


1 Pudong New Area Mental Health Center, Tongji University School of Medicine, 200124 Shanghai, China
2 Department of Gynaecology and Obstetrics, Tongji Hospital, Tongji University School of Medicine, 200065 Shanghai, China
3 Department of Psychiatry, Tenth Peoples’ Hospital, Tongji University School of Medicine, 200072 Shanghai, China
Academic Editor: Michael H. Dahan
Abstract
Background: The distance between clitoris and urethral meatus (CUMD)
for women has been considered to likely reflect the extent of prenatal androgen
exposure, being similar to the anogenital distance (AGD) and the digit length
ratio. But no published work has examined the association between CUMD and AGD or
digit ratio, and the effects of body weight on the CUMD and AGD.
Methods: The CUMD and two AGD measurements, including the anus to the
anterior clitoris (AGD-AC) and the anus to the posterior fourchette (AGD-AF),
were taken in 117 Chinese women (18–45 years), using a digital caliper. The
digit ratios were measured from photos by a digital camera. Meanwhile, data of
their height, weight, and body mass index (BMI) were collected. Results:
In bivariate correlation analyses of all 117 subjects, two AGD measurements
(AGD-AC and AGD-AF) were moderately correlated with one another (r = 0.474,
p
Keywords
- clitoris to urethral meatus distance
- anogenital distance
- prenatal androgen exposure
- digit length ratio
Anogenital distance (AGD) is identified as the distance from the anus to the genitals [1, 2]. In the majority of mammals, male AGD is 50% to 100% longer than in females [3], thus the AGD is regarded as a sexually dimorphic phenotype with males’ AGD measuring longer than females. Based on evidences from animal models, the AGD is considered as a sensitive marker of in utero exposure to androgens [1, 2]. In the rat experiment, studies identified a fetal masculinization programming window (MPW), within which androgen action determines adult reproductive organ size and AGD [1, 4]. As the human critical period of fetal androgen exposure in the womb is out of reach, the AGD measurement provides the possibility of reflecting this hidden process [1, 2]. The studies on anthropometric measurements of human AGD disclosed that the AGD was relatively stable from childhood to adult age in healthy individuals [1, 2]. Numerous researchers have cared about the population data of the AGD, and utilized the methods to assess fetal androgen action across a wide range of clinical disorders and study androgen-induced individual differences and gender development [1, 2, 5, 6]. The AGD also appears to be a valid biomarker to evaluate the effects of adverse environmental compounds on human reproductive development [2, 7]. Consistent with rat experimental data, the AGD measured in men was found to be associated with male reproductive health including congenital malformations, testis size, penis length, spermcount/semen quality, testosterone levels, and prostate cancer [8, 9, 10, 11, 12, 13, 14, 15]. In women, associations with the AGD were suggested with fertility, clitoris length, adult testosterone levels, ovarian function, endometriosis, polycystic ovary syndrome (PCOS), and pelvic organ prolapse [16, 17, 18, 19, 20, 21, 22, 23, 24].
The AGD in women was usually measured in two ways [1, 2]. One way is to measure the distance from the anus to the anterior clitoris (AGD-AC); other way is to measure the distance from the anus to the posterior fourchette (AGD-AF). Both AGD-AC and AGD-AF are reliable and replicable measurements among examiners using a standard way, but they are probably affected by body mass index/adiposity, particularly the AGD-AC [1, 25, 26]. Besides AGD-AC and AGD-AF, clitoris to urethral meatus distance (CUMD) has been also considered to likely reflect the extent of prenatal androgen exposure [27], but it was less studied. Women with longer CUMD measures are supposed to be exposed to higher levels of prenatal androgens than women with shorter distances, and a shorter CUMD in a woman was deemed to increase her likelihood of experiencing orgasm in sexual intercourse [27].
The 2:4 digit ratio also shows sexually dimorphic with men’ ratio less than women, and is a putative indication of prenatal sex hormone exposure, but inconsistently between studies [1]. According to recent findings, the AGD is more likely to provide an accurate biomarker of fetal androgen exposure in humans, compared with the 2:4 digit ratio [1, 5, 6].
To our knowledge, no published work has examined the association between the CUMD and the AGD or digit ratio in women. The aim of this study was to investigate the correlation of CUMD with the AGD or digit ratio, and the effect of body weight on the CUMD and AGD.
The 117 subjects are Han Chinese women who visited the gynecological or psychosomatic clinic of hospitals between June 2018 and December 2020, and agreed on participation after listening to the purpose of the study. Eligibility criteria were referred to the literature and our previous studies [22, 28], briefly including age 18–45, regularly menstruating, nulliparous with no pregnancy lasting more than ten weeks, not currently receiving any treatments to control or influence the secretion of hormones, no history of injury to or surgery on the genital region, no history of congenital anatomical abnormalities in genital organs, and no history of an injury to the 2nd or 4th digit of both hands.
The researches were in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki) for the study involving humans, and were approved by the Ethics Committee at the Pudong New Area Mental Health Center affiliated to Tongji University School of Medicine. The written informed consent was obtained from all subjects.
Anthropometric data were collected on the enrollment day. Height and Weight were
measured by rounding off to the nearest tenth in centimeter (cm) or kilogram
(kg), respectively. Body mass index (BMI) was calculated as weight in kilograms
divided by squared height in meters. BMI generally correlates highly with
adiposity, BMI cut-offs for underweight, normal range of weight and overweight
are
The AGD and CUMD were measured using a digital caliper (Carbon Fiber Composites Digital Caliper, Wuxi Kaibaoding Tool Limited Company, Jiangsu, China), the procedures were described in the literature and our previous studies [22, 27, 28]. The subjects were in the supine position, then changed to the lithotomy position in which the legs are spread apart to be accessed for measurements. The AGD-AC was the distance from the center of the anus to the anterior clitoral surface, and the AGD-AF was the distance from the center of the anus to the posterior fourchette. The CUMD was measured as the distance from the underside of clitoral glans to the center of the urinary meatus. In order to improve accuracy, measurements were collected in triplicate by two independent professionals, the mean value of the six measurements of each distance was used.
Measurement of Digit Ratio was same as described in the literature and our previous studies [28, 30], namely that a digital camera was used to photograph both hands of subjects. The lengths of index and ring fingers of both hands were measured from the bottom crease of each digit to the finger tip, using tools in Adobe Photoshop [28, 30]. For each hand, the digit ratio (2D:4D) was subsequently calculated. Mean of right and left hand ratio was taken as mean 2D:4D ratio for each individual. All subjects reported being right handed.
The summary statistics on subjects for the variables of interest were
calculated. The five outcome variables CUMD, AGD-AF, AGD-AC, 2D:4D right hand,
and 2D:4D left hand, as well as several potential covariates (height, weight,
BMI), were examined. The variables were documented by the mean
All subjects, who met the inclusion criteria, were recruited. Table 1 shows the
general characteristics of the study subjects. The mean age was 28.5
| Characteristic | Mean |
| Age (years) | 28.5 |
| Height (cm) | 163.0 |
| Weight (kg) | 57.1 |
| BMI (kg/m |
21.5 |
| CUMD (mm) | 23.0 |
| AGD-AC (mm) | 94.9 |
| AGD-AF (mm) | 28.4 |
| 2D:4D (left) | 0.98 |
| 2D:4D (right) | 0.96 |
| n: number of subjects. | |
In bivariate correlation analyses, no statistically significant associations
were observed with the CUMD and AGD measurements (Table 2). Although the two AGD
measurements (AGD-AC and AGD-AF) were moderately correlated with one another (r =
0.474, p
| AGD-AC | AGD-AF | 2D:4D Left | 2D:4D Right | |
| CUMD | 0.172 (0.063) | –0.014 (0.879) | –0.160 (0.084) | –0.060 (0.519) |
| AGD-AC | – | 0.474 (0.000) | 0.074 (0.427) | 0.037 (0.690) |
| AGD-AF | – | – | –0.056 (0.550) | 0.011 (0.907) |
| n: number of subjects. | ||||
| Height | Weight | BMI | |
| CUMD | 0.102 (0.272) | 0.063 (0.500) | 0.049 (0.603) |
| AGD-AC | –0.005 (0.956) | 0.290 (0.002) | 0.341 (0.000) |
| AGD-AF | –0.010 (0.911) | 0.189 (0.041) | 0.204 (0.027) |
| n: number of subjects. | |||
For further understanding of influences of weight/BMI on AGD-AC, AGD-AF or CUMD,
we compared the general characteristics of three groups with different body
weight (Table 4). The CUMD between normal range -weight group and overweight
group was no different (23.2
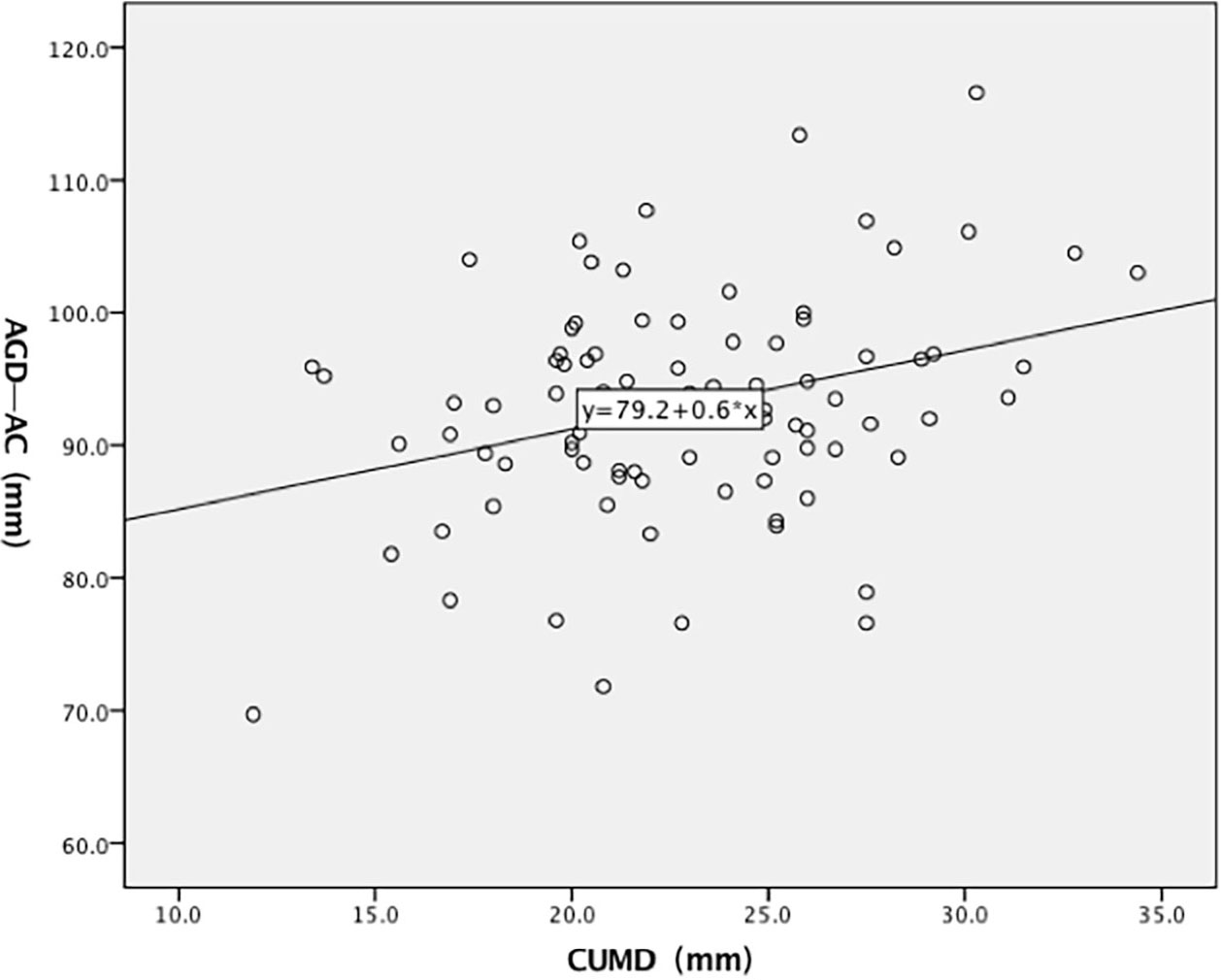 Fig. 1.
Fig. 1.Bivariate relationships between CUMD and AGD-AC measure in the non-overweight subjects.
| Variable | Overweight (n = 31) | Normal (n = 67) | Underweight (n = 19) |
| Age | 31.1 |
27.6 |
27.5 |
| Menarcheal Age | 12.8 |
13.3 |
13.6 |
| Height (cm) | 162.0 |
163.0 |
164.7 |
| Weight (kg) | 68.4 |
54.7 |
47.1 |
| BMI (kg/m |
26.0 |
20.6 |
17.3 |
| CUMD (mm) | 23.2 |
23.1 |
21.8 |
| AGD-AC (mm) | 100.3 |
93.6 |
90.6 |
| AGD-AF (mm) | 30.6 |
27.3 |
28.3 |
| Left 2D:4D Ratio | 1.00 |
0.97 |
0.98 |
| Right 2D:4D Ratio | 0.97 |
0.96 |
0.96 |
| n: number of subjects. * p = 0.01; **p | |||
In our studies, the CUMD was measured from the underside of clitoral glans to
the center of the urinary meatus, and the clitoral glans was not included. The
mean CUMD (23.0
The distance from clitoris to urethral orifice (CUMD), as one of genital dimensions of normal women, or as a possible factor associated with sexual function was studied [27, 31, 32, 33]. The embryogenesis and development of perineum is androgen mediated as evidenced by the larger anogenital distance (AGD) observed in men compared with women [1, 2, 18]. The CUMD is a section of female perineum, it is hopeful as an assumed biomarker of prenatal androgen exposure, and probably equivalent to well-defined AGD-AC or AGD-AF. However, CUMD was weakly associated with AGD-AC in our primary analysis of all subjects, but fell short about being statistically significant, although the correlation between AGD-AC and AGD-AF reached a moderate level, corresponding to the result reported elsewhere [34].
Androgen exposure during the MPW determines the maximum “potential” adult size of AGD, but secondary changes in AGD in adults may also have occurred, while the androgen-estrogen balance has been altered (e.g., obesity, pregnancy, aging, and late-onset hypogonadism) [1, 2, 4, 25, 26]. Our data in further studies clearly demonstrated that the AGD-AC and AGD-AF of adult women, particularly the former, were lengthened with obesity. Meanwhile, the CUMD was not affected with increase or decrease of body weight. Adjusting for obesity, the CUMD was significantly correlated with AGD-AC, it suggested that the CUMD, very likely same as AGD-AC, was affected by fetal androgen. Furthermore, the CUMD, as an assumed marker of prenatal androgen exposure, was not affected by the body weight. This was the advantage of CUMD indicator, compared to AGD-AC/AGD-AF indicators which were frequently used in the studies of possible role of prenatal androgen exposure. For an example, several recent studies demonstrated that AGD-AC/AGD-AF in adult patients with PCOS were longer than control, implying that extreme prenatal androgen exposure contributes to the PCOS [22, 23]. Assessment of AGD-AC/AGD-AF was suggested as a diagnostic tool in PCOS [35]. But the PCOS patients usually have metabolic problems and obesity symptoms [36], eliminating the influence of obesity thus should be emphasized when using the AGD-AC/AGD-AF as auxiliary diagnostic indictors for the PCOS. The AGD-AC/AGD-AF are frequently used as an effective readout in human epidemiological studies to correlate fetal exposure to endocrine disrupting chemicals [7], the problem of obesity also has to be faced. Therefore, we proposed that the CUMD should be included in the future studies as a possible clinical or toxicological marker for fetal androgen action and risk for female reproductive disorders.
The ratio between the second and fourth digit is associated with the estimated ratio of prenatal testosterone relative to prenatal estradiol, and the digits development is probably androgen/estrogen mediated [37]. Additionally, the sexual dimorphic growth of digits from birth to adulthood could also be influenced by postnatal or pubertal factors [1]. The digit ratios was not correlated to AGD-AC/AGD-AF in our studies, it is consistent with the results from the subjects with no history of digit injuries, reported by Barret et al. [34]. Therefore, it is not surprising that the correlations between digit ratios and CUMD in our studies were not statistically significant.
Several study limitations should be noted. The sample was small, and the populations in our study were not healthy subjects who were randomly selected, they were patients suffered from various gynecological or psychosomatic diseases, although the admission and exclusion criteria were strictly enforced. The body fat distribution (such as measuring the circumference of chest, waist and hip) was not studied, the lower abdominal or gluteal-femoral obesity might have a stronger impact on the AGD-AC/AGD-AF. Whereas, we mainly used the Spearman’s correlations for statistical analysis, it had limitations and issues of the strengths.
In conclusion, our results indicated that the CUMD , as an assumed marker of prenatal androgen exposure, was not affected by the body weight, thus being superior to AGD-AC or AGD-AF.
The data and materials described in the current study are available from the corresponding author on reasonable request.
BZ took part in project development, manuscript writing; ZL collected data, analyzed data and contributed to manuscript writing. MJX, HX, and HFL were involved in collection of data. All authors read and approved the final manuscript.
Ethical approval (NR. 2017003) was obtained from the Ethics Committee at the Pudong New Area Mental Health Center affiliated to Tongji University School of Medicine. The written informed consent was obtained from all subjects.
We would like to express our gratitude to all the peer reviewers for their opinions and suggestions and thanks to all those who helped us during the writing of this manuscript.
This study was supported by the Shanghai Pudong Municipal Health commission, China (PWZzk2017-20; PWYgy2018-10).
The authors declare no conflict of interest.