

 , Najah R Hadi 2,*
, Najah R Hadi 2,* , Abdulla Shehab 3, Galal Elkilany 4
, Abdulla Shehab 3, Galal Elkilany 41 Department of Medicine, Halbeg Hospital and Research Institute, 244001 Moradabad, India
2 Faculty of Medicine, University of Kufa, 54001 Najaf, Iraq
3 Department of Cardiovascular Medicine, UAE University, 19666 Al-Ain, UAE
4 Medical Departments, Sentara Northern Virginia Medical Center, Woodbridge, VA 22191, USA
Despite increased availability of drugs for treatment of heart failure (HF), the
Four Pillar Directed Therapy (FPDT) does not provide absolute protection in its
treatment [1, 2, 3, 4, 5]. Interestingly, contemporary therapy of HF emphasizes early
initiation and rapid up-titration of four classes of basic drugs, including
angiotensin converting enzyme (ACE)/receptor blockers or angiotensin
receptor-neprilysin inhibitors (ARNI), sodium-glucose cotransporter 2 (SGLT2)
inhibitors,
In issue 4 of this journal in 2026, a review emphasizes that GDMT, along with vericiguat, may significantly improve survival and quality of life in patients with both reduced and preserved ejection fraction (HFpEF) [8]. Despite advances in the management of HF, it remains a leading cause of morbidity and mortality, partly due to the suboptimal implementation of GDMT [2, 3, 4, 5]. Poor adherence to pharmacological therapy may result from therapeutic inertia and concerns about hypotension during treatment [1, 2, 3]. In addition, it is also possible that other mechanisms of heart failure are not fully addressed by GDMT. Approximately half of all cases of HF are attributed to decreased left ventricular systolic function, known as HFrEF. However, mortality rates are similar between HFrEF and HFpEF.
Vericiguat, formerly indicated solely for patients with low ejection fraction,
is now recommended for all patients with HF by most of the agencies, including
the International College of Cardiology [3, 4, 5, 6, 7]. Efficacy in HFmrEF supports this
medication’s promotion to class IIB recommended status for this population. These
medications include ACE inhibitors, ARBs or ARNIs, beta-blockers, SGLT2
inhibitors, and mineralo-corticoid receptor antagonists (MRAs) [5]. In the recent
VICTOR trial, performed at 482 centers across 36 countries, among patients (n =
6105, median age 68.0 years, 4665 (76.4%) were males), with HFrEF
(
No significant differences in all-cause mortality were observed between the intervention group and control groups (377 [12.3%] vs 440 [14.4%]; HR 0.84) [6]. Adverse effects were also similar between groups. Thus, the VICTOR trial’s primary outcome was neutral; it did not show a benefit for the composite endpoint of CV death or HF hospitalization.
Recently, a pooled analysis was conducted of the VICTORIA and VICTOR trials to
provide compelling data that vericiguat reduces mortality in HFrEF, indicating
that it should be considered a foundational fifth pillar of GDMT. The VICTOR
trial was neutral for the primary endpoint, but its nominally significant
mortality benefit made it consistent with the signal observed in the pooled
analysis [6]. The individual participant data analysis of the VICTORIA (n = 5050)
and VICTOR (n = 6105) trials (total n = 11,155) showed that vericiguat
consistently decreases the risk of cardiovascular death or hospitalization for HF
in patients with HFrEF across a wide spectrum of risk factors [7]. The
treatment benefit was consistent regardless of the risk profile, with notable
efficacy seen in patients with NT-proBNP
Since diuretics are insufficient to control volume overload in many patients with HF, this emphasizes the need for developing novel medicinal approaches to treating HF, which may be the Fifth Pillar of HF therapy. Potential therapies for HFrEF have recently been examined, including sGC agonists and other members of a novel family of medicines that target various portions of the cyclic guanosine monophosphate (cGMP) pathway [9]. In a study with a mean follow-up of 10.8 months, vericiguat substantially decreased the risk of the main composite endpoint, which was composed of cardiovascular mortality and the first hospitalization for HF (35.5% vs 38.5%, p = 0.02) [10]. These findings revealed that the decline in HF hospitalizations was the main contributor to the difference, although deaths from cardiovascular causes were almost the same in both groups. It is of interest that although this agent did not reduce the composite endpoint in one trial [6], it is still a candidate for a pillar, possibly because it targets a different pathway and provides a mortality benefit with safety when the results of the trial are combined with another more recent trial [7].
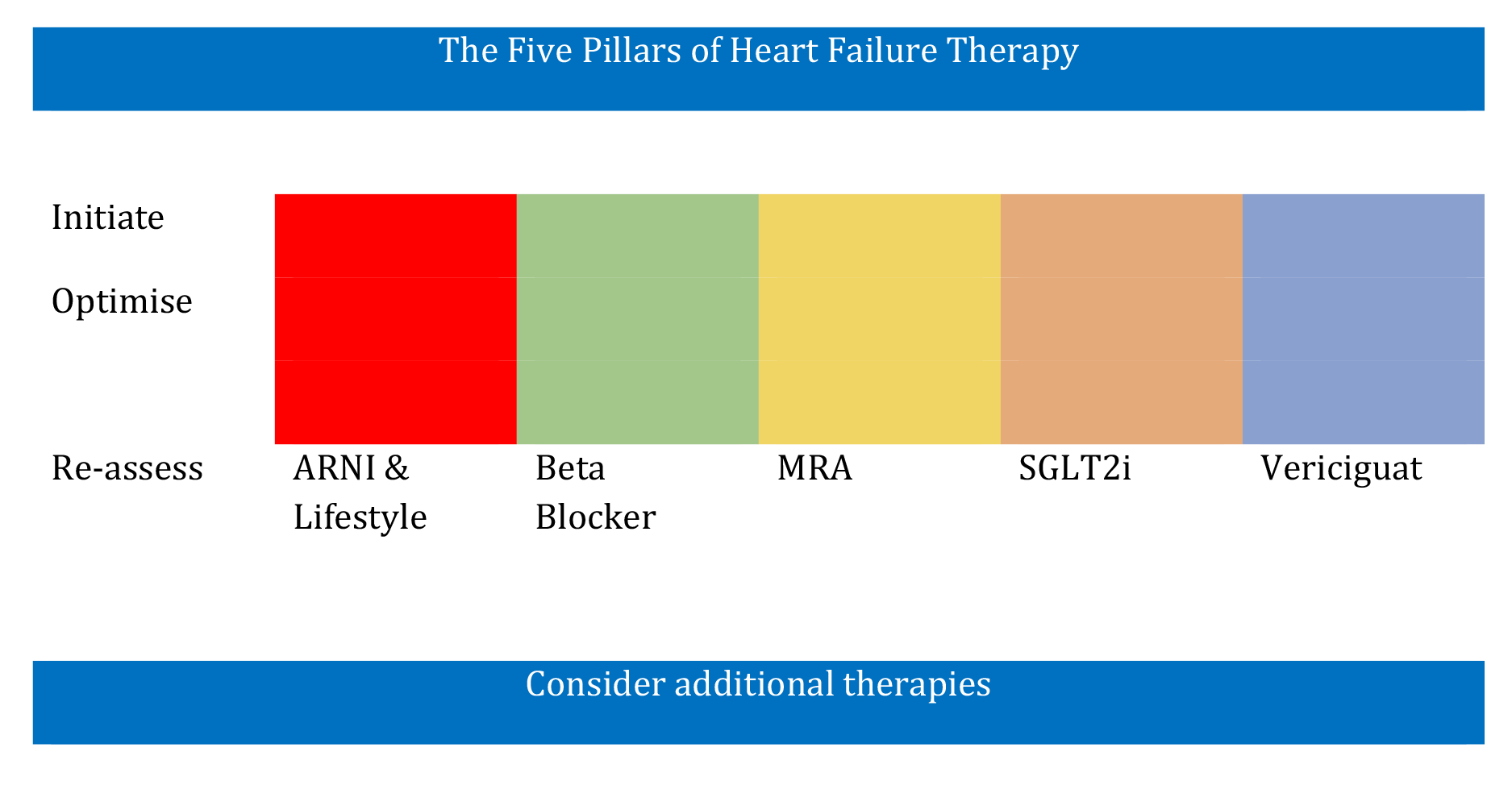
The role of the “four pillars” of HF therapy, including beta blockers, ARNI/angiotensin receptor blockers (ARBs), MRAs, and sodium-glucose co-transporter 2 Inhibitors (SGLT2i), is established [11], but some patients continue to die or remain uncontrolled during the management of HF [1, 2, 3]. Therefore, it may be proposed that vericiguat could be the Fifth Pillar of HF (Fig. 1, Ref. [1]).
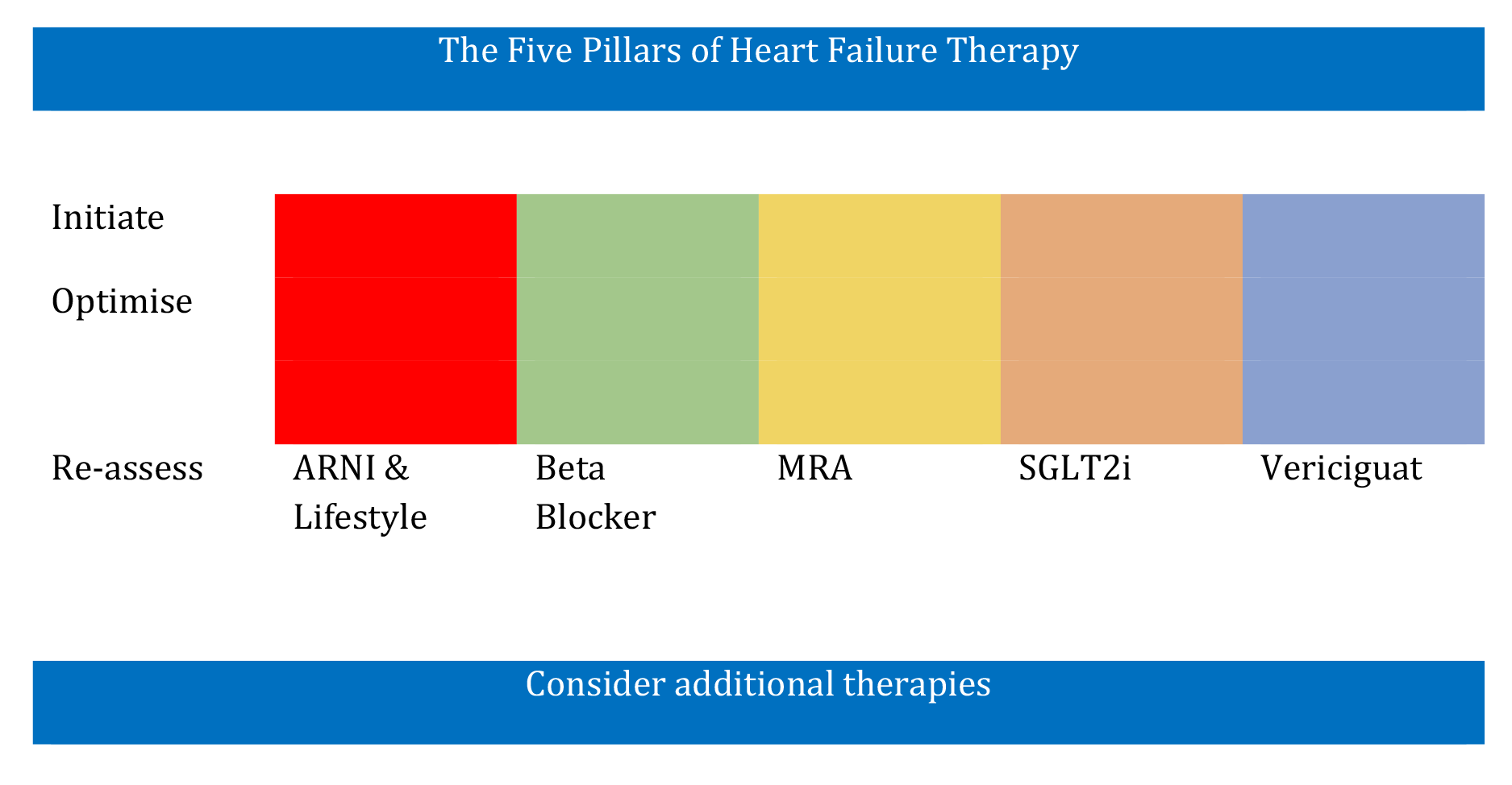 Fig. 1.
Fig. 1.
Five pillars of heart failure management. ARNI, angiotensin receptor-neprilysin inhibitor; MRA, mineralocorticoid receptor antagonist; SGLT2i, sodium-glucose co-transporter 2 inhibitors.
It is possible that in the future, methods to improve outcomes may be the integration of multiomic profiling involving personalized medicine and innovative designs of clinical trials such as chronotherapy, to address residual risk for identification of new therapeutic targets.
The Four Pillars of heart failure include SGLT2i, which is also recommended for HFpEF. Other pillars of heart failure are ACE inhibitors and ARBs, or ARNIs, along with beta-blockers and MRAs. ARNIs are preferred because of their independent mechanism of selective action in heart failure. Vericiguat may be the Fifth Pillar of heart failure because it has a unique mortality benefit, and it also has an independent mechanism of action. Therefore, its potential beneficial role calls for an update to the current GDMT.
RBS and NRH conceived the first draft, which was sent to other authors. AS and GE design the manuscript. All authors read and made critical suggestions to redraft and revise the final draft to improve the hypothesis for critical appraisal and revision as well as for editing. All the authors have read and agreed to be accountable of the accuracy and the content of the editorial.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflicts of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.