3 hFab-treated mice, as compared to PBS control. The results suggest that aflibercept, but not anti-Scg3 hFab, adversely inhibits physiological angiogenesis, thereby deleteriously affecting developing kidneys, consistent with our previous studies using aflibercept and anti-Scg3 mAb [16].
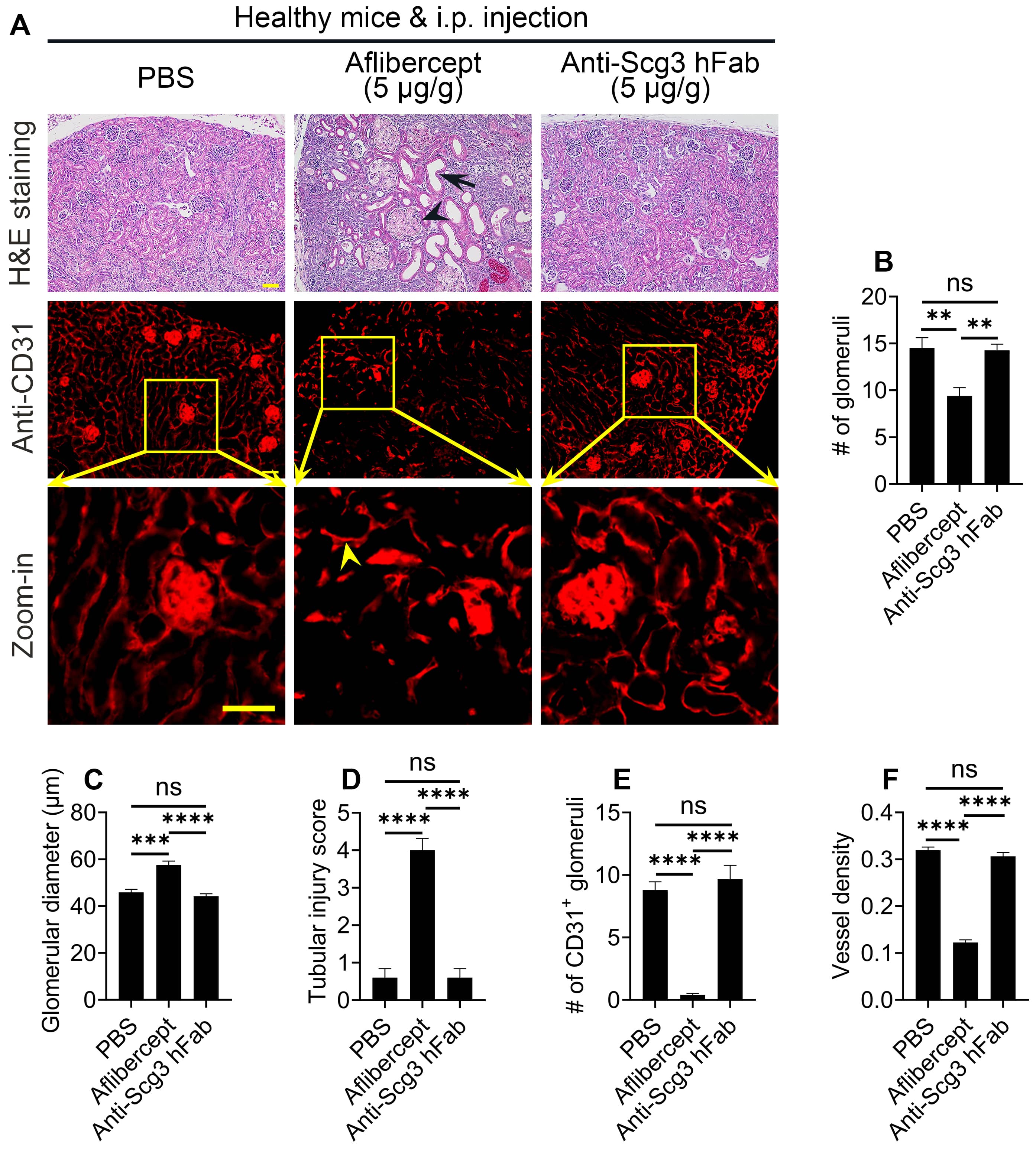 Fig. 4.
Fig. 4.Aflibercept, but not anti-Scg3 hFab, adversely affects the
structure of the developing kidney. Aflibercept, anti-Scg3 hFab (5
Electron microscopy revealed changes in kidney ultrastructure (Fig. 5). Systemic aflibercept disrupted the glomerular ultrastructure with abnormal cells (Fig. 5, top row), reduced the foot processes of podocytes (Fig. 5, middle row), and induced mitochondrial swelling (bottom row). In contrast, systemic anti-Scg3 hFab did not adversely impact the normal renal ultrastructure, compared with PBS.
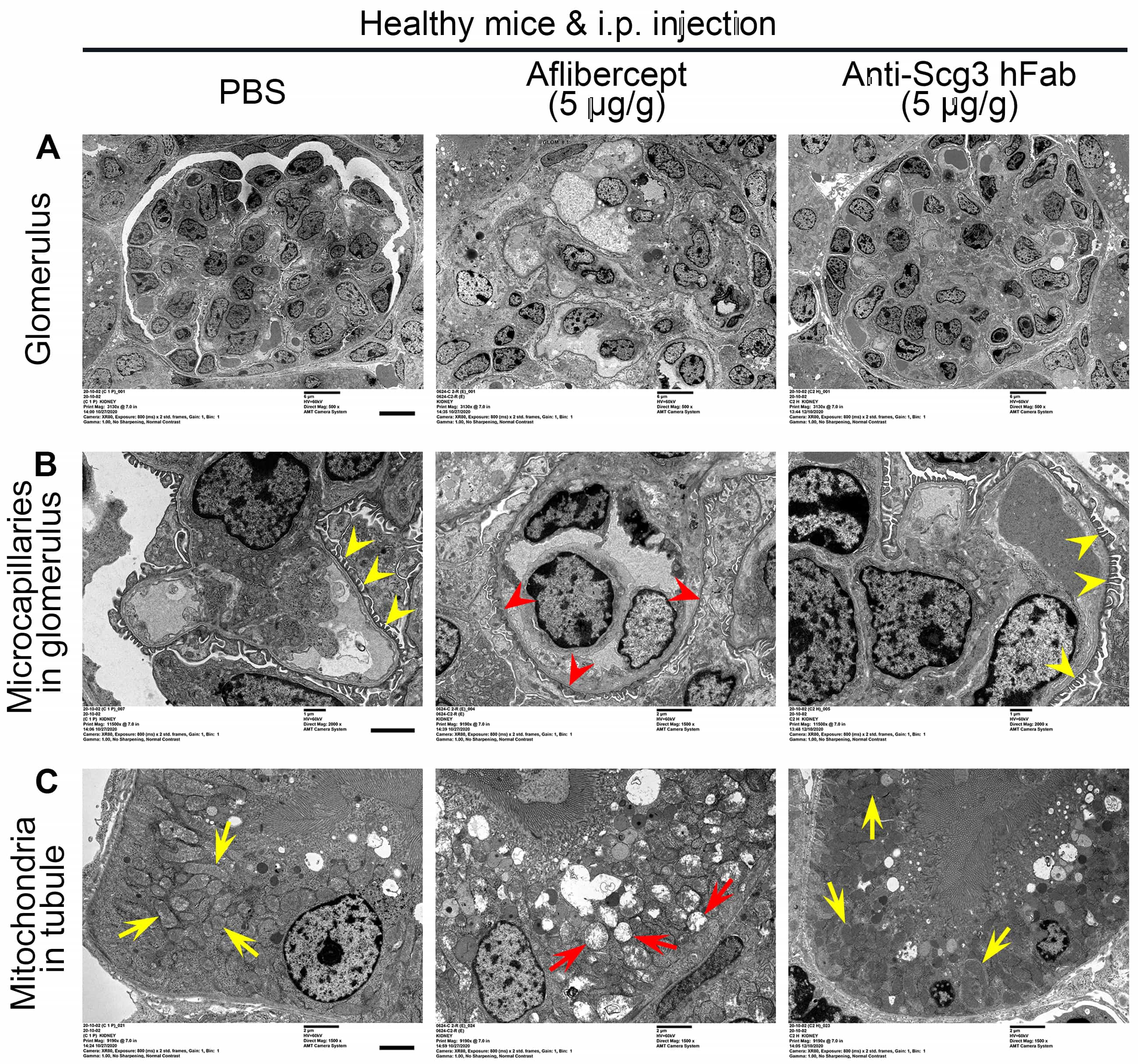 Fig. 5.
Fig. 5.Systemic aflibercept, but not anti-Scg3 hFab, adversely alters
the ultrastructure of the developing kidney. Neonatal mice were i.p. treated
with aflibercept, anti-Scg3 hFab (5
Systemic inhibition of healthy vessel development in neonatal mice may reduce
global blood supply and adversely affect organ development and body weight gain.
Here, we injected i.p. anti-Scg3 hFab, aflibercept (5
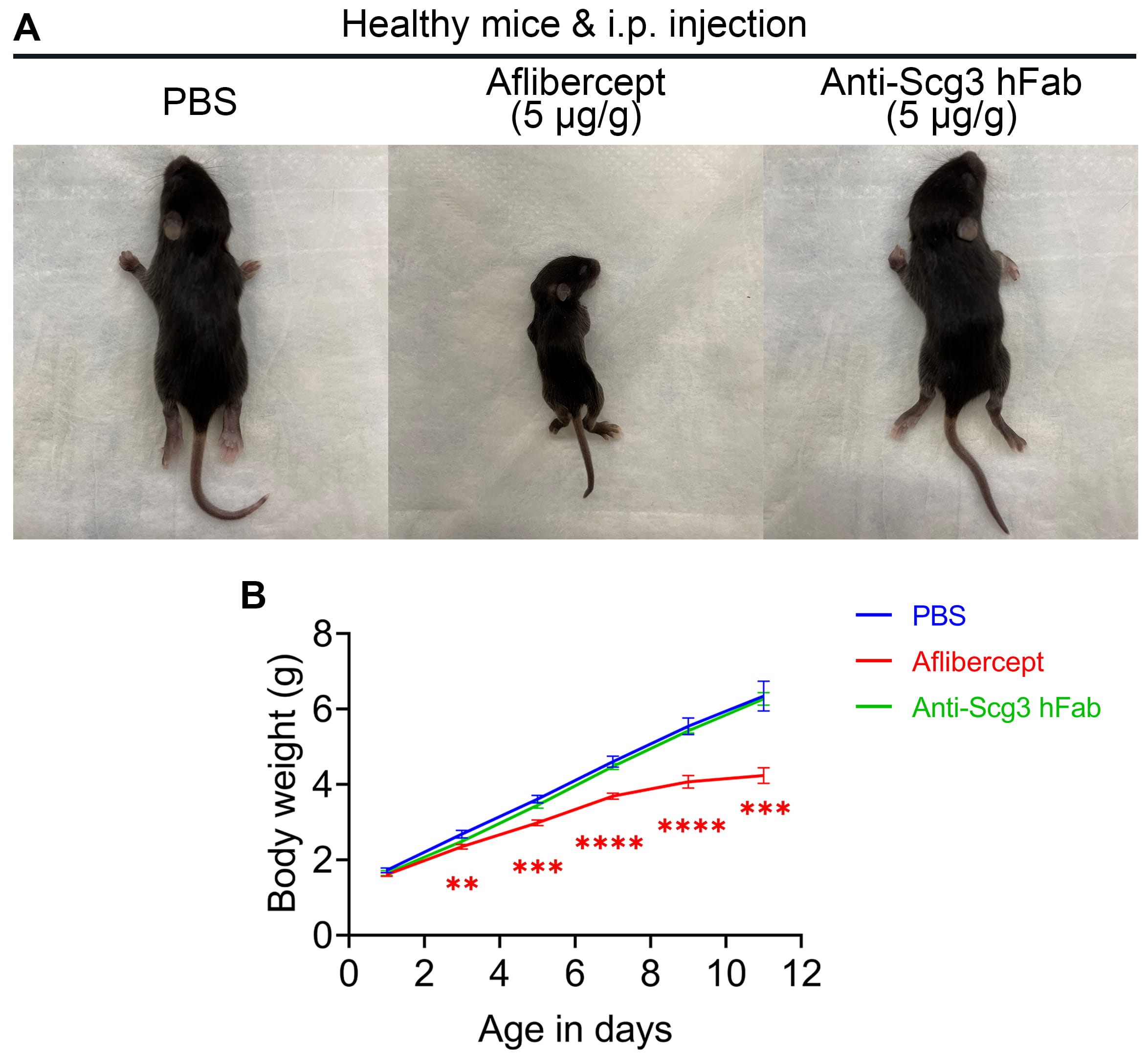 Fig. 6.
Fig. 6.Anti-Scg3 hFab does not affect body weight gain of neonatal
mice. Aflibercept, anti-Scg3 hFab (5
Two unique features of ROP, including (i) concurrent physiological and pathological angiogenesis in the developing retina and (ii) a predominant bilateral involvement [24, 25], present outstanding clinical challenges for safe and effective therapy.
Firstly, ROP occurs primarily in preterm infants whose developing retinas depend on VEGF and other angiogenic factors for physiological RNV and vascular remodeling. In contrast, other ocular neovascular diseases, such as neovascular AMD, proliferative DR, corneal neovascularization and neovascular glaucoma, occur principally in adults and the elderly, wherein mature and quiescent healthy vessels are more resistant to VEGF inhibition. Consequently, by blocking physiological angiogenesis in the developing retinas of ROP infants, anti-VEGF therapy is predicted to adversely interfere with retinal development, thereby conferring abnormalities in retinal structure and function. Indeed, intravitreal injection of aflibercept in neonatal mice and dogs was reported to inhibit retinal vessel development, alter retinal structure and reduce electroretinography (ERG) amplitudes [26, 27]. Because VEGF is a well-known growth factor for both endothelial cells and neurons [9, 10], anti-VEGF-induced abnormalities in ERG may be due to the direct inhibition of retinal neuron development, indirect adverse effects on neurons via angiogenesis inhibition or both. In ROP clinical trials, eyes treated with intravitreal bevacizumab conferred significant vascular and macular abnormalities [28, 29, 30]. Intravitreally injected bevacizumab may leak from the eye and decrease serum VEGF level [31], thereby leading to lower motor scores and higher rates of neurodevelopmental disability at 18 months of age [32, 33]. Because of these safety concerns, no drug therapy has been approved for ROP in the U.S.
Secondly, other major categories of ocular neovascular disease, including neovascular AMD, proliferative DR and neovascular glaucoma, are initially manifested as unilateral diseases, although the fellow eyes remain at elevated risks [34, 35]. In contrast, ROP is predominantly a bilateral disease [24, 25]. This is because both eyes of premature infants are simultaneously exposed to the same level of high oxygen, followed subsequently by relatively low ambient oxygen [2, 3, 4]. Whereas only the affected eye in the former categories of ocular vascular diseases requires unilateral anti-angiogenic therapy via intravitreal injection, most ROP cases require treatment of both eyes. Compared to adult eyes, ROP eyes are likely more susceptible to injection-related adverse side effects, such as retinal detachment and hemorrhage [36], due to premature connective tissues and/or extracellular matrix that hold the retina together. Therefore, systemic anti-angiogenic therapy of ROP offers to not only circumvent intravitreal injection-related side effects but also provides the benefit of simultaneously treating ROP in both eyes. Although previously investigated for wet AMD, systemic anti-VEGF therapy is not approved for any ocular disease due to severe systemic adverse side effects [11, 12]. Therefore, a challenge is to develop a safe and effective systemic anti-angiogenic therapy for ROP.
By applying an innovative technology of comparative ligandomics, we discovered Scg3 as a highly diabetes-restricted angiogenic factor that binds to and promotes angiogenesis of diabetic but not healthy vessels [15]. Subsequently, we independently verified that Scg3 selectively binds to OIR neovessels but not healthy retinal neovessels in neonatal mice, whereas VEGF binds to both OIR and healthy neovessels equally well [18]. Our results also showed that intravitreal injected anti-Scg3 hFab stringently inhibited pathological but not physiological angiogenesis in OIR mice, whereas aflibercept administered through the same route indiscriminately blocks both pathological and physiological angiogenesis with narrow therapeutic windows (Figs. 1,2,3,4), consistent with our recent findings through intravitreal injection [18].
The normal phenotypes of Scg3
Although anti-Scg3 hFab and aflibercept have similar efficacy to alleviate OIR, Scg3 and VEGF were reported with distinct receptor signaling pathways [15]. This is supported by their distinct endothelial binding activities and patterns to OIR vs. healthy retinal vessels as well as CNV vs. healthy choroidal vessels [17, 18]. Indeed, the combination of anti-Scg3 hFab and aflibercept synergistically alleviated CNV [17], likely through different mechanisms of action. The expression of Scg3, VEGF and VEGFR2 in OIR and healthy retinas has been previously reported [18, 41]. However, Scg3 receptor and its expression in the retina are yet to be described.
Despite the previously reported high efficacy of anti-Scg3 mAb to alleviate OIR [15, 16], the mouse-derived mAb cannot be used for ROP therapy in humans due to potential immunogenicity. Anti-Scg3 hFab is a humanized antibody, which is expected to have minimal immunogenicity for human use. However, relatively low immunogenicity of the hFab is yet to be confirmed in clinical trials.
We chose anti-Scg3 hFab for this study because of its small size (45 kDa), facilitated tissue penetration and potential for fewer side effects. However, one of the potential concerns is its small molecular weight of ~49 kDa with possible relatively short serum half-life. Systemic anti-Scg3 hFab therapy for OIR may also benefit from the relative short treatment time required for anti-angiogenesis, and the low immune response of the immature immune systems of ROP infants. The next step is to compare the pharmacokinetics of anti-Scg3 hFab vs. full-length hAb before choosing an appropriate antibody format for clinical therapy.
We have recently characterized the expression of Scg3 and VEGF in OIR vs. healthy retinas. Scg3 is minimally increased in the OIR retina and vitreous by Western blot or immunohistochemistry [15, 18]. VEGF is upregulated in OIR retinas [18]. Anti-Scg3 therapy has no effect on VEGF expression [18]. Previous studies reported conflicting results of VEGFR2 expression in OIR. Whereas several studies showed no upregulation of VEGFR2 in OIR retinas of mice and rats [42, 43, 44], other groups reported significant induction of the receptor in OIR retinas [41, 45]. Our in vivo ligand binding assay detected equivalent VEGF binding activities to retinal vessels in OIR and healthy mice, suggesting that VEGFR2 was unlikely upregulated in the disease condition [18].
We confirm excellent safety and efficacy profile of anti-Scg3 hFab that is consistent with our previous work on anti-Scg3 mAb therapy for OIR [15, 16]. Our results support further clinical development and testing of anti-Scg3 hFab therapy for OIR.
AF488-IB4, Alexa Fluor 488-conjugated isolectin B4; AMD, age-related macular degeneration; DR, diabetic retinopathy; hAb, humanized antibody; hFab, human or humanized antibody Fab fragment; mAb, monoclonal antibody; OIR, oxygen-induced retinopathy; RNV, retinal neovascularization; ROP, retinopathy of prematurity; Scg3, secretogranin III; VEGF, vascular endothelial growth factor.
CD designed and performed experiments and data analysis. HT provided reagents and technical support. AB, GS and KAW provided scientific advice. WL conceived the project, supervised experiments and analyzed data. CD, WL wrote and revised manuscript. KAW revised manuscript. All authors read and approved the final manuscript.
All animal procedures in this project were approved by the Institutional Animal Care and Use Committee at Baylor College of Medicine (Protocol #AN-8362).
The authors thank Yingbin Fu for scientific discussion, and Ralph Nichols for TEM at the Imaging Core Facility, Cullen Eye Institute, Baylor College of Medicine.
This work was partially supported by NIH R01EY027749 (WL), R24EY028764 (WL and KAW), R24EY028764-01A1S1 (WL and KAW), R43EY031238 (HT, KAW and WL), R43EY031643 (HT), R43EY032827 (HT and WL), R41EY027665 (WL and HT), NIH P30EY002520, Knights Templar Eye Foundation Endowment in Ophthalmology (WL) and unrestricted institutional grants from Research to Prevent Blindness (RPB) to the Department of Ophthalmology, Baylor College of Medicine.
HT and WL are shareholders of Everglades Biopharma, LLC and LigandomicsRx, LLC. WL is an inventor of issued and pending patents. The remaining authors declare no conflict of interest.