
 , Teresita de Jesús Saucedo-Molina 1, Lilián Elizabeth Bosques-Brugada 2, Claudia Unikel-Santoncini 3,*
, Teresita de Jesús Saucedo-Molina 1, Lilián Elizabeth Bosques-Brugada 2, Claudia Unikel-Santoncini 3,*
1 Academic Area of Nutrition, Institute of Health Sciences, Autonomous University of Hidalgo, San Agustín Tlaxiaca, Hidalgo 42184, Mexico
2 Academic Area of Psychology, Institute of Health Sciences, Autonomous University of Hidalgo, San Agustín Tlaxiaca, Hidalgo 42184, Mexico
3 Directorate of Epidemiological and Psychosocial Research, National Institute of Psychiatry Ramón de la Fuente Muñiz, 14370 Mexico City, Mexico
Abstract
Disorder eating behaviors (DEB) are precursors to eating disorders, and can cause biopsychosocial dysfunction.
The effect of two universal prevention based on Cognitive Dissonance, specifically the Body Project (BP) and the Prevention of Unhealthy Eating Behaviors and Sedentary Lifestyles (Spanish acronym PECANSS) on DEB, thin-ideal internalization (TII), drive for muscularity (DM), body dissatisfaction (BD), negative-affect (NA), moderate-vigorous physical activity (MVPA) and body mass index (BMI) were evaluated in a non-probabilistic sample of Mexican university students. It was a quasi-experimental and longitudinal study (pretest-posttest-one-year follow-up) of four intervention groups (IG) and two control groups (CG) by sex. Valid questionnaires were administered to 318 students to measure the variables (65% women; Mage = 19.35 years; SD = 1.83).
In women at the intragroup level, reported a decrease in IGs over time in DEB (IG-1-PECANSS-R; IG-4-BP-R; IG-5-BP), TII (IG-4-BP-R; IG-5-BP), DM (IG-4-BP-R), BD (IG-5-BP), NA (IG-4-BP-R) and increased MVPA (IG-1-PECANSS-R), BMI (IG-2-PECANSS; IG-4-BP-R). Among intragroup men, decreased NA (IG-5-BP) and, increased MVPA (IG-2-PECANSS), BMI (IG-4-BP-R). There were no differences between groups in the variables at the end of the interventions.
The results suggest that depending on participants' sex and IG, the programs had an intragroup effect on DEB and other variables evaluated.
Keywords
- disordered eating behaviors
- prevention program
- cognitive dissonance
- university students
- Mexico
Disordered eating behaviors (DEB; Rodriguez et al, 2010) are contributory factors to the development of eating disorders (ED). Examples of DEB include restrictive diets, bingeing, purgative and laxative behaviors, and fasting to avoid weight gain (Lameiras et al, 2008; Lora and Saucedo-Molina, 2006). Although DEB and ED mainly affect adolescents (Neumark-Sztainer et al, 2018), they are also common in young adults such as university students having to cope with various critical, stressful situations such as leaving home to begin their higher education (Harrer et al, 2020).
The etiology of DEB and ED, primarily present in women, includes the sociocultural pressure on the latter to achieve the thin-ideal (Hsu, 1989), resulting in a 10:1 female-to-male ratio of ED (Caballero, 2005). In men, DEB and ED are mainly caused by the desire to achieve a strong, athletic body with well-defined muscles (Karazsia et al, 2017). Although the presence of eating disorders is lower in men, Yager and O’Dea (2008) observed that five to ten out of every 100 American male university students suffer from them. The prevalence of DEB in female university students fluctuates from 4% to 23.6% and from 1% to 14.4% in men (Calderón, 2006; Tozun et al, 2010; Yu et al, 2015). In Mexico, rates range from 5.6% to 18.9% in women and from 8.7% to 12.7% in men (Cruz et al, 2008; Palmeros-Exsome et al, 2022). In Hidalgo, Mexico, the prevalence of DEB in female university students ranges from 3.4% to 7.9% and from 2.3% to 4.2% in male university students (Saucedo-Molina and Unikel, 2010; Saucedo-Molina et al, 2015).
Other factors associated with DEB and ED are thin-ideal internalization (Saucedo-Molina and Unikel, 2010), drive for muscularity (Arellano-Pérez et al, 2019), body dissatisfaction (Culbert et al, 2015; Jiménez-Limas et al, 2022), and negative affect (Polivy and Herman, 2002), as well as overweight and obesity (Jiménez-Limas et al, 2022). In Mexico, the National Health and Nutrition Survey on covid 2021 (ENSANUT-COVID 21) reported a combined prevalence of overweight and obesity of 72.4% for adults (according to this survey, the adult population includes those aged 20 and over; Shamah-Levy et al, 2022), meaning that it constitutes a nationwide public health problem. In Hidalgo, the combined prevalence for adolescents and university students rose from 17% in 2007 (Saucedo-Molina et al, 2008) to 34% in 2017 (Arellano-Pérez et al, 2019).
Another unhealthy behavior among the youth population is their sedentary lifestyle and physical inactivity (Noriega et al, 2015). According to the World Health Organization (WHO), one in four adults worldwide fails to engage in sufficient physical activity (WHO, 2022) while in Mexico, ENSANUT 2018 showed that 29% of adults aged 20 and over do not meet international recommendations (Shamah-Levy et al, 2020). Prior to the pandemic, 51.1% of Mexican adults aged 20 and over engaged in some form of physical activity, whereas during the pandemic, this decreased among 68.6% of those surveyed (Shamah-Levy et al, 2022). In samples of Hidalgo adolescents, 79.5% of girls and 57.7% of boys in this age group engage in an insufficient level of physical activity (Arellano-Pérez et al, 2019).
Initially, programs to prevent DEB and ED among university students were mainly
psychoeducational (Stice et al, 2007). They were gradually modified,
eventually incorporating strategies based on cognitive dissonance (CD). There is
evidence of the effect of this type of intervention (Brown et al, 2017; Ridolfi and Vander Wal, 2008; Saucedo-Molina et al, 2018; Saucedo-Molina et al, 2022; Stice et al, 2012; Stice et al, 2013; Stice et al, 2017; Unikel-Santoncini et al, 2019; Unikel-Santoncini et al, 2023; Wilson et al, 2020), which includes reducing DEB, body dissatisfaction, and thin-ideal
internalization (Stice et al, 2000). This effect has been maintained from
one to three years (Stice et al, 2012; Stice et al, 2013), in both
adolescents and university students (Stice et al, 2000), guaranteeing their
success even if the interventions are given by other students (Perez et al, 2010). However, these strategies focusing on university students of both sexes
are scarce and comprise a range of designs (Ridolfi and Vander Wal, 2008), study
variables, and different types of administration, such as the virtual means for
their implementation (Stice et al, 2017). At the same time, interventions
differ in regard to the length of time they are administered. For example,
Wilson et al (2020) conducted a brief, dissonance-based, non-dieting intervention
with female college students. This intervention consisted of two 90–120-minute
interactive group sessions designed to foster the rejection of
dieting, increase body acceptance, and develop healthy eating habits. Assessment
measures were collected at baseline, post-treatment, and one-month follow-up.
Other programs also seek to prevent obesity by including nutritional content and
physical activity (Stice et al, 2013). Interestingly, the only intervention
designed for men identified in the literature is The Body Project: More Than
Muscles (Brown et al, 2017). Another challenge that has been proposed for
several years is to achieve larger effect sizes for ED prevention programs, and
in this respect, the use of booster sessions has been suggested as an alternative
(Berger et al, 2008; Ciao et al, 2014; Schwartz et al, 2019; Stice et al, 2007). It has even been recommended that these booster sessions be provided
twice a year to prevent treatment effects from diminishing over time (Phelps et al, 2000). One program that has achieved positive results with this type of
strategy is Student Bodies™, proposed by researchers at Stanford
University and created for university women with body weight and shape concerns.
Although the intervention uses cognitive-behavioral strategies, in a randomized
sample of 480 university women (Mage = 20.8 years, SD = 2.6) after eight
weeks of the online intervention, in addition to an optional booster session for
nine months post-intervention, the results demonstrated that in comparison with
the waitlist control group, students in the group that received the Student
Bodies™ intervention experienced significant reductions in body
dissatisfaction, thinness bias, and eating disorder pathology (assessed with the
EDE-Q) at post-intervention and 1-year follow-up. Furthermore, in a subgroup of
participants [those with body mass index (BMI)
In Mexico, one of the first interventions focusing on female university students (Unikel-Santoncini et al, 2019), based on the Body Project (BP) (Stice et al, 2000), succeeded in reducing DEB and body dissatisfaction scores at one-year follow-up. It has been observed that the Body Project encourages participants who initially buy into the thin ideal to be critical of it. It includes activities designed to produce cognitive dissonance, which reduces the degree to which they accept the thin ideal, which in turn appears to result in improvements in dissatisfaction with body image, negative affect and ED symptoms (Stice et al, 2000). At the same time, three interventions for both sexes were identified. The first was a pre-post-intervention pilot study and three-month follow-up with a two-control group. The aim of this study was to examine the feasibility and acceptability of a disordered eating and obesity prevention program called Stop Obesity and Eating Disorders (StopOBEyTA) among 45 university students. The experimental group received an eight-session intervention, designed to promote healthy eating habits and a positive body image. The control group was divided, with half the group receiving eight sessions designed to improve learning skills, and the other half receiving no intervention. The results showed that StopOBEyTA effectively reduced DEB among women at the intragroup level (Castillo et al, 2016). The second was the Obesity and Eating Disorders (OBEyTA), implemented to examine the effects of an integrated program for university students through an exploratory controlled study targeting specific predisposing factors for disordered eating and obesity-related problems, which measured healthy eating, physical activity, body image satisfaction, and perceived pressure to be thin. The program had one group which received the intervention and two control conditions (study skills vs. non-intervention). Each group participated in a total of eight workshops lasting 90 minutes. The results showed that the program had no effect on male students, while internalization of the thin-ideal and negative attitudes towards food only decreased in female students (Castillo et al, 2019). Finally, the third research project was a pre-experimental, pre-post-test study undertaken by Unikel-Santoncini et al (2023). The BP was implemented to identify changes at one-year follow-up of a universal prevention intervention for disordered eating behaviors, thin-ideal internalization, and drive for muscularity. Workshops were held in groups comprising men and women, each coordinated by one or two trained facilitators. Five hour-and-a-half to two-hour sessions were given, in which verbal, written, and interactive behavioral exercises were completed. The results showed a reduction in DEB and thin-ideal internalization in women, and drive for muscularity in men.
Prevention of Unhealthy Eating Behaviors and Sedentary Lifestyles (PECANSS), designed by Saucedo-Molina et al (2018) seeks to prevent the culture of thinness and the impact of fashion trends on the body, including the global strategy for diet and physical activity proposed by the WHO (2010, 2013, 2018). The program, based on CD, differs from the BP in the original way it integrates information and activities to prevent DEBs, including the design of healthy menus and physical activity sessions. It includes a psychoeducational, interactive approach, its main objective being to prevent the development of symptoms related to EDs and a sedentary lifestyle in non-symptomatic subjects, focusing on the factors that condition their emergence and maintenance. The first administration of PECANSS significantly reduced DEBs in adolescent female students and increased moderate-vigorous physical activity (MVPA), maintaining these results at six months. It also decreased, albeit not significantly, the DM score in adolescent males and the prevalence of overweight and obesity in both sexes (Saucedo-Molina et al, 2018). Its second administration achieved a significant decrease in DEBs in both men and women in the Experimental Group, as well as in the risk of DM in men at one-year follow-up (Arellano-Pérez et al, 2019; Saucedo-Molina et al, 2022).
Against this background, one of the contributions of PECANSS to this research is the age group in which it was administered, which differs from that of the research by Saucedo-Molina et al (2018) studying adolescents of both sexes between the ages of 15 and 18. In this respect, in the present article, the programs were implemented in young adults between the ages of 18 and 29. Other contributions include the fact that it was administered remotely and that the physical activation sessions were modified so that they could be performed individually rather than in groups as they were in the article published in 2018. At the same time, it is essential to implement prevention strategies for DEBs and their risk factors, using technology for the well-being of the university community of both sexes. There is also a need to seek strategies that will maintain their effects in the long term, reinforcing protective factors and minimizing the risk factors for the development of EDs. This study was designed to evaluate the effect of two universal prevention programs based on CD, specifically the BP and the Mexican program known as PECANSS (Saucedo-Molina et al, 2018, Saucedo-Molina et al, 2022), on DEB, thin-ideal internalization, body dissatisfaction, negative affect, and drive for muscularity, as well as physical activity and BMI in a sample of Mexican university students of both sexes. The first hypothesis was that in both interventions, significant changes would be expected in DEBs and the risk factors associated with EDs over time compared to the corresponding control group in each program. The second hypothesis was that in the intervention groups in which PECANSS was administered, a significant increase in physical activity would be recorded over time, compared to the intervention groups that received the BP intervention. Finally, it was hypothesized that greater changes would be expected in the intervention groups in which a booster was given six months after starting the intervention, compared to the intervention groups that did not receive it and the corresponding control groups.
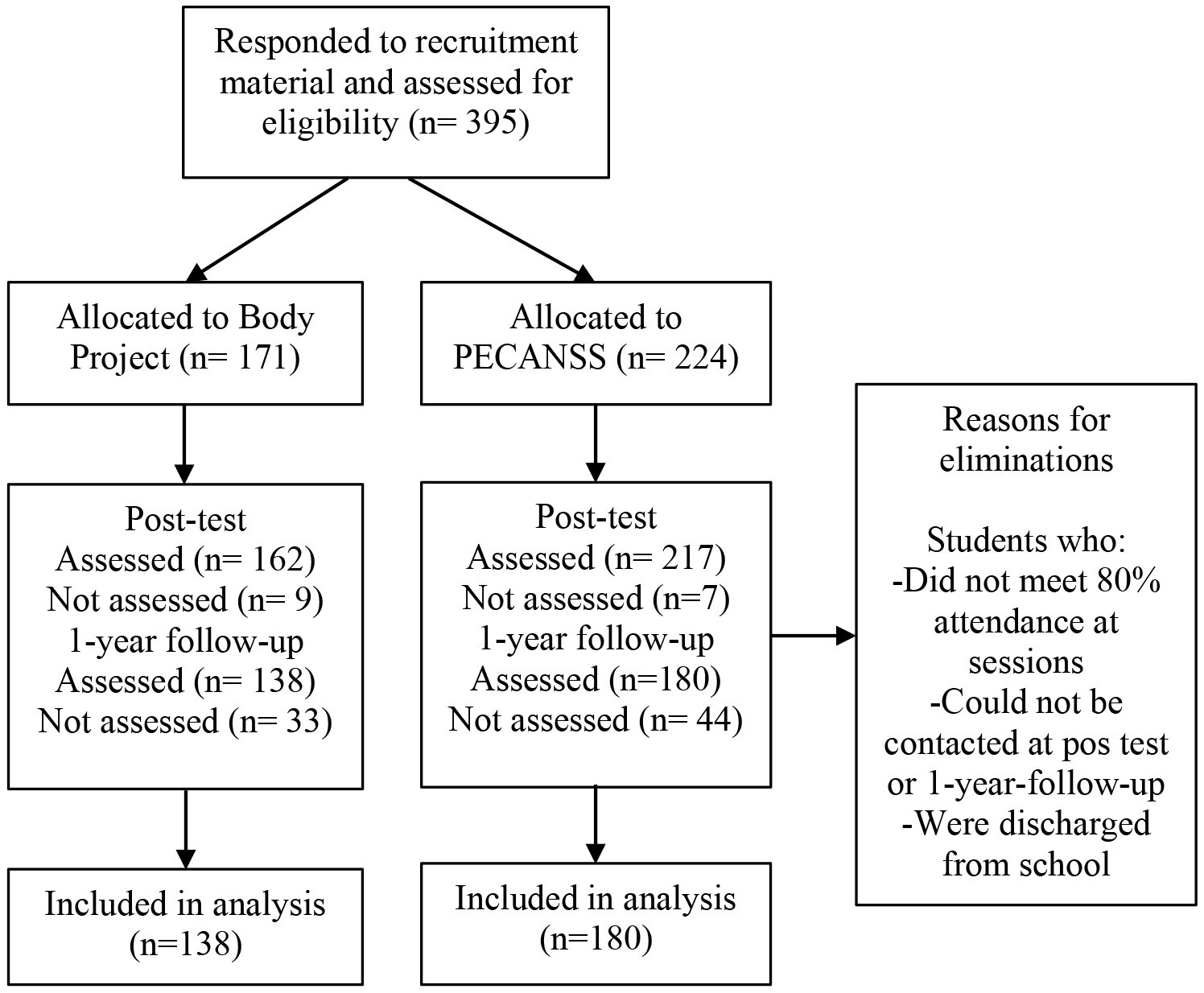
The non-probabilistic sample initially comprised 395 participants (65% women)
aged 18 to 29 (Mage = 19.35 years; SD = 1.83). At one-year follow-up, a
19.8% attrition rate reduced the number of participants to 318 (65% women; see
Fig. 1). Inclusion criteria for the study were being an undergraduate student at
the Universidad Autónoma del Estado de Hidalgo (UAEH) in Mexico. Exclusion
criteria were being pregnant, not agreeing to participate or provide their data
for tracking in the follow-up phase while the elimination criterion was failing
to attend a minimum of 80% of the sessions. Conducting a logistic regression
analysis in the final sample with dichotomous variables using the G*Power 3.1.9.7
program (Faul et al, 2009; Düsseldorf, Germany;
https://www.psychologie.hhu.de/arbeitsgruppen/allgemeine-psychologie-und-arbeitspsychologie/gpower),
yielded a statistical power of 80% (95% CI, Error
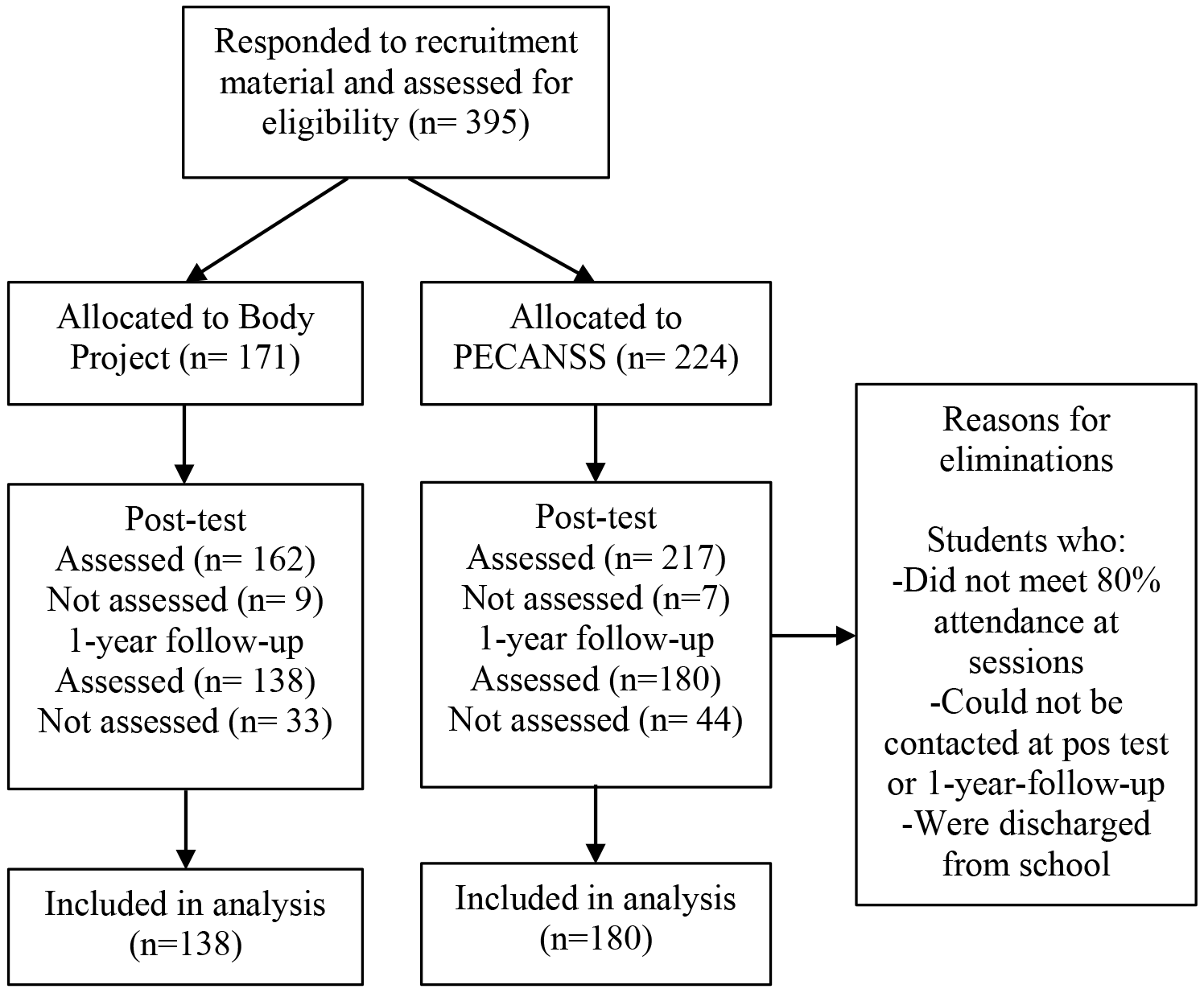 Fig. 1.
Fig. 1.
Participant flow throughout study. PECANSS, Prevention of Unhealthy Eating Behaviors and Sedentary Lifestyles.
(a) Brief Questionnaire to measure Disordered Eating
Behaviors (BQDEB) (“Cuestionario breve para medir conductas alimentarias de riesgo”,
CBCAR; Unikel-Santoncini et al, 2004). The BQDEB comprises 10 questions
measuring concern about weight gain, binge eating, and restrictive and purgative
behaviors in the three months prior to the evaluation. It has four response
options (ranging from 0 = never or almost never, to 3 = very frequently [more
than twice a week]). The cut-off points are no risk of developing an ED (0–6),
moderate risk of developing an ED (7–10; Unikel et al, 2017) and high risk
of doing so
(b) Attitudes towards Body Figure Questionnaire (ABFQ; Unikel et al, 2006). The ABFQ measures thin-ideal internalization using 15 questions
with four response options: 1 = never or almost never, 2 = sometimes, 3 =
frequently and 4 = always. Its cut-off point
(c) Drive for Muscularity Scale (DMS)
(“Cuestionario de obsesión por la
musculatura”; COM; Escoto et al, 2013). The DMS evaluates attitudes and
behaviors related to the increase in muscle mass, dietary supplement use and
treatment adherence. The version validated for the Mexican population was used,
with 15 questions classified from 1-never to 6-always. A cutoff point of
(d) Positive and Negative Affect Schedule-Expanded Form (PANAS-X;
Watson and Clark, 1992). The Negative Affect subscale was used in this
study. This subscale measures the degree to which participants have experienced
negative emotional states. It comprises 20 questions, with options ranging from 1
= very little or not at all to 5 = a lot. Based on the mean score plus one
standard deviation, the cut-off point was
(e) Body Shape Dissatisfaction Questionnaire (BSDQ;
Berscheid et al, 1973). This questionnaire evaluates satisfaction and
dissatisfaction with body parts using nine items with options ranging from 1 =
very dissatisfied to 5 = very satisfied. The cut-off point for satisfaction (mean
score plus one standard deviation) was
(f) International Physical Activity Questionnaire (IPAQ; Medina et al, 2013a). The short version validated for the Mexican population was used with eight items to measure physical activity in the past seven days. To determine the level of moderate-vigorous physical activity (MVPA) performed by the participants, data were adjusted using the equation proposed by Medina et al (2013b) and classified according to the cut-off points proposed by WHO (2022).
(g) Body Mass Index (BMI). This index evaluates the relationship between weight and height to identify the nutritional status of individuals (Eknoyan, 2008). Due to the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic, this indicator was obtained through the self-report of weight in kilograms and height in meters provided by each participant. According to the literature, there is a high correlation between self-reported and actual BMI in university students (Escandón-Nagel and Larenas Said, 2020; Hastuti et al, 2017; Quick et al, 2015) and young adults with and without higher education (Martínez-Torres et al, 2014; Nikolaou et al, 2017; Olfert et al, 2018). The WHO criteria for adults aged 18 or older were used for classification (WHO, 2021).
Quasi-experimental, longitudinal field study with repeated measures (pretest, posttest at five weeks and one-year follow-up) in four intervention groups and two control groups by sex:
IG-1-PECANSS-R: PECANSS intervention group with booster intervention at six months.
IG-2-PECANSS: PECANSS intervention group without booster intervention.
CG-3-PECANSS: PECANSS control group (questionnaires only).
IG-4-BP-R: BP intervention group with six-month booster intervention.
IG-5-BP: BP intervention group without booster intervention.
CG-6-BP: BP control group (questionnaires only).
Body Project was initially presented to the director of the Institute of Health Sciences (ICSa) while PECANSS was presented to the director of the Institute of Agricultural Sciences (ICAp) for the authorization of its administration to students. It was subsequently presented to professors and students in the third and fourth semesters of the Bachelor’s Degree Program in Nutrition and Gerontology at ICSa and in Veterinary Medicine and Animal Husbandry and Agronomy for Sustainable Production at ICAp. When a teacher agreed to participate in the study, the entire group of students was assigned to one of the intervention subgroups, in the order in which each teacher agreed to participate. The first two groups were assigned to IG-1-PECANSS-R and IG-4-BP-R, the third and fourth groups to IG-2-PECANSS and IG-5-BP, and the last two groups formed CG-3-PECANSS and CG-6-BP. After providing their informed consent, each of the participants answered the entire battery of questions. Both interventions were administered from February to March 2021 in an online format. Each group (with 10 to 15 participants) was coordinated by a facilitator during five two-hour weekly sessions. The facilitators were trained by experts to administer both the Body Project and PECANSS to the students; all of them were graduates of the Bachelor’s Degree Program in Nutrition from UAEH and agreed to participate in the project as part of their social service. CG-3-PECANSS and CG-6-BP only answered the questionnaires at three moments. The protocol was approved by the Ethics and Research Committee of the UAEH Institute of Health Sciences (Code: CEI-2020-012).
This project, based on CD, was designed to reduce thin-ideal internalization (Stice et al, 2000) using verbal, written and behavioral exercises conducted in the sessions and the inter-session period. The workshop was divided into five two-hour weekly sessions, and the facilitator had a handbook for coordinating the group’s activities (available at http://www.bodyprojectsupport.org).
This Mexican psychoeducational and interactive program incorporating strategies based on CD consists of five two-hour sessions, in which students engage in playful physical activity (Saucedo-Molina et al, 2022). Session one begins with an appraisal of the concept of beauty in history, emphasizing the drastic changes in size in female and male models. Session two focuses on myths and realities about dieting and supplements. Sessions three and four contain nutritional content to correct false beliefs about eating and nutrition and to provide information on the nutrient content in food, healthy eating behaviors, and sample healthy menus. The final 90-minute session consists of three parallel workshops and is organized in such a way that all the groups participated in the three workshops on the same day. In the first session, participants made posters opposing the culture of thinness. For the second, students designed a healthy menu. The third was a rally in which participants engaged in various physical activities using materials such clothes (sweaters, pants, sweatshirts), plastic bottles, chairs, and kitchenware. PECANSS has digital manuals for teaching each of the sessions and organizing playful physical activity (Saucedo-Molina et al, 2018). Its contents include the global strategy for diet and physical activity proposed by WHO (WHO, 2022; Shamah-Levy et al, 2020).
Six months after the posttest, a booster session was given for the groups assigned to this modality, which lasted two hours and was taught by the same facilitators. In the session that received the IG-4-BP-R, topics such as costs (adverse effects) associated with the quest for the thin ideal, and the importance of body image were addressed; a dynamic (role-play) was organized to discourage the quest for the thin ideal and work was done on challenges, behavioral challenges and body activism. For IG-1-PECANSS-R, a workshop called Culture of Thinness was held, taking up aspects seen in several of the PECANSS presentations to show how the physical changes people have undergone over the years are not solely caused by the process of natural evolution, but rather by fashion trends that are often unhealthy.
Normality Shapiro-Wilk (n
The Results section presents the data collected. The data should be reported in sufficient detail to justify the conclusions. The most relevant results should be mentioned, including those that do not support the hypothesis. To determine whether the groups were comparable before administering the interventions, the sample was divided by sex and the Kruskal-Wallis test was administered. Although no differences were found among women, significant differences were observed among men in drive for muscularity (p = 0.011) and BMI (p = 0.039) (Table 1).
| Variables | Women | Men | ||||
| Mdn | (percentile 25; 75) | p | Mdn | (percentile 25; 75) | p | |
| Disordered eating behaviors | 5.00 | (3.00, 8.00) | 0.099 | 5.00 | (2.00, 8.00) | 0.177 |
| Thin ideal-internalization | 26.00 | (20.00, 33.00) | 0.633 | - | - | |
| Drive for muscularity | 24.00 | (19.00, 31.00) | 0.233 | 32.00 | (24.00, 42.00) | 0.011* |
| Body dissatisfaction | 24.00 | (20.00, 28.00) | 0.520 | 25.00 | (20.00, 32.00) | 0.407 |
| Negative affect | 31.00 | (24.99, 42.00) | 0.317 | 29.00 | (22.00, 37.00) | 0.213 |
| Moderate to vigorous physical activity | 208.39 | (134.88, 292.71) | 0.302 | 254.07 | (181.28, 365.78) | 0.287 |
| Body mass index | 22.86 | (20.43, 24.54) | 0.300 | 24.22 | (22.15, 27.14) | 0.039* |
Note: * p
In the groups of women, according to the Friedman test, the median value in DEB decreased over time in IG-1-PECANSS-R (p = 0.002; post-hoc pretest vs. posttest [p = 0.003]), IG-4-BP-R (p = 0.022; post-hoc pretest vs. posttest [p = 0.057]) and IG-5-BP (p = 0.007; post-hoc pretest vs. posttest [p = 0.033] and pretest vs. one-year follow-up [p = 0.033]). In regard to thin-ideal internalization, IG-4-BP-R (p = 0.0001; post-hoc pretest vs. posttest [p = 0.0001] and pretest vs. one-year follow-up [p = 0.049]) and IG-5-BP (p = 0.020; pretest vs. posttest [p = 0.033]) scores decreased over time, as did the drive for muscularity of the IG-2-PECANSS (p = 0.047). No significant differences were found in the post-hoc or IG-4-BP-R (p = 0.0001; post-hoc pretest vs. posttest [p = 0.0001] or pretest vs. one-year follow-up [p = 0.004]). Body dissatisfaction only decreased significantly over time in the IG-5-BP (p = 0.004; post-hoc pretest vs. posttest [p = 0.006]). In this variable, a higher score indicates greater satisfaction. Negative affect only decreased in the IG-3-BP-R (p = 0.004) pre-posttest, returning to slightly above the baseline value at follow-up (post-hoc posttest vs. one-year follow-up [p = 0.030]). MVPA increased in minutes/week in the IG-1-PECANSS-R over time (p = 0.043; post-hoc pretest vs. one-year follow-up [p = 0.042]), whereas in the IG-5-BP, it increased from pre to posttest (p = 0.044), almost returning to the baseline value at follow-up (no significant differences were found with post-hoc). In regard to BMI, Table 2 shows how three intervention groups experienced significant changes, decreasing between pre and posttest, yet returning to slightly above the initial value at one-year follow-up. The same happened with the CG-3-PECANSS, albeit with almost marginal significance (p = 0.049). After conducting post-hoc tests, significant differences were only found in the IG-2-PECANSS group (pretest vs. one-year follow-up [p = 0.043]) and IG-4-BP (posttest vs. one-year follow-up [p = 0.036]) (Table 2).
| Variable | Groups | Pretest | Posttest | One-year follow-up | W | |
| Median (p25, p75) | Median (p25, p75) | Median (p25, p75) | ||||
| Disordered eating behaviors (score) | IG-1-PECANSS-R | 5.00 (4.00–8.00) | 5.00 (3.00–6.00) | 4.50 (2.00–7.00) | 12.623 (0.002)’# | 0.16* |
| IG-2-PECANSS | 4.00 (2.25–9.00) | 5.00 (3.00–6.00) | 5.50 (2.25–8.75) | 0.725 (0.696) | 0.02 | |
| CG-3-PECANSS | 5.00 (2.00–7.00) | 6.00 (2.00–8.00) | 4.00 (2.00–8.00) | 2.974 (0.226) | 0.03 | |
| IG-4-BP-R | 5.00 (2.00–8.00) | 3.00 (2.00–5.75) | 4.00 (2.00–5.75) | 7.644 (0.022)’# | 0.10* | |
| IG-5-BP | 6.00 (5.00–11.00) | 5.00 (3.00–8.50) | 5.00 (3.00–8.00) | 10.047 (0.007)’# | 0.20* | |
| CG-6-BP | 4.00 (1.00–8.00) | 5.00 (1.00–9.00) | 5.00 (2.00–8.00) | 1.377 (0.502) | 0.02 | |
| Thin-ideal-internalization (score) | IG-1-PECANSS-R | 25.00 (22.00–31.50) | 22.00 (19.25–27.00) | 25.50 (19.25–31.75) | 9.243 (0.010)’# | 0.12* |
| IG-2-PECANSS | 27.50 (20.00–38.50) | 22.00 (17.50–35.75) | 27.00 (20.25–37.25) | 10.554 (0.005)’# | 0.26* | |
| CG-3-PECANSS | 26.00 (20.00–34.00) | 24.00 (19.00–35.00) | 27.00 (20.00–34.00) | 0.640 (0.726) | 0.01 | |
| IG-4-BP-R | 25.00 (20.25–30.00) | 20.00 (18.00–23.00) | 21.50 (18.00–25.00) | 22.110 (0.0001)’# | 0.28* | |
| IG-5-BP | 25.00 (22.00–36.50) | 22.00 (17.50–29.00) | 24.00 (21.00–33.00) | 7.832 (0.020)’# | 0.16* | |
| CG-6-BP | 30.00 (38.00–20.00) | 30.00 (20.00–35.00) | 27.00 (19.00–35.00) | 1.481 (0.477) | 0.02 | |
| Drive for muscularity (score) | IG-1-PECANSS-R | 22.00 (18.00–30.75) | 20.50 (16.25–28.75) | 22.00 (16.0–29.00) | 3.263 (0.196) | 0.04 |
| IG-2-PECANSS | 21.00 (15.00–27.00) | 18.00 (15.00–25.25) | 19.50 (15.25–29.75) | 6.136 (0.047)’# | 0.15* | |
| CG-3-PECANSS | 24.00 (20.00–30.00) | 23.00 (17.00–27.00) | 23.00 (19.00–28.00) | 5.053 (0.080) | 0.05 | |
| IG-4-BP-R | 25.00 (21.25–31.25) | 20.00 (17.00–27.75) | 23.00 (18.25–32.25) | 23.712 (0.0001)’# | 0.30** | |
| IG-5-BP | 26.00 (21.00–36.00) | 26.00 (16.00–33.00) | 25.00 (19.00–32.50) | 2.696 (0.260) | 0.05 | |
| CG-6-BP | 24.00 (19.00–33.00) | 24.00 (17.00–33.00) | 28.00 (18.00–32.00) | 0.339 (0.844) | 0.01 | |
| Body dissatisfaction (score) | IG-1-PECANSS-R | 24.00 (19.50–26.75) | 25.00 (19.00–29.75) | 23.50 (19.00–28.50) | 2.122 (0.346) | 0.03 |
| IG-2-PECANSS | 24.00 (19.00–29.75) | 23.00 (19.00–26.75) | 26.00 (18.50–31.00) | 0.861 (0.650) | 0.02 | |
| CG-3-PECANSS | 26.00 (18.00–34.00) | 24.00 (19.00–31.00) | 23.00 (17.00–31.00) | 5.270 (0.072) | 0.06 | |
| IG-4-BP-R | 24.00 (21.00–29.75) | 27.50 (21.25–34.00) | 25.00 (21.00–31.75) | 4.821 (0.090) | 0.06 | |
| IG-5-BP | 24.00 (22.00–26.00) | 31.00 (24.00–39.00) | 26.00 (19.50–37.50) | 11.109 (0.004)’# | 0.22* | |
| CG-6-BP | 22.00 (19.00–26.00) | 22.00 (19.00–27.00) | 22.00 (19.00–25.00) | 0.748 (0.688) | 0.01 | |
| Negative affect (score) | IG-1-PECANSS-R | 35.50 (25.50–52.75) | 30.50 (23.00–40.00) | 34.00 (25.50–47.00) | 5.228 (0.073) | 0.07 |
| IG-2-PECANSS | 32.00 (25.25–40.50) | 26.00 (23.00–35.75) | 32.00 (23.25–45.75) | 3.818 (0.148) | 0.10* | |
| CG-3-PECANSS | 32.00 (24.00–42.00) | 29.00 (22.00–49.00) | 37.00 (24.00–51.00) | 5.404 (0.067) | 0.06 | |
| IG-4-BP-R | 26.50 (23.00–35.00) | 23.50 (21.25–27.50) | 27.00 (21.50–34.00) | 13.813 (0.001)’# | 0.17* | |
| IG-5-BP | 31.00 (24.50–42.00) | 32.00 (22.00–39.00) | 32.00 (23.00–41.50) | 2.067 (0.356) | 0.04 | |
| CG-6-BP | 29.00 (25.00–44.00) | 31.00 (24.00–43.00) | 31.00 (24.00–43.00) | 4.952 (0.084) | 0.07 | |
| Moderate to vigorous physical activity (min/week) | IG-1-PECANSS-R | 181.25 (93.67–261.95) | 215.10 (147.31–336.95) | 230.34 (158.82–323.18) | 6.278 (0.043)’# | 0.08 |
| IG-2-PECANSS | 141.19 (100.60–276.49) | 205.37 (154.15–276.72) | 264.91 (188.06–417.46) | 4.641 (0.098) | 0.12* | |
| CG-3-PECANSS | 222.02 (156.99–276.20) | 236.11 (128.18–340.87) | 196.80 (145.35–306.42) | 0.553 (0.758) | 0.01 | |
| IG-4-BP-R | 224.63 (159.70–296.19) | 196.05 (141.25–298.41) | 197.54 (132.68–245.84) | 1.070 (0.586) | 0.01 | |
| IG-5-BP | 208.39 (153.21–354.37) | 278.32 (157.92–397.65) | 209.79 (174.56–339.12) | 6.268 (0.044)’# | 0.13* | |
| CG-6-BP | 225.95 (149.95–308.33) | 193.80 (146.95–294.70) | 222.02 (108.34–274.07) | 0.955 (0.620) | 0.01 | |
| Body mass index (kg/m2) | IG-1-PECANSS-R | 22.66 (20.31–24.44) | 22.63 (20.02–24.80) | 23.03 (20.89–24.49) | 7.930 (0.019)’# | 0.10* |
| IG-2-PECANSS | 23.07 (21.94–25.21) | 22.85 (21.94–26.14) | 23.95 (22.06–26.26) | 8.269 (0.016)’# | 0.21* | |
| CG-3-PECANSS | 22.60 (20.07–26.22) | 21.71 (19.83–25.39) | 23.04 (20.54–26.22) | 6.035 (0.049)’# | 0.06 | |
| IG-4-BP-R | 22.28 (20.10–23.98) | 22.24 (19.88–23.80) | 22.71 (20.69–24.20) | 7.456 (0.024)’# | 0.09 | |
| IG-5-BP | 23.61 (22.39–24.97) | 23.87 (22.07–25.91) | 24.12 (21.19–25.25) | 0.273 (0.873) | 0.01 | |
| CG-6-BP | 21.63 (19.79–23.43) | 22.65 (20.13–23.55) | 21.92 (20.56–23.43) | 0.053 (0.974) | 0.00 |
Note: PECANSS, Prevention of Unhealthy Eating Behaviors and Sedentary Lifestyle;
BP, Body project; IG-1-PECANSS-R (n = 40), PECANSS intervened group with booster
intervention; IG-2-PECANSS (n = 20), PECANSS intervened group without booster
intervention; CG-3-PECANSS (n = 47), PECANSS control group; IG-4-BP-R (n = 40),
Body Project intervened group with booster intervention; IG-5-BP (n = 25), Body
Project intervened group without booster intervention; CG-6-BP (n = 35), Body
Project control group. ’# Indicates significant differences p
Administering the Friedman test to male university students showed that negative affect only maintained a significant decrease over time in the IG-5-BP (p = 0.013; post-hoc pretest vs. posttest [p = 0.018]). It was interesting to observe how the pre-post-test score decreased in the CG-3-PECANSS (p = 0.014; post-hoc pretest vs. posttest [p = 0.022]) and the CG-6-BP (p = 0.014; post-hoc posttest vs. one-year follow-up [p = 0.017]), returning to the baseline value at follow-up. For MVPA, it only increased over time in IG-2-PECANSS (p = 0.005; post-hoc pretest vs. one-year follow-up [p = 0.004]). The IG-1-PECANSS also showed an increase over time in this variable, albeit not to a significant extent. Finally, BMI only increased significantly over time in the IG-4-BP-R (p = 0.010; post-hoc pretest vs. one-year follow-up [p = 0.041] and posttest vs. one-year follow-up [p = 0.041]) (Table 3).
| Variable | Groups | Pretest | Posttest | One-year follow-up | W | |
| Median (p25, p75) | Median (p25, p75) | Median (p25, p75) | ||||
| Disordered eating behaviors (score) | IG-1-PECANSS-R | 6.00 (3.25–7.75) | 4.00 (3.00–6.00) | 5.00 (2.00–7.75) | 1.107 (0.575) | 0.04 |
| IG-2-PECANSS | 5.00 (2.00–7.00) | 4.00 (2.00–5.00) | 4.00 (2.50–6.50) | 4.785 (0.091) | 0.10* | |
| CG-3-PECANSS | 4.50 (2.00–6.75) | 4.00 (1.00–6.00) | 3.50 (2.00–6.00) | 1.505 (0.471) | 0.02 | |
| IG-4-BP-R | 3.00 (1.00–7.00) | 3.00 (1.00–6.00) | 2.00 (1.00–6.00) | 0.980 (0.613) | 0.03 | |
| IG-5-BP | 7.50 (4.25–9.75) | 5.00 (3.25–7.00) | 5.00 (1.25–8.25) | 5.600 (0.061) | 0.23* | |
| CG-6-BP | 6.00 (3.00–9.00) | 5.00 (3.00–14.00) | 4.00 (1.00–11.00) | 4.850 (0.088) | 0.22* | |
| Drive for muscularity (score) | IG-1-PECANSS-R | 30.00 (23.00–34.50) | 28.00 (22.00–34.50) | 28.00 (19.00–34.00) | 0.918 (0.632) | 0.03 |
| IG-2-PECANSS | 31.00 (21.00–36.50) | 28.00 (17.50–38.00) | 27.00 (20.50–33.50) | 3.717 (0.156) | 0.07 | |
| CG-3-PECANSS | 26.50 (21.25–39.25) | 27.50 (20.00–37.75) | 27.00 (21.00–43.50) | 0.717 (0.699) | 0.01 | |
| IG-4-BP-R | 32.00 (26.00–40.00) | 32.00 (25.00–36.00) | 29.00 (24.00–35.00) | 0.464 (0.793) | 0.02 | |
| IG-5-BP | 44.00 (36.25–53.25) | 36.00 (30.75–49.75) | 41.00 (29.25–53.00) | 2.478 (0.290) | 0.10* | |
| CG-6-BP | 37.00 (27.00–53.00) | 30.00 (24.00–53.00) | 36.00 (22.00–47.00) | 0.333 (0.846) | 0.02 | |
| Body dissatisfaction (score) | IG-1-PECANSS-R | 21.00 (18.00–29.25) | 23.50 (19.50–27.75) | 25.00 (20.00–30.75) | 4.102 (0.129) | 0.13* |
| IG-2-PECANSS | 25.00 (18.00–30.50) | 27.00 (22.00–32.00) | 24.00 (19.00–29.50) | 1.400 (0.497) | 0.03 | |
| CG-3-PECANSS | 27.00 (21.25–36.75) | 26.00 (21.25–31.00) | 26.50 (22.50–29.50) | 4.222 (0.121) | 0.07 | |
| IG-4-BP-R | 24.00 (21.00–29.00) | 27.00 (25.00–34.00) | 26.00 (20.00–31.00) | 3.704 (0.157) | 0.12* | |
| IG-5-BP | 25.50 (18.00–27.75) | 27.00 (25.25–29.75) | 27.00 (21.50–35.25) | 5.511 (0.064) | 0.23* | |
| CG-6-BP | 24.00 (16.00–37.00) | 25.00 (9.00–34.00) | 25.00 (11.00–36.00) | 0.667 (0.717) | 0.03 | |
| Negative affect (score) | IG-1-PECANSS-R | 29.50 (23.25–35.75) | 29.50 (21.25–37.25) | 27.50 (20.50–39.00) | 0.036 (0.982) | 0.00 |
| IG-2-PECANSS | 22.00 (20.00–33.50) | 21.00 (20.00–32.50) | 23.00 (20.00–34.50) | 2.694 (0.260) | 0.05 | |
| CG-3-PECANSS | 30.50 (23.00–41.50) | 24.00 (21.00–42.50) | 29.00 (21.50–36.75) | 8.495 (0.014)’# | 0.13* | |
| IG-4-BP-R | 30.00 (21.00–49.00) | 23.00 (21.00–45.00) | 24.00 (20.00–49.00) | 4.039 (0.133) | 0.14* | |
| IG-5-BP | 31.00 (26.00–45.50) | 24.00 (20.25–37.75) | 25.50 (20.25–45.25) | 8.714 (0.013)’# | 0.37** | |
| CG-6-BP | 29.00 (23.00–41.00) | 25.00 (21.00–45.00) | 29.00 (23.00–80.00) | 8.600 (0.014)’# | 0.39** | |
| Moderate to vigorous physical activity (min/week) | IG-1-PECANSS-R | 215.29 (182.87–366.97) | 255.92 (182.87–407.84) | 280.22 (237.04–360.17) | 0.875 (0.646) | 0.03 |
| IG-2-PECANSS | 205.55 (143.48–280.35) | 242.24 (160.69–354.28) | 304.50 (219.35–362.55) | 10.577 (0.005)’# | 0.21* | |
| CG-3-PECANSS | 270.84 (179.46–347.59) | 244.65 (175.07–323.18) | 300.61 (189.45–362.96) | 5.688 (0.058) | 0.09 | |
| IG-4-BP-R | 258.65 (171.29–330.38) | 242.24 (153.21–326.81) | 236.11 (128.18–356.03) | 1.458 (0.482) | 0.05 | |
| IG-5-BP | 282.11 (214.57–408.86) | 231.08 (193.03–388.24) | 389.45 (291.11–439.26) | 4.167 (0.125) | 0.17* | |
| CG-6-BP | 364.17 (181.28–472.22) | 330.38 (227.25–406.80) | 302.56 (156.99–510.44) | 1.273 (0.529) | 0.06 | |
| Body mass index (kg/m2) | IG-1-PECANSS-R | 26.13 (22.32–29.46) | 25.80 (21.82–29.05) | 25.94 (22.64–29.10) | 1.298 (0.523) | 0.04 |
| IG-2-PECANSS | 26.64 (23.16–27.55) | 25.92 (23.00–2771) | 25.95 (24.24–29.06) | 5.614 (0.060) | 0.11* | |
| CG-3-PECANSS | 23.63 (21.22–25.99) | 24.01 (21.04–26.19) | 24.19 (20.76–26.65) | 4.544 (0.103) | 0.07 | |
| IG-4-BP-R | 23.73 (18.82–25.71) | 23.76 (18.04–25.95) | 24.24 (20.06–25.95) | 9.170 (0.010)’# | 0.31** | |
| IG-5-BP | 23.78 (21.79–25.20) | 23.51 (21.92–25.07) | 24.75 (22.68–26.63) | 2.167 (0.338) | 0.09 | |
| CG-6-BP | 24.56 (23.18–28.05) | 24.91 (23.16–27.71) | 25.71 (23.35–27.73) | 0.632 (0.729) | 0.03 |
Note: PECANSS, Prevention of Unhealthy Eating Behaviors and Sedentary Lifestyle;
BP, Body project; IG-1-PECANSS-R (n = 16), PECANSS intervened group with booster
intervention; IG-2-PECANSS (n = 25), Intervened group without booster
intervention; CG-3-PECANSS (n = 32), PECANSS control group; IG-4-BP-R (n = 15),
Body Project intervened group with booster intervention; IG-5-BP (n = 12), Body
Project intervened group without booster intervention; CG-6-BP (n = 11), Body
Project control group. ’# indicates significant differences p
An examination of the effect of the interventions between groups failed to
identify significant differences over time between the IGs and CGs. However,
after conducting post-hoc tests, we observed that in women, the internalization
of thinness registered differences (p
After presenting the results, the author is in a position to evaluate and interpret their implications, especially with respect to the original hypothesis. The author is free to analyze, interpret and qualify the results, as well as to draw inferences from them. The theoretical implications of the results and the validity of the conclusions can be emphasized.
The objective of this study was to evaluate the effect of two universal prevention programs based on CD, specifically the BP and the PECANSS, on DEB, thin-ideal internalization, body dissatisfaction, negative affect, drive for muscularity, and moderate-vigorous physical activity and BMI in a sample of Mexican university students of both sexes.
After the programs had been implemented, intragroup changes were identified in
some of the variables, mainly among female participants. DEBs were reduced in
women due to both interventions in all the IGs over time, whereas the CGs showed
no significant changes. These findings are similar to those of Wilson et al (2020), whose EAT-26 scores decreased in IG as opposed to CG students.
However, significant changes were only observed from pre- to post-test, and were
not maintained at one-month follow-up. Using Stop Obesity and Eating Disorders
(StopOBEyTA), Castillo et al (2016) found a significant interaction by
intervention group-time and a greater decrease in DEBs at follow-up in the IG, in
comparison with groups that did not receive the program. Using the BP,
Unikel-Santoncini et al (2019) achieved a decrease in DEB in a sample of men
and women at one-year follow-up. Conversely, using the Obesity and Eating
Disorders (OBEyTA) in a sample of university students of both sexes, Castillo et al (2019) failed to achieve effects in men. In women, it only had an effect
on attitudes toward food (EAT-26). Unikel-Santoncini et al (2023), again
using the BP but in university students of both sexes, only recorded a decrease
in DEB in women at one-year follow-up. These similarities with the findings of
the present study suggest that prevention programs based on CD are primarily
effective in women. In our study, non-significant changes in men could be due to
a floor effect (Saucedo-Molina et al, 2018; Saucedo-Molina et al, 2022; Stice et al, 2007) supported by their baseline score, which was well below the BQDEB
cut-off point (
Regarding thin-ideal internalization, evaluated in women, only the IG-1-PECANS-R, IG-2-PECANSS and IG-5-BP significantly decreased their pretest-posttest scores. The IG-4-BP-R group alone maintained this decrease over time. This is similar to what was reported by Stice et al (2013) through Healthy Weight 2 (HW2) in a sample of female university students, among whom body dissatisfaction and ED symptoms, as well as the incidence of ED, were reduced during the two-year follow-up comparing the IG and CG. Another evaluation of the BP in female students at three American universities revealed a significant reduction in the internalization of thinness, showing differences between the IG and CG (Stice et al, 2012). Through the OBEyTA, Castillo et al (2019) also managed to significantly reduce the score of this same variable at three-month follow-up although only in women. Using the BP, Unikel-Santoncini et al (2023) achieved an intragroup effect (in both sexes) by reducing thin-ideal internalization. To summarize our results, in 75% of the IG, thin-ideal internalization decreased pretest-posttest, whereas the IG-4-BP-R managed to maintain this decrease at one-year follow-up. This suggests that the booster intervention had a greater effect on this variable, which should be considered in future interventions given the importance of the latter in increasing the risk of an ED (Saucedo-Molina and Unikel, 2010).
Although men reported higher scores in drive for muscularity compared to women, which coincides with the literature (Barrientos-Martínez et al, 2014; Karazsia et al, 2017), our findings differ from what was reported in The Body Project: More Than Muscles (Brown et al, 2017), the only intervention designed for male university students in whom this variable decreased in the IG in comparison with the CG over the course of a month. In the present study, it only decreased intragroup in women in the IG-2-PECANSS and the IG-4-BP-R over time, suggesting that women currently oscillate between the idealization of a thin and/or muscular body.
Body dissatisfaction only decreased over time intragroup in women in the IG-5-BP who did not receive a booster intervention. This is consistent with the results of Stice et al (2012) in that body dissatisfaction decreased in the IG from pretest to two-year follow-up with the HW2 program. However, when the IG was compared with the CG, no significant differences were observed at follow-up. Additionally, Wilson et al (2020) reduced body dissatisfaction pretest-posttest, without maintaining this at one-month follow-up. Research projects that have successfully reduced dissatisfaction in the IG and CG in women include those run by Ridolfi and Vander Wal (2008) and Stice et al (2017), who specifically achieved change in groups with physician- or peer-led BP facilitators. Regarding this last intervention, in its virtual version (eBody Project), no changes were obtained in body dissatisfaction. Given that our research on the epidemiological situation (SARS-Cov-2) was conducted virtually, this probably limited its effect on the results.
Negative affect only decreased in the IG-4-BP-R pretest-posttest in women, rising slightly above the baseline score at one-year follow-up. Negative affect is a factor associated with the development of ED (Polivy and Herman, 2002). In the research directed by Stice et al (2017) using the BP in female university students, the authors managed to significantly reduce negative affect over time in the three IGs. Unlike our study, theirs did not report increases in values at six-month follow-up. In the case of men, the IG-5 BP showed a reduction in negative affect over time, suggesting that the BP was effective for them even without a booster intervention. However, the CG scores of both the BP and the PECANSS also decreased pretest-posttest, almost returning to the initial scores at one-year follow-up. What happened with the CG was probably merely due to the fact of administering the evaluation instrument that created an effect per se.
One of the central variables in this research was MVPA because PECANSS, as previously noted, seeks to prevent a sedentary lifestyle by promoting physical activity (PA). This is how the women in the IG-1-PECANSS-R and the men in the IG-2-PECANSS maintained an increase in MVPA over time. At the same time, the IG-5-BP of women increased significantly pretest-posttest, nearly returning to the baseline level at follow-up. These findings confirm the effectiveness of the PECANSS, since in a previous evaluation of adolescents of both sexes, it managed to increase MVPA in the entire sample at six-month follow-up (Stice et al, 2007). By administering HW2, Stice et al (2012), only increased pretest-posttest PA in the IG of female students, with researchers only reporting a significant difference in the posttest between IG and CG. Finally, Castillo et al (2019) did not record interactions by sex, group, or time for PA in their intervention.
As for BMI, the three PECANSS groups and the IG-4-BP-R in women showed a pretest-posttest decrease and an increase above baseline levels at one-year follow-up. These results differ from those reported in other research projects in which there was no effect on the BMI of participants (Castillo et al, 2016; Castillo et al, 2019; Stice et al, 2012; Wilson et al, 2020). This decrease in BMI in pretest-posttest women was probably due to the sessions focusing on myths and realities about dieting, correcting false beliefs about eating and nutrition, providing information on the nutrient content in food, healthy eating behaviors, and designing healthy menus. The increase in BMI at one-year follow-up probably occurred because during data collection, the pandemic was ending (February–March, 2022), diluting the effect of the interventions. In men, the IG-1-BP-R showed a sustained increase over time for BMI, probably related to the decrease in MVPA. Although this change was not significant, the medians decreased over time. These findings in men partly coincide with those reported by Castillo et al (2019), who failed to find a significant interaction between group type and time for this variable.
Regarding the effect between groups, after one-year follow-up with both programs, no significant differences were observed between the IG and CG in any of the variables evaluated. It was therefore impossible to determine whether any of them had a greater effect on DEB, psychological variables, MVPA, or BMI.
Even though other interventions have achieved changes between groups in short-term follow-ups at one to three months (Brown et al, 2017; Castillo et al, 2016; Wilson et al, 2020) or one and four years (Stice et al, 2012; Stice et al, 2013; Stice et al, 2017; Unikel-Santoncini et al, 2019; Unikel-Santoncini et al, 2023), they have not had an effect on all the variables included (Stice et al, 2013), or in the same way in men as in women. For example, in their study sample of both sexes, Castillo et al (2019) only reported differences in two of the eight variables evaluated, specifically in women.
It can therefore be concluded that the BP and PECANSS have a specific effect on the behavioral and cognitive variables evaluated. The BP is effective in reducing DEB, thin-ideal internalization, drive for muscularity, body dissatisfaction in women (intragroup) and negative affect in men. PECANSS, in turn, decreased DEB and drive for muscularity in women (intragroup) and increased moderate-vigorous physical activity in both sexes (intragroup). At the same time, considering the suggestions and results of other research on booster sessions, it would be important to conduct further research on this subject, since at the intragroup level, particularly in women, it was observed that positive results were achieved in almost all variables in the subgroups that received booster sessions of both the BP and PECANSS. However, a comparison of results at one-year follow-up found no differences between the groups with and without a booster session, coinciding with the findings of Taylor et al (2006), who, through an online ED prevention program, did not find that the booster session was beneficial. Furthermore, the main limitation of this study was having worked with a non-probabilistic sample, which prevents results from being generalized. In addition, the study should be replicated with other populations and age groups, particularly with adolescents who are at a high risk for the development of eating disorders. It would also be useful to reduce the imbalance between men and women, since 65% of the sample were women. Notwithstanding the above, through this article, we are contributing to knowledge of the prevention of disordered eating behaviors and eating disorders in the youth population, by determining the effectiveness of two interventions conducted online with men and women based on cognitive dissonance theory.
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
TJSM and CUS designed the research study. YGA, TJSM and CUS performed the research. LEBB provided help and advice on the programme intervention. TJSM, YGA, LEBB and CUS analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was carried out in accordance with the guidelines of the Declaration of Helsinki. The protocol was approved by the Ethics and Research Committee of the UAEH Institute of Health Sciences (Code: CEI-2020-012). All patients or their families/legal guardians gave their informed consent for inclusion before they participated in the study.
Not applicable.
Yazmín González-Alvarado was a PhD student with a grant from the Consejo Nacional de Humanidades, Ciencias y Tecnologías and a beneficiary of the scholarship program through the PhD Program in Food Science and Human Health at the Autonomous University of Hidalgo.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.