



 , Panagiotis Iliakis 1, Kyriakos Dimitriadis 1, Paschalis Karakasis 2, Panayotis K. Vlachakis 1, Eirini Dri 1, Konstantinos Pamporis 1, Alexios Antonopoulos 1, Constantina Aggeli 1, Konstantinos Aznaouridis 1, Dimitris Tousoulis 1, Konstantinos Tsioufis 1
, Panagiotis Iliakis 1, Kyriakos Dimitriadis 1, Paschalis Karakasis 2, Panayotis K. Vlachakis 1, Eirini Dri 1, Konstantinos Pamporis 1, Alexios Antonopoulos 1, Constantina Aggeli 1, Konstantinos Aznaouridis 1, Dimitris Tousoulis 1, Konstantinos Tsioufis 11 Department of Cardiology, “Hippokration” General Hospital of Athens, 11527 Athens, Greece
2 Department of Cardiology, Ippokrateio General Hospital of Thessaloniki, 54642 Thessaloniki, Greece
Abstract
Mitral regurgitation (MR) is a prevalent and prognostically relevant valvular disease, especially in patients with heart failure, in whom MR contributes to adverse remodeling, increased symptom burden, and higher mortality. Surgical repair or replacement remains the standard of care for suitable candidates, but many patients are excluded because of advanced age, comorbidities, or high surgical risk. Transcatheter methods have emerged as transformative alternatives, including mitral transcatheter edge-to-edge repair (MTEER) with devices such as MitraClip and PASCAL, annuloplasty-based devices such as Carillon and Cardioband, and transcatheter mitral valve replacement (TMVR) with devices such as Tendyne, Intrepid, and others under development. Data from randomized trials and registries have established that MTEER lowers hospital readmission rates and improves mortality in carefully selected secondary MR subjects, and that device upgrades improve procedural success and anatomical versatility. Annuloplasty provides targeted repair for functional MR with annular dilation, whereas TMVR offers an alternative for anatomically complex cases or those ineligible for MTEER, albeit with distinct procedural risks. Management of severe mitral annular calcification remains difficult and demands meticulous pre-procedural planning and customized device strategies. Careful patient selection based on MR etiology, proportionality, ventricular function, and anatomical suitability is essential for optimizing outcomes in this rapidly evolving field.
Keywords
- mitral regurgitation
- transcatheter mitral valve repair
- MitraClip
- PASCAL
- annuloplasty
- transcatheter mitral valve replacement
Mitral regurgitation (MR) remains one of the most prevalent and challenging valvular heart diseases globally, especially in aging populations with increasing comorbidities. MR has traditionally been managed with medical therapy and surgical repair or replacement. However, the advent of transcatheter approaches has significantly expanded treatment options. These innovations offer life-saving interventions to patients previously deemed inoperable due to high surgical risk. In recent years, mitral transcatheter edge-to-edge repair (MTEER) and transcatheter mitral valve replacement (TMVR) technologies have rapidly evolved. These advances have expanded treatment options for both primary and secondary MR. This review provides a comprehensive update on current transcatheter therapies for MR, emphasizing their mechanisms, evidence base, and evolving clinical roles.
The development of MR can be the result of the disruption of any part of the valvular apparatus (leaflets, annulus, chordae, papillary muscles). It can be either primary (PMR), due to intrinsic valve disease, or secondary (SMR), resulting predominantly from left ventricular dysfunction and dilation, but also from left atrial dilatation. The Carpentier classification provides a systematic approach to categorizing MR based on the underlying mechanism of valve dysfunction. It classifies MR into three types: Type I, characterized by normal leaflet motion with annular dilation or leaflet perforation; Type II, defined by excessive leaflet motion due to chordal elongation or rupture, as seen in mitral valve prolapse; and Type III, which involves restricted leaflet motion, either during diastole (Type IIIa, due to rheumatic disease) or systole (Type IIIb, often secondary to left ventricular dysfunction in heart failure). This classification is essential for guiding therapeutic decisions, as it helps differentiate primary from secondary MR and determines the most appropriate surgical or interventional approach.
MR plays a significant role in the progression and severity of heart failure (HF), contributing to increased morbidity and mortality [1]. As a common valvular abnormality, MR increases left atrial pressure and promotes ventricular remodeling. These changes exacerbate HF symptoms such as dyspnea and fatigue. For SMR in particular, the prognostic implications are crucial. In a meta-analysis comprising 53 studies and 45,900 patients, the presence of SMR was associated with increased all-cause mortality (risk ratio (RR) 1.79, 95% confidence interval (CI) 1.47–2.18), hospitalization for HF (HHF) (RR 2.26, 95% CI 1.92–2.67), and cardiac mortality (RR 2.62, 95% CI 1.87–3.69) [2].
Treatment options for MR include guideline-directed medical therapy (GDMT), cardiac resynchronization therapy, and structural interventions. Clinical trials have shown a reduction in SMR with HF medication, namely angiotensin receptor neprilysin inhibitors (ARNIs) and sodium-glucose co-transporter-2 inhibitors (SGLT2i) [3, 4]. However, a sub-analysis of a recent randomized trial in patients with HF and SMR showed that many patients are unable to tolerate one or more drug classes or achieve target doses [5]. Standard cardiac resynchronization therapy and conduction system pacing are also a mainstay in the management of SMR when dyssynchrony is present, as confirmed by a recent meta-analysis showing a reduced MR prevalence post-device implantation [6].
In an attempt to further decrease the excess morbidity and mortality associated with MR, research efforts have focused on the invasive correction of MR through transcatheter approaches. Table 1 summarizes representative transcatheter devices currently used or under investigation. However, the list is not exhaustive, as numerous TMVR platforms are currently in different stages of clinical development worldwide.
| Device (Manufacturer) | Mechanism | MR type | Access | Technical complexity | Procedural duration | Main advantages | Limitations-complications |
| MitraClip (Abbott) | MTEER | Secondary MR | TF-TS | Moderate | 60–120 min | Extensive clinical data | Severe leaflet calcification |
| Degenerative MR with focal prolapse | Minimally invasive | Short posterior leaflet | |||||
| Widely available | Large flail gap ( | ||||||
| Commissural jets | |||||||
| PASCAL | MTEER | Complex degenerative MR | TF-TS | Moderate-High | 90–150 min | More leaflet-friendly than MitraClip | Severe annular calcification in grasping zone |
| (Edwards Lifesciences) | Functional MR with wide gap | Better suited for large coaptation gaps | Very small mitral valve area | ||||
| DragonFly (Valgen MedTech) | MTEER | Degenerative MR | TF-TS | Moderate–high | 90–110 min | Central compressible filler with independent leaflet capture | Severe leaflet calcification in grasping zone |
| Leaflet length | |||||||
| MVA | |||||||
| ValveClamp (Hanyu Medical) | MTEER | Degenerative and functional MR | TA | High | 60–120 min | Direct transapical access providing improved coaxial alignment with the mitral valve and facilitating stable leaflet capture | Severe leaflet calcification in grasping zone |
| Insufficient leaflet length for grasping | |||||||
| Small mitral valve area with risk of mitral stenosis | |||||||
| Carillon (Cardiac Dimensions) | Indirect annuloplasty via coronary sinus | Secondary MR | TJ | Low-Moderate | 45–90 min | Preserves native valve | Severe MR |
| Minimally invasive | Coronary sinus-circumflex artery proximity issues | ||||||
| Suitable for SMR | |||||||
| Primary MR | |||||||
| Cardioband (Edwards Lifesciences) | Direct annuloplasty, cinching mitral annulus | Secondary MR with annular dilation | TF-TS | High | 120–180 min | Mimics surgical annuloplasty | Extensive annular calcification |
| Adjustable post-implantation | Posterior annular anatomy unsuitable for anchoring | ||||||
| Tendyne (Abbott) | TMVR | Severe degenerative or mixed MR | TA | High | 120–180 min | Complete MR elimination | Small LV cavity (LVOT obstruction risk) |
| Fully repositionable and retrievable | |||||||
| MAC-associated MR | High surgical risk for apical access | ||||||
| Intrepid (Medtronic) | TMVR | Functional MR with large annulus | TA | High | 120–180 min | No need for annular anchoring | LVOT obstruction risk |
| TF-TS | Suitable for diverse anatomies | Severe small LV cavity | |||||
| Sapien M3 (Edwards Lifesciences) | TMVR | Degenerative MR | TF-TS | High | 120–150 min | Fully percutaneous transseptal delivery | Requires precise docking |
| Small LVOT | |||||||
| High procedural success | Thrombosis risk | ||||||
| Durable MR elimination | |||||||
| Allows future valve-in-valve reintervention |
MTEER, mitral transcatheter edge-to-edge repair; TMVR, transcatheter mitral valve replacement; TF-TS, transfemoral–transseptal; TJ, transjugular; TA, transapical; MR, mitral regurgitation; SMR, secondary mitral regurgitation; MVA, mitral valve area; MAC, mitral annular calcification; LV, left ventricular; LVOT, left ventricular outflow tract.
MTEER is perhaps the most decorated method of percutaneous mitral valve intervention. The technique involves the percutaneous placement of a device, such as the MitraClip (Abbott, IL, USA) or the PASCAL (Edwards Lifesciences, CA, USA), to approximate the mitral valve leaflets, reducing regurgitant flow. By mimicking the surgical Alfieri stitch, MTEER creates a double-orifice valve, enhancing coaptation and restoring more efficient valve function.
The MITRA-FR and COAPT trials were two landmark randomized controlled studies that evaluated the role of MTEER using the MitraClip in patients with SMR and HF. While both trials sought to determine the efficacy of MitraClip compared to GDMT alone, there were important differences in patient selection and trial design (Table 2). These differences meant that MITRA-FR included patients with proportionate MR (where MR severity matched the degree of LV dysfunction), whereas COAPT focused on patients with disproportionate MR, meaning MR was excessively severe relative to the degree of LV dysfunction. The results of the two trials diverged significantly. MITRA-FR found no significant benefit of MitraClip over GDMT [7], while COAPT showed a significant benefit with MitraClip compared to GDMT alone [8]. These findings highlight the importance of careful patient selection when considering MTEER for SMR. The concept of proportionate vs. disproportionate MR has since become a crucial framework for deciding which patients will derive the greatest benefit from MitraClip therapy [9]. However, even though it provides a useful conceptual explanation for the divergent results of MITRA-FR and COAPT, patient selection for MTEER should not rely on this concept alone. Instead, treatment decisions should integrate MR severity, left and right ventricular size and function, and anatomical suitability, among others, within a multidisciplinary Heart Team evaluation.
| MITRA-FR | COAPT | |
| Sample size | 304 patients | 614 patients |
| LVEF inclusion criteria | 20–50% | |
| EROA | ||
| LVEDV | Larger (135 |
Smaller (101 |
| Severity of MR | Moderate-to-severe | Severe |
| GDMT | Less rigorously optimized | Strictly optimized and monitored |
| Primary endpoint | All-cause death or unplanned HF hospitalization | HF hospitalization at 24 months |
| Outcome | No difference in mortality or HF hospitalizations | Significant reduction in both |
| Interpretation | MR proportional to LV dysfunction (less likely to benefit from MTEER) | Disproportionate MR (more likely to benefit) |
LVEF, left ventricular ejection fraction; EROA, effective regurgitant orifice area; LVEDV, left ventricular end-diastolic volume; GDMT, guideline-directed medical therapy; HF, heart failure; MR, mitral regurgitation; MTEER, mitral transcatheter edge-to-edge repair.
Recently, the RESHAPE-HF2 trial assessed the efficacy of MTEER using MitraClip
in symptomatic HF patients with grade 3+/4+ SMR despite maximally tolerated GDMT
(Table 3) [10]. A total of 505 patients (mean age 70 years, 20% female, median
LVEF 32%) were randomized to MTEER + GDMT (n = 250) or GDMT alone (n = 255) with
a median follow-up of 18.8 months [10]. The primary outcome, a composite of first
or recurrent HF hospitalization or cardiovascular death at 24 months, was
significantly lower in the MTEER group (37.0 vs. 58.9 events per 100
patient-years, RR 0.64, number needed to treat = 5.1) [10]. Recurrent HF
hospitalizations, combined cardiovascular hospitalizations and all-cause
mortality, and days lost to death or HF hospitalization were also reduced with
MTEER [10]. At 12 months, MR
| Trial | Device | Design | Population | N | Primary outcome | Key result |
| MITRA-FR | MitraClip vs SoC | RCT | Secondary MR + HF | 304 | Death or HF hospitalization | OR 1.16 (no benefit vs GDMT) |
| COAPT | MitraClip vs SoC | RCT | Secondary MR + HF | 614 | HF hospitalization | HR 0.53 |
| CLASP IID | PASCAL vs MitraClip | RCT | Degenerative MR | 300 | MR |
95.8% vs 93.8% |
| DRAGONFLY-DMR | DragonFly | Prospective, single-arm | Degenerative MR | 112 | Freedom from all-cause mortality, mitral valve reintervention, and MR |
87.5% |
| REDUCE-FMR | Carillon | RCT | Secondary MR | 120 | LVESV reduction | –7.1 mL vs control |
| ENCIRCLE | Sapien M3 | Prospective, single-arm trial | Severe MR unsuitable for MTEER | 299 | Death or HF hospitalization | 25.2% at 1 year |
RCT, randomized controlled trial; SoC, standard of care; GDMT, guideline-directed medical therapy; HF, heart failure; MR, mitral regurgitation; LVESV, left ventricular end-systolic volume; OR, odds ratio; HR, hazard ratio.
The PASCAL transcatheter valve repair system is an alternative to the MitraClip for MTEER in patients with significant MR. Developed as a next-generation device, PASCAL offers key design modifications aimed at improving procedural outcomes, particularly in patients with complex mitral anatomy or challenging leaflet morphology. The PASCAL device is wider (10 mm vs. MitraClip’s 6 mm) and features a central spacer, which fills the regurgitant orifice. This helps distribute forces across the valve and reduces leaflet stress. At the same time, the MitraClip does not have a spacer, relying entirely on leaflet coaptation, which may be less effective in certain anatomies. Moreover, PASCAL has elongated, atraumatic paddles and clasps designed to minimize leaflet tension and improve leaflet capture, while MitraClip’s shorter, rigid arms may exert more stress on the leaflets, particularly in fragile or highly mobile valves.
The CLASP IID (Edwards PASCAL Transcatheter Valve Repair System Pivotal Clinical
Trial) was the first study directly comparing PASCAL versus MitraClip in patients
with degenerative mitral regurgitation (DMR) who were at high surgical risk [12].
It was a multicenter, prospective, randomized controlled trial conducted in the
United States and Europe. It enrolled 300 patients with severe symptomatic DMR.
PASCAL (95.8%) and MitraClip (93.8%) achieved MR
Importantly, the PASCAL MTEER system could be safely and effectively deployed in
patients once deemed unsuitable for MTEER based on anatomic characteristics,
namely, presence of
In its post-marketing MiCLASP study [15], the PASCAL system reproduced its
efficacy and safety in patients with significant MR of any etiology.
Specifically, incidence rates of major adverse events at 30 days were acceptable
(6.8%), with sustained MR reduction at 1 year (
Continuous improvement of PASCAL technology is also critical to the success of
the device. The REPAIR study was a multicenter, observational registry that
included 2165 patients treated with the PASCAL system across 14 centers in
Germany from 2019 to 2024 [16]. Unlike randomized controlled trials, REPAIR did
not apply strict inclusion/exclusion criteria, making it a real-world evaluation
of PASCAL’s performance. Patients were categorized into three groups based on the
iteration of the PASCAL system used: P10-only cohort (first-generation PASCAL
device), P10/AceGen1 cohort (introduction of the smaller PASCAL Ace device),
P10/AcePrec cohort (introduction of the PASCAL Precision delivery system). The
primary endpoint was the achievement of MR
Another transcatheter edge-to-edge repair system that has recently emerged is
the DragonFly (Valgen MedTech). The system is delivered via a transfemoral
transseptal approach and consists of a steerable delivery system and a clip
implant available in multiple sizes to accommodate varying mitral anatomies [18].
A distinctive feature of the device is the presence of a central compressible
filler, which expands within the regurgitant orifice when the device arms are
closed, enhancing leaflet coaptation while potentially limiting excessive leaflet
tension [18]. In addition, the device allows independent leaflet grasping and
controlled arm angulation, which may facilitate treatment of complex mitral
anatomies and improve device positioning [18]. Early clinical experience has
demonstrated encouraging procedural and short-term outcomes. In a multicenter
first-in-human study involving patients with severe MR at high surgical risk,
device implantation was successful in all treated patients, with MR
Another MTEER platform developed in China is the ValveClamp system (Hanyu
Medical Technology), which is performed through a transapical approach. The
system consists of a clamp device delivered through a 16-Fr introducer sheath and
incorporates a spherical valve-crossing device designed to prevent entanglement
within the chordae tendineae during advancement across the mitral valve [20]. The
clamp features V-shaped matching arms and a closed-ring mechanism that
facilitates leaflet capture and stabilization while creating a double-orifice
mitral valve configuration [20]. The transapical route provides a short and
direct trajectory to the mitral valve, potentially improving coaxial alignment
and procedural control compared with transseptal approaches [20]. Early
feasibility studies have demonstrated encouraging procedural performance. In a
prospective series of patients with functional MR, device implantation was
successful in 100% of cases, with most patients requiring a single clamp and a
mean procedural time of approximately 60 minutes. MR reduction to
Despite encouraging early results, the available evidence for those emerging MTEER platforms remains limited. Data arises from non-randomized studies, which restricts the ability to determine comparative efficacy relative to established devices such as MitraClip or PASCAL. In addition, enrolled patients were typically highly selected, often consisting of individuals with degenerative MR at high or prohibitive surgical risk and with favorable mitral valve anatomy suitable for leaflet-based repair. Such selection criteria may introduce referral and anatomical selection bias and limit the generalizability of these findings to broader MR populations encountered in routine practice. Furthermore, follow-up durations remain relatively short, and longer-term data are needed to assess device durability, recurrent MR, and the need for reintervention.
The Carillon Mitral Contour System (Cardiac Dimensions, WA, USA) is a percutaneous indirect annuloplasty device designed to treat SMR by reshaping the mitral annulus. Unlike leaflet-based MTEER systems, the Carillon device focuses on annular reduction, leveraging the anatomical relationship between the coronary sinus and the mitral annulus. By implanting a self-expanding nitinol device within the coronary sinus, Carillon applies external compression to reduce annular dilation and improve leaflet coaptation. This minimally invasive approach is particularly appealing for patients with HF and FMR, as it preserves native valve anatomy and allows for future interventions if needed.
The feasibility of this technology was proven more than a decade ago, through
the AMADEUS study of 30 patients receiving this device, demonstrating acceptable
major adverse event rates and improvement in quality of life [23]. The REDUCE-FMR
was the first sham-controlled trial evaluating its efficacy in improving SMR,
involving symptomatic patients with impaired LVEF, LV end-diastolic diameter
The Cardioband Mitral System (Edwards Lifesciences, CA, USA) is a transcatheter direct annuloplasty device designed to treat functional SMR by reducing mitral annular dilation and restoring leaflet coaptation. Unlike indirect annuloplasty systems such as Carillon, Cardioband is implanted directly onto the mitral annulus via a transfemoral, transseptal approach. The device consists of an adjustable, implantable band that is anchored along the posterior annulus using multiple fixation screws. Once securely placed, the band is incrementally cinched, effectively reducing annular size and improving mitral valve function. As with the Carillon system, this technique mimics surgical annuloplasty, preserving the native valve and allowing for future interventions if needed. Cardioband is particularly suited for patients with annular dilation and preserved leaflet mobility, offering a physiological and customizable approach to MR reduction while minimizing procedural risks compared to surgery.
The Cardioband feasibility study evaluated the safety and efficacy of the
Cardioband transcatheter mitral annuloplasty system in high-risk patients with
SMR [28]. Conducted across five European centers, the study enrolled 31 patients
with moderate-to-severe or severe MR despite optimal medical therapy. The
Cardioband was successfully implanted in all patients, with a 93.6% technical
success rate. Adjustment of the device led to a significant reduction in
septolateral annular dimension (from 36.8 mm to 29.0 mm, p
A subsequent study evaluated the 1-year outcomes of transcatheter mitral valve
repair using the Cardioband system in patients with moderate-to-severe or severe
SMR [29]. Conducted across 11 European centers, the study enrolled 60 patients
who were symptomatic despite receiving GDMT. The technical success rate was 97%,
and device success, based on Mitral Valve Academic Research Consortium (MVARC)
criteria, was 72%. Over one year, MR reduction was achieved in most patients
(95% had MR
Transcatheter mitral valve replacement (TMVR) is an emerging therapy for patients with significant MR who are poor candidates for conventional surgery, or in cases of MTEER failure/unsuitability. For MTEER specifically, anatomical constraints should be acknowledged, such as severe mitral annular dilation, short posterior leaflet, extensive calcification, or severe leaflet restriction where leaflet coaptation cannot be restored adequately. It may also be considered in cases of recurrent or residual MR after MTEER, where another MTEER procedure is unlikely to succeed. Current TMVR devices, such as Tendyne (Abbott, IL, USA), Intrepid (Medtronic, MN, USA), Sapien M3 (Edwards Lifesciences, CA, USA), and Evoque (Edwards Lifesciences, CA, USA), are expanding treatment options for these complex cases. However, dedicated TMVR systems remain investigational, and currently available evidence largely reflects early feasibility studies and registries, emphasizing procedural success and short-term outcomes rather than long-term efficacy and durability.
Transesophageal echocardiography (TEE), particularly three-dimensional (3D) TEE, plays a pivotal role in patient selection and procedural planning for TMVR by providing high-resolution visualization of the mitral valve apparatus and surrounding structures [31]. A comprehensive pre-procedural TEE assessment includes evaluation of mitral annular dimensions, leaflet morphology and mobility, commissural anatomy, and subvalvular structures, which may influence device feasibility and procedural complexity [31]. 3D-TEE allows dynamic assessment of the mitral annulus throughout the cardiac cycle, with measurements typically obtained at end-systole when annular dimensions are maximal [31]. In addition, TEE contributes to risk stratification for left ventricular outflow tract (LVOT) obstruction by assessing baseline LVOT area, anterior mitral leaflet length, septal thickness, and the mitral–aortic angle [31]. Functional parameters, including left and right ventricular function, pulmonary pressures, and left atrial size, are also important components of pre-procedural evaluation, as they influence procedural feasibility and clinical outcomes [31]. Furthermore, TEE enables detailed assessment of the interatrial septum and optimal transseptal puncture site, which is critical for achieving appropriate trajectory and device coaxiality during transseptal TMVR procedures [31].
Cardiac multidetector computed tomography (CT) plays a central role in pre-procedural planning for TMVR by providing comprehensive anatomical and procedural guidance. It enables precise characterization of mitral annular geometry (annular area/perimeter, intercommissural and anteroposterior measurements) to assist device sizing and appropriate oversizing to prevent paravalvular leak or device embolization [32]. The mitral annulus is typically modeled using a 3D saddle-shaped or D-shaped reconstruction to account for its complex geometry. In addition, CT allows detailed assessment of the mitral leaflets and subvalvular apparatus, including anterior mitral leaflet length and papillary muscle insertion, which may influence device anchoring and contribute to left ventricular outflow tract (LVOT) obstruction. A major component of CT-based planning is the simulation of virtual valve implantation to estimate the predicted neo-LVOT area, a key determinant of post-procedural LVOT obstruction risk, with values below approximately 1.7–2.0 cm2 associated with higher risk. Other anatomical predictors assessed by CT include septal thickness, left ventricular geometry, and the aorto-mitral angle. Furthermore, CT is essential for evaluating mitral annular calcification (MAC) distribution, thickness, and circumferential extent to determine the adequacy of the landing zone and anchoring stability. Finally, CT provides procedural guidance by enabling planning of the optimal transapical or transseptal access trajectory and determining fluoroscopic projection angles to facilitate coaxial device deployment.
Tendyne represents a promising transcatheter solution for patients unsuitable for repair, expanding treatment options for high-risk MR patients who previously had limited surgical alternatives. It is a self-expanding, bioprosthetic valve made of a tri-leaflet porcine pericardial valve within a nitinol frame [33]. It is delivered via a transapical approach through a small left thoracotomy [33]. The system is fully repositionable and retrievable before final deployment, allowing for optimal placement. Unlike surgical mitral valve replacement, Tendyne is secured using an apical tether, which stabilizes the valve within the native annulus and prevents migration [33]. This design accommodates a wide range of mitral anatomies, including patients with functional, degenerative, or mixed MR, as well as those with severe annular dilation or MAC.
Several disadvantages should be acknowledged. The implantation requires a mini-thoracotomy and transapical access, which increases procedural risk compared to transfemoral techniques. It should be stressed that, due to the apical puncture, there is an increased risk of bleeding, pericardial effusion, and tamponade. The apical tethering system exerts tension on the LV myocardium, potentially contributing to LV remodeling or dysfunction over time. Furthermore, Tendyne, like other TMVR devices, can obstruct the LVOT, leading to hemodynamic instability or severe obstruction, with patients having a small LV cavity size or a prominent anterior mitral leaflet being at higher risk.
The Tendyne Global Feasibility Trial evaluated the safety and efficacy of the Tendyne system in high-risk patients with symptomatic MR [34]. The technical success rate was 93.3%, with successful valve implantation in 28 out of 30 patients. At 30 days, 96.2% of patients had complete MR elimination, with only one patient experiencing mild residual MR. Additionally, left ventricular end-diastolic volume significantly decreased, suggesting positive left ventricular remodeling. The safety profile was favorable, with no intraprocedural deaths, strokes, or myocardial infarctions. The 30-day freedom from major adverse events was 83.3%, and only 13.8% required rehospitalization for HF. The Tendyne 2-Year Outcomes Study showed sustained MR elimination in 93.2% of surviving patients, with no cases of greater than mild MR [35]. The technical success rate was 97%, and HF hospitalization rates were significantly reduced. All-cause mortality was 39% at 2 years, with most deaths (43.6%) occurring within the first 90 days, reflecting the high-risk nature of the population. The safety profile remained acceptable, with low rates of stroke (5%), endocarditis (5%), and structural valve deterioration (0%).
Along the same lines, the TENDER study, a real-world, European multicenter
registry evaluating transapical mitral valve implantation with the Tendyne system
in high-risk patients (median age 77 years, 40% female) with symptomatic
moderate-to-severe MR of any etiology showcased a technical success rate of 95%,
with MR reduced to
The Intrepid system is a TMVR device composed of a bioprosthesis and a transapical delivery system [38]. The bioprosthesis features a trileaflet bovine pericardial valve housed in a dual-structure nitinol frame, with an inner circular stent for valve support and a flexible outer fixation ring designed to conform to the dynamic anatomy of the mitral annulus [38]. This outer ring provides fixation and sealing via its variable radial stiffness and a champagne cork-like shape that resists migration, while a brim aids imaging and tissue ingrowth [38]. The valve, available in various outer diameters, is designed to preserve native structures and minimize outflow obstruction [38]. Covered in polyester fabric, it prevents leaks and promotes long-term integration [38]. The transapical delivery system uses hydraulic actuation for precise, rotation-free deployment, eliminating the need for leaflet capture [38].
The study by Bapat et al. [39] reported the early clinical experience with the Intrepid TMVR system in patients who were deemed high or extreme risk for cardiac surgery. Conducted across 14 international centers, the pilot study enrolled 50 patients (mean age 73), with 86% in NYHA class III or IV, and most having SMR. The TMVR device was successfully implanted in 48 patients (96%). At 30 days, mortality was 14%, primarily due to bleeding or HF, but all surviving patients showed significant symptomatic improvement and mild or no residual MR [39]. The device showed no malfunction, thrombosis, or structural valve degeneration during a median follow-up of 173 days [39]. A subsequent cohort study followed up 252 patients treated with transapical Intrepid implantation, reporting all-cause mortality rates of 13.1%, 27.3%, and 36.2% at 30 days, 1 year, and 2 years, respectively [40]. Bleeding events were documented in 22.3% of the participants at 30 days [40]. Importantly, at 2 years, most of the alive participants were in good functional status (82.1% in NYHA class I/II) and had at most mild MR [40]. Over five years, the early Intrepid transapical TMVR device provided durable valve performance, sustained elimination of MR, and lasting symptom improvement in those high-risk patients, despite high overall mortality reflecting the population’s advanced disease [41].
Lately, a newer-generation, 35-F transfemoral transseptal access system has been introduced in the delivery of the Intrepid TMVR system. The study by Zahr et al. [42] presented 1-year results from the Early Feasibility Study of this approach in patients with symptomatic moderate-to-severe or severe MR at high surgical risk. Conducted at nine U.S. centers, 33 patients were enrolled, with 94% successfully receiving valve implants. At 30 days, there were no deaths or strokes, though 24% experienced vascular complications [42]. At 1 year, all-cause mortality was 6.7%, MR was nearly eliminated in all patients, and 92% of survivors were in NYHA class I or II, reflecting sustained symptom improvement [42]. Quality of life scores improved significantly, and valve performance remained stable, with low gradients and minimal regurgitation [42]. While vascular complications and venous thromboembolism were noted, no strokes or device-related deaths occurred [42]. These findings suggest that the transfemoral transseptal Intrepid TMVR system offers a promising, less invasive alternative for high-risk patients, with durable hemodynamic and clinical benefits.
The SAPIEN M3 system (Edwards Lifesciences) is a fully percutaneous, transseptal TMVR platform designed to treat severe, symptomatic MR in patients considered unsuitable for surgery or MTEER. The system uses a novel two-component design: a nitinol “dock” that encircles and stabilizes the subvalvular apparatus to create a secure landing zone, followed by implantation of a balloon-expandable SAPIEN M3 valve within this dock. This approach aims to overcome anatomical challenges that limit MTEER success, avoid the morbidity of transapical access, and provide a repeatable, repositionable platform that allows for future valve-in-valve reintervention if needed.
In the prospective, multicenter ENCIRCLE pivotal trial, the first large-scale evaluation of a fully percutaneous transseptal TMVR system, 299 patients underwent attempted implantation, with device success in 96% of cases [43]. These were elderly, high-risk patients (median age 77 years, mean STS-PROM 6.6%) with predominantly severe (grade 4) MR and significant comorbidity burden [43]. Clinical outcomes at one year demonstrated safety and effectiveness: the primary composite endpoint of all-cause mortality or HF rehospitalization was 25.2%, significantly outperforming the prespecified 45% benchmark based on contemporary medical therapy trials [43]. Mortality at one year was 13.9%, 30-day mortality was only 0.7%, and there were no intraprocedural deaths or conversions to surgery [43]. MR reduction was durable, with 96% of patients achieving mild or less MR at one year, accompanied by meaningful improvements in NYHA class (88% in class I-II at one year) and quality of life (mean +18-point KCCQ improvement) [43]. Rates of disabling stroke (3.9%), valve thrombosis (6.7%), and reintervention (6.4%) were notable but manageable within this high-risk cohort [43]. However, as a prospective single-arm study in patients unsuitable for surgery or MTEER without a randomized comparator group, the ability to draw definitive conclusions regarding comparative efficacy and safety is restricted. Additionally, the trial population was highly selected based on strict anatomical and clinical eligibility criteria, potentially limiting applicability to broader real-world cohorts of patients with MR. Larger studies with longer follow-up are required to better establish its long-term safety and efficacy.
Several additional TMVR systems are currently under clinical investigation, highlighting the rapidly evolving landscape. The AltaValve system (4C Medical Technologies, MN, USA) is a transapical or transseptal supra-annular TMVR device, designed to reduce the risk of LVOT obstruction by positioning the prosthesis above the mitral annulus, minimizing interaction with subvalvular structures [44]. In an early feasibility study and compassionate use series, 14 patients (mean age 77.9 years, 71% women, mean STS score 5.4%) with severe symptomatic MR, including those with atrial functional MR, were treated with AltaValve [45]. Eleven underwent transseptal and three underwent transapical implantation. The procedure achieved technical success and MR reduction to none/trace in all cases and there were no instances of LVOT obstruction [45]. At 30 days, all-cause mortality was 14%, and NYHA class III/IV symptoms were eliminated (reduced from 79% to 0%) [45]. Among surviving patients, 91% had no or trace MR and 9% had mild MR [45], supporting the feasibility of this supra-annular TMVR approach. Another feasibility study showed that the AltaValve TMVR system can be implanted safely and effectively, providing high procedural success, sustained MR reduction, and improved symptoms and quality of life over six months in high-risk patients unsuitable for surgery [46]. Clinical experience with AltaValve remains limited, however, and future studies are needed to assess long-term durability, thrombotic risk, and clinical outcomes beyond short-term follow-up.
The Cephea TMVR system (Abbott, IL, USA) is a fully percutaneous, transseptally delivered valve designed to accommodate a wide range of mitral anatomies using an atrial anchoring mechanism and a self-expanding nitinol frame. Its unique design avoids entanglement with subvalvular structures, aiming to minimize LVOT obstruction and paravalvular leak. A preclinical study has demonstrated promising feasibility and safety. In a chronic bovine model, surgical antegrade transatrial implantation showed excellent hemodynamic performance over 30–90 days, with stable valve position, minimal paravalvular leak, no LVOT obstruction, and favorable healing with no thrombosis or endocarditis [47]. Additionally, a dedicated transseptal delivery system was acutely tested in a porcine model, confirming accurate positioning and excellent immediate valve performance on echocardiography and autopsy [47]. These experimental results were followed by a first-in-human series involving three elderly patients (mean age 79 years) with severe PMR who were at prohibitive surgical risk and unsuitable for MTEER due to anatomic factors [48]. Successful transfemoral-transseptal valve implantation was achieved in all cases, with no procedural complications [48]. Post-implant, valve function remained normal with a mean gradient of 3 mmHg, no significant regurgitation, and no LVOT obstruction [48]. At 6-month follow-up, quality of life improved significantly, and imaging confirmed valve durability, geometric stability, and absence of structural deterioration [48]. An ongoing feasibility study (NCT05061004) along with additional evidence is, however, required.
The HighLife system (Highlife SAS, Paris, France) employs a dual-component design, combining a subannular ring delivered via the transfemoral arterial route with a valve prosthesis implanted transapically [49]. This configuration aims to enhance anchoring stability and reduce the risk of valve embolization. In a prospective, multicenter, nonrandomized feasibility study, 30 patients (mean age 75.6 years, 90% with secondary MR, median LVEF 43%) with moderate-to-severe or severe symptomatic MR underwent treatment with the HighLife TMVR system [50]. Technical success was achieved in 90% of cases, with device success at 30 days in 83% [50]. At 1-year follow-up, no mitral valve reinterventions were required, and MR was eliminated or reduced to trace/mild in all successfully implanted patients [50]. Importantly, the device demonstrated a favorable hemodynamic profile (mean mitral gradient 5.1 mmHg) with no LVOT obstruction (mean gradient 2.0 mmHg), supporting its safety and feasibility in this high-risk cohort [50].
MAC is a chronic, degenerative process characterized by progressive calcium deposition at the fibrous base of the mitral valve. It is prevalent in the elderly, with reported rates up to 40% in this population, and is strongly associated with cardiovascular risk factors, including chronic kidney disease, hypertension, and coronary artery disease [51]. Beyond being a marker of systemic atherosclerosis, MAC contributes directly to mitral valve dysfunction, and when severe, poses significant challenges to both surgical and transcatheter mitral interventions [51].
Surgical management of MAC-associated mitral disease is complex due to difficulties in annular decalcification, increased procedural risk, and elevated early mortality in frail or comorbid patients [52]. Transcatheter options, including mitral valve-in-MAC procedures using balloon-expandable aortic valves, have shown improvements in symptoms and hemodynamics but are limited by high mortality rates and strict anatomic eligibility, since only a small subset of MAC patients has suitable circumferential annular calcification for anchoring [53].
The advent of dedicated TMVR devices has opened new avenues for treating patients with severe MAC, many of whom are ineligible for MTEER due to poor leaflet quality or calcification in the grasping zone (Fig. 1).
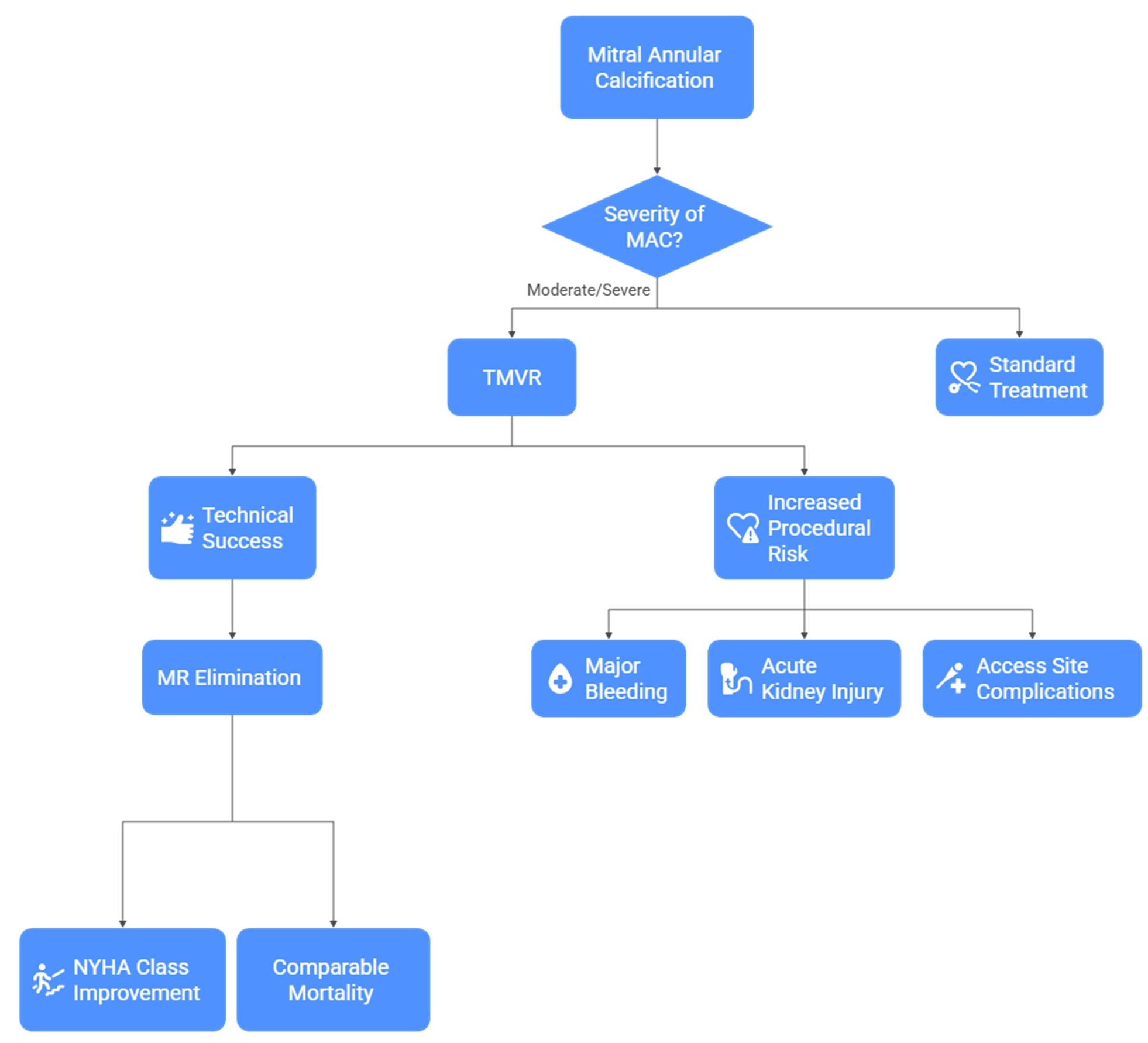 Fig. 1.
Fig. 1.
Decision pathway for the management of mitral annular calcification (MAC). This schematic outlines the clinical decision process in patients with moderate or severe MAC. In appropriately selected patients, TMVR can achieve high technical success and effective elimination of mitral regurgitation, leading to improvements in NYHA functional class and mortality comparable to alternative therapies. However, TMVR is also associated with increased procedural risks, including major bleeding, acute kidney injury, and access-site complications. TMVR, transcatheter mitral valve replacement; MR, mitral regurgitation.
In this context, the CHOICE-MI (Choice of Optimal Transcatheter Treatment for Mitral Insufficiency) registry offers critical insights into the feasibility of TMVR in patients with varying degrees of MAC [54]. In a recent analysis of 279 patients undergoing TMVR using eight dedicated devices, 57 patients (20.4%) had moderate or severe MAC. Despite higher baseline comorbidities, particularly extracardiac arteriopathy, patients with moderate/severe MAC had similar rates of technical success, MR elimination, and NYHA class improvement at 1 and 2 years compared to those with none or mild MAC [54]. Importantly, all-cause and cardiovascular mortality at 2 years were comparable between the groups [54]. However, the presence of moderate-to-severe MAC was associated with increased procedural risk, including higher rates of major bleeding (21.6% vs 8.8%), acute kidney injury (26.8% vs 8.2%), and access site–related complications [54]. These findings suggest that while MAC itself may not directly worsen long-term outcomes post-TMVR, it contributes to a more fragile procedural profile that is not currently captured by standard risk models. Given the rising prevalence of MAC and its overlap with aging and comorbidity, this study underscores the need for tailored transcatheter strategies, thorough preprocedural planning using advanced imaging, and ongoing device refinement. Recently, the SUMMIT-MAC trial showed that the Tendyne TMVR system can be safely and effectively implanted in high-risk patients with severe MAC, with high technical success and acceptable 30-day mortality [55]. At one year, most patients were free from death or heart failure hospitalization, and they experienced marked improvements in symptoms and quality of life [55]. Future randomized trials will be essential to establish evidence-based guidelines for this complex subset.
It should be noted that pre-procedural cardiac CT (CT) may assist in TMVR planning in patients with severe MAC. CT allows detailed assessment of the extent, distribution, and morphology of annular calcium, which determines the adequacy of the calcified landing zone for device anchoring and sealing [56]. Virtual valve implantation on CT is used to estimate the predicted neo-LVOT area, an important determinant of LVOT obstruction risk [56]. In addition to neo-LVOT measurements, CT helps evaluate the interaction between the prosthesis skirt and the calcified annulus, as sufficient circumferential contact between the valve skirt and calcium is required for anchoring and paravalvular leak prevention [56]. Implantation depth represents a key trade-off. Specifically, deeper ventricular positioning may improve sealing but increases the risk of LVOT obstruction [56]. However, a more atrial position may reduce LVOT compromise but predispose to paravalvular leak or device instability [56]. Furthermore, CT-based neo-LVOT prediction may be less accurate in Valve-in-MAC compared with valve-in-valve or valve-in-ring procedures because heavy calcification can alter the landing zone geometry and influence final device position [57].
Importantly, MAC does not uniformly represent a contraindication to TMVR. Rather, it should be considered a spectrum of anatomic risk. MAC may represent a relative contraindication when CT predicts severe LVOT obstruction, inadequate calcium for anchoring, or high embolization risk. Conversely, in selected patients, MAC may represent a modifiable procedural risk, particularly when CT planning demonstrates an adequate landing zone and when strategies to mitigate LVOT obstruction are feasible.
The decision-making process for selecting an appropriate transcatheter therapy in patients with significant MR is multifaceted and hinges on MR etiology, symptom burden, ventricular function, and procedural risk. Fig. 2 illustrates a simplified flowchart for therapy selection.
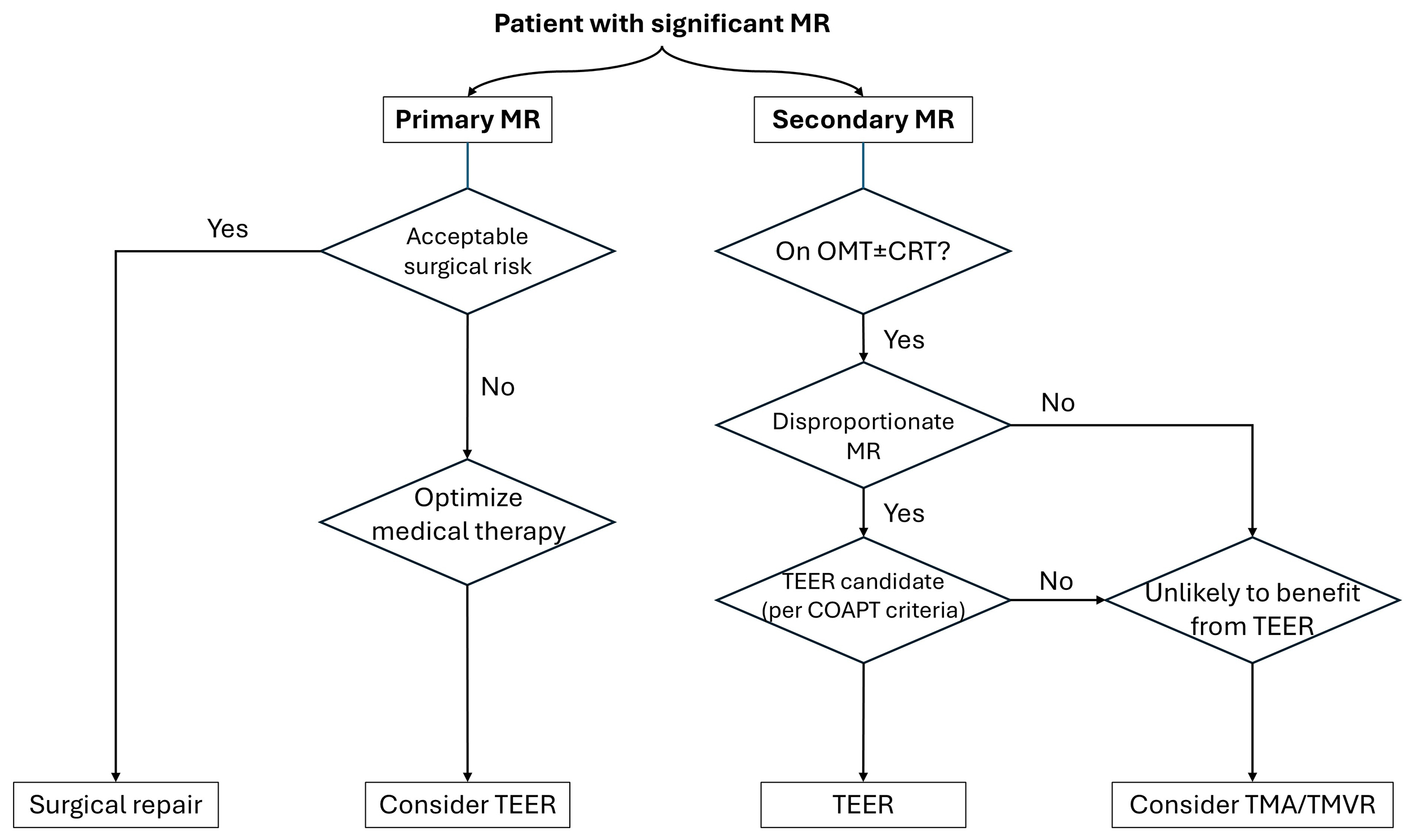 Fig. 2.
Fig. 2.
Selection algorithm for transcatheter mitral therapies. This flowchart outlines the decision-making pathway for patients with significant mitral regurgitation (MR), based on MR etiology (primary vs. secondary), surgical risk, medical therapy optimization, and anatomical considerations. MR, mitral regurgitation; MTEER, mitral transcatheter edge-to-edge repair; MAC, mitral annular calcification; OMT, optimal medical therapy; CRT, cardiac resynchronization therapy; TMA, transcatheter mitral annuloplasty; TMVR, transcatheter mitral valve replacement.
For patients with PMR, surgical repair remains the gold standard in those with acceptable operative risk. However, in high-risk or inoperable individuals, MTEER with devices such as MitraClip or PASCAL is a well-established alternative. Careful anatomical assessment is essential to confirm suitability for MTEER, including sufficient leaflet tissue, absence of prohibitive calcification, and favorable mitral valve geometry.
In contrast, SMR requires a nuanced approach. Initial management includes GDMT and, when indicated, CRT. In patients who remain symptomatic despite optimal medical therapy and demonstrate disproportionate MR relative to left ventricular dilatation (per COAPT criteria), MTEER has been shown to reduce hospitalization and mortality. Conversely, patients with proportionate MR or adverse valve anatomy may not derive benefit from MTEER and should be considered for alternative strategies such as transcatheter mitral annuloplasty or TMVR. Ultimately, all cases should undergo evaluation by a multidisciplinary heart team to ensure a tailored and evidence-based approach.
In patients with significant mitral annular calcification (MAC), treatment decisions require additional consideration, as extensive annular calcification may limit the feasibility of MTEER and influence the choice of TMVR. Careful pre-procedural CT assessment is therefore essential to evaluate anchoring stability and predict the risk of LVOT obstruction.
The rapid evolution of transcatheter therapies has substantially expanded treatment options for patients with significant mitral regurgitation who are unsuitable for surgery. From a clinical perspective, patient selection remains the most critical determinant of benefit. For secondary MR, optimization of guideline-directed medical therapy and device-based heart failure treatment remains the first step, with MTEER offering the most robust evidence of benefit in carefully selected patients with disproportionate MR and persistent symptoms. Annuloplasty-based approaches may provide an alternative strategy in selected patients with annular dilation and preserved leaflet mobility, while TMVR represents an important option for individuals with unfavorable anatomy for repair or recurrent MR after previous interventions. In clinical practice, these therapies should be considered complementary rather than competitive, with treatment decisions guided by detailed imaging assessment and multidisciplinary Heart Team evaluation.
Despite the promising results reported across transcatheter platforms, several limitations of the current evidence base should be acknowledged. First, most data for newer devices, particularly TMVR systems, derive from early feasibility studies, single-arm trials, or registries, often involving highly selected high-risk populations. Consequently, comparisons between different technologies remain indirect and susceptible to selection bias. Second, long-term durability and structural valve performance remain incompletely characterized, particularly for dedicated TMVR devices, where follow-up rarely exceeds one year. Third, uncertainties persist regarding optimal antithrombotic strategies and the incidence of valve thrombosis, an issue of particular relevance in transcatheter mitral prostheses due to their large prosthetic surface area and low-flow left atrial environment. Finally, procedural risk profiles, including LVOT obstruction, vascular complications, and bleeding, remain significant considerations that require careful preprocedural planning.
Future research should focus on several key areas. First, randomized trials comparing transcatheter strategies with optimized medical therapy or surgical intervention are needed to better define the role of newer technologies across different MR phenotypes. Second, studies evaluating head-to-head comparisons between repair and replacement strategies may help clarify the optimal treatment pathway for patients with complex mitral anatomy. Third, longer-term follow-up is essential to determine durability, valve thrombosis risk, and the need for reintervention after transcatheter mitral therapies. Advances in imaging-guided procedural planning, computational modeling, and device design are also likely to expand the anatomical eligibility for transcatheter interventions while reducing complications such as LVOT obstruction. Ultimately, continued integration of clinical trials, real-world registries, and device innovation will be essential to refine patient selection and establish evidence-based treatment algorithms for mitral regurgitation in the era of structural heart interventions.
Transcatheter interventions for MR have fundamentally transformed the management of both PMR and SMR in patients unsuitable for surgery. MTEER systems like MitraClip and PASCAL have demonstrated efficacy in well-selected patients, while annuloplasty and replacement technologies offer tailored alternatives for anatomically or clinically complex cases. As device iterations improve and randomized evidence accumulates, the landscape of MR therapy continues to shift toward a more individualized, anatomy-specific approach. Future studies comparing strategies head-to-head and clarifying optimal timing and patient selection will be key to maximizing outcomes in this evolving field.
PT: Conceptualization, Investigation, Visualization, Writing – original draft. PI: Investigation, Analysis, Writing – review and editing. KD: Conceptualization, Supervision, Writing – review and editing. PK: Investigation, Analysis, Writing – review and editing. PKV: Investigation, Writing – review and editing. ED: Investigation, Analysis, Writing – review and editing. KP: Investigation, Analysis, Writing – review and editing. AA: Supervision, Analysis, Writing – review and editing. CA: Analysis, Supervision, Writing – review and editing. KA: Analysis, Supervision, Writing – review and editing. DT: Analysis, Supervision, Writing – review and editing. KT: Analysis, Supervision, Writing – review and editing. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
Dimitris Tousoulis is serving as one of the Editorial Board members of this journal. We declare that Dimitris Tousoulis had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Chengming Fan. The remaining authors declare no conflicts of interest.
During the preparation of this work, the authors used ChatGPT-5.3 in order to check spelling and grammar. After using this tool, the authors reviewed and edited the content as needed, and take full responsibility for the content of the publication.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.