








 , Rong Zhu 1, Yue Jin 1
, Rong Zhu 1, Yue Jin 11 Department of Obstetrics and Gynecology, The First Affiliated Hospital, College of Medicine, Zhejiang University, 310006 Hangzhou, Zhejiang, China
Abstract
To construct and compare the predictive efficacy of the random forest (RF) model and gradient boosting machine (GBM) model for long-term recurrence of endometriosis (EMs) treated by laparoscopy combined with gonadotropin releasing hormone agonist (GnRHa).
A total of 254 patients with EMs who underwent laparoscopy combined with GnRHa in The First Affiliated Hospital, College of Medicine, Zhejiang University from July 2022 to December 2023 were retrospectively collected. All patients were followed up for 1 year, and the long-term number of recurrences was recorded. The corresponding influencing factors were obtained by single factor analysis, and the risk prediction model of the long-term recurrence of sub-EMs was constructed based on RF and GBM models. At the same time, the receiver operating characteristic (ROC) curve and calibration were used to compare the predictive value of the model constructed by the two algorithm models for long-term recurrence of EMs.
Univariate analysis showed that the course of disease, preoperative dysmenorrhea history, preoperative uterine cavity operation history, tender posterior fornix and revised American Fertility Society (r-AFS) stage were the influencing factors of postoperative recurrence in patients with EMs treated by laparoscopy combined with GnRHa (p < 0.05). Based on univariate analysis, RF and GBM models were constructed. The order of importance of the predictors of laparoscopy combined with GnRHa in the treatment of EMs was r-AFS staging, course of disease, tender posterior fornix, history of intrauterine operations and history of preoperative contraception. The ROC curve results of the RF model showed that the area under curve (AUC) of the model in the training set was 0.902 (95% CI: 0.857–0.947), and the sensitivity and specificity were 100.00% and 63.50%, respectively. The AUC in the validation set was 0.859 (95% CI: 0.741–0.976), and the sensitivity and specificity were 69.20% and 92.90%, respectively. The results of the ROC curve of the GBM model showed that the AUC of the GBM model in the training set was 0.851 (95% CI: 0.781–0.920), and the sensitivity and specificity were 89.20% and 68.20%, respectively. The AUC in the validation set was 0.852 (95% CI: 0.713–0.990), and the sensitivity and specificity were 76.90% and 87.50%, respectively. The calibration curve shows that the prediction probabilities of the RF model and the GBM model are highly consistent with the actual prediction in both the training set and the validation set. The results of Delong test showed that the training set AUC of RF model was better than that of GBM model, and the difference was statistically significant (Z = 2.838, p = 0.005). There was no significant difference in the validation set AUC between the RF model and the GBM model (Z = –0.239, p = 0.811).
r-AFS staging, course of disease, tender posterior fornix, history of intrauterine operations and history of preoperative laparoscopy are the influencing factors in the long-term recurrence of EMs treated by laparoscopy combined with GnRHa. RF and GBM models can effectively predict the recurrence of such patients after treatment.
Keywords
- laparoscopy
- gonadotropin-releasing hormone agonist
- endometriosis
- recurrence
Endometriosis (EMs) is a common gynecological and hormone-dependent disease [1, 2]. It is estimated that 25%–50% of infertility patients have EMs, and 30% to 50% of EMs patients have difficulty in conception [3, 4]. In addition, EMs is also one of the most important causes of female infertility, which has brought a burden to many families who are eager to give birth [5, 6]. The typical features of EMs is the abnormal growth of endometrial tissue outside the uterus, such as pelvic organs, peritoneum, and even distant organs. This abnormal growth can cause a series of symptoms that seriously affect the quality of life of patients, among which chronic pelvic pain is the most common, and some patients have severe pain, which seriously interferes with daily activities [7, 8].
With the progress of modern medical technology, laparoscopic surgery has become the mainstream method for the treatment of EMs due to its significant advantages such as small trauma, rapid postoperative recovery and short hospitalization time. Under laparoscopic direct vision, doctors can accurately locate and effectively remove or destroy ectopic endometrial lesions, significantly alleviating the symptoms of patients [9]. At the same time, gonadotropin-releasing hormone agonist (GnRHa) plays a key role in postoperative adjuvant therapy [10]. GnRHa inhibits the secretion of gonadotropins by binding to the receptors on the surface of pituitary gonadotropin cells, thereby reducing the level of estrogen in the body, shrinking the ectopic endometrial tissue due to the lack of estrogen support, and achieving the purpose of inhibiting its growth [11]. However, although laparoscopic combined with GnRHa treatment can effectively improve the symptoms and quality of life of patients in the short term, the long-term recurrence problem has always been a major problem in clinical treatment. According to research statistics, there is a significant difference in the recurrence rate of endometriosis. The average recurrence rate of 2 years is between 20% (0%~89%), while the average recurrence rate of 5 years is in the range of 50% (15%~56%) [12, 13]. Disease recurrence not only means that patients must bear physical problems again, such as increased pain, infertility, and even deterioration, but also brings a heavy economic burden to patients and their families. In addition, the difficulty of treatment after multiple relapses increases significantly, and more aggressive treatment may be needed, which can further affect the patient’s physical and mental health. Therefore, it is of great importance to explore the influencing factors of EMs recurrence and construct a risk prediction model, which is helpful to identify high-risk patients of EMs recurrence as soon as possible and take targeted preventive interventions to improve the clinical prognosis of EMs patients.
Previous prediction of long-term recurrence of EMs has mainly depended on the experience of clinicians and some simple clinical indicators, such as patient age, disease stage, and surgical method [14, 15]. However, these methods are greatly affected by subjective factors, and cannot comprehensively consider the patient’s complex condition, so it is difficult to comprehensively and accurately predict the recurrence risk of individual patients. However, most of the existing prediction models are based on traditional statistical methods, which have problems such as insufficient data volume, insufficient model complexity, poor generalization ability, and are difficult to cope with complex clinical scenarios. In recent years, the rapid development of big data and machine learning technology has brought new opportunities for research and practice in the medical field. Machine learning algorithms can thoroughly mine and analyze massive and complex data, find potential associations and patterns, and build more accurate prediction models. The random forest (RF) model and gradient boosting machine (GBM) model in machine learning have unique advantages in dealing with complex data and constructing prediction models. The RF model has good generalization ability and anti-overfitting ability by constructing multiple decision trees and synthesizing their results for prediction. The GBM model is based on the gradient descent algorithm, and gradually iterates to improve the performance of the weak learner to build a more powerful prediction model. In other disease areas, such as breast cancer, hip fracture and cardiovascular disease, etc. [16, 17, 18, 19], these two models have been successfully applied to early screening and prognosis prediction of diseases. In the field of EMs, the application of RF and GBM models in the prediction of long-term recurrence after laparoscopy combined with GnRHa treatment is still scarce. In view of the high recurrence rate of EMs and the limitations of traditional prediction methods, this study aims to use RF and GBM models to comprehensively analyze the multiple factors affecting the long-term recurrence of EMs, and to construct an accurate recurrence prediction model. It provides a scientific basis for clinicians to formulate personalized treatment plans and implement effective recurrence prevention measures, in order to reduce the long-term recurrence rate of EMs in patients and improve the overall prognosis of EMs.
This study retrospectively collected data from 254 patients diagnosed with EMs who visited The First Affiliated Hospital, College of Medicine, Zhejiang University between July 2022 and December 2023. Inclusion criteria were as follows: (1) Patients met the relevant standards outlined in the EMs diagnosis and treatment guidelines [20] and were confirmed to have EMs through imaging studies and clinical evaluation; (2) Patients staged according to the American Fertility Society’s classification of endometriosis (r-AFS stages I–IV) [21]; (3) No recent use of hormonal medications; (4) Good compliance, capable of tolerating GnRHa therapy; (5) Absence of endocrine diseases; (6) Complete clinical data available. Exclusion criteria included: (1) Cognitive dysfunction or altered consciousness; (2) Coexisting conditions such as uterine fibroids, pelvic inflammatory disease, ectopic pregnancy, or other gynecological disorders; (3) Presence of organ dysfunction affecting heart, liver, kidneys, lungs, or severe diseases including hematologic disorders, neurological conditions, or malignancies; (4) History of surgical intervention for EMs or abdominal surgeries; (5) Inability to complete one year of follow-up.
All patients were selected to undergo laparoscopic surgery within 1 week after the end of menstruation, and the surgery was performed by single-hole laparoscopic surgery or four-hole laparoscopic surgery. All patients received intramuscular injections of GnRHa (manufacturer: Beijing Boente Pharmaceutical Co., Ltd., Sinopharm Approval No.: H20093809, production place: Beijing, China) 3.5 mg 5 days before the first menstrual period after surgery, once every 4 weeks, for a total of 6 injections.
All patients were followed up for 1 year after treatment. During the follow-up period, they returned to the hospital for re-examination every 3 months, including routine gynecological examination, ovarian function, biomarkers related to EMs, and pelvic ultrasound examination. Recurrence criteria [22]: ① Recurrence or even aggravation of clinical symptoms 3 months after surgery; ② Postoperative pelvic positive signs appeared again or aggravated to the level before treatment; ③ Postoperative ultrasound reexamination showed new lesions; ④ The level of medium sugar chain antigen 125 (CA125) in serum increased again. Excluding the influence of other disease factors, a patient must have met ① and either ②, ③, ④ to be classed as having had a recurrence. According to the recurrence of patients, they were divided into the recurrence group and the non-recurrence group.
Clinical data of patients were collected through the hospital medical record system, including age, age of menarche, course of disease, body mass index (BMI), preoperative delivery, cyst diameter, disease type, lesion side, smoking status, drinking history, preoperative history of dysmenorrhea, previous history of uterine operations, previous history of intraocular abnormalities, postoperative tenderness of the fornix, and r-AFS stage. Preoperative laboratory indicators: carbohydrate antigen 125, human epididymis protein 4, carbohydrate antigen 199.
SPSS 29.0 (Manufacturer: IBM Corporation, Armonk, NY, USA,
https://www.ibm.com/spss) was used for data analysis. Continuous variables
that conform to the normal distribution were expressed in the form of (mean
After 1 year of follow-up, there were 50 cases (19.68%) of recurrence and 204
cases (80.31%) of non-recurrence in 254 patients. Univariate analysis showed
that the course of disease, preoperative dysmenorrhea history, preoperative
uterine cavity operation history, postoperative fornix tenderness and r-AFS stage
were the influencing factors of postoperative recurrence in patients with EMs
treated by laparoscopy combined with GnRHa (p
| Factors | Recurrence group (n = 50) | Non-recurrence group (n = 204) | t/ |
p | |
| Age (years) | 33.04 |
34.18 |
0.896 | 0.371 | |
| Age of menarche (years) | 12.84 |
12.92 |
0.494 | 0.621 | |
| Course of disease [n (%), months] | 17.072 | ||||
| 9 (18.00) | 69 (33.82) | ||||
| 12–24 | 11 (22.00) | 76 (37.25) | |||
| 30 (60.00) | 59 (28.92) | ||||
| BMI (kg/m2) | 0.050 | 0.824 | |||
| 17 (34.00) | 66 (32.35) | ||||
| 33 (66.00) | 138 (67.65) | ||||
| Preoperative parity [n (%), times] | 1.185 | 0.553 | |||
| 0 | 28 (56.00) | 107 (52.45) | |||
| 1 | 15 (30.00) | 76 (37.26) | |||
| 7 (14.00) | 21 (10.29) | ||||
| Cyst diameter [n (%), cm] | 2.314 | 0.128 | |||
| 12 (24.00) | 72 (35.29) | ||||
| 38 (76.00) | 132 (64.71) | ||||
| Type of disease [n (%)] | 1.916 | 0.166 | |||
| Peritoneal type | 26 (52.00) | 84 (41.18) | |||
| Ovarian type | 24 (48.00) | 120 (58.82) | |||
| Lesion side [n (%)] | 0.795 | 0.373 | |||
| Unilateral | 38 (76.00) | 142 (69.61) | |||
| Bilateral | 12 (24.00) | 62 (30.39) | |||
| Smoking [n (%)] | 0.100 | 0.751 | |||
| Yes | 10 (20.00) | 45 (22.06) | |||
| No | 40 (80.00) | 159 (77.94) | |||
| Drinking [n (%)] | 0.091 | 0.763 | |||
| Yes | 11 (22.00) | 49 (24.02) | |||
| No | 39 (78.00) | 155 (75.98) | |||
| Preoperative dysmenorrhea history [n (%)] | 16.901 | ||||
| Yes | 39 (78.00) | 93 (45.59) | |||
| No | 11 (22.00) | 111 (54.41) | |||
| Previous history of uterine cavity operation [n (%)] | 16.406 | ||||
| Yes | 25 (50.00) | 44 (21.57) | |||
| No | 25 (50.00) | 160 (78.43) | |||
| History of endometriosis surgery [n (%)] | 0.498 | 0.480 | |||
| Yes | 8 (16.00) | 25 (12.25) | |||
| No | 42 (84.00) | 179 (87.75) | |||
| Tender posterior fornix [n (%)] | 5.031 | 0.025 | |||
| Yes | 26 (52.00) | 71 (34.80) | |||
| No | 24 (48.00) | 133 (65.20) | |||
| r-AFS stage [n (%), stage] | 30.884 | ||||
| I~II | 7 (14.00) | 118 (57.84) | |||
| III~IV | 43 (86.00) | 86 (42.16) | |||
| Carbohydrate antigen 125 (U/mL) | 51.04 |
52.68 |
0.704 | 0.482 | |
| Human epididymis protein 4 (pmol/L) | 28.20 |
26.80 |
1.379 | 0.169 | |
| Carbohydrate antigen 199 (U/mL) | 26.20 |
25.51 |
0.654 | 0.6514 | |
GnRHa, gonadotropin-releasing hormone agonist; EMs, endometriosis; BMI, body mass index; r-AFS, Revised American Fertility Society.
The variables with statistical significance in the single factor analysis in 2.1 were included in the RF model. The number of pre-selected variables at each tree node in the forest was set to the square root of all variables, and the number of random seeds was set to 12,345. When ntree = 500, mtry = 5 is the optimal model. At this time, ntree = 300, the error tended to be stable, and the dynamic relationship between the RF prediction error and the number of random trees is shown in Fig. 1A. According to the average reduction of the Gini index, the variables that predict the recurrence of EMs after laparoscopy combined with GnRHa treatment were ranked in order of importance, as r-AFS staging, course of disease, tender posterior fornix, history of intrauterine operations and history of preoperative endometriosis, as shown in Fig. 1B.
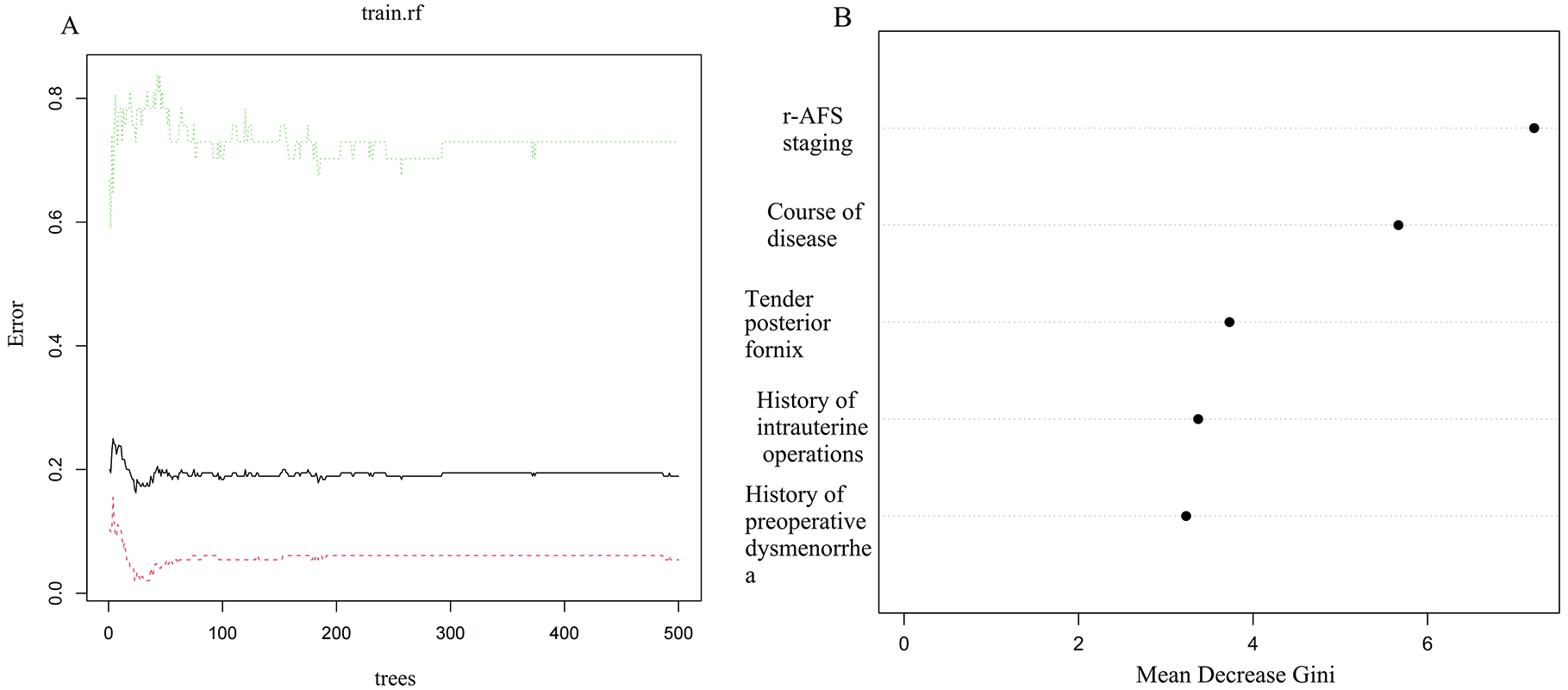 Fig. 1.
Fig. 1.
The establishment of the RF model and the relative importance of characteristic variables. (A) Dynamic relationship between RF model prediction error and the number of random trees. (B) RF model variable importance ranking. RF, Random Forest.
Variables with p
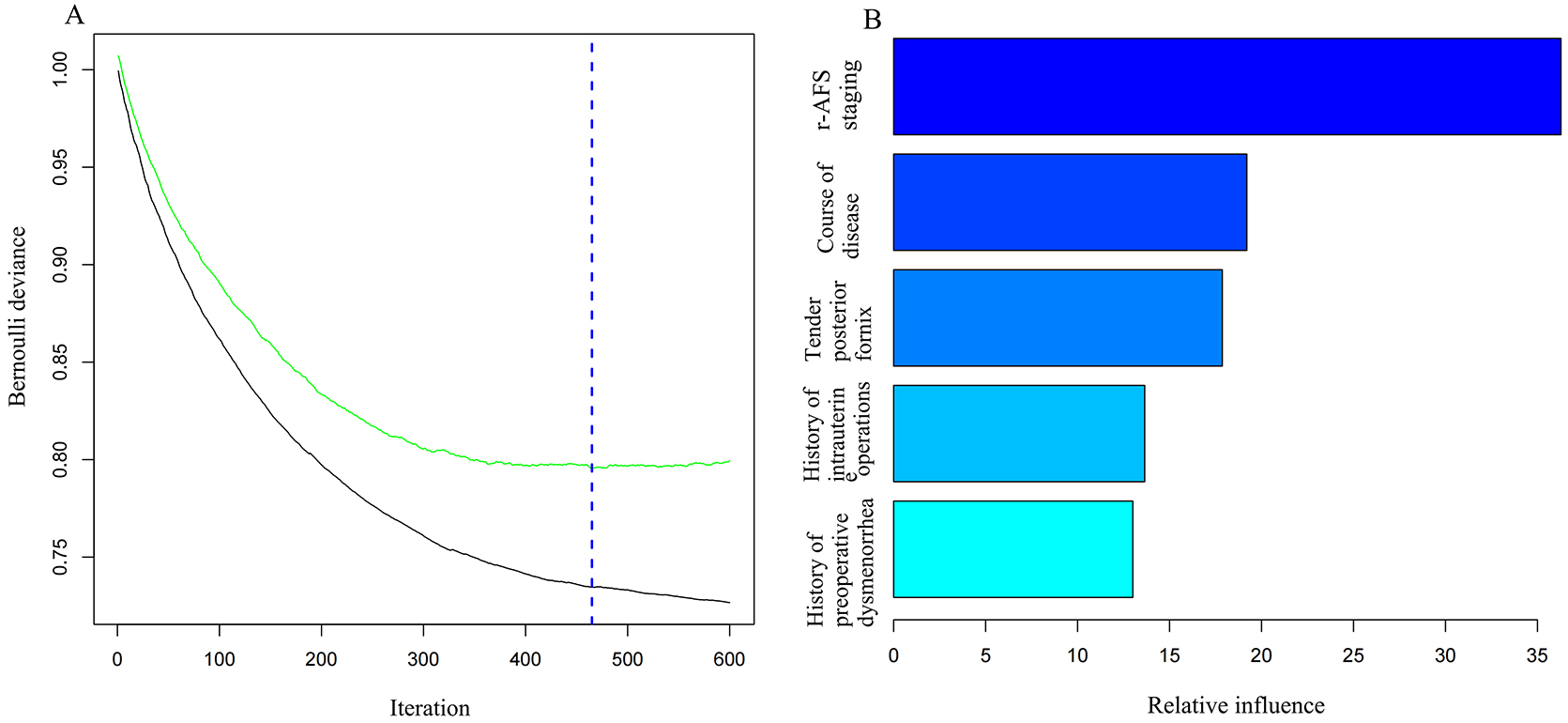 Fig. 2.
Fig. 2.
The GBM model establishment and relative importance ranking of feature variables. (A) The graph of iteration times and error rate. (B) The relative importance of variables in the GBM model. GBM, Gradient Boosting machine.
The ROC curve of the RF model showed that the AUC of the model in the training set was 0.902 (95% CI: 0.857–0.947), the sensitivity and specificity were 100.00% and 63.50%, respectively. In the validation set, the AUC was 0.859 (95% CI: 0.741–0.976), and the sensitivity and specificity were 69.20% and 92.90%, respectively (Fig. 3). The calibration curve results show that RF model prediction probability is in good agreement with actual prediction in both the training set and validation set. Fig. 4 highlights this.
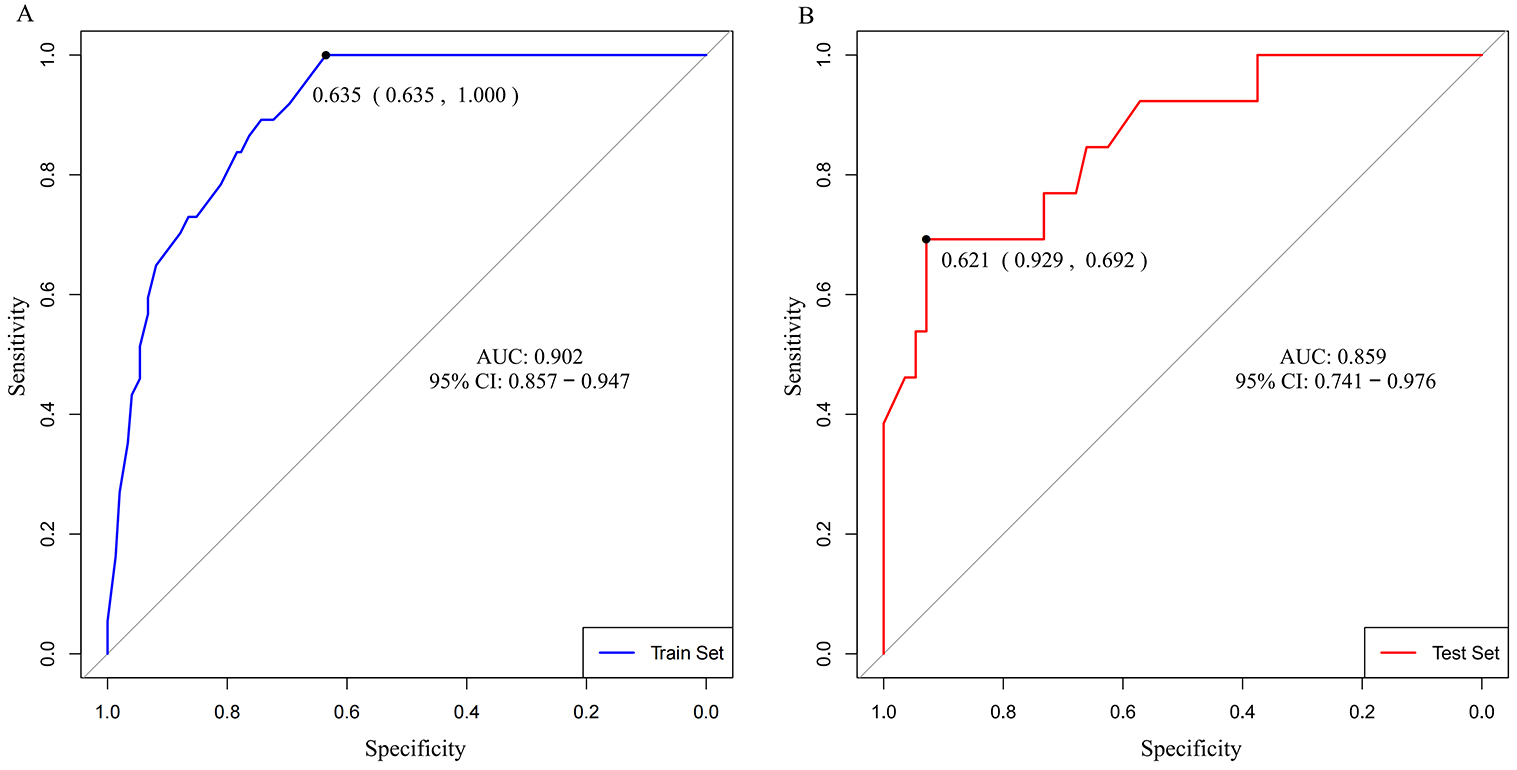 Fig. 3.
Fig. 3.
ROC curve of the RF model predicting the long-term recurrence of endometriosis treated by laparoscopy combined with GnRHa. (A) Training set. (B) Validation set. AUC, area under curve; ROC, receiver operating characteristic; RF, Random Forest; GnRHa, gonadotropin releasing hormone agonist.
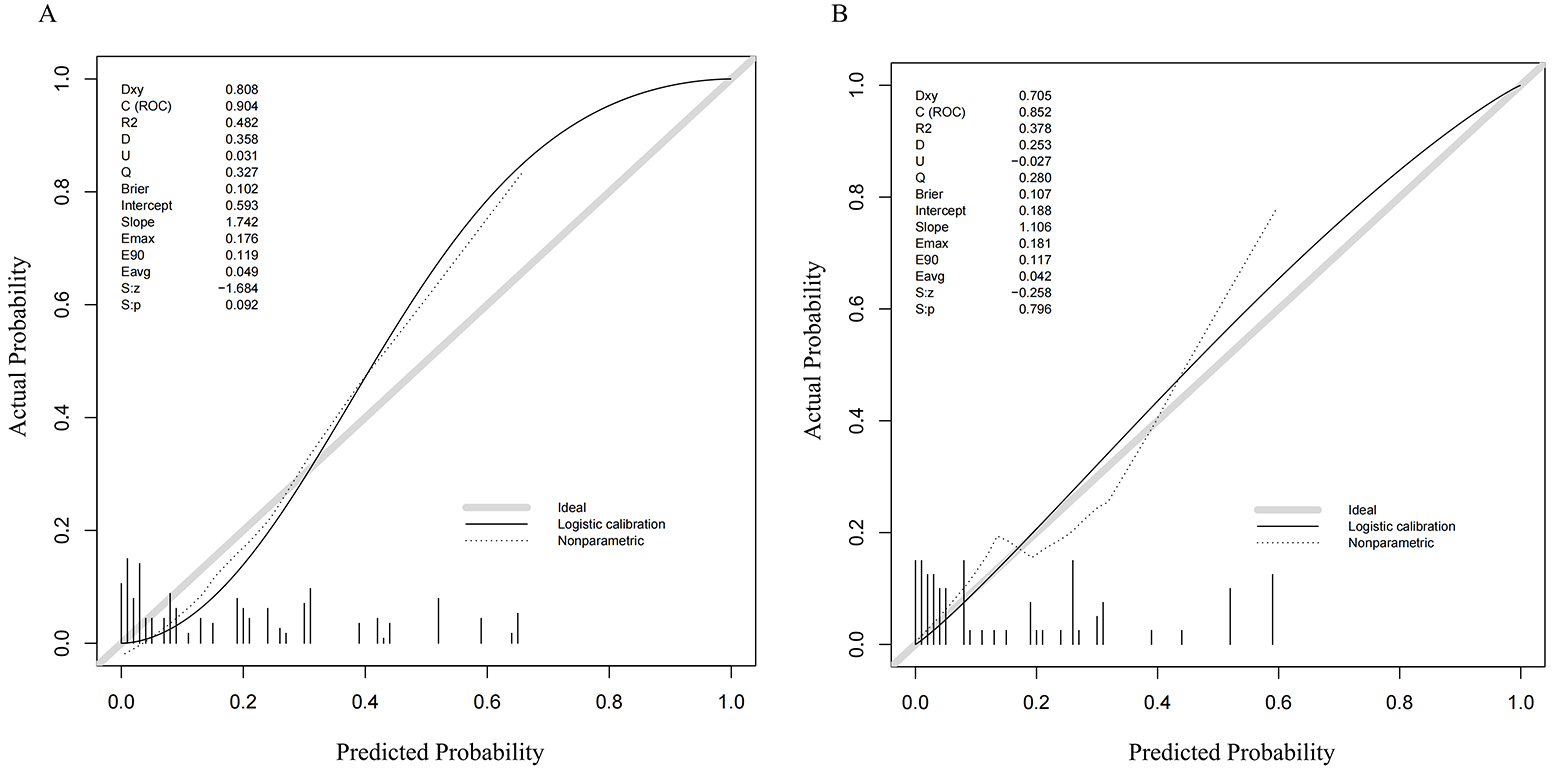 Fig. 4.
Fig. 4.
Calibration curve of the RF model predicting the long-term recurrence of endometriosis treated by laparoscopy combined with GnRHa. (A) Training set. (B) Validation set. RF, Random Forest.
The ROC curve of the GBM model showed that the AUC of the model in the training set was 0.851 (95% CI: 0.781–0.920), and the sensitivity and specificity were 89.20% and 68.20%, respectively. In the validation set, the AUC was 0.852 (95% CI: 0.713–0.990), and the sensitivity and specificity were 76.90% and 87.50%, respectively (Fig. 5). The results of calibration curve show that the GBM model’s prediction probability is consistent with the actual prediction in both the training set and the validation set. Fig. 6 shows this. Delong test results showed that the training set AUC of the RF model was better than that of GBM model, and the difference was statistically significant (Z = 2.838, p = 0.005). There was no significant difference in the validation set AUC between the RF model and the GBM model (Z = –0.239, p = 0.811).
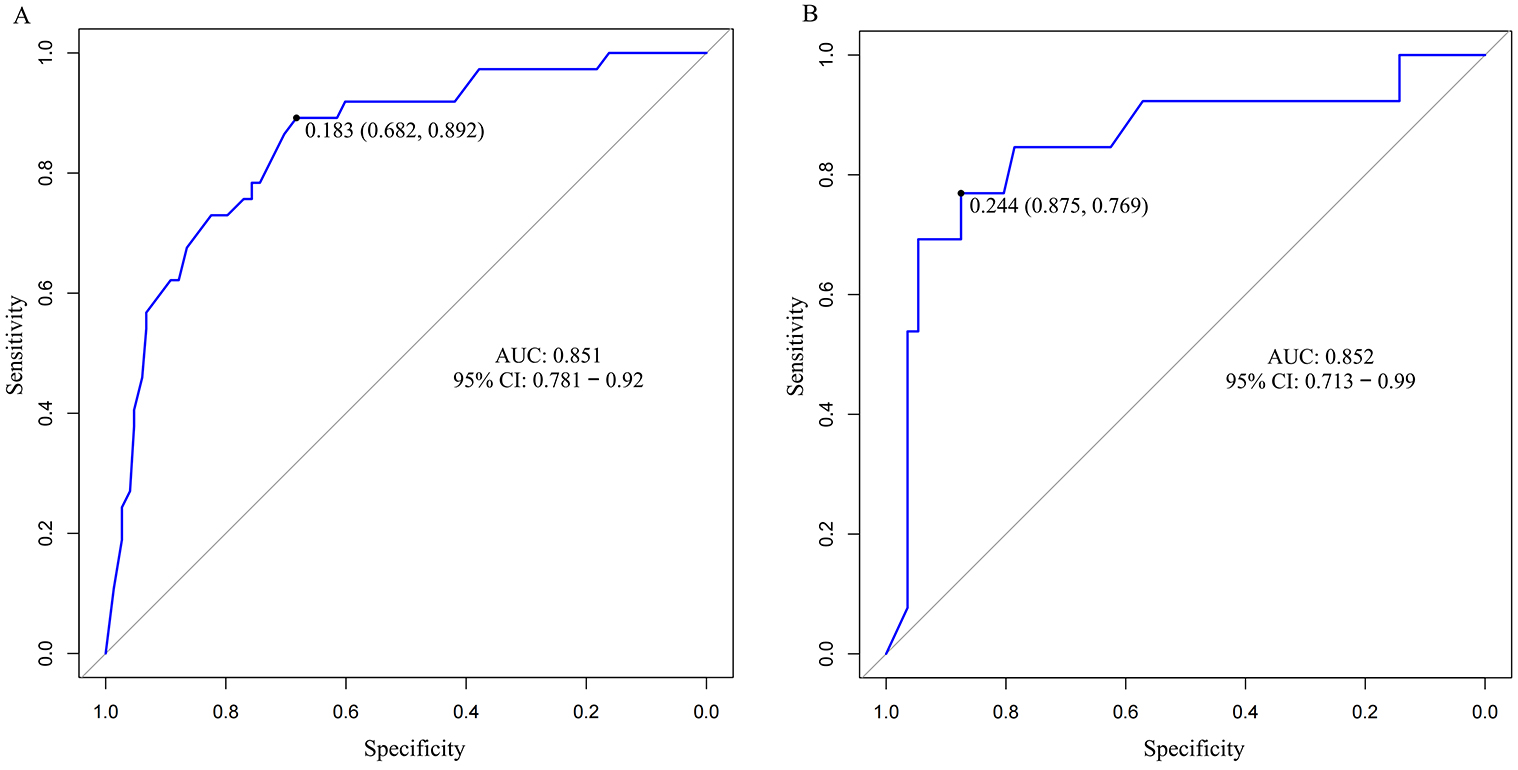 Fig. 5.
Fig. 5.
ROC curve of the GBM model predicting the long-term recurrence of endometriosis treated by laparoscopy combined with GnRHa. (A) Training set. (B) Validation set. GBM, Gradient Boosting machine.
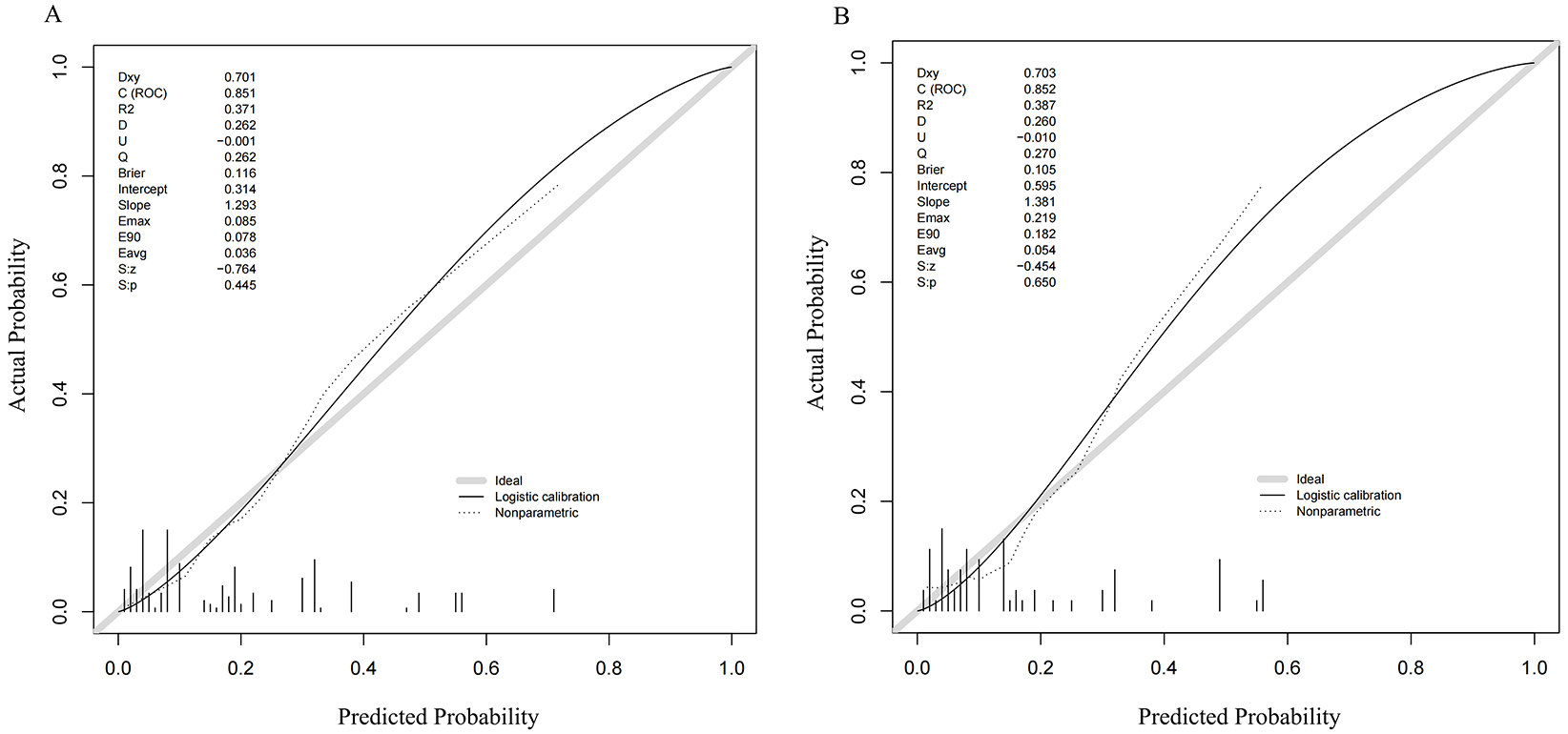 Fig. 6.
Fig. 6.
ROC curve of the GBM model predicting long-term recurrence of EMs treated by laparoscopy combined with GnRHa. (A) Training set. (B) Validation set. GBM, Gradient Boosting machine; EMs, Endometriosis.
Laparoscopic surgery is an effective method for the treatment of EMs, but the recurrence rate is high [23]. Incomplete surgical resection, residual lesions and new lesions are closely related to EMs recurrence [24, 25]. Patients with recurrent EMs have an increased risk of organ damage and ovarian function damage during reoperation, and the postoperative pregnancy rate is significantly decreased [26, 27]. GnRHa can inhibit pituitary activity, reduce estrogen levels, and block ectopic endometrial growth [28]. A number of studies have reported that the effective rate of laparoscopy combined with GnRHa is as high as more than 90%, and the effect on severe infiltration or occult lesions is significant [24, 29, 30]. However, recent studies have shown that the treatment still has the risk of recurrence [31], and the side effects of the drug will affect the reproductive function [32, 33]. This study found that the recurrence rate of EMs patients after laparoscopy combined with GnRHa treatment for 1-year was 19.68%, suggesting that laparoscopy combined with GnRHa treatment for EMs patients still cannot avoid the risk of recurrence. The analysis may be related to the different inclusion and exclusion criteria, follow-up time and research methods of the subjects. How to effectively reduce the risk of postoperative recurrence of EMs patients has attracted more and more attention from the medical community. Traditional prediction methods mainly rely on doctors’ clinical experience and simple clinical indicators, which are limited in accuracy and difficult to meet clinical needs. Therefore, it is particularly necessary to explore and apply more advanced prediction models.
The RF and GBM algorithms have high diagnostic ability and accuracy in disease risk prediction. They can provide the important evaluation of each variable for disease risk prediction, and provide reference information for subsequent clinical decision-making through data dimensionality reduction, pre-screening candidate features, and variable importance ranking [34, 35]. In this study, RF and GBM models were applied to the prediction of long-term recurrence of EMs treated by laparoscopy combined with GnRHa. Based on univariate analysis, the order of importance of the predictors of laparoscopic combined with GnRHa in the treatment of EMs based on the two groups of models was r-AFS staging, course of disease, tender posterior fornix, history of intrauterine operations and history of preoperative endometriosis. The reason for the analysis may be: patients with higher r-AFS staging are more likely to relapse after surgery, which may be due to the deeper infiltration of lesions with higher staging, easy adhesion, and the difficulty of thorough dissection [36]. Tobiume et al. [37] showed that r-AFS score was independently associated with recurrence after EMT, and patients with high r-AFS score were more likely to relapse. The palpable nodules in the posterior fornix were invaded by endometriosis lesions into the rectovaginal septum and uterosacral ligament. The longer the course of the disease, the higher the stage, the deeper the infiltration of the lesions, and the greater the difficulty of complete clearance of the treatment, which increases the risk of residual lesions and is more likely to lead to relapse. In severe cases, they may lead to the closure of the uterine rectal fossa, oppress the sensory nerve at the lesion site, and cause pain in the posterior fornix. The research has shown that posterior fornix tender nodules are risk factors for EMs after surgery [22]. Most of the lesions of the posterior fornix tenderness nodules are hidden, and the infiltration is deep. It is difficult to completely remove them during surgery, resulting in a greater risk of postoperative recurrence [38]. Patients with a history of uterine cavity operation and dysmenorrhea have a higher recurrence rate, which may be related to the late stage of dysmenorrhea patients, usually accompanied by pelvic adhesions, and pelvic lesions are difficult to completely peel off, and excessive uterine cavity surgery can easily lead to lesions being planted in the ovary and pelvic peritoneum, leading to repeated occurrence of endometriosis [39, 40]. Study has found that estrogen and its receptors are highly expressed in patients with endometriosis dysmenorrhea. Lessey and Young [41] proposed that the growth of ectopic lesions depends on estrogen and its receptors, which may also be a reason for improving the postoperative recurrence rate of such patients. Previous anti-endometriosis drug treatment can cause endometrial lesions atrophy, edema and other morphological changes, but to cover up the formation of the lesion, meaning it is difficult to completely remove the lesion during surgery, which then leaves the hidden danger of postoperative recurrence [42].
In this study, the performance of the two models was compared. The results showed that on the training set, the RF model showed a higher AUC value of 0.902, and the sensitivity was 100%. This shows that the RF model has excellent discrimination ability on training data and can accurately identify positive and negative samples. In contrast, the AUC of the GBM model was 0.851, and the sensitivity and specificity were 89.20% and 68.20%, respectively. The Delong test results further confirmed that the AUC of the RF model on the training set was significantly better than that of the GBM model (Z = 2.838, p = 0.005). The advantages of the RF model on the training set may be due to its algorithmic characteristics. RF makes its predictions by constructing multiple decision trees and combining their results. This integrated learning method allows the model to have a stronger generalization ability when dealing with complex data, and can effectively avoid overfitting. In addition, the RF model uses a random sampling method for the construction of each decision tree during the training process, which increases the diversity of the model and improves its learning ability for different feature combinations [33]. The GBM model uses a gradient boosting strategy to gradually optimize model performance by iteratively training multiple weak learners. However, due to its fine fitting of training data, it may lead to over-learning certain specific patterns on the training set, affecting the generalization ability of the model, and then lagging behind the RF model on the AUC of the training set.
On the validation set, the AUC of the RF model was 0.859, and the GBM model was 0.852. The Delong test showed that there was no significant difference between the two models (Z = –0.239, p = 0.811). The sensitivity and specificity of the RF model were 69.2% and 92.9%, respectively, and the sensitivity and specificity of the GBM model were 76.9% and 87.5%, respectively, which indicated that the RF model and the GBM model performed well in predicting EMs recurrence samples, and the discrimination ability and prediction effect of the two models were comparable. The calibration curve shows that the RF and GBM models have high consistency between the prediction probability and the actual results in the training set and the validation set. This indicates that the two models are more accurate in predicting the probability of event occurrence, and jointly provide a quantitative decision-making basis for patients to formulate individualized intervention programs (such as GnRHa treatment duration, follow-up density) and optimize medical resource allocation (reducing excessive examination and treatment). In practical applications, if the fitting effect of training data is required to be high, the RF model is a better choice; If more attention is paid to the stability of the model on the data, both RF and GBM models can be considered. In addition, when the model is applied to the actual scene, it is also necessary to consider the factors such as the interpretability and computational cost of the model, and make decisions after comprehensive trade-offs. Therefore, RF and GBM models have their own advantages, and the choice of which model or whether to use it in combination should be determined according to the specific situation and needs.
However, this study also has some limitations: (1) First of all, this study is a single-center retrospective study, the sample size is relatively small, there may be selection bias, and the extrapolation of the model needs to be verified further. (2) Secondly, this study only included limited clinical features as predictors. In the future, biomarkers such as genes and proteins can be further combined to improve the predictive efficacy of the model. (3) In addition, the interpretability of machine learning models is relatively poor. Although some methods (such as variable importance analysis) can be used to explain the decision-making process of the model, it is still difficult to explain the relationship between variables and outcomes as intuitively as traditional statistical models. Therefore, in the future, doctors can better understand the decision-making process of the model and improve the application value of the model in clinical practice by developing visualization tools or explanatory algorithms.
In summary, r-AFS staging, course of disease, tender posterior fornix, history of intrauterine operations and history of preoperative laparoscopy are the influencing factors of long-term recurrence of EMs treated by laparoscopy combined with GnRHa. The recurrence of such patients after treatment can be effectively predicted by constructing RF and GBM models. The RF model was preferentially selected for the initial screening of recurrence risk to avoid missed diagnosis, and the dynamic risk update was combined with the GBM model to optimize the intervention strategy. This study provides a quantitative tool for individualized management of EMs patients, which can accurately formulate GnRHa treatment duration and follow-up plan through model prediction probability, and provide a paradigm for machine learning prediction model transformation of benign diseases.
Data is available from the corresponding author on reasonable request.
KZ, RZ and YJ designed this study. KZ conducted research. KZ provided assistance in the design of the research plan and suggestions for the overall writing approach of the manuscript. RZ and YJ analyzed these data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was conducted in accordance with The guiding principles of the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of The First Affiliated Hospital, College of Medicine, Zhejiang University (Approval Number: 2025B0730). Informed consent was obtained from all patients or their families/legal guardians prior to participation.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.