







 , Lulu Zhu 1, Miaomiao Qi 1, Jing Yu 1,*
, Lulu Zhu 1, Miaomiao Qi 1, Jing Yu 1,*
1 Department of Cardiology, Lanzhou University Second Hospital, 730030 Lanzhou, Gansu, China
Abstract
Sex hormones play a critical role in the development of cardiovascular disease (CVD); however, the associations between specific circulating sex hormones and cardiovascular outcomes differ by sex, and the evidence remains inconclusive.
A systematic review and meta-analysis of 23 prospective cohort studies was conducted to examine the associations between sex hormones and cardiovascular outcomes. Hazard ratios (HRs) with 95% confidence intervals (CIs) were extracted, and random- or fixed-effects models were applied based on heterogeneity. Subgroup analyses were performed by hormone type, age, and sex.
In men, higher total testosterone (TT) levels were associated with a reduced risk of CVD. No consistent associations were found between sex hormone-binding globulin (SHBG), calculated free testosterone (cFT), and estradiol with CVD. In women, elevated TT and cFT were linked to increased CVD risk. Estradiol exhibited a modest and uncertain protective effect. An outcome-specific analysis revealed that higher dehydroepiandrosterone (DHEA) levels were linked to an increased risk of heart failure, while SHBG was associated with reduced cardiovascular mortality. Conversely, higher estradiol concentrations correlated with increased cardiovascular mortality.
Sex hormones exert complex, sex-specific, and outcome-dependent effects on cardiovascular risk. In men, higher testosterone levels are associated with lower overall CVD risk, whereas in women, these levels are linked to higher CVD and heart failure risk. Estradiol demonstrated a protective trend against major adverse cardiovascular events (MACEs), yet was linked to increased cardiovascular mortality. Higher SHBG levels are associated with lower cardiovascular mortality, whereas higher DHEA levels correlate with increased heart failure risk. Together, these findings underscore the importance of integrating sex, age, and endocrine context into cardiovascular risk stratification and prevention strategies.
CRD42024551055, Registration Link: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024551055.
Keywords
- gonadal steroid hormones
- cardiovascular disease
- sex factors
- androgens
- estrogens
- postmenopause
Cardiovascular disease (CVD) is the leading cause of morbidity and mortality globally, responsible for an estimated 17.3 million deaths annually, with projections indicating an increase to 23.3 million by 2030 [1, 2]. Historically, CVD has been considered predominantly a male-dominant disease. However, contemporary evidence reveals that women, particularly postmenopausal women, face a comparable or even greater cardiovascular burden than men. Sex hormones have emerged as independent modulators of cardiovascular health, potentially explaining these sex-related differences in risk [3].
Female-specific conditions, such as pregnancy-related complications, polycystic ovary syndrome (PCOS), and premature menopause, are significant contributors to elevated cardiovascular risk and adverse long-term outcomes [4, 5]. Premenopausal women typically show a lower incidence of CVD compared to age-matched men [6]. However, this protection diminishes or reverses after menopause, suggesting hormonal dysregulation as a critical mechanism. In response to these disparities, the American Heart Association (AHA) issued its first clinical guidelines for the prevention of CVD in women in 1999, marking an important milestone in raising awareness of sex-specific cardiovascular risk [7]. Despite these efforts, significant gender-based differences in risk factors and disease prevalence persist, highlighting the continued need for tailored prevention and treatment strategies.
Emerging evidence highlights the complex relationship between estrogen exposure and cardiovascular outcomes. In women, the severity of coronary artery disease (CAD) is more strongly correlated with the duration of the postmenopausal period and age at menopause than with chronological age [8, 9]. A 20-year cohort study further found an inverse association between age at menopause and CVD mortality, suggesting that later menopause is associated with a reduced cardiovascular risk [10]. These findings highlight the critical role of declining ovarian function and reduced estrogen levels in influencing postmenopausal cardiovascular risk. Although men generally experience an earlier onset of CVD, the cumulative lifetime risk ultimately converges between sexes.
Despite these insights, the effects of specific sex hormones on cardiovascular outcomes remain controversial. To address this gap, a systematic review and meta-analysis of prospective cohort studies was conducted to evaluate the relationships between sex hormones and cardiovascular outcomes, with a focus on gender-specific differences. This study aims to provide comprehensive evidence on the impact of sex hormones on CVD, informing strategies for precision prevention and management in both men and women.
This study adhered to the Meta-Analysis of Observational Studies in Epidemiology (MOOSE) protocol. The search strategy formulation, establishment of inclusion and exclusion criteria, and execution of statistical analyses were conducted following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [11, 12].
A comprehensive literature search was performed across the PubMed, Embase, Cochrane Library, and Web of Science databases, covering articles published from the year 2000 to 2025. The search utilized the following terms: (cardiovascular disease OR heart failure OR coronary artery disease OR heart disease) AND (estradiol OR estrogen OR androgen OR testosterone OR sex hormone OR dehydroepiandrosterone) AND (cohort study). This search strategy was designed to identify studies aligned with the predefined inclusion criteria, ensuring a thorough and systematic review of the literature (Fig. 1).
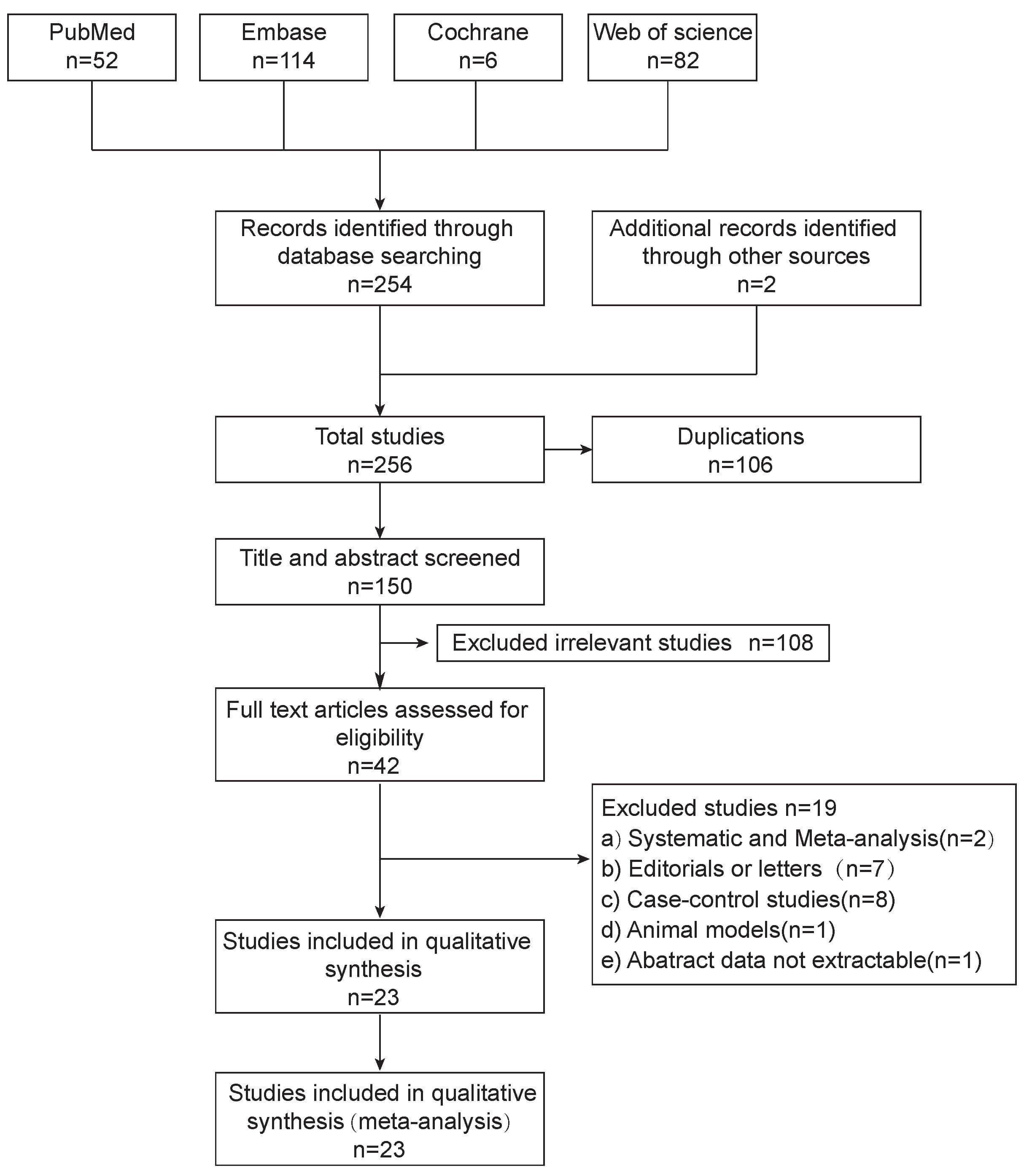 Fig. 1.
Fig. 1.
Flow diagram. Flowchart of study selection according to PRISMA guidelines.
Studies eligible for inclusion were retrospective or prospective cohort studies investigating the relationship between sex hormones and CVD. Hazard ratios (HRs) and 95% confidence intervals (95% CIs) of sex hormones’ impact on CVD were extracted. There was no restriction on the language of publication during the literature search; however, all 23 cohort studies meeting the predefined inclusion criteria were published in English, and no non-English original articles were ultimately included.
(a) Reviews, case reports, case-control studies, cross-sectional studies, letters, and other non-legible articles were excluded; (b) Studies that did not provide data suitable for meta-analysis were excluded.
In accordance with the PROSPERO-registered protocol, the primary analyses
pre-specified in this study involved evaluating the associations of total
testosterone (TT), calculated free testosterone (cFT), sex hormone–binding
globulin (SHBG), dehydroepiandrosterone (DHEA), and estradiol (E2) with overall
CVD risk, stratified by sex (female vs male) and age (
Additionally, several exploratory analyses were conducted to further investigate heterogeneity and generate new hypotheses. This included outcome-specific meta-analyses by CVD outcomes (heart failure, MACE, cardiovascular mortality, and all-cause mortality), subgroup analyses based on hormone assay technology, and pooled analyses restricted to postmenopausal women. These analyses were not pre-specified as primary hypothesis tests in the PROSPERO protocol, and their findings should be interpreted with caution, warranting further confirmation in future studies.
The title, primary author, publication year, region, mean age, sample size, study population, sex hormones exposure, sex hormones assay technologies, primary cardiovascular outcomes, duration of follow-up, HRs, and corresponding 95% CIs were systematically extracted and independently summarized by the principal investigator. HRs were preferentially extracted from models labeled by the authors as “fully adjusted”, “multivariable-adjusted”, or similar terms to minimize confounding (Supplementary Table 1). For studies using multiple assay methods or repeated hormone measurements, a single set of effect estimates is derived based on the baseline hormone levels or their own hormone categories. Therefore, “higher” versus “lower” exposure, relative to higher versus lower levels within each source population and assay system, and within-study standardized HRs were pooled rather than absolute hormone concentrations.
Stratification by menopausal status and age followed the grouping and reporting schemes of the original studies. Due to the lack of individual-level data on perimenopausal status and exact age at menopause, age and menopausal status could not be modeled as continuous variables. Studies in which menopausal status was unclear or included women with mixed menopausal status were uniformly classified as “mixed female populations”. The quality of all included cohort studies was assessed using the Newcastle–Ottawa Scale (NOS) [13] (Supplementary Table 2).
Heterogeneity across studies was assessed using Cochran’s Q (Chi-square) test,
alongside I2 and
Statistical analyses were conducted using R, version 4.4.1 (R Foundation for Statistical Computing, Vienna, Austria) with the meta package, ensuring a robust and standardized approach to data synthesis and interpretation.
A total of 23 studies, involving 8,068,754 participants (7,792,150 men and 276,604 women), were included in this meta-analysis. The mean age of male participants ranged from 46.98 to 76.3 years, while the mean age of female participants ranged from 31 to 74 years (Supplementary Fig. 1). The first author, publication year, mean age, region, sample size, follow-up duration, hormones exposure, and outcomes are summarized in Table 1 (Ref. [14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36]). Additionally, assay technologies and the quality assessment of the included cohort studies are provided in Supplementary Table 2.
| First author/Year | Mean age (years) | Region | Population/sex | Sample size | Follow-up (years) | Hormones exposure | Outcomes |
| Schederecker F, et al., 2020 [14] | Male (61.6) Female (63.1) |
Germany | Men and mixed female populations | 3080 | 8.7 | SHBG, TT, cFT, DHT, E2 | Cardiovascular mortality |
| Yeap BB et al., 2022 [15] | 58.0 (M) | United Kingdom | Men | 210,700 | 9 | TT, SHBG, cFT | MACE/Heart failure |
| Islam RM et al., 2022 [16] | 74.0 (F) | Australia | Postmenopausal women | 9180 | 4.5 | DHEA, TT, | MACE |
| Zhao D et al., 2018 [17] | 64.9 (F) | United States | Postmenopausal women | 2834 | 12.1 | TT, cFT, DHEA, SHBG, E2 | CVD/Heart failure |
| Collet TH et al., 2020 [18] | 72.4 (M) | United States | Men | 552 | 7.4 | TT, E2, SHBG | CVD |
| Meun C et al., 2018 [19] | 70.19 (F) | Netherlands | Postmenopausal women | 2578 | 11.36 | TT, SHBG, DHEA | CVD |
| Yeap BB et al., 2014 [20] | 76.2 (M) | Australia | Men | 12,203 | 7.1 | TT, cFT, DHT, E2 | Heart failure |
| Zhao D et al., 2020 [21] | Male (63.2) | United States | Men and Postmenopausal women | 8946 | 9.1 | TT, DHEA, SHBG | Heart failure |
| Female (62.8) | |||||||
| Wang A et al., 2021 [22] | 64.0 (F) | Sweden | Postmenopausal Women | 2848 | 19.2 | TT, cFT. SHBG | CVD/Heart failure |
| Pascual-Figal DA et al., 2009 [23] | 53.1 (M) | Spain | Men | 104 | 6.1 | SHBG | Cardiovascular mortality |
| Laughlin GA et al., 2010 [24] | 73.8 (F) | United States | Postmenopausal women | 639 | 12.3 | TT | CAD |
| Chen Y et al., 2011 [25] | 60.2 (F) | United States | Postmenopausal women | 99 | 19 | E2, SHBG | CAD |
| Yeap BB et al., 2021 [26] | 58.0 (M) | United Kingdom | Men | 149,436 | 11.3 | TT, SHBG, cFT | Cardiovascular mortality |
| Lim J et al., 2024 [27] | Male (56.32) | United Kingdom | Men and Postmenopausal women | 358,036 | 12.5 | TT, E2 | Heart failure |
| Tuorila K et al., 2024 [28] | 31/46 (F) | Finland | Pre-menopausal Women | 5889 | 22 | TT, SHBG, cFT | CVD |
| Harris K et al., 2023 [29] | Male (58) | United Kingdom | Men and Postmenopausal women | 479,797 | 12.5 | TT, SHBG, cFT | MI |
| Female (557) | |||||||
| Zhan X et al., 2024 [30] | 46.98 (M) | United States | Men | 6841 | 11 | TT | Heart failure |
| Hsu B et al., 2016 [31] | 76.9 (M) | Australia | Men | 1705 | 5 | TT, DHT, cFT, SHBG, E2 | Cardiovascular mortality |
| Chan YX et al., 2016 [32] | 50.3 (M) | Australia | Men | 1804 | 14.9 | TT, cFT, DHT, E2 | CVD |
| Shores MM et al., 2014 [33] | 76.3 (M) | United States | Men | 1032 | 9 | TT, cFT, DHT, | CVD |
| Ohlsson C et al., 2011 [34] | 75.4 (M) | Sweden | Men | 2416 | 5.1 | TT, SHBG, cFT, E2 | MACE |
| Khaw KT et al., 2007 [35] | 57 (M) | United Kingdom | Men | 1489 | 7 | TT | Cardiovascular mortality |
| Arnlov J et al., 2006 [36] | 56 (M) | United States | Men | 2048 | 10 | TT, DHEA, E2 | CVD |
Footnote: TT, total testosterone; SHBG, sex hormone-binding globulin; cFT, calculated free testosterone; E2, estradiol; DHEA, dehydroepiandrosterone; DHT, dihydrotestosterone; MACE, major adverse cardiovascular events; CVD, Cardiovascular disease; CAD, coronary artery disease; MI, myocardial infarction.
According to the pre-specified primary analysis plan, the association between
sex hormones and overall CVD risk in men was first quantified. Higher TT levels
were associated with a 9% reduction in CVD risk (HR = 0.91, 95% CI (0.84,
0.98)) (Fig. 2). Given the age-related variability in sex hormone levels, we
conducted subgroup analyses stratified by age (
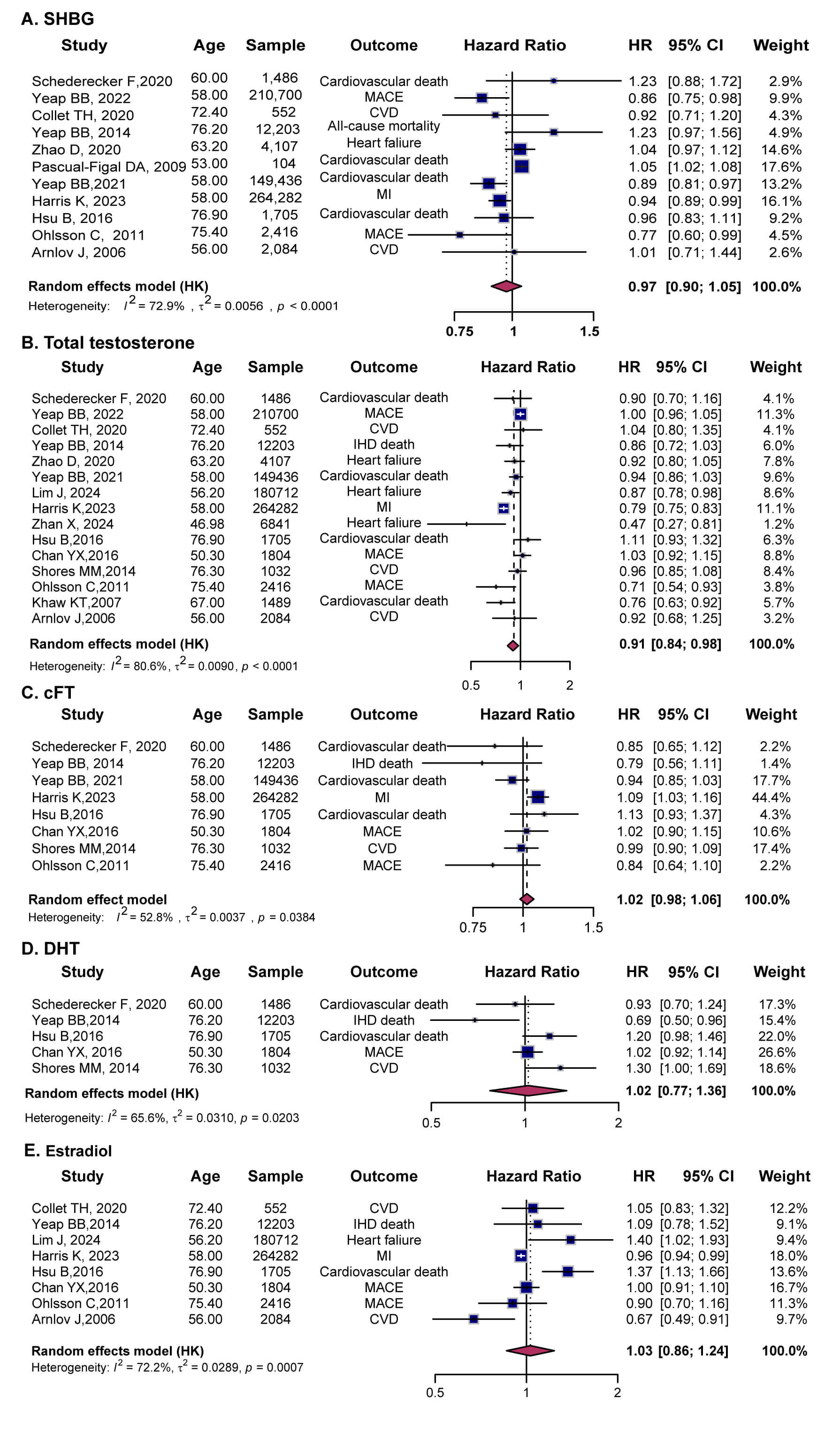 Fig. 2.
Fig. 2.
Forest plots showing the associations between sex hormones and cardiovascular outcomes in males. (A) SHBG, (B) TT, (C) cFT, (D) DHT, and (E) E2. Squares represent individual study HRs with 95% CIs, and diamonds indicate pooled estimates from random-effects models. SHBG, sex hormone-binding globulin; TT, total testosterone; cFT, calculated free testosterone; DHT, dihydrotestosterone; E2, Estradiol.
Ten studies evaluated the relationship between SHBG and CVD risk in men. The
pooled analysis showed no significant relationship (HR = 0.97, 95% CI (0.90,
1.05)), with moderate heterogeneity (I2 = 72.9) (Fig. 2A).
Age-stratified analysis revealed no significant association between SHBG and CVD
risk in either the
A pooled analysis of ten studies assessing the relationship between TT and CVD
risk indicated that higher TT levels were associated with a 9% reduction in CVD
risk (HR = 0.91, 95% CI (0.84, 0.98)), though with substantial heterogeneity
(I2 = 80.6) (Fig. 2B). Subgroup analyses confirmed consistent protective
associations across age groups, with TT reducing CVD risk by 8% in men
The pooled analysis of eight studies showed no significant association between cFT and CVD risk (HR = 1.02, 95% CI (0.98, 1.06)), with modest heterogeneity (I2 = 52.8) (Fig. 2C). Subgroup analyses stratified by age indicated that the association between cFT and CVD was consistent across age groups (Supplementary Fig. 2C). Additionally, meta-regression with 10-year age bands as a continuous moderator showed that age did not substantially modify the association between cFT and CVD (Supplementary Table 3).
Four studies examined the relationship between DHT and CVD. The pooled analysis found no significant association (HR = 1.02, 95% CI (0.77, 1.36)) (Fig. 2D). Although Yeap BB et al., 2014 [20] observed a 31% reduction in risk with higher DHT levels (HR = 0.69, 95% CI (0.50, 0.96)); the findings from the other three studies were not significant.
Eight studies assessed the association between E2 and CVD risk in men. The pooled results showed no significant association (HR = 1.03, 95% CI (0.86, 1.24)) (Fig. 2E). Age-stratified analyses revealed no clear association between higher E2 levels and CVD risk (Supplementary Fig. 2E). Consistent with this, meta-regression treating mean age as a continuous moderator showed that age did not significantly influence the E2 and CVD relationship (Supplementary Table 3). Furthermore, meta-regression with assay technology as a categorical moderator did not reach statistical significance; assay type accounted for approximately 22% of the heterogeneity (R2 = 21.8%). Overall, these results suggest a largely null association between estradiol and CVD risk, with some assay-related discrepancies between liquid chromatography–tandem mass spectrometry (LC–MS/MS)- and radioimmunoassay (RIA)-based measurements, which warrant confirmation in future studies (Supplementary Table 6).
According to the pre-specified primary analysis plan, a meta-analysis was conducted to pool the associations between each sex hormone and overall CVD risk in women. The pooled results indicated that higher TT and cFT were associated with a 10% (HR = 1.10, 95% CI (1.04, 1.16)) and 20% (HR = 1.21, 95% CI (1.10, 1.33)) increase in CVD risk, respectively. Additionally, higher E2 levels were associated with a borderline reduction in CVD risk (HR = 0.96, 95% CI (0.91, 1.00)) (Fig. 3).
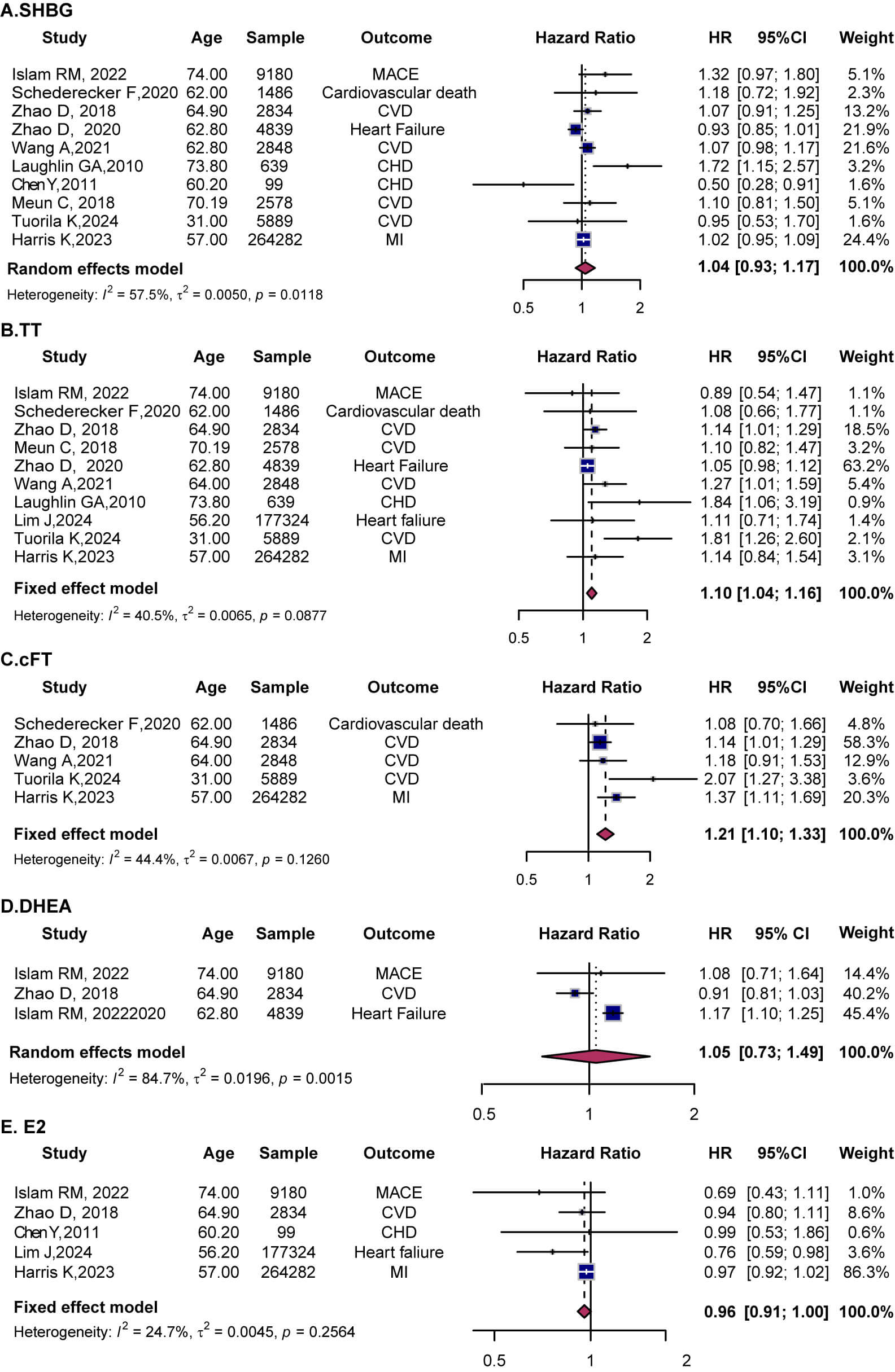 Fig. 3.
Fig. 3.
Forest plots showing the associations between sex hormones and cardiovascular outcomes in females. (A) SHBG, (B) TT, (C) cFT, (D) DHEA, (E) E2. HR with 95% CI are presented for each study (squares) and pooled estimates (diamonds) from random- or fixed-effects models. SHBG, sex hormone-binding globulin; TT, total testosterone; cFT, calculated free testosterone; DHEA, dehydroepiandrosterone; E2, estradiol.
Ten studies assessed the relationship between SHBG and CVD in women. In the
overall analysis, SHBG was not significantly associated with CVD (HR = 1.04, 95%
CI (0.93, 1.17)) (Fig. 3A), though substantial heterogeneity was observed
(I2 = 57.5). Age-stratified analyses showed no significant
associations in either subgroup (
The pooled results of ten studies demonstrated a significant association between
higher TT levels and increased CVD risk (HR = 1.10, 95% CI (1.04, 1.16),
I2 = 40.5) (Fig. 3B). Age-stratified analyses indicated elevated
risk in both older (
Five studies assessed the relationship between cFT and CVD risk in women. The
pooled results revealed a significant association with increased CVD risk HR =
1.21, 95% CI (1.10, 1.33), I2 = 44.4) (Fig. 3C). Subgroup analyses
confirmed elevated in both women
Three studies explored the association between DHEA and CVD risk in women. The pooled analysis found no significant association (HR = 1.05, 95% CI (0.73, 1.49)) (Fig. 3D). Additionally, five studies evaluated the role of E2 in female CVD risk. The pooled results suggested a borderline reduction in CVD risk (HR = 0.96, 95% CI (0.91, 1.00) I2 = 24.7) (Fig. 3E). Age-stratification analyses revealed no significant association between E2 levels and CVD risk in any age group (Supplementary Fig. 4D).
In exploratory outcome-specific analyses, the associations between sex hormones and heart failure, MACE, cardiovascular mortality, and all-cause mortality were assessed.
A random-effects meta-analysis was conducted to evaluate the associations of SHBG, TT, and DHEA with heart failure risk. SHBG was not significantly associated with heart failure (HR = 0.98, 95% CI (0.93, 1.03)), while high DHEA levels were significantly associated with an increased risk (HR = 1.11, 95% CI (1.06, 1.16)) (Fig. 4).
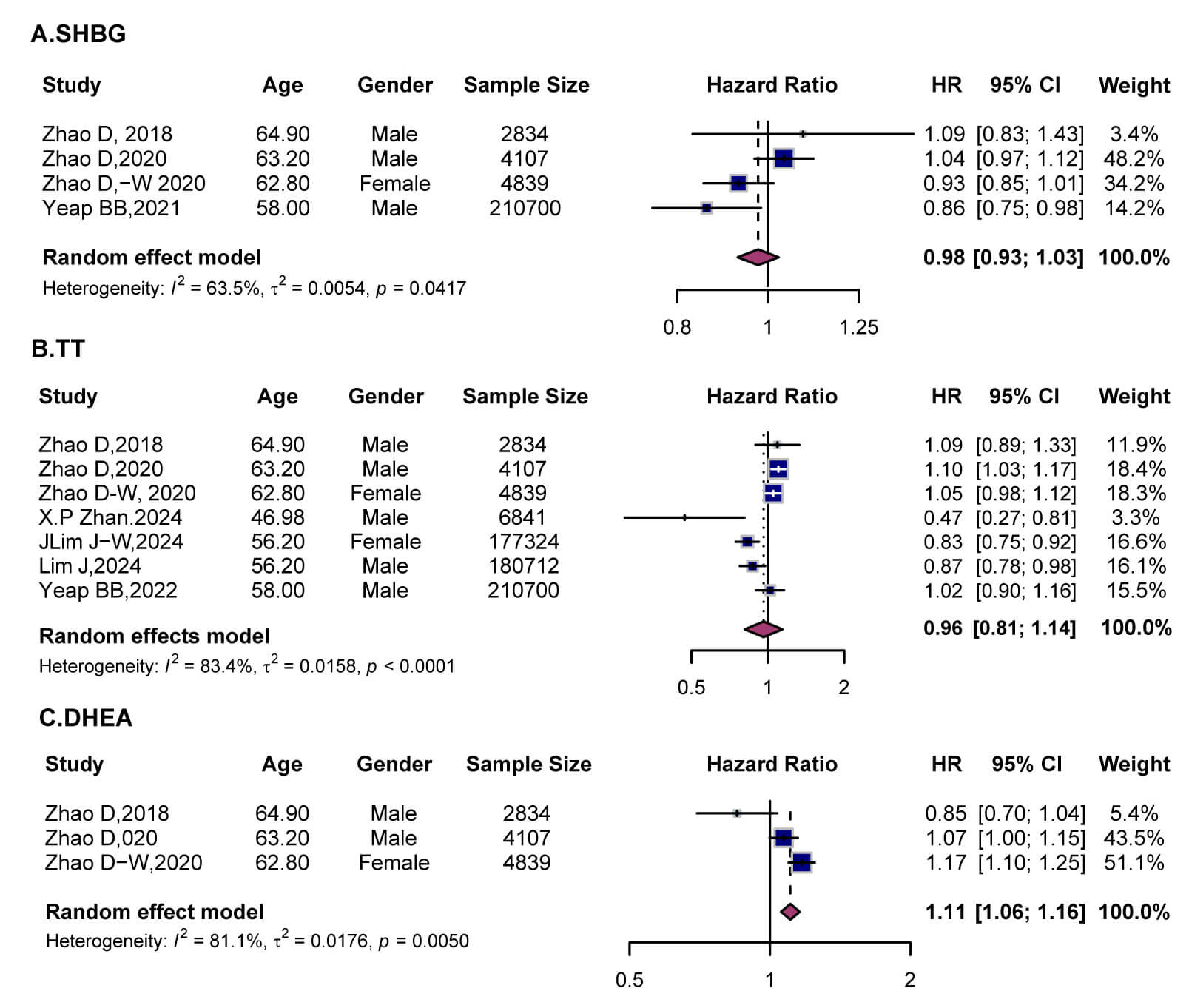 Fig. 4.
Fig. 4.
Forest plots showing the associations between sex hormones and the risk of heart failure. (A) SHBG, (B) TT, and (C) DHEA. Squares indicate HR with 95% CI for individual studies, and diamonds represent pooled estimates derived from random-effects models. SHBG, sex hormone-binding globulin; TT, total testosterone; DHEA, dehydroepiandrosterone.
For SHBG, the pooled analysis showed no overall association with heart failure (Fig. 4A). Subgroup analyses indicated a potential positive trend in women (Zhao et al., 2020 [21] and 2018 [17]), although the estimates were not statistically significant. In contrast, Yeap BB et al., 2021 [26] reported a protective effect (HR = 0.86, 95% CI (0.75, 0.98)). Sex- and age-stratified analyses revealed no significant effect modifications (Supplementary Fig. 6A and 7A).
For TT, pooled estimates in men showed no significant association with heart
failure (HR = 0.96, 95% CI (0.81, 1.14), I2 = 83.4) (Fig. 4B).
Only two studies were available for women, with inconsistent results
(Supplementary Fig. 6B). Notably, age-stratified analyses revealed an
apparent “age paradox”. In individuals
For DHEA, pooled results from three studies confirmed a significant positive association with heart failure (HR = 1.11, 95% CI (1.06, 1.16)) (Fig. 4C). Subgroup analyses revealed stronger effects in women (HR = 1.17) compared to men (HR = 1.07) (Supplementary Fig. 6C).
Meta-analysis of SHBG, TT, and E2 revealed heterogeneous associations with MACE
risk (Fig. 5). For SHBG, pooled results demonstrated no significant association
(HR = 0.98, 95% CI (0.94, 1.02)) (Fig. 5A). Subgroup analyses found no sex
differences (Supplementary Fig. 8A). Age-stratified analyses showed no
association in individuals
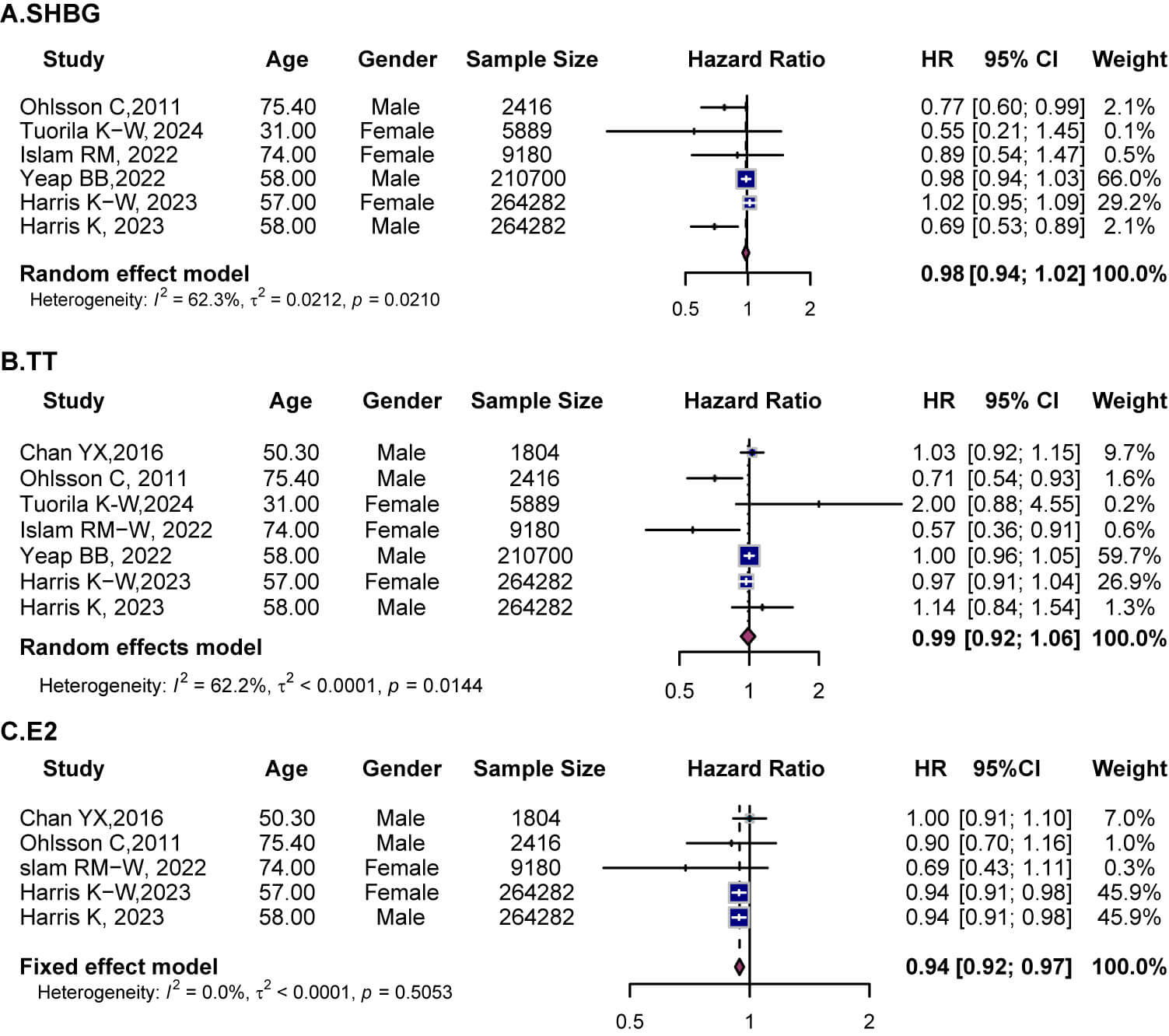 Fig. 5.
Fig. 5.
Forest plots showing the associations between sex hormones and the risk of MACE. (A) SHBG, (B) TT, (C) E2. Squares indicate HRs with 95% CI for individual studies, and diamonds represent pooled estimates derived from random-effects models. SHBG, sex hormone-binding globulin; TT, total testosterone; E2, Estradiol.
For TT, pooled analysis indicated no overall association with MACE (HR = 0.99,
95% CI (0.92, 1.06)) (Fig. 5B). Subgroup analyses found no sex differences
(Supplementary Fig. 8B). Age-stratified results showed neutral effects
in individuals those
For E2, fixed-effects analysis demonstrated a significant inverse association
with MACE (HR = 0.94, 95% CI (0.92, 0.97)) (Fig. 5C). Results were robust with
low heterogeneity. Protective effects were observed in both sexes (men, HR =
0.95, 95% CI (0.92, 0.98), women, HR = 0.94, 95% CI (0.90, 0.97))
(Supplementary Fig. 8C). Subgroup analyses indicated protection was
mainly present in younger individuals, while null associations were found in
those
The effects of SHBG, TT, cFT, DHT, and E2 on cardiovascular mortality were
examined (Fig. 6). The pooled result indicated that circulating SHBG levels were
not significantly associated with cardiovascular mortality (HR = 1.02, 95% CI
(0.92, 1.13)) (Fig. 6A). Sex-stratified analyses (Supplementary Fig.
10A) revealed largely null associations between SHBG and cardiovascular
mortality. Age-specific meta-analyses (
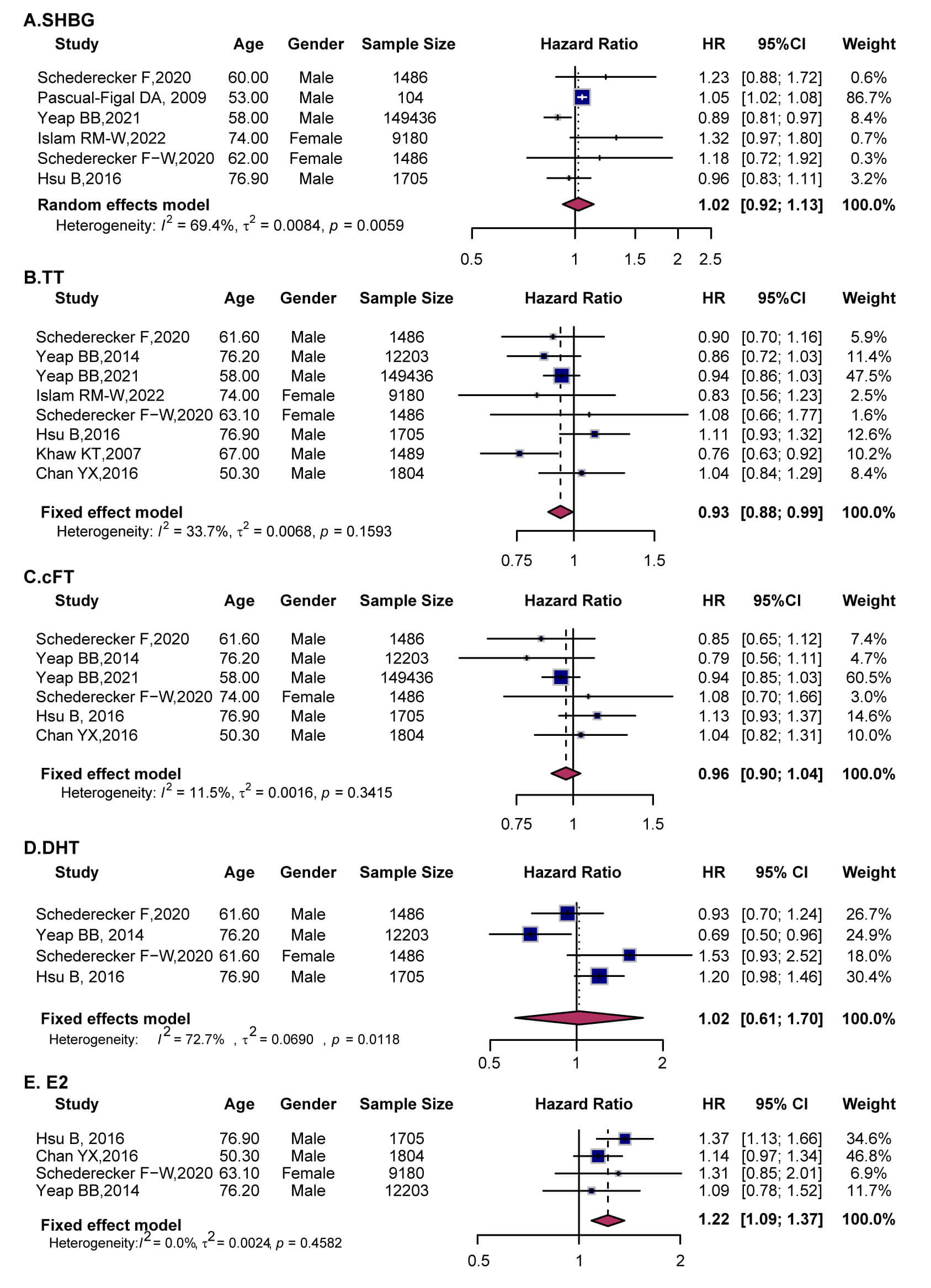 Fig. 6.
Fig. 6.
Forest plots showing the associations between sex hormones and the risk of cardiovascular mortality. (A) SHBG, (B) TT, (C) cFT, (D) DHT, and (E) E2. Squares indicate HRs with 95% CIs for individual studies, and diamonds represent pooled estimates derived from random-effects models. SHBG, sex hormone-binding globulin; TT, total testosterone; cFT, calculated free testosterone; DHT, dihydrotestosterone; E2, Estradiol.
TT was significantly associated with a lower risk of cardiovascular mortality (HR = 0.93, 95% CI (0.88, 0.99)), particularly in men (HR = 0.94, 95% CI (0.88–1.00)), with low heterogeneity (Fig. 6B). Although age-stratified analyses did not reveal a clear association between TT and cardiovascular mortality (Supplementary Fig. 11B), sex-stratified analyses showed that higher TT levels were associated with a lower risk of cardiovascular death in both men and women (Supplementary Fig. 10B).
cFT showed no significant association (HR = 0.96, 95% CI (0.90, 1.04)) (Fig. 6C). The finding suggests that cFT is not significantly associated with cardiovascular mortality, and no evidence suggests that age or sex substantially modifies this relationship.
DHT demonstrated no significant association (HR = 1.02, 95% CI (0.61, 1.70)), with high heterogeneity across studies (Fig. 6D). In contrast, elevated E2 was robustly associated with increased cardiovascular mortality (HR = 1.22, 95% CI (1.09, 1.37)) (Fig. 6E). Age-stratified analyses showed significant positive associations in middle-aged and older individuals (Supplementary Fig. 11E), while sex-stratified analyses demonstrated a robust excess risk in men (Supplementary Fig. 10E), with a similar, though less precise, pattern in women. Overall, these results suggest that elevated estradiol is a relatively stable risk marker for cardiovascular death, regardless of age and sex.
This study analyzed the associations of SHBG, TT, and cFT with all-cause mortality (Fig. 7). The pooled results showed no significant associations for SHBG (HR = 0.92, 95% CI (0.64, 1.32)) or TT (HR = 1.02, 95% CI (0.97, 1.07)), while higher cFT levels were significantly associated with an 8% increase in all-cause mortality risk (HR = 1.08, 95% CI (1.03, 1.12)).
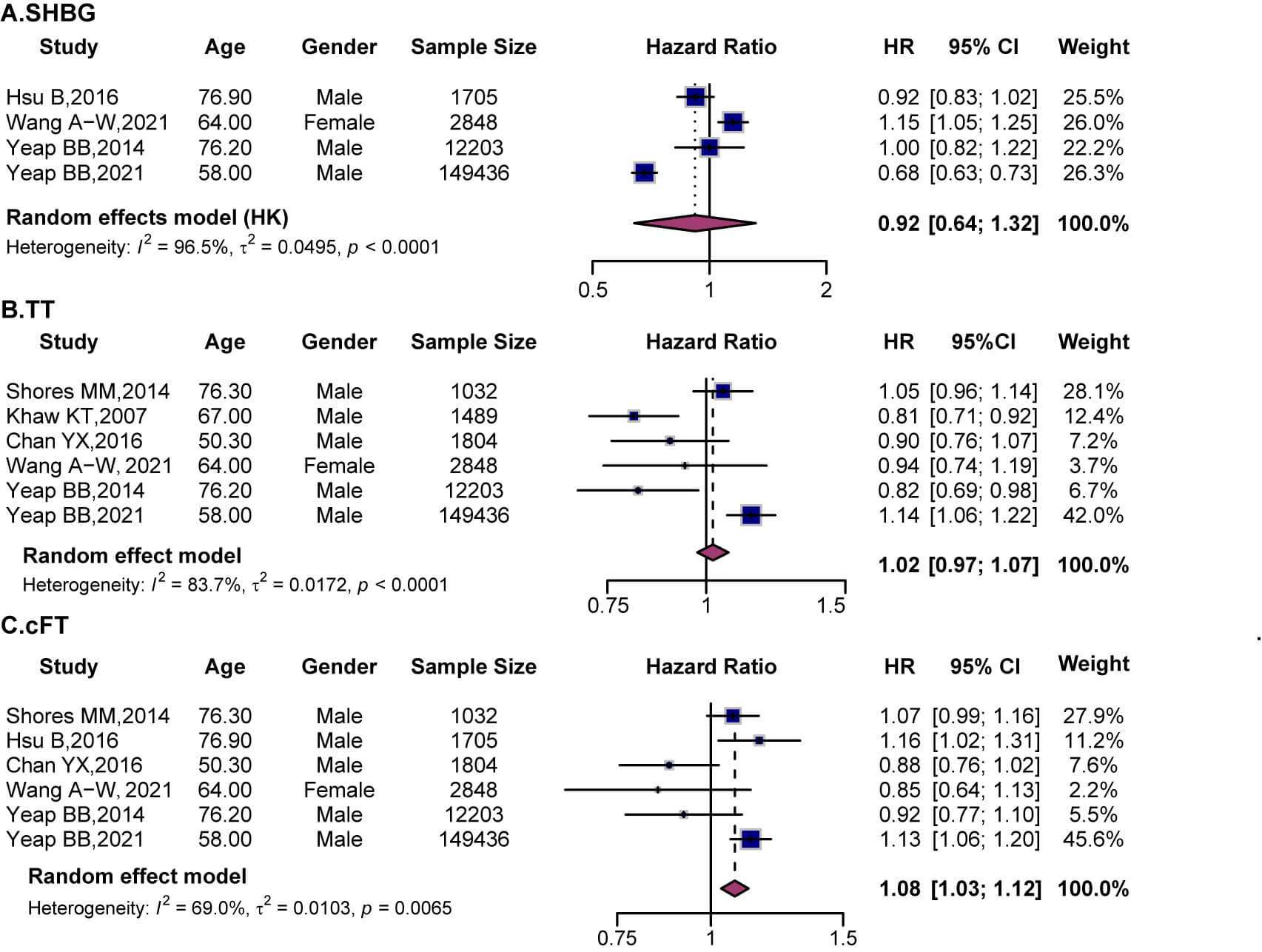 Fig. 7.
Fig. 7.
Forest plots showing the associations between sex hormones and the risk of all-cause mortality. (A) SHBG, (B) TT, and (C) cFT. Squares indicate HRs with 95% CIs for individual studies, and diamonds represent pooled estimates derived from random-effects models. SHBG, sex hormone-binding globulin; TT, total testosterone; cFT, calculated free testosterone.
The pooled analysis showed no significant association between SHBG and all-cause mortality (HR = 0.92, 95% CI (0.64, 1.32)) (Fig. 7A). Subgroup analyses revealed no significant differences by sex (Supplementary Fig. 12A) or age (Supplementary Fig. 13A), suggesting inconsistent and heterogeneous findings. TT also showed no overall association (HR = 1.02, 95% CI (0.97, 1.07)), although study results varied widely (Fig. 7B). Subgroup analysis by sex found no significant association in men (HR = 0.95, 95% CI (0.82, 1.09)), while only one study assessed women and reported no significant effect (Supplementary Fig. 12B). Age-stratified analyses showed no differences across older and younger subgroups (Supplementary Fig. 13B).
cFT was significantly associated with an increased risk of all-cause mortality (HR = 1.08, 95% CI (1.03, 1.12)) (Fig. 7C). Subgroup analysis indicated that elevated cFT was associated with increased all-cause mortality in men (HR = 1.08, 95% CI (1.04, 1.13)). These results suggest that higher cFT levels are linked to increased all-cause mortality risk, with a more pronounced effect in men.
Additionally, in postmenopausal women, the associations between sex hormones and CVD were evaluated through pooled analyses. As shown in Supplementary Fig. 14, SHBG (HR = 0.98, 95% CI (0.93, 1.03)) and TT (HR = 1.03, 95% CI (0.90, 1.20)) were not significantly associated with CVD risk. cFT showed a non-significant trend toward elevated CVD risk (HR = 1.03, 95% CI (0.86, 1.24)), while higher E2 levels were associated with a slight reduction in CVD risk, though not statistically significant (HR = 0.98, 95% CI (0.87, 1.10)). These results suggest that relative androgen excess, particularly elevated TT and cFT, may predispose postmenopausal women to increased CVD risk, while SHBG and E2 do not display clear protective associations.
This meta-analysis examined the associations between sex hormones and CVD risk, revealing notable sex-specific, age-dependent, and hormone type–specific differences. In men, higher TT levels were significantly associated with reduced CVD risk. This aligns with prior evidence linking low testosterone states to adverse health conditions, including type 2 diabetes [37], non-alcoholic fatty liver disease [38], CAD, and chronic obstructive pulmonary disease [39]. Low androgen levels may indicate overall frailty or systemic metabolic impairment [40]. In elderly men, both low TT and cFT independently predict cardiovascular events and mortality [40]. This observation is consistent with our finding that higher TT levels correlate with a reduced risk of cardiovascular mortality. Since low cFT often coexists with abnormal SHBG levels, this hormone pattern may exacerbate metabolic dysfunction and elevate CVD risk [41]. These data, together with the complex interactions among TT, cFT, and SHBG, emphasize the need for mechanistic and population-specific studies to distinguish causal effects from the impact of underlying metabolic frailty.
In women, the pattern is reversed. Elevated TT and cFT levels are significantly associated with an increased CVD risk. This sex divergence may reflect the loss of estrogen’s protective influence and the unopposed actions of androgens on vascular and cardiac remodeling [42, 43, 44]. Observational studies have shown that elevated TT is an independent risk factor for CVD and subclinical atherosclerosis in postmenopausal women [45]. Higher TT levels are associated with blood pressure variability and left ventricular hypertrophy [46]. However, the association between TT and CVD in postmenopausal women is not uniform [47]. Differences in population characteristics, including the prevalence of obesity and metabolic syndrome, may contribute to this heterogeneity [48]. Additionally, in postmenopausal women, the biological effects of androgens depend not only on total TT levels but also on SHBG and cFT, which together regulate androgen bioavailability [49, 50]. The relationship between TT and CVD risk is unlikely to be strictly linear and may involve threshold effects [24]. Such nonlinearity could partially explain the variability in both the strength and direction of the association across studies. Overall, these findings highlight a pronounced sex dependence in the relationship between TT and CVD risk.
SHBG, the primary transport protein for sex steroids, exerts complex, context-dependent effects. Low SHBG often coexists with obesity, insulin resistance, and dyslipidemia [51], all of which are well-established drivers of CVD [41]. Conversely, high SHBG, by lowering free testosterone, has also been identified as an independent predictor of CVD in certain male cohorts [40, 52]. In women, SHBG’s role is strongly influenced by estrogen. In premenopausal women with sufficient estrogen levels, elevated SHBG may serve as a marker of favorable metabolic health and exert indirect protective effects through mechanisms such as anti-inflammatory regulation [53] and improved insulin sensitivity [54]. However, in postmenopausal women with significantly reduced estrogen, high SHBG may further decrease bioavailable estrogen, thereby attenuating cardioprotective effects [19]. In metabolic disorders such as PCOS, low SHBG is a marker of disease severity and heightened CVD risk, further emphasizing its role as a regulator of metabolic and inflammatory burdens [55]. These observations suggest that the cardiovascular impact of SHBG and sex steroids must be interpreted within the broader context of endocrine-metabolic and therapeutic factors, rather than in isolation.
Recent data from hormone replacement therapy (HRT) trials support this context-dependent view. In postmenopausal women, the clinical significance of hormone concentrations is influenced by the surrounding endocrine–metabolic environment [56]. The associations between endogenous sex hormones and CVD risk observed in this study likely reflect the combined influence of hormone levels, obesity/metabolic phenotype, systemic inflammation, and HRT exposure [57]. Different HRT regimens and routes of administration also confer distinct cardiovascular and thrombotic risks [58]. These findings highlight the importance of considering the interactions among hormonal environment, metabolic status, and treatment exposure, and they caution against interpreting CVD risk based solely on serum sex hormone levels.
Elevated circulating DHEA showed no significant association with overall CVD risk, but was significantly linked to an increased risk of heart failure. DHEA, an adrenal-derived weak androgen that can be converted into more potent androgens, may have deleterious cardiovascular effects, including promoting cardiac hypertrophy [59, 60], driving adverse ventricular remodeling [61, 62], and inducing metabolic dysregulation [63]. The testosterone and DHEA may offer vaso-protective and anti-inflammatory benefits, but excessive or prolonged exposure can lead to mitochondrial dysfunction and maladaptive cardiac remodeling [64, 65]. These findings suggest that DHEA and testosterone exert a context-dependent “double-edged sword” effect on the heart. It should be noted that the specific mechanisms underlying this dual effect are inferred from and consistent with prior experimental and clinical studies. They are presented here as plausible mechanistic interpretations, rather than as conclusions directly demonstrated by the present meta-analysis.
Although estrogen is traditionally considered cardioprotective [66, 67], its effects appeared attenuated and heterogeneous in this study [68]. Overall, CVD and MACE are primarily composed of non-fatal myocardial infarction, non-fatal stroke, and coronary events requiring hospitalization, which typically represent earlier or intermediate stages of atherosclerotic disease. In these stages, moderately higher estradiol levels may offer protection by improving endothelial function, promoting vasodilation, optimizing lipid metabolism, and suppressing inflammation [69, 70, 71]. This aligns with the inverse associations between estradiol and overall CVD and MACE observed in women. In contrast, cardiovascular mortality is more often indicative of late-stage disease in older individuals with a high burden of comorbidities. Elevated estradiol levels are more likely to reflect an adverse endocrine–metabolic environment than a truly protective effect [72, 73]. Additionally, the cohort in the estradiol–MACE analyses was predominantly middle-aged to older individuals or early high-risk populations with mostly non-fatal events and relatively low heterogeneity. Differences in population characteristics and measurement methods across studies [74, 75] may further explain inconsistencies in effect estimates. Therefore, the apparently “protective” versus “harmful” associations of estradiol with cardiovascular outcomes likely reflect heterogeneous effects across different disease stages, outcome types, and metabolic–inflammatory contexts rather than contradictory biological actions.
Age emerged as a critical effect modifier. Associations between testosterone and
overall CVD risk were stronger in individuals
Notably, all associations observed in this meta-analysis are derived from observational cohort studies, and therefore cannot establish a causal relationship between sex hormones and cardiovascular outcomes. While multivariable models adjusted for age, conventional cardiovascular risk factors, and, in most studies, measures of adiposity and glucose metabolism were preferentially extracted, residual confounding due to obesity, insulin resistance, and related “metabolically unhealthy” phenotypes remains unavoidable. This is particularly relevant in postmenopausal women, where elevated androgens and reduced SHBG often reflect adverse metabolic states characterized by visceral adiposity, insulin resistance, and systemic inflammation—factors that themselves significantly contribute to increased cardiovascular risk.
In summary, this study reveals the multifaceted and outcomes-dependent roles of sex hormones in cardiovascular health. These findings highlight the need for future research and clinical practice to account for sex, age, and endocrine context, thereby enabling more precise cardiovascular risk stratification and individualized preventive strategies.
This study has several limitations. First, the included studies were highly
heterogeneous in terms of cardiovascular outcomes and sex hormone indices. While
no significant publication bias was detected for outcomes with
Third, this study included only cohorts with Newcastle–Ottawa Scale (NOS)
scores
Despite these limitations, this meta-analysis provides a relatively comprehensive synthesis of current evidence on sex- and age-specific associations between sex hormones and CVD. Future research should prioritize large, prospective cohort and interventional studies with standardized hormone measurement protocols and extended follow-up, in order to more accurately clarify causal relationships between the modulation of sex hormone levels—particularly hyperandrogenic states in postmenopausal women—and cardiovascular risk.
This meta-analysis demonstrates that sex hormones exert context-dependent effects on cardiovascular risk. Testosterone was associated with a lower risk of CVD in men but with a higher risk in women. Estradiol was associated with a reduced risk of MACE but an increased risk of cardiovascular mortality. SHBG and DHEA exhibited opposing effects, with higher SHBG levels associated with a reduced risk of cardiovascular mortality, while higher DHEA levels were associated with an increased risk of heart failure. These findings highlight the importance of incorporating sex, age, and endocrine context into cardiovascular risk assessment and prevention strategies.
All data generated or analyzed during this study are included in this published article and its supplementary information files. The raw datasets, original Western blot images, and additional experimental materials are available from the corresponding author upon reasonable request.
WW conceived and designed the study, collected the data, performed the statistical analyses, drafted the manuscript, and had overall responsibility for the reliability and integrity of the data and its interpretation. LZ conducted the literature search, extracted the data, and assisted with data analysis and figure preparation. MMQ provided methodological support, verified the data, and critically revised the manuscript for important intellectual content. JY supervised the study, obtained funding, and gave final approval of the version to be published. All authors contributed to the interpretation of the data, revised the manuscript, read and approved the final version, and agree to be accountable for all aspects of the work.
Not applicable.
We gratefully acknowledge the assistance and instruction from Chuyan Feng.
This study was supported by the National Natural Science Foundation of China (NSFC No. 81960086, 82160089, 82460086), the Key Incubation Project Funds of the Second Hospital & Clinical Medical School of Lanzhou University (No. 2025-21-zdfy-005 and 2025-24-zdy-003); and the Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital (No. CY2021-MS-A13 and CY2023-QN-A03). Additional support was provided by the Special Fund Project for Doctoral Training of Lanzhou University Second Hospital (No. YJS-BD-24), the International Science and Technology Cooperation Base (No. PR0124002), and the University Faculty Innovation Fund (No. 2024B-021).
The author declares that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
During the preparation of this work, the author used an artificial intelligence–based large language model tool (ChatGPT, GPT-5 mini) in order to polish the language and improve clarity and readability for an international audience. The tool was used solely for editing and optimizing the wording; it did not contribute to the study design, data collection, statistical analysis, or interpretation of the results. All scientific content was independently generated, verified, and approved by the authors, who take full responsibility for the accuracy and integrity of the manuscript
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/RCM47678.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.