






 , Andrea Giuseppe Porto 2, Paolo Zappulla 3, Giuseppe Sgarito 4
, Andrea Giuseppe Porto 2, Paolo Zappulla 3, Giuseppe Sgarito 41 Division of Cardiology, Department of Internal Medicine, Section of Cardiac Electrophysiology, The Carver College of Medicine, University of Iowa Health Care Center, University of Iowa, Iowa City, IA 52242, USA
2 U.O.C. di Cardiologia con UTIC ed Emodinamica, Ospedale Cannizzaro, 95126 Catania, Italy
3 Divisione di Cardiologia, Azienda Ospedaliero Universitaria Policlinico “G.Rodolico - San Marco”, 95123 Catania, Italy
4 IRCCS ISMETT-UPMC Heart Center, Institute for Transplantation and Advanced Specialized Therapies, 90127 Palermo, Italy
Abstract
Cardioneuroablation (CNA) has emerged as a promising therapeutic strategy for functional bradyarrhythmias, particularly in cases of cardioinhibitory neurocardiogenic syncope and certain forms of atrial fibrillation. Indeed, by targeting vagal innervation through endocardial radiofrequency catheter ablation, CNA can obviate the need for pacemaker (PM) implantation. This technique involves denervation of specific vagal nerve structures within the atria to modulate autonomic balance and prevent symptomatic bradycardia. The efficacy of this approach stems from the recognition that an imbalance between sympathetic and parasympathetic tones, often characterized by excessive vagal activity, underpins these arrhythmogenic conditions. Indeed, CNA may be more effective than a permanent PM implantation in some patients, as this method addresses the underlying etiology rather than merely treating symptoms. Specifically, modulating autonomic nervous system (ANS) signaling through procedures such as CNA holds considerable promise for preventing and treating a range of cardiac arrhythmias. This review aims to synthesize current knowledge regarding various CNA techniques, exploring the associated mechanisms, clinical applications, and outcomes across diverse patient populations.
Keywords
- syncope
- sinus arrest
- atrioventricular block
- vasovagal syncope
- cardioneuroablation
Vasovagal syncope (VVS) is one of the most common forms of syncope, with a cumulative lifetime incidence estimated at 32% in men and 42% in women by age 60 [1]. It is triggered by an imbalance in the autonomic nervous system (ANS), characterized by increased vagal activity, which leads to bradycardia and/or peripheral vasodilation, ultimately causing transient cerebral hypoperfusion [2]. The clinical course of VVS is typically benign; however, up to 35% of patients experience recurrent episodes within a year, significantly impairing their quality of life and increasing the risk of injuries [3]. Standard management includes lifestyle adjustments, physical counterpressure maneuvers, and medications such as fludrocortisone or midodrine, which can carry several side effects, especially in young patients. Despite guideline-directed therapy (GDMT), about 20% of patients remain symptomatic [4]. Selected patients over 40 years of age who experience a prevalent cardioinhibitory form of VVS may benefit from dual-chamber pacemaker (PM) implantation [5, 6]. However, potential drawbacks associated with long-term device-related issues must be carefully considered.
Over the last two decades, cardioneuroablation (CNA) has emerged as a therapeutic option for functional bradyarrhythmias and cardioinhibitory VVS. This transcatheter ablation procedure targets the cardiac ANS by ablating to some extent the ganglionated plexi (GPs), which are clusters of intrinsic autonomic nerves predominantly situated in the epicardial fat pads of the atria. By doing so, CNA can suppress the vagal hyperactivity and restore autonomic balance [7, 8, 9]. Early clinical evidence suggests that CNA can provide promising results in carefully selected VVS patients with a prevalent cardioinhibitory response [7, 8, 10]. Nevertheless, several challenges remain unresolved, including the definition of optimal patient selection criteria and the establishment of standardized ablation protocols, which currently limit its broader application [11].
In this paper, we will review the existing CNA techniques for the treatment of cardioinhibitory VVS and functional bradyarrhythmias, starting from the cardiac ANS anatomical background. We will then report the outcomes of the most relevant studies, developments in the procedure, existing uncertainties, potential complications, and the future horizon of CNA.
The vast majority of studies published so far are observational, non-randomized, and open-label. The only available randomized controlled trial published in 2023 was not blinded and included a small population of 48 patients with highly symptomatic VVS (24 treated with CNA vs 24 treated with optimal non-pharmacological therapy). Syncope recurrence rate at 2 years was 8% in the CNA arm compared with 54% in the control arm (p = 0.0004), with an excellent safety profile with no procedural complications reported [12]. A recent single-arm meta-analysis published in 2025 included 28 studies (observational in the vast majority but including also the aforementioned randomized trial) with a total of 1153 patients (median age 39.6 years, 51.86% female sex) with VVS, where CNA’s potential efficacy was tested [13]. The baseline median number of syncope occurrences over the previous year was 3.8. The syncope recurrence rate after the CNA was 5.94% (95% CI 3.37–9.01) with a median follow-up of 21.4 months. Syncope recurrence at 12 months was 2.61% (95% CI 0.45–5.87). The syncope recurrence rate was higher among patients treated with right atrial (RA) GP ablation only than with biatrial ablation (15.8% vs 4.4%). Recurrences were also more frequent in those patients in whom the procedure used only an electroanatomical map (EAM) to target the GP, compared with the combination technique of EAM plus fractionated electrogram (EGMs) or EAM plus high-frequency stimulation (HFS), 8.33%, 5.14%, and 4.04%, respectively. Finally, the prevalence of CNA procedure complications was 0.99% (95% CI 0.14–2.33), with most of them represented by groin hematomas and rarely by pericardial issues. Similarly, in the 2024 European Heart Rhythm Association (EHRA) statement on CNA in VVS, 28 papers were analyzed, and CNA efficacy ranged from 73.2% to 100% [14].
In summary, CNA showed a potential value, especially for patients with VVS. However, the design and quality of available contemporary studies still prevent us from determining the definite net clinical benefit of CNA compared with current GDMT (pacemakers included). Specifically, CNA efficacy might be overestimated due to a placebo effect, elevated spontaneous remission rates of VVS, and effective pharmacological and non-pharmacological therapies in addition to the CNA procedures performed in the studies. Finally, potential CNA side effects, such as long-lasting inappropriate sinus tachycardia (described mainly in case reports) or a post-CNA proarrhythmic state, were not specifically addressed by the majority of the studies considered so far [10]. A sham trial is currently ongoing, evaluating RA CNA in patients with neuromediated syncope (NCT04755101).
The ANS is classically delineated into extrinsic (spatially distant from the
heart) and intrinsic (adjacent to the heart) components. Each of these systems
plays distinct yet interdependent roles in regulating cardiac function. The
extrinsic sympathetic system originates from preganglionic neurons in the spinal
cord (T1–T5), which synapse in cervical and thoracic ganglia, most notably the
stellate and middle cervical ganglia [15]. The resulting postganglionic fibers
form extensive innervation through the cardiac plexus, penetrating deeply into
the ventricular and atrial myocardium and endocardium, as well as the sinoatrial
(SA) and atrioventricular (AV) nodes. Norepinephrine acts via
- the right superior GP (RSGP), near the SVC–right superior PV (RSPV) junction and in close proximity to the interatrial septum. From this ganglion, most of the efferent parasympathetic fibers travel into the atria through the medial part of the SVC and the aortic root. The RSGP location is usually quite consistent among individuals, and this GP predominantly influences SA nodal function [22];
- the right inferior GP (RIGP), which modulates AV nodal conduction;
- the posteromedial left atrial GP (PMLGP), which is located on the posteromedial surface of the LA around the ostium of the CS and, like the RIGP, modulates the AV node function;
- the left superior (LSGP) and left inferior GP (LIGP), which exert mixed nodal effects;
- the Marshall tract GP (MTGP), which is associated with the ligament of Marshall containing cholinergic fibers.
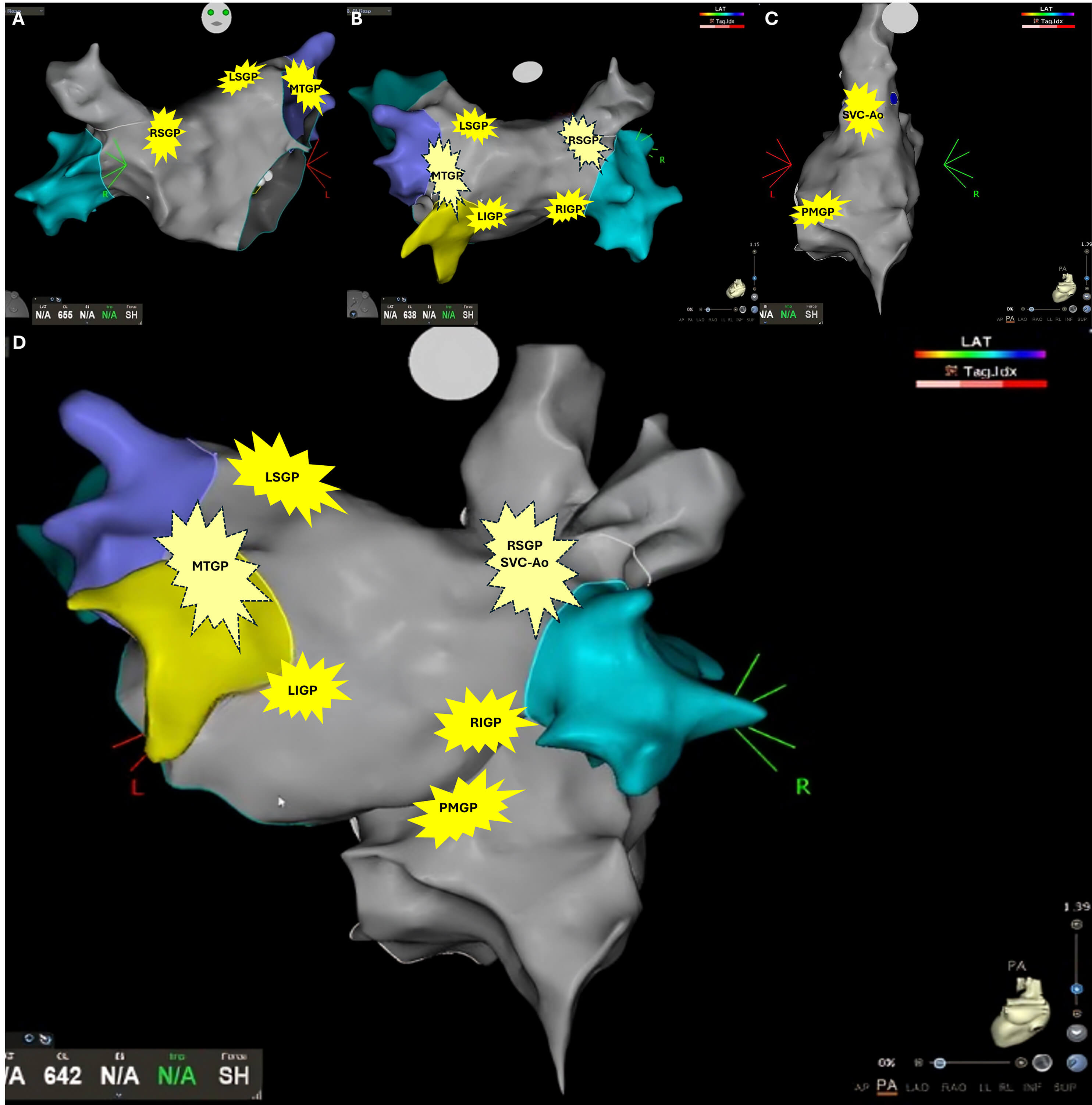 Fig. 1.
Fig. 1.
Schematic localization of ganglionated plexi (GPs). (A) Right anterior oblique visualization of the left atrium. (B) Posterior visualization of the left atrium. (C) Posterior visualization of the right atrium. (D) Combined posterior visualization of the left and right atrium. Legend: RSGP, right superior GP; LSGP, left superior GP; MTGP, Marshall tract GP; LIGP, left inferior GP; RIGP, right inferior GP; PMGP, postero-medial GP; SVC-Ao, superior vena cava – aortic GP.
All these GPs form an interconnected network that enables autonomic cross-communication and regulation [23]. The larger GP can contain up to 400 neurons [20]. The peculiar location of the ICNS on the epicardial side of the thin-walled atria, which typically measure 3–4 mm in thickness, makes it accessible by radiofrequency (RF) ablation. In particular, the RSGP, RIGP, and PMLGP can be reached by RF application from the RA without the need to access the LA. These anatomical and functional insights provide the foundation for CNA. By targeting and ablating these epicardial GPs via an endocardial approach, the procedure reduces excessive vagal outflow, thereby correcting the autonomic imbalance that is central to cardioinhibitory VVS and related bradyarrhythmias [14]. First developed in 2005 by Pachon and colleagues [7], CNA is a technique designed to selectively disrupt parasympathetic pathways while preserving, or even enhancing, sympathetic dominance, thus restoring autonomic equilibrium. Since parasympathetic fibers regenerate slowly, CNA can provide sustained relief in the long term. In contrast, sympathetic regrowth occurs more rapidly, resulting in a selective long-term suppression of parasympathetic activity.
Cardioinhibitory VVS and functional bradyarrhythmias are closely linked, both involving an overactive parasympathetic system causing bradycardia leading to syncope. Clinical characteristics are summarized in Table 1. The exact pathophysiologic mechanism of VVS is still unknown. Two main theories are described: (1) The “peripheral theory” and (2) The “central theory” [24]. In the “peripheral theory”, patients prone to excessive pooling of peripheral venous blood have a subsequent decrease in cardiac preload, stroke volume, and cardiac output. A reduction in blood pressure will activate the sensitive stretch baroreceptors in the blood vessel wall. Receptors that are under-stretched usually increase the sympathetic tone and diminish the parasympathetic activity. However, in VVS, the sympathetic tone is significantly reduced or abolished; therefore, heart rate and peripheral vasculature tone further decrease the cardiac preload. In volume-depleted ventricles, the myocardial contraction activates the ventricular mechanoreceptors (Bezold-Jarisch reflex), which are unmyelinated vagal afferent C-fibers. The final feedback response will send efferent parasympathetic signals to activate the postganglionic fibers, located in the para-cardiac GPs. In cardioinhibitory VVS, increased parasympathetic activity, combined with abolished sympathetic activity, reduces total peripheral resistance and cardiac automatism, leading to syncope from bradycardia, AV blocks, or sinus arrest. In the “central theory”, the reduction in the cerebral blood flow triggers the VVS symptoms. The cerebral blood vessels are innervated by regulatory mechanisms involving sympathetic and parasympathetic fibers, which decrease cerebral arteriolar vascular resistance to maintain brain perfusion when systemic blood pressure is reduced. In patients with VVS, a “paradoxical cerebral vasoconstriction” results from an increase in cerebrovascular resistance when systemic blood pressure decreases, leading to cerebral blood flow below the lower limit and syncope.
| Triggers | Prodromal symptoms | Sinus bradycardia | Atrioventricular block | Response to atropine | |
| Vasovagal syncope | Present. | Present. | Present during the episodes. | Present during the episodes. | Effectively treats cardioinhibitory VVS. Less effective in vasodepressor. |
| Prolonged standing, intense emotions/pain, medical procedures, excess heat, dehydration, bowel movements/urination, coughing. | Fatigue, warm feeling, profuse sweating, pallor, nausea, yawning, vision changes, and dizziness. | Precedes sinus pauses/arrest or asystole. | II-degree AVB, 2:1, or higher-degree AVB. | ||
| Hypervagotonic sinus node dysfunction | Usually not present. | Usually not present. | SNRT, SACT, and chronotropic response are typically normal. Evidence of paroxysmal sinus pauses, sinoatrial block, and sinus arrest. | Occasionally associated. | Increase in sinus rate |
| May be exacerbated by intense pain/emotions, intense physical activities, bowel movements/urination. | Symptoms reported during the bradycardia episodes: fatigue, weakness, shortness of breath, reduction in exercise capabilities, lightheadedness, dizziness, nausea, and syncope. | ||||
| Functional atrio-ventricular block | Usually not present. | Usually not present. | Occasionally associated. | Normal HV. | Resolution of AVB. |
| May be exacerbated by intense pain/emotions, intense physical activities, bowel movements/urination. | Symptoms reported during the bradycardia episodes: fatigue, weakness, shortness of breath, reduction in exercise capabilities, lightheadedness, dizziness, nausea, and syncope. | Transition from normal conduction to advanced AVB is usually preceded by bradycardia. |
AVB, atrioventricular block; VVS, vasovagal syncope; SNRT, sinus node recovery time; SACT, sinoatrial conduction time; HV, His-ventricular.
Functional bradyarrhythmias are a specific type of conduction disorder characterized by excessive parasympathetic activity, rather than by intrinsic or degenerative diseases affecting the SA or AV node. This excessive activity can lead to significant pauses in heart rhythm, sinus arrest, or atrioventricular block (AVB) (Fig. 2). The two primary forms associated with this mechanism are functional AVB and hypervagotonic sinus node dysfunction (SND). Traditionally, the standard treatment for severe bradyarrhythmias has been the implantation of a permanent PM. However, an increasing amount of evidence suggests that for carefully selected patients with a clear vagally mediated phenotype, CNA can effectively suppress harmful vagal reflexes, eliminate symptoms, and reduce the need for a PM in most cases. This approach has demonstrated a favorable safety profile and provides lasting symptom relief [14, 25, 26, 27, 28, 29]. This chapter will focus on the diagnosis and identification of suitable patients, which are essential for proper referral for CNA, and will critically evaluate the clinical outcomes associated with this treatment. Indications, diagnostic criteria, and expected outcomes are summarized in Table 2 (Ref. [14, 30, 31, 32, 33]).
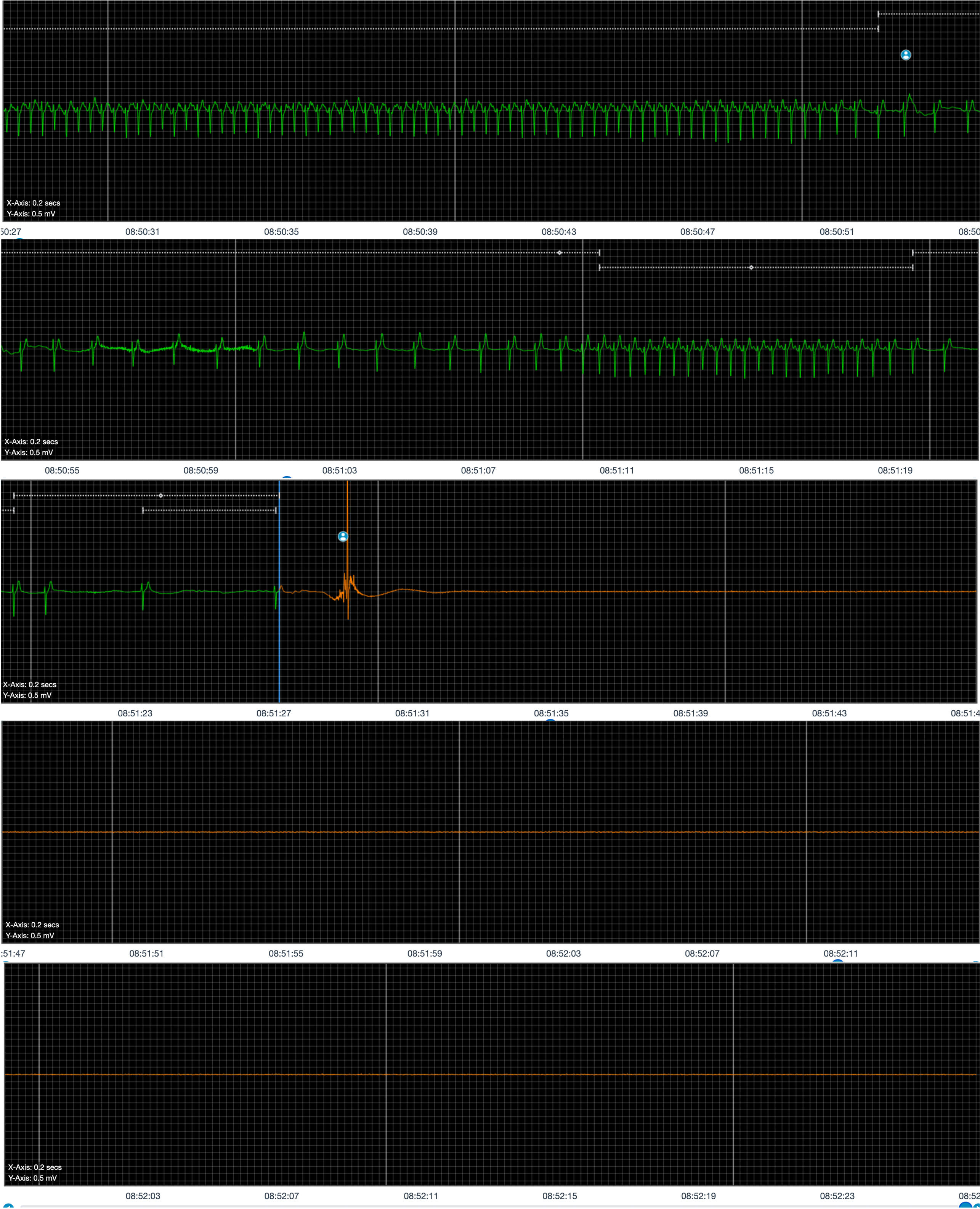 Fig. 2.
Fig. 2.
Monitoring of a patient with severe hypervagotonic sinus node dysfunction (SND).
| Indications | Diagnostic criteria | Expected outcomes | |
| Vasovagal syncope | Young patients ( May be considered as an alternative to pacing in patients aged |
At least one documented episode of spontaneous cardio-inhibitory VVS, ECG/Holter/ILR evidence of spontaneous asystolic syncope, or symptomatic |
The primary outcome is freedom from syncope or significant reduction in syncope recurrence. Secondary outcomes are currently based on periodical resting ECG, Holter ECG/ILR, and HRV evaluation. EHRA/HRS/APHRS/LAHRS Scientific Statement [14]. |
| AND | |||
| a positive response to atropine challenge ( |
|||
| Hypervagotonic sinus node dysfunction | Young and highly symptomatic intermittent or persistent sinus bradycardia documented on prolonged ECG monitoring/ILR with frequent, debilitating symptoms and impaired quality of life. | Intermittent or persistent sinus bradycardia on prolonged ECG monitoring/ILR, without typical. clinical history for cardio-inhibitory VVS, AND symptomatic cardio-inhibitory pauses |
Substantial increase in resting sinus rate, freedom from syncope, and avoidance of pacing. U.S. multicenter registry reported outcomes in the SND subgroup comparable to the overall cohort [33]. |
| AND | |||
| a |
|||
| Functional atrio-ventricular block | Young and highly symptomatic intermittent or persistent AVB documented on prolonged ECG monitoring/ILR with frequent, debilitating symptoms and impaired quality of life. | At least one syncopal episode and documentation of daytime second or third-degree AVB, | Atrio-ventricular conduction normalization, freedom from syncope, avoidance of pacing [30, 31, 32]. |
| AND | |||
| normalization of atrio-ventricular conduction during atropine challenge. |
CNA, Cardioneuroablation; ILR, implantable loop recorder; HR, heart rate; HRV, heart rate variability; EHRA, European Heart Rhythm Association; HRS, Heart Rhythm Society; APHRS, Asia Pacific Heart Rhythm Society; LAHRS, Latin American Heart Rhythm Society; SND, sinus node dysfunction.
Functional AVB typically occurs in young or middle-aged patients with
structurally normal hearts. These patients experience sudden, paroxysmal episodes
of high-grade or complete AVB that are fully reversible. Episodes often occur at
night, after meals, or are triggered by reflex syncope. They are frequently
accompanied by sinus slowing, indicating a strong vagal influence. Holter or
implantable loop recorder (ILR) monitoring typically reveals the sudden
transition from normal conduction to advanced AVB, followed by spontaneous
recovery. The atropine challenge is a reliable screening test for patients who
may benefit from CNA. A heart rate increase of more than 25% or exceeding 90
bpm, and/or resolution of complete AVB after atropine administration, strongly
suggests a vagally mediated mechanism (Fig. 3). Electrophysiological studies
(EPS) can help differentiate functional from intrinsic disease; a normal HV
interval (
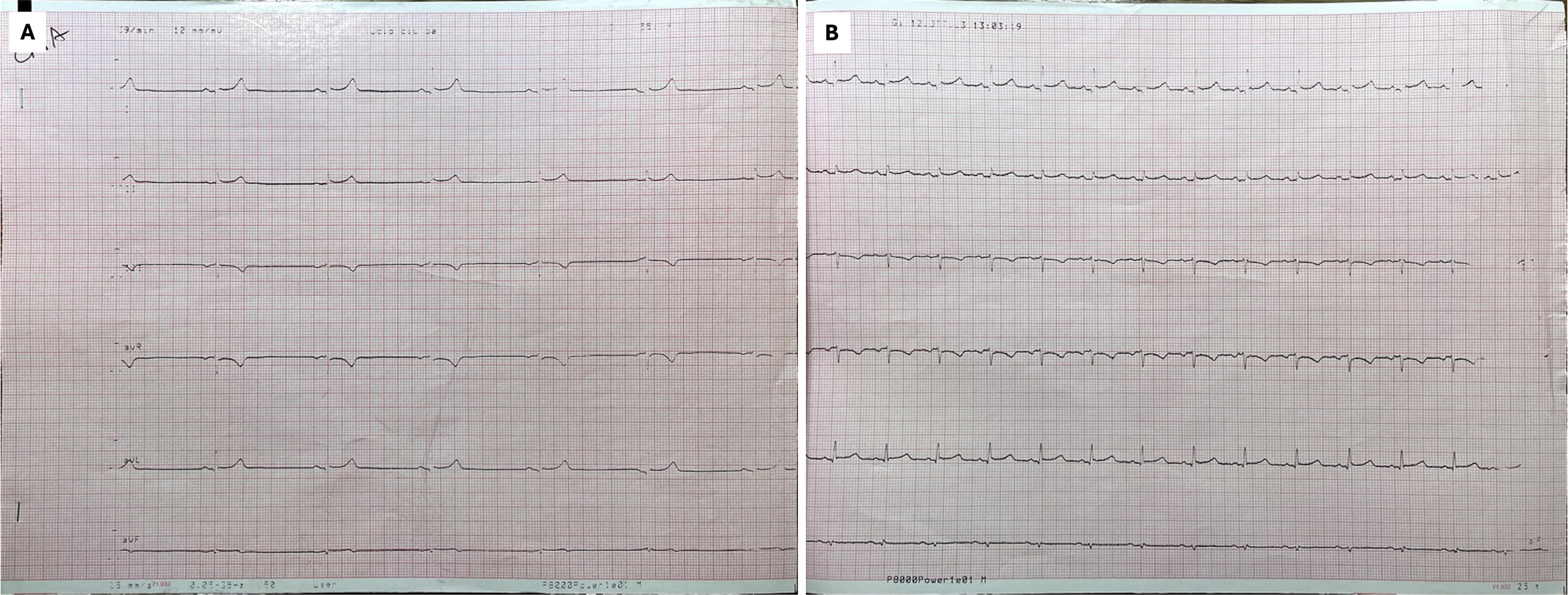 Fig. 3.
Fig. 3.
12-lead ECG before (A) and after (B) atropine challenge. A significant increase in heart rate is evident.
The early Brazilian experiences demonstrated that CNA can eliminate vagally mediated AVB and prevent syncope, achieving an acute procedural success rate of over 90%, enabling long-term PM avoidance in the majority of patients [7, 25, 26] (Fig. 4). These results have been confirmed in larger and more diverse cohorts. Aksu et al. [30] first described CNA as a therapeutic approach to functional AVB. In this population, they reported a substantial reduction in recurrence of functional AVB episodes after CNA during follow-up with avoidance of pacemaker [30]. Subsequently, the PIRECNA multicenter registry, which included 130 patients, reported an acute success rate of 96% and only a 14% recurrence rate of bradyarrhythmia at a median follow-up of ten months, with more than 85% of patients avoiding pacemaker implantation despite initial indications for it [31]. A single-center prospective cohort study conducted in China, involving 60 participants, reported a 95% acute success rate, approximately 10% recurrence at one year, and no major complications [34]. Additionally, mechanistic case series have shown that CNA can eliminate late functional AVB occurring after atrioventricular nodal reentrant tachycardia (AVNRT) ablation, with no reported recurrences during follow-up [32]. The largest contemporary dataset, a U.S. multicenter registry including 205 patients, documented an average increase of 20 bpm in resting sinus rate, 78% freedom from syncope, 97% avoidance of pacemaker implantation, and a major complication rate of only 1.4% at a median follow-up of 14 months [33].
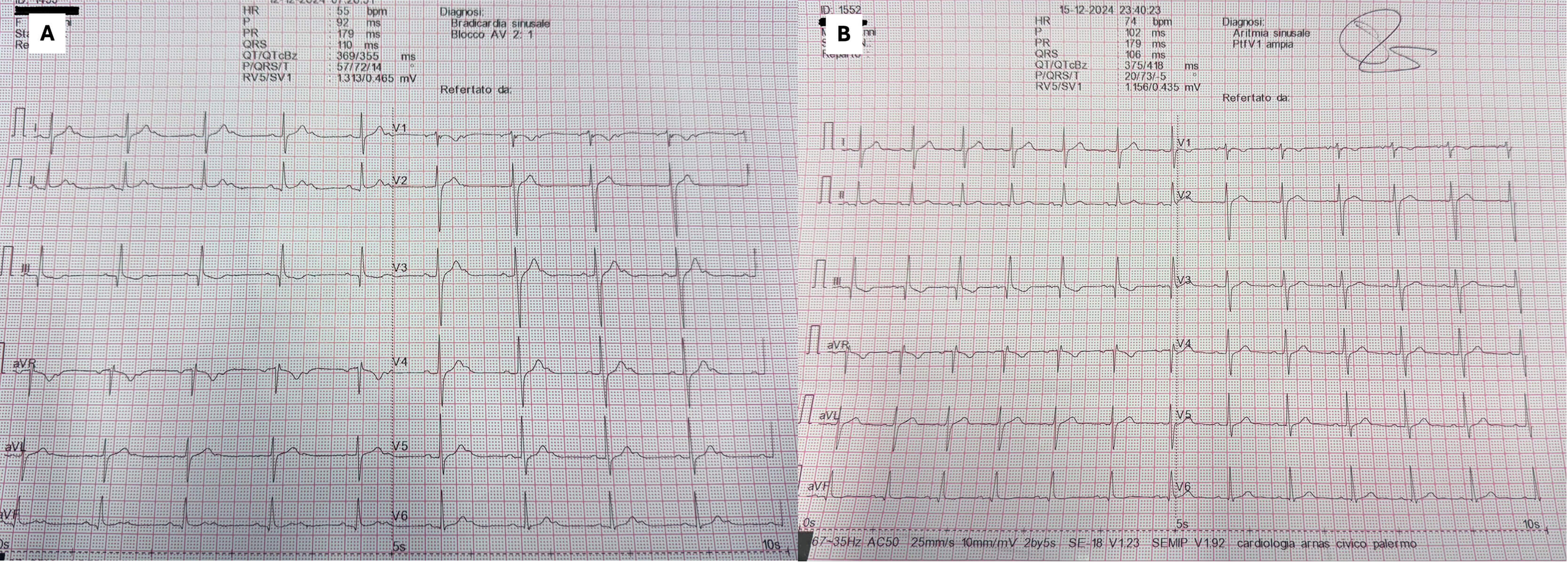 Fig. 4.
Fig. 4.
12-lead ECG of functional atrio-ventricular block before (A) and after (B) CNA.
The strength of these results is further supported by data on VVS, a disorder characterized by the same vagal mechanism. In VVS, a randomized controlled trial involving 48 highly symptomatic patients showed a two-year syncope recurrence rate of only 8% in the CNA group compared to 54% in the control group (p = 0.0004), and there were no procedural complications [12]. A recent meta-analysis of 28 studies with 1153 patients reported a pooled syncope recurrence rate of 5.94% (95% CI 3.37–9.01) at a median follow-up of 21 months, with a 12-month recurrence rate of 2.61% and a procedural complication rate of less than 1%, mostly consisting of minor vascular events. Outcomes were significantly better with biatrial ablation compared to right-sided-only procedures (recurrence: 4.4% vs 15.8%) and when combined anatomical and functional targeting was used, yielding recurrences of 4–5% compared to anatomical mapping alone (8.3%) [13]. The EHRA 2024 consensus statement corroborates these findings, citing the CNA efficacy of 73.2%–100% across published VVS series [14]. Although most comparative data derive from VVS, the shared vagal mechanism provides compelling indirect evidence that CNA can safely and effectively treat functional AVB, with high rates of acute success, durable symptom control, and very low complication rates, making it a viable alternative to permanent pacing in appropriately selected patients.
Hypervagotonic SND is a significant clinical concern in patients, particularly
young individuals who are otherwise healthy. This clinical entity overlaps with
patients with cardioinhibitory VVS. The diagnosis is based on clinical history
and can be confirmed by evaluating the sinus rate response to atropine infusion.
In the case of hypervagotonic SND, atropine infusion results in resolution of the
bradycardia. These patients often experience recurrent fainting spells or
prolonged pauses in their heart rate, which can occur during sleep or in reflex
situations, despite having normal sinus function at baseline and maintaining a
healthy chronotropic response outside of vagal episodes. Prolonged ECG monitoring
or ILR documentation of paroxysmal sinus arrest or severe bradycardia provides
diagnostic confidence. A positive atropine test and normal exercise chronotropic
response further support a vagal mechanism. EPS typically shows normal sinus node
recovery time (SNRT) and sinoatrial conduction time (SACT). Similar to AVB, HUT
can reveal cardioinhibitory pauses
Evidence supporting CNA in hypervagotonic SND has grown from early mixed cohorts, prospective series, multicenter registries, and mechanistic case reports. Although the literature is smaller than that for functional AVB, the direction and magnitude of benefit are remarkably consistent when a vagally mediated mechanism is rigorously documented. Initial mixed experiences indicated that targeting atrial GPs can restore sinus node function, resulting in high acute success rates and lasting symptom relief during follow-up, with most patients avoiding PM implantation [7, 25, 28]. Prospective single-center studies have confirmed these findings. When a hypervagotonic phenotype was rigorously validated—using ILR documentation of paroxysmal sinus arrest, a positive atropine test, preserved chronotropic reserve, and normal SNRT/HV intervals—the rate of acute success approached 95–100%. This was accompanied by significant reductions in pause burden and sustained freedom from syncope during mid-term follow-up [34]. The U.S. multicenter registry reported outcomes in the SND subgroup that were comparable to the overall cohort. The results showed a substantial increase in resting sinus rate (approximately +20 bpm), about 80% freedom from syncope, approximately 95–97% avoidance of PM use, and a major complication rate of about 1–2% at around 14 months [33].
In patients with structurally normal hearts and positive atropine responses, targeted denervation—often starting at the RSGP near the SVC/RSPV—resulted in immediate and sustained sinus acceleration, elimination of pauses, and maintained freedom from symptoms for 6–12 months [35]. Anatomical and neuromodulation studies support these observations, emphasizing the dense vagal innervation of the sinus node region and reinforcing the idea that strategic denervation at “gateway” plexi can restore autonomic balance in the sinus node.
Pediatric data, though necessarily limited, are particularly noteworthy. In pediatric patients with vagally mediated SND (some also exhibiting functional AVB), CNA achieved complete symptom resolution and PM avoidance after one year. Given the long-term risks associated with pacing in young patients (such as lead failure, infection, and the need for multiple generator replacements), these results are clinically significant and underscore the value of CNA when a hypervagotonic phenotype is clearly documented [36, 37, 38].
In hypervagotonic SND, the recurrence rate of bradyarrhythmia is generally low, around 10–20% over 1 to 2 years, and is often linked to autonomic reinnervation. While re-ablation may occasionally be necessary, most relapses are partial and can be managed without the need for PM implantation. Major complications are rare, occurring in about 1–2% of cases, with the most common functional side effect being inappropriate sinus tachycardia (IST), which is typically self-limiting or easily managed with medication [39]. Although there is a lack of randomized evidence specific to SND, we can cautiously infer from studies on VVS due to shared vagal physiology. A randomized controlled trial in VVS showed a two-year recurrence rate of syncope of 8% with CNA compared to 54% with standard care, with no procedural complications reported. Additionally, a meta-analysis of 28 studies involving 1153 patients indicated a pooled recurrence rate of approximately 6% over roughly 21 months and a complication rate of less than 1%. The analysis found that biatrial ablation and combined anatomical and functional targeting outperformed single-atrium or purely anatomical strategies [13]. Overall, these findings support CNA as an alternative treatment option for hypervagotonic SND, particularly in younger patients, for whom permanent pacing could pose long-term device-related risks.
We acknowledge that most data on CNA are from retrospective or prospective non-randomized studies. However, across all cohorts, CNA for cardioinhibitory VVS, functional AVB, and hypervagotonic SND demonstrates a favorable safety profile. Major complications are rare, with rates around 1–2% in large registries [33]. The most common functional adverse effect is IST, which arises from excessive vagal withdrawal; however, IST is typically self-limiting or can be effectively managed with medication. However, long-term burden, impact on quality of life, and its management are not fully explored. The potential risk of tachycardiomyopathy should be considered. However, CNA is not the only ablation procedure that may cause IST. Similarly, heart rate acceleration has been described in patients undergoing thermal AF ablation. It is not surprising because several areas where RF energy is delivered during PV isolation are the same as those ablated during CNA, especially at the anterior ridge of the RSPV. It has been shown that the extent of parasympathetic denervation after AF ablation is similar to that occurring after CNA, and several reports suggest the increase in sinus rate to be a good predictor of AF ablation efficacy. Nonetheless, no increase in the rate of complications associated with faster heart rate nor elevated risk of death following AF ablation has been reported so far, which is encouraging when the risk of IST after CNA is evaluated [40, 41].
Recurrence of bradyarrhythmia happens in about 10–20% of patients, often due to autonomic reinnervation. While some cases may necessitate repeat ablation, many can be treated conservatively. From a clinical standpoint, the most significant implication of CNA is its ability to prevent the need for permanent pacing in most appropriately selected patients. This is particularly beneficial for younger and pediatric populations, who might otherwise require decades of device therapy along with its associated risks [14]. These findings establish CNA as a safe and effective alternative to PM implantation when the vagal mechanism is clearly documented and intrinsic disease has been ruled out. Standardizing diagnostic criteria—such as tilt-test thresholds, atropine response, and ILR documentation—remains a priority. Additionally, randomized controlled trials are needed to confirm long-term efficacy and durability. Until such evidence becomes available, the current multicenter and meta-analytic data provide a strong foundation for recommending CNA to patients with well-documented vagally mediated bradyarrhythmias.
In their first report of CNA procedure, Pachon et al. [25] described an ablation procedure guided by standard electrophysiological parameters evaluation, such as reduction in SNRT, increase of sinus rate, reduction in Wenckebach’s cycle length (WCL), and the evaluation of the response to atropine administration at the end of the ablation. However, these measurements may often be unreliable, influenced by sympathetic and parasympathetic balance or by medication used during general anesthesia, muscle relaxation, or mild sedation. To overcome these limitations, Pachon et al. [42] introduced a technique called extracardiac vagal stimulation (ECVS). This method offers a more accurate measurement of the vagal effect before, during, and after CNA [2]. ECVS provides a systematic, stepwise, and objective assessment of the acute efficacy of CNA. To perform ECVS, a decapolar steerable electrode catheter is advanced under fluoroscopic guidance through the SVC and the internal jugular vein near the right or left jugular foramen, which is the location nearest to the vagus nerve. Stimulation is performed using a neurostimulator that delivers a pulsed electric field within the jugular vein. At baseline, ECVS causes sinus arrest and atrioventricular node (AVN) conduction block. After CNA, these effects disappear, confirming successful vagal denervation induced by the procedure. ECVS is currently the only reliable tool available to assess the acute efficacy of CNA. Recently, a prospective study with up to 5 years of follow-up demonstrated that ECVS-controlled CNA resulted in a 4-fold reduction in symptom recurrence compared with empirical CNA [43]. This approach provides a more objective, rational, and systematic assessment, allowing targeted treatment of three distinct vagal innervation territories based on clinical indications: the sinus node, AVN, and atrial walls. These territories or domains are somewhat independent, exhibiting different patterns of innervation and denervation. Characterization of these domains is performed with ECVS. Sinus node innervation (domain 1) is simply proved by applying ECVS, causing sinus arrest. AVN innervation (domain 2) is demonstrated by the induction of high-degree AVB caused by ECVS. Atrial wall innervation (domain 3) is also tested with ECVS, utilizing the Vagal AF Induction Test (VAFIT) protocol and measuring Effective Atrial Refractory Period (EARP) shortening. Depending on the specific clinical indication, CNA may target one or more domains, each with a unique topography. Typically, for cardioinhibitory VVS and carotid sinus syndrome, denervation of domains 1 and 2 is generally indicated. In hypervagotonic SND in the absence of AVB, denervation of domain 1 is selectively targeted. In cases of functional AVB, AVN denervation is prioritized (domain 2), which is evaluated with ECVS applied to the left vagus nerve. Using this technique, CNA proceeds incrementally to eradicate vagal effects in the designated region (domain), terminating upon confirmed efficacy to preclude over-ablation [44].
The impact of ECVS on the efficacy of CNA remains uncertain. Comparative data between ECVS and conventional electrophysiological (EP) parameters as endpoints for CNA are limited. No randomized, prospective studies have addressed this question; available evidence is restricted to retrospective observational studies, which may only generate hypotheses. Recent studies reported a trend toward improved outcomes with ECVS. When data are combined, ECVS appears to be associated with a higher rate of freedom from syncope recurrence (91% versus 82%) [29, 43, 45]. Published evidence suggests that ECVS is particularly valuable for patients with reflex syncope due to functional AVB, as ablation in these cases is typically more extensive, requiring a bi-atrial approach that includes the inferior septal GPs, CS, and regions near the left PVs, in contrast to patients experiencing isolated sinus pauses [46, 47].
Although Armour et al. [19] described possible anatomical locations of major atrial GPs in human postmortem specimens, precise localization during CNA remains essential for targeted and circumscribed ablation. Several mapping techniques have been used, including endocardial HFS, visual assessment of fractionated EGMs, and anatomical approaches with 3D-electroanatomical mapping systems [48]. Each method, however, has notable limitations.
The GPs mapping technique guided by fractionated EGM was initially described by
Pachon et al. [25], which identifies autonomic innervation areas by
highly fractionated atrial EGMs, while the surrounding atrial tissue shows normal
or less fractionated EGMs. Fast Fourier transform analysis categorizes the atrial
myocardium is classified into two distinct types: (1) “compact”
myocardium or normal atrial tissue, which displays dominant frequencies of
~40 Hz and a uniform spectral profile due to tightly
interconnected cardiomyocytes, and (2) “fibrillar” myocardium or
autonomic innervation areas, marked by fractionated EGMs, heterogeneous
conduction, and frequencies
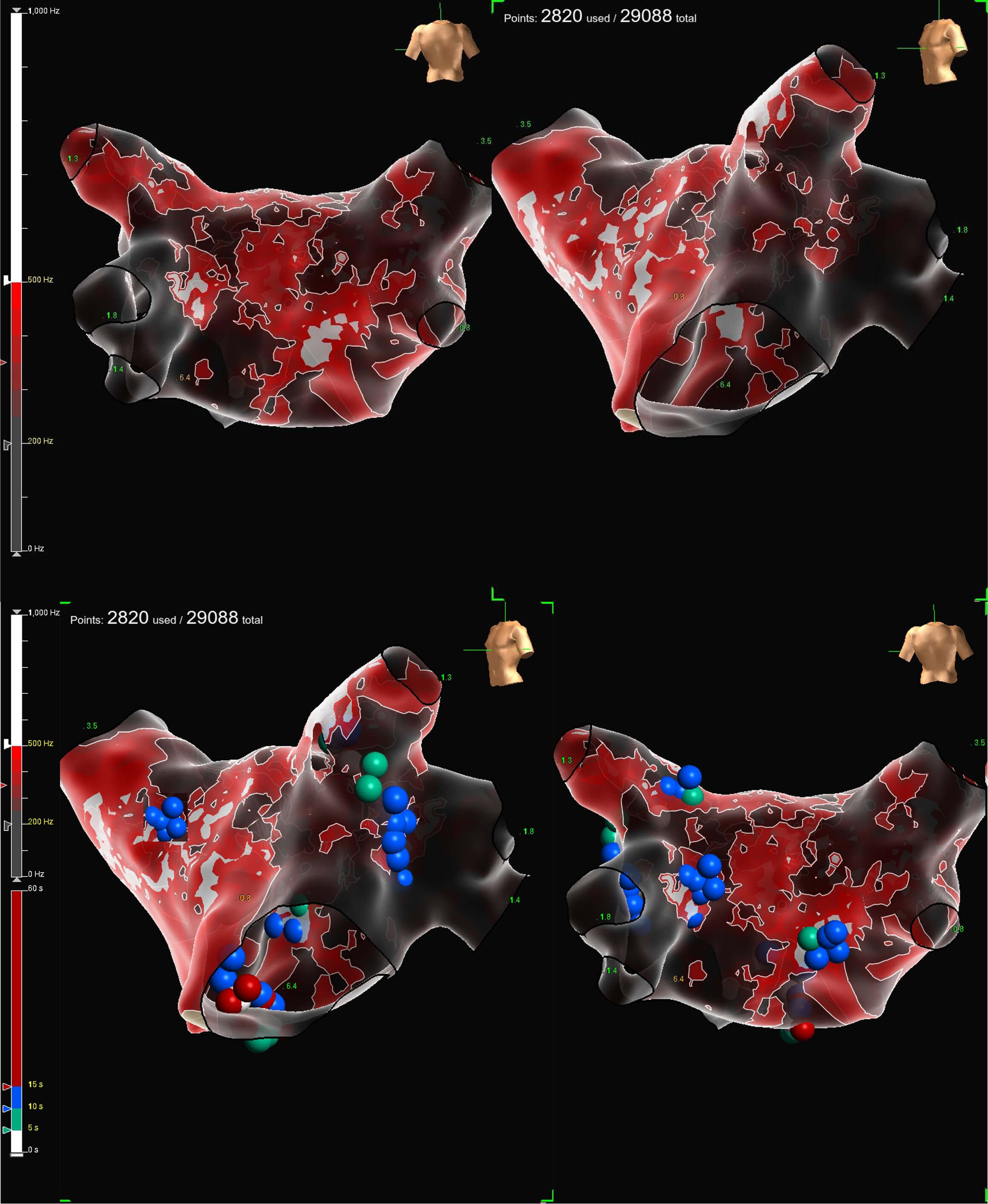 Fig. 5.
Fig. 5.
Fractionation EGMs map of the left atrium during cardioneuroablation (CNA). The use of Omnipolar Technology Near-Field (OTNF™) with peak frequency of 550 Hz (white areas) is useful to identify target region for ablation. Blue, green, and red dots represent the ablation lesions on the Left Superior GP, Marshall Tract GP, Left Inferior GP, Right Superior GP, and Right Inferior GP. Image from Conti S, Sgarito G. Omnipolar Technology Near Field to Evaluate Anatomic Location of Ganglionated Plexi During Cardioneuroablation. Clinical Case Reports, 2026; 14: e72311 [52].
Vagal response during radiofrequency delivery in the area of the left superior ganglionated plexus (LSGP). Video associated with this article can be found, in the online version, at https://doi.org/10.31083/RCM48106.
Additionally, the use of a different software to identify GP location has been
reported: the complex atrial fractionated electrograms (CFAE) software embedded
in the CARTO3 3D-electroanatomical mapping system (Biosense, Webster, Inc.,
Diamond Bar, CA, USA). The target signal was characterized by
To date, there are no studies demonstrating that any software is superior to the visual analysis of EGMs. Large, multicenter randomized studies are needed to confirm any advantages of different approaches.
In the past, anatomical studies have shown that most human atrial neurons are
located between the origins of the two vena cavae. Armour et al. [19]
identified ganglia on the posterior surface of the two atria and in the
interatrial septum, noting a particularly high concentration of atrial epicardial
GPs at the level of the Waterston’s groove. Since the 1990s, extensive studies
have been conducted to identify the intrinsic components of the cardiac ANS,
which include neurons situated on the epicardial surface, generally embedded
within the epicardial fat pads. The anatomy and physiology of the ICNS are still
being elucidated [20, 54, 55, 56]. However, it has been clearly demonstrated that
cardiac autonomic ganglia are organized into discrete epicardial regions, termed
GPs. Nerve fibers from these GPs directly innervate the SA and AV nodes, along
with numerous other atrial and ventricular areas [7, 35, 48, 54, 55]. Notably, while
GPs are primarily situated in the epicardium, extensive networks of afferent and
efferent nerve fibers are also present at myocardial and endocardial levels
[19, 20]. In aggregate, the human heart is estimated to harbour approximately
14,000 neurons within these ganglia [19]. Importantly, the autonomic innervation
of the SA node and AVN is distinct. This separation enables tailored ablation
strategies to address different types of cardio-inhibitory responses, such as
sinus arrest and functional AVB [57]. In particular, the junction between the SVC
and the septal aspect of the right superior pulmonary vein (RSPV) contains the
greatest density of epicardial GPs innervating the SA node [20, 58]. Differently,
the endocardial nerve fibers projecting from the epicardial GPs to the AVN are
smaller and less distinctly defined. The primary GP area, known as the
infero-septal GP, is typically situated in the pyramidal space between the CS
ostium and the septal side of the inferior vena cava (IVC) and right inferior
pulmonary vein (RIPV). Mechanistically, selectively ablating the septal GPs,
including the RSGP and the inferior-septal GP, is generally enough to obtain the
requisite denervation. This is consistent with clinical evidence indicating that
targeted ablation of the inter-atrial septal GPs adjacent to the right PVs
produces reliable vagal denervation of the SA and AV nodes [7, 59, 60]. The
anatomical approach to CNA has been reported by Rivarola et al. [61, 62],
reporting an efficacy of
In conclusion, ECVS, fractionated EGM analysis and mapping, and anatomical approach can be used as stand-alone techniques to guide CNA, or they can be integrated to increase the efficacy and safety of the procedure, since no method has demonstrated superiority in randomized comparative trials, and reproducibility and operator dependency remain key limitations.
The role of the ANS as a trigger for the initiation and maintenance of atrial fibrillation (AF) is well established. Coumel et al. [64] firstly reported in a small case series of 18 patients without structural heart disease who had recurrent paroxysms of AF and atrial flutter, which appeared to be initiated by sinus rate slowing and atrial coupling attributed to vagal overactivity. Derangements in sympathetic tone are also thought to play a central role in AF, possibly via cellular, structural, and electrical changes that occur in the setting of states of heightened adrenergic tone.
Several clinical trials have explored the use of GP ablation in the management of AF. As a stand-alone treatment strategy for AF, GP ablation success rates have been poor. In one study examining the long-term impact of GP ablation during a 3-year follow-up period showed that isolated GP ablation was associated with significantly lower rates of freedom from atrial arrhythmias without antiarrhythmic drug therapy when compared to circumferential pulmonary vein isolation (PVI) (34.3% versus 65.7%, p = 0.008) [65]. As an additional strategy to PVI, the results of these studies have been favorable, with decreased rates of AF recurrence when compared to PVI alone [66, 67]. However, there is no standardized method for performing these ablations. Several pooled analyses, including an RCT-only meta-analysis, showed that GP ablation as an additional strategy to PVI may be more beneficial in patients with paroxysmal rather than persistent AF [68]. It has been hypothesized that nerve regeneration and reinnervation post-ablation may limit the durability of GP ablation on freedom from AF. However, given that additional GP ablation plus PVI has been demonstrated to be more effective than PVI alone, the nerve regeneration hypothesis may not be universally true, or it may suggest that additional factors independent of nervous inputs may be involved in this population and warrant further investigation.
There is increasing enthusiasm in the cardiac electrophysiology community regarding CNA. However, there are several grey zones that need to be further evaluated. First, we have data from studies with relatively small sample sizes and short follow-up durations. Second, various techniques are utilized for CNA, which include targeting specific areas (right atrial, left atrial, or biatrial), employing different ablation strategies (anatomical versus GPs identification), and defining procedural endpoints. Interprocedural variability is likely due to different procedural investigations aimed at determining which patients benefit most from each approach. However, as the evidence base strengthens, it will be crucial to establish relatively standardized approaches and reach a consensus on both immediate and clinically significant long-term endpoints. This is particularly important for the design and interpretation of randomized controlled trial results.
Additionally, CNA results in significant attenuation of cardiac parasympathetic tone that manifests as increased mean HR and decreased heart rate variability (HRV) [25, 26]. Reduced HRV and low baroreflex sensitivity have been shown to predict mortality following a myocardial infarction, independently of conventional risk factors [69]. In cases of myocardial infarction, congestive heart failure, and left ventricular dysfunction, reduced HRV also predicts both sudden and non-sudden cardiac death [70]. Additionally, maintaining intact cardiovagal innervation may help reduce infarct size and the incidence of ventricular arrhythmias after myocardial ischemia [71]. Recent studies in animal models have demonstrated that the ablation of cardiac cholinergic neurons increases susceptibility to ventricular arrhythmias. This heightened risk is likely due to the suppression of the cardioprotective effects of vagal innervation following central nervous system damage [72]. Given the possible detrimental long-term effects of CNA, the possibility of placebo effects should also be addressed. In patients with VVS, parasympathetic overdrive is a transient phenomenon. The risk of extensive and unnecessary denervation to treat transient vagosympathetic imbalance cannot be overlooked.
Finally, there has been some discussion regarding the need for a randomized, sham-controlled, double-blind clinical trial to evaluate the true efficacy of CNA in VVS [73]. According to previous studies, patients with recurrent syncope may be prone to medical or device placebos. Permanent pacing was associated with a reduced risk of recurrent syncope in unblinded studies and in studies comparing different pacemaker algorithms. However, no significant effect was observed in double-blinded trials. Awareness of having a functional, permanent pacemaker was associated with a substantial “expectation” effect, which independently reduced the risk of recurrent syncope [74]. Indeed, a sham trial is currently ongoing, and it will provide more insight into the real effects of CNA (NCT04755101).
In addition to syncope recurrence and freedom from PM as outcomes of ongoing and future registries and trials, it will be necessary to include quality of life (QoL) measurements and patient-reported outcomes to further evaluate the efficacy and impact of CNA. Some findings suggest that CNA is related to an improvement in QoL in patients with VVS [11]. The CNA for the Management of Patients with Recurrent Vasovagal Syncope and Symptomatic Bradyarrhythmias (CNA-FWRD) Registry is a multicenter prospective registry evaluating acute and long-term outcomes of VVS and AVB patients treated by conservative therapy and CNA [75]. In this registry, data regarding the impact of syncope on QoL will be collected before and after CNA. The results of the CNA-FWRD registry, as well as other ongoing randomized studies (Efficacy of a Right-sided Ablation of the Anterior Ganglionated Plexus for Neurally Mediated Syncope (CardNMH3) - NCT04755101 - and Cardiac Ganglionated Plexus Ablation Before Permanent Pacemaker Implantation in Patients with Sick Sinus Syndrome (GAPS) - NCT04149886), are awaited to evaluate the long-term safety and effectiveness of CNA.
CNA is an emerging therapeutic approach for unpredictable and recurrent VVS with cardioinhibitory responses and for functional bradyarrhythmias. Multiple observational studies support lasting benefits in preventing recurrent symptoms and bradycardia. Ongoing studies will shed more light on the safety, efficacy, and long-term benefits of CNA.
SC and GS designed the research study. AGP and PZ collected and analyzed literature data. SC, AGP, and PZ drafted the manuscript. SC and GS reviewed the manuscript. All authors contributed to the critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
The authors would like to acknowledge Marco Riina, Giulia Scalia, and Giuseppe Giardina for the precious technical support.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.