




1 School of Nursing, Guangdong Pharmaceutical University, 510310 Guangzhou, Guangdong, China
Academic Editor: Johannes Ott
Abstract
Background: To evaluate the preventive effect of different exercise
programs on perinatal depression and to provide practical suggestions to guide
the maternal daily exercise plan. Methods: Nine electronic bibliographic
databases were searched from inception until 18 January 2022. Meta-analysis of
all data was performed using RevMan 5.4. Results: Sixteen RCTs
consisting of 2233 maternal cases were included. Compared to women in the control
group, women who received exercise effectively prevented maternal perinatal
depression (Std. mean difference [SMD] = –1.31, 95% confidence interval [CI]
–1.40 to –1.21). Prenatal exercise (SMD = –1.45), aerobic
exercise (SMD = –1.78), personal exercise (SMD = –2.03),
Keywords
- exercise
- perinatal depression
- preventive effect
- meta-analysis
Perinatal depression (PDN) is a psychiatric disorder that occurs during pregnancy (prenatal depression) or within one year after delivery (postpartum depression (PPD)) [1, 2]. The prevalence of PDN ranges from 11.4% to 17.4% worldwide [3, 4]. PDN can directly affect maternal health and pregnancy outcomes [5]. Therefore, preventing the occurrence of PDN becomes particularly important.
At present, the primary methods to treat PDN include drug treatment and psychotherapy; however, there are side effects of drug intervention, and the cost of psychotherapy is relatively high. Exercise intervention has the advantage of low cost and is easy to complete, attracting wide attention from scholars at home and abroad [6]. Studies have shown that exercise intervention can relieve PDN; however, existing research primarily focuses on the effect of exercise on improving the symptoms of perinatal women with a history of depression [7]. There are few reports of perinatal women with no history of depression before pregnancy being able to prevent depression by exercising during the perinatal period. This study conducts a meta-analysis of perinatal exercise research and reveals the prevention effect of exercise on PDN, analyzes the influence of different exercise programs on PDN, and explores an ideal exercise plan to prevent PDN.
The systematic review and meta-analysis were conducted following the PRISMA guidelines [8] and registered at the International Prospective Register of Systematic Reviews (CRD42022314645).
We systematically searched five English databases (PubMed, Web of Science, The Cochrane Library, EBSCO, and APA/PsycNET) and four Chinese databases (CNKI, CBM, WanFang, and VIP) from their inception to 18 January 2022. Three groups of terms were combined according to the syntax rules for each database: (1) Perinatal period-related terms, including puerpera, pregnancy, expectant mother, antenatal, postpartum period, puerperium, postpartum care, postnatal care, and perinatal care; (2) exercise-related terms, including sports, exercise, physical activity, movement behavior, yoga, walking, running, jogging, swimming, aerobic, anaerobic, and pilates; (3) depression-related terms, including depressive symptoms, depression, depressive disorder, PDN, baby blues, mental health, psychological health, psychological function, mental function, and psychological. In addition to the digital bibliographic databases, we searched the Chinese clinical trial registry and World Health Organization (WHO) international clinical trial registry for unpublished trials relevant to this systematic review.
(1) Pregnant women and women within one year after delivery were included. (2)
Patients with psychiatric disorders were excluded. (3) Pregnant women with a
history of depression, that is, if they met one of the following criteria, were
excluded: ① score
The women in the intervention group underwent regular exercise for a fixed period. The various sub-elements analyzed included exercise start time, exercise content, exercise frequency, practice form, and duration of exercise.
The women in the control group received routine care, including psychological care and health education, but did not practice any form of exercise intervention.
The primary outcome measure was depression symptoms, determined using the
following scales: Edinburgh Postpartum Depression Scale (EPDS)
Randomized control trials (RCTs) were included.
Endnote X9 software (Thomson Scientific, Philadelphia, PA, USA) was used to import all references and remove duplicates. Two independent authors evaluated the remaining studies according to inclusion and exclusion criteria first by screening the abstract and then the full text of potentially relevant papers. Any disagreements with respect to eligibility were resolved by a third independent author (H.C.H.).
Two authors (S.Y.M. and Y.L.) independently evaluated the risk of bias of eligible studies using the Cochrane Risk of Bias assessment tool [9], which evaluates for presence of selection bias, performance bias, detection bias, attrition bias, reporting bias, and other biases. According to the evaluation criteria, each item was classified as low, high, and unclear. Any disagreements were resolved by a third independent author (X.Y.Y.).
Two authors (S.Y.M. and Y.L.) independently extracted relevant data from eligible articles, including the author, sample size, age, intervention, control, start time of exercise, exercise content, exercise frequency, practice form, single duration of exercise and results. Any differences between the two authors (S.Y.M. and Y.L.) were resolved by a third author (X.Y.Y.).
Statistical analysis was performed using RevMan 5.4 (Nordic Cochrane Centre,
Hillerød, Denmark). Std. Mean differences (SMDs) and 95% confidence intervals
(CIs) were calculated for continuous results. I
This search strategy yielded 4596 potentially relevant citations from the nine electronic databases. Following the removal of 651 duplicate records, 3661 articles were excluded based on the selection of titles and abstracts, and the remaining 284 studies were evaluated in full text. Another 268 studies were excluded from the full text evaluation and a total of sixteen studies [12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27] were included in the final analysis (Fig. 1).
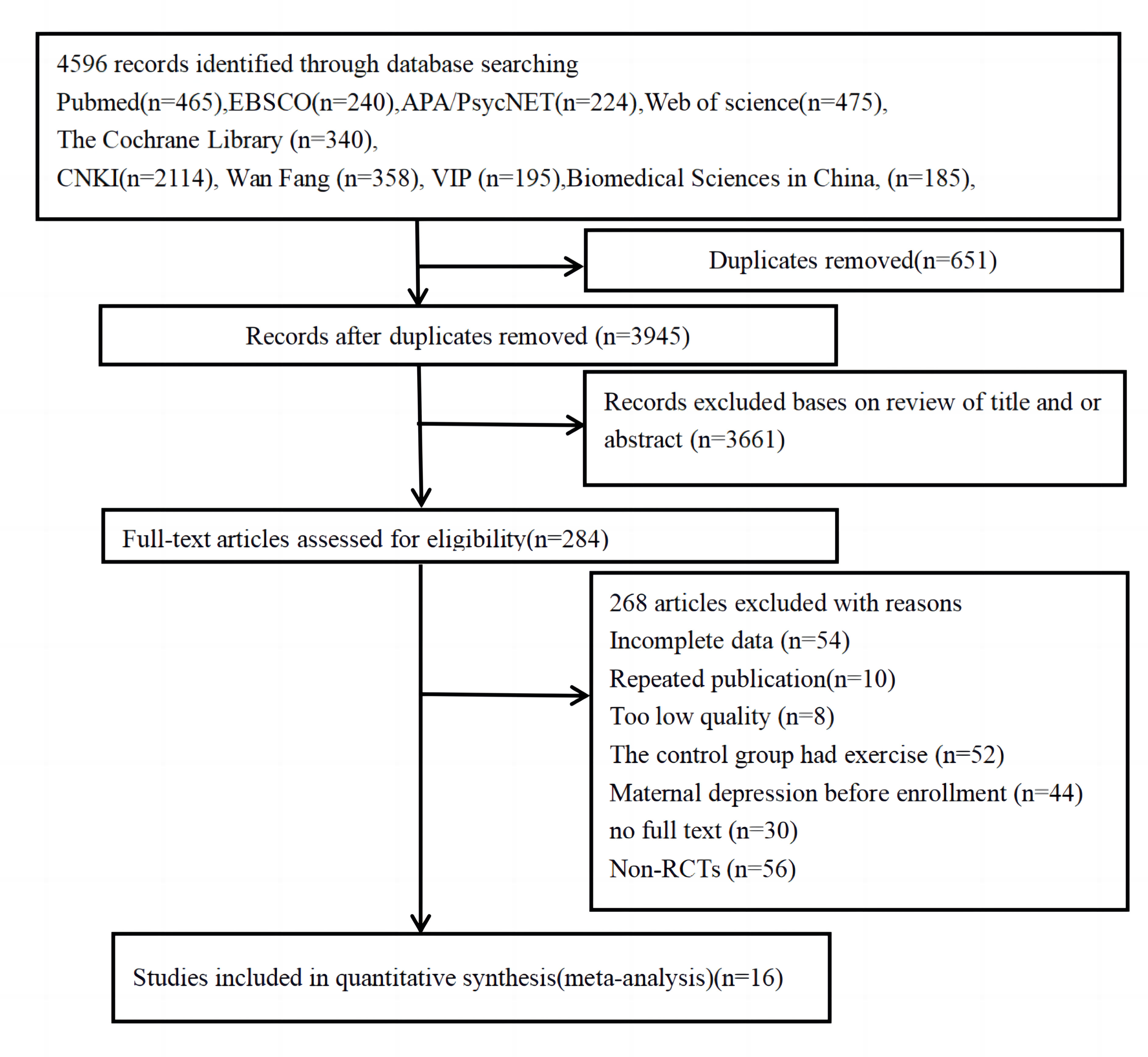 Fig. 1.
Fig. 1.Database search flow diagram.
A total of 16 randomized controlled trials (RCTs) were selected for analysis. The RCTs were conducted in four countries—China, Spain, the U.S. and Australia—and published between 2010–2021. The studies included 2233 participants [12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27]): 1124 (50.3%) in the intervention group and 1109 (49.7%) in the control group. The participants’ age ranged from 25 to 37. The baseline characteristics of the 16 RCTs were comparable between the two groups, and each RCT evaluated the preventive effect of exercise on PDN. A detailed summary is shown in Table 1 (Ref. [12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27]).
| First author | Particular year | Country/ region | Age | Sample capacity | Exercise programs | Outcomes | ||||||
| I | C | I | C | Start time | Content | Frequency | Duration | Form | ||||
| Gao [14] | 2021 | China | 27.92 |
28.63 |
19 | 12 | postpartum | yoga | personal | ① | ||
| Yan [12] | 2021 | China | 36.65 |
36.85 |
100 | 106 | prenatal | dance gymnastics | 30–60 min | combination | ① | |
| Wu [19] | 2019 | China | 32.24 |
32.6 |
34 | 35 | prenatal | aerobic exercise | 30–60 min | combination | ④ | |
| Hu [15] | 2020 | China | 25.16 |
25.08 |
49 | 49 | prenatal | aerobic exercise | combination | ④ | ||
| Tang [25] | 2014 | China | 23 |
100 | 100 | prenatal | dance gymnastics | personal | ④ | |||
| Ming [20] | 2019 | China | 26.35 |
27.85 |
80 | 80 | prenatal | dance gymnastics | N/A | personal | ③ | |
| Huang [16] | 2020 | China | 280 | 280 | prenatal | aerobic exercise | group | ① | ||||
| Fan [22] | 2017 | China | 25.89 |
26.02 |
80 | 80 | prenatal | yoga | N/A | personal | ④ | |
| Li [13] | 2021 | China | 31.15 |
30.21 |
40 | 40 | prenatal | aerobic exercise | N/A | N/A | ④ | |
| Wang [23] | 2017 | China | 34.33 |
31.82 |
30 | 30 | prenatal | aerobic exercise | N/A | ④ | ||
| Rodriguez [17] | 2020 | Spain | 32.12 |
30.58 |
65 | 64 | prenatal | water sports | group | ⑤ | ||
| Gallagher [18] | 2019 | USA | 30.44 |
27.65 |
48 | 31 | prenatal | yoga | personal | ③ | ||
| Yi [27] | 2007 | TaiWan | 34.17 |
34.33 |
31 | 30 | prenatal | yoga | group | ② | ||
| Norman [26] | 2010 | Australia | 29.3 |
30.1 |
62 | 73 | postpartum | strength exercise | group | ① | ||
| Aguilar [21] | 2018 | Spain | 34.52 |
33.67 |
16 | 22 | prenatal | water sports | group | ① | ||
| Perales [24] | 2014 | Spain | 31.08 |
31.66 + 3.86 | 90 | 77 | prenatal | aerobic exercise | 30–60 min | N/A | ② | |
| Note: I: Intervention Group; C: Control Group; ① EPDS; ② CES-D; ③ HADS; ④ SDS; ⑤ HRQOL . | ||||||||||||
The risk of bias analysis for the included RCTs is summarized in Fig. 2. Nine RCTs described the use of the random number table method to generate random sequences, and five RCTs described the use of the sealed envelope method for allocation and concealment. Of all RCTs, 14 RCTs had their patients and staff blinded, and six RCTs had their calculation results blinded. The results of 16 RCTs were considered complete and confirmed as low risk. Eight selective reporting for those RCTs were determined as unclear risk. 16 RCTs had a low risk in other possible biases.
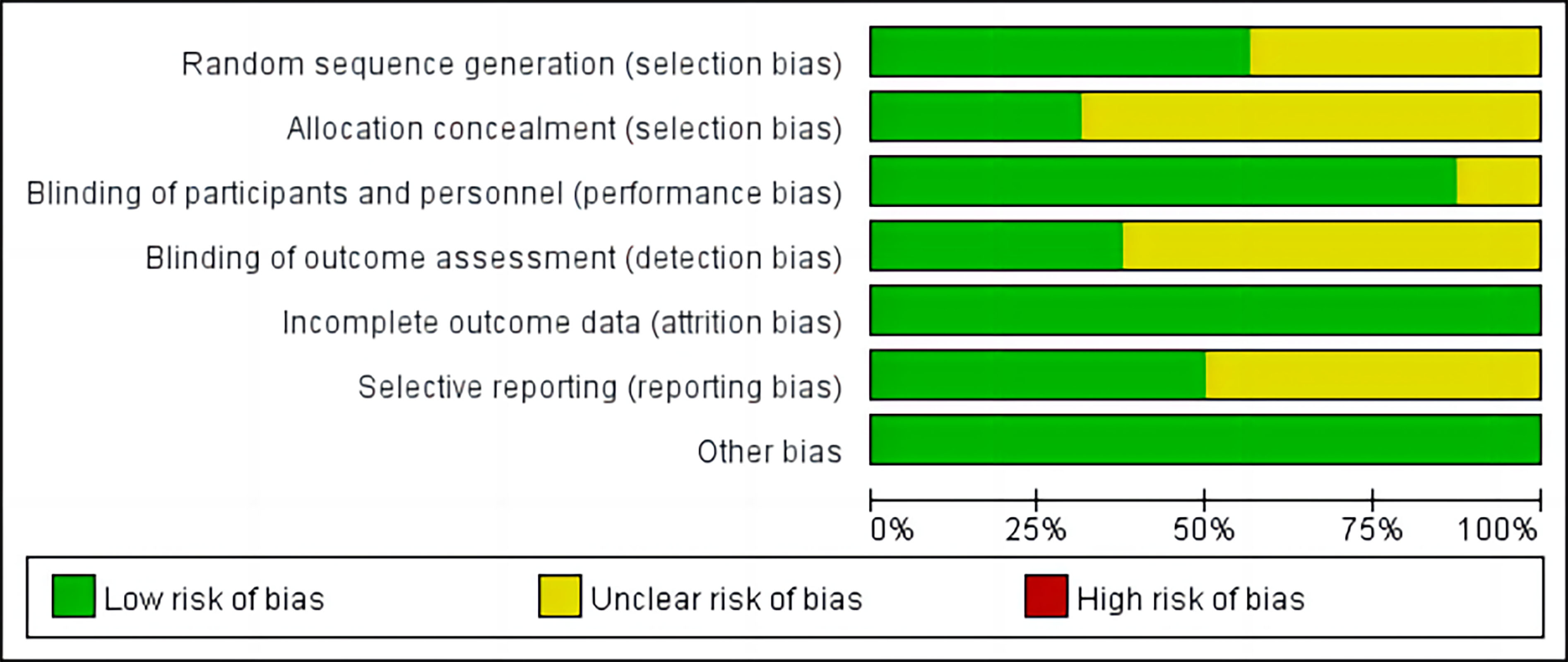 Fig. 2.
Fig. 2.Risk of bias graph.
16 RCTs were compared between the intervention group and the control group to
evaluate the preventive effect of different exercise programs on PDN. The total
heterogeneity test result was
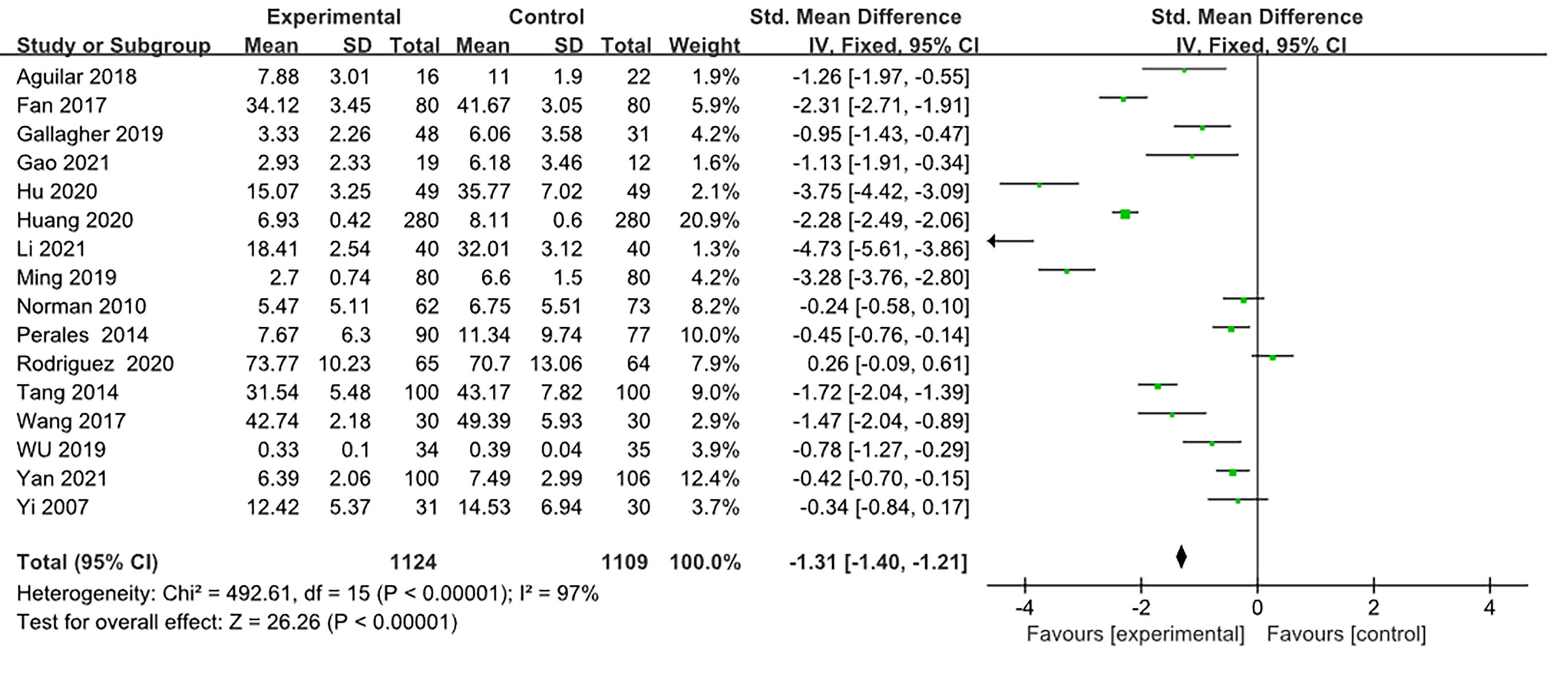 Fig. 3.
Fig. 3.Effects of exercise intervention on perinatal depression.
In order to explore the reasons for the high heterogeneity, through the sensitivity analysis by excluding the included studies one by one, the overall effect value did not change significantly during the one-by-one exclusion process, suggesting less bias caused by individual studies. Therefore, the relevant subgroup analysis was carried out.
Five sub-elements of the exercise intervention were analyzed: exercise start time, exercise content, exercise frequency, practice form, and duration of exercise.
The results showed that both prenatal and postpartum exercise effectively
prevented depression symptoms (p
| Variable | Subunit | Article offer measure | Sample size | Total number of samples | SMD | [95% CI] | Two-tailed test | |
|---|---|---|---|---|---|---|---|---|
| Z | p | |||||||
| Start time | Antenatal | 13 | 2006 | 2233 | –1.45 | [–1.56, –1.35] | 27.16 | |
| Postpartum | 3 | 227 | –0.37 | [–0.63, –0.10] | 2.72 | 0.007 | ||
| Sports content | Yoga | 4 | 331 | 2233 | –1.34 | [–1.59, –1.09] | 10.55 | |
| Comprehensive aerobic exercise | 6 | 1034 | –1.78 | [–1.94, –1.63] | 23.03 | |||
| water sports | 2 | 167 | –0.03 | [–0.34, 0.28] | 0.20 | 0.840 | ||
| Dance gymnastics | 3 | 566 | –1.34 | [–1.54, –1.15] | 13.65 | |||
| Power movement | 1 | 135 | –0.24 | [–0.58, 0.10] | 1.38 | 0.170 | ||
| Practice form | Personal practice | 7 | 770 | 2233 | –2.03 | [–2.21, –1.84] | 21.89 | |
| group practice | 6 | 1090 | –1.06 | [–1.19, –0.92] | 15.44 | |||
| Combination practice | 3 | 373 | –0.89 | [–1.11, –0.66] | 7.66 | |||
| Frequency | 7 | 1155 | 2233 | –1.01 | [–1.91, –0.12] | 2.22 | 0.030 | |
| 9 | 1078 | –1.91 | [–2.73, –1.10] | 4.59 | ||||
| Duration of exercise | 4 | 899 | 1833 | –1.84 | [–2.00, –1.68] | 22.78 | ||
| 30–60 min | 3 | 442 | –0.49 | [–0.68, –0.30] | 5.05 | |||
| 6 | 492 | –0.54 | [–0.73, –0.35] | 5.46 | ||||
The types of exercise in the 16 RCTs included yoga, aerobics, dance gymnastics,
water sports, and strength exercise. The effect of all types of exercise on
depression was evaluated: yoga (SMD = –1.34, 95% CI = –1.59 to –1.09),
aerobics (SMD = –1.78, 95% CI = –1.94 to –1.63), and dance gymnastics (SMD =
–1.34, 95% CI = –1.54 to –1.15) had statistically significant effect on
depression (p
The exercise frequency was classified as
The duration of a single exercise was divided into
The practice form mainly included personal practice at home, group practice, and
combination practice. Practice form effected depression as follows: personal
exercise: SMD = –2.03, 95% CI = –2.21 to –1.84; group exercise: SMD = –1.06,
95% CI = –1.19 to –0.92; combined exercise: SMD = –0.89, 95% CI = –1.11 to
–0.66 (p
Related research has focused on intervention experiments and review analysis, This study by systematically reviewing 16 RCTs, evaluated and compared the effect of different exercise programs on the prevention of PDN. Evidence-based results showed that all exercises were effective in preventing PDN symptoms. Dipietro et al. [28] found that physical exercise is as effective as psychoactive drugs on the prevention of PDN.
The findings showed that prenatal exercise had a better effect in preventing PDN than postpartum exercise. According to related studies, the incidence of PPD is highly correlated with the presence of depression during pregnancy [29], indicating that prenatal depression is the strongest predictor of PPD. Exercise during pregnancy reduces prenatal depression and, consequently, the occurrence of PPD [30]. Thus, prenatal exercise is of great value in preventing PDN and promoting fetal development and smooth delivery [31].
Yoga, aerobics, and dance gymnastics effectively prevented depression, with aerobics achieving the best results. Based on the change in maternal body function and risks associated with exercise, walking and Baduanjin are the most common exercises for pregnant women [32]. These exercises promote the blood circulation and metabolism of the maternal body, improve cardiopulmonary function, and are conducive to fetal delivery and maternal body recovery [33].
To avoid fatigue and stress [34], pregnant women should not exercise too
frequently or for a longer duration. Evidence-based results found that exercising
Personal exercise programs are more effective in improving PDN than other forms of exercise. This may be related to the advantages of individual exercise, which is not limited by time, place, and economy. However, compared to group practice, personal practice lacks the necessary exercise monitoring and technical support, and pregnant women tend to abandon the exercise programs. Research shows that only 23.6% of pregnant women in China insist on exercising, and the main reasons for not exercising include insecurity, lack of a strong will, and no companionship [37]. It is suggested that the rapidly advancing internet technology should be used to establish digital maternal sports management platforms and WeChat groups to develop personal maternal exercise programs [38] to prevent PDN.
This study analyzes only RCTs and provides strong evidence for evaluating the preventive effect of different exercise programs on PDN. However, there may be clinical heterogeneity affecting the results; more high-quality studies are required to verify the reliability of the results.
Exercise is a low-cost strategy. This study summarizes the current situation of the preventive effect of different exercise programs on PDN, providing a basis for inspection for future clinical trials. Before designing exercise programs for pregnant women, medical personnel should be aware of their exercise history, including exercise duration and frequency.
To sum up, exercise is effective in preventing PDN. It is recommended that
pregnant women follow a personalized aerobics exercise regime of
Future research will be expanded in the following aspects: (1) to improve the pertinence and adaptability of exercise intervention programs, that is, to optimize exercise programs and conduct precise training according to their pregnancy cycle, postpartum recovery cycle, maternal age and related complications. (2) Strengthen the monitoring of exercise intervention, that is, in view of the special changes of maternal physical function, heart rate and psychological changes, strengthen the monitoring of the exercise process from the aspects of maternal subjective perception, maximum heart rate and maximum oxygen consumption, so as to avoid the risk of maternal exercise to the maximum extent.
SM and YL drafted this manuscript; XY made substantial contributions to the conception and design of the review; HH, SM and YL participated in the acquisition of the data, the analysis, and interpretation of the data; XY revised the article critically for important intellectual content; XY approved the version of the article to be published. All authors read and approved the final manuscript.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.