


1 Department of Anesthesia, Obstetrics & Gynecology Hospital, Fudan University, 200090 Shanghai, China
Abstract
Previous research has revealed that utilizing videos or images to educate primiparas about labor analgesia yields significantly superior results. WeChat supports various types of media, making it an ideal carrier for educational content. We have established a WeChat public account where educational content is presented through videos, images, and relevant scientific articles. We will investigate the effectiveness of WeChat public platform in primiparas analgesia education.
Primiparas were randomly assigned to either the WeChat public account education group (W group) or traditional bedside education group (B group). The labor analgesia knowledge questionnaires, self-rating anxiety scales, and the time taken for positioning were compared between the two groups. Additionally, satisfaction with labor analgesia was evaluated post-delivery.
A total of 90 primiparas were completed the study. Compared to the B group, primiparas in the W group had higher scores on labor analgesia knowledge questionnaire (55 ± 11.1 vs. 65 ± 9.2, p = 0.001), lower anxiety scores (51.4 ± 5.4 vs. 48.9 ± 4.6, p = 0.02), shorter positioning time (27.5 ± 7.9 s vs. 20.1 ± 9.2 s, p = 0.001) than those in the B group. The satisfaction of anesthesiologists with body positioning and the satisfaction of primiparas with labor analgesia were similar between the two groups.
The use of WeChat public platform for labor analgesia education can enhance primiparas understanding and cooperation during the procedure, decreasing maternal anxiety. It also benefits anesthesiologists by improving work efficiency. It has significant clinical value and promising prospects for promotion.
The study was registered with the Chinese Clinical Trial Registry (ChiCTR1900025231).
Keywords
- public platform
- primiparas
- anxiety
- labour analgesia
It is common for pregnant women to experience varying degrees of fear during childbirth [1]. Fear of labor refers to the negative perceptions and anxieties that pregnant women have about the process of giving birth. In China, more than 50% of pregnant women experience fear of labor [2]. Research has shown that strengthening health education and providing accurate information about labor analgesia can significantly reduce the fear of labor in primiparas, increase their confidence in labor, and increase their preference for natural childbirth [3].
Currently, the most effective and least harmful method for labor analgesia is intrathecal blockade [4]. Special positions for intrathecal blockade are important aspects of education [5]. However, traditional bedside education has limitations due to factors such as the duration of the analgesia, nurses’ communication skills, the ability of the primiparas to understand, and contraction pain. Our previous research revealed that using videos or pictures to educate primiparas about labor analgesia yields better results [6].
Like Facebook, Tencent’s free application WeChat, released in 2011, has become the most widely and frequently used social networking platform in China [7]. As a new media platform, WeChat enables the sending of various types of media, including text, voice, images, and videos, making it an ideal carrier for educational content [8]. The target audience for labor analgesia education is primiparas, who are young, and the WeChat public platform is more aligned with the lifestyle and communication habits of their age group. Therefore, we have established a WeChat public account called “Hong Fang Zi Anesthesia”, where educational content is presented through videos, images, and relevant scientific articles. We also compared the effectiveness of this approach with that of traditional bedside education methods.
The study was registered with the Chinese Clinical Trial Registry (ChiCTR1900025231) and conducted at the Obstetrics and Gynecology Hospital from August 2019 to December 2020. All participants provided informed consent, and the protocol was approved by the China Ethics Committee of Registering Clinical Trials (ChiECRCT20200030) in accordance with the Declaration of Helsinki.
Singleton full-term primiparas with American Society of Anesthesiologists (ASA) physical status II who were willing to receive labor analgesia in the delivery room were included. The exclusion criteria included contraindications to spinal anesthesia, communication barriers, inability to cooperate with the study protocol, physical activity disorders requiring positioning assistance (e.g., pubic symphysis separation), prior exposure to spinal anesthesia (e.g., history of spinal anesthesia surgery or health care workers), refusal to follow the WeChat public account, and primiparas who did not undergo or complete labor analgesia for various reasons, such as emergency cesarean section.
The participating anesthesia nurses sequentially numbered the enrolled primiparas and then, based on a random number table generated in Excel, randomly divided them into two groups. This table was created by first generating 90 random numbers with 1–90 numbering, and then sorting these numbers in descending order to produce a new list of numbered random numbers. Primiparas with sequence numbers in the first half of this list were assigned to Group W, while those in the second half were assigned to Group B.
WeChat education group (W group): Primiparas scanned the quick response (QR) code to follow our hospital’s “Red House Anesthesia” WeChat public account, which was maintained by our anesthesiology department. The platform included three main menus: before labor analgesia, during labor analgesia, and after labor analgesia. The submenus provided special positioning videos for anesthetic procedures, important notes for labor analgesia (marked as must-read), operational procedures for labor analgesia, related risks of labor analgesia, historical information about labor analgesia, and other educational articles on various topics in a concise and understandable manner through video, images, and text (Supplementary Fig. 1). Additionally, the WeChat public account provided convenient access to essential information for primiparas by setting up keyword-triggered links. Primiparas independently learned about labor analgesia by subscribing to the public account.
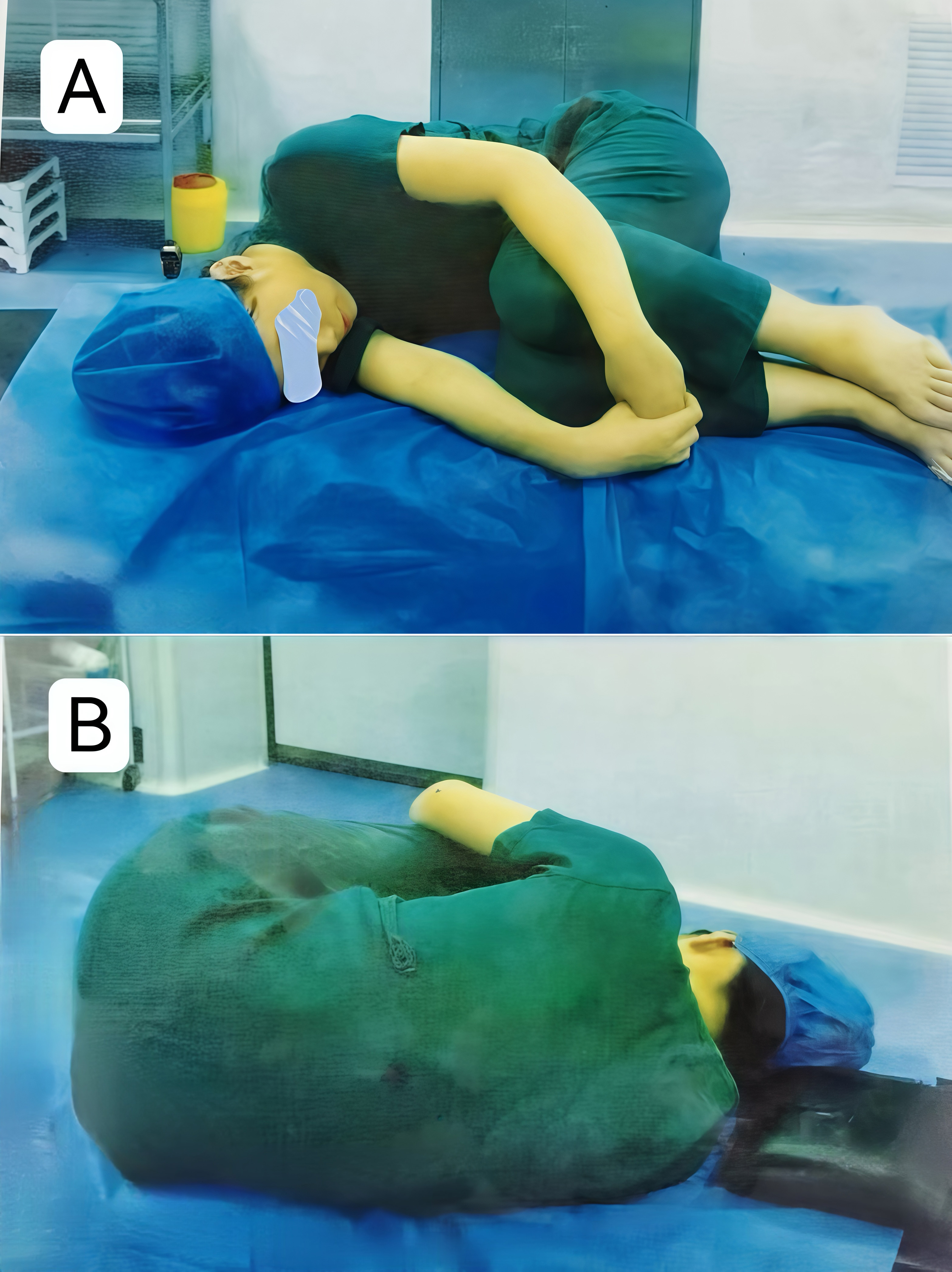
Bedside education group (B group): Traditional bedside education was conducted by a designated anesthesia nurse who verbally educated primiparas via the same images (Fig. 1A,B, Ref. [6]) or videos (Supplementary Video 1), which had showed in our previous study [6]. while providing instructions on labor analgesia positions and precautions.
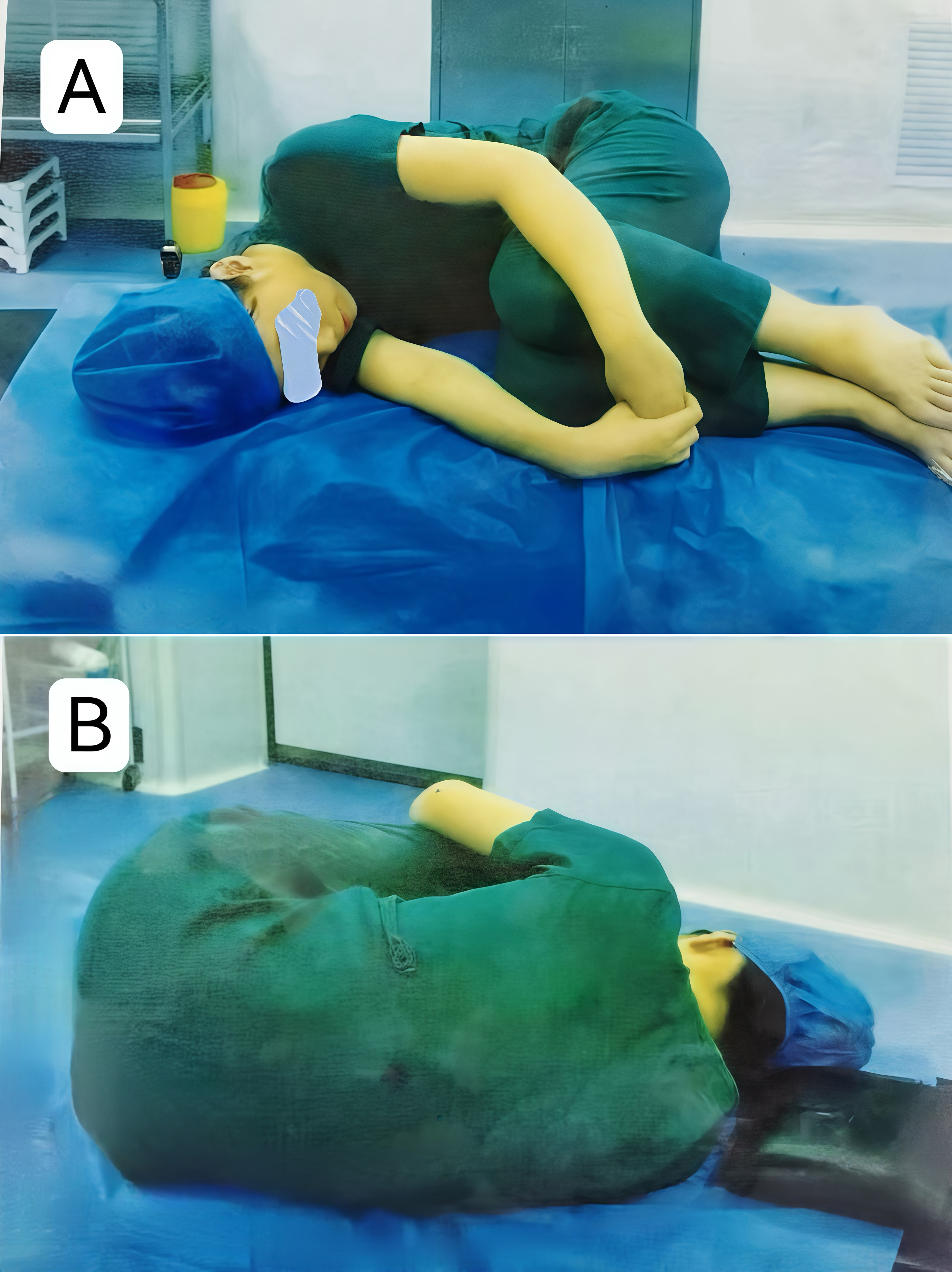 Fig. 1.
Fig. 1.
Educational pictures. Two images demonstrating the position from both the anterior and posterior perspectives [6]. (A) The position from an anterior perspective. (B) The position from a posterior perspective.
After entering the maternity ward, primiparas who met the inclusion criteria were introduced to the study by the anesthesia nurse responsible for the research. Those who agreed to participate signed informed consent forms and had their general condition recorded. Subsequently, education was provided according to the assigned groups. Before implementing labor analgesia, the anesthesia nurse documented their general condition while obtaining informed consent and distributing questionnaires on labor analgesia knowledge and self-assessed anxiety levels. During anesthetic preparation, the research anesthesiologist stood beside the primiparas’ head to ensure safety while recording the time taken for positioning. A senior anesthesiologist, who was not involved in the study and was solely responsible for spinal anesthesia, assessed and adjusted the primiparas’ position if necessary, without further timing. Both groups subsequently underwent conventional analgesic procedures with patient-controlled epidural analgesia pumps. After labor analgesia completion and removal of the epidural catheter, the W group received a satisfaction questionnaire through the platform, whereas the B group received a self-administered satisfaction questionnaire on labor analgesia from the anesthesia nurse.
A comprehensive comparison of labor analgesia education effects between the two groups was conducted in terms of the following aspects:
(1) A questionnaire on knowledge of labor analgesia was administered to assess the understanding level of primiparas. It consisted of 10 multiple-choice questions, with 10 points awarded for correct answers and no penalty for incorrect answers.
(2) A self-rating anxiety scale (SAS) was used to assess anxiety levels, with
standardized scores obtained after the questionnaires were collected. A SAS
standardized total score of
(3) Anesthesiologist satisfaction rating for operational positioning is based on four criteria: holding knees with both hands, bringing thighs close to the abdominal wall, bending the head toward the chest as much as possible, and maintaining a curved shape in the back while keeping it aligned vertically with the bed surface. If all the criteria are met without any further adjustment needed, it is considered satisfactory. If one criterion requires local adjustment, it is considered average. However, if two or more criteria require significant adjustment, it is considered unsatisfactory [6].
(4) Primiparas’ satisfaction questionnaire on labor analgesia: This questionnaire is clinically routine and involves overall satisfaction with labor analgesia, adverse reactions, effectiveness of analgesia during the second stage of labor, etc. Only satisfaction with labor analgesia (YES/NO) is compared.
Data analysis was performed via SPSS (Version 22.0, SPSS Inc., Chicago, IL,
USA). The distribution of univariate data was assessed using the
Kolmogorov‒Smirnov test. Normally distributed continuous data variables were
presented as the means
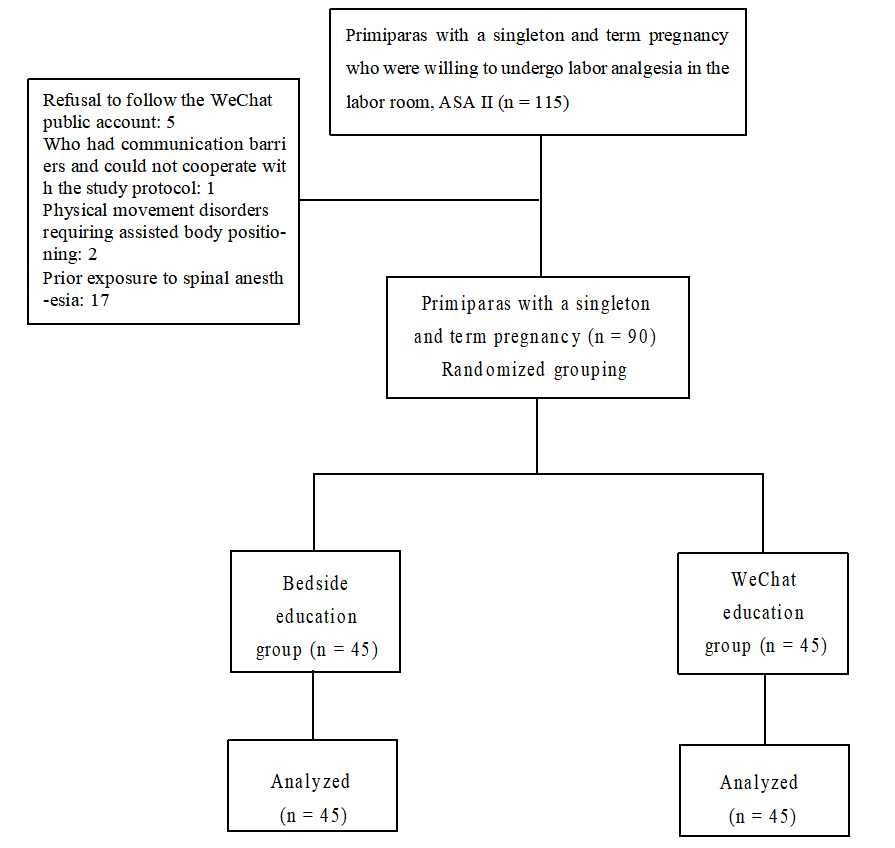
A total of 115 primiparas were initially recruited for the study. Twenty-five were excluded on the basis of the exclusion criteria, and 90 primiparas completed the study in the final statistical analysis, with 45 cases in each group (Fig. 2). A comparison of the demographic characteristics between the two groups is shown in Table 1, age of primiparas in the W group was slightly higher than that in the B group, and others were no significant difference between the two groups.
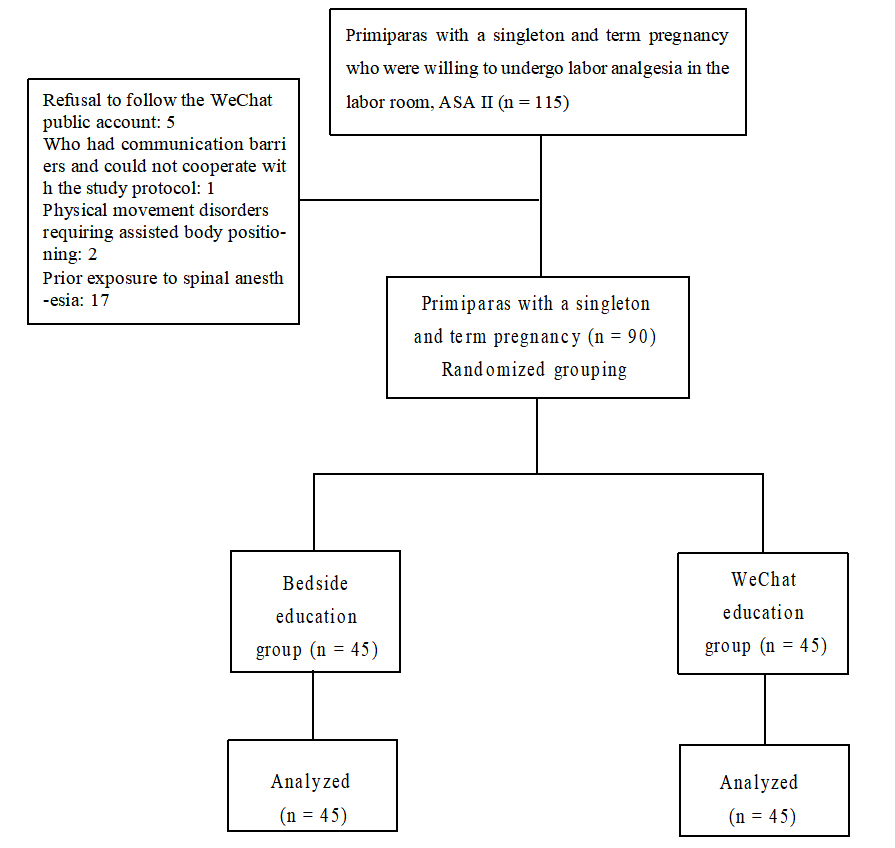 Fig. 2.
Fig. 2.
Flow chart. The flowchart illustrates the step-by-step process of this study. ASA, American Society of Anesthesiologists Physical Status.
| B group | W group | p | |
| n = 45 | n = 45 | ||
| Height (cm) | 163.8 |
163.7 |
0.91 |
| Weight (kg) | 70.7 |
69.0 |
0.52 |
| Age (years) | 29.2 |
30.7 |
0.03* |
| Weeks of gestation (weeks) | 39.4 |
39.6 |
0.43 |
| Educational background (high school or lower/university/graduate school) | 3/25/17 | 4/27/14 | 0.78 |
B group, bedside education group; W group, WeChat education group.
The values are the means
*Statistically significant difference between the two groups p
A comparison of labor analgesia education effects between the two groups is
shown in Table 2. Labor analgesia knowledge questionnaire scores were
significantly higher in the W group than in the B group (55
| B group | W group | p | |
| n = 45 | n = 45 | ||
| Questionnaire score on knowledge of labor analgesia | 55 |
65 |
0.001* |
| Self-rating anxiety scale | 51.4 |
48.9 |
0.02* |
| Positioning time (s) | 27.5 |
20.1 |
0.001* |
| Anesthesiologist satisfaction with positioning (satisfied/neutral/unsatisfied) | 20/21/4 | 28/14/3 | 0.237 |
| Satisfied with labor analgesia, n (%) | 39 (86.7%) | 43 (95.6%) | 0.266 |
B group, bedside education group; W group, WeChat education group.
The values are the means
*Statistically significant difference between the two groups p
This study revealed that primiparas who received labor analgesia education through WeChat public accounts had a better understanding of the educational content, lower SAS scores, and greater cooperation during the procedure, than those who received traditional bedside education.
According to previous studies, 83% of human information is obtained through vision, 11% through hearing, 3.5% through smell, 1.5% through touch, and 1% through taste. People are able to remember only 10% of what they read, 20% of what they hear, and 30% of what they see. However, in regard to audio‒visual content, 70% of the information is retained [10]. Previous studies have shown that using pictures and videos in preoperative care and patient education can lead to higher patient satisfaction and lower levels of preoperative anxiety [11, 12], which can ultimately improve patient outcomes [13]. The application of video education in preoperative anesthesia visits not only improves patient satisfaction and reduces preoperative anxiety [14], but also significantly shortens the duration of visits [15]. Anesthesiologists also demonstrate greater satisfaction with this approach [16]. Our previous studies confirmed the advantages of using videos and images in labor analgesia education [6]. However, bedside education that utilizes pictures and videos is time-consuming and limited by staffing resources, making it difficult to provide individualized care for multiple patients simultaneously.
The WeChat public account’s integration of video and imagery offers primiparas on-demand access to educational resources, facilitating repeated viewings and fundamentally resolving key issues. This strategy not only maintains the satisfaction of anesthesiologists with positioning and primiparas satisfaction with labor analgesia but also enables the content to be consumed on the primiparas’ own terms. This enhances the educational experience and alleviates labor anxiety.
Labor anxiety refers to the common emotions of tension, fear, and unease experienced by pregnant women during the perinatal period. This anxiety may affect the physical and mental health of the pregnant woman and even the health of the fetus. Lack of understanding of the labor process and fear of pain are likely the main reasons for labor anxiety. Studies have shown that as full-term primiparas gradually enter labor, a lack of accurate knowledge about pain relief can further deepen the fear of childbirth [17], increasing labor anxiety. The WeChat public platform, while featuring videos and images, also enhances its content with text-based popular science knowledge related to labor analgesia. Education is no longer limited by time, space, or human resources, and can be watched repeatedly. This is why primiparas in Group W had a better understanding of the educational content, lower anxiety scores, and shorter times for positioning during the procedure.
With increasing public health awareness, new media as a means of obtaining health-related information will become increasingly popular [18]. WeChat is an effective platform for building communication between hospitals and patients [19, 20], with notable advantages in hospital health education [21, 22]. Like Facebook’s use in public health management [23, 24], the WeChat public platform has been utilized in chronic disease management, such as coronary heart disease [25, 26] and perioperative care for surgical patients [27, 28]. However, this is the first study to apply the WeChat public platform to health education for primiparas in labor analgesia. This confirms the superiority of the Hong Fang Zi Anesthesia Public Account in labor analgesia education, and it has clinical promotion value for the use of the WeChat public account to conduct labor analgesia education for primiparas.
Limitations and future directions: (1) Statistical findings revealed that the average age of primiparas in the W group was slightly higher than that in the B group, while other demographic characteristics were similar, which did not affect the main conclusions. Additionally, younger age may be associated with a higher acceptance of new media, potentially leading to better educational outcomes. (2) The study was conducted at the maternity ward, with education effectiveness tied to uterine contraction frequency and intensity. Future research should consider advancing education to the last prenatal visit for better outcomes. (3) Questionnaire scores were used as observation indicators, potentially introducing subjective bias. However, anesthesia timing and satisfaction scores from anesthesiologists enhanced objectivity. Future studies could employ more objective evaluation measures. (4) WeChat public platform functions, such as adding groups for mutual learning among primiparas and expanding knowledge dissemination to family members, were underutilized. With ongoing improvements, dynamic management during labor and postoperative follow-up can be expanded.
The use of the WeChat public platform for maternal labor analgesia education can increase maternal mastery of educational content, improve cooperation during labor analgesia procedures, reduce maternal anxiety, and benefit anesthesiologists by improving work efficiency. This approach has clinical value and broad development prospects.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
LJM, YC and CY designed the research study. LJM and YC performed the research. HLL and WJY was responsible for the conception of the analysis and interpretation of the results. CY provided substantial contributions with respect to analysis and interpretation of the results and to revising the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the China Ethics Committee of Registering Clinical Trials (ChiECRCT20200030).
We sincerely appreciate the selfless support and invaluable assistance of Professor Huang Shaoqiang, Director of Anesthesiology Department at the Obstetrics and Gynecology Hospital affiliated to Fudan University, for our research work.
This research was supported by Clinical Research Program of Obstetrics and Gynecology Hospital of Fudan University (NO: FC2021CR206).
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG26052.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.