


1 Pharma Nord (UK) Ltd, NE61 2DB Morpeth, UK
2 School of Pharmacy and Biomolecular Sciences, Liverpool John Moores University, L3 3AF Liverpool, UK
†These authors contributed equally.
Academic Editor: Graham Pawelec
Abstract
Coenzyme Q10 (CoQ10) deficiency is broadly divided into two types, primary and secondary. Primary CoQ10 deficiencies are relatively rare disorders resulting from mutations in genes directly involved in the CoQ10 biosynthetic pathway, and are not a subject of this article. Secondary CoQ10 disorders are relatively common, and may occur for a variety of reasons; these include mutations in genes not directly related to the synthetic pathway, oxidative stress induced reduction of CoQ10, and the effects of pharmacological agents such as statins. CoQ10 is of key importance in cell metabolism; in addition to its role in mitochondrial oxidative phosphorylation, it is a major endogenous antioxidant, and has a role in the metabolism of sulphides, lipids and amino acids. Given its importance in cell metabolism, it is unsurprising that secondary CoQ10 deficiency has been linked with a wide range of disorders. In this article, we have reviewed evidence of secondary CoQ10 deficiency in both common and less common disorders, and highlighted those disorders in which CoQ10 supplementation has been shown to be of significant clinical benefit.
Keywords
- coenzyme Q10
- ubiquinone
- secondary deficiency
- heart failure
- kidney disease
- diabetes
- liver disease
- neurological disorders
- pulmonary disorders
- periodontal disease
Coenzyme Q10 (CoQ10) is usually described as a vitamin-like substance, although it is endogenously synthesised within most cell types. CoQ10 has a number of functions of vital importance to normal cell function; these include (i) its key role in cellular energy supply/ATP synthesis via mitochondrial oxidative phosphorylation; (ii) its role as a major endogenously synthesised lipid soluble antioxidant, protecting cellular/subcellular organelle membranes from free radical induced oxidative damage; (iii) its role in the metabolism of lysosomes, sulphides, amino acids and cholesterol; (iv) its role as an anti-inflammatory agent [1, 2]. Because of the multiplicity of roles in cell function, it is not surprising that deficiency of CoQ10 has been implicated in the pathogenesis of a wide range of disorders. CoQ10 deficiency is broadly divided into primary and secondary types [3]. Primary CoQ10 deficiency results from mutations in genes involved in the CoQ10 biosynthetic pathway. At least 10 genes are required for the biosynthesis of functional CoQ10, a mutation in any one of which can result in a deficit in CoQ10 status. Secondary coenzyme Q10 deficiency results from mutations in genes that are not directly related to the CoQ10 biosynthetic pathway, or to non-genetic factors associated with various disorders-examples of the latter category include increased oxidative stress and the use of statin type pharmaceuticals, as summarised in Fig. 1. In this article, we have reviewed both common and less common secondary disorders in which a deficiency of CoQ10 has been identified, and highlighted those disorders in which CoQ10 supplementation has been shown to be of significant benefit; the article is specifically concerned with clinical studies, and pre-clinical studies in animal models of disease have in general not been reviewed.
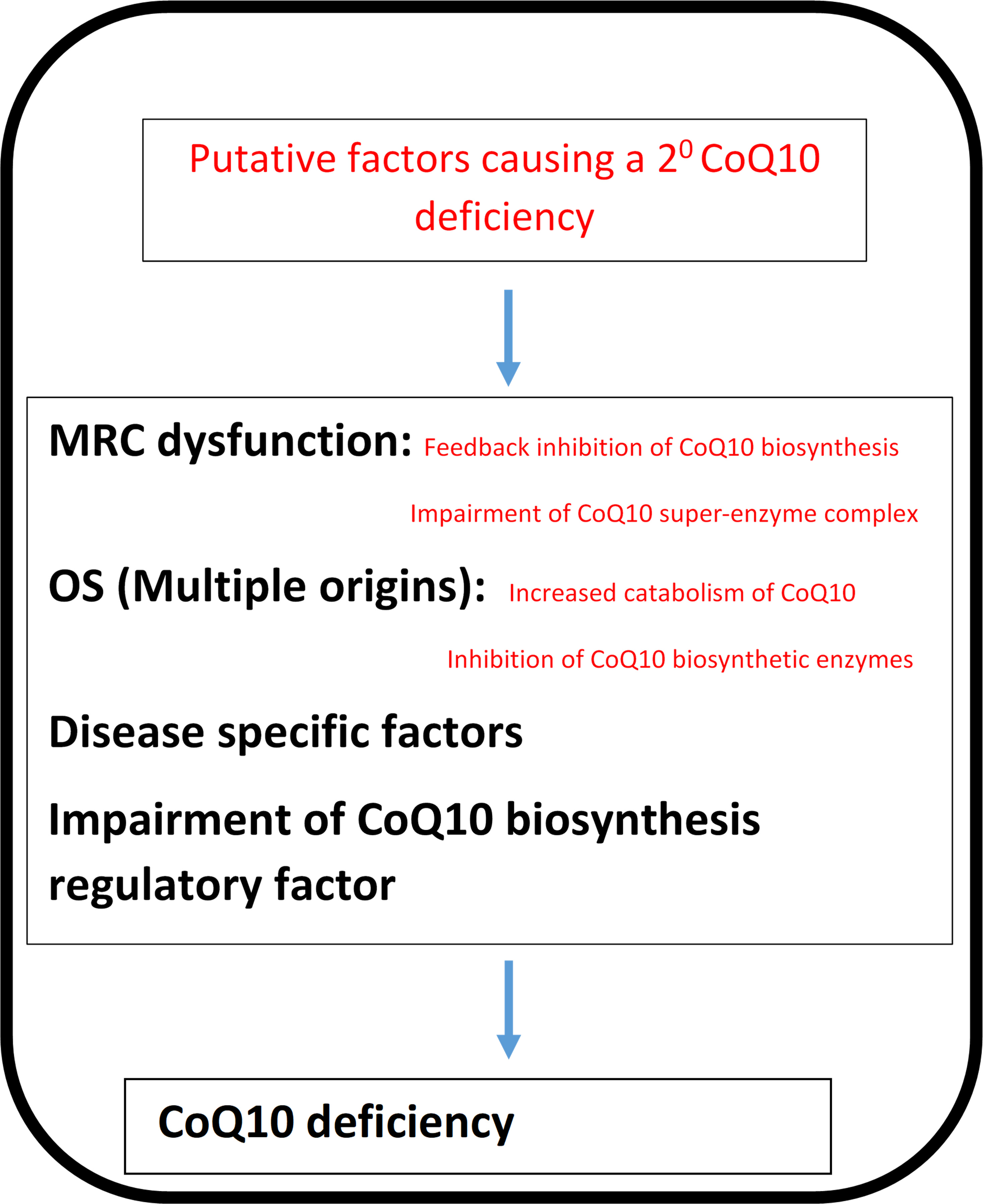 Fig. 1.
Fig. 1.The potential factors responsible for a secondary CoQ10 deficiency. COQ10, Coenzyme Q10; OS, Oxidative stress; MRC, Mitochondrial respiratory chain.
In this section of the article, we have reviewed organs/systems in which secondary deficiency of CoQ10 has been reported, including the heart, kidneys, liver and central nervous system (CNS).
The most well-known example of a secondary CoQ10 deficiency disorder is heart
failure. By definition, heart failure is a condition in which the heart is unable
to maintain circulation of the blood sufficiently to supply the requirements of
the body. Heart failure can be considered to be a condition of myocardial energy
starvation, characterised by mitochondrial dysfunction, reduced ATP production,
increased free radical generation/oxidative stress, and inflammation [4].
Depletion of both circulatory and cardiac tissue levels of CoQ10 have been
reported. Plasma levels of CoQ10 in healthy subjects have been reported to be in
the range of 0.8–1.2
Plasma CoQ10 levels have been reported to be significantly lower in chronic
kidney disease (CKD) patients (with or without haemodialysis), compared to
healthy controls [8]. CoQ10 supplementation may improve renal function and reduce
the need for dialysis in patients with CKD. In a randomised controlled study, 97
CKD patients were given supplementary CoQ10 (3
With regard to liver disease, blood CoQ10 levels are reportedly depleted in non-alcoholic fatty liver disease (NAFLD) patients, with the decrease in CoQ10 status correlating with increased liver inflammation and cirrhosis [9]. Randomised controlled trials found that supplementation with CoQ10 (100 mg/day for 1–3 months) resulted in significantly decreased systemic levels of biochemical markers of liver damage, inflammation and oxidative stress (aspartate aminotransferase, gamma-glutamyl peptidase, C-reactive protein) as reviewed by Mantle & Hargreaves [9].
Several studies have reported significantly reduced blood CoQ10 levels in type II diabetic patients, correlating with increased levels of plasma glucose, HbA1C and markers of oxidative stress. Kolahdouz Mohammadi et al. [10] reported that CoQ10 supplementation (200 mg/day for three months) significantly reduced HbA1c levels in type II diabetics. Similarly, Zahedi et al. [11] found that CoQ10 supplementation (150 mg/day for three months) significantly improved fasting plasma glucose and HbA1C levels, and Hosseinzadeh-Attar et al. [12] reported a significant improvement in HbA1c levels following supplementation with 200 mg/day for three months. The benefit of CoQ10 supplementation on glycaemic control and blood lipid levels has been confirmed in a recent meta-analysis by Zhang et al. [13].
In Parkinson’s disease (PD), a deficiency in cerebral CoQ10 status has been reported; a decrease in CoQ10 status has also been reported in both the plasma and platelets of PD patients [14]. In a phase II clinical trial conducted by Shults et al. [15], oral CoQ10 supplementation (300–1200 mg/day) was found to reduce the functional decline of patients with early-stage PD. A subsequent phase III clinical trial involving six hundred patients was undertaken with PD patients receiving CoQ10 dosages of 1200 or 2400 mg/d [16]. Despite 1200 mg/d being the highest dosage used in the previous study, the mean change in Unified Parkinson’s Disease Rating Scale (UPDRS) score of treated patients was not found to be significantly lower than that of the placebo group; the researchers concluded that since CoQ10 appeared to show no apparent clinical benefit, they could not recommend its use in the treatment of early-stage PD. The contrasting findings of the clinical studies by Shults et al. [15] and Beal et al. [16] may reflect the broad range of sporadic PD patients used in the two clinical trials, with the heterogeneous patient populations contributing to their contradictory findings. Furthermore, no assessment of an underlying CoQ10 deficiency was determined in the PD patients prior to commencing CoQ10 supplementation in the study by Beal et al. [16], which may explain the limited therapeutic potential of CoQ10 reported. In multiple sclerosis, supplementation of patients with CoQ10 (500 mg/day for 3 months) reduced blood biomarkers of oxidative stress (malondialdehyde, total antioxidant capacity), reduced pro-inflammatory cytokine levels (IL-6, TNF alpha), and improved levels of fatigue [17, 18, 19].
Fibromyalgia patients have been shown to have depleted tissue levels (typically 40–50% of normal) of CoQ10, together with increased levels of mitochondrial dysfunction, oxidative stress and inflammation, both in adults and juveniles [20, 21]. A randomised controlled clinical study by Cordero et al. [20] in 20 fibromyalgia patients found supplementation with CoQ10 (Pharma Nord Bio-Quinone, 300 mg/day for 40 days) significantly reduced (by more than 50%) pain and fatigue; there was a corresponding improvement in mitochondrial energy generation (via increased mitochondrial biogenesis), and reduced oxidative stress and inflammation. In this study, psychopathological symptoms (including depression) were also significantly improved; this was linked to the effect of supplemental CoQ10 in reducing oxidative stress and inflammation, as well as increased levels of serotonin [22, 23]. In addition, Cordero et al. [24] correlated headache symptoms with reduced CoQ10 levels and increased oxidative stress in fibromyalgia patients, with headache symptoms and oxidative stress levels significantly improved following CoQ10 supplementation (300 mg/day for 3 months). Finally, in juvenile fibromyalgia patients, Miyamae et al. [21] reported coQ10 supplementation (100 mg/day for 3 months) significantly improved fatigue.
A randomised controlled trial found supplementation with CoQ10, in combination with carnitine and omega-3 fatty acids, over a 12-month period improved visual function in patients with age related macular degeneration [25]. A randomised controlled trial of CoQ10, in combination with vitamin E (applied to the eye as an opthalmic solution, CoQun ® Visufarma SpA, Italy), in patients with open-angle glaucoma is currently in progress [26]. A randomised controlled trial in patients with dry eye syndrome found application of eye drops containing CoQ10 and hyaluronic acid daily for 3 months was effective in improving symptoms [27].
The potential benefit of CoQ10 supplementation has been investigated in a number of pulmonary disorders, including chronic obstructive pulmonary disease (COPD), COVID, influenza and asthma. There is evidence for mitochondrial dysfunction, oxidative stress and inflammation in the pathogenesis of COPD, indicating a potential therapeutic role for supplementation with CoQ10 [28]. Blood levels of CoQ10 are reportedly decreased in COPD patients [29]. There have been two randomised controlled trials supplementing CoQ10 in COPD, using doses of 50 mg/day for 8 weeks [30] and 180 mg/day for 8 weeks [31] respectively; both showed a significant improvement in respiratory function (as assessed via spirometry) following CoQ10 supplementation. Mitochondrial dysfunction has been implicated in the mechanism of COVID-19 infection [32]. In patients with COVID-19, blood platelet mitochondrial function and CoQ10 levels were significantly reduced [33]. The potential role of supplemental CoQ10 in the management of COVID-19 patients has been reviewed by Hargreaves & Mantle [34]. In patients with influenza, blood CoQ10 levels are reportedly reduced in both seasonal and pandemic (H1N1) forms [35, 36], although to date there have been no randomised controlled trials supplementing CoQ10 in influenza. Asthma is a disorder characterised by increased oxidative stress and inflammation of the airways. Blood levels of CoQ10 are reduced in asthma patients [37]. Supplementation with CoQ10 (100 mg/day for 4 weeks) improved airflow in asthmatic patients [38].
Evidence of decreased plasma concentrations of CoQ10 has been reported in patients with cancer (breast cancer, myeloma, lymphoma, and lung cancer) [39, 40]. Low plasma CoQ10 levels have been linked to an increased risk of breast cancer [41]. Jolliet et al. [42] reported decreased levels of plasma CoQ10 in both patients with breast cancer, and also in patients with nonmalignant breast disease. These results indicated that the decreased CoQ10 levels may also be responsible for benign mammary cell growth. Clinical studies supplementing CoQ10 (390 mg/day for 3 years) in cancer patients were pioneered by Dr. Karl Folkers [43, 44], in which improved patient survival was reported. Hertz & Lister [45] reported improved survival in patients with end stage cancers following supplementation with CoQ10 (300 mg/day for up to 9 years). To date there have been relatively few randomised controlled trials supplementing CoQ10 in cancer. Supplementation with CoQ10 (InnerPower ® for 21 days) was reported to benefit fatigue in breast cancer patients by Iwase et al. [46], whilst Lesser et al. [47] reported no significant benefit. The anti-angiogenic action of CoQ10 (100 mg/day for 3 months, in combination with riboflavin and niacin) in breast cancer patients undergoing tamoxifen therapy has been described by Premkumar et al. [48]. Supplementary CoQ10 has been used to protect against anthracycline induced cardiotoxicity in patients with leukemia [49].
There have been several randomised controlled clinical trials relating to CoQ10 and semen parameters in male infertility. Supplementation with CoQ10 (200–300 mg/day for 12–26 weeks) resulted in significant improvements in sperm count, morphology and motility in infertile men [50, 51, 52, 53]. Pre-treatment with CoQ10 (600 mg/day for 2 months) improved the ovarian response to stimulation and embryological parameters in young women with poor ovarian reserve in IVF-ICSI cycles [54].
CoQ10 levels in blood [55, 56, 57] and thyroid tissue [58] are reportedly reduced in hyperthyroid patients. Supplementation with CoQ10 (120 mg/day for 1 week) improved cardiac performance in hyperthyroid patients [59, 60]. Moncayo & Moncayo have described a therapeutic regime (60 mg/day ongoing) for the correction of CoQ10 deficiencies in patients with thyroid disease [61].
In a randomised controlled clinical trial, supplementation with CoQ10 (200 mg/day for 8 weeks) significantly reduced levels of inflammatory markers and disease severity, and improved quality of life in patients with mild to moderate ulcerative colitis [62, 63]. There are no studies listed on Medline relating to CoQ10 and Crohn’s disease, celiac disease, irritable bowel syndrome or gastric reflux.
A randomised controlled trial by Nachvac et al. [64] found that supplementation of rheumatoid arthritis patients with CoQ10 (100 mg/day for 2 months) resulted in a reduction in matrix metalloproteinase activity (a contributor to joint damage), reduced joint swelling and pain score, and improved clinical outcome. A randomised controlled trial reported by Abdollahzad et al. [65] found supplementation of rheumatoid arthritis patients with CoQ10 (100 mg/day for 2 months) reduced blood levels of pro-inflammatory cytokines (IL-6 and TNF alpha) and the oxidative stress marker malondialdehyde.
Periodontitis is a chronic condition in which degeneration of the supporting periodontal tissues (gingiva, periodontal ligaments, alveolar bone) ultimately results in tooth loss [66]. The initial cause of this condition is infection by various types of pathogenic Gram negative anaerobic bacteria, including Fusobacterium, Bacteroides, Porphyromonas and Prevotella species [67]. The formation of the resulting bacterial biofilm (plaque) on teeth initiates an immune response in the host, involving both the innate and adaptive immune systems [68]. Whilst some damage to the periodontal tissues results from the direct destructive action of these bacteria (via release of proteolytic enzymes), the majority of tissue damage results from over activation of the host immune system, resulting in a self-reinforcing cycle of inflammation, mitochondrial dysfunction and free radical induced oxidative stress [69]. CoQ10 is of potential relevance to periodontal disease, since it has potent anti-bacterial, antioxidant and anti-inflammatory action.
Several studies have provided evidence for a deficiency in coenzyme Q10 status in patients with periodontal disease. Thus a deficiency of CoQ10 in gingival biopsies of diseased tissue was identified, compared to biopsies taken from non-diseased areas in the same patients [70, 71, 72]. Similarly, Hansen et al. [73] found significant gingival and leukocytic deficiencies (typically 20%–60%) of coenzyme Q10 in patients with periodontal disease. In earlier supplementation studies, systemic or topical application of coenzyme Q10 in randomized placebo controlled clinical trials reported significant improvement in clinical status (e.g., pocket depth, gingival crevicular fluid flow, plaque scores) in patients with periodontal disease [74, 75]. Despite these findings, the use of supplemental CoQ10 for the treatment of periodontal disease was questioned by Watts [76].
However, a number of more recent studies have provided evidence that topical application of CoQ10 (Perio Q10 gel ® containing 10% CoQ10 in a vegetable oil base, 2 mL for 3 months) as an adjunct to scaling and root planing results in a significant improvement in periodontal disease status compared to scaling and root planning alone. In a randomised controlled trial comprising 40 patients who were smokers, topical application of CoQ10 resulted in a significant improvement in plaque index, pocket probing depth, sulcular bleeding index and clinical attachment level over a 3-month period, compared to scaling and root planning alone [77]. It is of note that smokers often respond more poorly to conventional periodontal treatment, since cigarette smoke is itself a potent source of free radicals. Similarly, a study by Shaheen et al. [78] reported topical application of CoQ10 resulted in a significant improvement in periodontal parameters compared to scaling and root planing alone. In contrast, in a study of 16 patients with periodontitis, topical application of CoQ10 significantly increased crevicular antioxidant status (quantified as superoxide dismutase), but did not significantly affect periodontal parameters (pocket depth, plaque index, gingival index) compared to scaling and root planing alone [79].
Multiple system atrophy (MSA) is an example of one of the less common neurological disorders. MSA results from progressive degeneration of neurons and glia, with subsequent dysfunction of the autonomic nervous system. The pathogenesis of MSA has been linked to the dysfunction of an enzyme (COQ2; 4-parahydroxybenzoate: polyphenyl- transferase) in the CoQ10 synthetic pathway [80]. Several studies have reported a reduction in plasma or post-mortem brain tissue. Thus, in a series of 44 MSA patients, Mitsui et al. [81] found a significant reduction in the mean plasma CoQ10 level of approximately 30% compared to controls. Barca et al. [82] found CoQ10 levels to be significantly depleted (by 40%) in post-mortem cerebellar tissue from MSA patients, compared to controls. In addition, in a study using induced pluripotent stem cell (iPSC)-derived neurons, CoQ10 levels were significantly reduced in MSA patients, particularly those with COQ2 functional variants [83]. To date, there have been no randomised controlled trials of CoQ10 in MSA.
Progressive supranuclear palsy (PSP) is a disorder resulting from tau protein aggregation in brain tissue, causing problems with balance, movement and vision. To date there have been two randomised controlled trials of supplementary CoQ10 in PSP. In the study by Stamelou et al. [84] of 20 PSP patients, supplementation with 5 mg/kg/day CoQ10 for 6 weeks resulted in improved cerebral energy metabolism assessed via magnetic resonance spectroscopy, as well as an improvement in PSP rating scale. In the study by Apetauerova et al. [85] of 60 PSP patients, supplementation with 2400 mg/day CoQ10 for up to 12 months did not significantly improve PSP symptoms or disease progression; however, the study had a high patient drop-out rate and lacked the precision to exclude a moderate benefit of CoQ10.
Hereditary ataxias (loss of coordination) can result from defects in a number of genes; these can be broadly divided into two types, resulting in primary or secondary CoQ10 deficiencies respectively. Cerebellar ataxia resulting from primary CoQ10 deficiency is a good example of a condition where CoQ10 administration can have a profound effect on clinical outcome, if supplementation is given at an early stage of disease. However, this article is concerned with secondary CoQ10 deficiencies, which in this case include Friedreich’s ataxia (resulting from defective production of the protein frataxin), ataxia telangiectasia (resulting from a defective gene involved in DNA repair), spinocerebellar ataxia (SCA, resulting from defective production of the protein ataxin). There has been one randomised double blind, variable dose clinical trial to date supplementing CoQ10 in Friedreich’s ataxia patients [86]; 50 patients were given either 600 mg CoQ10 and 2100 IU vitamin E daily, or 30 mg CoQ10 and 24 IU vitamin E daily, for a 2-year period. When compared to cross sectional data, approximately 50% of patients showed improved International Cooperative Ataxia Ratings Scale (ICARS) scores, with high and low dose treatments being equally effective. The study also identified responder and non-responder patient groups, with a low plasma CoQ10 level being the best predictor of positive clinical response to supplementation.
A clinical study of patients with SCA types 1, 2, 3 and 6 found previous administration of CoQ10 (mean 600 mg/day for 3 years) resulted in reduced Scale for Assessment and Rating of Ataxia (SARA) scores and improved clinical outcome in individuals with SCA 1 or SCA 3 [87]. In a study using cultured fibroblasts, Cornelius et al. [88] reported increased levels of oxidative stress and mitochondrial dysfunction in fibroblasts from SCA 2 patients, compared to controls; in addition, treatment with CoQ10 could partially reverse changes in these parameters in SCA 2 fibroblasts.
In lysosomes CoQ10 is thought to play an essential role in the transport of
protons across the lysosomal membrane, which is required for maintaining the
acidic pH (4.5–5) of the lumen of the organelle [89]. Proton translocation into
the lumen is linked to the activity of a tentative respiratory chain (RC), where
CoQ10 is believed to act as both an electron carrier and proton translocator
[89]. The of the lumen is essential for the activity of lysosomal enzymes, such
as those affected in San Filippo disease or mucopolysaccharidosis III (MPS III)
[90]. MPS III is an autosomal recessive disorder caused by a mutation the genes
encoding the enzymes required for the lysosomal degradation of heparin sulphate
[91]. MPS III is characterized by childhood onset of speech delay, behavioural
problems, progressive cognitive decline, loss of motor skills and epilepsy. A
study by Delgadillo et al. [92] assessed the plasma CoQ10 level in 30
patients with a range of mucopolysaccharidosis disorders, including 19 with MPS
III and found evidence of a CoQ10 deficiency in the majority of the MPS III
patients. A subsequent study by Yubero et al. [93] which assessed the
nutritional status of 9 of the original 19 patients from the former study
confirmed evidence of a plasma CoQ10 deficiency in 8 out of the 9 patients,
together with an associated loss of circulatory pyridoxal phosphate (PLP, the
active form of vitamin B6). Importantly, PLP is required for initial
transamination of tyrosine into 4-hydroxyphenylpyruvic acid in the CoQ10
biosynthetic pathway, and a study by Willis et al. [94] has indicated a
strong correlation between blood CoQ10 and vitamin B6 levels. Therefore, the
lowered circulatory level of PLP may have contributed to the plasma CoQ10
deficiency detected in the MSP III patients. Furthermore, the decreased
circulatory levels of CoQ10 in MPS III patients may be associated with
malabsorption of CoQ10 from the gut, due to increased submucosal thickening or
diarrhea, both of which are commonly associated with MPS III. In view of the
possible involvement of oxidative stress in the pathogenesis of MSP III,
increased reactive oxygen species (ROS) induced consumption of CoQ10 may
also be a contributory factor to the lowered circulatory levels of CoQ10 [95].
Decreased fibroblast CoQ10 status has also been reported in patients with MPS
III, although cellular CoQ10 biosynthesis appeared to be unimpaired [96]. This
latter result is supported by the normal levels of circulatory cholesterol
reported in MPS III patients which indicates a functioning mevalonate pathway, a
biosynthetic pathway shared by both CoQ10 and cholesterol, and therefore the
deficit in CoQ10 status reported in this disorder may be an example of secondary
CoQ10 deficiency. A recent study by Montero et al. [97] has reported
evidence of plasma CoQ10 deficiency in a range of MPS patients including MSP III.
The mechanism proposed to account for this diminution in circulatory CoQ10 levels
was the possibility that heparan sulphate or mucopolysaccharides may create
adducts with PLP, leading to a loss of vitamin B
Evidence of a CoQ10 deficiency has also been reported in the lysosomal storage
disorder Niemann Pick disease Type C (NPC), which is a neurodegenerative disease
characterised by impaired intracellular cholesterol and lipid trafficking [98].
The preponderance of cases of NPC are caused by mutations in the genes encoding
for the transmembrane lysosomal proteins NPC1 and NPC2. Although the exact
mechanisms of disease pathophysiology have yet to be elucidated, defective NPC1
and NPC2 proteins result in the accumulation of intracellular un-esterified
cholesterol and glycosphingolipids in the liver, brain and spleen of patients
[98]. Decreased CoQ10 status and biosynthetic capacity has been reported in
fibroblasts from patients with NPC. The aberrant CoQ10 synthetic capacity in this
disorder has been suggested to result from the accumulation in cholesterol which
may down regulate
Prader-Willi syndrome (PWS) is a genetic disorder of children, characterised by a variety of physical and neurological problems, in turn resulting from loss of function of genes on chromosome 15. There is some evidence that PWS is associated with mitochondrial dysfunction and reduced cellular energy metabolism [101]. Butler et al. [102] found plasma CoQ10 levels were significantly reduced in PWS patients compared to normal controls, but not when compared to obese controls. Miller et al. [103] found no significant difference in plasma CoQ10 levels between PWS patients and normal controls, although the authors questioned whether analysis of muscle biopsies, leucocytes or cultured fibroblasts may have been a more appropriate means of identifying abnormalities in CoQ10 metabolism. Eiholzer et al. [104] reported improved psychomotor development following supplementation with CoQ10 (2.5 mg/kg/day for 12 months). CoQ10 supplementation has been widely used in the management of PWS patients; of particular note is the work of Dr. William Judy of the SIBR research organisation (see http://www.cytomed.net), who has supplemented CoQ10 in more than 100 children with Prader-Willi syndrome over the course of more than 20 years. A randomised controlled cross-over clinical trial to determine the potential benefit of CoQ10 supplementation in PWS patients is currently in progress led by Dr. Ingrid Tein, Hospital for Sick Children, Toronto, Canada.
Leigh’s syndrome is a neurodegenerative disorder manifesting in early childhood,
resulting in genetic defects affecting the process of oxidative phosphorylation;
these can include dysfunction in the metabolism of pyruvate dehydrogenase or
coenzyme Q10. Chen et al. [105] described the successful treatment of a
child with Leigh’s syndrmoe resulting from the m.10197 G
Kearns-Sayre syndrome is a neuromuscular disorder resulting from mitochondrial DNA deletions; the disorder is associated with characteristic visual problems, including ptosis and corneal lesions. In a cohort of 5 Kearns-Sayre patients, CoQ10 supplementation (150 mg/day) improved abnormal metabolism of pyruvate and NADH oxidation in skeletal muscle; ECG abnormalities and neurologic symptoms also improved [111]. There have been several case studies of individual Kearns-Sayre patients whose symptoms (lactate/pyruvate metabolism, ocular movement, cardiac function) improved following supplementation (150 mg/day for up to 3 years) with CoQ10 [112]. Kim et al. [113] described improvements in corneal disease in two children with Kearns-Sayer syndrome following supplementation with CoQ10.
Down syndrome is a genetic development disorder resulting from the presence of an extra chromosome 21. There is evidence for involvement of mitochondrial dysfunction, oxidative stress and inflammation in the pathogenesis of Down syndrome; several clinical studies have demonstrated improved levels of oxidative stress/inflammation in DMD patients following supplementation with CoQ10 (10 mg/kg/day for 3 months) [114, 115, 116].
Duchenne muscular dystrophy (DMD) is an X-linked genetic disorder (resulting in the absence of dystrophin protein) manifesting in male children, characterised by progressive wasting of skeletal muscles, with death in the late teens/early twenties following involvement of the respiratory and cardiac musculature. The blood levels of CoQ10 were significantly reduced in DMD patients, in common with other forms of muscular dystrophy [117]. Several randomised controlled clinical studies have reported a significant improvement in respiratory function in DMD patients following supplementation (900 mg/day for up to 6 years) with idebenone [118].
As noted in the introduction to this article, secondary CoQ10 deficiencies can result from a variety of causes, which typically may reduce CoQ10 synthesis or increase its catabolism, as summarized in Fig. 1. In view of the central role of CoQ10 in cellular metabolism, it is unsurprising that a deficiency in endogenous CoQ10 status may be associated with a wide range of clinical presentations. In the present article we have identified a wide range of such disorders, both common and uncommon, in which secondary CoQ10 deficiencies have been reported. Whether such CoQ10 deficiencies occur as a cause or consequence of these disorders has still to be fully elucidated. However, not withstanding cause or consequence, the important issue is whether supplementation with CoQ10 can result in significant symptomatic benefit; this is particularly the case for those disorders for which conventional therapies are ineffective, or not available at all. We have therefore reviewed a similar range of disorders in which secondary CoQ10 deficiency has been corrected following oral CoQ10 supplementation, resulting in a significant improvement in clinical status, as validated in randomised controlled clinical trials.
The best documented secondary CoQ10 deficiency disorder in which CoQ10 supplementation has been shown to provide significant patient benefit is heart failure. There have been some 30 randomised controlled trials supplementing CoQ10 in heart failure, almost all of which have reported significant patient benefit [119]. The efficacy and safety of supplemental CoQ10 for treatment of heart failure have been confirmed by meta-analysis [120, 121]. Heart failure may develop as a complication of other disorders; patients with type II diabetes, non-alcoholic fatty liver disease (NAFLD) and CKD are at increased risk of developing heart failure. Supplementation with CoQ10 in patients with these disorders may therefore help to prevent heart failure; in addition, there is evidence from randomised controlled trials that supplementary CoQ10 can improve blood glucose control, liver and renal function in these disorders respectively, as noted in the relevant sections of this article.
Supplementation with CoQ10 has not been universally successful in all secondary CoQ10 deficiency disorders; the lack of benefit in some randomised controlled trials may result from a number of factors, including bioavailability, dosage of CoQ10, duration of therapy, patient selection, and unknown factors in CoQ10 metabolism may influence the efficiency of this treatment.
Supplemented CoQ10 is absorbed in the small intestine where it is fully reduced into its ubiquinol form in enterocytes before entry into the lymphatic system and release into the circulation [122]. Bioavailability is a particular problem; the bioavailability of CoQ10 is low, typically of the order of 5% at best [122]. Bioavailability is highly dependent on supplement formulation, in particular the degree of CoQ10 crystal dispersion as demonstrated in the study by Lopez-Lluch et al. [123]. Despite its limitations, there is presently no alternative method of administering CoQ10; whilst intravenous administration of CoQ10 has been described in animal models of disease, there have been no randomised controlled trials using this administration method to date. Supplementation of CoQ10 in neurological disorders such as PD has been particularly disappointing; this in turn may result from a lack of knowledge of some aspects of CoQ10 metabolism, for example whether CoQ10 can cross the blood-brain barrier in man, and how CoQ10 is subsequently transported between and within brain cells [14]. For some of the less common disorders described in this review, current treatments may lack efficacy, so patient benefit following CoQ10 supplementation is of potential importance, and worthy of further clinical investigations. Furthermore, at present there is no consensus on dosage or circulatory level of CoQ10 which may be of therapeutic value in the treatment of disease.
The assessment of CoQ10 status is well established in specialist laboratories [124]. In general, clinical assessment is based on serum/plasma determinations, with an established reference interval ranging from 0.5 to 1.7 uM. The actual reference range can vary between laboratories depending on the precise method of analysis employed. Generally, high performance liquid chromatography (HPLC) with either ultra violet (UV; at 275 nm) or electrochemical detection is used, although mass spectrographic (M) analysis is becoming more readily accessible. On the basis of the data provided in this review, we suggest that the measurement of endogenous CoQ10 status should become more of a routine assay in hospital clinical biochemistry laboratories, and that supplemental CoQ10 should be more widely utilised in clinical practice than is currently the case.
COQ10, coenzyme Q10; OS, oxidative stress; MRC, mitochondrial respiratory chain.
DM, NT and IPH wrote the manuscript and prepared the figure. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
Not applicable.
Not applicable.
This research received no external funding.
Mantle is medical adviser to Pharma Nord (UK) Ltd. Iain P. Hargreaves is serving as Guest Editor of this journal. We declare that Iain P. Hargreaves had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Graham Pawelec.