

 , Imán Yazbeck Morell 3, María-José Sánchez-López 4, Marta García Pla 5, Olga Parra Ordaz 2,6, Adrià Arboix 7,*
, Imán Yazbeck Morell 3, María-José Sánchez-López 4, Marta García Pla 5, Olga Parra Ordaz 2,6, Adrià Arboix 7,*
1 Neurology Service, Sleep Disorders Unit, Hospital Universitari Sagrat Cor, Grupo Quirónsalud, 08029 Barcelona, Spain
2 Medicine Department, University of Barcelona, 08036 Barcelona, Spain
3 Department of Internal Medicine, Hospital Universitari Sagrat Cor, Grupo Quirónsalud, 08029 Barcelona, Spain
4 Medical Library, Hospital Universitari Sagrat Cor, Grupo Quirónsalud, 08029 Barcelona, Spain
5 Family and Community Medicine, CAP La Mina (ICS), 08930 Sant Adrià de Besòs, Barcelona, Spain
6 Department of Pneumology, Sleep Disorders Unit, Hospital Universitari Sagrat Cor, Grupo Quirónsalud, 08029 Barcelona, Spain
7 Cerebrovascular Division, Department of Neurology, Hospital Universitari Sagrat Cor, Grupo Quirónsalud, Universitat de Barcelona, 08029 Barcelona, Spain
Abstract
Central sleep apnea (CSA) syndromes and acute ischemic stroke are linked by a complex, bidirectional relationship. After ischemic stroke, CSA prevalence rises markedly compared with the general population, in which it is usually below 1%. In stroke cohorts, CSA frequencies of around 8%–12% have been reported, although estimates are heterogeneous owing to differing diagnostic criteria. In this scoping review we map the evidence on CSA syndromes during sleep in patients with stroke, summarizing prevalence, mechanisms, clinical correlates, and prognostic implications.
The Medline (PubMed), Scopus, Cochrane Reviews, and Web of Science databases were searched for observational and interventional studies published from inception to August 31 2025 in English and Spanish assessing CSA syndromes in adults with ischemic stroke. Two reviewers independently screened records, selected studies, and extracted data on study design, stroke characteristics, CSA definitions, comorbidities, and clinical outcomes; disagreements were resolved by consensus with a third reviewer.
Fifty-five studies including several thousand patients with ischemic stroke were identified. Across studies, post-stroke CSA prevalence ranged from approximately 8% to 12%, clearly exceeding rates in the general population. CSA was often reported in the absence of overt cardiac comorbidities, and patients with CSA tended to have lower body mass index and fewer classic cardiovascular risk factors than those typically described with obstructive sleep apnea. Pathophysiological analyses emphasized disturbed central ventilatory control after cerebral ischemia; however, several studies did not show a consistent association between specific lesion locations and CSA occurrence, suggesting that stroke may unmask CSA in predisposed individuals rather than cause it solely through focal damage. In older adults, CSA appeared as an independent correlate of ischemic stroke and a potential marker of silent cerebral injury or impaired central respiratory regulation.
Available evidence indicates that CSA syndromes during sleep are substantially more frequent in patients with ischemic stroke than in the general population and may be associated with increased cerebrovascular risk and subclinical brain injury. Heterogeneity in CSA definitions, diagnostic protocols, and outcome measures limits firm conclusions. Standardized criteria and adequately powered prospective studies are needed to clarify the mechanistic and prognostic role of CSA in stroke.
Keywords
- central sleep apnea
- sleep apnea syndromes
- stroke
- ischemic
- sleep-disordered breathing
- brain ischemia
Ischemic stroke remains a leading cause of death and long-term disability worldwide, and its prognosis is strongly influenced by coexisting cardiovascular and respiratory comorbidities [1]. Sleep‑disordered breathing is highly prevalent in patients with acute ischemic stroke and has emerged as a potentially modifiable factor that may affect both early neurological recovery and long‑term vascular outcomes. Within the spectrum of sleep‑disordered breathing, central sleep apnea (CSA) syndromes have received comparatively less attention than obstructive sleep apnea, yet they may be particularly relevant in the cerebrovascular setting because they reflect instability of central ventilatory control rather than upper airway collapse.
Obstructive sleep apnea is characterized by repeated upper-airway collapse during sleep, whereas central sleep apnea reflects reduced or absent respiratory effort due to instability of central ventilatory control. In stroke patients, these two entities may coexist, but they differ in their predominant pathophysiology, diagnostic scoring, and potential management. CSA is characterized by recurrent episodes of absent or markedly reduced ventilatory effort during sleep, leading to cyclical fluctuations in ventilation, oxygen saturation, and autonomic activity [2]. In the general population, CSA is considered uncommon, with a prevalence well below 1%. In contrast, several cohort studies have shown that the frequency of CSA increases substantially after acute ischemic stroke, with reported prevalence estimates in the range of approximately 8–12%, although figures vary depending on diagnostic criteria, recording methods, and timing of the sleep study relative to the index event [3]. This disproportionate rise in CSA burden after stroke, compared with its rarity in community samples, underscores the possibility of a specific pathophysiological link between cerebral ischemia and disordered central control of breathing during sleep.
The mechanisms underlying CSA in the post‑stroke setting appear multifactorial and are not yet fully understood. Experimental and clinical data indicate that lesions involving supratentorial autonomic networks or infratentorial structures, particularly the medulla, can disrupt the integration of chemoreceptor input and the generation of respiratory rhythm, thereby predisposing to ventilatory instability and central apneic events. However, several imaging‑based studies have failed to demonstrate a consistent association between particular lesion locations and the occurrence of CSA, suggesting that ischemic injury may act as a facilitator or trigger in individuals with pre‑existing vulnerability rather than as a single, focal “lesion site” responsible for CSA [3]. This uncertainty regarding lesion topography and causal pathways complicates risk stratification and the design of targeted interventions. Although the included studies support a network-level disturbance of central ventilatory control, they provide little direct molecular or biomarker evidence on neurotransmitter pathways or chemoreceptive signaling in post-stroke CSA.
Clinically, CSA after ischemic stroke has important potential consequences. Observational evidence indicates that the presence of CSA is associated with higher mortality, poorer functional recovery, and an increased risk of cardiovascular complications [4]. These associations are biologically plausible: CSA promotes ventilatory instability, intermittent nocturnal hypoxemia, and surges in sympathetic nervous system activity, all of which may exacerbate ongoing cerebral injury, impair neuroplasticity, and adversely affect cardiac function. Unlike obstructive sleep apnea, CSA in stroke patients often occurs in the relative absence of obesity and with fewer traditional cardiovascular comorbidities such as long‑standing hypertension or diabetes, highlighting that its prognostic impact may not be fully captured by classical vascular risk scores [3]. Importantly, however, current data do not conclusively demonstrate that CSA increases the risk of recurrent ischemic events, and the directionality of the association between CSA burden and stroke outcomes remains incompletely defined.
Management of sleep‑disordered breathing in stroke is an area of active debate. European guidelines encourage systematic screening and treatment of sleep apnea in the acute phase of stroke as part of secondary prevention strategies, whereas American Heart Association and American Stroke Association documents do not mandate routine screening at this stage, reflecting persisting uncertainty about the strength of evidence and feasibility in acute care. Therapeutic decisions depend on the predominant type and severity of sleep apnea. Continuous positive airway pressure (CPAP) is the standard of care for obstructive sleep apnea, but in patients with predominantly central events and high apnea–hypopnea indices, especially in the setting of ventilatory instability without hypercapnia, adaptive servo‑ventilation (ASV) is often considered the preferred modality. In hypercapnic forms of CSA, non‑invasive ventilation may be necessary to provide adequate ventilatory support [3].
Existing interventional studies suggest that treatment with CPAP or ASV in stroke populations is generally safe and may improve daytime symptoms, quality of life, and certain measures of neurological recovery. Nevertheless, the evidence base remains limited, and the impact of treating CSA on long‑term survival, recurrent stroke risk, and broader cardiovascular outcomes is far from settled. Moreover, most clinical trials and observational cohorts have focused primarily on obstructive sleep apnea, leaving CSA and mixed central patterns under‑represented and often analyzed only in small subgroups. As a result, there are currently no specific, evidence‑based recommendations dedicated to the management of CSA syndromes in the context of ischemic stroke, and clinical practice is largely extrapolated from other populations or guided by expert opinion.
In view of these gaps, a comprehensive mapping of the literature on CSA syndromes during sleep in patients with ischemic stroke is urgently needed. A scoping review, conducted according to the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) extension for scoping reviews (PRISMA‑ScR), is particularly well suited to capture the breadth and heterogeneity of available evidence, including diverse study designs, varying definitions of CSA and central periodic breathing, and a wide range of clinical and imaging outcomes. The aim of this scoping review is therefore to systematically chart the characteristics, pathophysiological insights, and clinical implications of CSA syndromes after ischemic stroke, and to identify key knowledge gaps that should inform future mechanistic and interventional research.
In the present review, CSA is used as an umbrella term for central apneas and central hypopneas, whereas central periodic breathing and Cheyne–Stokes respiration are treated as descriptive phenotypes that may occur within the broader CSA spectrum
This review was conducted in accordance with the PRISMA‑ScR, following a predetermined protocol agreed upon by all authors (Supplementary Material-PRISMA checklist). Institutional review board approval was not required because the study analysed only previously published data. The study protocol was registered with the Open Science Framework (OSF) under the identifier DOI: 10.17605/OSF.IO/H59RJ.
The objective of this scoping review was to identify and synthesize the available evidence on CSA syndromes in adults with ischemic stroke. The primary research question was: What is the extent of evidence on the prevalence, clinical manifestations, diagnostic methods, management strategies, and outcomes of CSA syndromes in adults with ischemic stroke across different care settings and disease phases?
Population: Studies were eligible if they included adults (
Concept: Eligible studies explored the impact of CSA syndromes on stroke patients, including aspects of pathophysiology, diagnosis, treatment, clinical progression, or prognostic significance.
Context: Studies conducted in any healthcare setting (acute hospital units,
rehabilitation centers, or community environments) and at any stage of illness
(acute
All types of quantitative, qualitative, and mixed‑methods research were eligible. These included randomized controlled trials, non‑randomized controlled studies, before‑and‑after or interrupted time‑series designs, prospective and retrospective cohorts, case‑control and cross‑sectional studies, as well as descriptive studies such as case series. Qualitative research using phenomenology, grounded theory, or ethnographic approaches was also accepted. In addition, systematic or scoping reviews meeting the inclusion criteria were considered for inclusion.
Exclusion criteria included:
Studies involving pediatric or non‑human populations.
Editorials, commentaries, and letters to the editor.
Conference abstracts, protocols, or documents without full text.
Papers without specific data on CSA syndromes or without confirmed ischemic stroke populations.
No restriction regarding geographic region was applied.
The literature search covered PubMed (https://pubmed.ncbi.nlm.nih.gov), Scopus (https://www.scopus.com/), Web of Science (Core Collection) (https://www.webofscience.com/wos/woscc/basic-search), and the Cochrane Library (https://www.cochranelibrary.com) databases from inception to 31 August 2025. Searches were restricted to articles published in English or Spanish. An initial pilot search was performed in PubMed to identify key Medical Subject Headings (MeSH) terms and free‑text related to two broad blocks of search terms: “sleep apnea, central” (“periodic breathing”, or “Cheyne-Stokes respiration” or “central breathing disorders”) and ischemic stroke (“brain stem infarctions” or “cerebral infarction” or “brain infarction” or “brain ischemia” or “cerebrovascular disorders”). The final PubMed strategy was adapted for the other databases (Supplementary Material I). To ensure completeness, the reference lists of all included papers and relevant systematic reviews were manually examined for additional studies. Grey literature and non‑peer‑reviewed publications were excluded.
All references retrieved from electronic databases were imported into Zotero 7 for Windows (v. 7.0.22) (Corporation for Digital Scholarship, https://www.zotero.org/) for reference management and duplicate removal. The selection process was conducted in two stages.
First, two independent reviewers screened article titles and abstracts for relevance against the predetermined inclusion criteria. Second, full‑text versions of all potentially eligible studies were obtained and evaluated independently by the same reviewers. Any disagreements were resolved by discussion or consultation with a third reviewer. Data extraction was conducted independently by two reviewers using a customized Microsoft Excel‑based extraction form designed specifically for this review (Supplementary Material II). Extracted data included the authorship, year of publication, country, study design, sample size, stroke type, lesion location, phase of disease, diagnostic methods, quantitative respiratory indices (CAI, Cheyne–Stokes respiration percentage, total AHI), comorbidities (atrial fibrillation, congestive heart failure, pulmonary disease), and reported outcomes including neurological severity (NIHSS), functional recovery (mRS, Barthel Index), mortality, and therapeutic interventions (e.g., CPAP or adaptive servo‑ventilation). Any inconsistencies identified during data extraction were discussed and resolved by consensus. Revisions to the extraction form made during the process were documented to ensure transparency.
Extracted data were organized according to the following variables:
Study characteristics (design, country, publication year).
Population data and stroke characteristics (phase, lesion location).
Diagnostic procedures applied for identifying CSA syndromes.
Main clinical and neurological outcomes (NIHSS, mRS, mortality).
Reported management and therapeutic strategies for CSA syndromes.
Each article’s main findings were summarized to describe the scope and nature of evidence addressing the predefined research question.
Because of the methodological heterogeneity of included studies, a quantitative meta‑analysis was not feasible. Instead, findings were synthesized in a narrative framework and systematically analyzed according to level of evidence, following the hierarchical standards of evidence‑based medicine.
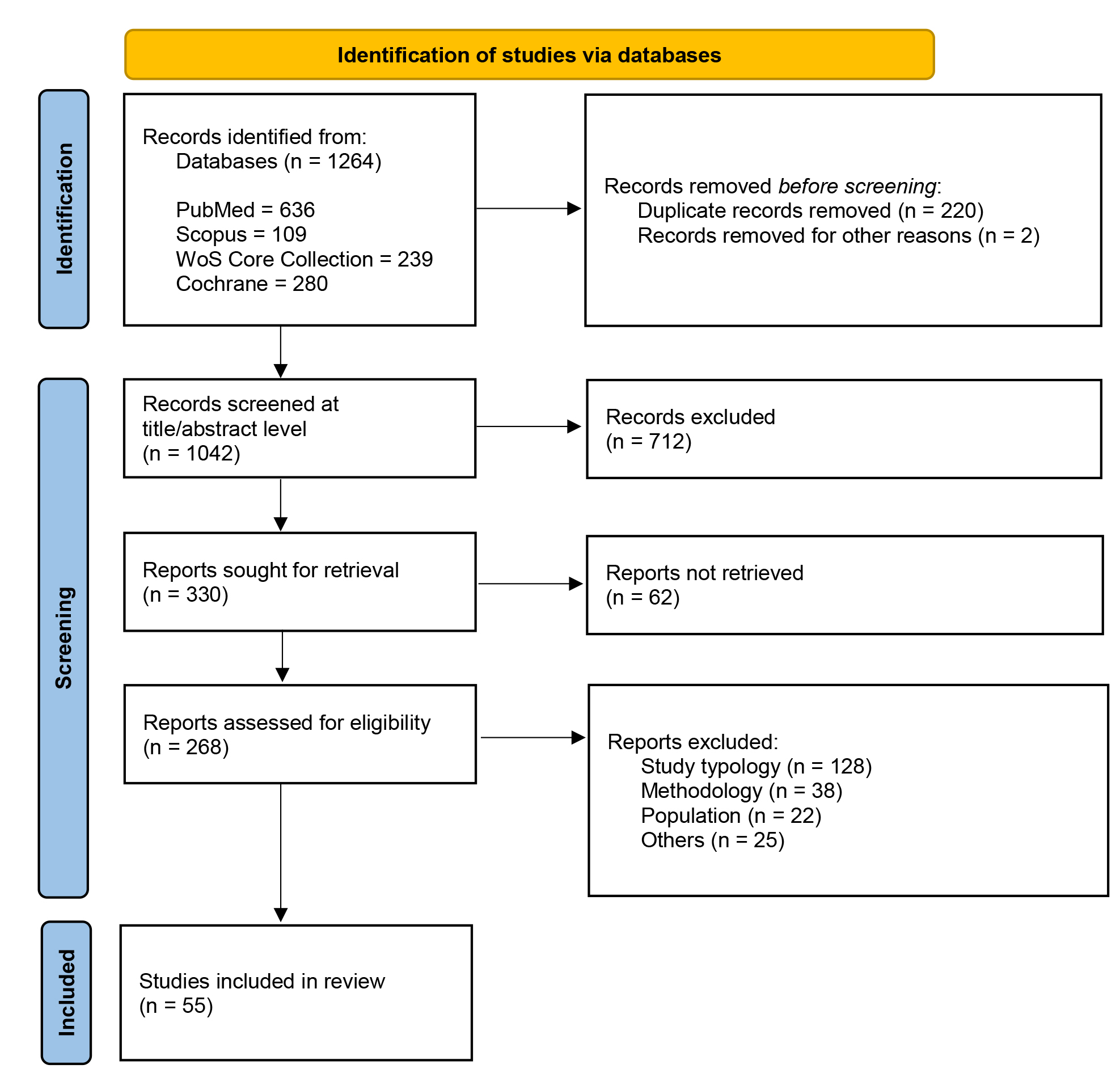
At the database level, 1264 records were identified (PubMed n = 636, Scopus n = 109, Web of Science Core Collection n = 239, Cochrane n = 280), with 220 duplicate records and 2 additional records removed before screening. After de‑duplication, 1042 records were screened at title/abstract level, and 712 were excluded. Of 330 reports sought for retrieval, 62 could not be retrieved; 268 full texts were assessed for eligibility, and 213 were excluded mainly due to study typology (n = 128), methodology (n = 38), population (n = 22), or other reasons (n = 25). The final scoping review included 55 studies (Fig. 1).
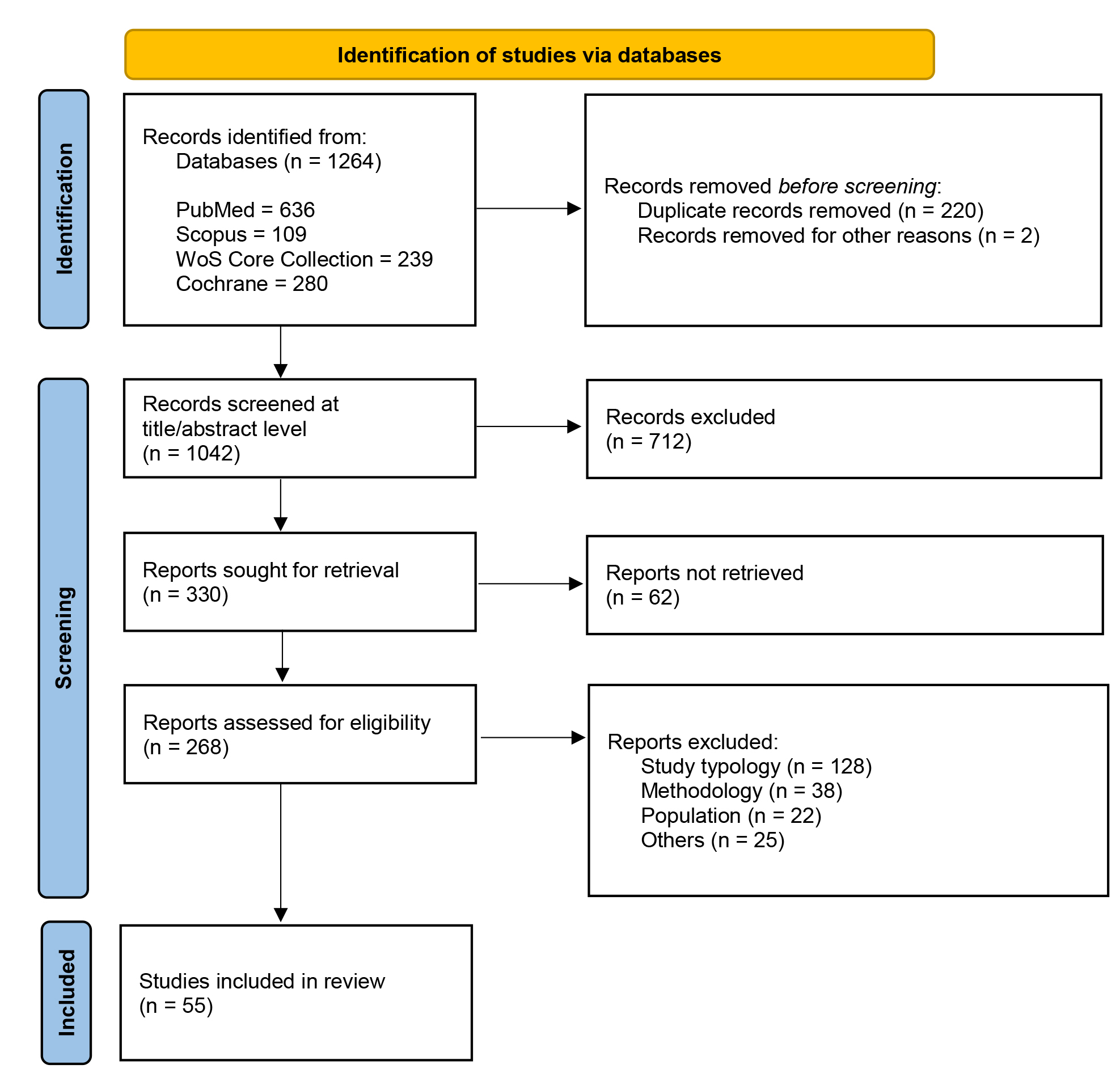 Fig. 1.
Fig. 1.
PRISMA 2020 flow diagram of study selection. The systematic search across four databases identified 1264 records. Fifty-five studies met final criteria for analysis. PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
Across the 55 included studies Table 1 (Ref. [3, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57]), 20 provided original CSA or central periodic breathing (CPB)/Cheyne–Stokes respiration (CSR) data in adult patients with ischemic stroke or mixed stroke cohorts including ischemic stroke [3, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17] to larger observational cohorts (n = 139 [6]; n = 156 [7], 2006; n = 182 [11], 2018; n = 166 [12], 2020) and a population‑based home sleep apnea test (HSAT) cohort of 1346 ischemic stroke patients [17].
| Author & Year | Study design | Sample size (N) | Stroke phase (acute/subacute/chronic) | Type of sleep study (PSG/polygraphy) | Definition of CSA/CSB (index) | CAI or AHI (central-related) | Main clinical outcomes reported (CSA/CSB-related) | Level of Evidence (OCEBM) | |
| 1 | Baillieul S et al., 2022 [3] | Prospective monocentric cohort; cross-sectional analysis at |
185 first ischemic stroke patients | Chronic (median 134.5 days after stroke onset) | Full-night in-laboratory polysomnography | Central AHI (cAHI); coexisting and central sleep apnea defined by cAHI/AHI |
Central AHI reported (events/h) and proportion of central events (cAHI/AHI) | Prevalence of coexisting/central sleep apnea 42.9% among moderate–severe SDB; higher cerebellar lesion frequency and heightened hypercapnic ventilatory response in coexisting/central SA vs no/mild SDB; association of infratentorial lesions, male sex, obesity and age |
Level 1b |
| 2 | Parenti A et al., 2005 [21] | Case report with neuropathologic examination (two fatal cases) | 2 patients | Chronic CSA with acute fatal medullary ischemic–hypoxic lesions; stroke lesions described as acute at death in medullary tegmentum | Diagnostic nocturnal polysomnography before death | Central sleep apnea described by central apneas per hour; no explicit CAI label; CSA defined clinically by central apneas with hypoxia and hyperventilation phases | Case 1: 38 central sleep apneas/hour; Case 2: 35 central sleep apneas/hour | Acute bilateral ischemic–hypoxic lesions of solitary tract nuclei in chronic CSA; suggestion that CSA-related hypoxemia contributes to selective stroke of solitary tract nuclei and that CSA may contribute to stroke pathogenesis via hypoxia/hemodynamic oscillations | Level 4 |
| 3 | Qu XR et al., 2024 [22] | Single-patient case report with detailed diagnostic and PAP titration studies | 1 patient | Subacute (sleep study performed about 3 months after acute medullary/bulbar infarction) | In-laboratory nocturnal polysomnography with PAP titration and transcutaneous CO2 monitoring | Central apnea–hypopnea index (central AHI); CSA defined as acquired central sleep apnea after medullary infarction with central AHI predominating, occurring almost exclusively in Rapid Eye Movement (REM)sleep | Central apnea–hypopnea index 70.1 events/h (baseline PSG) | REM-predominant CSA with severe desaturations (ODI 50.8/h, nadir SpO2 72%); marked reduction of central events after CPAP 16 cm H2O and near resolution with BiPAP ST 17/13 cm H2O when PtcCO2 maintained above apneic threshold; sustained symptomatic improvement at 6 months of home NIV | Level 4 |
| 4 | Bassetti C et al., 1997 [23] | Prospective observational study of consecutive acute stroke patients | 39 patients with first acute ischemic stroke | Acute (polysomnography mean 10 days after stroke onset; range 1–49 days) | Bedside overnight polysomnography | Sleep apnea diagnosed if AHI |
AHI in NREM and REM reported; central vs obstructive proportions given; no single CAI but central apnea burden described within CSB and central SA definitions | 67% had sleep-disordered breathing; OSA in 54%, CSB in 28% (often coexisting with OSA); abnormal breathing during wakefulness in 18%; prevalence and severity of SDB similar in supra- vs infratentorial strokes; trend to poorer short-term outcome in those with breathing abnormalities, especially CSB and wake abnormalities | Level 2b |
| 5 | Power WR et al., 1982 [24] | Single-patient case study with two polysomnographic nights | 1 patient | Chronic (sleep complaints and CSA dating back 10 years after cerebral infarction) | Full-night polysomnography on two separate nights | Cheyne–Stokes respiration (CSR) characterized as central periodic breathing; no explicit CAI; CSA defined by cyclical central apneas and hyperpneas; analysis by proportion of CSA time in each sleep stage | No numeric CAI; CSA occupied 88% of light NREM and 83% of slow-wave sleep; 2% of REM sleep time showed CSA, 98% regular respiration | CSA predominantly during NREM sleep with near-normal respiration in REM; CSA-linked arousals (≈23/h during CSA vs 8/h with normal breathing) caused severe sleep fragmentation and insomnia; supports concept of separate CNS mechanisms for REM vs NREM respiratory control | Level 4 |
| 6 | Rowat AM et al., 2006 [7] | Prospective observational cohort of acute stroke patients with portable respiratory monitoring and imaging correlation | 134 patients with acute stroke | Acute (patients included within 24 h of a suspected first or recurrent ischemic or hemorrhagic stroke) | Validated portable continuous monitoring equipment (Embletta PDS, Medcare Flaga) recording breathing patterns; no full polysomnography described | Central periodic breathing (CPB), including Cheyne–Stokes respiration, defined as cyclical increases in rate and depth of breathing alternating with hypopnea/apnea; no numeric CAI cut-off given | Not reported as CAI or central AHI; CPB presence (yes/no) and proportion of time are described but no explicit CAI/AHI values provided | CPB was associated with large acute cerebral hemispheric lesions, severe mass effect, and previously reported poor functional outcome at 3 months; no association with severity of prior cerebrovascular disease | Level 2 |
| 7 | Siccoli MM et al., 2008 [9] | Prospective observational study of consecutive first-ever acute ischemic stroke patients with nocturnal respirography and cardiac workup | 74 patients | Acute (patients admitted within 96 hours after stroke onset; first night after admission studied) | Overnight respirography with a validated portable device (Autoset Embletta PDS, ResMed), not full PSG | CPBS defined as |
In all patients: central apnea index 7 |
CPBS was frequent (present in 72%; |
Level 2 |
| 8 | Sacchetti ML and Della Marca G, 2014 [25] | Narrative hypothesis/theoretical article proposing a classification of stroke plus SDB phenotypes; not an original patient cohort study | Not applicable (no explicit patient series with N; article is conceptual) | Discusses ischemic stroke in general; acute/subacute/chronic phases are mentioned conceptually but no defined phase for a specific cohort | Refers broadly to polysomnography (PSG) and analysis of sleep microstructure (CAP) in stroke patients, but no single study protocol is reported | Discusses OSA, CSA, Cheyne–Stokes respiration, complex sleep apnea, loop gain and CAP, but does not define CSA/CSB by a specific numeric index such as CAI or central AHI | Not reported; indices such as AHI/CAI are mentioned in cited literature and figures but no explicit central index values are presented for a defined stroke cohort within this paper | Main outcome is a proposed four-subgroup classification of stroke plus SDB phenotypes to help identify potential best responders to CPAP; no primary clinical outcome data (e.g., mortality or functional scores) reported | Level 5 |
| 9 | De Paolis F et al., 2012 [26] | Single-patient case report with serial cardio-respiratory monitoring | 1 patient | Acute post-stroke (central sleep apnea documented three days after a cardio-embolic ischemic stroke) | Portable cardiorespiratory monitoring (nasal flow, thoracic/abdominal movements, oxygen saturation, heart rate); not full PSG | Central sleep apnea syndrome with central apnea index; Cheyne–Stokes breathing mentioned in background, but CSA is characterized by central apnea index rather than a separate CSB label | Before stroke: AHI 28/h, central apnea index 3/h; three days after stroke: AHI 70/h, central apnea index 56/h; under BiPAP: AHI 1/h, ODI 2/h | Stroke in a patient with OSAS led to conversion to severe central sleep apnea syndrome, requiring change from CPAP to BiPAP to control central events; illustrates that acute lacunar stroke can unmask or induce CSA in OSAS | Level 4 |
| 10 | Brill AK, et al., 2014 [18] | Single-centre retrospective analysis of ASV treatment for CSA in post-acute ischemic stroke patients without CHF | 15 patients with CSA related to ischemic stroke out of 154 ASV-treated patients | Post-acute/chronic: ASV started a median of 11 months after the acute cerebrovascular event; patients with acute stroke |
Polysomnography or cardiorespiratory polygraphy used to diagnose non-hypercapnic CSA before ASV; follow-up based on ventilator-reported residual events | CSA defined as non-hypercapnic central sleep apnea/ with |
Baseline AHI 46.7 |
ASV significantly reduced AHI and tended to reduce Epworth Sleepiness Scale scores, with mean nightly ASV use 5.4 |
Level 3 |
| 11 | Hermann DM et al., 2007 [8] | Prospective case series from a cohort (31 acute first-ever stroke patients, 3 with CPBS described in detail) | 31 stroke patients total; 3 with CPBS | Acute (polysomnography and respirography within first 10 days, mean 4.6 |
Polysomnography plus respirography (Autoset) | CPBS defined as |
AHI used; CPBS patients had predominantly central apneas/hypopneas (e.g., AHI 5, 25, 28/h in acute phase; Autoset central AHI also reported) | Presence of CPBS in unilateral supratentorial/thalamic strokes; association with lesions in insula, cingulate cortex, thalamus; spontaneous partial resolution of CPBS and improvement in AHI and desaturations at 1–3 months | Level 4 |
| 12 | Rowat AM et al., 2006 [7] | Prospective observational cohort study | 156 monitored stroke patients; 138 with usable breathing recordings; 33 with CPB | Acute (recording started median 4 h after stroke; within 24 h of onset; follow‑up 3 months) | Portable multi‑channel respiratory monitoring (nasal pressure, thoracic/abdominal bands, pulse oximetry; not full PSG) | CPB defined as regular crescendo–decrescendo pattern with apnea (cessation) or hypopnea ( |
No specific CAI; CPB quantified as % of valid recording time with CPB (median 38 min; many |
CPB present in 24%; associated with more severe strokes, congestive heart failure, dysphagia, reduced consciousness; independently associated with death or dependency (mRS |
Level 2 |
| 13 | Rupprecht S et al., 2010 [27] | Cross‑sectional prospective study | 59 patients with internal carotid artery stenosis: 49 extracranial (eICA), 10 intracranial (iICA) | No clinical stroke phase; asymptomatic carotid stenosis (non‑stroke population) | Standard overnight polysomnography | CSA defined by cAHI |
cAHI (central apnea–hypopnea index); relation of cAHI to stenosis severity and HRV parameters reported | CSA occurred in 39% with eICA stenosis, none with isolated iICA stenosis; CSA associated with severe ( |
Level 3 |
| 14 | Muñoz R et al., 2012 [28] | Population‑based prospective cohort study | 394 stroke‑free, community‑dwelling subjects |
No baseline stroke (primary prevention); incident ischemic stroke during follow‑up in elderly | Fully attended overnight polysomnography | Central apnea index (CAI; number of central events per hour). CSA episodes defined by central apneas (no thoraco‑abdominal movement) with |
CAI (central apnea index); CAI categories ( |
Higher CAI associated with increased risk of incident ischemic stroke; event‑free survival lowest in highest CAI group; adjusted HR ≈2.65 for CAI |
Level 2 |
| 15 | Schütz SG et al., 2021 [17] | Population‑based cohort of ischemic stroke patients with cross‑sectional HSAT assessment soon after stroke | 1346 ischemic stroke participants with analyzable home sleep apnea tests | Recent ischemic stroke; HSAT median 13 days after stroke recognition (IQR 6–21 days) | Home sleep apnea test (ApneaLink Plus; limited‑channel polygraphy, not full PSG) | CAI (central apnea index) = central apneas per hour; CSA defined as CAI |
CAI reported (median 0/h overall); CSA prevalence 1.4% (19/1346) | CSA prevalence low (1.4%) after ischemic stroke; CSA more common in males and in non‑obese (normal/overweight) vs obese; no significant association of CSA with NIHSS, heart failure, or most comorbidities; suggests CSA is uncommon after stroke and HSAT may be acceptable when PSG not feasible | Level 2–3 |
| 16 | Nogueira RC et al., 2021 [29] | Single-patient case report (case study) | 1 | Acute phase “during the acute phase of stroke” and 1 day after admission, NIHSS 20 at onset, thrombolysis 3.5 h after ictus | No polysomnography; respiratory pattern and Cheyne–Stokes respiration assessed with transcranial Doppler, blood pressure Finometer, and end-tidal CO2 capnography | Cheyne–Stokes respiration described clinically only no numeric index, no CAI/CSB threshold given | Not reported; only qualitative presence of CSA-related oscillations in cerebral blood flow velocity and blood pressure | CSA associated with large periodic oscillations in cerebral blood flow velocity, blood pressure, and end-tidal CO2, with impaired myogenic control (abnormal resistance-area product) in the affected hemisphere, while metabolic control (critical closing pressure) followed CO2 changes | Level 4 |
| 17 | Franklin KA, 2002 [30] | Narrative clinical review (non-systematic) of human studies on cerebral haemodynamics in obstructive sleep apnea and Cheyne–Stokes respiration | Not applicable review article synthesising multiple published studies; no single N | Mixed phases; includes acute, subacute, and chronic post-stroke and heart failure populations from prior studies, but no single phase defined for this review | Various methods summarized from prior work including transcranial Doppler, Xenon‑133 regional cerebral blood flow, SPECT, and polysomnography however, the review does not present a single, unified sleep-study modality or dataset | Discusses central apnea and Cheyne–Stokes respiration conceptually but does not define CSA/CSB by a specific index threshold within this article | Reports example values such as central AHI patterns and cerebral blood flow velocity changes from individual cited studies, but no single CAI/AHI for a defined study cohort is presented in this review | Central apnea with Cheyne–Stokes respiration shows decreased cerebral blood flow velocity during apnea and increased flow after apnea termination, whereas obstructive apnea shows the opposite pattern with potentially hazardous cerebral hypoperfusion after apnea; obstructive sleep apnea is suggested as a potential risk factor for stroke because of repeated nocturnal cerebral hypoperfusion | Level 5 |
| 18 | Nopmaneejumruslers C et al., 2005 [10] | Prospective cohort study of consecutive stroke patients with polysomnography and echocardiography | 93 stroke patients | Subacute/early rehabilitation; echocardiography 40 |
Full overnight polysomnography with standard scoring; central and obstructive events differentiated using respiratory inductance plethysmography and thoracoabdominal movement patterns | CSA defined as central apneas and hypopneas |
Central AHI 24.7 |
CSA prevalence 19 in rehabilitation stroke cohort; CSA associated with lower mean nocturnal transcutaneous PCO2 (39.5 vs 43.0 mmHg) and a higher prevalence of LV ejection fraction |
Level 2 |
| 19 | Hasan F et al., 2021 [19] | Systematic review and meta-analysis of observational studies (prospective, retrospective, case–control, cross-sectional) reporting prevalence of sleep disorders after stroke/TIA | 64,047 adults from 169 studies 14,032 stroke survivors and 1061 TIA cases in SDB analyses; larger numbers for insomnia and RLS groups | All three phases separate analyses for acute ( |
Sleep-disordered breathing and PLMS diagnosed mainly by in‑laboratory polysomnography (77 studies) or home-based polysomnography (55 studies); insomnia and RLS assessed by diagnostic criteria or questionnaires | Most SDB studies combined obstructive and central sleep apnea; the meta-analysis does not provide a specific CSA/CSB definition or index cut-off (e.g., separate CAI) for central events alone | Pooled prevalence of mild SDB AHI |
Sleep-disordered breathing, insomnia, periodic leg movements in sleep, and restless legs syndrome are highly prevalent throughout acute, subacute, and chronic phases after stroke/TIA; moderate–severe SDB prevalence appears to decrease over time; age, sex, comorbidities, smoking, and region significantly moderate prevalence; findings support importance of systematic screening and treatment of sleep disorders across stroke phases | Level 1 |
| 20 | Nachtmann A et al., 1995 [5] | Prospective observational study of consecutive acute ischemic stroke inpatients with respiratory monitoring and a non-stroke control group | 32 conscious patients with acute ischemic stroke and 20 age‑matched controls | Acute phase patients admitted within 3 days after onset of ischemic stroke and monitored while still acute | Bedside respiratory monitoring for |
Cheyne–Stokes respiration defined as periodic modulation of respiratory motion amplitude |
Central-related indices given as frequency of CSA cycles mean modulation frequency 0.7/min; no CAI or central AHI value is reported | CSR present in 17/32 (53%) of acute ischemic stroke patients (59% supratentorial and 40% infratentorial strokes), unrelated to infarct location; CSA associated with periodic drops in arterial oxygen saturation, with mean and minimal SaO2 lower than controls, and both intravenous theophylline and low‑flow oxygen inhalation promptly normalized breathing pattern and oxygen saturation without adverse effects | Level 3 |
| 21 | Hardavella G et al., 2006 [31] | Narrative review (physiopathology, clinical data, therapy) | Not applicable (review) | Not specified as a single phase; discusses acute and longer‑term after stroke | Not a primary sleep‑study; summarizes prior work (no single PSG/polygraphy protocol reported) | Discusses Cheyne–Stokes respiration as recurrent central apneas with crescendo–decrescendo tidal volume; no quantitative CAI/AHI cut‑off defined | Not reported as a specific CAI/AHI; only qualitative description of central apneas/Cheyne–Stokes cycles | Cheyne–Stokes respiration described as common after stroke, associated with severe neurological derangement and possibly higher mortality, and considered a marker of poor prognosis especially with coexisting heart failure | Level 5 |
| 22 | Kim Y et al., 2018 [11] | Observational cohort (prospective registry‑based analysis of consecutively admitted acute ischemic stroke patients with sleep test) | 182 ischemic stroke patients with analyzable sleep studies | Acute ischemic stroke (onset within 1 week; sleep test at mean |
Portable cardiorespiratory sleep study (limited‑channel polygraphy; no electroencephalogram (EEG) | CSA defined per 2016 AASM v2.3: |
Central apnea index significantly higher in CSA vs non‑CSA (median CAI 14.2 vs 1.33 events/h) | CSA present in 19.1 of patients; independently associated with higher premorbid mRS, bilateral hemispheric lesions, left‑atrial enlargement (higher LAVI) and left‑ventricular ejection fraction |
Level 2b |
| 23 | Mekky J et al., 2023 [16] | Case–control study (first‑ever ischemic stroke patients vs age‑matched controls with overnight PSG) | 93 ischemic stroke patients and 50 controls | Subacute phase (PSG within 1 week after stroke; NIHSS followed at 1 month) | Full attended overnight PSG | Central sleep apnea reported via “CSA index” and central AHI component; no specific numeric CAI threshold given for CSA definition beyond standard AASM scoring | Central sleep apnea index higher in stroke vs controls (mean CSA index 1.77 vs 0.14 events/h) and AHI higher in cortical than other sites; desaturation index and lowest SpO2 worse in sizable infarcts | Stroke patients had worse sleep architecture and higher AHI, CSA index, and desaturation index than controls; cortical strokes showed higher moderate–severe AHI; sizable infarcts had higher limb movement index, higher desaturation index, and lower minimal SpO2; lower minimal SpO2 at 1 week correlated with worse NIHSS at 1 month | Level 3b |
| 24 | Srijithesh PR et al., 2024 [32] | Prospective observational longitudinal cohort | 111 recruited ischemic stroke patients; 105 with adequate baseline PSG; 56 with follow‑up PSG | Subacute/early chronic: baseline PSG within 6 weeks of ischemic stroke onset; repeat PSG at |
Full overnight level‑1 PSG | Central sleep apnea quantified by central apnea index; SDB defined by total AHI (cut‑offs: AHI |
At baseline, 7.6 had CAI |
High prevalence of SDB after ischemic stroke (mainly obstructive); AHI and arousal index decreased over 3–4 months, with improvements in sleep efficiency and REM sleep; moderate–severe SDB (AHI |
Level 2b |
| 25 | Johnson KG & Johnson DC, 2010 [33] | Systematic review and meta‑analysis of observational studies | 29 studies, 2343 patients with ischemic/hemorrhagic stroke or TIA | Mixed phases (acute to chronic): timing ranged from within 1 week to |
Mix of full PSG with EEG, limited‑channel studies, and auto‑CPAP diagnostic mode | Central sleep apnea/Cheyne–Stokes reported as “primarily central apnea” proportion and via AHI thresholds; 17 studies reported percentage of patients with primarily central apneas (no uniform CAI cut‑off reported) | Across 17 studies, 7 (95% CI 4.5–12.0) of patients had primarily central apnea; global SDB prevalence: AHI |
SDB is very common after stroke/TIA (mostly obstructive); only a small proportion have predominantly central apnea; SDB prevalence did not differ significantly by event type, timing after stroke, or monitoring type; higher SDB rates seen in males, recurrent strokes, and strokes of unknown etiology, lower in cardioembolic strokes | Level 2a |
| 26 | Huhtakangas JK et al., 2022 [34] | Prospective observational cohort of consecutive ischemic stroke patients with sleep study and long-term follow-up | 204 ischemic stroke patients with cardiorespiratory polygraphy | Acute (sleep study within first 48 h after symptom onset) with 6-year follow-up | Unattended cardiorespiratory polygraphy (portable type 4 device, ApneaLink Plus) | Central apnea index (CAI, events·h-1) used; central sleep apnea defined when |
Mean CAI 3.9/h overall; CAI higher in non-survivors (over twofold vs survivors; exact values not separately tabulated); in REI |
Higher CAI, greater nocturnal hypoxemia (longer T90, lower minimum SaO2) associated with increased long-term mortality after ischemic stroke, but polygraphy variables including CAI did not predict recurrent ischemic events; CPAP users had fewer recurrent events but numbers were small | Level 2b |
| 27 | Hudgel DW et al., 1993 [35] | Physiologic comparative study of convalescent unilateral stroke patients vs healthy elderly controls, with detailed respiratory mechanics during sleep | 8 stroke patients and 8 age-, sex-, and size-matched healthy elderly controls (respiratory analysis subset) | Subacute/chronic ( |
Full polysomnography with additional upper airway resistance and EMG measurements | Central vs obstructive events differentiated by presence/absence of inspiratory EMG; Cheyne–Stokes–like periodic breathing described; no explicit numeric CAI definition label, but central vs obstructive apneas classified for AHI and pattern analysis | Group mean apnea–hypopnea index 44 |
Stroke patients showed larger oscillations in upper airway resistance and tidal volume during NREM sleep leading to more obstructive apneas/hypopneas and greater oxygen desaturation; periodic/irregular breathing with mechanical (upper airway) component demonstrated in convalescent stroke | Level 3 |
| 28 | Lisabeth LD et al., 2019 [36] | Population-based prospective cohort with repeated sleep studies and GEE modeling | 414 first-ever ischemic stroke patients with at least one portable sleep apnea test (total 1656 sleep studies across time points) | Mixed acute/subacute/chronic: baseline at median 5 days after stroke, then 3, 6, and 12 months | Portable home sleep apnea testing (ApneaLink Plus) at hospital or home | Central apnea index (CAI, central apneas·h-1) and obstructive apnea index (OAI) as components of respiratory event index (REI, apneas+hypopneas·h-1); central apneas defined by absent respiratory effort on pneumatic effort sensor | Baseline mean CAI 1.6 |
SDB (elevated REI) was common and remained stable through 12 months; obstructive component worsened slightly, whereas central component increased only in non-Hispanic Whites; ethnic differences in CAI trajectory identified but central events did not remit overall | Level 2b |
| 29 | Gregori-Pla C et al., 2019 [37] | Pilot physiologic study (prospective case series) of acute ischemic stroke patients with simultaneous diffuse correlation spectroscopy and respiratory polygraphy | 28 screened with pulse oximetry; 5 patients with |
Acute (within first 7 days after anterior circulation ischemic stroke; median 4 days) | Respiratory polygraphy (Embletta MPR PG) plus pulse oximetry, simultaneous with near‑infrared diffuse correlation spectroscopy for CBF | Apneas classified as obstructive, central, or mixed by standard polygraphy (absence vs presence of respiratory effort); AHI (events·h-1) and ODI3 used; one patient showed predominantly central apneas with Cheyne–Stokes–like periodic breathing; no standalone CAI label reported | Reported AHI values per case: 13–63.8 events/h, including one patient with mainly central apneas and another with obstructive events; central vs obstructive indices not separately quantified beyond pattern description | Individual apneas/hypopneas were associated with biphasic bilateral microvascular CBF changes (≈27–29% increase then ≈19–21% decrease) and concurrent HR increase and SpO2 fall; patients with highest AHI (including central pattern) had most severe strokes and poor 3‑month outcome (two deaths), suggesting potential detrimental hemodynamic impact of CSA/CSB in acute stroke | Level 4 |
| 30 | Kario K et al., 2004 [38] | Single-patient case report | N = 1 (67‑year‑old man with congestive heart failure, carotid occlusion, and nocturnal ischemic stroke) | Chronic cerebrovascular disease with new nocturnal-onset ischemic stroke; sleep study performed about 1 month after the episode | Nocturnal pulse oximetry plus full polysomnography | Central apnea–dominant sleep-disordered breathing documented: polysomnography AHI 55/h with 71% central apneas (explicit central predominance of Cheyne–Stokes–type breathing) | AHI 55 events/h, 71% central; nocturnal pulse oximetry showed 29.2 episodes/h of |
Newly developed central sleep‑disordered breathing with frequent desaturations temporally associated with nocturnal-onset ischemic stroke in a patient with congestive heart failure and carotid occlusion; authors propose nocturnal hypoxemia and blood pressure reduction as triggers of nocturnal ischemic events in patients with marginal cerebral perfusion | Level 4 |
| 31 | Javaheri S et al., 2017 [39] | Narrative review of observational and interventional studies | Not applicable (review) | Mixed; includes chronic heart failure and post‑stroke populations, not confined to a single stroke phase | Full polysomnography and limited-channel studies are described, but no single uniform protocol; multiple modalities across cited studies | CSA and Hunter–Cheyne–Stokes breathing generally defined by central apneas and periodic breathing with apneic threshold physiology rather than a single numeric CAI/AHI cut-off | Central AHI values vary across cited studies a typical example is baseline AHI ≈40 events/h with CSA/HCSB predominance in CANPAP and SERVE‑HF, but no single central index is defined for all cohorts | In stroke and other cerebrovascular disease, CSA/HCSB is associated with hyperadrenergic state and may improve with PAP or ASV central-event suppression improved sympathetic markers and ejection fraction in heart failure cohorts, while post‑stroke CSA tends to decrease over time unless driven by comorbid heart disease | Level 3–4 |
| 32 | Stevens D et al., 2018 [40] | Narrative mini‑review | Not applicable (review) | Covers acute and chronic post‑stroke phases; notes SDB is more severe in acute phase and persists in |
Both full polysomnography and respiratory polygraphy are discussed wide use of polygraphy in stroke cohorts is emphasized | CSA generally defined by central apneas |
Reports that stroke cohorts have higher prevalence of CSA |
CSA after stroke is common but its specific impact on functional recovery, mortality and lesion‑location relationships remains unclear limited data suggest central events often decrease over months, and ASV for post‑stroke CSA has only retrospective support without outcome data | Level 3–4 |
| 33 | Riglietti A et al., 2021 [15] | Prospective physiological cohort study with 3‑month follow‑up | 70 screened; 60 analyzed with baseline and 3‑month follow‑up sleep studies | Acute (within 10 days of onset; median 3.4 |
Respiratory polygraphy (Nox T3 cardiorespiratory monitoring; no EEG) | CSA defined by “dominant central sleep apnea (d‑CSA)” when |
In acute phase, d‑CSA group had mean central AHI AHIc 27.5 |
Central patterns including CSA and mixed CSA/OSA improved substantially over 3 months, whereas obstructive patterns remained frequent CSA was associated with distinct autonomic profile (higher baroreflex gain and ANSI in d‑CSA without hypertension and in infratentorial lesions), suggesting different autonomic adaptations vs OSA | Level 2b |
| 34 | Martínez‑García MA et al., 2004 [6] | Prospective observational cohort | 139 patients with acute ischemic stroke | Acute: polysomnography within 72 hours of symptom onset (mean 1.4 |
Limited‑channel respiratory polysomnography with Autoset Portable Plus II; automated AHI plus manual scoring of apnea type | Central apneas defined by absence of thoracoabdominal movement on belt; Cheyne–Stokes breathing defined as characteristic crescendo‑decrescendo central pattern for |
Central apnea index (AIc) 2.4 |
Central events and Cheyne–Stokes breathing were uncommon (5 patients with CSA) compared with obstructive events; nocturnal strokes had higher AHI and more obstructive apneas, supporting pre‑existing OSA as a stroke risk particularly for night‑onset events | Level 2b |
| 35 | Liu X et al., 2021 [20] | Systematic review and meta‑analysis of observational cohorts | 75 studies; 8670 stroke patients in pooled analysis | Mixed phases; stroke phase categorized as acute ( |
Type 1 attended full PSG, type 2 unattended full PSG, and type 3 devices; only studies using PSG (types 1–3) included | CSA defined as central events making up |
Central sleep apnea prevalence 10.0% (95% CI 6.5–14.9) among stroke patients obstructive events accounted for 53.1% of cases overall; central prevalence estimates pooled across different CAI cut‑offs and definitions | Central sleep apnea is less common than obstructive events but present in a substantial minority; prevalence varies with stroke subtype (higher in hemorrhagic, supratentorial, cardioembolic) and phase, but heterogeneity remains high and central vs obstructive patterns are not consistently separated in outcomes | Level 2a |
| 36 | Folgueira A et al., 2021 [14] | Descriptive, cross‑sectional, retrospective study of hospitalized acute ischemic stroke patients with nocturnal PSG | 53 | Acute (PSG within first 7–10 days after stroke onset) | Full‑night polysomnography with oximetry (PSG nivel 1 and 2) | Central apneas defined and quantified; report “índice de apneas centrales” and tendency to more central apneas in infratentorial lesions (index used CAI/central apnea index) | Central apnea index reported (Índice de apneas centrales); global AHI mean 24.5 |
High prevalence of SDB/OSA (84.9%) in acute ischemic stroke; infratentorial lesions showed lower minimal oxygen saturation and greater tendency to central apneas, suggesting more severe respiratory compromise in these locations | Level 3 |
| 37 | Ott SR et al., 2020 [12] | Prospective, multinational, multicentre observational cohort with full‑night PSG at baseline and 3‑month follow‑up | 166 with baseline PSG; 105 with both baseline and 3‑month PSG | Acute stroke/TIA with PSG within first 7 days; follow‑up at 3 months (chronic phase) | Attended full‑night polysomnography (PSG) scored by AASM 2012 criteria | SDB defined as AHI |
Mean AHI 21.4 |
High prevalence and persistence of SDB after acute stroke/TIA; CSA more often severe and associated with higher AHI and ODI; AHI at baseline predicted worse functional outcome (mRS |
Level 2 |
| 38 | Pavšič K et al., 2020 [13] | Prospective observational cohort with serial PSG in acute ULMI and follow‑up | 28 | Acute and subacute (PSG at |
Polysomnography (portable PSG in ward during acute phase, full PSG in sleep lab at follow‑up) | Central sleep apnea defined by central AHI (cAHI) |
Median acute‑phase AHI 16.5 (5.5–43.3); cAHI 11.0 (3.3–29.1); CAI 8.3 (2.2–23.8) events/h; at follow‑up AHI and cAHI significantly decreased (p = 0.007 and p = 0.003) while obstructive AHI did not change | CSA was very common in acute ULMI (CSA alone in 43%, plus additional patients with mixed patterns); central events frequently occurred in NREM sleep and during wakefulness; central indices improved over months, suggesting stroke‑induced instability of respiratory control with partial recovery | Level 2 |
| 39 | Noradina AT et al., 2006 [41] | Cross‑sectional, prospective study of recent ischemic stroke patients with portable sleep study (type 4) | 28 | Recent/acute–subacute (sleep studies within 1–4 weeks after stroke onset) | Limited portable monitoring (ResMed Autoset Portable II; airflow and SaO2 only, no EEG/EMG; corresponds to respiratory polygraphy) | SDB defined by AHI |
AHI used as global index; mean AHI 17.5 |
Very high prevalence of SDB after recent ischemic stroke; diabetes mellitus and smoking were independent predictors of significant SDB (AHI |
Level 3 |
| 40 | Lee MC et al., 1976 [42] | Prospective observational study of respiratory patterns in acute brainstem infarction using impedance pneumography and arterial blood gases | 23 | Acute (patients admitted within 72 hours of symptom onset, monitored during first 2 weeks) | Impedance pneumography with chart recording of respiratory pattern; not a PSG or standard polygraphy (no sleep staging, no AHI/CAI) | Central pattern disturbances defined clinically as Cheyne–Stokes respiration (CSR) and Cheyne–Stokes variant (CSV), cluster breathing, tachypnea; no numerical CAI/AHI indices | No CAI/AHI reported; patterns (CSR/CSV/tachypnea) described qualitatively and related to lesion size and bilaterality; blood gases showed respiratory alkalosis with CSR and tachypnea | CSR and CSV occurred frequently in acute brainstem infarction; prominent CSR or sustained tachypnea were associated with extensive bilateral pontine lesions and poor prognosis (high mortality), whereas normal/CSV‑predominant patterns with unilateral lesions had better outcomes | Level 3 |
| 41 | Hermann DM and Bassetti CL, 2003 [43] | Narrative review/opinion statement (Current Treatment Options in Neurology) | Not applicable | All phases discussed; includes acute and 3‑month follow-up data from cited studies | Describes respiratory polygraphy for acute stroke; polysomnography for complex cases | Refers to “central sleep apnea” and “Cheyne–Stokes breathing (CSB)” but no single numeric CAI threshold; SDB severity mainly by AHI | Reports SDB prevalence using AHI |
Suggests CSB and central events improve with oxygen or theophylline; CPAP or other ventilatory support may suppress central apnea/CSB and improve oxygenation in acute ischemic stroke cases | Level 5 |
| 42 | Baillieul S et al., 2022 [44] | Narrative review in Lancet Neurology | Not applicable | Explicitly covers acute ( |
Discusses polysomnography (type 1 and 2) as gold standard and respiratory polygraphy (type 3 and 4) as alternative screening/diagnostic tools | Defines central sleep apnea as |
Summarises central sleep apnea prevalence 8–12% using central AHI criteria (central AHI |
States that evidence on CSA effects on mortality and functional outcome after stroke is scarce and inconsistent, but suggests central events may persist and require re‑evaluation; focuses clinical outcome data mainly on obstructive events | Level 2 |
| 43 | Tanayapong P and Kuna ST, 2021 [45] | Clinical review (narrative review) in Sleep Medicine Reviews | Not applicable | Reviews SDB before stroke (risk) and after stroke; includes acute and chronic phases but not restricted to a single phase | Focuses on in‑laboratory polysomnography as diagnostic standard; mentions home sleep apnea testing as possible tool | Defines SDB with AHI; distinguishes OSA vs CSA by |
Provides pooled data that CSA occurs in |
Concludes CSA data are too sparse to firmly link CSA to incident stroke or to clear recurrence/mortality risk, whereas SDB/OSA clearly worsen neurological recovery and increase recurrence and mortality; CSA impact remains uncertain | Level 2 |
| 44 | Alexiev F et al., 2018 [46] | Narrative review (Journal of Thoracic Disease) | Not applicable | Addresses SDB both as risk factor and as consequence of stroke; considers acute and longer‑term evolution of SDB after stroke | Refers broadly to sleep studies (apnea–hypopnea index from polysomnography or respirography); specific modality varies across cited work, not a single uniform method | Notes that CSA/CSB are frequent in early days after stroke and linked to older age, stroke severity/extension, and LV dysfunction; does not set a numeric CSA/CSB index definition beyond general AHI use | Summarises that one‑third of stroke survivors have AHI |
States that both OSA and CSA appear to increase long‑term mortality risk in stroke patients and that early CSB/CSA correlate with worse severity and LV dysfunction, but quantitative CSA‑specific outcome effects remain limited | Level 5 |
| 45 | Plomaritis P et al., 2023 [47] | Single-center prospective observational longitudinal study | 130 acute stroke patients (110 ischemic stroke, 20 intracerebral hemorrhage) | Acute stroke (polysomnography within 72 h from symptom onset; 3‑month functional follow‑up) | Type 2 unattended overnight polysomnography with full EEG/EOG/EMG, airflow, respiratory effort, oximetry, position, ECG | SDB defined as AHI |
Mean AHI 33.5 |
CSA presence (vs OSA) strongly associated with congestive heart failure (OR 18.295 for central apnea detection); higher AHI and higher NIHSS independently predicted worse 3‑month functional outcome (mRS 0–1 vs 2–6), indicating SDB severity adversely affects recovery, while central vs obstructive type itself was not an independent outcome predictor | Level 2 |
| 46 | Bonnin-Vilaplana M et al., 2009 [48] | Prospective observational cohort of consecutive lacunar stroke patients | 68 (with radiologically proven lacunes) | Acute (respiratory study within first 48–72 h after stroke onset) | Respiratory polygraphy (portable respiratory recording device, validated vs PSG) | Central apnea index (CAI); Cheyne–Stokes respiration defined as periodic breathing with central apnea/hypopnea |
20.6% of patients had CAI |
Cheyne–Stokes respiration present in 20.6% of acute lacunar stroke patients; higher CAI and Cheyne–Stokes respiration associated with higher AHI; smoking and capsular/pontine lacunes associated with higher SRBD burden; no clear short-term outcome difference, but recommendation that smokers with capsular/pontine lacunar stroke be screened for SRBD | Level 2 |
| 47 | Pajediene E et al., 2020 [49] | Prospective observational study with questionnaire screening and PSG in a selected subgroup | 66 total; 13 underwent PSG | Acute (patients examined 3–10 days after first stroke symptoms) | Full-night PSG with video (portable system, AASM scoring) | Central sleep apnea defined as |
Central apnea index not given as a mean; CSA present alone in 1 patient and combined OSA+CSA in 2; AHI used for OSA severity, but central-related summary limited to presence/absence | In this highly symptomatic acute stroke subgroup, 12/13 had a sleep disorder: 1 CSA, 2 OSA+CSA, several with PLMD and/or RBD and insomnia; non-breathing disorders (PLMD, RBD, insomnia) were as frequent as breathing disorders; no significant association between stroke type/location and PSG measures; findings support routine screening beyond sleep apnea alone | Level 3 |
| 48 | Patrizz A et al., 2023 [50] | Experimental animal study (mouse model; randomized to MCAO or sham, with physiological and behavioral testing) | Not expressed as human N; multiple groups of young and aged mice (numbers per group given for each experiment, e.g. stroke n ≈ 14–17, sham n ≈ 10–11 in key analyses) | Experimental post-stroke period (post-ischemic days 3–42; translation to acute/chronic human phases not directly defined) | Whole-body plethysmography (not PSG) for breathing; no classical human sleep study, but apnea/Cheyne–Stokes–like patterns quantified | Apnea frequency (apneas/min) used as main index; Cheyne–Stokes–like periodic breathing pattern described; CO2 and hypoxic ventilatory responses measured but no CAI label | Apneas markedly increased after MCAO; minute ventilation reduced (hypoventilation) with Cheyne–Stokes–like pattern; severity of apneas correlated with progressive cognitive decline (Barnes maze, fear conditioning); distal MCAO produced apnea and cognitive deficits only in aged mice; chemoreceptor gain largely preserved, suggesting network/plant-gain mechanisms | Not reported | Level 5 |
| 49 | Mayer-Suess L et al., 2024 [51] | Narrative review of human and animal studies (non-systematic literature review) | Not applicable (review article) | Covers acute and chronic phases (risk before stroke and post-stroke evolution; not limited to one phase) | Summarizes multiple modalities (PSG, polygraphy, questionnaires, experimental recordings) from prior studies; no primary sleep study performed | Discusses CSA and Cheyne–Stokes breathing conceptually (e.g., CSA after brainstem stroke, Cheyne–Stokes breathing as primary CSA subtype), but no single operational index defined in this paper | Reports that CSA is an independent stroke risk factor, often improves with recovery but is associated with poorer prognosis; central events frequently seen after brainstem stroke and in Cheyne–Stokes breathing, but detailed pooled CAI/AHI data not primary focus | Not reported | Level 5 |
| 50 | Cai H et al., 2021 [52] | Narrative review on management (non-systematic; includes tabulated RCTs and cohort data) | Not applicable (review article) | Discusses all phases (acute and chronic post-stroke as well as pre-stroke risk) | Summarizes prior PSG-based and polygraphy-based trials (especially CPAP and other interventions); no new sleep recordings | CSA and Cheyne–Stokes breathing discussed as central apnea syndromes; mentions apnea–hypopnea index and central apnea index conceptually, but no new operational definition introduced | Describes CSA as having lower prevalence than OSA but common in cardiac/cerebrovascular disease; notes that CSA is an independent risk factor and negatively correlated with prognosis; mentions that CPAP/BiPAP may not optimally control CSA and that ASV or mechanical ventilation may be more effective in some post-stroke CSA phenotypes | Not reported | Level 5 |
| 51 | Parra O et al., 2000 [53] | Prospective cohort with repeated measures (acute and 3‑month follow-up) | 161 (acute phase); 86 re-studied at 3 months | Acute (48–72 h after admission) and stable at 3 months (chronic/subacute) | Unattended portable respiratory recording (respiratory polygraphy) validated against PSG | Central apnea index (CAI); Cheyne–Stokes breathing (CSB) defined as periodic breathing with central apnea/hypopnea in crescendodecrescendo pattern |
Acute: CAI 5.6 |
High prevalence of SRBD (71.4% with AHI |
Level 2 |
| 52 | Huhtakangas JK et al., 2020 [54] | Prospective observational single-center study | 204 ischemic stroke patients (final analyses) | Acute ischemic stroke, sleep study within 48 h after onset of stroke symptoms | Nocturnal unattended portable 3‑channel cardiorespiratory polygraphy (type 4 device, ApneaLinkPlus) | Central apnea index (CAI); central sleep apnea (CSA) defined as |
Automatically analyzed CAI 0.57 |
Manual scoring identified CSA ( |
Level 2 |
| 53 | Schütz SG et al., 2022 [55] | Population-based observational cohort with repeated cross-sectional sleep studies over time | 1215 stroke participants with home sleep apnea testing; 2811 with Berlin Questionnaire | Post-ischemic stroke (tested within 30–45 days; early subacute phase) | Home sleep apnea test with ApneaLink Plus (nasal pressure, oximetry, respiratory effort; manually reviewed polygraphy) | Central apnea index reported; central sleep apnea defined via central apnea index within REI, but no explicit syndrome threshold (used REI |
Median central apnea index 0 (IQR 0–2) events/h; SDB defined as REI |
Prevalence and severity of SDB after ischemic stroke increased over 2010–2019 (SDB from 61% to 76%; REI +0.56 events/h per year); central sleep apnea remained uncommon, indicating trends driven mainly by obstructive events rather than CSA/CSB | Level 2 |
| 54 | Brunner H, 2008 [56] | Preliminary open-label trial (case series with pre–post comparison; non-randomized, uncontrolled) | 10 stroke inpatients with sleep apnea (9 male, 1 female) | Subacute/chronic stroke: mean duration of illness before first PSG 52.6 |
Full overnight polysomnography (2200–0600) | Respiratory disturbance index (RDI) includes obstructive, central and mixed apneas plus hypopneas; central apnea index and mixed apnea index (RDI central, RDI mixed) reported, but no explicit CSA/CSB syndrome definition beyond indices | Baseline central apneas 12.4 |
Mirtazapine improved sleep efficiency and reduced RDI by |
Level 4 |
| 55 | Huhtakangas JK et al., 2018 [57] | Prospective cohort with 6‑month follow-up (thrombolysis vs no thrombolysis groups) | 204 ischemic stroke patients at baseline (110 with thrombolysis, 94 without); 177 with follow-up sleep study (98 thrombolysis, 79 non-thrombolysis) | Acute ischemic stroke at baseline (sleep study during initial hospitalization); 6‑month post‑stroke follow-up (chronic phase) | Unattended 3‑channel type 4 cardiorespiratory polygraphy (ApneaLink Plus) both at baseline and 6 months | Central apnea index (CAI); obstructive apnea index; mixed apnea index; sleep apnea defined by REI |
Baseline central apnea index 3.6 |
Sleep apnea prevalence remained very high at 6 months (92.7%); obstructive apneas declined while central apneas increased in both groups; in the non-thrombolysis group, risk of new sleep apnea diagnosis at 6 months was 6.1‑fold higher vs thrombolysis; thrombolysis and CPAP together predicted decline in REI, and thrombolysis was independently associated with lower incidence of new post‑stroke sleep apnea; central events increased despite stable high overall prevalence, highlighting evolving pattern from obstructive to more central events over time | Level 2 |
CSA, central sleep apnea; CPB, central periodic breathing; CSR,
Cheyne–Stokes respiration; SDB, sleepdisordered breathing; OSA, obstructive
sleep apnea; AHI, apnea–hypopnea index; CAI, central apnea index; cAHI, central
apnea–hypopnea index; PSG, polysomnography; HSAT, home sleep apnea test; TIA,
transient ischemic attack; LVEF, left ventricular ejection fraction; NIHSS,
National Institutes of Health Stroke Scale; mRS, modified Rankin Scale; BMI, body
mass index; TOAST, Trial of Org 10172 in Acute Stroke Treatment; CPBS, central periodic
breathing during sleep; PLMS, Periodic limb movements during sleep; RLS, restless leg
syndrome; OCEBM, the Oxford Centre for Evidence-Based Medicine, Levels of Evidence framework;
Most CSA data came from the acute or early subacute phase. Recordings within 24
hours to 10 days after stroke onset were reported in several cohorts using
polysomnography (PSG) or cardiorespiratory monitoring [5, 6, 7, 8, 9, 11, 13, 14, 15]. Subacute
or early rehabilitation phase CSA was described around 40–44 days after stroke
in a rehabilitation unit cohort [10], and within approximately one week in
another full‑night PSG study [16]. Chronic post‑stroke CSA or coexisting central
sleep apnea was assessed
Definitions and diagnostic modalities for CSA varied substantially between
studies. Many cohorts used full‑night attended PSG, including
EEG and standard respiratory channels, to identify central versus obstructive
events by the absence of thoraco‑abdominal effort [10, 12, 13, 16, 23, 44]. Central
sleep apnea was commonly defined as CSA when
CSR and central periodic breathing during sleep
(CPBS) were usually defined by a crescendo–decrescendo pattern of tidal volume
and central apneas/hypopneas. Kim et al. [11] defined CSR as
Several case reports and small series documented CSA conversion or
REM‑predominant CSA after stroke using PSG or portable monitoring. De Paolis
et al. [26] reported an increase in central apnea index from 3 to 56
events per hour three days after a cardioembolic ischemic stroke, with total AHI
70 events per hour. Qu et al. [22] reported REM‑predominant CSA after
medullary infarction with a baseline central AHI of 70.1 events per hour. Older
acute ischemic stroke series assessed CSR using bedside respiratory motion and
pulse oximetry without EEG or detailed CAI; Nachtmann et al. [5] defined
CSR as periodic modulation of respiratory amplitude
In several reviews [19, 20, 30, 31], CSA was conceptually defined as central
apneas with absent respiratory effort and often as
In acute ischemic stroke cohorts, the proportion of patients with CSR ranged from approximately 19% to more than 50% when defined by pattern rather than CAI alone. In an acute ischemic stroke cohort of 182 patients assessed with overnight sleep apnea testing, CSR was present in 35 patients (19.1%) [11]. In a 156‑patient acute stroke cohort monitored within 24 hours of onset, CPB was present in 33 of 138 patients with usable breathing recordings (24%) when defined as central crescendo–decrescendo periodic breathing occupying a quantifiable fraction of recording time [7]. In a 32‑patient acute ischemic stroke series with bedside respiratory monitoring, CSR was detected in 17 of 32 patients (53%) [5].
When CSA was defined by cAHI or CAI thresholds, prevalence estimates tended to
be lower. In a rehabilitation cohort of 93 stroke patients, CSA (central AHI
Central indices also showed broad ranges. In Siccoli et al. [9], the
central apnea index in 74 acute first‑ever ischemic stroke patients averaged 7
In lesion‑specific cohorts, central indices were often high. In 28 patients with
unilateral lateral medullary infarction, median acute AHI was 16.5 (interquartile
range 5.5–43.3), cAHI 11.0 (3.3–29.1), and CAI 8.3 (2.2–23.8) events per hour;
CSA alone was present in 43% and mixed patterns in additional patients [13]. In
Riglietti et al. [15], dominant CSA (
Case‑level CSA severity was very high in some reports. In two fatal CSA cases with medullary lesions, 38 and 35 central apneas per hour were documented [21], and REM‑predominant CSA after bulbar infarction showed central AHI 70.1 events per hour [22]. In a case of CSA conversion after stroke, central apnea index increased from 3 to 56 events per hour three days after a cardioembolic ischemic stroke, with total AHI 70 events per hour [26].
One meta‑analysis that included mixed stroke types reported CSA prevalence
10.0% (95% confidence interval 6.5–14.9%) among stroke patients when CSA was
defined as
Cardiac comorbidities were frequently evaluated. In Nopmaneejumruslers
et al. [10], CSA (central AHI
In multivariable logistic regression, Kim et al. [11] found that
previous modified Rankin Scale (mRS) score, bilateral hemispheric lesions,
left‑atrial volume index (per 10 mL/m2) and LVEF
Rowat et al. [7] reported that CPB presence was associated with more severe strokes (higher National Institutes of Health Stroke Scale, NIHSS), congestive heart failure, dysphagia, and reduced consciousness, while severity of prior cerebrovascular disease was not associated with CPB. Siccoli et al. [9] found that more severe CPBS was associated with older age, higher stroke severity, electrocardiographic abnormalities, and lower LVEF.
Age, sex and body mass index (BMI) were recurrent correlates of sleep‑disordered
breathing overall, although not always specifically of CSA. In the chronic
Baillieul cohort [44], moderate–severe sleep‑disordered breathing (SDB),
including coexisting or central sleep apnea defined by cAHI/AHI ratios, was
associated with male sex, obesity, age
Other vascular risk factors showed inconsistent relationships with CSA across studies. In Kim et al. [11], hypertension was more frequent in the CSA group in univariate analysis (71.4% vs 55.8%) but was not independently associated with CSA, and smoking was less frequent in the CSA group but did not remain significant after adjustment. In Nopmaneejumruslers et al. [10] and some other cohorts, stroke type and location were not significantly related to CSA, whereas cardiac function parameters were. Some physiological cohorts described CSA in relation to autonomic measures. Riglietti et al. [15] reported that CSA and mixed CSA/OSA patterns in acute stroke were associated with specific autonomic profiles (e.g., higher baroreflex gain and autonomic nervous system indexes) compared with obstructive patterns, but numerical autonomic values were study‑specific and not directly comparable with other cohorts. In an asymptomatic carotid stenosis cohort (not post‑stroke), CSA prevalence of 39% among patients with extracranial internal carotid artery stenosis was linked to severe stenosis and autonomic imbalance [27], but this population was not included in the ischemic stroke clinical outcome analyses.
In large acute hemispheric and mixed stroke cohorts, some studies did not find strong associations between CSA and specific vascular territories, while others highlighted bilateral or infratentorial involvement. In the study of Kim et al. [11], CSA presence was not significantly associated with vascular territory, supra‑ versus infratentorial location, or laterality when considered separately; however, bilateral hemispheric lesions were more frequent in the CSA group and remained independently associated with CSA in multivariable analysis. In Nachtmann et al. [5], CSA was present in 59% of supratentorial and 40% of infratentorial ischemic strokes, and the authors reported no clear dependence of CSA occurrence on infarct location when categorized simply as supratentorial versus infratentorial.
Martínez García et al. [6] reported that central apnea index and CSA were relatively uncommon (five patients with Cheyne–Stokes breathing) and that polysomnographic variables, including the central apnea index, did not vary significantly according to stroke site (left hemisphere, right hemisphere, vertebrobasilar territory, or undetermined) or lacunar versus non‑lacunar extent. Nocturnal‑onset strokes in that cohort, however, had higher total AHI and higher central apnea index than daytime strokes.
Some studies focused on specific lesion locations. Hermann et al. [8]
described three patients with CPBS among 31 acute first‑ever stroke patients;
lesions involved the left cingulate cortex, left insula, and right paramedian
thalamus on diffusion‑weighted MRI, and CPBS occupied 18–24% of total sleep
time, improving on follow‑up recording. Pavšič et al. [13]
investigated 28 patients with unilateral lateral medullary infarction and found
that CSA, defined by central AHI
Rowat et al. [7] reported that CPB was associated with large acute cerebral hemispheric lesions and severe mass effect on neuroimaging, though detailed volumetric data were not provided; CPB was not associated with the severity of prior cerebrovascular disease. Siccoli et al. [9] found that CPBS was more severe in extensive hemispheric strokes and less frequent in strokes involving the left insula and mesencephalon, based on imaging classifications. In the cohort of Baillieul et al. [44], coexisting or central sleep apnea among patients with moderate–severe SDB was associated with a higher frequency of cerebellar lesions, and moderate–severe SDB in general was associated with infratentorial lesions.
In the observational cohort of Kim et al. [11], a subgroup analysis limited to large‑artery atherosclerosis without cardiac disease showed that patients with CSA were older and more likely to have both supra‑ and infratentorial lesions, but in multivariable analysis only the previous mRS score remained significant in that subgroup. Several narrative reviews [30, 31, 40] discussed medullary, pontine, insular and thalamic involvement in relation to CSA, but did not contribute new, independent lesion–CSA datasets beyond the primary studies already described.
A substantial proportion of the 55 studies did not systematically relate CSA to detailed neuroimaging findings; in many of those studies, lesion location was either not reported in a form usable for CSA‑specific correlation or was described without stratifying respiratory patterns by location.
In Rowat et al. [7], CPB presence was independently associated with
death or dependency (modified Rankin Scale
In the SAS‑CARE 1 cohort [12], higher baseline AHI (including central and
obstructive events) was associated with poor functional outcome (mRS
In Mekky et al. [16], stroke patients had higher AHI, CSA index and desaturation index and lower minimal oxygen saturation compared with age‑matched controls; within the stroke group, lower minimal SpO2 at one week correlated with worse NIHSS at one month. The study did not report functional outcomes stratified solely by CSA status, and no mortality analysis was presented specific to CSA.
In Nopmaneejumruslers et al. [10], clinical outcomes such as mortality or long‑term disability by CSA status were not the primary focus; the study concentrated on CSA prevalence and its relationship with cardiac function and transcutaneous carbon dioxide tension (CSA‑specific outcomes not reported). In Pavšič et al. [13], outcomes of interest were changes in AHI and cAHI over time in unilateral lateral medullary infarction; functional or mortality endpoints stratified by CSA were not detailed (not reported).
Kim et al. [11] reported baseline NIHSS and premorbid mRS differences between CSR and non‑CSR groups but did not present separate long‑term functional outcome or mortality rates according to CSR status beyond the logistic regression models for CSR determinants (CSR‑specific prognostic data not reported). In Martínez García et al. [6] and Nachtmann et al. [5], respiratory patterns were described and comparisons with general population or control data were made, but CSA‑specific mortality or disability statistics were not reported.
Narrative reviews and meta‑analyses [19, 20, 31, 39, 40] commonly stated that CSA after stroke are associated with more severe neurological impairment or higher mortality, but did not provide new numerical outcome data for CSA‑only groups beyond the primary studies already summarized.
Therapeutic data were limited to small observational reports and case series; one retrospective series found that adaptive servoventilation reduced apnea–hypopnea index and improved symptoms in post-acute stroke patients with persistent CSA, while other reports described partial spontaneous resolution or treatment-related changes in central indices [18, 22, 26].
Overall, among the 55 studies included in this scoping review, a limited subset provided quantitative outcome measures that were explicitly stratified by CSA, CPB or CSR status in ischemic stroke; in many cohorts, outcomes were reported for sleep‑disordered breathing as a whole or were not separated by respiratory pattern, resulting in “not reported” for CSA‑specific functional status, complication rates or mortality in a considerable proportion of the evidence base.
Across the 55 studies, CSA appear as context‑dependent phenomena rather than a single, uniform syndrome after ischemic stroke. High CSA rates in acute, pattern‑based cohorts contrast with low CSA prevalence when strict central apnea index thresholds or home testing are used, showing that prevalence largely reflects how “central” breathing is defined and measured [5, 7, 10, 11, 55]. The consistent clustering of central patterns in patients with cardiac dysfunction, prior disability and more extensive or bilateral lesions suggests that CSA after stroke usually marks combined cardio‑cerebrovascular vulnerability rather than an isolated respiratory problem [7, 9, 10, 11, 44].
The variability in CSA prevalence and phenotype can be explained by the different ways stroke and comorbid disease alter ventilatory control. Unilateral lesions in insula, cingulate cortex, thalamus and medulla were sufficient to generate CPB or CSA in patients without severe heart disease, with partial resolution over weeks or months, supporting a direct neurogenic contribution from damage to central respiratory networks [8, 13, 21]. At the same time, several cohorts showed that central patterns concentrate in patients with reduced left ventricular ejection fraction, enlarged left atrium, lower nocturnal carbon dioxide and atrial fibrillation, indicating that circulation delay and high loop gain frequently interact with stroke‑related injury to produce CSA [10, 11]. Longitudinal data—central indices falling in some lesion‑focused series but rising in broader stroke cohorts—suggest that as the brain recovers and cardiac status evolves, the balance between obstructive and central events shifts, which accounts for apparently conflicting time‑course findings [8, 12, 13, 15, 57].
The pathophysiology of CSA in ischemic stroke appears multifactorial, involving disruption of central respiratory networks and interaction with cardiac dysfunction and ventilatory instability. From a clinical standpoint, identifying CSA may help risk-stratify stroke patients, but the evidence for specific management strategies remains limited and largely non-randomized.
These mechanisms help interpret why central patterns carry prognostic information in several studies. Because CSA tends to occur in patients with more severe neurological deficits and worse cardiac status, their presence identifies individuals who already have a high risk profile, which explains the observed associations with death or dependency rather than implying direct causality [7, 12, 23]. Early sleep testing captures transient but prognostically relevant central instabilities, yet feasibility constraints mean that the sickest patients are often not studied, so current data likely underestimate the burden of CSA in real‑world stroke [11, 58]. Case reports and small series showing conversion from obstructive to central patterns and response to bilevel or adaptive servo‑ventilation illustrate that management may need to adapt dynamically as central instability emerges, but also highlight that some central patterns resolve spontaneously, supporting careful, individualized decision‑making [18, 22, 26] (Fig. 2).
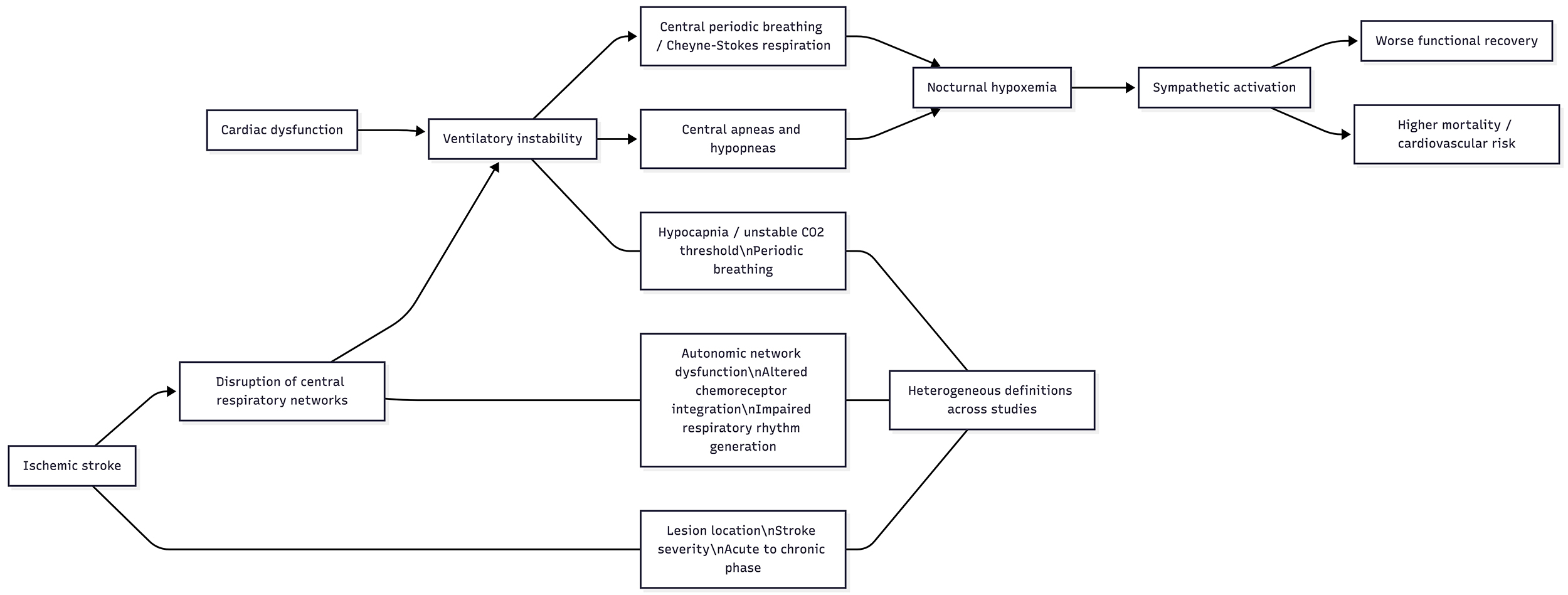 Fig. 2.
Fig. 2.
Conceptual framework of central sleep apnea after ischemic stroke. The figure summarizes the main pathways described in the literature, including disruption of central respiratory networks, altered chemoreceptive and autonomic control, ventilatory instability, and the interaction with cardiac dysfunction, which may lead to central apneas, periodic breathing, and adverse clinical outcomes.
The way the existing evidence is structured points directly to what is needed next. Harmonized, stroke‑specific definitions that integrate central indices and pattern descriptors would reduce artificial heterogeneity and make future studies comparable [9, 10, 11, 44, 55]. Prospective multicenter cohorts that include severe strokes and repeat standardized sleep studies from the acute phase into the chronic stage are required to disentangle transient neurogenic CSA from more persistent, heart‑failure–related phenotypes and to clarify how lesion topography, cardiac function and autonomic markers jointly shape central instability [8, 12, 13, 15, 57]. Finally, pragmatic interventional trials embedded in stroke services—comparing diagnostic strategies and treatment pathways for patients with prominent central patterns—are needed to test whether identifying and treating CSA after ischemic stroke can meaningfully change functional outcomes or vascular risk, rather than simply describe another marker of severity [7, 18, 22, 26].
The current evidence supports a prioritized research agenda. Future studies should first adopt standardized, stroke-specific definitions of CSA and related central breathing phenotypes. They should then incorporate longitudinal phenotyping across the acute-to-chronic stroke continuum, stratify results by stroke subtype and lesion location, and evaluate potential modifiers such as sex, age, and cardiac function. Finally, pragmatic interventional studies are needed to determine whether identification and treatment of CSA after ischemic stroke improve functional recovery and other clinical outcomes.
This scoping review has several limitations. It is based solely on the 55 available studies, which are heterogeneous in design, CSA definitions, sleep‑study methods, stroke phases and outcome reporting, and many cohorts exclude the most severe strokes or lack detailed CSA‑specific analyses, so selection and reporting biases cannot be excluded. These constraints limit the comparability of results and the strength of causal inferences regarding central sleep apnea after ischemic stroke.
Key knowledge gaps remain despite the 55 included studies. The absence of a
harmonized, stroke‑specific definition of central sleep apnea (CSA) and
Cheyne–Stokes respiration (CSR) means that current discrepancies in prevalence
and risk estimates may reflect methodology more than biology [59, 60, 61].
Longitudinal information is limited to a few cohorts and does not clearly
separate transient, stroke‑triggered central instability from more chronic,
heart‑failure–driven CSA phenotypes. Lesion–symptom relationships and ischemic
stroke subtypes are underexplored: small series suggest roles for insular,
thalamic, cerebellar and medullary lesions, but larger imaging‑based cohorts
stratified by lacunar, cardioembolic, atherothrombotic and other etiologies are
lacking. Virtually no study systematically examines sex differences or focuses on
very old patients (
Central sleep apnea and Cheyne–Stokes respiration after ischemic stroke emerge from the combined impact of focal brain lesions, cardiac dysfunction and timedependent changes in ventilatory control, clustering particularly in patients with bilateral or extensive lesions, reduced ejection fraction, atrial enlargement and higher premorbid disability. Existing studies suggest that these central patterns often signal a highrisk cardiocerebrovascular profile and may accompany poorer functional outcomes, but inconsistent definitions, heterogeneous methods, selective sampling and the very limited, smallscale experience with adaptive servoventilation or other targeted therapies—without any randomized trials—mean that their independent prognostic weight and treatability remain uncertain, underscoring the need for standardized criteria, broader longitudinal cohorts and robust intervention studies specifically evaluating servoventilation and related approaches in this population.
The datasets generated and analyzed during this scoping review are available from the corresponding author on reasonable request.
KU and AA conceived the review, defined the research questions, and supervised the project. IYM, OP, and KU conducted the literature search and study selection. M-JS-L designed and refined the search strategy and managed reference screening. MGP, OP, and KU extracted and curated the data. KU drafted the first version of the manuscript. IYM, M-JS-L, MGP, OP, and AA critically revised the manuscript for important intellectual content. All authors read and approved the final version of the manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
The authors thank the staff of the Sleep Disorders Unit and the Medical Library of Hospital Universitari Sagrat Cor for their administrative and technical support during the conduct of this review.
This research received no external funding.
The authors declare no conflicts of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/RN49726.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.