






Frontiers in Bioscience-Elite (FBE) is published by IMR Press from Volume 13 Issue 2 (2021). Previous articles were published by another publisher on a subscription basis, and they are hosted by IMR Press on imrpress.com as a courtesy and upon agreement with Frontiers in Bioscience.

1 Department of Environmental Health, College of Public Health, Imam Abdulrahman Bin Faisal University, P.O.Box 1982, Dammam 31441, Saudi Arabia
Abstract
Coronavirus disease (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a member of the human coronavirus (HCoV) family that targets the lower part of the respiratory tract and causes severe acute respiratory syndrome (SARS). In a short span of time, this infection has led to a global pandemic and has become a significant threat to the existence of present human society. Currently, there are no treatments for this infection and the measures established across various countries such as social distancing, usage of mask to prevent entry of the virus into the respiratory tract, quarantine, and containment together have reduced the prevalence of this disease and mortality in highly susceptible individuals. Here, we examine the structure, replication cycle, phylogeny and genomic organization of this virus and discuss the role of spike (S) protein of the virus, an important structure that interacts with the host ACE2 receptor facilitating viral entry. Further, we explore the epidemiology, symptoms of the disease, describe the reverse transcriptase-polymerase chain reaction (RT-PCR) that establishes the diagnosis of the disease and also review its unique diagnostic features in the chest CT-Scan. Finally, we review the current approaches to develop therapies and vaccines as a measure for disease prevention and control.
Keywords
- Coronaviruses
- COVID-19
- ACE2
- S spike protein
- SARS-CoV-2
- Pathogenesis
- Genomic Organization
- Transmission Diagnosis
- Review
An emerging infectious disease causing severe acute respiratory syndrome (SARS) was recently detected in Wuhan, China (1-3). According to the Coronavirus Study Group (CSG), the novel virus is named as SARS coronavirus 2 (SARS-CoV-2) (4) and the resulting disease as Coronavirus disease (COVID-19). Due to the COVID-19 outbreak, there is an increasing interest to comprehensively understand the phylogeny, epidemiology and pathogenesis of the virus caused by the growing concern for people’s health.
Several members of the coronavirus families cause many zoonotic diseases such as enteritis in cows, pigs, pangolins, and birds, as well as lung diseases in chicken (5-7). In the past decade, two outbreaks have been caused by beta coronaviruses, namely, SARS-CoV-1 and MERS-CoV, causing global anxiety without widespread effects (8). However, the recent disease caused by the newly identified novel coronavirus SARS-CoV-2 has been declared as a global pandemic that brings about severe acute respiratory disease (9). This pandemic has attracted a greater attention of the scientific community, health organizations, and policy makers because of the serious threat it poses to global health, social, and economic systems. The main aim of this review was to update information concerning the COVID-19 outbreak with a special emphasis on the COVID-19 genome highlighting its structure, genomic organization and its mechanism of replication. Further, the virulence of COVID -19 in humans and the role of ACE2 in its pathogenesis have been comprehensively covered. This review also intends to fill in the gaps in knowledge regarding epidemiology, methods of SARS-CoV-2 infection, diagnosis, possible therapeutics and vaccines. Finally, major challenges that hinder the measures to control or prevent viral transmission from person-to-person at the national and international levels have also been discussed.
Due to the recent COVID-19 outbreak, there has been a considerable interest in knowing the phylogeny of SARS-CoV-2 or HCoV-19 virus (10-11). Generally, coronaviruses are zoonotic viruses belonging to the order Nidovirales that includes three families, namely, Coronaviridae, Arteriviridae, and Roniviridae. Coronaviridae is subsequently divided into the following two subfamilies: Torovirinae and Coronavirinae. On the basis of serological analysis and phylogeny, members of the latter subfamily are further categorized into four groups: alpha, beta, gamma, and delta coronaviruses (4).
Seven coronaviruses are known to cause infections in humans ranging from mild to severe respiratory symptoms. Of these, four are endemic human coronaviruses HCoV-229E (alpha), HCoV-NL63 (alpha), HCoV-OC43, and HCoV-HKU1 (beta), which are responsible for mild common cold symptoms mostly in lung infections and are mostly associated with bats, rodents, cows and pigs (12). The remaining three are the most dangerous viral candidates that cause severe lower respiratory infections, such as the two epidemic-causing coronaviruses SARS-CoV and MERS-CoV, and a third novel pandemic-causing coronavirus, SARS-CoV-2, belonging to the beta coronavirus group. Remarkably, bats could be the natural reservoirs of the three human coronaviruses with palm civet, dromedary camels or pangolin acting as intermediate amplifying and transmitting host, respectively (5-6,12).
Like other human coronaviruses, the enveloped positive-sense RNA viruses such as SARS-CoV-2 is composed of approximately 30 kilobase (kb) genome (13). Organizational structure of the SARS-CoV-2 genome encompasses six open reading frames (ORFs) (Figure 1). Two-thirds of the genome contains the first translated ORF (ORF1a/b), that comprises of 16 highly conserved nonstructural polyproteins (nsps1-16), encoding the replication-transcription (RTC) complex in the double-membrane vesicles (DMVs). A group of nested single stranded RNA genome (sgRNA) sequences are synthesized by RTC in a discontinuous transcription manner due to the interception of ORFs by transcriptional regulatory sequences. The remaining one third of the genome encodes various structural proteins, responsible for nucleocapsid polymorphisms that act as an adaptive response to new hosts. This region of the genome is coded by four main ORFs to synthesize the viral structure proteins: S, M, E and N as well as other sgRNAs accessory genes (Figure 1) (6, 13-14).
 Figure 1
Figure 1Genome organization of human coronavirus COVID-19. The genome size is approximately 30 kilobase (kb). The two-third region encodes for the two main overlapping open reading frames (ORF 1a/b) encode conserved nonstructural polyproteins required for replication-transcription complex (RTC) and virus synthesis (above). The last third of the genome coded for the main structural component proteins including S, E, M and N and a set of accessory genes including ORF3a, 3b, ORF6, ORF7a, 7b, ORF8a, 8b and 9b.
Results of the genomic sequence analysis indicated that the genomic organizational structure of the SARS-CoV-2 coronavirus is highly similar to beta coronaviruses genomes. Chan et al. (15) mentioned that the genetic material of the novel coronavirus has approximately 89% and 82% identity with bat SARS-like-CoVZXC21 and human SARS-CoV, respectively. Phylogenetically, the genome sequence of the novel coronavirus that came from Wuhan city, was very close to Bat SARS-like viruses, such as SL-ZC45 and SL-ZXC21 (87.6 and 87.7%, respectively), and more distantly related to SARS and MERS (79% and 51.8%, respectively) (16). Moreover, Rothan and Byrareddy (10) revealed that the novel COVID-19 virus has approximately 80% and 50% identity to SARS and MERS of bat origin, respectively.
Interestingly, no modifications were recorded for nonstructural proteins NSP7, NSP13 and the structured and accessory proteins p6 and 8b. However, key modifications were recorded for nonstructural proteins NSP2, NSP3 and the structured spike protein underpinning subdomain, i.e., RBD (17). Indeed, Chan et al. (15) reported that this external subdomain shows 40% identity in amino acid sequences in comparison with sequences of SARS-related coronaviruses. Also, several scientists revealed that mutations in NSP2 and NSP3, as well as exposure of certain spike protein sites to selective pressure, could play a crucial role in enhancing COVID-19 infectivity, differentiation and adaption to new host (18-19). Interestingly, genome analyses of 558 SARS-CoV-2 coronaviruses indicated that the genes encoding spike proteins and nucleoproteins as well as RNA dependent (RD) RNA-polymerase and primase undergo frequent mutations that could allow better tracking of the virus epidemics (20).
On the other hand, the comparative genome analysis by Andersen et al (21) revealed that SARS-CoV-2 originated through natural selection and not from a laboratory manipulation. This could be attributed to the high affinity of SARS-CoV-2 receptor-binding domain to human ACE2 receptor protein in animal host or in human after zoonotic transfer (3, 21-22). Moreover, Tang et al. (23) revealed that the genomic variation between SARS-CoV-2 and bat SARSr-CoV (RaTG13) is only 4% and 17% at neutral sites. Likewise, changes in high affinity of the receptor-binding domain of the spike protein in SARS-CoV-2 and from pangolin virus SARSr-CoVs are mainly due to mutations and natural selection. Interestingly, the higher degree of bat ACE2 receptor homology with other animals indicates that it is an intermediate host for COVID-19 (24). Collectively, these results could be used for arguments denying the rumors about SARS-CoV-2’s use as a biological weapon. Analyses of 103 genomes of the novel virus revealed the possible existence of two types of COVID-19 coronavirus, namely, 70% L type and 30% S ancestral type (23). Moreover, human interventions might contribute to a highly select for the L type, leading to more severity and aggressiveness of COVID-19. However, more studies should be performed on the genomic and epidemiological levels to support this finding.
As previously described, coronaviruses are a unique group of spherically enveloped particles harboring a single stranded positive-sense RNA genome (+ssgRNA) along with a nucleoprotein and a protein capsid. Characteristic club-shaped glycoprotein spikes project from the virus envelop and interestingly carry the main antigenic determinants or “epitopes” recognized by the antibodies. The positive-sense RNA is characterized by the presence of 5’ terminal cap and a poly A tail structure, thus having the ability to acts as an mRNA for subsequent transcription (7, 22, 25). Similar to other human coronaviruses, the major distinctive feature of the COVID-19 viral replication is the direct translation of the upstream open reading frame (ORF) into replicase-transcriptase protein. This region comprises two-thirds of the viral genome and involves two main ORFs (ORF1a and ORFb1) and 16 other non-structural proteins. The last one-third of the genome contains four genes that code for the structural proteins including the spike, envelope, membrane and nucleocapsid (7, 25).
The life cycle of SARS-CoV-2 in humans begins with the attachment of the viral spikes to an ACE2 cellular receptor (Figure 2). Using cryo-EM, Song et al. (26) have recorded that in the prefusion conformation structure of SARS-CoV-2 spike proteins, S proteins are observed to have high affinity for the cellular receptor protein ACE2, compared to the previously reported coronaviruses. Following their entry, the viral genome is unveiled with ORF1a and ORF 1ab being translated to the two polyproteins pp1a and ab, that further undergo proteolysis by papain-like (PLpro) and chymotrypsin-like proteases to yield 16 nonstructural proteins (16 nsps). These protein elements constitute the RNA replicase-transcriptase protein complex and controls single stranded RNA genome (sgRNA) production, replication and transcription. The positive-sense RNA genome (+gRNA) is produced by replication and a set of nested 7-9 sgRNA are formed through discontinuous transcription. The sgRNAs are translated into structural and nonstructural proteins from the transcription of the first ORF close to 5’ end. Subsequently, +gRNA and nucleocapsids are assembled in the host cytosol and bud into the lumen of Endoplasmic reticulum-Golgi intermediate compartment (ERGIC). Mature viral particles are then released from the host cell via its internal membrane through exocytosis (Figure 2) (5, 13).
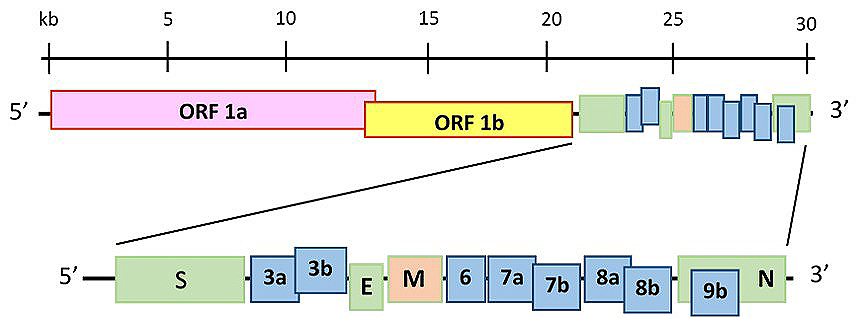 Figure 2
Figure 2Schematic diagram showing the replication cycle of SARS-CoV-2 in a host cell. SARS-CoV-2 attached to the host cell through spikes that bind to ACE2 cellular receptor. Following entry, positive-sense genomic viral RNA (+gRNA) is exposed in the cytoplasm. ORF1a and ab are translated to produce pp1a and pp1ab polyproteins, undergo proteolysis to yield 16 nonstructural proteins (16 nsps) that comprises RNA replicase-transcriptase protein complex. This complex controls -gRNA production, transcription and replication. The +gRNA is produced by replication and group of 7-9 nested sgRNA are formed by discontinuous transcription. Those sgRNAs translated into structural and nonstructural proteins from the first ORF close to 5’ end. Subsequently, +gRNA and nucleocapsids are assembled in the cytoplasm, followed by budding into ERGIC lumen. Finally, mature virus particle released from the host cell through exocytosis.
Epidemiologic studies indicated that the outbreak started from a seafood market selling live animals in Wuhan, China; subsequently transmitted to humans and further spread from person-to-person (1, 10, 22, 27). For COVID-19, the main route of human transmission occurs through respiratory tracts via droplets, respiratory secretions and direct contact (22, 28). When the infected person coughs, sneezes, or talks, he/she can transmit the disease through aerosolized droplets that can travel indoor for meters, even in minuscule quantities (29-30). Though the rate of viral transmission by the notably symptomatic diseased individual is high, the extent of the transmission is highly unreliable especially due to the location and medical interventions of the COVID-19 patient (1,31-32).
Furthermore, SARS-CoV-2 infections can also be transmitted to the major routes of viral entry such as eyes, nose, or mouth by touching previously contaminated surfaces. Epidemiology of the virus depends on several factors including viral load in upper respiratory tract and capability of asymptomatic carriers to transmit the disease (33-35). Transmission of COVID-19 by asymptomatic individuals has been reported but needs to be investigated further (28, 36-37).
A study conducted to evaluate the viral transmission caused due to the stability of the COVID-19 virus in aerosols and surfaces, reported that it was highly probable. According to van Doremalen et al. (34) the virus remains viable for at least 3 hours in aerosols and surfaces. In the same study, SARS-CoV-2 wasn’t detected after 4 hours on certain metal surfaces such as copper, whereas viable SARS-CoV-2 was detected till 24 hours on cardboard. Serological analyses have detected the viral genomic material in blood and stool specimens (9,26 24) and the probability of isolating the virus from fecal swabs and blood of COVID-19 patients indicate the existence of other means of viral transmission (38).
As the case with other coronaviruses, COVID-19 is transmitted primarily through airborne droplets to the nasal mucosa. However, the pathogenicity of this virus is highly complicated. The virus replicates specifically in cells of the ciliated epithelium (specifically the lung AT2 alveolar epithelial cells), causing severe damage and inflammation that sometimes manifests as a “cytokine storm” (5,39). High levels of plasma pro-inflammatory cytokines have been reported in many COVID-19 patients with severe respiratory syndromes (10). Unfortunately, the cell damage activates an inflammatory response, hence increased nasal secretions, local inflammation and swelling. In most cases, IL-6 production by leukocytes induces B lymphocyte differentiation, thermoregulation, bone maintenance and regulation of the central nervous system (CNS). Interestingly, as the levels of interleukin rise during COVID-19, underlying diseases such as autoimmune disorders and certain types of cancer are aggravated, thereby increasing the health risk and virus virulence in patients with such underlying conditions (39).
Several scientists have reported ACE2 to act as a host receptor in acute lung diseases and as a potential therapeutic target against COVID-19 (40-43). ACE2 expression has been reported to play a crucial role in many diseases such as myocardial disease, respiratory diseases, gastrointestinal diseases, kidney and liver damage, even provides receptor-mediated entry for SARS-CoV-2 and thereby increasing the risk of COVID-19 (42). Fang et al. (44) reported that renin-angiotensin system (RAS) is important for the cardiovascular regulatory system and helps in maintaining blood pressure homeostasis. Angiotensin II, a negative regulator of RAS, is generated by the ACE from angiotensin I in the lung blood capillaries and contributes towards the pathogenesis of many inflammatory lung diseases such as acute respiratory distress syndrome (ARDS). Recently, ACE2 was recognized as a key receptor in SARS infections, including COVID-19. Protective action of ACE2 in case of lung infections as observed in model animal with ARDS, encouraged scientists to use ACE2 as a novel treatment approach for many respiratory infections (42). On the other hand, Fang et al. (44) concluded that patients suffering from hypertension and diabetes have an increased risk for COVID-19, as they show an increased ACE2 expression in the epithelial cells of lungs and other organs including intestine, kidney, and blood vessels. This is because, the treatment for hypertension with ACE inhibitors and diabetes with angiotensin II type-I receptor blockers (ARBs) increases ACE2 expression and subsequently the risk for COVID-19 (44). Additionally, since smoking can upregulate ACE2 receptor expression, it could be a potential risk for the COVID-19 disease (45). On the contrary, Kuster et al. (46) revealed that the inhibition of the RAS might be protective toward COVID-19.
The receptor binding and membrane fusion processes of SARS-CoV-2 coronavirus are mediated by trimeric S spike glycoproteins. The gene coding for the S spike protein is organized up-stream of a signal peptide (SP) followed by the main sequence of S spike protein (Figure 3). Proteases such as trypsin and cathepsin L cleave the S protein into two major subunits, S1 and S2. The process of infection and pathogenesis has been reported to start with the recognition and binding of the S1 subunit in RBD through its receptor-binding motif (RBM), to the ACE2 receptor of the host cell. Subsequently, the viral progression and its transmembrane fusion are mediated by conformational changes in S2 subunit due to conserved fusion peptide (FP) (47-48). Xia et al. (49) were able to design an inhibitory drug that inhibits spike protein and interferes with membrane fusion.
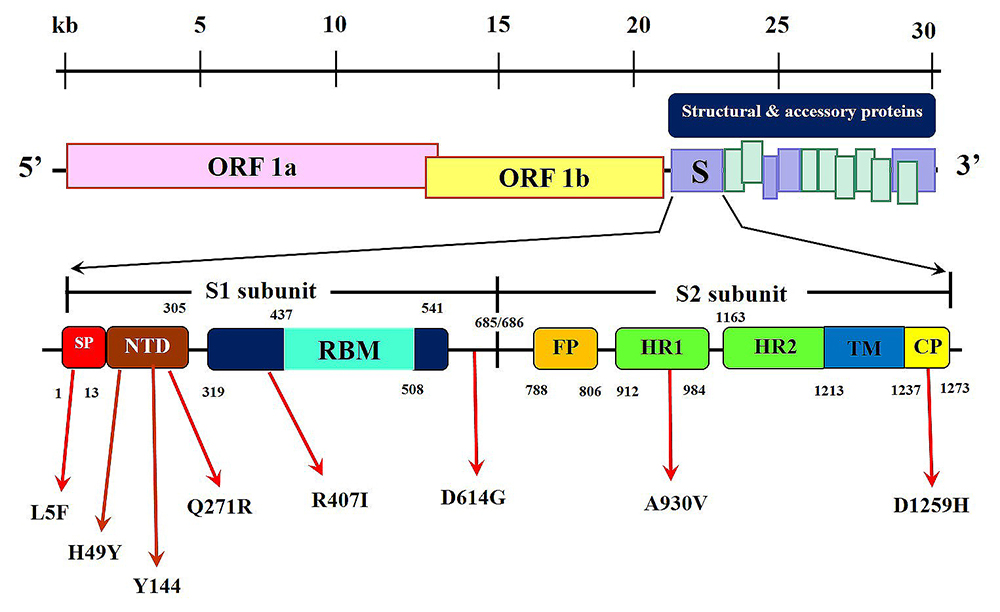 Figure 3
Figure 3Genomic organization of SARS-CoV-2 S spike protein. The upstream region coded by a signal peptide followed by two major subunits S1 and S2. S1 protein subunit contains N-terminal domain NTD), the receptor-binding domain (RBD) that incorporates the receptor-binding motif that binds specifically with ACE2 receptor protein. S2 contain a short fusion protein (FP) followed by two heptad repeats (HR1 and HR2), transmembrane domain (TM) and an intracellular cytoplasmic protein (CM). Sites of expected mutations along the S spike protein encoding genomic from different virus isolates.
Alignment studies between SARS-CoV-2 and SARS-like BatCoV-RaTG13 coronavirus, revealed a high similarity in the S protein (Figure 4) (47,50). By comparing the S protein sequence of 2019-nCoV with SARS-GZ02, Pradhan et al. (51) detected four unique insertions showing high similarity to the variable regions (V1, V4, and V5) of HIV1 envelope glycoprotein gp120 or HIV-1 Gag of certain unique strains from three different countries, namely, Thailand, Kenya, and India, supporting the speculation that 2019-nCoV is a recombinant virus. As shown in Figure 4, three of those insertions already exist in SARS-like BatCoV-RaTG13 and bears no similarity with any sequence from HIV-1. In concordance with this finding, Xiao et al. (52) demonstrated that there was no evidence that those sequences were HIV-1 specific or that the 2019-nCoV viruses obtained these insertions from HIV-1. These results collectively indicate the natural genetic variation in the S protein gene and eliminate reservations regarding SARS-CoV-2 being a synthetic virus. Only a four amino acid residue, 681PRRA684, has been recorded as a unique insert among all the known SARS-CoV-2 coronaviruses (Figure 4) (47). Together with this, the conserved R685 amino acid could be recognized as the site for proteolytic action for S1/S2 cleavage. Nevertheless, a recombinant viral construct with the SARS-CoV backbone encoding S protein from bat SHC014 has been able to demonstrate the potential to use multiple human ACE2 receptor orthologs for its entry and doesn’t respond to any neutralization vaccines, providing previously unknown insights regarding the evolution and pathogenicity of SARS-CoV-2 coronavirus (53). Interestingly, a highly conserved unique 111-fragment has been detected in all verified S proteins of human coronaviruses except MERS (data not shown), and therefore, could be possibly used as a therapeutic target while designing vaccines (50).
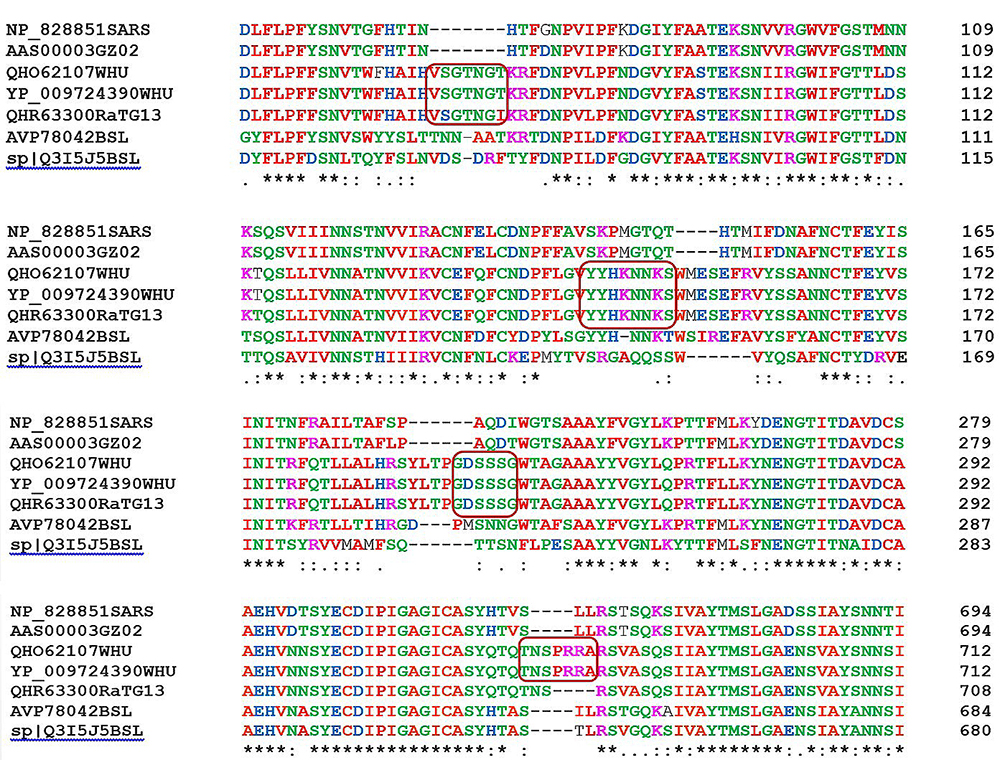 Figure 4
Figure 4Multiple amino acid sequence alignment between SARS-CoV-2 and other coronaviruses using CLUSTAL Omega online tool, EMBL-EBI UK, https://www.ebi.ac.uk/Tools/msa/clustalo/. Four unique sequences highlighted, the first showed high similarity with Bat SARS-like BaTG13.
Analyses of COVID-19 genomes from different isolates revealed several mutations up- and down-stream of the receptor binding domain (RBD) (Figure 3). These mutations have a direct influence on the secondary structure of the S1 domain and on the interaction of the S spike protein with ACE2 receptor. Several substitutions were detected during multiple alignments of various genomic sequences of spike proteins from several isolates (Figure 5). Mutations in positions Q271R and D614G, in the S1 domain of SARS-CoV-2 S spike domain were detected in isolates from many countries, with the latter being more frequent in isolates from regions such as North America, Europe and in countries like India (Table 1) (54-56). It is assumed that the D614G mutation, in which aspartic acid is changed to glycine, could lead to a conformational change in the spike protein that reduces the interaction between the S1 and S2 subunits, enabling the detachment of S1 from the viral-membrane-bound S2 (57).
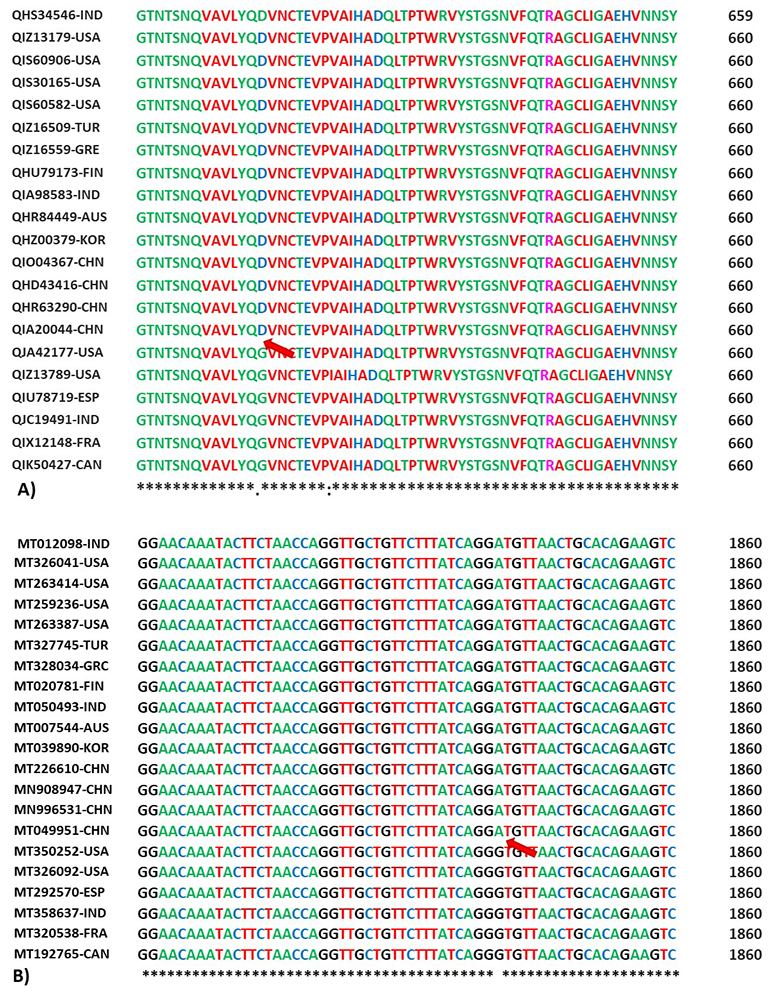 Figure 5
Figure 5Multiple sequence alignment of amino acid (A) and nucleotide (B) sequences of the S spike protein (surface glycoprotein) of SARS-CoV-2 and other coronaviruses using CLUSTAL Omega online tool, EMBL-EBI, UK, https://www.ebi.ac.uk/Tools/msa/clustalo/. S spike protein sequences accession numbers from GenBank, NIH, USA. Alpha-3 country code: according to ISO 3166 international standard. The red arrow reveals the position of the most frequent D614G substitution in amino acids and nucleotide sequences of the spike protein gene in different isolates from North America, Europe and India.
| Accession Number/ Country | Type of amino acid mutation (substitutions or deletions) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| L5F1 | Y28N | H49Y1 | S71F | N74K | Y1441 | I197V | S221W | S247R | Q271R1 | R407I1 | K574X | D614G1 | V621I | V772I | A930V1 | V1064L | D1259H1 | |
| QHS34546-IND | L | Y | H | S | N | -3 | I | S | S | Q | I2 | K | D | V | V | A | V | D |
| QIZ13179-USA | L | Y | H | F2 | N | Y | I | S | S | Q | R | K | D | V | V | A | V | D |
| QIS60906-USA | F2 | Y | H | S | N | Y | I | S | S | Q | R | K | D | V | V | A | V | D |
| QIS30165-USA | L | Y | H | S | N | Y | I | S | S | Q | R | K | D | V | V | A | V | D |
| QIS60582-USA | L | Y | H | S | N | Y | I | S | S | Q | R | K | D | V | V | A | V | H2 |
| QIZ16509-TUR | L | Y | H | S | N | Y | I | S | S | Q | R | K | D | V | I2 | A | V | D |
| QIZ16559-GRC | L | Y | H | S | N | Y | V2 | S | S | Q | R | K | D | V | V | A | V | D |
| QHU79173-FIN | L | Y | Y2 | S | N | Y | I | S | S | Q | R | K | D | V | V | A | V | D |
| QIA98583-IND | L | Y | H | S | N | Y | I | S | S | Q | R | K | D | V | V | V2 | V | D |
| QHR84449-AUS | L | Y | H | S | N | Y | I | S | S | Q | R | K | D | V | V | A | V | D |
| QHZ00379-KOR | L | Y | H | S | N | Y | I | W2 | R | Q | R | K | D | V | V | A | V | D |
| 0QIO04367-CHN | L | Y | H | S | K2 | Y | I | S | S | Q | R | K | D | V | V | A | V | D |
| QHD43416-CHN | L | Y | H | S | N | Y | I | S | S | Q | R | K | D | V | V | A | V | D |
| QHR63290-CHN | L | N2 | H | S | N | Y | I | S | S | Q | R | K | D | V | V | A | V | D |
| QIA20044-CHN | L | Y | H | S | N | Y | I | S | S | Q | R | K | D | V | V | A | V | D |
| QJA42177-USA | L | Y | H | S | N | Y | I | S | S | Q | R | K | G2 | V | V | A | L2 | D |
| QIZ13789-USA | L | Y | H | S | N | Y | I | S | S | Q | R | K | G2 | I2 | V | A | V | D |
| QIU78719-ESP | L | Y | H | S | N | Y | I | S | S | Q | R | X2 | G2 | V | V | A | V | D |
| QJC19491-IND | L | Y | H | S | N | Y | I | S | S | R2 | R | K | G2 | V | V | A | V | D |
| QIX12148-FRA | L | Y | H | S | N | Y | I | S | S | Q | R | K | G2 | V | V | A | V | D |
| QIK50427-CAN | L | Y | H | S | N | Y | I | S | S | Q | R | K | G2 | V | V | A | V | D |
COVID-19, caused by a member of the coronaviruses, shares common symptoms with other beta coronavirus infections. The major symptoms of this disease include fever, dry cough, fatigue, and mostly appear after approximately 5-6 days after contracting the disease (1,58-59). Cascella et al. (39) reported that a fever with cough as well as rhonchi or coarse breathing sounds coming from lungs were the main signs of severe COVID-19. Phlegm production, headache, hemoptysis, diarrhea, dyspnea, and lymphocytopenia could also be observed (1,60). Rothana and Byrareddy (10) reported diarrhea to be a major gastrointestinal symptom developed in COVID-19 patients. However, fluctuations in the incidence of gastrointestinal symptoms have also been recorded (61). Development of various diagnostic methods, to detect the virus transmitted through several means, is urgently required to minimize the viral transmission. Also, a comprehensive epidemiological investigation together with modern diagnostic methods could help in the early detection of asymptomatic carriers (37).
There is an accelerated effort to develop diagnostic methods to use for the detection of SARS-CoV-2. Several scientists have worked on designing primers for the molecular detection of the virus, just by utilizing the COVID-19 genomic data published in open access databases. Due to the close relation between SARS coronavirus and 2019-nCoV, it has been possible to design probes to detect the recent virus (62). Colson et al. (63) described the timeline for COVID-19 virus detection by an ultra-rapid diagnostic molecular method (RT-PCR) in 3 hours, complete genome sequencing in 11 hours and culture isolation in 72 hours. As with other acute respiratory infections, RT-PCR is recorded as the most efficient method of virus detection, specifically in secretions. A wide number of scientists have hastened the process of designing RT-PCR based tests that use specific probes to detect the virus. To understand the efficacy of these diagnostic kits, molecular diagnosis of the novel SARS-CoV-2 was carried out in 19 patients using three different fluorescent RT-PCR kits. While the virus was detectable in 47.4% of patients’ oropharyngeal samples, 90% had the virus in their stools and none in their blood and urine samples. Unfortunately, since 52.6% of the patients were undiagnosed by these molecular detection kits, other diagnostic methods like, Chest CT scan should be used for virus detection (64).
Since COVID-19 mainly attacks the lower respiratory system, this can be visualized by CT chest scan to further confirm the disease. The most common symptoms of coronaviruses that can be detected on the chest CT scans are mutual-sided ground-glass opacities (19 16, 58-59). In fact, the chest CT scans of some COVID-19 patients show the occurrence of grand-glass opacities in their lungs (65-66). Indeed, several marginal ground-glass opacities were observed in the subpleural regions of lungs bilaterally with an increased inflammation and no improvement even with interferon inhalation. In most cases dyspnea with hypoxemia has been associated with deep infiltration in the superior sections of the lung (67).
Usually, the chest CT scan for the diagnosis of confirmed COVID-19 patients revealed ground-glass opacities accompanied by deprived consolidative bilateral deviations, coinciding with viral pneumonia (68-69). As compared to RT-PCR, the chest CT scan shows a high sensitivity towards SARS-CoV-2 diagnosis (70). This comparative diagnostic study showed that amongst all COVID-19 patients, 59% have been recorded as RT-PCR-positive, while 88% were chest CT scan-positive. In fact, the sensitivity of the chest CT scan in diagnosis of SARS-CoV-2 was 97% based on positive RT-PCR. Among the negative RT-PCR patients, 75% recorded positive results in CT scan. In conclusion, the chest CT scan is recommended as a more practical approach for diagnosing COVID-19 early due to its better sensitivity, consistency, and reliability.
Finding a vaccine for the coronavirus has become a public health priority. Simultaneously, there is also a progressive increase in research led by several pharmaceutical companies to design a suitable drug and find new vaccines for COVID-19. The discovery of new vaccines is an overwhelming process and takes a very long time for their approval. Due to the surge in number of SARS-CoV-2-infected patients and the consequent public health emergency, there is an urgent need to identify proper treatment options for appropriate administration. Due to the lack of specific drugs or vaccines against SARS-CoV-2 infection, treatment of symptoms and offering respiratory support are the most available options in terms of medical intervention (14). Most of the current efforts targeting research and development of a new drug depend on the strong similarity between SARS-CoV and SARS-CoV-2 specifically in viral entry, replication and genomic organization. Liu et al. (71) has highlighted the major therapeutics and vaccines that have been already approved or under investigation for COVID-19 treatment.
Many antiviral drugs used for influenza and certain inhibitors are commonly recommended for therapeutic use against COVID-19 (10). Adenosine nucleotide analogue Remdesivir, with a broad antiviral activity against RNA viruses, and chloroquine, commonly used in the treatment of malaria, showed great activity against SARS-CoV-2 infection (14 21). Similar strategies have been used to deal with other coronavirus infections that cause severe acute respiratory diseases like SARS and MERS (72). Moreover, protease inhibitors such as Lopinavir/Ritonavir, commonly used in HIV treatment, demonstrated to have a potential against SARS-CoV and MERS-CoV, and hence, these could also be used for COVID-19 treatment (73-75). These drugs together with aerosol inhalation of interferon-alpha have been used for treating the disease symptoms to clinically manage the COVID-19 patients (58). Other broad-spectrum antiviral drugs include, Neuraminidase inhibitors, peptide (EK1), RNA synthesis inhibitors, such as, Nitazoxanide, Favipiravir, Nafamostat have also been recommended (14,72) (Table 2). The transfer of plasma from convalescent COVID-19 patients (supposed to contain antibodies against COVID-19), is an endorsed COVID-19 treatment measure that has been used to suppress the disease in its early stages (76). Through the identification of the first viral genome and molecular modelling, the drug Baricitinib has been identified, and is predicted to interrupt the viral entry and assembly in the lung cells (74) (Table 2). Finally, discovering suitable therapeutics and vaccines require a larger allocation of funds and more importantly a significant interest in reestablishing the general health of the public to overcome the COVID-19 outbreak.
| Drug | Description/Mode of Action | Reference Disease or Target | Reference(s) |
|---|---|---|---|
| Chloroquine |
9-aminoquinolin, elevates endosomal pH, immunomodulator, autophagic blocker | Malaria, autoimmune disease | 39,82,83,84 |
| Remdesivir (GS-5734) | Nucleotide analogue product, inhibitor of RNA polymerase Interfere with viral entry | With activity against Ebola and other RNA viruses | 39, 85, 86, 87 |
| lopinavir/ritonavir | Protease inhibitor, block HIV-1 protease action leading to viral immaturity | AIDS, SARS, MERS | 39, 88, 89 |
| Ribavirin | Synthetic guanosine nucleoside, interfering with the synthesis of viral mRNA | HCV, SARS, MERS | 87, 90 |
| Tolicizumab | Immunotherapy, humanized IgG1 moAB against the IL-6 receptor | Treatment of rheumatoid arthritis | 39 |
| Arbidol | Angiotensin-converting enzyme 2 (ACE 2), viral receptor protein that binds to viral S protein | Influenza virus, SARS-CoV-2 | 22, 91 |
| Camostat mesylate | Host-cell mediated Serine 2 Transmembrane protease, facilitate binding to ACE2 and intervening with replication process | SARS-CoV-2 and other HCoVs | 71 |
| Favipiravir | Nucleoside analogue, acts as RNA polymerase inhibitor (RdRp inhibitor), preventing viral reproduction | Ebola, influenza A(H1N1) |
22, 87 |
| Nafamostat | Synthetic serine protease inhibitor, blocks membrane fusion by reducing the release of cathepsin B; anticoagulant activities | Influenza, MERS, Ebola | 87, 92, 93 |
| Shufeng Jiedu Capsule (SFJDC, a traditional Chinese medicine) | Anitviral compounds from plants, blocks viral 3CL protease and inhibits RdRp activity | Active against human viruses including SARS, influenza, and HCoVs | 22, 84 |
| Nitazoxanide | Antiprotozoal agent, modulating biological activities and replication of various microbes | Human and animal coronaviruses | 87 |
| convalescent plasma | convalescent plasma containing neutralizing antibody | antibodies against COVID-19 | 80 |
| Baricitinib | inhibition of clathrin-mediated endocytosis, interrupt virus entry and assembly processes in lung cells | COVID-19 | 78, 94 |
Currently, most countries have been observed to direct their efforts in controlling the COVID-19 outbreak through strict protective measures that enable reduction of the viral spread (Figure 6). At an individual level, considerable measures must be taken to restrict person-to-person transmission of the virus (1). Some of the more efficient non-therapeutic interventions to prevent COVID-19 spread in society are maintaining hand hygiene, social distancing and quarantining, all of which could reduce the number of secondary infections (77). However, the usage of masks to reduce viral transmission remains controversial (78). The impact of non-pharmaceutical interventions to prevent viral transmission was investigated using mathematical models. These models highlighted the crucial importance of traditional public health outbreak responses such as social distancing, contact-tracing, quarantine, and face masks in determining the future of the COVID-19 pandemic (79). If such measures were proven to be inefficient, “community-wide containment’ is recommended to control the further spread of COVID-19 (80).
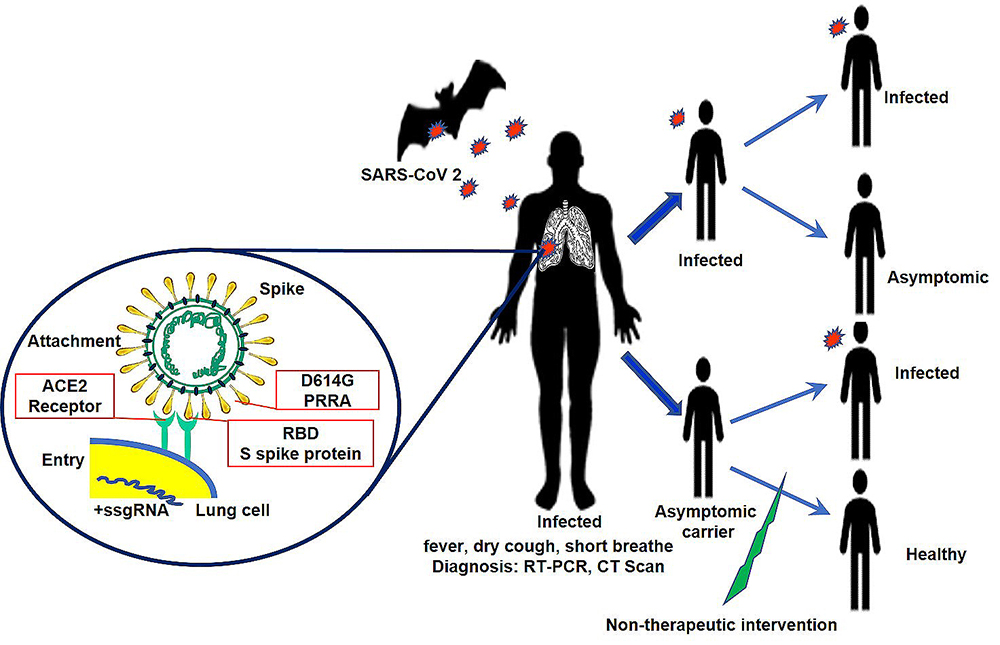 Figure 6
Figure 6Pathogenesis, symptomatology, diagnostic and non-therapeutic intervesions of COVID-19.
Besides hand washing and social distancing, efforts should be made to get rid of virus laden air droplets especially indoors by allowing proper ventilation (30). Also, priority must be given to the most vulnerable candidates including elderly people, patients with cardiovascular diseases, hypertension and diabetes due to their weak immune system (10). Apart from the practical guidelines provided by the world health organization (WHO) for risk assessment of COVID-19 outbreaks, public should be routinely reminded and encouraged to use hand sanitizers and disinfectants. More importantly, physical contact with contaminated materials like feces and urine should be avoided (31). Some of the major challenges include tracing the suspected cases and determining the severity of cases among those tested positive without obvious clinical signs of the disease and more specifically the ability of asymptomatic carriers for disease transmission (33,35-36). Along with the WHO technical guidelines regarding mass gatherings, special attention should be given to points of entry based on the susceptibility to COVID-19 outbreak. The impact of international air travel in dissemination of COVID-19 has been reported by Bogoch et al. (81) during the early stages of the outbreak. Therefore, the most characteristic action taken by nearly all countries is to halt transport and travel and enforce strict quarantine measures in all aspects of community living.
Nowadays, there is an excessive anxiety about the global preparedness in facing international challenges to respond effectively in curtailing the COVID-19 outbreak. The major points of contention exposed by the SARS-CoV-2 outbreak include communities’ response; political, structural, institutional, and environmental preparedness; and scientific and technical readiness required to address the SARS-CoV-2 pathogen-related issues. With respect to the international level, the most overwhelming effect would be on the low-income or poor countries, countries with weak health care systems, and even those that endure conflicts. The situation in such countries would be highly critical due to the inherent difficulties they face for viral detection and containment. Therefore, to bridge this, there is a concerted effort by several countries to discover effective diagnostic drugs and vaccines to overcome this public health outbreak.
This work was funded by the Deanship of Scientific Research, Imam Abdulrahman Bin Faisal University, Eastern Province, Saudi Arabia (Grant application No. Covid19-2020-017-CPH).
SARS-CoV
Severe Acute Respiratory Syndrome Coronavirus
Middle East Respiratory Syndrome Coronavirus
coronavirus disease-19, a disease caused by SARS-CoV-2
human coronavirus
angiotensin-converting enzyme 2
endoplasmic reticulum-Golgi intermediate compartment
replication-transcription complex
double-membrane vesicles
spike
membrane
envelope
nucleocapsid
interleukin 6
negative-sense genomic RNAs
subgenomic RNA
positive-sense genomic RNA
receptor-binding domain
receptor-binding motif
acute respiratory distress syndrome
Influenza A virus “swine flu”, hemagglutinin Type 1 and Neuraminidase Type 1
Acquired Immune Deficiency Syndrome
Human Immunodeficiency virus