
 , Shengnan Zhang 1, Dan Li 1,2, Baoji Li 1, Zhouyao Hu 3,*
, Shengnan Zhang 1, Dan Li 1,2, Baoji Li 1, Zhouyao Hu 3,*
1 Department of Neurology, The Affiliated Hospital of Hangzhou Normal University, 311121 Hangzhou, Zhejiang, China
2 Translational Medicine Center, The Affiliated Hospital of Hangzhou Normal University, 311121 Hangzhou, Zhejiang, China
3 Department of Neurology, Hangzhou First People's Hospital Tonglu Campus (Tonglu First People's Hospital), 311500 Hangzhou, Zhejiang, China
Abstract
Spinocerebellar ataxia (SCA) is a rare group of hereditary degenerative disorders with major symptoms such as unsteady gait, dysarthria, and finger-nose instability. At present, the Berg Balance Scale (BBS) is a widely utilized balance assessment tool for SCA patients, exhibiting high reliability. The objective of this study was to ascertain whether the Semans Scale and the Balance Coordination Test can also be utilized for balance assessment in SCA patients.
A total of 32 patients with SCA who had been diagnosed according to previously reported molecular criteria were recruited between 2021 and 2022. In addition, all patients completed assessments for all three scales.
The results of the study demonstrated a moderate positive correlation between the BBS and both the Semans Scale and Balance Coordination Test scores (BBS versus Semans: r = 0.568, p < 0.001; BBS versus Balance Coordination Test: r = 0.625, p < 0.001). However, the Wilcoxon signed-rank test showed statistically significant differences between BBS and both Semans Scores (Z = –2.955, p = 0.003) and Balance Coordination Test scores (Z = –3.666, p < 0.001).
The Semans Scale and Balance Coordination Test reflect the balance function of SCA patients to a certain extent and can be used as valid complements to the BBS, providing additional information for clinical treatment and rehabilitation.
Keywords
- spinocerebellar ataxia
- Berg Balance Scale
- Semans Scale
- Balance Coordination Test
- ICARS
The background of the study is as follows: spinocerebellar ataxia (SCA) is a rare group of inherited neurological disorders characterized by ataxic symptoms [1]. These disorders are typically caused by the aberrant amplification of CAG repeats in genes, which results in the aberrant aggregation of proteins and degenerative changes in nerve cells [2]. The pathogenesis of SCA remains incompletely understood. However, studies have demonstrated a strong correlation between SCA and gene mutations and aberrant protein aggregation. The principal clinical manifestations of SCA include unsteady gait, dysarthria, oculomotor disorders, and ataxia of the limbs [3]. These symptoms have a profound impact on patients’ quality of life and ability to perform daily activities [4].
Despite the absence of efficacious pharmacological treatments for SCA, prompt diagnosis and effective symptom management are crucial in enhancing patients’ quality of life. In clinical practice, the assessment of ataxia and disease progression in patients with SCA is a crucial foundation for the development of treatment and rehabilitation programs. The most common assessment instruments include the Scale for the Assessment and Rating of Ataxia (SARA), the International Cooperative Ataxia Rating Scale (ICARS), and the Berg Balance Scale (BBS) [5, 6, 7, 8]. Among these, the BBS is a standardized scale for assessing balance function that is widely used in the assessment of balance function in SCA patients due to its high reliability and validity [9]. ICARS was selected because it provides a comprehensive assessment of multiple domains of ataxia, which was relevant to the objectives of this study.
The Semans Balance Scale and Balance Coordination Scale are also commonly utilized balance assessment tools that are primarily employed to evaluate the balance abilities of patients with stroke and pediatric cerebral palsy [10]. The Semans Balance Scale is an observational assessment method that evaluates the subject’s ability to maintain balance in three positions: standing, kneeling, and two-knee kneeling [11]. Low scores indicate poor balance. Unlike the BBS, the SBS provides a more granular assessment of static postural control and stability during lower-level developmental positions, which are often compromised in SCA patients before they lose complete standing balance. The Balance Coordination Test is used to assess the subject’s balance coordination ability in various tasks and postures. Nevertheless, the utilization of these two scales in SCA patients has not been sufficiently validated, and the extent to which they can be relied on to assess balance function in SCA patients remains uncertain. While the BBS measures “whether” a task is completed, the Balance Coordination Test (BCT) places more emphasis on the smoothness and coordination of postural adjustments during limb movements.
Given these considerations, the objective of this study is to examine the feasibility of utilizing the Semans Balance Scale and Balance Coordination Test in SCA patients and assess their potential as instruments for evaluating balance function in SCA patients. The present study will analyze the correlation and variability of the ICARS, BBS, Semans Balance Scale, and Balance Coordination Test in assessing balance function in patients with SCA. To this end, these tests will be evaluated in 32 patients who have been genetically diagnosed with SCA. Furthermore, the applicability of the Semans Balance Scale and the Balance Coordination Test in patients with SCA will be validated.
A total of 32 patients with SCA who had been diagnosed according to previously reported molecular criteria were recruited from the Department of Neurology at the Affiliated Hospital of Hangzhou Normal University between 2021 and 2022. All participants have signed informed consent forms. To be included in the study, participants had to meet the following criteria: they had to have a confirmed diagnosis of SCA, and they could not have had any unspecified genotypes or disseminated phenotypes. Additionally, they had to have been able to cooperate during the research process and had been assessed using the scales. In our study, the diagnosis of spinocerebellar ataxia (SCA) was confirmed by genetic testing. The included patients were genetically confirmed cases of SCA, including SCA1, SCA2, and SCA3.
The ICARS, BBS, Semans, and Balance Coordination Test were evaluated by a single assessor. The BBS was primarily designed to assess balance in patients with SCA; However, additional balance scales are also required to supplement or serve as references for BBS. The BBS was a measure of multitasking ability comprising 14 items requiring the participant to balance during a variety of tasks and in different positions, with the level of difficulty varying across items. Each item was assigned a score on a scale from 0 to 4, with a maximum score of 56. A lower score indicated an elevated risk of falling [12]. The Semans test was primarily utilized to assess a patient’s capacity to maintain equilibrium [11]. The test comprised eight items, each requiring the participant to balance in a different position. These items were grouped into a total of eight levels (0–7 scores). The BCT is a 17-item assessment designed to evaluate balance capacity and motor coordination. Each item is scored on a 0–4 scale, yielding a maximum possible score of 68. The higher the score, the better the balance function.
All data were analyzed using IBM SPSS version 26.0 (IBM Corp., Armonk, NY, USA).
Continuous data were assessed for normality using the Shapiro-Wilk test (Supplementary Table 1).
Descriptive statistics (mean
Table 1 presents the clinical data of 32 patients with SCA. The cohort comprised
16 males and 16 females, with a mean age of 39.23
| Variables | mean |
| Numbers | 32 |
| Sex (Male/Female) | 16/16 |
| AAO (Age at onset) | 30.72 |
| Age, years | 39.23 |
| Disease Duration, years | 8.22 |
| ICARS | 27.47 |
| Posture and Gait Disturbance | 12.38 |
| Kinetic Function | 11.19 |
| Speech Disorder | 2.41 |
| Oculomotor Disorders | 1.78 |
| BBS | 42.53 |
| Semans Balance | 5.37 |
| Balance Coordination Test | 39.56 |
SCA, spinocerebellar ataxia.
In the present study, we employed the BBS, Balance Coordination Test, and Semans
Scale to assess the balance abilities of SCA patients. The results of the
correlation analysis demonstrated significant correlations between the scale
scores and key clinical variables, as detailed in Table 2. Specifically, the BBS,
Balance Coordination Test, and Semans Scale scores were all found to be
significantly negatively correlated with ICARS scores (r = –0.863, –0.574,
–0.574, p
| Variables | BBS | BCT | SB |
| Age | –0.108 | 0.030 | –0.287 |
| Disease Duration | –0.322 | –0.135 | –0.254 |
| ICARS | –0.863** | –0.574a** | –0.574** |
| Posture and Gait. Disturbance | –0.947** | –0.613** | –0.650** |
| Kinetic Function | –0.660** | –0.517a** | –0.496** |
| Speech Disorder | –0.574** | –0.544** | –0.502** |
| Oculomotor Disorders | –0.289 | –0.139 | –0.067 |
SB, Semans Balance; BCT, Balance Coordination Test; a, Pearson’s test;
**p
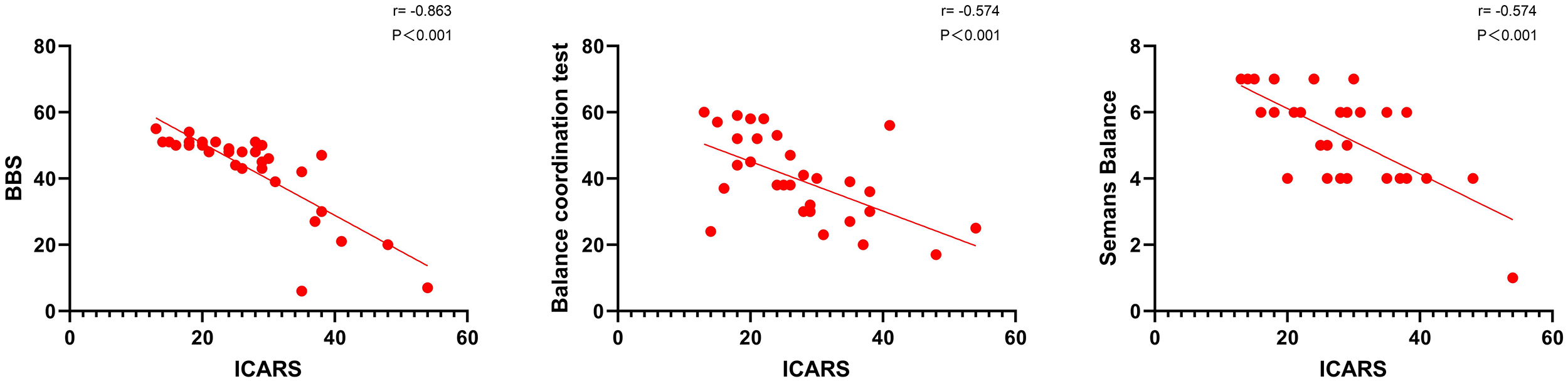
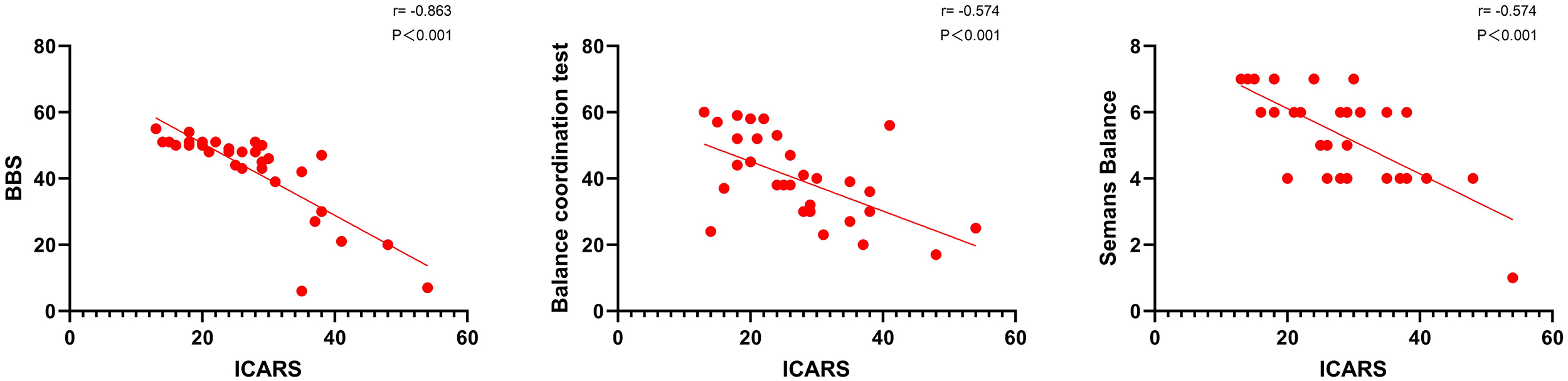 Fig. 1.
Fig. 1.
Correlation analysis of each scale and ICARS. The BBS, Balance Coordination Test, and Semans Scale scores were all found to be significantly negatively correlated with ICARS scores in Spearman’s correlation analysis. BBS, Berg Balance Scale; ICARS, International Cooperative Ataxia Rating Scale.
Reliability analysis showed excellent internal consistency for both instruments,
with a Cronbach’s alpha of 0.946 for the BBS and 0.946 for the BCT. Regarding
scale variability, the BBS scores showed a CV of 30.24%, while the BCT scores
showed a CV of 32%. The high Cronbach’s alpha (0.946) further confirms the low
measurement error of both instruments. Spearman’s correlation analysis revealed a
moderate positive correlation between the BBS and both Semans Scale and Balance
Coordination Test scores (BBS versus Semans Scale: r = 0.568, p
| Group | Median (P25, P75) | Wilcoxon signed-rank test | Spearman’s correlation test | ||
| Z | p | r | p | ||
| BBS | 86% (76%, 90%) | –3.666 | 0.625 | ||
| BCT | 56% (44%, 76%) | ||||
| BBS | 86% (76%, 90%) | –2.955 | 0.003** | 0.568 | |
| SB | 75% (50%, 85%) | ||||
| BCT | 56% (44%, 76%) | –2.303 | 0.021* | 0.372 | 0.036* |
| SB | 75% (50%, 85%) | ||||
*p
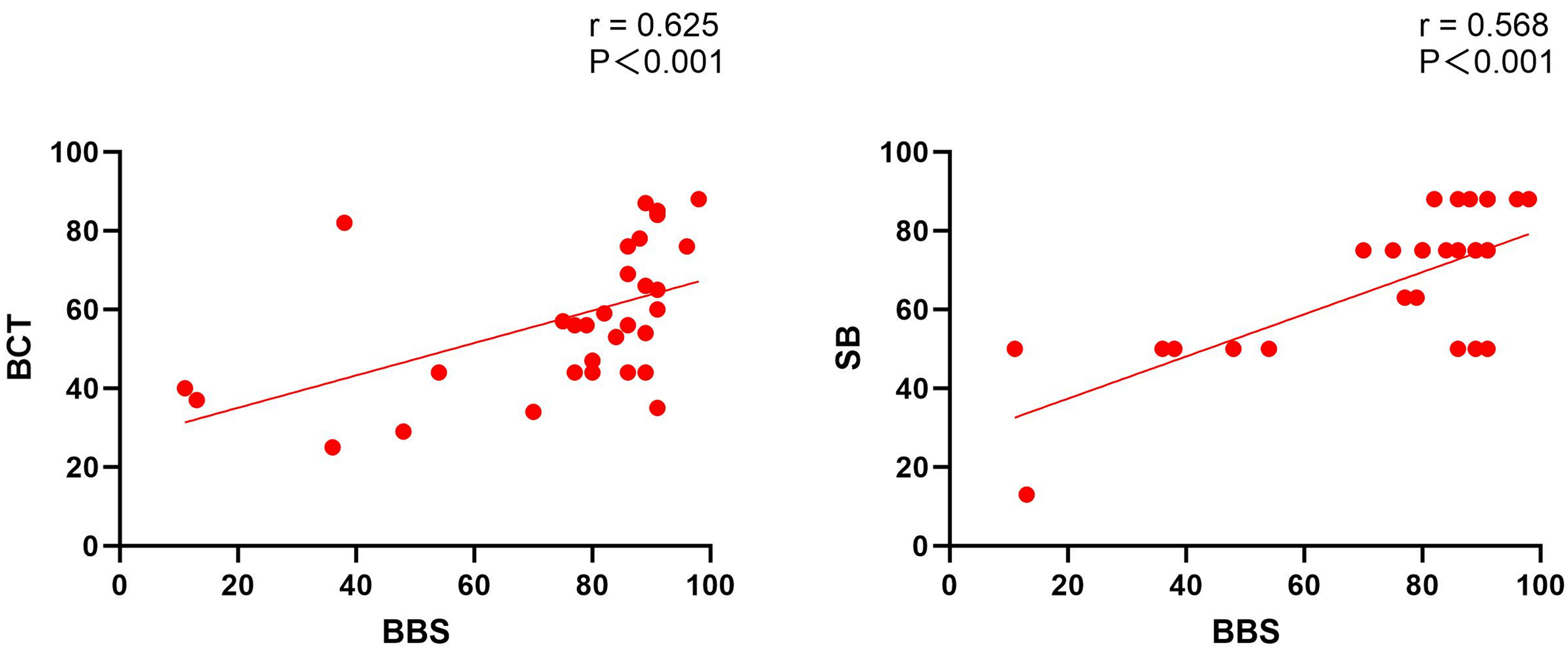
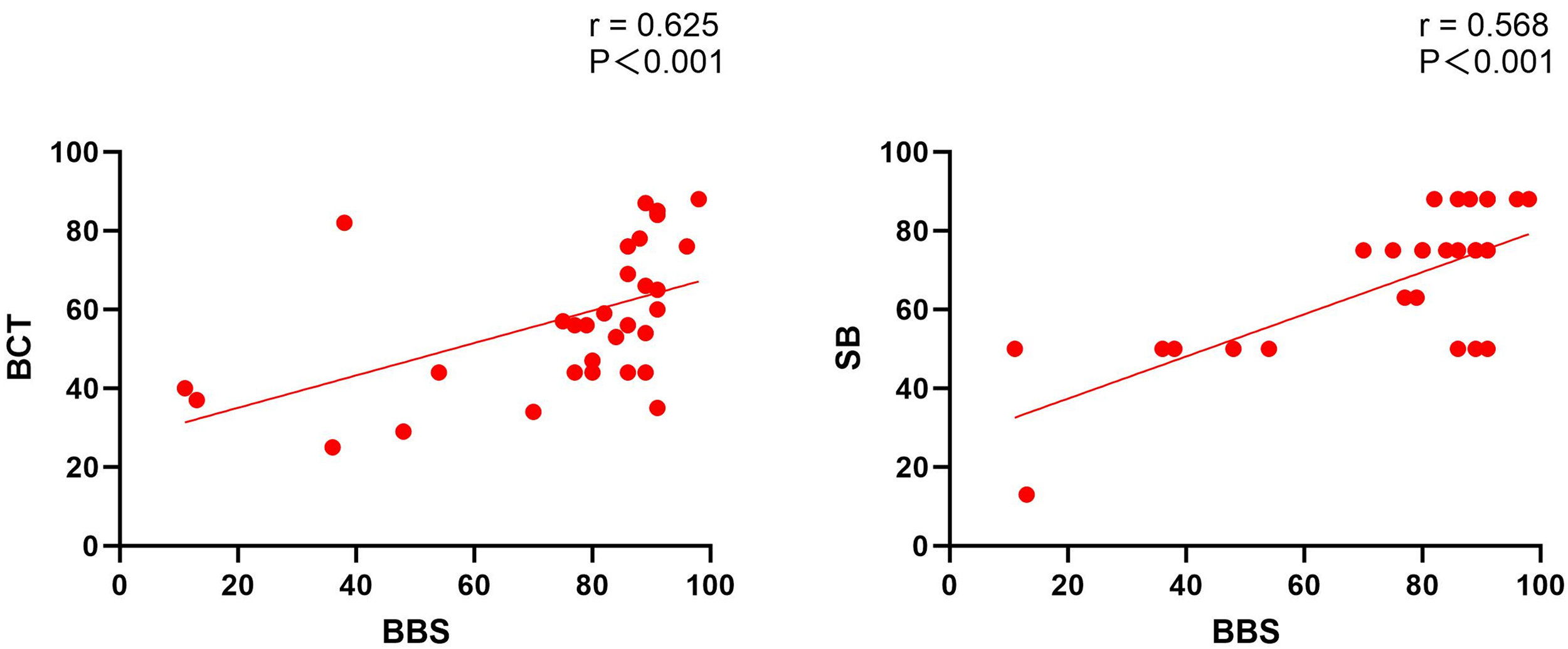 Fig. 2.
Fig. 2.
Correlation analysis of other scales and BBS. Spearman’s correlation analysis revealed a significant positive correlation between the BBS and both Semans Scale and Balance Coordination Test scores.
Furthermore, the Wilcoxon signed-rank test results indicated that the
differences among the three scales reached statistical significance levels (BBS
vs BCT: Z = –3.666, p
Furthermore, Cronbach’s alpha coefficients were calculated for the Balance Coordination Test scale. The results demonstrated that the Cronbach’s alpha coefficient was 0.946, indicating that the Balance Coordination Test scale exhibited a notably high level of internal consistency reliability. This indicates that the 17 sub-items of the Balance Coordination Test scale exhibited high consistency in scores when measuring the same underlying construct, namely the relevant symptom or function in patients with SCA.
The results of the study indicate that while the Semans Scale and Balance Coordination Test have a degree of agreement with the BBS in terms of assessing balance in patients with SCA, they differ significantly in terms of the specific content and sensitivity of the assessment. The BBS scale is an effective tool for assessing balance dysfunction in SCA patients and provides valuable insights into the efficacy of disease treatment in this population. In this study, we evaluated the BBS, Semans Scale, and Balance Coordination Test for use with patients with SCA [10, 11]. We assessed the results using Spearman’s rank correlation and a Wilcoxon signed-rank test to determine the correlations between and differences in scores for these scales when assessing balance in SCA patients. The results demonstrated that the BBS, Balance Coordination Test, and Semans Scale exhibited significant positive correlations in terms of assessing balance ability in SCA patients. However, notable discrepancies were observed in the specific content and sensitivity of the assessments.
Spearman’s correlation analysis demonstrated significant positive correlations between BBS scores and both Balance Coordination Test and Semans Scale scores, suggesting that the Balance Coordination Test and Semans Scale reflect overlapping aspects of balance function. The BBS scale is widely utilized in patients with SCA and is considered highly reliable [15]. The BBS scale exhibited significant correlations with both the Balance Coordination Test and the Semans Scale, providing supportive evidence that these instruments are relevant to assessment of balance function in patients with SCA. Because the three scales have different scoring ranges, direct comparison of their raw scores is not statistically appropriate. Therefore, in the revised analysis, all scores were converted to percentage scores before pairwise comparison. After conversion to percentage scores, the Wilcoxon signed-rank test showed significant differences between each pair of scales, indicating that although the three instruments are correlated, their standardized score distributions are not identical and that they differ in assessment focus and sensitivity. The significant differences involving the Semans Scale may reflect its distinctive item composition and its sensitivity to certain specific aspects of balance functions. The Semans Scale was originally developed for the balance assessment in patients with stroke and pediatric cerebral palsy [11, 16]. Some of its items may not fully correspond to the specific balance deficits by SCA patients, which partly explain the observed differences in standardized scores compared with the BBS and Balance Coordination Test. Nevertheless, it’s significant in correlations with both the BBS and Balance Coordination Test, indicating that it still has some validity in assessing overall balance functioning. The Balance Coordination Test showed a high correlation with the BBS, suggesting that BCT has good consistency with the BBS in evaluation of balance functioning. However, after percentage-score transformation, the Wilcoxon signed-rank test also showed a significant difference between the Balance Coordination Test and the BBS, indicating that the two scales are related but not directly interchangeable. Overall, the Balance Coordination Test may serve as a supplementary instrument for evaluating balance function in SCA patients, particularly when a more detailed assessment of balance coordination is needed.
Furthermore, the Cronbach’s alpha coefficient for the Balance Coordination Test scale was 0.946, indicating that the internal consistency reliability of the Balance Coordination Test scale is exceptionally high. A high level of internal consistency reliability is indicated by the fact that the 17 sub-items of the Balance Coordination Test scale yield highly consistent scores when measuring the same underlying construct (i.e., the relevant symptom or function in SCA patients). This provides further evidence to support the reliability and validity of the Balance Coordination Test scale in clinical assessment. A high level of reliability indicates that the scale is stable and consistent across the SCA patient population, which is a valuable attribute for clinical assessment and research purposes. The high internal consistency reliability of the study results enhances the credibility of the findings and supports the use of the Balance Coordination Test scale for further clinical diagnosis and research. Unfortunately, there was no significant correlation between disease duration and various balance scales. Generally, as the disease course progresses, patients’ conditions tend to worsen and balance function gradually deteriorates. However, our study did not observe any correlation between these two factors. We speculate that this may be attributed to insufficient sample size.
The findings of this study indicate that a comprehensive assessment employing multiple scales may prove more beneficial in clinical practice, facilitating a comprehensive understanding of the state of balance function in SCA patients. The BBS, as a standardized scale, can provide a reliable assessment of balance ability, while the Balance Coordination Test and Semans Scale can be utilized as complementary tools to provide further insight into balance ability. This multi-scale assessment method can assist clinicians in developing effective individualized rehabilitation plans and improving treatment outcomes. Further studies are required to validate the applicability and validity of the Balance Coordination Test and Semans Scale in various patient groups, particularly in relation to various types of SCA patients, and to explore their potential value in assessing specific balance dysfunctions. Furthermore, additional research is required to ascertain the sensitivity and specificity of the scales, thus ensuring that the assessment tools can accurately reflect changes in patients’ balance abilities and provide accurate data to support clinical decision-making.
With the advancement of research, various instruments have emerged that can objectively assess the balance function of SCAs. For instance, the FOOTSCAN platform and Wearable IMUs, which are equipped with multiple sensors, can measure various data during standing or walking, such as Total Travel Way, Confidence Ellipse Area, Gait Variability, Toe-out/Toe-off Angle, etc. [17, 18]. These objective measurement data not only help differentiate between patients and healthy individuals but also hold significance for early disease identification. Future investigations should integrate these objective assessment tools alongside traditional subjective scales; such a multi-faceted approach will not only mitigate the limitations of subjective assessment data but also significantly bolster the empirical rigor and credibility of the study outcomes.
First, the number of enrolled patients was relatively small. Due to the rarity of the disease and the high cost of genetic testing, the number of confirmed SCA patients was limited, resulting in insufficient sample size, which had a certain impact on the research findings. Additionally, healthy control subjects were not included in this study to provide normative reference data, making direct comparisons impossible. Secondly, the scale assessment did not follow the random test, which may lead to fatigue in the later scale assessment and affect the results.
The BBS exhibited a significant correlation with Balance Coordination Test and Semans Scale in SCA patients, despite differences in the content and sensitivity of the assessment tools employed. The Balance Coordination Test and Semans Scale are effective complementary tools for use in the assessment of balance in SCA patients. Further research is required to validate these scales.
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to containing information that could compromise research participant privacy.
MY, SNZ, DL, BJL and ZYH initiated the project. MY, SNZ, DL and BJL collected and analyzed the data. MY wrote the manuscript. ZYH and MY commented and revised on the manuscript. DL and ZYH supervised all aspects of the project. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was approved by the Ethics Committee for Human Research in the Affiliated Hospital of Hangzhou Normal University (Ethics Committee Number: 2021-(E2)-HS-078). Informed consents were obtained from the participants prior to enrollment in the study. The study was carried out in accordance with the guidelines of the Declaration of Helsinki.
We gratefully acknowledge all participants for their help and willingness to participate in this study.
This study was supported by the Medical and Health Science and Technology Project of Zhejiang Province to Mei Ye (2022KY261).
The authors declare no conflicts of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/RN48265.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.