
 , Lifan Yang 3,†, Jianing Fan 1,2, Zilong Weng 1,2, Yuliang Long 1,2, Wenzhi Pan 1,2,*
, Lifan Yang 3,†, Jianing Fan 1,2, Zilong Weng 1,2, Yuliang Long 1,2, Wenzhi Pan 1,2,* , Daxin Zhou 1,2, Junbo Ge 1,2
, Daxin Zhou 1,2, Junbo Ge 1,21 Department of Cardiology, Zhongshan Hospital, Fudan University, 200032 Shanghai, China
2 National Clinical Research Center for Interventional Medicine, 200032 Shanghai, China
3 Department of Cardiology, Shanghai Geriatric Medical Center, 201100 Shanghai, China
†These authors contributed equally.
Abstract
Transcatheter aortic valve replacement (TAVR) is now recognized as an important treatment for pure severe aortic regurgitation (PSAR). Some patients with PSAR also suffer from functional mitral regurgitation (FMR). However, whether TAVR can improve FMR in patients with PSAR and the predictors of this improvement remain unknown. Thus, this study aimed to explore predictors of FMR improvement in patients with PSAR undergoing TAVR.
Patients with PSAR and ≥mild FMR who underwent TAVR at the Zhongshan Hospital Affiliated with Fudan University were enrolled from June 2020 to June 2024. Participants were divided into groups with or without FMR improvement depending on whether FMR improved 1 month post-TAVR. Baseline data, imaging results, and follow-up data of the patients were collected.
This study included 111 patients, among whom 59 had improved FMR, and 52 did not. Compared to patients without FMR improvement, significantly fewer patients in the FMR-improved group were diagnosed with renal insufficiency (0% vs. 10%; p = 0.015) and left bundle branch block (0% vs. 8%; p = 0.030). Moreover, more were diagnosed with hypertension (80% vs. 56%; p = 0.007), and right bundle branch block (10% vs. 0%; p = 0.018). On transthoracic ultrasound, patients with FMR improvement were more likely to have a lower left ventricular ejection fraction (LVEF) and larger left ventricular end-diastolic (LVED) dimensions. In both groups, the degree of aortic regurgitation was significantly improved during 1-day and 1-month follow-ups post-TAVR (p < 0.001). No significant differences in the incidence of postoperative adverse events were found between the two groups during the short-term follow-up. Patients with higher degrees of FMR, lower LVEF, and hypertension were more likely to experience improvement in FMR post-TAVR.
FMR improvement is observed in approximately half of PSAR patients undergoing TAVR. Higher FMR, lower LVEF, and hypertension before a TAVR are independent predictors of improvement in FMR.
Keywords
- mitral regurgitation
- pure severe aortic regurgitation
- transcatheter aortic valve replacement
- predictors
- logistic regression
Aortic regurgitation (AR) is a common form of valvular heart disease that is characterized by the reflux of blood from the aorta into the left ventricle (LV) during diastole. Abnormalities within the aortic valve, aortic root, and ascending aorta contribute to AR [1]. The prevalence of AR in the population is estimated to be approximately 4.9%, with 0.5% of individuals experiencing moderate or greater AR [2, 3]. Surgical aortic valve replacement (SAVR) is the gold standard for treating pure severe aortic regurgitation (PSAR). Nevertheless, as many as one in five patients can only be treated conservatively because they are at high risk or have contraindications to surgery and have a higher mortality rate [4].
Over the past two decades, transcatheter aortic valve replacement (TAVR) has emerged as a less invasive alternative to surgery for the treatment of symptomatic severe aortic stenosis (AS), and its indications have gradually been extended to younger, low-risk patients with longer life expectancies [5, 6]. In recent years, TAVR has been increasingly used in patients with PSAR who have unfavorable risk profiles [7, 8]. Several meta-analyses have demonstrated the feasibility and safety of TAVR in treating selected PSAR patients who are unsuitable for SAVR [9, 10].
Mitral regurgitation is defined as retrograde systolic blood flow from the left ventricle to the left atrium, and can be independent or secondary to AR. Epidemiological data have found that moderate or severe regurgitation is the most common valvular disease in the United States [11] and the second most common valvular heart disease requiring surgery in Europe [4]. For AS patients treated with TAVR, significant mitral regurgitation (MR) at baseline and persistent MR after surgery is associated with an increased risk of all-cause mortality, cardiac death, and cardiac hospitalization [12, 13, 14]. However, the role of TAVR in treating patients with AR and MR remains unknown. Therefore, this study sought to investigate the safety and efficacy of TAVR in patients with AR and MR.
Patients who were diagnosed with PSAR and
Based on whether FMR improved post-TAVR, patients were divided into the
MR-improved group and the MR-nonimproved group according to echocardiography.
Clinical information on the patients was collected from medical records and the
catheterization laboratory information system for retrospective analysis. The
baseline information of patients, such as hypertension, diabetes, pulmonary
arterial hypertension, atrial fibrillation, heart failure, and renal
insufficiency before surgery, was documented. Patients underwent multidetector
computed tomography (CT) and echocardiography examinations, and postoperative
follow-up echocardiography was performed. Parameters such as left ventricular
ejection fraction (LVEF), left atrial and left ventricular dimensions, degree of
aortic valve regurgitation, and mean transvalvular pressure of the aortic valve
were recorded. MR grading was established according to the European Society of
Echocardiography diagnostic criteria [5]. It was quantified as none or trace,
mild, mild-moderate, moderate, moderate-severe, or severe. Grading of AR severity
was based on the valve regurgitant jet area obtained from echocardiography: none,
trace, mild, moderate, and severe. FMR, which was improved post-TAVR, was defined
as
All patients underwent TAVR via intravenous anesthesia by the structural heart disease surgery team in the Department of Cardiology, Zhongshan Hospital. When using Venus, an auto-expandible device to treat AR, the length from the base of the left coronary sinus to the midpoint of the anterior mitral leaflet should be greater than 25 mm; otherwise, the mitral valve function would be affected. Patients had a follow-up visit at the outpatient department 30 days postoperatively, at which time transthoracic echocardiography (TTE) and electrocardiography (ECG) examinations were performed and perioperative endpoint events recorded. The definition of clinical outcomes followed the Valve Academic Research Consortium-3 (VARC-3) criteria [12]. The primary endpoints included all-cause death and cardiovascular death. The secondary endpoints included TAVR-related complications, such as myocardial infarction, major bleeding events, major vascular complications, acute kidney injury, stroke, endocarditis, new-onset atrial fibrillation, implantation of a new pacemaker, coronary artery obstruction, moderate or greater paravalvular leak, and rehospitalization.
Statistical analysis of the data was conducted using Stata 15.1 software (StataCorp LLC, College Station, TX, USA). The
mean
A total of 111 patients were enrolled, including 52 with persistent MR, with a
mean age of 72.47
| Patient characteristics | MR improved (n = 59) | MR nonimproved (n = 52) | p value |
| Age, years | 73.29 |
71.54 |
0.198 |
| Male, n (%) | 39/59 (66%) | 30/52 (58%) | 0.362 |
| Body mass index (kg/m2) | 22.06 |
21.71 |
0.629 |
| Smoke, n (%) | 6/59 (10%) | 6/52 (12%) | 0.817 |
| Hyperlipidemia, n (%) | 17/59 (29%) | 17/52 (33%) | 0.658 |
| Hypertension, n (%) | 47/59 (80%) | 29/52 (56%) | 0.007 |
| Diabetes mellitus, n (%) | 4/59 (7%) | 6/52 (12%) | 0.382 |
| Atrial fibrillation, n (%) | 15/59 (25%) | 10/52 (19%) | 0.436 |
| COPD, n (%) | 5/59 (10%) | 6/52 (10%) | 0.922 |
| Previous PCI, n (%) | 2/59 (3%) | 5/52 (10%) | 0.178 |
| PPM, n (%) | 2/59 (3%) | 3/52 (6%) | 0.546 |
| Peripheral vascular disease, n (%) | 0/59 (0%) | 2/52 (4%) | 0.128 |
| Renal insufficiency, n (%) | 0/59 (0%) | 5/52 (10%) | 0.015 |
| Left bundle branch block, n (%) | 0/59 (0%) | 4/52 (8%) | 0.030 |
| Right bundle branch block, n (%) | 6/59 (10%) | 0/52 (0%) | 0.018 |
| Atrioventricular block, n (%) | 10/59 (17%) | 7/52 (13%) | 0.611 |
| NYHA functional class III/IV, n (%) | 52/59 (88%) | 42/52 (81%) | 0.282 |
| Hemoglobin (g/L) | 125.61 |
124.40 |
0.736 |
| Serum creatinine (mg/dL) | 112.70 |
94.06 |
0.218 |
| NT-proBNP (pg/mL) | 1569.86 |
1896.64 |
0.411 |
| ALT (U/L) | 27.27 |
24.29 |
0.327 |
| STS risk score (%) | 5.52 |
5.51 |
0.718 |
Abbreviations: MR, mitral regurgitation; COPD, chronic obstructive pulmonary disease; PCI, percutaneous coronary intervention; PPM, permanent pacemaker; NYHA, New York Heart Association; NT-proBNP, N-terminal pro-B-type natriuretic peptide; ALT, alanine aminotransferase; STS, Society of Thoracic Surgeons.
Compared to patients without FMR improvement, significantly less patients in the
FMR-improved group were diagnosed with renal insufficiency (0% vs. 10%,
p = 0.015), left bundle branch block (0% vs. 8%, p = 0.030),
and more were diagnosed with hypertension (80% vs. 56%, p = 0.007), and
right bundle branch block (10% vs. 0%, p = 0.018). There were no
significant differences in age, male sex, height, weight, body mass index,
smoking, hyperlipidemia, diabetes mellitus, atrial fibrillation, previous
percutaneous coronary intervention (PCI), permanent pacemaker (PPM), peripheral
vascular disease, symptoms, atrioventricular block, New York Heart Association
(NYHA) functional class III or IV, hemoglobin, serum creatinine, N-terminal
pro-B-type natriuretic peptide, alanine aminotransferase (ALT), or Society of
Thoracic Surgeons (STS) risk score between the two groups (Table 1). The TTE
examination showed that patients in the MR-improved group had a lower ejection
fraction (49.45
| MR improved (n = 59) | MR nonimproved (n = 52) | p value | |||
| Echocardiography | |||||
| LVEF (%) | 49.45 |
60.53 |
|||
| LAED (mm) | 44.21 |
42.92 |
0.332 | ||
| LVEDd (mm) | 55.96 |
54.29 |
0.203 | ||
| LVEDs (mm) | 41.91 |
38.10 |
0.010 | ||
| IVS (mm) | 11.15 |
10.84 |
0.314 | ||
| LVOTD (mm) | 30.56 |
29.75 |
0.317 | ||
| Aortic valve peak velocity (m/s) | 2.14 |
2.00 |
0.370 | ||
| Mean valve gradient (mmHg) | 10.9 |
10.23 |
0.931 | ||
| Effective orifice area (cm2) | 2.73 |
2.85 |
0.321 | ||
| Severe AR, n (%) | 59/59 (100%) | 52/52 (100%) | - | ||
| MR degree, n (%) | |||||
| None or trace | 0 (0%) | 0 (0%) | |||
| Mild | 10 (17%) | 29 (56%) | |||
| Mild to moderate | 16 (27%) | 22 (42%) | |||
| Moderate | 20 (34%) | 1 (2%) | |||
| Moderate to severe | 7 (12%) | 0 (0%) | |||
| Severe | 6 (10%) | 0 (0%) | |||
| Moderate or greater TR, n (%) | 11/59 (22%) | 2/52 (5%) | 0.014 | ||
| PASP (mmHg) | 52.98 |
52.25 |
0.685 | ||
| Computed tomography | |||||
| Aortic annulus area (mm2) | 533.12 |
502.58 |
0.106 | ||
| Aortic annulus perimeter (mm) | 84.85 |
82.56 |
0.142 | ||
| Aortic annulus long axis diameter (mm) | 28.87 |
27.72 |
0.060 | ||
| Largest diameter of ascending aorta (mm) | 35.48 |
35.99 |
0.690 | ||
Abbreviations: LVEF, left ventricular ejection fraction; LAED, left atrial end dimension; LVEDd, left ventricular end-diastolic dimension; LVEDs, left ventricle end-systolic dimension; LVOTD, left ventricular outflow tract diameter; IVS, interventricular septal thickness; AR, aortic regurgitation; MR, mitral regurgitation; TR, tricuspid regurgitation; PASP, pulmonary artery systolic pressure.
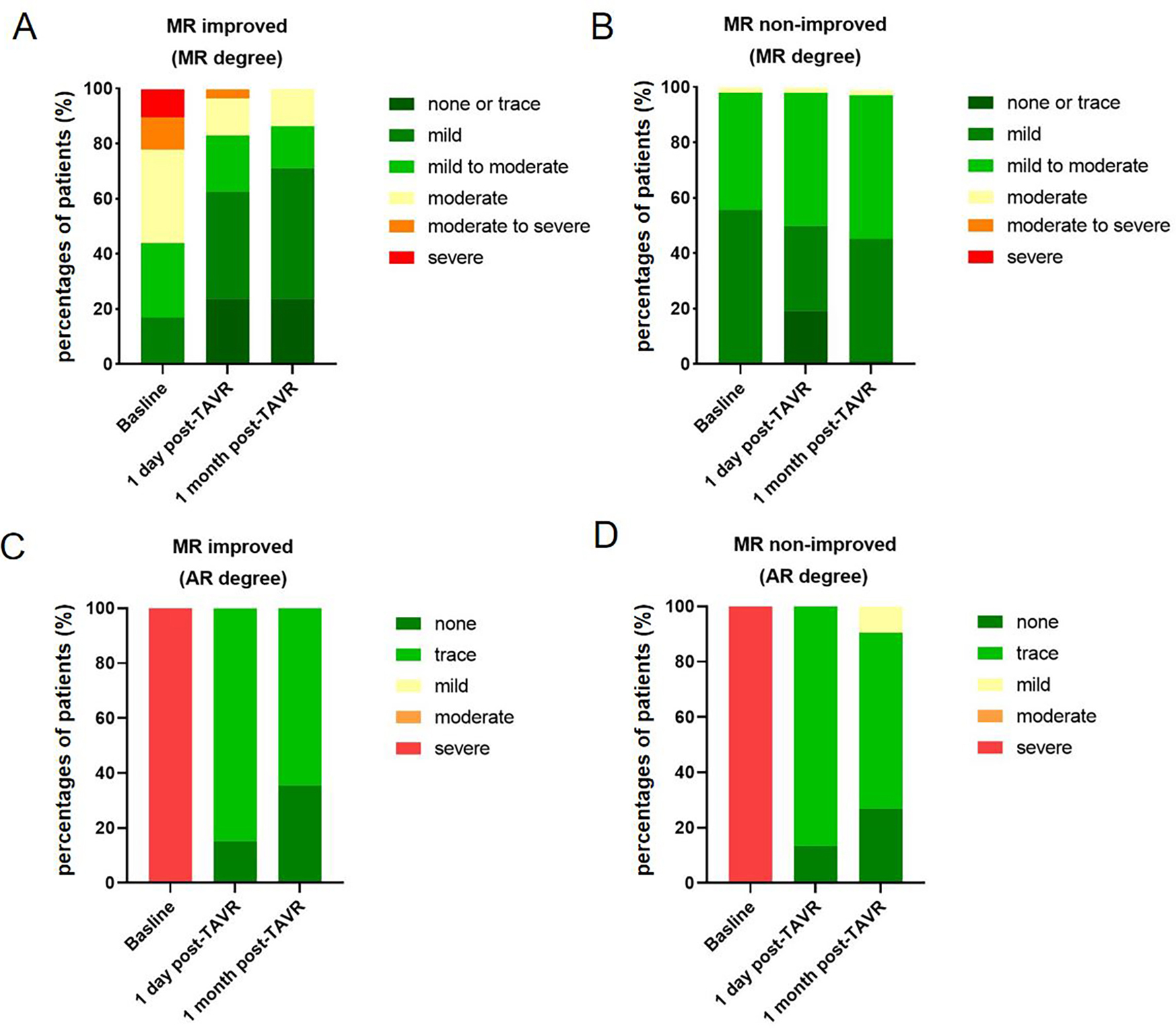
The overall decrease in MR severity after TAVR was observed only in the
MR-improvement group (preoperative vs. postoperative day 1 vs. postoperative
month 1, p = 0.001), whereas postoperative AR severity significantly
improved in both groups (preoperative vs. postoperative day 1 vs. postoperative
month 1, p
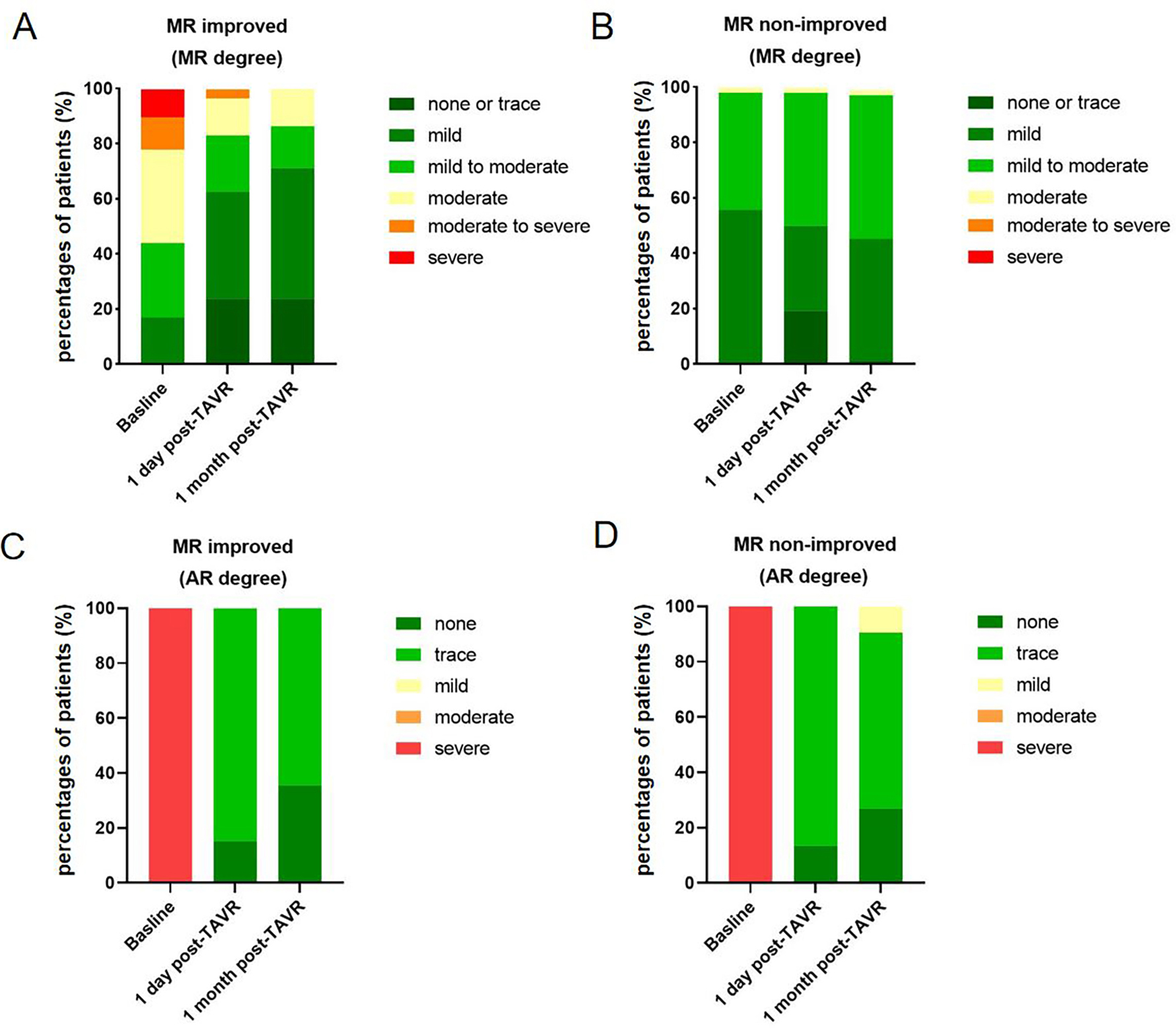 Fig. 1.
Fig. 1.
Changes of AR and MR before and after TAVR were assessed in both groups. (A) MR degree at baseline, 1-day post-TAVR, and 1-month post-TAVR in MR improved group. (B) MR degree at baseline, 1-day post-TAVR, and 1-month post-TAVR in MR non-improved group. (C) AR degree at baseline, 1-day post-TAVR, and 1-month post-TAVR in MR improved group. (D) AR degree at baseline, 1-day post-TAVR, and 1-month post-TAVR in MR non-improved group. MR, mitral regurgitation; AR, aortic regurgitation; TAVR, transcatheter aortic valve replacement.
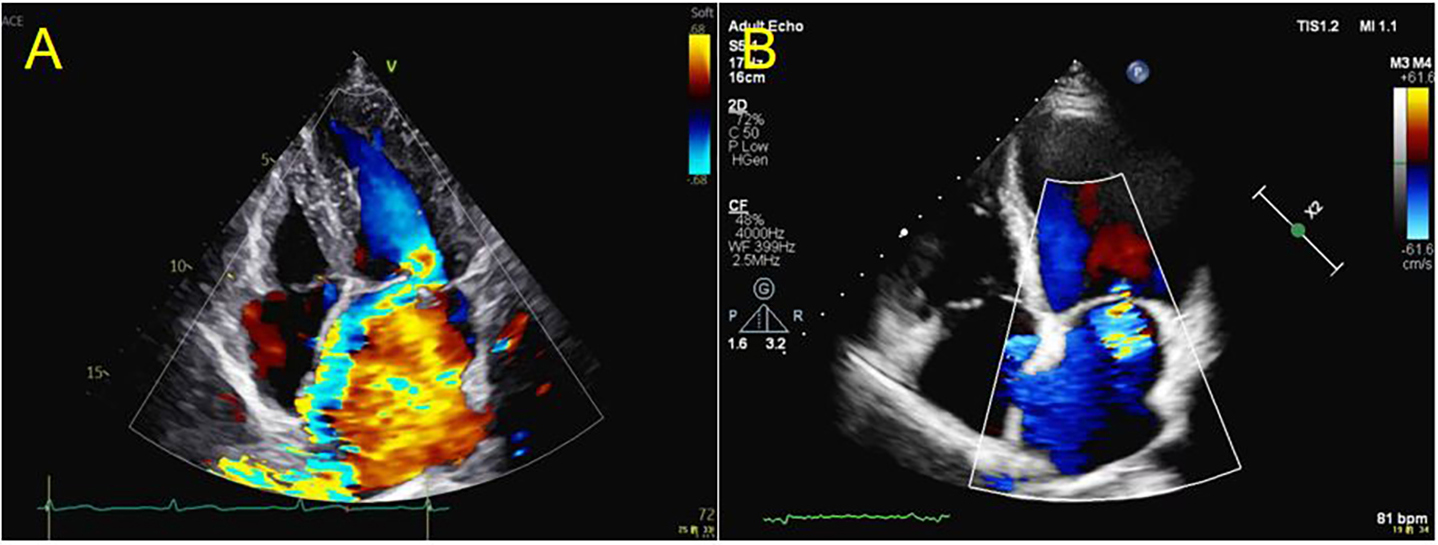
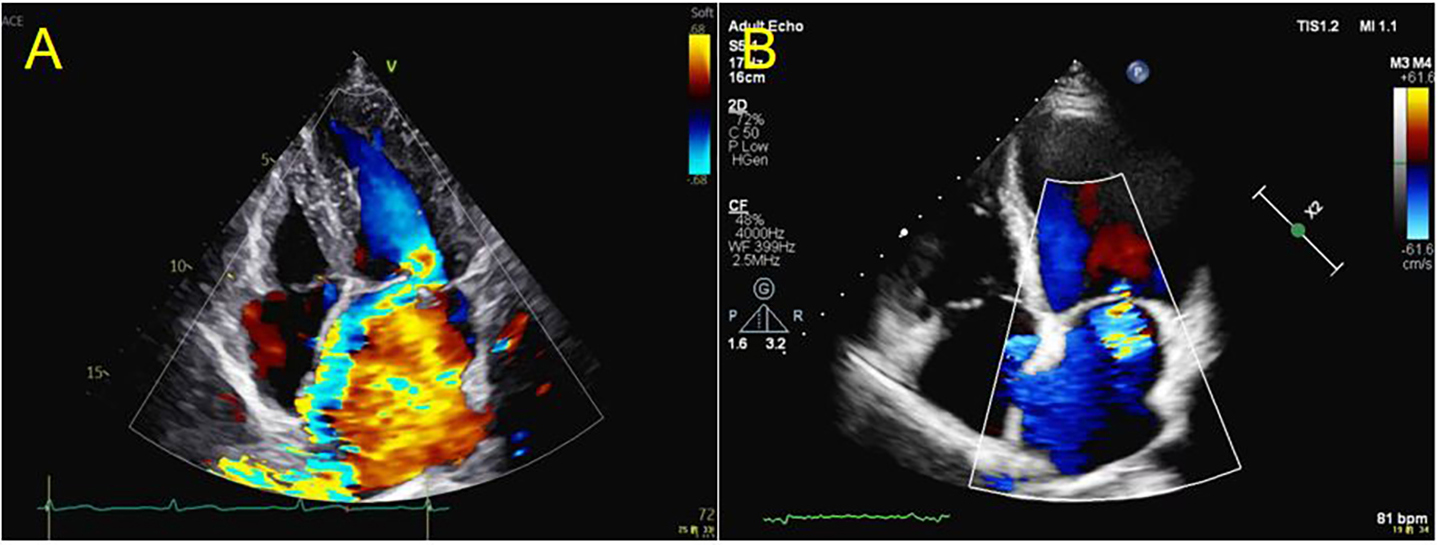 Fig. 2.
Fig. 2.
The echocardiography examination showing the AR and MR before TAVR and 1-month post-TAVR. (A) The echocardiography examination showed severe MR before TAVR. (B) The echocardiography examination showed trace MR one-month post-TAVR. AR, aortic regurgitation; MR, mitral regurgitation; TAVR, transcatheter aortic valve replacement.
There was no significant difference in primary and secondary endpoints in patients with or without improvement of MR who underwent TAVR in the hospital and 1 month after the operation. All-cause death or cardiac death did not occur in the two groups. During hospitalization, bleeding events, major vascular complications, stroke, new-onset atrial fibrillation, new-onset left bundle branch block, new-onset atrioventricular block, permanent pacemaker implants and moderate-to-severe paravalvular leaks were 0%, 2%, 0%, 11%, 19%, 18%, 19%, and 11% in the MR improved group and 4%, 2%, 4%, 13%, 12%, 23%, 13%, and 13% in the MR nonimproved group, respectively. In the 1-month follow-up, 2% stroke, 2% new-onset atrioventricular block, 2% new permanent pacemaker implantation, 8% paravalvular leak (PVL), and 4% rehospitalization were observed in the MR-improved group. The non-improved MR group had 4% bleeding events, 2% stroke, 4% new left bundle block, 2% new-onset atrioventricular block, 2% permanent pacemaker, 7% moderate or greater paravalvular leaks, and 9% rehospitalization (Table 3).
| Clinical end-points, n (%) | In-hospital | 1-month | |||||
| MR improved (n = 59) | MR nonimproved (n = 52) | p | MR improved (n = 59) | MR nonimproved (n = 52) | p | ||
| Primary endpoints | |||||||
| All-cause mortality | 0 (0%) | 0 (0%) | - | 0 (0%) | 0 (0%) | - | |
| Cardiovascular mortality | 0 (0%) | 0 (0%) | - | 0 (0%) | 0 (0%) | - | |
| Secondary endpoints | |||||||
| Bleeding event | 0 (0%) | 2 (4%) | 0.180 | 0 (0%) | 2 (4%) | 0.180 | |
| Major vascular complication | 1 (2%) | 1 (2%) | 0.928 | 0 (0%) | 0 (0%) | - | |
| Acute renal failure | 0 (0%) | 0 (0%) | - | 0 (0%) | 0 (0%) | - | |
| Stroke | 0 (0%) | 2 (4%) | 0.180 | 1 (2%) | 1 (2%) | 0.928 | |
| Myocardial infarction | 0 (0%) | 0 (0%) | - | 0 (0%) | 0 (0%) | - | |
| New AF | 6 (11%) | 6 (13%) | 0.817 | 0 (0%) | 0 (0%) | - | |
| New LBBB | 9 (19%) | 7 (12%) | 0.788 | 0 (0%) | 2 (4%) | 0.180 | |
| New AVB | 10 (18%) | 11 (23%) | 0.572 | 1 (2%) | 1 (2%) | 0.928 | |
| New PPM | 11 (19%) | 6 (13%) | 0.300 | 1 (2%) | 1 (2%) | 0.928 | |
| Endocarditis | 0 (0%) | 0 (0%) | - | 0 (0%) | 0 (0%) | - | |
| Perivalvular leakage | 6 (11%) | 6 (13%) | 0.817 | 4 (8%) | 3 (7%) | 0.827 | |
| Rehospitalization | 0 (0%) | 0 (0%) | - | 2 (4%) | 4 (9%) | 0.317 | |
Abbreviations: AF, atrial fibrillation; LBBB, left bundle branch block; AVB, atrioventricular block; PPM, permanent pacemaker; PVL, paravalvular leak.
The results of univariable and multivariable logistic regression analyses for
the FMR improvement are shown in Table 4. Age, male, BMI, LAD, and AF were
incorporated into the univariable and multivariable logistic regression analysis.
Among the variables, MR degree, LVEDs, hypertension, and LVEF were associated
with FMR improvement (all p
| Variables | Univariate analysis | Multivariate analysis | ||||
| OR | 95% CI | p | OR | 95% CI | p | |
| Age | 1.036 | 0.982–1.093 | 0.198 | 0.967 | 0.880–1.061 | 0.476 |
| Male | 1.805 | 0.834–3.904 | 0.134 | 0.410 | 0.107–1.574 | 0.194 |
| BMI | 1.043 | 0.941–1.155 | 0.425 | 1.047 | 0.869–1.261 | 0.631 |
| MR degree | 1.753 | 1.190–2.582 | 0.004 | 4.361 | 1.835–10.365 | 0.001 |
| LVEDs | 1.054 | 1.003–1.109 | 0.038 | 0.980 | 0.901–1.067 | 0.647 |
| Hypertension | 2.597 | 1.136–5.925 | 0.024 | 3.950 | 1.007–15.489 | 0.049 |
| LVEF | 0.959 | 0.921–0.999 | 0.046 | 0.882 | 0..814–0.955 | 0.002 |
| LAD | 0.990 | 0.924–1.060 | 0.766 | 0.983 | 0.876–1.104 | 0.777 |
| AF | 1.432 | 0.579–3.539 | 0.437 | 0.867 | 0.196–3.823 | 0.850 |
Abbreviations: CI, confidence interval; BMI, body mass index; MR, mitral regurgitation; LVEDs, left ventricular end-systolic dimension; LVEF, left ventricular ejection fraction; LAD, left atrial diameter; AF, atrial fibrillation.
This study investigated the improvement in FMR post-TAVR in patients with PSAR. The key findings are as follows: (1) FMR in more than half of the patients (53.15%) improved with TAVR for PSAR. (2) A higher FMR degree, lower LVEF, and hypertension before TAVR are independent predictors of FMR improvement. (3) No significant differences were found in the incidence of postoperative adverse events between the two groups during the short-term follow-up.
In our study, with a limited sample size, the prevalence of FMR in PSAR patients is up to 45%. The reflux of blood and subsequent increased back pressure lead to significant volume overload, resulting in significant MR. Yang et al. [15] found that patients with both significant AR and secondary MR resulted in a 2.34-fold increase in risk for mortality relative to the expected survival of an age- and sex-matched population, while the group with pure AR only had a 1.25-fold excess mortality risk. In addition, patients with residual mild MR after mitral valve repair have an increased risk of early adverse outcomes [16, 17, 18]. However, the best therapy for that group of patients remains undecided [19]. Some studies recommend SAVR because MR and AR can be treated simultaneously [19]. However, surgery would not be suitable for some patients, especially those with higher STS scores or elderly patients. In contrast to SAVR, patients who undergo TAVR do not routinely undergo concomitant interventions on the mitral valve, even if significant MR is present at the time of the procedure. Therefore, we explored whether TAVR could improve not only AR but also FMR. The present study found that 53.15% of patients were observed to have an improvement in FMR via TAVR for PSAR. Therefore, for those patients with PSAR who would have an improvement in FMR post-TAVR, TAVR can be considered an effective strategy for PSAR, which can kill two birds with one stone.
We found that patients with lower LVEF and hypertension are more likely to have improved FMR post-TAVR. The underlying mechanisms may be as follows: First, hypertension increases the load on the aortic valve, inducing AR, subsequently increasing left ventricular pressure, and leading to greater pressure on the mitral valve, leading to FMR. After the AR improved, the pressure on the mitral valve decreased, and the FMR improved. Second, a higher degree of FMR indicates the existence of increased mitral valve transvalvular gradients and more reflux. Therefore, when regurgitation was decreased, the change in MR reflux was greater in the higher-level FMR degree group than in the lower-level FMR group. Third, a higher level of AR at baseline would result in more blood retention in the left ventricle, which leads to decreased LVEF over time and causes the left ventricle to become larger, which leads to increased FMR. This study is the first report to explore the predictors of MR improvement post-TAVR for PSAR. A previous study investigated the predictors of MR improvement after TAVR for AS, and ejection fraction and LVED were found to be predictors [20]. Our study did not distinguish between atrial FMR and ventricular FMR, which may have different responses to TAVR. Therefore, the classification of FMR needs to be considered when conducting further studies.
During the 1-month follow-up, no major adverse events were found in either group. The results demonstrated that it is safe and efficient for PSAR patients with mild to severe FMR to undergo TAVR. Zheng et al. [21] also demonstrated the safety and efficacy of transfemoral TAVR with the Venus A-Valve in the treatment of patients with AR. In addition, no significant differences were found in the incidence of postoperative adverse events between the MR improved group and the non-MR improved group during the short-term follow-up. However, we did not have a longer follow-up period, and the results may be different with a longer follow-up period. Mavromatis et al. [22] found that, in contrast with the MR improved group, the patients without MR improvement undergoing TAVR for AS had an increased mortality and the need for heart failure rehospitalization.
This study also has some limitations. First, the lack of CT parameters for FMR
restricted our further investigation on tenting height, valve leaflet motion, and
mitral calcification, which should be taken into consideration in future studies.
Second, the number of patients in our study is small, and more patients should be
enrolled in future research. Third, further screening and study of the population
with the presence of
FMR improvement is observed in approximately half of PSAR patients undergoing TAVR. A higher degree of FMR, lower LVEF, and hypertension pre-TAVR are independent predictors. TAVR appears to be a safe and efficient treatment for patients with simultaneous PSAR and FMR.
All data generated or analyzed during this study are included in this published article.
DL and LY were in charge of the research’s overall execution and manuscript writing. JF, ZW, YL, WP, DZ, and JG performed the data analysis, interpretation, and drafted the manuscript. WP, DZ, and JG were responsible for reviewing, critically revising manuscripts, and communicating with the journal and editorial office during the submission process, throughout peer review, and during publication. All authors contributed to the critical revision of the manuscript for important intellectual content, reviewed, and approved the manuscript prior to submission. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was carried out in accordance with the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the Zhongshan Hospital Affiliated with Fudan University (Protocol No. B2025-077). Informed consent was obtained from the patients and their legal guardians for this study.
Not applicable.
This work was supported by the Shanghai Clinical Research Center Project for Interventional Medicine (19MC1910300) and Youth Fund of Zhongshan Hospital, Fudan University (ZSZP202517).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.