

1 Department of Prenatal Diagnostic Laboratory, The Fourth Hospital of Shijiazhuang (Shijiazhuang Obstetrics and Gynecology Hospital), 050000 Shijiazhuang, Hebei, China
Abstract
The purpose of the study was to explore the relationship between sudden sensorineural hearing loss (SSNHL) and serum sex hormone levels in perimenopausal women, as well as to further investigate the influence of these indicators for SSNHL in perimenopausal women.
A total of 156 patients with SSNHL and 149 healthy individuals during perimenopause who received treatment or underwent physical examination in the Fourth Hospital of Shijiazhuang from August 2023 to December 2023 were selected to participate in this retrospective cohort study. The variances in fundamental patient data were analyzed using the Mann-Whitney U test and Chi-square test. We employed multivariate logistic regression to examine the association between serum levels of follicle stimulating hormone (FSH), luteinizing hormone (LH), estradiol (E2), progesterone (P), testosterone (T), prolactin (PRL) levels and the occurrence of SSNHL in perimenopausal women. Spearman analysis was used to analyze the correlation between perimenopausal women serum sex hormone levels and SSNH.
Compared to the non SSNHL group, the SSNHL group women had lower serum levels of E2 and P ((35.08 ± 12.49) pmoL/L and (0.63 ± 0.24) nmoL/L) vs. ((43.46 ± 10.17) pmoL/L and (0.84 ± 0.13) nmoL/L) (p < 0.05). Multiple logistic regression analysis demonstrated that E2 and P were both at higher risk with the development of SSNHL. Spearman correlation analysis found that E2 and P are negatively correlated with pure tone hearing threshold in perimenopausal women.
SSNHL in perimenopausal women may be related to their serum levels of sex hormones.
Keywords
- sudden sensorineural hearing loss
- perimenopausal
- sex hormones
Sudden sensorineural hearing loss (SSNHL) is a common clinical disease, defined
as sudden and unexplained sensorineural hearing loss that occurs within 72 hours
and affects at least two adjacent frequencies with a hearing loss of
The relationship between hormonal changes and hearing loss has been reported in previous studies [9, 10]. For example, when a woman is pregnant, the secretion of estrogen and progesterone in the body will significantly increase. These changes in female hormones will cause excessive retention of salt and water, which will lead to a significant increase in extracellular fluid volume, thus increasing the probability of hearing loss [11]. When hormonal fluctuations occur in the cochlea, the chemical components of endolymphatic and periauricular fluid can also be disturbed. Although many studies have suggested that sex hormones may interfere with cochlear microcirculation and contribute to sudden hearing loss, the correlation analysis between sex hormone levels and hearing loss is still uncertain [12]. This study explored the relationship between SSNHL and serum sex hormone (follicle stimulating hormone (FSH), luteinizing hormone (LH), estradiol (E2), progesterone (P), testosterone (T), prolactin (PRL)) levels in perimenopausal women, which can be used to guide the diagnosis and treatment of female SSNHL patients.
A total of 156 patients with SSNHL and 149 healthy individuals during
perimenopause who received treatment or underwent physical examination in the
Fourth Hospital of Shijiazhuang from August 2023 to December 2023 were selected
to participate in this retrospective cohort study. The average age of patients in
the SSNHL study group was 51.62
| Variables | Control (n = 149) | SSNHL (n = 156) | p-value | |
| BMI (kg/m2) | ||||
| 51 (34.2) | 57 (36.5) | 0.673b | ||
| 98 (65.8) | 99 (63.5) | |||
| Years of education (n%) | ||||
| 85 (57.0) | 87 (55.8) | 0.822b | ||
| 64 (43.0) | 69 (44.2) | |||
| Family yearly income (n%) | ||||
| 71 (47.7) | 79 (50.6) | 0.602b | ||
| 78 (52.3) | 77 (49.3) | |||
| Drinking | ||||
| Yes | 23 (15.4) | 36 (23.1) | 0.091b | |
| No | 126 (84.6) | 120 (76.9) | ||
| Migraine | ||||
| Yes | 8 (5.4) | 22 (14.1) | 0.010b | |
| No | 141 (94.6) | 134 (85.9) | ||
| Family history of diabetes | ||||
| Yes | 12 (8.1) | 16 (10.3) | 0.505b | |
| No | 137 (91.9) | 140 (89.7) | ||
| Smoking | ||||
| Yes | 5 (3.4) | 11 (7.1) | 0.148b | |
| No | 144 (96.6) | 145 (92.9) | ||
| Calcium (mmol/L) | 2.15 (2.10–2.21) | 2.12 (2.08–2.16) | 0.037a | |
| Iron (μmol/L) | 11.52 (7.45–16.18) | 11.39 (7.15–15.84) | 0.514a | |
| Zinc (μmol/L) | 6.13 (5.04–7.82) | 6.29 (5.37–7.46) | 0.153a | |
| Copper (μmol/L) | 29.04 (25.36–34.17) | 27.98 (23.14–35.71) | 0.278a | |
| CRP (mg/L) | 54.38 (24.73–77.19) | 59.76 (28.19–80.49) | 0.026a | |
BMI, body mass index; CNY, Chinese Yuan; CRP, C-reactive protein; SSNHL, sudden sensorineural hearing loss.
The differences between the SSNHL and Control groups were obtained using the
Mann-Whitney U test (a) and the Chi-square test (b), p
The definition of SSNHL utilized in this study is a sensorineural hearing loss
of
The selection criteria for the perimenopausal period were adult women aged 40 to
60 years old, and the menstrual changes complied with the following conditions:
5 mL of venous blood was collected from all patients fasting in the early morning, and the serum was collected after centrifugation. Electrochemiluminescence method (Chemiluminescence instrument, Hormone detection kits, Roche Diagnostics GmbH, Mannheim, Germany) was used to detect FSH, LH, E2, P, T, and PRL levels. The range and intra and inter-assay coefficients of variability for the test indicators used in the study are shown in the Table 2.
| FSH (IU/L) | LH (IU/L) | E2 (pmol/L) | P (nmol/L) | T (nmol/L) | PRL (nmol/L) | |
| Range | 0.3–200 | 0.1–200 | 0.2–200 | 0.02–20 | 0.01–20 | 0.002–21.4 |
| Intra-assay | 1.3–1.9 | 0.6–1.2 | 1.4–2.3 | 1.2–1.9 | 0.8–1.7 | 1.3–3.0 |
| Inter-assay | 3.2–4.1 | 1.6–2.2 | 2.1–4.6 | 2.3–5.1 | 1.5–3.3 | 1.9–5.2 |
FSH, follicle stimulating hormone; LH, luteinizing hormone; E2, estradiol; P, progesterone; T, testosterone; PRL, prolactin.
We utilized SPSS 22.0 (IBM-SPSS Statistics, Chicago, IL, USA) for conducting
statistical analysis on the data. The median (range) and frequencies (percentage)
were used to describe continuous and categorical variables, respectively. The
Mann-Whitney U test was employed to assess the significant variance among
non-normally distributed continuous variables, while Chi-square test was utilized
for comparing categorical variables. Multivariate logistic regression analysis
was conducted to examine the association between SSNHL and FSH, LH, E2, P, T, and
PRL respectively. The Pearson analysis method was used for correlation analysis.
All statistical analyses with significant differences were considered to be
p
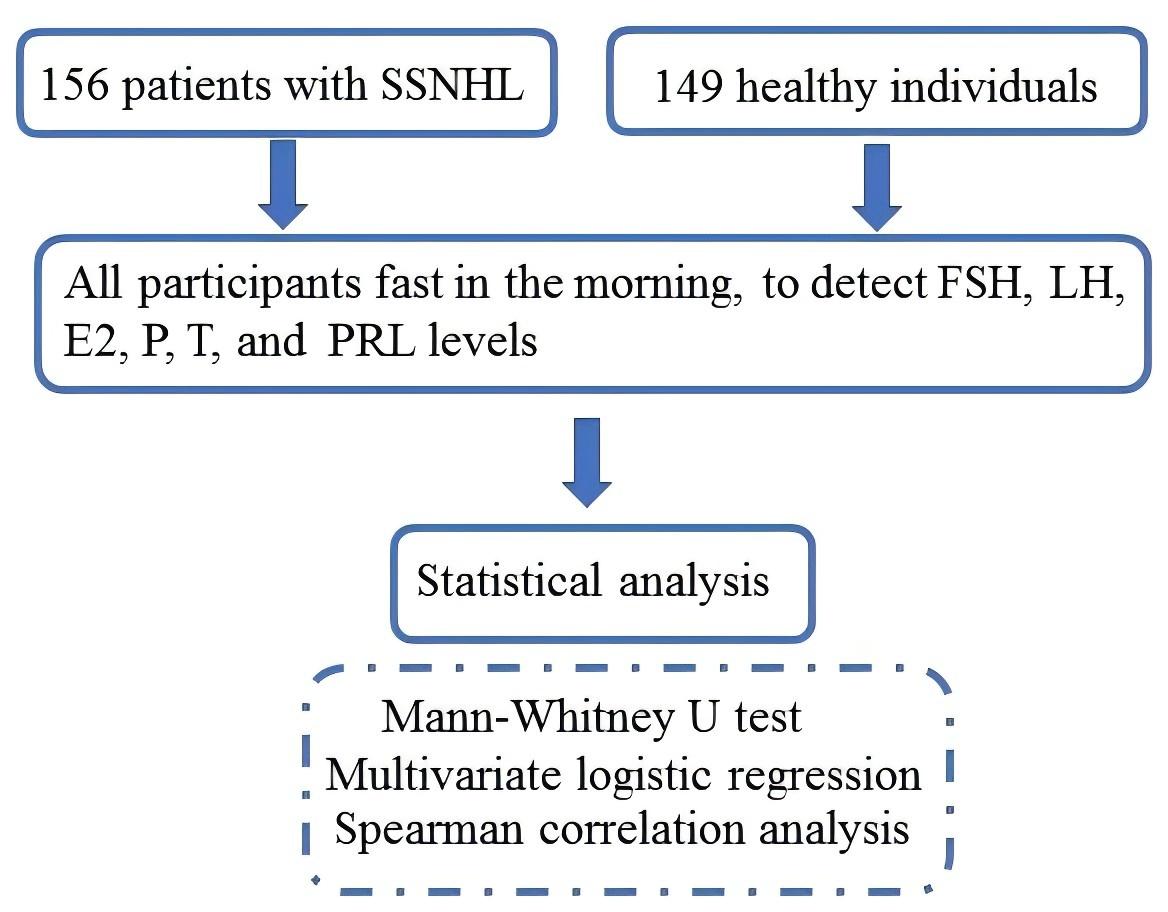
According to the inclusion and exclusion criteria, 305 participants were analyzed finally. Flow chart of participants participation in the study was showed in Fig. 1.
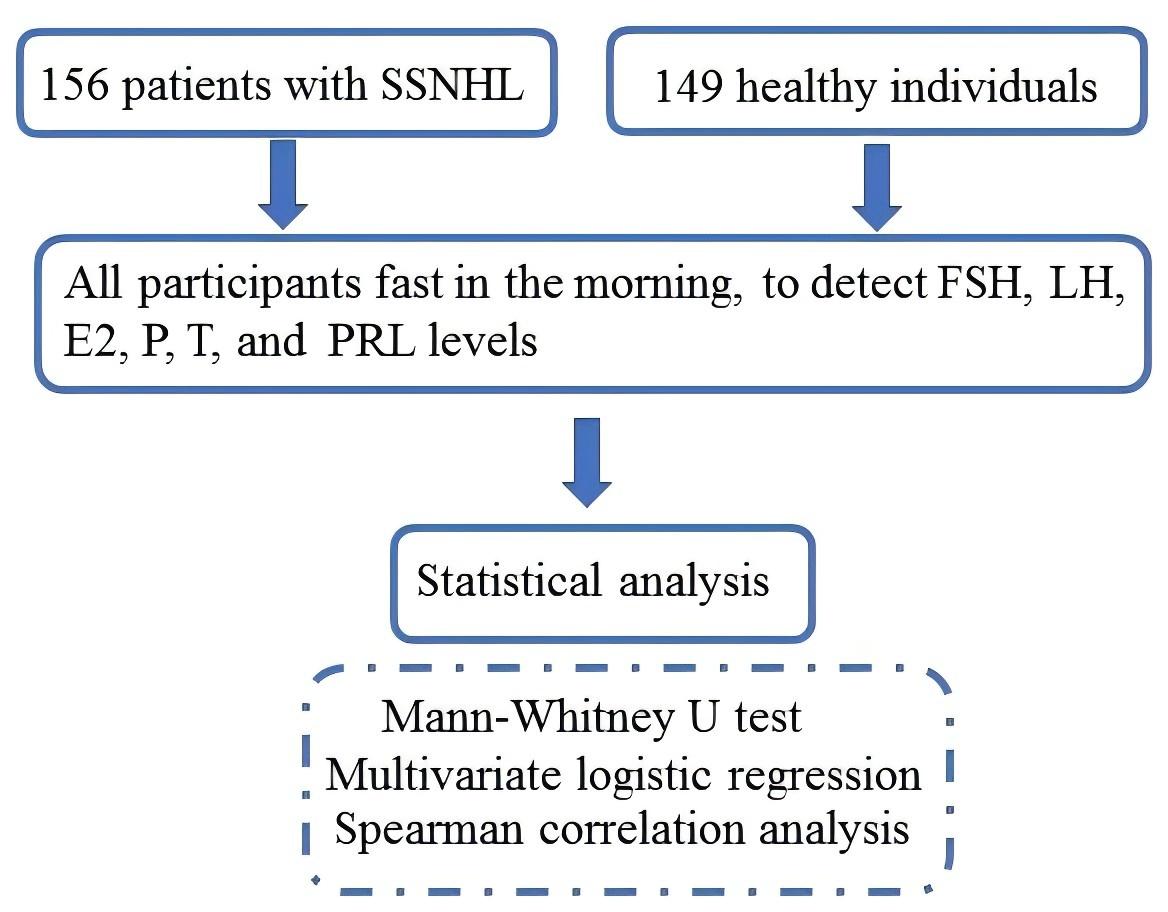 Fig. 1.
Fig. 1.
Flow chart of participants participation in the study. SSNHL, sudden sensorineural hearing loss; FSH, follicle stimulating hormone; LH, luteinizing hormone; E2, estradiol; P, progesterone; T, testosterone; PRL, prolactin.
We compared the sex hormone levels between SSNHL and normal controls in Table 3.
We found that the E2 and P levels in the SSNHL group were significantly lower
than those in the control group (p
| Variables | Control (n = 149) | SSNHL (n = 156) | p-value |
| FSH (IU/L) | 57.63 (42.37–70.56) | 57.12 (40.68–72.45) | 0.468 |
| LH (IU/L) | 36.55 (28.17–45.72) | 36.71 (26.51–45.98) | 0.377 |
| E2 (pmol/L) | 43.46 (38.49–60.71) | 35.08 (32.26–59.14) | 0.002 |
| P (nmol/L) | 0.84 (0.54–1.18) | 0.63 (0.31–0.97) | |
| T (nmol/L) | 0.62 (0.26–1.11) | 0.59 (0.24–0.93) | 0.073 |
| PRL (nmol/L) | 0.45 (0.27–0.73) | 0.44 (0.15–0.76) | 0.249 |
FSH, follicle stimulating hormone; LH, luteinizing hormone; E2, estradiol; P, progesterone; T, testosterone; PRL, prolactin.
The average pure tone hearing threshold of 156 patients in the perimenopausal
group was 56.74
| Variables | r | p-value |
| FSH (U/L) | –0.016 | 0.563 |
| LH (U/L) | 0.029 | 0.495 |
| E2 (pmol/L) | –0.277 | |
| P (nmol/L) | –0.312 | |
| T (nmol/L) | –0.046 | 0.423 |
| PRL (nmol/L) | –0.021 | 0.529 |
FSH, follicle stimulating hormone; LH, luteinizing hormone; E2, estradiol; P, progesterone; T, testosterone; PRL, prolactin; r, correlation coefficient.
We further performed a logistic regression analysis of the associations between
E2, P and the risk of SSNHL. Based on the mean concentration of all 305 subjects,
E2 and P were categorized into high-value and low-value groups, respectively, and
these groups were subsequently incorporated into the regression analysis as
categorical variables. The results revealed that E2 and P were associated with
the risk of SSNHL in either Model 1 (univariate regression analysis) and Model 2
(adjusted for maternal gestational age, body mass index (BMI), reproductive
history, FSH, LH) (p
| Variables | Model 1 | Model 2 | |||
| OR (95% CI) | p-value | OR (95% CI) | p-value | ||
| E2 | 1.058 (1.026–1.091) | 1.043 (1.012–1.059) | |||
| P | 1.035 (1.021–1.059) | 1.030 (1.010–1.048) | |||
E2, Estradiol; P, progesterone; OR, odds ratio; CI, confidence interval.
SSNHL affects a wide range of people and is common in middle-aged and elderly individuals. Internal ear circulation disorders, microvascular dysfunction and metabolic disorders are widely recognized as pathological mechanisms [14, 15]. Moreover, SSNHL is associated with platelet aggregation, activation, and abnormal lipid metabolism, and abnormal hormonal regulation may be the underlying cause of such metabolic abnormalities [16]. Perimenopause is a special stage for women, as their ovarian endocrine function begins to decline and sex hormone indicators begins to change, leading to a series of pathologies in various tissues and systems of the body [17, 18]. Therefore, it is imperative to study the correlation between hormone levels and sudden deafness in perimenopausal women.
In this study, we found that E2 and P levels were significantly decreased in perimenopausal women with SSNHL. It has been reported that estrogen receptors are widely expressed in the human inner ear in cochlear hair cells, spiral ganglia, vascular cords, spiral arteries, outer hair cells and inner hair cells [19]. This implies that women’s auditory function is related to fluctuations in estrogen. It is through these receptors that estrogen regulates the blood supply to the inner ear. When estrogen levels suddenly decrease, these receptors increase the blood viscosity in the inner ear, which not only affects the microcirculation of the inner ear, but also increases the risk of thrombosis [20, 21]. Yadav et al. [22] studied the relationship between menstrual cycle and female hearing, and found that female hearing was affected by the changes of estrogen and progesterone levels during the menstrual cycle. Kim et al. [23] conducted a study on perimenopausal women and found that these patients faced greater risk of hearing loss as the levels of E2 decreased in the body. The aforementioned reports bear similarities to the present study. Some researchers suggest that estrogen exerts a protective effect on nerve cells. As estrogen levels decline, this protective effect diminishes, and the vasomotor function becomes less stable, as a result, it may adversely affect hearing [24].
The study applied Spearman correlation analysis between sex hormones and pure
tone hearing threshold in perimenopausal women. We found that perimenopausal
women P and E2 levels were negatively associated with pure tone hearing threshold
values. Logistic regression analysis showed that E2 (odds ratio (OR) = 1.043,
p
By monitoring sex hormone indicators, it is helpful for clinicians to analyze the pathogenesis, therapeutic measures, and prognosis of perimenopausal patients with SSNHL. However, the effects of estrogen changes on the body are multifaceted, and the etiology and pathogenesis of perimenopausal SSNHL still need to be further investigated.
In conclusion, we demonstrate that E2 and P levels in the SSNHL patients were significantly lower than those in the normal perimenopausal women. No significant difference in FSH, LH, T, and PRL between the two groups. P and E2 levels in perimenopausal women were negatively associated with pure tone hearing threshold values. Perimenopausal women serum E2 and P were independent risk factors for SSNHL. Of course, our research also has certain shortcomings, such as the absence of data pertaining to the treatment process of SSNHL and the influence of hormone therapy on SSNHL. However, our research to some extent demonstrates the relationship between SSNHL and serum sex hormone levels in permanent women, which plays a significant role in guiding the diagnosis and treatment of female patients with SSNHL.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
SXW designed the research study. SXW and KW performed the research. DLS and JZ analyzed the data. SXW and DLS wrote the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the fourth Hospital of Shijiazhuang (20200133). The manuscript was a retrospective case review, and consent to participate was not applicable.
The authors would like to offer sincere thanks to a large team who worked together which included technical help, writing assistance and departmental head for their general support.
The study was funded by the Key Medical Scientific Research Project of Hebei province (No. 20231684).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.