



 , Yanhong Li 2, Wenjing Yao 2, Sijin Zhang 3, Sihan Chi 3, Yongtao Wang 4, Chen Wang 3, Yi Dang 2,*
, Yanhong Li 2, Wenjing Yao 2, Sijin Zhang 3, Sihan Chi 3, Yongtao Wang 4, Chen Wang 3, Yi Dang 2,* , Feifei Zhang 2
, Feifei Zhang 21 Department of Graduate School, North China University of Science and Technology, 063210 Tangshan, Hebei, China
2 Department of Cardiology Center, Hebei General Hospital, 050051 Shijiazhuang, Hebei, China
3 Department of Graduate School, Hebei Medical University, 050017 Shijiazhuang, Hebei, China
4 Department of Graduate School, Hebei North University, 075000 Zhangjiakou, Hebei, China
Abstract
The peri-coronary fat attenuation index (FAI) is a novel imaging biomarker of inflammation. This study aimed to investigate the association between combination therapy with sodium–glucose transporter 2 inhibitors (SGLT-2i) and glucagon-like peptide-1 receptor agonists (GLP-1RAs) and coronary artery inflammation, as assessed by the peri-coronary FAI, in patients with type 2 diabetes mellitus (T2DM).
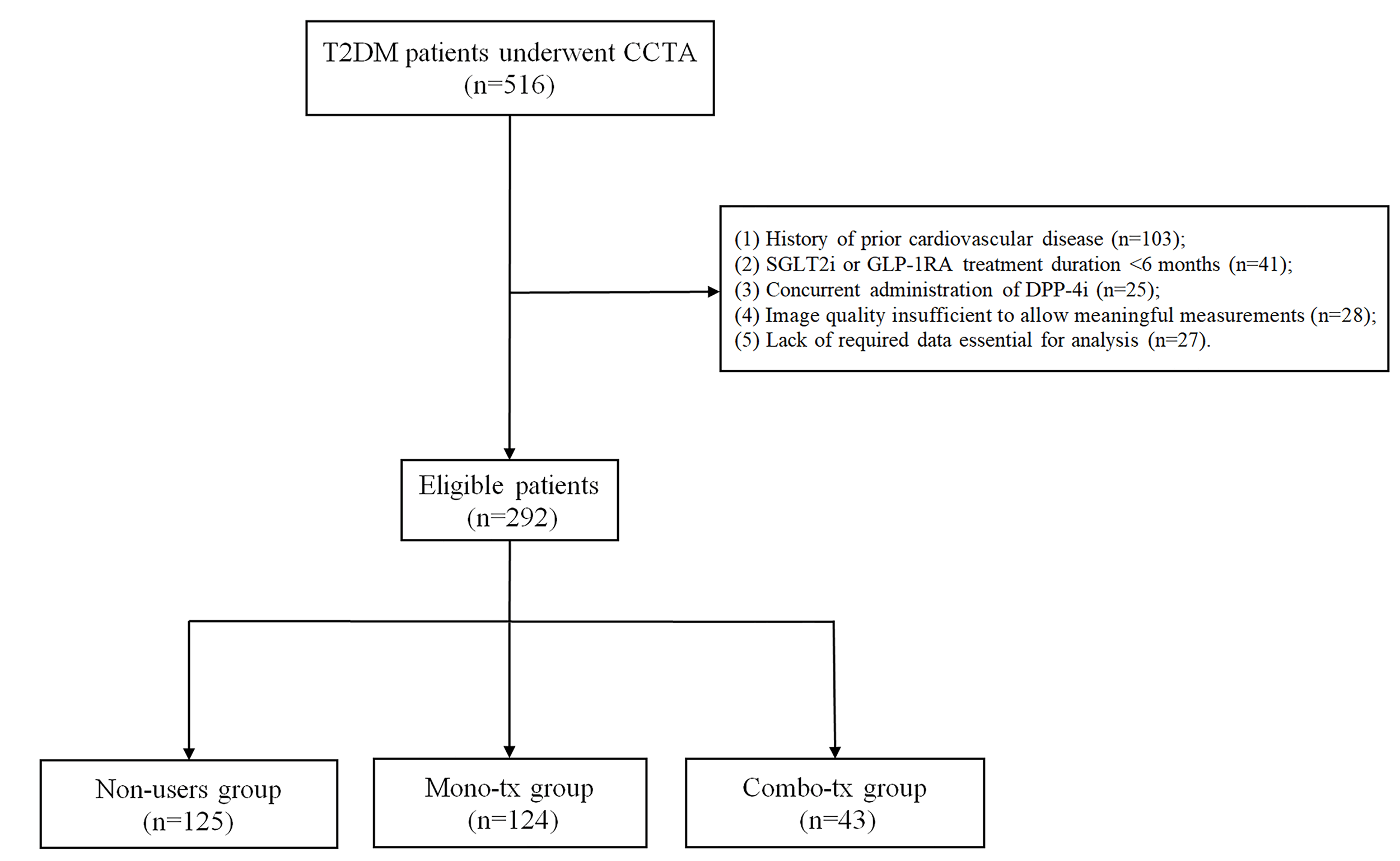
This retrospective analysis included 292 patients with T2DM who underwent coronary computed tomography angiography (CCTA) at Hebei General Hospital. Patients were divided into three groups: (1) non-SGLT-2i/GLP-1RA users (non-users, n = 125): Patients not receiving SGLT-2i or GLP-1RA therapy; (2) SGLT-2i/GLP-1RA monotherapy group (mono-tx, n = 124): Patients treated with either SGLT-2i or GLP-1RA alone; (3) SGLT-2i + GLP-1RA combination therapy group (combo-tx, n = 43): Patients receiving concurrent SGLT-2i and GLP-1RA therapy. Clinical parameters, laboratory biomarkers, and the peri-coronary FAI of patients were collected and comparatively analyzed among the three groups. Finally, multivariate linear regression models were constructed to elucidate the independent association between combined GLP-1RA and SGLT-2i therapy and the peri-coronary FAI.
One-way analysis of variance (ANOVA) revealed significant differences in the peri-coronary FAI among the three therapy groups. Specifically, compared with the non-user group, the combo-tx group had significantly lower peri-coronary FAI values in the left circumflex artery (LCX) and left anterior descending artery (LAD). Compared with the mono-tx group, the combo-tx group also had a significantly lower LCX FAI. Multivariate regression analysis further confirmed that combination therapy was independently associated with a lower FAI in the LAD, LCX, and right coronary artery (RCA). Subgroup analysis revealed a significant interaction by sex in the association between treatment regimen and LCX FAI.
The combined use of SGLT-2 inhibitors and GLP-1RAs may be associated with a decrease in the peri-coronary FAI in patients with T2DM, suggesting a potential role in reducing coronary inflammation. Thus, this combination therapy might offer advantages over monotherapy.
Graphical Abstract

Keywords
- peri-coronary fat attenuation index
- coronary inflammation
- type 2 diabetes mellitus
- sodium-dependent glucose transporter 2 inhibitor
- glucagon-like peptide-1 receptor agonist
Diabetes has become one of the most prevalent and severe chronic diseases in modern society. The estimated prevalence of diabetes worldwide in the 20–79-year-old population reached 10.5% (536.6 million people) in 2021, and forecasts suggest a surge to 12.2% by 2045 [1]. Worldwide, 32.2% of type 2 diabetes mellitus (T2DM) patients have comorbid cardiovascular disease (CVD), which has become the top cause of death in this population, with coronary artery disease and stroke being the primary contributors [2, 3]. Long-term hyperglycemia-induced endothelial dysfunction, vascular inflammation, and oxidative stress are strongly linked to the initiation and progression of CVD in T2DM patients [4]. Inflammation plays a central role in coronary atherosclerosis by promoting arterial plaque formation and progression, significantly augmenting the risk of cardiovascular disease [5, 6]. This establishes inflammation as a modifiable cardiovascular risk factor and therapeutic target, underscoring the need to explore treatment strategies to reduce coronary inflammation and improve cardiovascular outcomes in patients with T2DM.
The attenuation value of peri-coronary adipose tissue (PCAT) visualized by
coronary computed tomography angiography (CCTA) serves as a noninvasive biomarker
for evaluating coronary artery inflammation. As specialized epicardial adipose
tissue (EAT) surrounding coronary arteries, PCAT has dual functions in
maintaining vascular structural integrity and metabolic regulation [7, 8]. PCAT
secretes proinflammatory cytokines such as Interleukin-6 (IL-6) and Tumor
necrosis factor-
Sodium-glucose transporter 2 inhibitors (SGLT-2i) and glucagon-like peptide-1 receptor agonists (GLP-1RA) have attracted considerable attention of their cardiovascular benefits [14, 15, 16]. Mechanistically, SGLT2 inhibitors improve cardiovascular outcomes through both glucose-dependent pathways (e.g., promoting urinary glucose excretion) and independent mechanisms (e.g., reducing cardiac preload, reducing inflammation, and inhibiting vascular/myocardial fibrosis) [17, 18]. GLP-1 receptor agonists activate GLP-1 receptors to delay gastric emptying and suppress appetite, promoting weight loss. They also directly improve vascular endothelial function, reduce oxidative stress and inflammation, inhibit atherosclerotic plaque progression, and lower cardiovascular risk by reducing blood pressure and heart rate while enhancing left ventricular systolic function [19, 20]. Clinical evidence shows that SGLT-2i significantly reduce the risk of cardiovascular death, heart failure hospitalization, and composite renal endpoints in patients with heart failure with reduced ejection fraction and chronic kidney disease (CKD) [21, 22]. GLP-1 receptor agonists decrease the risk of major adverse cardiovascular events (MACEs) in T2DM patients with atherosclerotic cardiovascular disease (ASCVD) [23, 24]. However, the specific anti-inflammatory effects of these two drug classes on coronary arteries remain undefined.
Therefore, this study sought to investigate whether combination therapy with SGLT-2i and GLP-1RA can more effectively alleviate subclinical coronary inflammation as characterized by FAI in patients with T2DM without major cardiovascular events, thereby providing imaging-based evidence for early-stage anti-atherosclerotic intervention in this high-risk population.
This study was approved by the Ethics Committee of Hebei General Hospital (No.
2025-LW-0144), with a waiver of informed consent granted in accordance with
relevant regulatory guidelines. A total of 516 consecutive T2DM patients who
underwent CCTA at Hebei General Hospital between January 2023 and June 2024 were
retrospectively included. The eligibility criteria were as follows: (1) age
18–75 years, (2) body mass index (BMI)
The exclusion criteria included: (1) prior cardiovascular diseases, including
myocardial infarction, stroke, and heart failure, were included in the medical
history; (2) SGLT-2i or GLP-1RA treatment duration
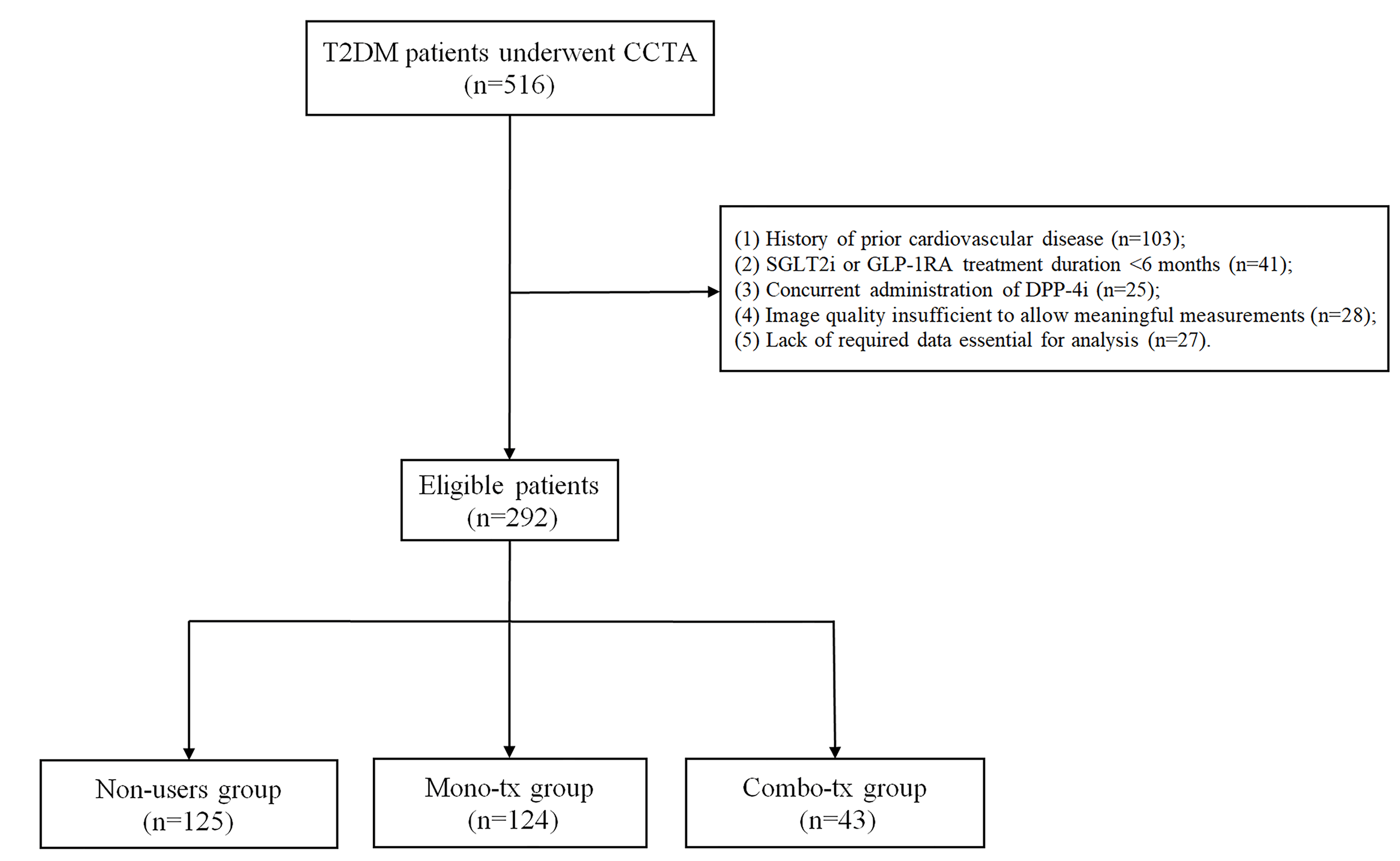 Fig. 1.
Fig. 1.
Study flowchart. T2DM, type 2 diabetes mellitus; CCTA, coronary computed tomography angiography; SGLT-2i, sodium-glucose transporter 2 inhibitors; GLP-1RA, glucagon-like peptide-1 receptor agonists; DPP-4i, dipeptidyl Peptidase-4 Inhibitors.
Specific details of the intervention drugs used by patients in this study are as
follows: SGLT-2i included dapagliflozin and empagliflozin; GLP-1RA included
semaglutide and liraglutide. Regarding dosages, the conventional daily dose of
dapagliflozin and empagliflozin was 10 mg; semaglutide was administered at a
conventional dose of 0.5 mg or 1.0 mg weekly, and liraglutide had a daily dose
range of 0.6–1.8 mg. All dosing regimens aligned with standard clinical practice
at our institution for achieving glycemic control and reducing cardiovascular
risk. All patients met the enrollment criterion for medication duration
(
In the Mono-tx group (n = 124), 87 patients received SGLT-2i monotherapy, and 37 patients received GLP-1RA monotherapy. Within the combination therapy group (n = 43), the specific drug pairings included dapagliflozin or empagliflozin combined with either semaglutide or liraglutide, reflecting real-world clinical prescribing patterns. The initiation modes of medication in the combination therapy group (n = 43) were categorized into two types: 29 cases (67.4%) involved sequential addition of medications, and 14 cases (32.6%) involved simultaneous initiation of both drugs. The most common medication adjustment pathway involved patients initially receiving SGLT-2i therapy, followed by the addition of GLP-1RA due to suboptimal glycemic control or insufficient weight management. Another subset of patients began with GLP-1RA therapy, followed by SGLT-2i, with adjustments made based on a comprehensive assessment of glycemic, weight, cardiovascular, and renal benefits.
Clinical characteristics and laboratory parameters, including demographic data
(age, sex, BMI), smoking history (current or past smoking
CCTA was performed at the Hebei General Hospital using a two-source CT scanner
(Somatom ForceCT, Siemens Healthcare GmbH, Erlangen, Bavaria, Germany). Patients
with a resting heart rate
After professional radiographers at our hospital selected the optimal image of coronary artery sequences, the images for each patient were uploaded to FAI measurement software (Shukun Technology, version 1.0.4, Beijing, China), which automatically identified the main trunks of the left anterior descending artery (LAD), left circumflex artery (LCX), and right coronary artery (RCA). The region of interest (ROI) was defined as follows: for the RCA, ranging from 10 mm distal to the origin to 50 mm (extending 40 mm) to avoid aortic interference; for the LAD and LCX, 40-mm segments extended distally from the coronary ostia. The FAI was automatically calculated by the software as the mean CT value (attenuation coefficient between –190 and –30 HU) of PCAT within an annular range where the radial distance from the vascular outer wall equals the average vessel diameter (Fig. 2). All image analysts underwent standardized protocol training. The measurements were performed by two independent analysts who were blinded to the patients’ clinical data, and discrepancies were resolved by consensus negotiation to ensure the consistency and reproducibility of the measurement parameters.
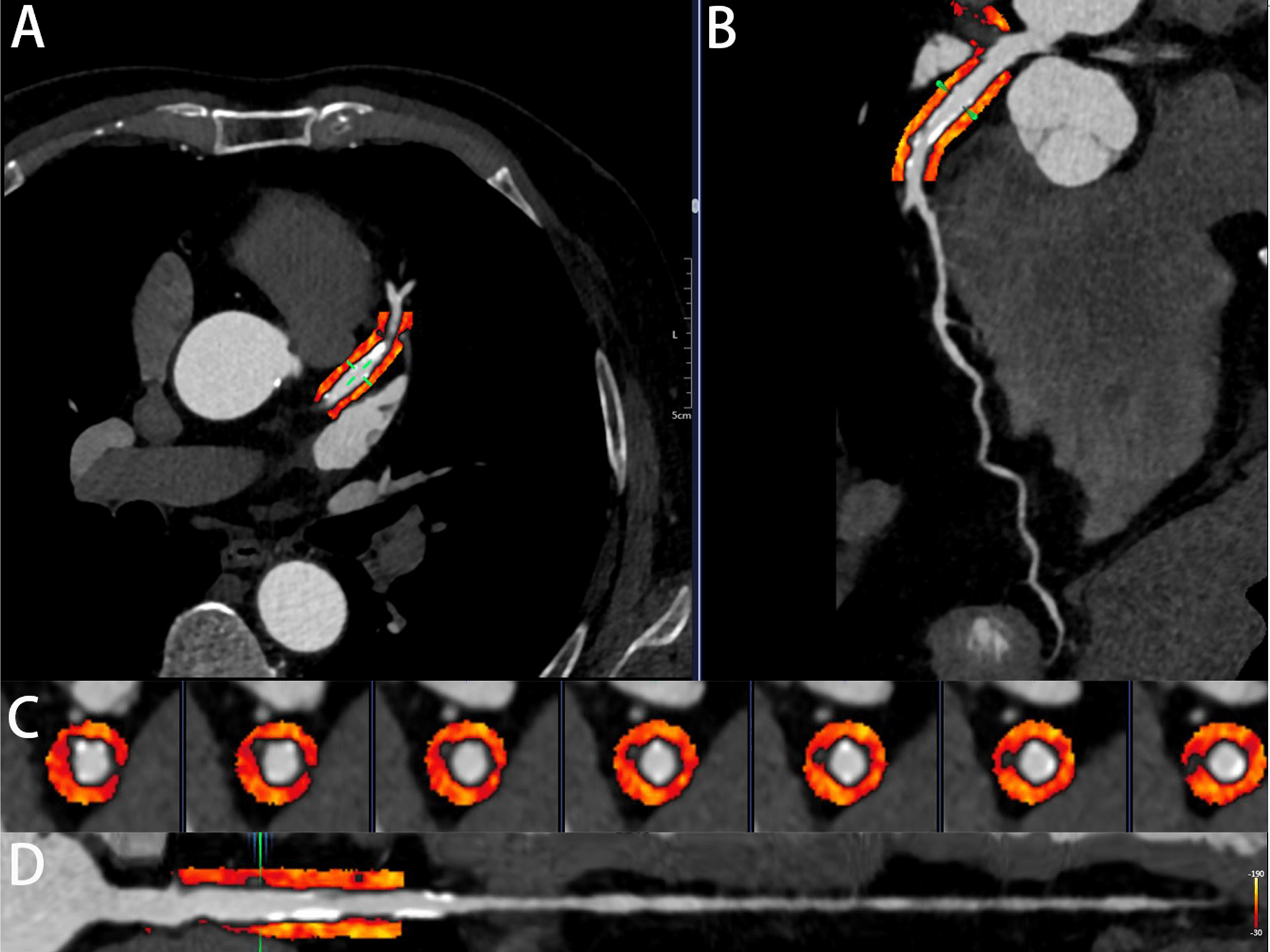 Fig. 2.
Fig. 2.
An illustrative case of PCAT attenuation in the LAD. (A) Cross-sectional view of PCAT. (B) Surface-recombined image of PCAT. (C) Straightened view of the proximal LAD segment. (D) Straightened view focusing on the proximal segment of the LAD. PCAT, peri-coronary adipose tissue; LAD, left anterior descending artery.
Categorical variables were reported as n (%) and compared via the chi-square
test. Continuous variables with a normal distribution were presented as the mean
The clinical characteristics and baseline demographics of the patients are
listed in Table 1. 292 patients were included in this retrospective analysis.
Compared with those in the Mono-tx group and Non-users group, patients in the
Combo-tx group were younger, with a mean age of 54.09
| Total | Non-users group | Mono-tx group | Combo-tx group | p | ||
| (n = 292) | (n = 125) | (n = 124) | (n = 43) | |||
| Age (years) | 59.65 |
61.23 |
59.99 |
54.09 |
||
| Male, n (%) | 193 (66.10) | 74 (59.20) | 82 (66.13) | 37 (86.05) | 0.006 | |
| T2DM duration (years) | 5.00 (1.25, 10.00) | 4.00 (0.50, 10.00) | 5.50 (2.00, 10.00) | 7.00 (2.00, 13.00) | 0.277 | |
| BMI (kg/m2) | 27.68 (25.88, 29.74) | 27.47 (25.71, 29.69) | 27.77 (25.81, 29.75) | 27.97 (26.39, 30.22) | 0.416 | |
| Smoking | 70 (23.97) | 29 (23.20) | 30 (24.19) | 11 (25.58) | 0.949 | |
| Hypertension, n (%) | 209 (71.58) | 95 (76.00) | 88 (70.97) | 26 (60.47) | 0.147 | |
| hyperlipidemia, n (%) | 153 (52.40) | 60 (48.00) | 68 (54.84) | 25 (58.14) | 0.400 | |
| Medication | ||||||
| Insulins (%) | 80 (27.40) | 30 (24.00) | 37 (29.84) | 13 (30.23) | 0.530 | |
| Metformin (%) | 100 (34.25) | 33 (26.40) | 48 (38.71) | 19 (44.19) | 0.041 | |
| 133 (45.55) | 52 (41.60) | 66 (53.23) | 15 (34.88) | 0.058 | ||
| Sulfonylurea (%) | 34 (11.64) | 13 (10.40) | 18 (14.52) | 3 (6.98) | 0.351 | |
| SGLT-2i (%) | 130 (44.52) | 0 (0.00) | 87 (70.16) | 43 (100.00) | ||
| GLP-1RA (%) | 80 (27.40) | 0 (0.00) | 37 (29.84) | 43 (100.00) | ||
| Antihypertensive (%) | 199 (68.15) | 88 (70.40) | 85 (68.55) | 26 (60.47) | 0.479 | |
| Anti-platelet drugs (%) | 237 (81.16) | 105 (84.00) | 98 (79.03) | 34 (79.07) | 0.563 | |
| Statin (%) | 259 (88.70) | 110 (88.00) | 109 (87.90) | 40 (93.02) | 0.625 | |
| PCSK9i (%) | 35 (11.99) | 18 (14.40) | 12 (9.68) | 5 (11.63) | 0.516 | |
| Laboratory indicators | ||||||
| Fast glucose (mmol/L) | 7.48 (6.30, 9.82) | 7.27 (6.10, 10.02) | 7.79 (6.43, 9.72) | 7.89 (6.83, 9.38) | 0.899 | |
| HbA1c (%) | 7.30 (6.70, 8.40) | 7.00 (6.49, 8.40) | 7.43 (6.80, 8.45) | 7.50 (7.05, 8.20) | 0.586 | |
| Total cholesterol (mmol/L) | 4.426 |
4.414 |
4.373 |
4.613 |
0.593 | |
| Triglycerides(mmol/L) | 1.560 (1.080, 2.388) | 1.490 (1.090, 2.290) | 1.575 (1.055, 2.345) | 1.890 (1.055, 3.030) | 0.863 | |
| HDL-C (mmol/L) | 1.118 |
1.124 |
1.119 |
1.099 |
0.854 | |
| LDL-C (mmol/L) | 2.747 |
2.734 |
2.701 |
2.918 |
0.411 | |
| Lipoprotein a (mg/L) | 114.60 (49.95, 298.80) | 112.50 (45.00, 273.03) | 125.90 (57.32, 298.80) | 92.70 (36.65, 332.10) | 0.946 | |
| Hemoglobin (g/L) | 139.82 |
137.37 |
138.55 |
150.56 |
||
| White blood cells ( |
6.69 |
6.62 |
6.67 |
6.96 |
0.525 | |
| Neutrophils ( |
4.36 |
4.36 |
4.31 |
4.54 |
0.679 | |
| Leukocytes ( |
1.80 |
1.78 |
1.81 |
1.83 |
0.863 | |
| Platelet count ( |
222.76 |
216.08 |
227.86 |
227.49 |
0.266 | |
| CRP (mg/L) | 2.93 |
2.91 |
2.83 |
3.24 |
0.447 | |
| LVEF (%) | 63.74 |
63.71 |
63.54 |
64.39 |
0.514 | |
| CCTA parameters | ||||||
| CACS | 52.36 (0.00, 273.94) | 45.37 (0.00, 273.70) | 44.12 (0.00, 227.24) | 90.25 (0.00, 353.35) | 0.574 | |
| FAI | ||||||
| LAD-PCAT (HU) | –80.25 |
–78.96 |
–81.00 |
–81.86 |
0.020 | |
| LCX-PCAT (HU) | –73.68 |
–73.27 |
–73.09 |
–76.57 |
0.030 | |
| RCA-PCAT (HU) | –80.32 |
–78.94 |
–81.40 |
–81.23 |
0.018 | |
Continuous variables following a normal distribution were reported as the mean
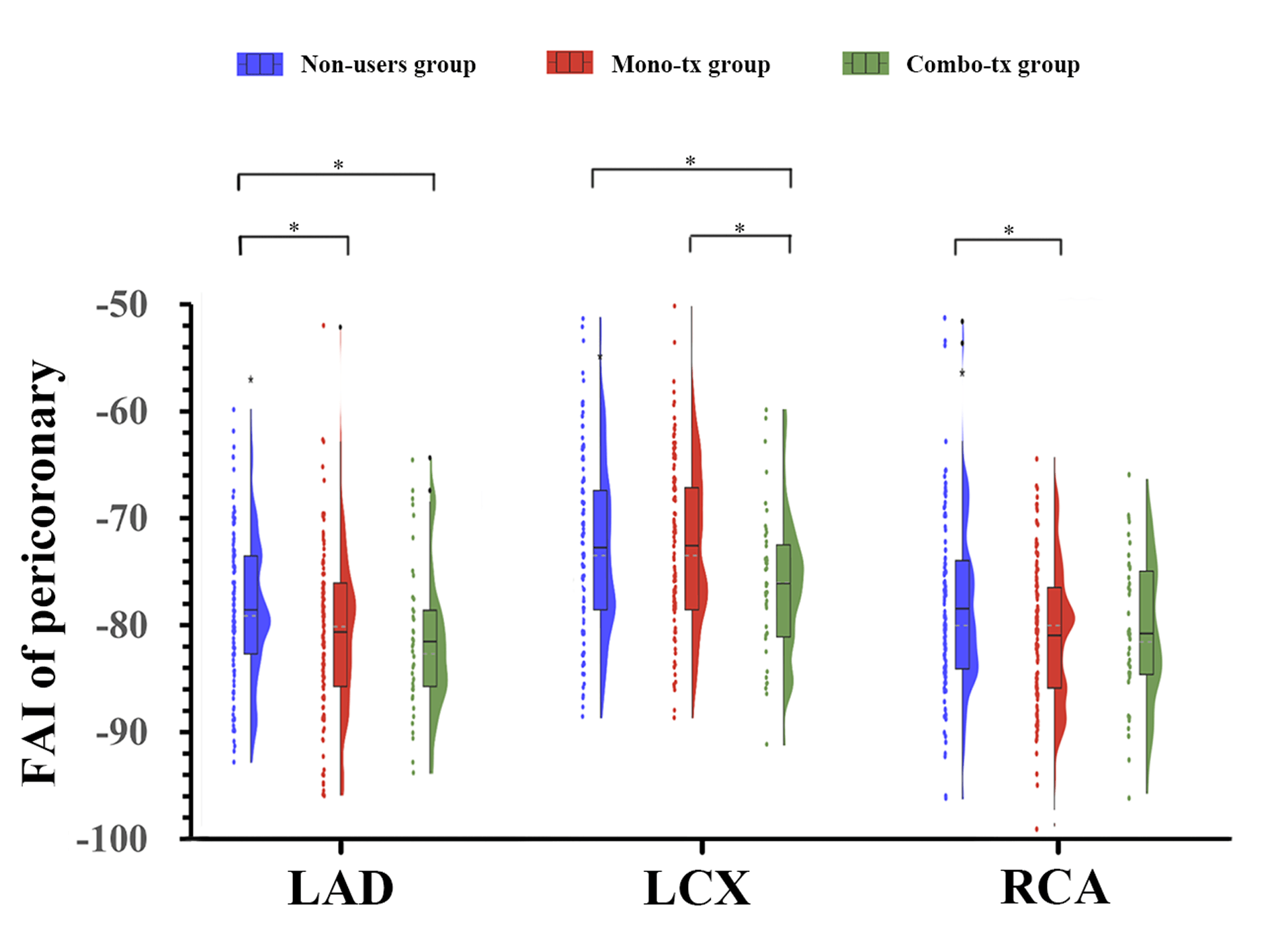 Fig. 3.
Fig. 3.
Pairwise comparisons of peri-coronary FAI values among the three
treatment groups. *p
Model 1 of the univariate linear regression indicated that monotherapy was
correlated with a lower peri-coronary FAI of the LAD (b = –2.042, 95% CI:
–3.783 to –0.301, p = 0.022) and RCA (b = –2.463, 95% CI: –4.249 to
–0.677, p = 0.007) in T2DM patients, but was not significantly
associated with a decreased peri-coronary FAI of the LCX (b = 0.179, 95% CI:
–1.739 to 2.098, p
| Group | Model 1 | Model 2 | |||||
| b (95% CI) | p | p for trend | b (95% CI) | p | p for trend | ||
| LAD-PCAT | Non-users | Reference | 0.007 | Reference | 0.005 | ||
| Mono-tx | –2.042 (–3.783 |
0.022 | –2.242 (–3.997 |
0.012 | |||
| Combo-tx | –2.902 (–5.331 |
0.020 | –3.054 (–5.625 |
0.020 | |||
| LCX-PCAT | Non-users | Reference | 0.061 | Reference | 0.052 | ||
| Mono-tx | 0.179 (–1.739 |
0.855 | 0.018 (–1.923 |
0.985 | |||
| Combo-tx | –3.302 (–5.978 |
0.016 | –3.602 (–6.446 |
0.013 | |||
| RCA-PCAT | Non-users | Reference | 0.015 | Reference | 0.005 | ||
| Mono-tx | –2.463 (–4.249 |
0.007 | –2.768 (–4.521 |
0.002 | |||
| Combo-tx | –2.293 (–4.783 |
0.072 | –2.745 (–5.313 |
0.036 | |||
Model 1: unadjusted; Model 2: adjusted for age, sex, BMI, hypertension status, T2DM duration, smoking history, statin, metformin, HbA1c, white blood cells, leukocytes, LDL-C, CACS, and LVEF. CI, confidence interval.
To investigate whether there were differences in the effects of SGLT-2i/GLP-1RA
monotherapy or combination therapy on the peri-coronary FAI across different
clinical subgroups, we conducted stratified analyses by sex, age, T2DM duration,
hyperlipidemia status, and smoking history based on the multivariate linear
regression model (Model 2). In addition, multivariate interaction tests between
treatment regimens and subgroup variables were performed to assess the
heterogeneity of treatment effects (Table 3). The interaction analysis revealed
that only the interaction between treatment regimens and sex exerted a
statistically significant effect on the FAI of LCX (p-interaction =
0.038). In contrast, no significant interactions were observed for other subgroup
variables with respect to the FAI of the LAD, LCX, and RCA (all
p-interaction
| Interaction with treatment regimen | LAD-PCAT | LCX-PCAT | RCA-PCAT |
| p-interaction | p-interaction | p-interaction | |
| Sex (Male vs. Female) | 0.798 | 0.038 | 0.526 |
| Smoking (Smoker vs. Non-smoker) | 0.138 | 0.668 | 0.690 |
| Age (years) | 0.433 | 0.522 | 0.794 |
| Duration of T2DM (years) | 0.780 | 0.882 | 0.483 |
| Hyperlipidemia (Yes vs. No) | 0.596 | 0.593 | 0.268 |
p-interaction: p-value for the interaction term (treatment
regimens
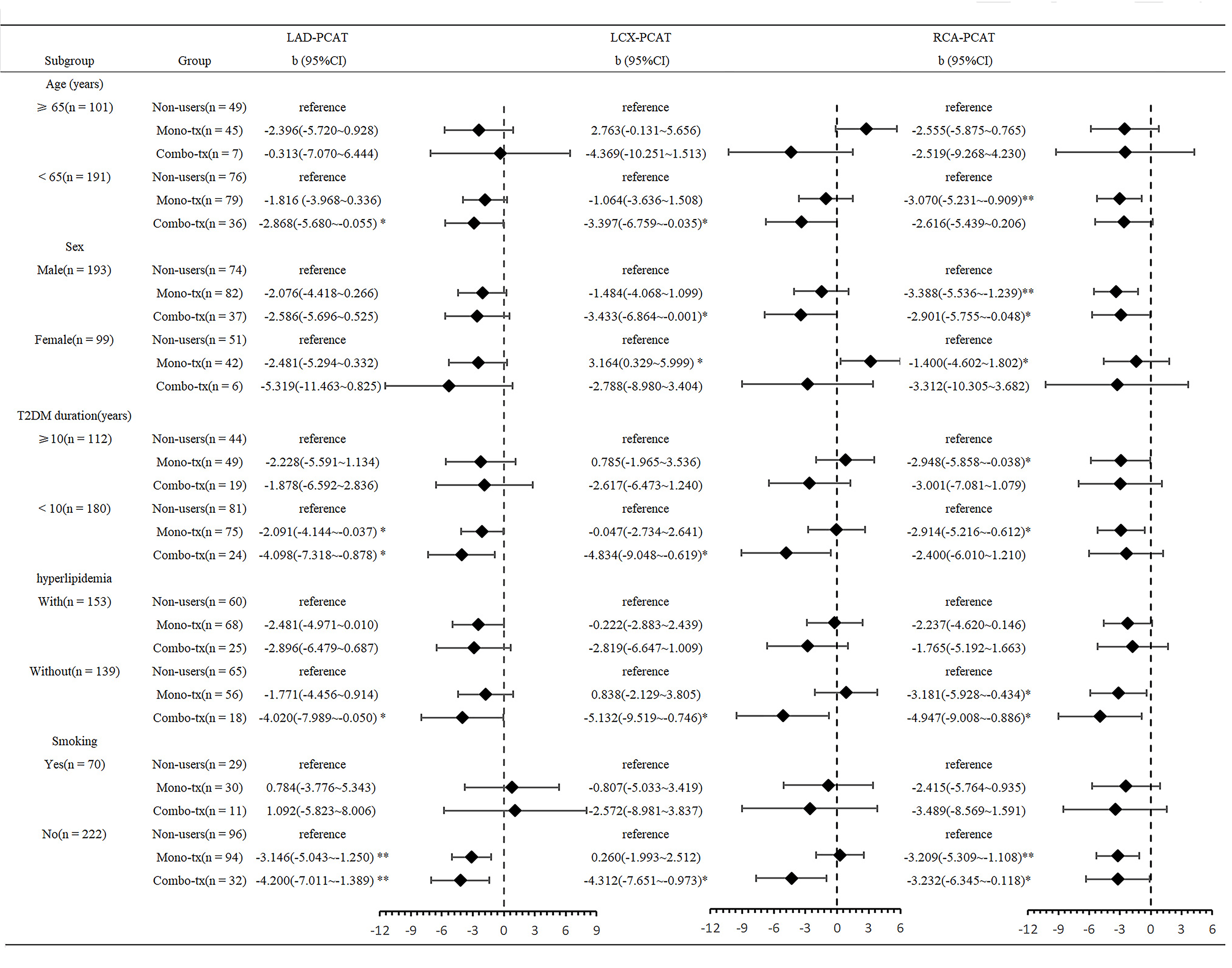 Fig. 4.
Fig. 4.
Exploratory stratified analyses of associations between three
treatment groups and peri-coronary FAI across different subgroups of T2DM
patients. *p
This study reports the results of the investigation of the relationship between the cardiovascular benefits of SGLT-2i combined with GLP-1RA and coronary inflammation in T2DM patients without known cardiovascular disease through the peri-coronary FAI, an imaging biomarker of coronary inflammation. This population is in a critical window period for atherosclerotic progression and urgently requires effective risk stratification and intervention strategies. As a tool capable of non-invasively detecting local coronary inflammation, FAI serves as an ideal surrogate endpoint for assessing early treatment responses. This study showed that SGLT-2i combined with GLP-1RA therapy was independently associated with a significant reduction in the FAI of the LAD, LCX, and RCA. After adjusting for confounders, the reduction in the LCX FAI with combination therapy was significantly greater than that with monotherapy, suggesting that combination therapy may confer cardiovascular benefits to T2DM patients by reducing coronary inflammation.
Multiple large-scale randomized controlled trials have confirmed that SGLT-2i and GLP-1RA can significantly reduce the risk of MACEs in T2DM patients [25, 26]. According to the 2025 American Diabetes Association (ADA) guidelines, in patients with T2DM complicated with ASCVD, heart failure, or CKD, SGLT-2i or GLP-1RA with proven cardiorenal protective evidence are preferentially recommended as first-line therapy (evidence level A) [27]. Observational studies have demonstrated the cardiovascular benefits of combined SGLT-2i and GLP-1RA therapy in patients with T2DM. For example, a UK CPRD cohort study showed that SGLT-2i/GLP-1RA combination therapy reduced the risk of MACEs by approximately 30% compared with monotherapy [28]. In a prospective observational study on T2DM patients with acute myocardial infarction (AMI), Marfella et al. [29] reported that, compared with either SGLT-2i or GLP-1RA monotherapy, combination therapy significantly reduced the risk of MACEs by 83%–84.6% and improved the myocardial salvage index (MSI). Further supporting these findings, a large retrospective cohort study by Chaiyakunapruk et al. [30] in the United States demonstrated that adding GLP-1RA to SGLT-2i reduced the risk of MACEs by 45%–46% in T2DM patients with ASCVD.
SGLT-2i reduce renal glucose reabsorption and promote glycosuria by inhibiting
the activity of SGLT-2 protein in the proximal renal tubules. Their cardiorenal
protective effects are achieved by alleviating volume overload to reduce cardiac
workload, as well as by improving cellular energy metabolism. This process is
often accompanied by activation of the AMP-activated protein kinase
(AMPK) pathway, enhanced mitochondrial function, and mitigated oxidative
stress. In addition, SGLT-2i exert prominent pleiotropic anti-inflammatory
effects. Hyperglycemia and excessive volume overload under diabetic conditions
lead to hyperactivation of the sympathetic nervous system, whereas SGLT-2i can
lower sympathetic nerve tone through effective alleviation of volume overload,
thereby suppressing neuroimmune-mediated inflammatory responses. SGLT-2i improve
systemic metabolic disorders and insulin resistance via multiple mechanisms,
including sustained glucose lowering, body weight reduction, and lipid profile
regulation, thus exerting anti-inflammatory effects. GLP-1RA binds to GLP-1
receptors in the vascular wall, modulating endothelial cells, monocytes,
macrophages, and vascular smooth muscle cells. This interaction not only enhances
vascular endothelial function but also suppresses NLRP3 inflammasome
activation, thereby reducing the release of proinflammatory cytokines (e.g.,
IL-1
The peri-coronary FAI, an emerging imaging biomarker based on CCTA, reflects
coronary inflammation and plaque stability by quantifying attenuation value
changes in PCAT. Studies have shown that the peri-coronary FAI can independently
predict MACEs. Patients with high peri-coronary FAI values face a 3.29-fold
greater risk of MACEs than those with low values [33, 34]. The CRISP-CT study
demonstrated that increased FAI values in the RCA and LAD are significantly
positively correlated with all-cause and cardiac mortality [35]. These findings
suggest that inflammation-targeted therapies may improve patient prognosis.
Notably, this study primarily included individuals with a BMI
A recent study confirmed that increased PCAT attenuation around the LAD in T2DM patients is significantly associated with cardiovascular events [37], suggesting that treatment strategies to reduce peri-coronary FAI may lower the risk of adverse cardiovascular events in T2DM patients. To date, investigations into the associations between SGLT-2i/GLP-1RA therapy and the peri-coronary FAI are relatively few. Studies by Liu et al. [38] and Li et al. [39] have shown that dapagliflozin and semaglutide may alleviate coronary inflammation in T2DM patients by lowering the peri-coronary FAI. Biesenbach et al. [40] demonstrated that liraglutide is linked to a lower LAD FAI in asymptomatic T2DM patients. However, the effect of the combined use of these two classes of drugs on the peri-coronary FAI remains unclear. Our study revealed that combined SGLT-2i and GLP-1RA treatment is negatively correlated with coronary inflammation in T2DM patients and has advantages over monotherapy in some cases. Subgroup analysis indicated that the association between combined SGLT-2i and GLP-1RA therapy and reduced FAI was consistent across patients stratified by age, T2DM duration, hyperlipidemia, or smoking history. A significant interaction was observed only for sex regarding its effect on LCX FAI, suggesting a potential sex-specific response. These findings offer insights for personalized treatment strategies in T2DM.
This study has several limitations. First, due to the limited sample size, we
grouped SGLT-2i and GLP-1RA into a single monotherapy group for analysis, thus
failing to evaluate the independent effects of these two drug classes on the
peri-coronary FAI, and were unable to fully exclude intra-group heterogeneity.
Second, the retrospective study design is subject to selection bias (e.g., a
higher proportion of young males in the combination therapy group and imbalances
in medication use across some groups), and it was not possible to control for
unmeasured confounding factors such as dietary patterns and physical activity.
Although adjustments were made via multivariate models, the lack of
randomization, blinding, and placebo control means this study can only reveal
associations rather than causal relationships. Third, the relatively small
overall sample size (n = 292) and the combination therapy subgroup (n = 43) may
have limited statistical power, potentially affecting the results of some
subgroup analyses. Fourth, we excluded patients with a BMI
The combined use of SGLT-2 inhibitors and GLP-1 receptor agonists may be correlated with a decrease in the peri-coronary fat attenuation index in T2DM patients, suggesting their potential role in alleviating coronary inflammation. Compared with monotherapy, this combination therapy might offer potential advantages.
The datasets utilized or analyzed during the current study are available from the corresponding author upon reasonable request.
TXW contributed to the study design, data collection, statistical analysis, and drafting of the manuscript. YHL participated in the study design and data collection and critically reviewed the manuscript. WJY, SHC, SJZ, YTW and CW participated in data collection, assisted in data collation and verification, and reviewed the manuscript section related to data acquisition. FFZ contributed to the study design and the editing and critical review of the manuscript. YD participated in the study design, contributed to the quality control of the data, and edited and critically reviewed the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was carried out in accordance with the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Hebei General Hospital (Protocol No. 2025-LW-0144). As this is a retrospective analysis, the requirement for patient informed consent was waived in accordance with the relevant regulatory guidelines.
Not applicable.
This work was supported by the government-funded project for training outstanding clinical medicine talent of Hebei Province (Grant No. ZF2024010) and the Hebei Provincial Major Science and Technology Support Program (Grant No. 252W7703D).
The authors declare no conflicts of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/RCM47415.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.