



 , Tian Lan 1,†, Wangjin Xu 1,*
, Tian Lan 1,†, Wangjin Xu 1,*
1 Department of Breast Surgery, Hangzhou TCM Hospital Affiliated to Zhejiang Chinese Medical University, 310007 Hangzhou, Zhejiang, China
†These authors contributed equally.
Abstract
Breast cancer among adolescent and young adult (AYA) women requires greater awareness and concern due to the aggressive nature of the tumor. Therefore, this study aimed to examine the spatiotemporal trends in the burden of breast cancer in AYA women between 1990 and 2019.
Data on breast cancer in AYA women were obtained from the Global Burden of Disease (GBD) 2019 study, and the estimated annual percentage change (EAPC) was computed to assess trends over time.
In 2019, the age-standardized prevalence rate (ASPR) of breast cancer among AYA women was 94.8 per 100,000 population, while the age-standardized incidence rate (ASIR) was 11.29 per 100,000 population. From 1990 to 2019, the age-standardized mortality rate (ASMR) declined from 3.02 (95% uncertainty interval (UI): 2.78–3.26) to 2.86 (95% UI: 2.58–3.17) per 100,000 population, and the EAPC was –0.41 (95% confidence interval (CI): –0.53 to –0.30). The age-standardized disability-adjusted life year (DALY) rate (ASDR) was 165.2 (95% UI: 148.54–182.26) in 2019, and the EAPC was –0.34 (95% CI: –0.46 to –0.23). The regions with a mid-level sociodemographic index (SDI) exhibited the fastest increases in both the ASPR and ASIR, with EAPCs of 1.77 (95% CI: 1.66 to 1.84) and 1.57 (95% CI: 1.45 to 1.67), respectively. There was an increased trend in the ASDR and ASMR in the low-middle and low SDI regions. The most substantial contributors to the DALYs and death were alcohol consumption, tobacco use, and low physical activity, which were closely followed by high fasting plasma glucose and higher red meat consumption.
We comprehensively evaluated the burden of breast cancer in AYA women while considering factors such as SDI, age, risk elements, and geographical distribution. These findings could inform resource allocation and the development of effective policies.
Keywords
- breast cancer
- adolescent and young adult
- Global Disease Burden 2019
- incidence
- mortality
Breast cancer is the most commonly diagnosed cancer among women, and approximately 4% of cases occur among adolescent and young adult (AYA) women [1, 2]. Age at diagnosis is a key determinant of tumor biology and outcomes and guides protocols for breast-cancer screening, therapeutic decisions, and survival predictions. The features of breast cancer in AYAs distinctly differ from those of older individuals. AYA breast cancer is also often characterized by more biologically aggressive features, such as larger tumor diameter, more lymph-node involvement, higher clinical staging, unfavorable molecular subgroups, poor prognoses, and increased likelihood of hereditary predisposition [3].
Many studies have relied on comprehensive data from various countries, regions, and global datasets to investigate breast cancer comprehensively [4, 5, 6, 7]. Numerous epidemiological studies have specifically focused on AYA breast cancer in certain countries, including China, Japan, and Nigeria [8, 9, 10]. Historically, the global occurrence of AYA breast cancer has received less attention from researchers despite its significance in the transitional phase between pediatric and adult oncology. Therefore, a thorough investigation into the epidemiological patterns and disease burden of AYA breast cancer is needed. In this study, we examined data from the Global Burden of Diseases (GBD), Injuries, and Risk Factors Study 2019 to assess the worldwide burden of AYA breast cancer, identify high-risk groups through age and socio-demographic index (SDI) stratification, and quantify the burden linked to risk factors.
The GBD 2019 dataset incorporated epidemiologic metrics for 369 pathological conditions and 87 risk factors (available at http://ghdx.healthdata.org/gbd-results-tool). These estimates encompassed 204 geopolitical entities and 21 subregions from 1990 to 2019 [11]. The SDI was estimated for each country according to education levels, birth rate, and per capita income. Using quintile stratification based on SDI metrics, global territories were categorized into five tiers: high, high-middle, middle, low-middle, and low-SDI regions. The requirements for ethical approval and informed consent were waived due to the public availability of the GBD 2019 database and the absence of identifiable information in the analyses.
AYA breast cancer is commonly defined as a diagnosis of breast cancer occurring between the ages of 15 and 39 years [12]. The data comprised information on prevalence, incidence, death, disability-adjusted life years (DALYs), and corresponding age-standardized rate (ASR), which were examined according to region, country, age, and year groups. DALYs were calculated by combining two components: years of life lost (YLLs) and years lived with disability (YLDs). YLDs were estimated as the product of disease prevalence and the associated disability weight for each health outcome, while YLLs were quantified by measuring deaths against a reference longevity standard. ASRs are widely used to enhance the accuracy of disease-burden comparisons as they consider age variations.
The truncated ASRs and corresponding uncertainty intervals (UIs) were calculated against the world standard population distribution (World Health Organization (WHO) 2000–2025) [13]. The ASR for AYA breast cancer was computed through multiplicative weighting of age-stratified incidence (aᵢ) against corresponding demographic strata weights (wᵢ) from the reference population [14]:
Temporal patterns were assessed by deriving the estimated annual percentage change (EAPC) and the corresponding 95% confidence interval (CI) using linear regression modeling. Two formulas were used:
where X is the calendar year (time variable),
Increasing ASR trends were inferred from EAPC values greater than zero, which were supported by positive lower bounds of the CIs. Negative values for EAPCs and upper limits of the CIs suggested a downward trend. Pearson’s correlation analysis was carried out to quantify the linear association between ASRs and SDI. All statistics and visualization were performed using R version 4.1.2 (Vienna, Austria, https://www.r-project.org). Several R packages were used, including tidyverse for data manipulation, ggplot2 and patchwork for visualization, epitools for epidemiological analysis, and ggmaps for geospatial mapping. Statistical significance was defined by p-values below 0.05.
The age-standardized prevalence rate (ASPR) of breast cancer among AYAs was 94.8 per 100,000 population in 2019. Similarly, the age-standardized incidence rate (ASIR) was documented as 11.29 per 100,000 population (Table 1, Supplementary Table 1). The EAPCs of ASPR and ASIR were 0.67 (95% CI: 0.59 to 0.75) and 0.60 (95% CI: 0.50 to 0.69), respectively, indicating an increasing trajectory over the last 30 years (Table 1, Supplementary Table 1, and Fig. 1). Notably, however, the age-standardized mortality rate (ASMR) declined from 3.02 (95% UI: 2.78–3.26) in 1990 to 2.86 (95% UI: 2.58–3.17) in 2019, and the EAPC was –0.41 (95% CI: –0.53 to –0.30) (Table 2, Fig. 1). The age-standardized DALY rate (ASDR) was 165.2 (95% UI: 148.54–182.26) in 2019, and the EAPC was –0.34 (95% CI: –0.46 to –0.23), indicating a declining trend (Supplementary Table 2, Fig. 1).
| ASIR in 1990 | ASIR in 2019 | EAPC 1990–2019 | ||
| No. (95% UI) | No. (95% UI) | No. (95% CI) | ||
| Global | 9.04 (8.48–9.59) | 11.29 (10.17–12.46) | 0.60 (0.50 to 0.69) | |
| SDI regions | ||||
| Low SDI | 4.47 (3.68–5.35) | 6.76 (5.53–8.10) | 1.35 (1.27 to 1.41) | |
| Low-middle SDI | 5.68 (4.70–6.73) | 8.68 (7.31–10.31) | 1.23 (1.09 to 1.36) | |
| Middle SDI | 6.83 (6.03–7.69) | 11.27 (9.86–12.82) | 1.57 (1.45 to 1.67) | |
| High-middle SDI | 9.90 (9.25–10.58) | 13.33 (11.58–15.40) | 0.92 (0.80 to 1.03) | |
| High SDI | 17.54 (16.80–18.32) | 17.04 (15.01–19.25) | –0.19 (–0.26 to –0.12) | |
| GBD regions | ||||
| High-income Asia Pacific | 11.55 (9.76–13.53) | 14.71 (11.59–18.35) | 1.01 (0.75 to 1.27) | |
| High-income North America | 22.04 (20.90–23.25) | 17.60 (13.95–21.97) | –0.90 (–1.06 to –0.75) | |
| Central Asia | 11.58 (10.54–12.73) | 11.02 (9.15–13.38) | –0.40 (–0.54 to –0.26) | |
| East Asia | 5.50 (4.35–6.81) | 11.37 (8.64–14.47) | 2.22 (1.91 to 2.47) | |
| South Asia | 4.60 (3.82–5.47) | 8.21 (6.55–10.04) | 1.85 (1.73 to 1.93) | |
| Southeast Asia | 11.16 (8.77–13.89) | 15.23 (12.59–18.48) | 1.05 (0.93 to 1.16) | |
| Central Europe | 12.19 (11.27–13.18) | 13.51 (11.04–16.35) | 0.38 (0.24 to 0.52) | |
| Eastern Europe | 12.24 (11.33–13.29) | 14.14 (11.34–17.61) | 0.33 (0.05 to 0.61) | |
| Western Europe | 19.70 (18.48–21.07) | 19.54 (16.11–23.38) | –0.17 (–0.25 to –0.10) | |
| Andean Latin America | 4.98 (4.02–6.13) | 7.17 (5.02–10.00) | 1.00 (0.83 to 1.16) | |
| Central Latin America | 6.61 (6.21–7.06) | 9.67 (7.72–11.97) | 1.34 (1.19 to 1.47) | |
| Southern Latin America | 10.11 (8.69–11.73) | 12.47 (8.51–17.66) | 0.64 (0.49 to 0.79) | |
| Tropical Latin America | 7.86 (7.29–8.55) | 10.97 (9.83–12.30) | 1.26 (1.13 to 1.37) | |
| Australasia | 18.57 (16.04–21.29) | 17.61 (12.45–24.66) | –0.34 (–0.48 to –0.21) | |
| Caribbean | 11.02 (9.25–12.91) | 13.60 (9.85–17.84) | 0.58 (0.46 to 0.69) | |
| North Africa and Middle East | 6.33 (5.44–7.45) | 12.08 (10.08–14.39) | 2.24 (2.17 to 2.26) | |
| Oceania | 16.73 (11.44–24.01) | 24.26 (16.50–35.32) | 1.24 (1.16 to 1.30) | |
| Central Sub-Saharan Africa | 5.82 (3.85–8.53) | 7.37 (4.79–10.79) | 0.70 (0.55 to 0.84) | |
| Eastern Sub-Saharan Africa | 4.59 (3.36–5.87) | 5.71 (4.41–7.22) | 0.50 (0.32 to 0.67) | |
| Southern Sub-Saharan Africa | 8.99 (7.53–10.56) | 7.95 (4.97–11.52) | –0.65 (–1.37 to 0.07) | |
| Western Sub-Saharan Africa | 4.52 (3.47–5.83) | 6.56 (4.76–8.80) | 1.32 (1.22 to 1.40) | |
AYA, adolescent and young adult; ASIR, age-standardized incidence rate; EAPC, estimated annual percent change; SDI, socio-demographic index; EAPC, estimated annual percentage change; GBD, Global Burden of Disease; UI, uncertainty interval; CI, confidence interval.
| Characteristics | ASMR in 1990 | ASMR in 2019 | EAPC 1990–2019 | |
| No. (95% UI) | No. (95% UI) | No. (95% CI) | ||
| Global | 3.02 (2.78–3.26) | 2.86 (2.58–3.17) | –0.41 (–0.53 to –0.30) | |
| SDI regions | ||||
| Low SDI | 2.79 (2.30–3.34) | 3.35 (2.78–4.01) | 0.51 (0.44 to 0.57) | |
| Low-middle SDI | 3.11 (2.58–3.73) | 3.45 (2.86–4.13) | 0.11 (–0.03 to 0.25) | |
| Middle SDI | 2.92 (2.60–3.29) | 2.87 (2.53–3.25) | –0.24 (–0.35 to –0.13) | |
| High-middle SDI | 2.94 (2.74–3.17) | 2.28 (2.04–2.55) | –1.21 (–1.39 to –1.05) | |
| High SDI | 3.25 (3.17–3.34) | 2.02 (1.90–2.14) | –1.80 (–1.97 to –1.67) | |
| GBD regions | ||||
| High-income Asia Pacific | 2.03 (1.93–2.14) | 1.44 (1.31–1.62) | –1.23 (–1.37 to –1.10) | |
| High-income North America | 3.70 (3.57–3.83) | 2.15 (1.99–2.31) | –1.96 (–2.21 to –1.75) | |
| Central Asia | 4.22 (3.93–4.53) | 3.04 (2.55–3.64) | –1.45 (–1.61 to –1.32) | |
| East Asia | 1.98 (1.57–2.46) | 1.59 (1.22–2.01) | –1.40 (–1.78 to –1.03) | |
| South Asia | 2.63 (2.21–3.12) | 3.40 (2.70–4.23) | 0.70 (0.59 to 0.81) | |
| Southeast Asia | 5.54 (4.38–6.96) | 5.02 (4.17–6.05) | –0.38 (–0.50 to –0.26) | |
| Central Europe | 3.41 (3.22–3.59) | 2.17 (1.81–2.61) | –1.65 (–1.85 to –1.48) | |
| Eastern Europe | 3.43 (3.21–3.67) | 2.56 (2.07–3.19) | –1.65 (–1.97 to –1.35) | |
| Western Europe | 3.82 (3.69–3.96) | 2.20 (2.05–2.35) | –2.12 (–2.29 to –2.00) | |
| Andean Latin America | 2.41 (1.99–2.92) | 1.96 (1.40–2.67) | –1.05 (–1.22 to –0.89) | |
| Central Latin America | 2.46 (2.34–2.58) | 2.23 (1.81–2.72) | –0.24 (–0.46 to –0.02) | |
| Southern Latin America | 3.80 (3.41–4.24) | 2.92 (2.38–3.5) | –0.96 (–1.18 to –0.75) | |
| Tropical Latin America | 3.08 (2.88–3.29) | 2.78 (2.53–3.07) | –0.23 (–0.31 to –0.15) | |
| Australasia | 3.54 (3.23–3.88) | 2.02 (1.65–2.44) | –2.18 (–2.39 to –2.03) | |
| Caribbean | 3.67 (2.96–4.56) | 4.14 (2.86–5.73) | 0.43 (0.30 to 0.56) | |
| North Africa and Middle East | 2.65 (2.28–3.12) | 2.80 (2.31–3.38) | 0.12 (0.07 to 0.17) | |
| Oceania | 8.80 (5.86–12.68) | 11.36 (7.73–16.22) | 0.93 (0.85 to 1.00) | |
| Central Sub-Saharan Africa | 3.41 (2.31–4.87) | 3.79 (2.46–5.54) | 0.20 (0.07 to 0.33) | |
| Eastern Sub-Saharan Africa | 2.93 (2.12–3.73) | 2.92 (2.29–3.68) | –0.26 (–0.44 to –0.09) | |
| Southern Sub-Saharan Africa | 4.43 (3.74–5.18) | 3.27 (2.11–4.63) | –1.12 (–1.94 to –0.30) | |
| Western Sub-Saharan Africa | 2.71 (2.13–3.5) | 3.16 (2.32–4.21) | 0.52 (0.40 to 0.63) | |
 Fig. 1.
Fig. 1.
The EAPC of age-standardized prevalence, incidence, death and DALYs rates for breast cancer in adolescents and young adults. DALYs, disability-adjusted life years.
High-SDI regions had the highest ASPR (152.13, 95% UI: 133.95–171.47) and ASIR (17.04, 95% UI: 15.01–19.25) for AYA breast cancer in 2019 (Table 1, Supplementary Table 1). The most rapid increase in ASPR and ASIR occurred in the middle-SDI regions (EAPC: 1.77 for ASPR; EAPC: 1.57 for ASIR) (Fig. 1). In the high-SDI regions, both ASIR and ASPR decreased gradually over time, which is supported by negative values of EAPC (–0.14 for ASPR; –0.19 for ASIR). Nevertheless, the ASMR (3.45, 95% UI: 2.86–4.13) and ASDR (197.24, 95% UI: 163.26–236.30) were highest in the low-middle SDI regions (Table 2, Supplementary Table 2). The EAPCs of ASMR and ASDR were positive values in the low-middle and low SDI regions, indicating a rising trend over time (Fig. 1). The results indicated a declining trend in ASMR and ASDR across the high, high-middle, and middle-SDI regions.
With respect to the GBD region, Oceania, Australasia, and Western Europe suffered the highest ASPR and ASIR (Table 1, Supplementary Table 1). The ASPR and ASIR were lowest in Eastern Sub-Saharan Africa, Andean Latin America, and Western Sub-Saharan Africa. An overall upward trajectory in ASPR and ASIR was evident globally except in five regions: Western Europe, high-income North America, Central Asia, Australasia, and Southern Sub-Saharan Africa (Fig. 1). The GBD region with the highest ASMR and ASDR was identified as Oceania (ASMR: 11.36, 95% UI, 7.73–16.22; ASDR: 637.79, 95% UI, 433.84–911.35) (Table 2, Supplementary Table 2). Andean Latin America, high-income Asia Pacific, and East Asia exhibited the lowest ASMR and ASDR for AYA breast cancer. Conversely, the most substantial increases in ASMR and ASDR were observed in North Africa and the Middle East, South Asia, and East Asia (Fig. 1).
The burden of AYA breast cancer exhibited considerable national-level disparities across the 204 countries. Pakistan, India, China, the United States of America, and Indonesia were recorded as the five foremost countries with the highest prevalence and incidence in 2019 (Supplementary Tables 3,4). Higher ASIR and ASPR were observed in Oceania (Solomon Islands, Cook Islands, Nauru, Palau, and Niue) and Western Europe (Monaco, San Marino, Netherlands, United Kingdom, France, and Portugal) (Supplementary Fig. 1A, Supplementary Fig. 1B). Saint Kitts and Nevis, Myanmar, and Kyrgyzstan had the lowest EAPC values for both ASPR and ASIR, which were all less than –2.0 (Supplementary Tables 3,4, and Supplementary Fig. 2A,B). The highest EAPCs for ASPR and ASIR were observed in North Africa and the Middle East (Saudi Arabia, Turkey, Yemen, Oman, and Lebanon), as well as Southern Sub-Saharan Africa (Botswana and Namibia).
The highest DALYs and death rates were documented in India, China, Indonesia, and Pakistan (Supplementary Tables 5,6). Pakistan, Indonesia, and some Oceania countries (Solomon Islands, Kiribati, Nauru, Fiji, Papua New Guinea, and Marshall Islands) had relatively high ASMR and ASDR for AYA breast cancer (Supplementary Fig. 1C,D). Out of the 204 countries, Solomon Island, Zimbabwe, Lesotho, Jamaica, and Yemen demonstrated the largest growth in ASMR and ASDR (Supplementary Tables 5,6, and Supplementary Fig. 2C,D). The EAPCs for these countries all exceeded 1.90.
The risk factors influencing DALYs and deaths varied across different GBD regions (Fig. 2). The burden of DALYs attributable to tobacco was disproportionately concentrated in East Asia (10.82%), high-income Asia Pacific regions (12.02%), and Southern Sub-Saharan Africa (12.89%). North Africa and the Middle East, Western Europe, and Eastern Sub-Saharan Africa displayed the greatest percentages of the DALYs attributed to alcohol use. Elevated fasting glucose accounted for the highest proportion of DALYs in Southern Sub-Saharan Africa. Low physical activity was the primary driver of DALYs in East Asia and Oceania. Both ASDR and ASMR of AYA breast cancer related to increased fasting glucose showed an increasing trend in all SDI regions (Fig. 3A–C, Supplementary Fig. 3A–C, and Supplementary Tables 7,8). In addition, there was an upward trend for ASDR attributed to all risk factors in low-SDI regions.
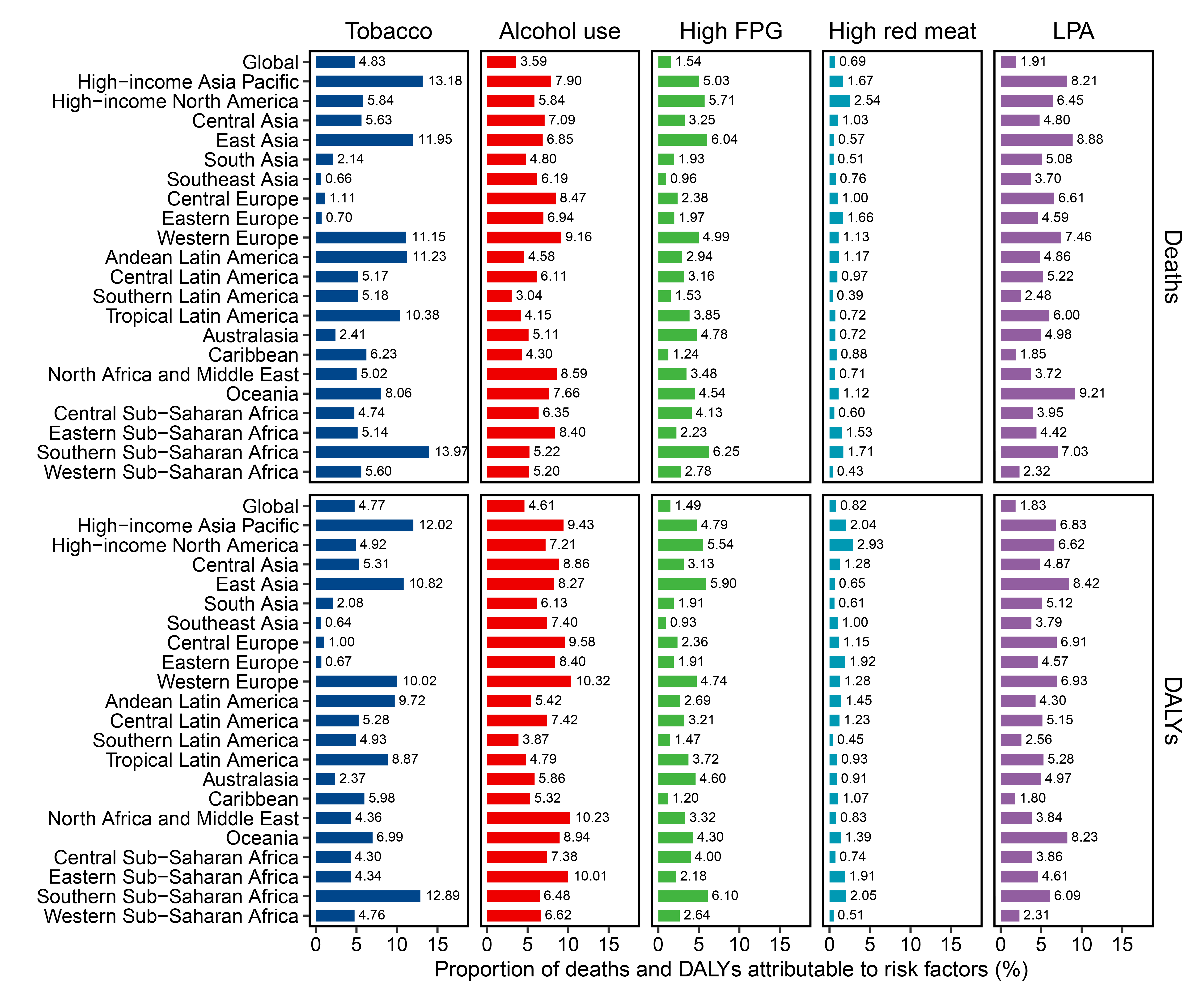 Fig. 2.
Fig. 2.
The proportion of AYA breast cancer deaths and DALYs attributable to risk factors among the GBD regions in 2019. DALY, disability adjusted life-year; FPG, fasting plasma glucose; LPA, low physical activity.
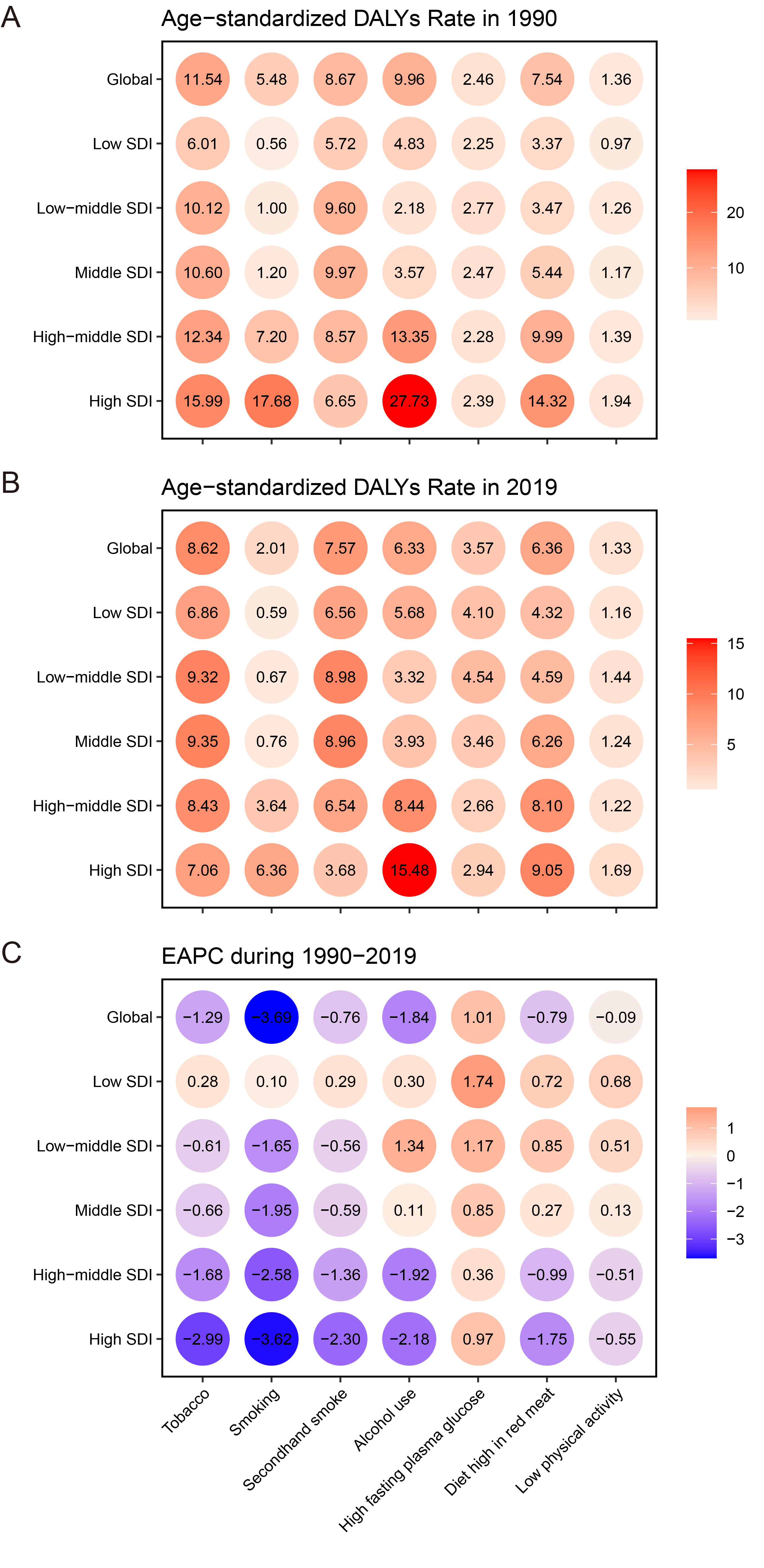 Fig. 3.
Fig. 3.
The age-standardized DALYs rate of AYA breast cancer attributable to risk factors across distinct SDI regions in 1990 and 2019 with corresponding EAPC. (A) The age-standardized DALYs rate in 1990; (B) age-standardized DALYs rate in 2019; (C) EAPC in 1990–2019.
The global prevalence, incidence, death rate, and DALY rate exhibited upward trends across the five subgroups of age (Supplementary Fig. 4). The prevalence and incidence rate increased gradually with the increase of SDI in the age subgroups of 25–29, 30–34, and 35–39 years. In contrast, for the age subgroups of 15–19 and 20–24 years, the highest incidence and prevalence rates of AYA breast cancer were identified in regions with low-middle SDI. The patterns of death and DALY rates among various SDI regions were similar among the five age subgroups. The low-middle and low SDI regions exhibited the greatest rates of both DALYs and deaths.
The trends of the four ASRs across SDI regions are presented in
Supplementary Fig. 5. Higher SDI levels were significantly
associated with increased ASIR and ASPR (Supplementary Fig.
6A,B). The results indicated a positive correlation between SDI and ASMR in the
GBD regions where the SDI was less than 0.4 (Supplementary Fig.
6C). The ASDR pattern related to SDI was similar to that of ASMR
(Supplementary Fig. 6D). An inverse relationship was found
between EAPC of ASRs and SDI (r: –0.40, p = 0.06 for ASMR;
r: –0. 46, p
This study systematically assessed the spatial and temporal trends of AYA breast cancer and the underlying risk factors from 1990 to 2019. We also explored the influence of diverse demographic factors (age, SDI, and risk factors). The trends of the four ASRs have changed over the past three decades. The ASR trends diverged substantially among differing geographic and SDI areas. Moreover, heterogeneities were observed in the burdens of AYA breast cancer resulting from different risk factors across different regions. The effective management and prevention of AYA breast cancer continue to be a formidable challenge.
There has been an increase in ASPR and ASIR of AYA breast cancer during past 30 years, whereas ASMR and ASDR showed a decline. The ASIR of AYA breast cancer (EAPC: 0.60) showed a remarkable surge and surpassed that of total breast cancer (EAPC: 0.41). Nevertheless, the declining trajectory of ASMR in AYA breast cancer (EAPC: –0.41) demonstrated a more gradual decline compared to that observed in total breast cancer (EAPC: –0.62) [15].
The relatively stagnant trend of ASMR in AYA breast cancer could be partially explained by the occurrence of aggressive subtypes, drug resistance, germline mutations predisposing to cancer, and poor prognosis [16, 17]. Our findings strongly advocate for the prompt implementation of tailored measures and strategies to effectively prevent and manage AYA breast cancer. There is still no definitive screening strategy for AYA breast cancer. It is imperative to emphasize the lower efficacy of mammography for screening in this age group due to the prevalence of high breast density among AYA women [18, 19]. Several approaches may potentially be invaluable for detecting breast tumors earlier in this population, such as ultrasonography and magnetic resonance imaging (MRI) [20, 21]. However, the use of MRI is substantially constrained by its high cost and limited feasibility in economically disadvantaged regions. To overcome these limitations, alternative solutions warrant consideration, such as nurse-led clinical breast assessments or compact portable ultrasound systems.
Our research has indicated a positive correlation of SDI with ASPR and ASIR. In addition, an inverse relationship was found between EAPC of ASRs and SDI. It has been reported that airborne fine particulate matter is associated with higher risk for breast cancer [22]. Low-SDI regions may face environmental challenges such as air pollution, but this requires further study. The high burden of AYA breast cancer in low-SDI regions likely stems from population growth [6]. The combination of insufficient healthcare access and low health awareness has increased the burden of AYA breast cancer, resulting in pronounced inequities in disease outcomes. Therefore, it is vital to focus on individuals who are at risk in both high and low SDI countries in order to effectively mitigate the burden of AYA breast cancer.
Tobacco use and alcohol consumption were identified as essential risk factors for AYA breast cancer. Our research indicated a rising trend of ASMR related to tobacco exclusively in low-SDI regions, as well as an increasing trend of ASMR due to alcohol in middle, low-middle, and low-SDI regions. The highest proportion of AYA breast DALYs due to tobacco use was observed in Southern Sub-Saharan Africa, East Asia, and high-income Asia Pacific regions. Additionally, Western Europe, North Africa and the Middle East, and Eastern Sub-Saharan Africa displayed the greatest percentage of the DALYs attributed to alcohol.
Tobacco is known to contain a significant number of carcinogens and increase the risk of breast cancer risk [23, 24]. Even the most minute quantities of alcohol intake pose a significant threat in regard to the onset of breast cancer due to alteration of DNA methylation [25]. The implementation of tobacco and alcohol tax policies, marketing restrictions, and advertisement bans may be efficient in reducing tobacco consumption and decreasing mortality from AYA breast cancer [26, 27, 28].
There was an upward trajectory for ASDR that was attributed to increased fasting plasma glucose, low physical activity, and red meat consumption in the middle, low-middle, low-SDI regions. Appropriate physical activity is recognized as a protective factor. Low physical activity independently contributes to heightened susceptibility to multiple forms of cancer, including breast cancer [29]. The biological mechanisms associated with physical activity involve sex hormones, inflammation, metabolic function, immunity, and insulin sensitivity [30].
Increasing physical activity during the ages of 5–19 years could significantly mitigate breast-cancer risk, which highlights the importance of early physical exercise intervention and health awareness [31]. Inactive individuals demonstrate a higher likelihood of experiencing abnormal blood glucose levels compared to those who are active [32]. Processed and red meats have been positively linked with the risk of breast cancer, which is attributable to the iron content, estrogen, and mutagenic compounds in such meats [33]. Significant promise in decreasing breast-cancer risk has been reported for the adoption of a dietary regimen known as the Mediterranean diet, which is abundant in vegetables, fruits, fiber, and whole grains, while red meats are limited [34].
The challenges associated with breast cancer in younger adults are more complicated than those faced by older adults. First, AYA breast cancer is heavily influenced by specific cancer-susceptibility genes, including breast cancer 1/2 (BRCA1/2), ataxia telangiectasia mutated (ATM), checkpoint kinase 2 (CHEK2), rad50 double strand break repair protein (RAD50), nijmegen breakage syndrome 1 (NBS1), and brca1 interacting protein c-terminal helicase 1 (BRIP1), among others [35, 36]. According to the European Society of Medical Oncology (ESMO) guidelines, all patients with AYA breast cancer should receive genetic counselling [37]. The poly (adenosine diphosphate (ADP)-ribose) polymerase (PARP) inhibitor olaparib represents a viable adjuvant treatment option that is capable of improving clinical outcomes for carriers of BRCA mutation [38], but the optimal treatment strategy for this population requires further investigation. Another challenge in AYA breast cancer is that long-term treatment could result in infertility. Embryo or oocyte cryopreservation is one possible method for preserving fertility. Goserelin could also protect against ovarian failure and improve the likelihood of pregnancy [39]. AYAs also have a substantial burden of emotional and psychosocial repercussions after diagnosis of breast cancer.
Considering the multifaceted nature of the condition, our focus in this study extended beyond screening, diagnosis, treatment, and follow-up to encompass epidemiological characteristics. This study explored the most recent epidemiological patterns and primary risk factors of AYA breast cancer in hopes of effectively bridging the gap in knowledge in this field. However, there were some limitations to this study, which necessitate careful interpretation of the results. Our research was a secondary analysis that used data from the GBD database. Inevitably, our study was influenced by variations in data acquisition techniques and mammogram screening practices between different nations. The absence of nationwide cancer registries in several low-income regions substantially limited the availability of accurate epidemiological data necessary for assessing the true burden of cancer. The reliability of our findings was contingent upon the quality of the GBD data.
Additionally, breast cancer is a heterogeneous disease. Several vital clinicopathological features were unavailable in the GBD database, including human epidermal growth factor receptor 2, estrogen receptor, progesterone receptors, tumor size, lymph node, and grade. Due to the paucity of data, we excluded these characteristics from our analysis.
This study has presented a comprehensive appraisal of the burden of AYA breast cancer. The ASR trends showed variations based on SDI, age, risk factors, and geographical regions. The findings underscore the pressing need for rational resource allocation and appropriate policy establishment to address this disease, particularly in low and middle-SDI regions.
The data that support the findings of this study are available from the corresponding author upon request.
The authors’ responsibilities were as follows: XYF and TL designed the study. XYF, TL, and WJX extracted the data, performed the analyses, interpreted the evidence. XYF, WJX and TL revised the article. XYF and TL wrote the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG43313.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.