



 , Xian Shao 3,†, Tian-Shu Gu 1, Yu-Kun Zhang 1, Su-Tao Hu 1, Chao Jiang 1, Jing-Kun Zhang 4, Xue Wu 5, Seung-Woon Rha 6, Xing Liu 1, Tong Liu 1, Kang-Yin Chen 1,*
, Xian Shao 3,†, Tian-Shu Gu 1, Yu-Kun Zhang 1, Su-Tao Hu 1, Chao Jiang 1, Jing-Kun Zhang 4, Xue Wu 5, Seung-Woon Rha 6, Xing Liu 1, Tong Liu 1, Kang-Yin Chen 1,*
1 Department of Cardiology, Second Hospital of Tianjin Medical University, Tianjin Key Laboratory of Ionic-Molecular Function of Cardiovascular disease, Tianjin Institute of Cardiology, 300211 Tianjin, China
2 Department of Cardiology, The Fourth Central Hospital Affiliated to Tianjin Medical University, 300140 Tianjin, China
3 Division of Nephrology, National Clinical Research Center for Kidney Disease, State Key Laboratory of Organ Failure Research, Nanfang Hospital, Southern Medical University, 510515 Guangzhou, Guangdong, China
4 Cardiovascular Research Institute, University of California, San Francisco, CA 94158, USA
5 Institute for Global Health Sciences, University of California, San Francisco, CA 94158, USA
6 Cardiovascular Center, Korea University Guro Hospital, 08308 Seoul, Republic of Korea
†These authors contributed equally.
Abstract
Dual antiplatelet therapy is essential for managing ST-elevation myocardial infarction (STEMI); however, the optimal choice of P2Y12 inhibitor in patients with thrombocytosis remains unclear. Therefore, this study aimed to compare the effects of clopidogrel and ticagrelor on the prognosis of patients with STEMI and platelet counts exceeding 350 × 109/L.
Utilizing data from the Tianjin Health and Medical Big Data platform (2010–2023), this retrospective cohort study included patients with acute myocardial infarction from 82 hospitals. After propensity score matching, 461 patients were assigned to two groups: ticagrelor and clopidogrel. Kaplan–Meier curves and Cox regression analyses were employed to evaluate outcomes, with major adverse cardiac and cerebrovascular events (MACCEs) as the primary outcome. Secondary outcomes included net adverse clinical events (NACEs), all-cause mortality, cardiac mortality, recurrent non-fatal myocardial infarction, coronary revascularization, cerebral infarction, and bleeding events (Bleeding Academic Research Consortium (BARC) types 3–5). A MACCE was defined as a composite of cardiac mortality, recurrent non-fatal myocardial infarction, and cerebral infarction, while a NACE encompassed a MACCE plus bleeding events (BARC types 3–5).
Ticagrelor significantly reduced MACCEs (6.9% versus 12.1%; p = 0.008), all-cause mortality (3.9% versus 9.5%; p < 0.001), cardiac mortality (3.5% versus 7.4%; p = 0.0096), and NACEs (8.2% versus 13.0%; p = 0.021) compared with clopidogrel. Exploratory multivariable analysis confirmed an independent association of ticagrelor with reduced risks of MACCEs (adjusted hazard ratio (aHR) = 0.59; 95% confidence interval (CI), 0.37–0.93), NACEs (aHR = 0.64; 95% CI, 0.42–0.98), and all-cause mortality (aHR = 0.47; 95% CI, 0.26–0.83).
Ticagrelor was associated with superior clinical outcomes in patients with STEMI and elevated admission platelet counts (≥350 × 109/L) compared with clopidogrel. In contrast to genetic testing, which is costly, time-consuming (≥24–72 hours), and impractical in emergencies, this simple, universally available platelet count threshold offers an immediate, practical biomarker for selecting potent P2Y12 inhibition in acute settings.
Keywords
- ST-segment elevation myocardial infarction
- thrombocytosis
- clopidogrel
- ticagrelor
- prognosis
Acute ST-segment elevation myocardial infarction (STEMI) constitutes a
significant cardiovascular emergency, characterized by high incidence and
mortality rates [1, 2]. Current management strategies prioritize dual antiplatelet
therapy, with P2Y12 inhibitors serving as critical agents alongside aspirin.
Among these, ticagrelor has gained prominence as a preferred option in general
STEMI populations owing to its rapid onset and potent, predictable inhibition of
platelet aggregation, circumventing the genetic limitations associated with
clopidogrel activation via CYP2C19 enzymes. Robust clinical evidence from
numerous registries and trials has established the superiority of ticagrelor in
mitigating major adverse cardiac and cerebrovascular events (MACCEs) in the
general STEMI population [3, 4, 5, 6, 7, 8, 9]. However, the pathophysiological necessity for
intensive antiplatelet therapy is considerably heightened in the substantial
subset of patients with STEMI presenting with elevated platelet counts.
Increasing evidence suggests that higher baseline platelet levels correlate with
enhanced platelet reactivity, accelerated thrombus formation, and consequently,
poorer clinical outcomes [10, 11, 12, 13]. This hyperreactive platelet phenotype
exacerbates atherosclerotic thrombosis and markedly increases the risk of stent
thrombosis and recurrent myocardial infarction following percutaneous coronary
intervention (PCI), complications that are directly associated with elevated
cardiac mortality [14, 15, 16]. Notably, registry data from the Thrombolysis in
Myocardial Infarction (TIMI) trials indicate a 34% higher 30-day mortality in
patients with STEMI and platelet counts exceeding the median value compared with
that in patients with lower counts [10]. In East Asian populations, large-scale
studies further delineate specific high-risk thresholds, such as admission
platelet counts
Despite this compelling pathophysiological rationale and consistent clinical
observations, current guidelines lack specific recommendations for selecting
platelet therapy based on platelet count. Moreover, existing comparative studies
on P2Y12 inhibitors predominantly focus on broad STEMI populations, potentially
obscuring differential treatment effects that may be crucial for patients with a
heightened thrombotic propensity attributed to thrombocytosis [3, 4, 5, 6]. This
knowledge gap is clinically significant, considering that over 40% of patients
with STEMI present with platelet counts exceeding normal ranges at admission
[10]. This phenomenon yields a skewed distribution (median: 218
To directly address this critical therapeutic void, our study performed the
first head-to-head comparison of ticagrelor with clopidogrel, exclusively in
patients with STEMI presenting with admission thrombocytosis. By elucidating the
optimal antiplatelet regimen for this vulnerable population, we aimed to (1)
provide evidence-based guidance specifically designed to alleviate their
excessive thrombotic risk attributed to elevated platelet counts and (2) enhance
long-term cardiovascular outcomes. This study adopted an elevated platelet count
(
The data for this study were derived from the coronary artery disease (CAD) specialized database within the Tianjin Health and Medical Big Data Super Platform (referred to as the “platform”). Tianjin Health and Medical Big Data Co., Ltd. serves as the authorized data provider responsible for the collection, management, and application of data on this platform. The platform aggregates clinical diagnosis and treatment information from 43 tertiary and 39 secondary hospitals in the Tianjin region, as well as data from the public health system.
After normalization and de-identification on the platform, the data were transformed into a specialized database for scientific research on the CAD database, which includes patients who were hospitalized at least once between January 1, 2010, and June 30, 2023, with discharge diagnoses of CAD. Comprehensive healthcare information for these patients was collected, encompassing demographic characteristics, disease diagnoses, medication and non-medication prescriptions, examination and laboratory test results, surgical information, cost details, community medication and health examination data, as well as public health mortality information.
This study employed the International Classification of Diseases, 10th Revision
(ICD-10) diagnostic codes to identify patients discharged with a diagnosis of
STEMI. Following STEMI diagnosis, patients were prescribed aspirin as a baseline
medication, in addition to either ticagrelor or clopidogrel. Patients were
required to have an initial admission platelet count
| Characteristics | Before PSM | After PSM | |||||||
| Clopidogrel group | Ticagrelor group | p value | SMD | Clopidogrel group | Ticagrelor group | p value | SMD | ||
| N = 1073 | N = 461 | N = 461 | N = 461 | ||||||
| Male (%) | 608 (56.7) | 297 (64.4) | 0.005 | 0.159 | 298 (64.6) | 297 (64.4) | 1.000 | 0.005 | |
| Age (%) | 62.0 (14.08) | 56.3 (13.06) | 0.417 | 56.0 (13.56) | 56.0 (13.06) | 0.970 | 0.002 | ||
| Killip class (%) | 0.872 | ||||||||
| I | 590 (55.0) | 297 (64.4) | 307 (66.6) | 297 (64.4) | |||||
| II | 274 (25.5) | 122 (26.5) | 111 (24.1) | 122 (26.5) | |||||
| III | 119 (11.1) | 18 (3.9) | 18 (3.9) | 18 (3.9) | |||||
| IV | 90 (8.4) | 24 (5.2) | 25 (5.4) | 24 (5.2) | |||||
| Complications | |||||||||
| Ventricular fibrillation (%) | 19 (1.8) | 9 (2.0) | 0.972 | 0.013 | 9 (2.0) | 9 (2.0) | 1.000 | ||
| Ventricular tachycardia (%) | 43 (4.0) | 11 (2.4) | 0.153 | 0.092 | 19 (4.1) | 11 (2.4) | 0.194 | 0.098 | |
| III atrioventricular block (%) | 12 (1.1) | 5 (1.1) | 1.000 | 0.003 | 4 (0.9) | 5 (1.1) | 1.000 | 0.022 | |
| Comorbidities | |||||||||
| Diabetes mellitus (%) | 289 (26.9) | 116 (25.2) | 0.510 | 0.040 | 116 (25.2) | 116 (25.2) | 1.000 | ||
| Hypertension (%) | 387 (36.1) | 169 (36.7) | 0.870 | 0.012 | 168 (36.4) | 169 (36.7) | 1.000 | 0.005 | |
| Atrial fibrillation (%) | 19 (1.8) | 6 (1.3) | 0.656 | 0.038 | 5 (1.1) | 6 (1.3) | 1.000 | 0.020 | |
| Hyperlipidemia (%) | 383 (35.7) | 186 (40.3) | 0.095 | 0.096 | 182 (39.5) | 186 (40.3) | 0.840 | 0.018 | |
| Chronic obstructive pulmonary disease (%) | 25 (2.3) | 8 (1.7) | 0.586 | 0.042 | 7 (1.5) | 8 (1.7) | 1.000 | 0.017 | |
| Stroke (%) | 194 (18.1) | 74 (16.1) | 0.376 | 0.054 | 79 (17.1) | 74 (16.1) | 0.723 | 0.029 | |
| Cerebral hemorrhage (%) | 105 (9.8) | 27 (5.9) | 0.016 | 0.147 | 33 (7.2) | 27 (5.9) | 0.504 | 0.153 | |
| Renal insufficiency (%) | 167 (15.6) | 73 (15.8) | 0.954 | 0.007 | 62 (13.4) | 73 (15.8) | 0.352 | 0.068 | |
| Peripheral vascular disease (%) | 92 (8.6) | 41 (8.9) | 0.916 | 0.011 | 34 (7.4) | 41 (8.9) | 0.470 | 0.056 | |
| Previous PCI (%) | 16 (1.5) | 2 (0.4) | 0.132 | 0.108 | 5 (1.1) | 2 (0.4) | 0.448 | 0.175 | |
Footnotes: Data are presented as n (%) and the mean (standard deviation (SD))
for categorical and continuous (age) variables, respectively. p values
were calculated using the
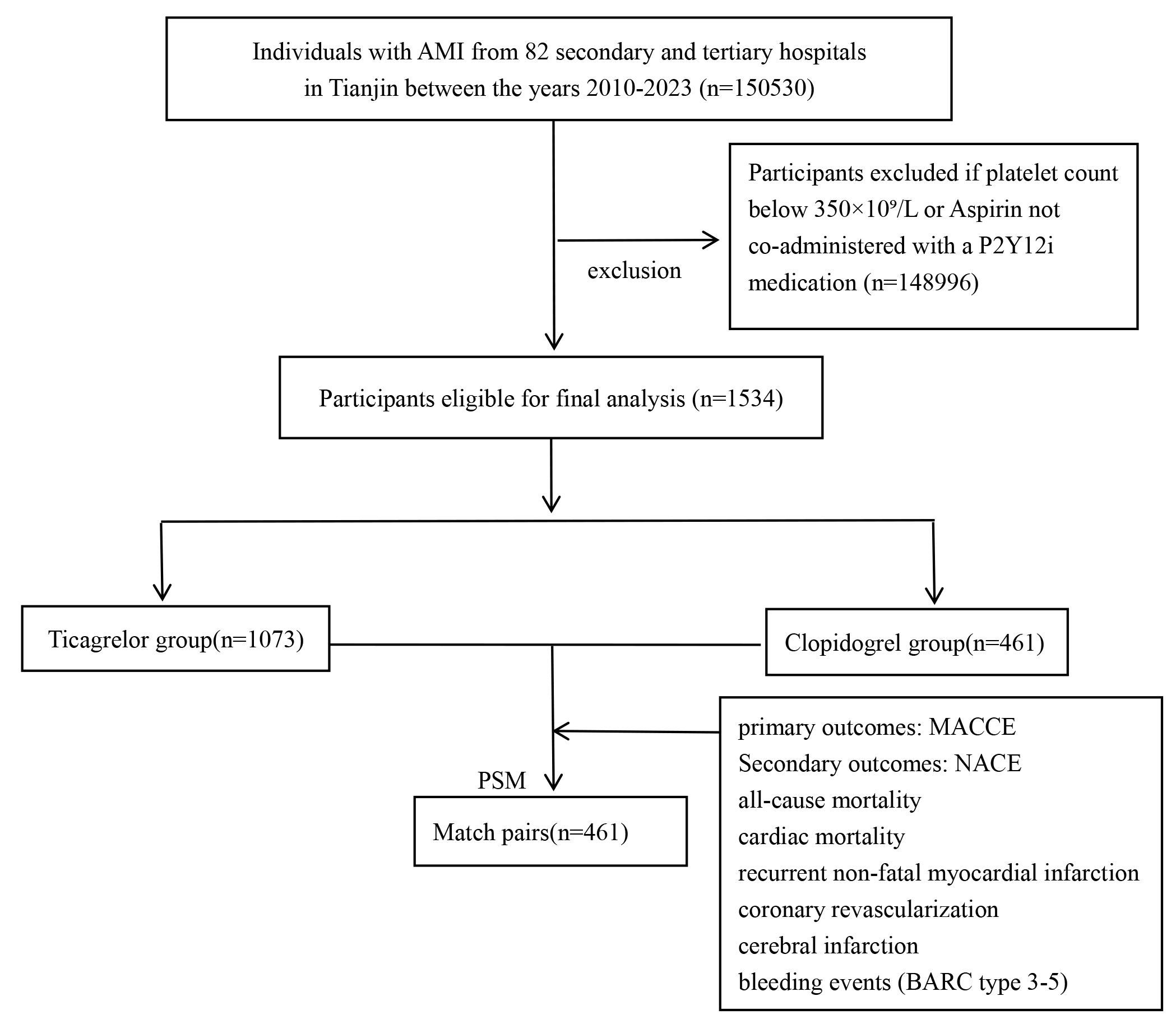 Fig. 1.
Fig. 1.
Study flowchart. MACCE, major adverse cardiac and cerebrovascular event; NACE, net adverse clinical event; AMI, acute myocardial infarction; PSM, propensity score matching; BARC, Bleeding Academic Research Consortium.
This study recorded basic information and clinical data, including sex, age,
Killip grade, and comorbidities (hypertension, hyperlipidemia, diabetes, atrial
fibrillation, stroke, cerebral hemorrhage, renal insufficiency, and peripheral
vascular disease). Hospitalization and discharge medications were also
documented, including aspirin, oral anticoagulants, statins, nitrates,
beta-blockers, renin–angiotensin system inhibitors (RASIs;
angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor
blockers (ARBs), or angiotensin receptor-neprilysin inhibitors (ARNIs)), calcium
channel antagonists, diuretics, levosimendan, and amiodarone. Laboratory tests
included D-dimer and fibrinogen assays. Data collection was conducted by trained
physicians using post-discharge electronic health records. Patients with AMI were
treated according to established guidelines—unless contraindicated or
explicitly rejected by family members—with dual antiplatelet therapy, coronary
artery reperfusion therapy, and subsequent ventricular anti-remodeling.
Successful PCI was defined as achieving post-procedure TIMI grade 3 flow with
In this study, MACCE constituted the primary outcome, while secondary outcomes included net adverse clinical events (NACEs), all-cause mortality, cardiac mortality, recurrent non-fatal myocardial infarction, coronary revascularization, cerebral infarction, and bleeding events (Bleeding Academic Research Consortium (BARC) type 3–5). MACCE were specifically defined as cardiac mortality, recurrent non-fatal myocardial infarction, and cerebral infarction, while NACE encompassed cardiac mortality, recurrent non-fatal myocardial infarction, cerebral infarction, and bleeding events (BARC type 3–5).
The study outcomes included both in-hospital adverse events and 1-year adverse
outcomes. Primary outcome measures comprised in-hospital and 1-year cardiac
mortalities. Secondary in-hospital adverse outcomes included malignant
arrhythmias not excluded from the study cohort, specifically ventricular
tachycardia, ventricular fibrillation, and ventricular flutter. Secondary 1-year
adverse outcomes included all-cause mortality, follow-up myocardial infarction,
revascularization events, stroke events, and bleeding events classified as BARC
type 3–5. Follow-up myocardial infarctions were defined as subsequent hospital
admissions for AMI recorded in the database after the baseline event. Stroke was
defined as new hospital admissions within 1 year owing to either new cerebral
infarction or hemorrhage. Revascularization events were defined as any
revascularization procedure performed on any segment of the coronary artery,
including branch vessels, after discharge from the baseline AMI. “BARC type
3–5” events were defined as bleeding incidents that satisfy the BARC criteria
for types 3 to 5, as recorded in the database. The breakdown is as follows: type
3a (overt bleeding with a hemoglobin decline of 3–5 g/dL or transfusion of 1–2
units), type 3b (hemoglobin decline
We conducted a complete-case analysis, ensuring no missing data or imputation of
missing values. All statistical analyses were performed using R software (version
4.3.2; R Foundation for Statistical Computing, Vienna, Austria). Variable
selection for the exploratory multivariable Cox proportional hazards regression
model employed a combined clinical and statistical approach. Clinically relevant
covariates identified in prior literature (for example, age, sex, Killip class,
hypertension, diabetes mellitus, prior stroke, renal insufficiency, and
in-hospital PCI) were included in the model irrespective of their univariate
significance. Additional variables with a p value
This analysis adhered to a predefined statistical analysis plan established before data extraction from the Tianjin Health and Medical Big Data Platform. The study protocol and analytic framework received approval from the Clinical Research Ethics Committee of the Second Hospital of Tianjin Medical University (KY2023052-01). Although the study was not prospectively registered in a public trial registry, all primary and secondary endpoints, covariate definitions, and model specifications were prespecified before statistical analysis commenced.
PSM was performed using a 1:1 nearest-neighbor matching algorithm without replacement, with caliper width set to 0.2 times the SD of the propensity score logit. 1:1 propensity score matching was performed using a greedy nearest-neighbor algorithm, maintaining a 1:1 ratio and a caliper width of 0.02 times the SD of the propensity score logit. Matched variables included sex, age, Killip classification, receipt of PCI during hospitalization, prior history of diabetes, hypertension, stroke, or hyperlipidemia, and the use of calcium channel blockers, beta-blockers, RASIs, statins, nitrates, or oral anticoagulants. Following the matching process, inter-group balance was evaluated using SMDs, with values less than 0.1 indicating adequate balance.
We compared baseline characteristics between the ticagrelor and clopidogrel
groups pre- and post-PSM. Continuous variables are presented as the mean
To achieve doubly robust estimation, inverse probability treatment weighting (IPTW) was applied to the full cohort, incorporating reperfusion variables (primary PCI (PPCI), elective PCI). Sensitivity analyses included Fine–Gray competing risk models for non-fatal endpoints (with death as a competing event) and landmark Cox models for timing-specific outcomes (in-hospital, 0–30 days, and 31–365 days). Subgroup analyses, based on age, sex, PPCI, renal function, and GPI use, employed interaction tests (p for interaction).
Survival analyses utilized Kaplan–Meier curves to estimate the cumulative incidence of adverse events, with the log-rank test employed to compare survival differences between treatment groups. Exploratory multivariable Cox proportional hazards regression was applied to evaluate the independent association between ticagrelor use and study outcomes. Additionally, due to the limited number of events (62 all-cause deaths and 50 cardiac deaths), the full multivariable Cox models that adjusted for nine prespecified covariates yielded a low events-per-variable ratio (approximately 6–7). These multivariable-adjusted hazard ratios should therefore be regarded as exploratory and interpreted with caution. The primary evidence for the benefits of ticagrelor derives from the more robust propensity score-matched intention-to-treat comparison and doubly robust IPTW analyses.
As depicted in Tables 1,2, significant pre-PSM differences were noted
between the clopidogrel and ticagrelor groups. The ticagrelor group exhibited a
greater proportion of men (64.4% versus 56.7%, p = 0.005) and a lower
mean age (56.3 versus 62.0 years, p
| Before PSM | After PSM | |||||||
| Clopidogrel group | Ticagrelor group | p value | SMD | Clopidogrel group | Ticagrelor group | p value | SMD | |
| N = 1073 | N = 461 | N = 461 | N = 461 | |||||
| PCI (%) | 585 (54.5) | 343 (74.4) | 0.425 | 348 (75.5) | 343 (74.4) | 0.761 | 0.025 | |
| PPCI (%) | 476 (44.4) | 321 (69.6) | 0.528 | 291 (63.1) | 321 (69.6) | 0.043 | 0.138 | |
| Thrombolytic (%) | 22 (2.1) | 11 (2.5) | 0.823 | 0.023 | 9 (2.0) | 11 (2.4) | 0.821 | 0.030 |
| Aspirin (%) | 1073 (100.0) | 461 (100.0) | 1.000 | 461 (100.0) | 461 (100.0) | 1.000 | ||
| Oral anticoagulant (%) | 17 (1.6) | 1 (0.2) | 0.043 | 0.145 | 0 (0.0) | 1 (0.2) | 1.000 | 0.066 |
| RASIs (%) | 641 (59.7) | 339 (73.5) | 0.296 | 334 (72.5) | 339 (73.5) | 0.767 | 0.024 | |
| 785 (73.5) | 371 (80.5) | 0.003 | 0.174 | 370 (80.3) | 371 (80.5) | 1.000 | 0.005 | |
| Calcium channel blockers (%) | 100 (9.3) | 40 (8.7) | 0.761 | 0.002 | 41 (8.9) | 40 (8.7) | 1.000 | 0.008 |
| Nitrates (%) | 571 (53.2) | 156 (33.8) | 0.398 | 160 (34.7) | 156 (33.8) | 0.835 | 0.018 | |
| Diuretic (%) | 517 (48.2) | 159 (34.5) | 0.281 | 178 (38.6) | 159 (34.5) | 0.218 | 0.086 | |
| Statins (%) | 1043 (97.2) | 460 (99.8) | 0.002 | 0.213 | 461 (100.0) | 460 (99.8) | 1.000 | 0.066 |
| Levosimendan (%) | 11 (1.0) | 5 (1.1) | 1.000 | 0.006 | 2 (0.4) | 5 (1.1) | 0.448 | 0.075 |
| Amiodarone (%) | 31 (2.9) | 8 (1.7) | 0.255 | 0.077 | 9 (2.0) | 8 (1.7) | 1.000 | 0.016 |
| Fib, g/L | 4.06 |
3.77 |
0.363 | 3.85 |
3.77 |
0.363 | 0.060 | |
| D-D, mg/L | 1.02 |
0.78 |
0.006 | 0.745 | 0.81 |
0.78 |
0.745 | 0.021 |
Footnotes: Data are presented as n (%) and the mean
Post-PSM, the differences were largely mitigated, enhancing comparability
between the groups. The proportions of men and the mean ages were balanced
(p = 1.000 and p = 0.970, respectively), and the distribution
of Killip classes was similar (p = 0.872). PCI usage varied
insignificantly (p = 0.761), although the PPCI rate remained slightly
higher in the ticagrelor group (69.6% versus 63.1%, p = 0.043),
representing potential residual confounding. Medication usage, including RASIs,
The clinical outcomes of the study, as detailed in Table 3 and Fig. 2, demonstrate significant differences in the effectiveness of ticagrelor compared with that of clopidogrel in patients with STEMI presenting with elevated platelet counts.
| Clopidogrel group | Ticagrelor group | p value | ||
| N = 461 | N = 461 | |||
| Primary outcome | ||||
| MACCE (%) | 56 (12.1) | 32 (6.9) | 0.008 | |
| Secondary outcomes | ||||
| NACE (%) | 60 (13.0) | 38 (8.2) | 0.021 | |
| All-cause Mortality (%) | 44 (9.5) | 18 (3.9) | ||
| Cardiac Deaths (%) | 34 (7.4) | 16 (3.5) | 0.0096 | |
| Recurrent MI (%) | 15 (3.3) | 11 (2.4) | 0.40 | |
| Revascularization (%) | 16 (3.5) | 19 (4.1) | 0.64 | |
| New Stroke (%) | 9 (2.0) | 6 (1.3) | 0.41 | |
| BARC type 3–5 (%) | 4 (0.9) | 6 (1.3) | 0.52 | |
Footnotes: The primary (MACCE: cardiac mortality, recurrent non-fatal myocardial
infarction, and cerebral infarction) and secondary (NACE: MACCE plus BARC type
3–5 bleeding events) endpoints are presented. Statistical significance was set
at p
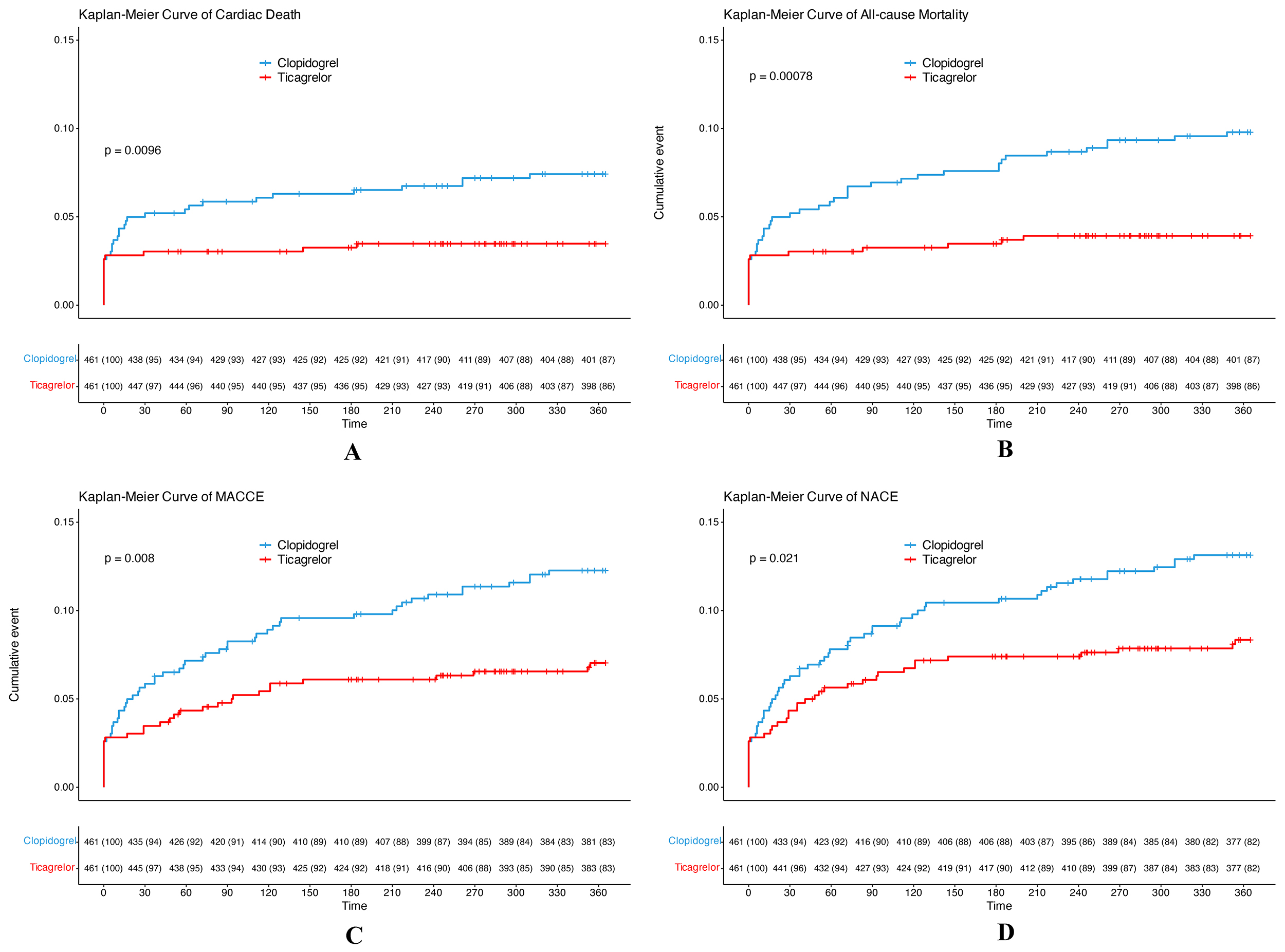 Fig. 2.
Fig. 2.
Kaplan–Meier survival curves illustrating cumulative incidences of various 1-year clinical outcomes in propensity score-matched patients ((A) Cardiac death; (B) All-cause death; (C) MACCE; and (D) NACE). Footnotes: The curves depict 1 minus the Kaplan–Meier survival probability, representing the cumulative incidence function. The step functions are constructed based on event times within specified intervals, with risk tables displaying at-risk numbers and censoring counts positioned below the x-axis at designated time points (days: 0, 30, 60, 90, 120, 150, 180, 210, 240, 270, 300, and 360). The y-axes are standardized to a 0%–25% scale. p values were obtained through a log-rank test comparing clopidogrel to ticagrelor within a propensity score-matched cohort (n = 461 per group at baseline). The analysis employed an intention-to-treat approach, with follow-up censored at 360 days or upon event/death. Abbreviations: MACCE, major adverse cardiac and cerebrovascular event (cardiac death/non-fatal myocardial infarction/cerebral infarction); NACE, net adverse clinical event (MACCE plus BARC type 3–5 bleeding).
The primary outcome, MACCE, was significantly less pronounced in the ticagrelor
group (6.9%) than in the clopidogrel group (12.1%, p = 0.008).
Similarly, NACE rates were significantly lower in the ticagrelor group (8.2%)
than in the clopidogrel group (13.0%, p = 0.021). Furthermore, the
ticagrelor group demonstrated a substantial reduction in all-cause mortality
(3.9%) relative to the clopidogrel group (9.5%, p
Nonetheless, other secondary outcomes—recurrent myocardial infarction, revascularization, new stroke, and “BARC type 3–5” bleeding events—revealed no significant differences between the two groups. Recurrent myocardial infarction incidence rates were 3.3% and 2.4% in the clopidogrel and ticagrelor groups, respectively (p = 0.40). The revascularization rate was 3.5% in the clopidogrel group and 4.1% in the ticagrelor group (p = 0.64). New strokes occurred in 2.0% and 1.3% of the clopidogrel and ticagrelor groups, respectively (p = 0.41). “BARC type 3–5” bleeding events were reported at 0.9% in the clopidogrel group and 1.3% in the ticagrelor group (p = 0.52). BARC type 3 or higher bleeding events refer to those classified by the BARC as types 3 to 5, as documented in the database.
Fig. 3 corroborates these conclusions by presenting aHRs and 95% CIs. The aHR
for MACCE was 0.59 (95% CI, 0.37–0.93; p = 0.02), indicating a
significantly reduced risk with ticagrelor. Regarding NACE, the aHR was 0.64
(95% CI, 0.42–0.98; p = 0.04). All-cause mortality yielded an aHR of
0.47 (95% CI, 0.26–0.83; p = 0.01), demonstrating a significant
survival benefit associated with ticagrelor. Nevertheless, no statistically
significant differences were noted for cardiac deaths, recurrent MI,
revascularization, new stroke, or “BARC type 3–5” bleeding events (p
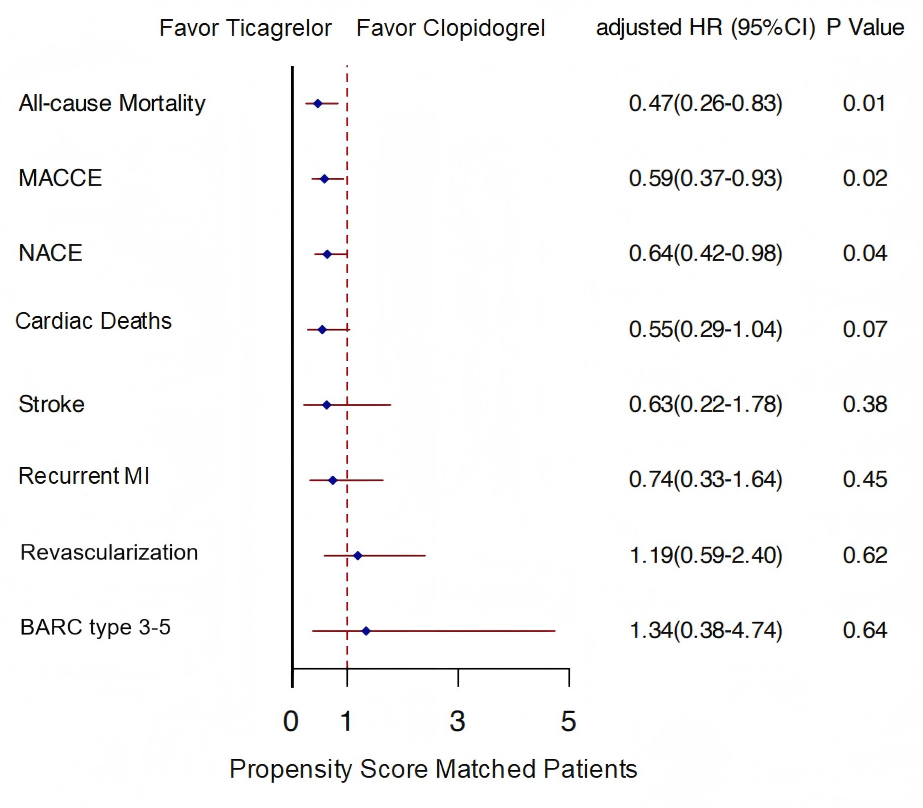 Fig. 3.
Fig. 3.
Adjusted forest plot of clinical outcomes with median follow-up
time. Footnotes: The forest plot displays exploratory multivariable-adjusted HRs with
95% CIs derived from Cox proportional hazards regression models within the
propensity score-matched cohort (N = 461 per group). The vertical line at HR =
1.0 indicates no difference between groups; points to the left of 1.0 favor
ticagrelor, whereas those to the right favor clopidogrel. Models were adjusted
for all baseline characteristics listed in Table 1 (including age, sex, Killip
class, comorbidities, and complications), as well as in-hospital treatments that
were significantly imbalanced after matching (primary PCI). The proportional
hazards assumption was verified using Schoenfeld residuals (global p
IPTW was applied to the entire pre-matching cohort for doubly robust estimation.
After IPTW, baseline characteristics were well balanced (all SMD
| Characteristic | Clopidogrel (weighted n = 1543.2) | Ticagrelor (weighted n = 1473.9) | p value | SMD | |
| Demographic | |||||
| Male (%) | 913.5 (59.2%) | 903.1 (61.3%) | 0.506 | 0.042 | |
| Age, years (mean |
60.03 |
59.13 |
0.283 | 0.066 | |
| Killip class (%) | 0.914 | 0.048 | |||
| I | 897.2 (58.1%) | 887.4 (60.2%) | |||
| II | 396.0 (25.7%) | 368.9 (25.0%) | |||
| III | 135.5 (8.8%) | 120.7 (8.2%) | |||
| IV | 114.4 (7.4%) | 96.9 (6.6%) | |||
| Complications | |||||
| Ventricular fibrillation (%) | 29.7 (1.9%) | 21.5 (1.5%) | 0.505 | 0.036 | |
| Ventricular tachycardia (%) | 64.1 (4.2%) | 36.3 (2.5%) | 0.170 | 0.095 | |
| Third-degree atrioventricular block (%) | 15.2 (1.0%) | 16.3 (1.1%) | 0.861 | 0.012 | |
| Comorbidities | |||||
| Diabetes mellitus (%) | 582.8 (37.8%) | 543.5 (36.9%) | 0.776 | 0.018 | |
| Hypertension (%) | 556.8 (36.1%) | 567.9 (38.5%) | 0.442 | 0.051 | |
| Atrial fibrillation (%) | 198.4 (12.9%) | 142.4 (9.7%) | 0.118 | 0.101 | |
| Hyperlipidemia (%) | 571.9 (37.1%) | 545.0 (37.0%) | 0.978 | 0.002 | |
| Chronic obstructive pulmonary disease (%) | 34.3 (2.2%) | 24.5 (1.7%) | 0.492 | 0.041 | |
| Stroke (%) | 266.3 (17.3%) | 237.0 (16.1%) | 0.623 | 0.032 | |
| Cerebral hemorrhage (%) | 53.2 (3.4%) | 48.4 (3.3%) | 0.879 | 0.009 | |
| Renal insufficiency (%) | 230.7 (14.9%) | 297.0 (20.1%) | 0.053 | 0.137 | |
| Previous PCI (%) | 24.7 (1.6%) | 4.6 (0.3%) | 0.015 | 0.133 | |
IPTW, inverse probability treatment weighting; PCI, percutaneous coronary intervention.
| Outcome | HR | 95% CI lower | 95% CI upper | p value |
| All-cause death | 0.557 | 0.299 | 1.036 | 0.064 |
| MACCE | 0.605 | 0.378 | 0.969 | 0.036 |
| NACE | 0.654 | 0.425 | 1.008 | 0.054 |
| Myocardial infarction | 0.779 | 0.366 | 1.657 | 0.516 |
| Revascularization | 1.977 | 1.035 | 3.776 | 0.039 |
| New-onset stroke | 0.392 | 0.155 | 0.991 | 0.048 |
| BARC 3 bleeding | 0.862 | 0.340 | 2.187 | 0.755 |
| Cardiovascular death | 0.668 | 0.347 | 1.288 | 0.229 |
IPTW, inverse probability treatment weighting; MACCE, major adverse cardiac and cerebrovascular event; NACE, net adverse clinical event; BARC, Bleeding Academic Research Consortium.
Sensitivity analyses stratified by treatment era (2010–2018 versus 2019–2023) showed consistent benefit of ticagrelor in the more recent period (2019–2023), with significant reductions in 1-year all-cause death (HR 0.412, 95% CI, 0.182–0.934), MACCE (HR 0.451, 95% CI, 0.244–0.834), and NACE (HR 0.503, 95% CI, 0.278–0.908), whereas no significant differences were observed in the earlier period (Table 6).
| Period | Outcome | HR | 95% CI | p value |
| 2010–2018 | DEATH_1Y | 0.507 | (0.185–1.388) | 0.187 |
| MACCE_1Y | 0.735 | (0.338–1.597) | 0.436 | |
| NACE_1Y | 0.819 | (0.408–1.645) | 0.574 | |
| MI_1Y | 1.909 | (0.427–8.532) | 0.397 | |
| Revascularization_1Y | 0.983 | (0.205–4.722) | 0.983 | |
| NGS_1Y | 0.541 | (0.144–2.023) | 0.361 | |
| BARC3-5_1Y | 3.086 | (0.141–67.623) | 0.474 | |
| CD_1Y | 0.863 | (0.308–2.420) | 0.780 | |
| 2019–2023 | DEATH_1Y | 0.412 | (0.182–0.934) | 0.034 |
| MACCE_1Y | 0.451 | (0.244–0.834) | 0.011 | |
| NACE_1Y | 0.503 | (0.278–0.908) | 0.023 | |
| MI_1Y | 0.362 | (0.134–0.983) | 0.046 | |
| Revascularization_1Y | 1.086 | (0.456–2.583) | 0.852 | |
| NGS_1Y | 1.780 | (0.154–20.581) | 0.644 | |
| BARC3-5_1Y | 1.965 | (0.192–20.156) | 0.570 | |
| CD_1Y | 0.405 | (0.165–0.996) | 0.049 |
MACCE, major adverse cardiac and cerebrovascular event; NACE, net adverse clinical event; BARC, Bleeding Academic Research Consortium; MI, myocardial infarction; NGS, new-onset stroke; CD, cardiac death.
Pre-specified subgroup analyses (age, sex, primary PCI, glycoprotein IIb/IIIa
inhibitor (GPI) use) showed no significant heterogeneity of treatment effect for
most outcomes, although numerical trends favoured greater benefit of ticagrelor
in patients without primary PCI and without GPI use (all p_interaction
Landmark analysis showed that the mortality benefit of ticagrelor was particularly pronounced beyond the first 30 days, with a significant reduction in all-cause death from day 31 to 365 (0.9% versus 4.6%; p = 0.001). The reduction in all-cause death within the first 30 days did not reach statistical significance (3.0% versus 5.0%; p = 0.179). For cardiovascular death, no statistically significant difference was noted in the first 30 days (3.0% versus 5.0%; p = 0.179), while a significant reduction was identified during the 31–365 day period (0.4% versus 2.4%; p = 0.025) (Table 7).
| Time period | Outcome | Clopidogrel (n = 461) | Ticagrelor (n = 461) | p value | SMD |
| 0–30 days | All-cause death | 23 (5.0%) | 14 (3.0%) | 0.179 | 0.100 |
| Cardiovascular death | 23 (5.0%) | 14 (3.0%) | 0.179 | 0.100 | |
| 31–365 days | All-cause death | 21 (4.6%) | 4 (0.9%) | 0.001 | 0.229 |
| Cardiovascular death | 11 (2.4%) | 2 (0.4%) | 0.025 | 0.166 |
IPTW, inverse probability treatment weighting.
Utilizing the Tianjin Health and Medical Big Data Platform (2010–2023), this
multicenter retrospective cohort study performed the first direct comparison of
ticagrelor with clopidogrel in patients with STEMI presenting with admission
thrombocytosis (platelet count
Elevated platelet counts are a significant risk factor for cardiovascular
diseases, particularly myocardial infarction and stroke. When exceeding 350
Mechanistically, the advantages of ticagrelor over clopidogrel in this context arise from its more potent and reversible P2Y12 receptor inhibition, circumventing CYP2C19-dependent activation limitations. Furthermore, beyond stronger P2Y12 inhibition, ticagrelor exhibits pleiotropic effects that may be particularly relevant in the proinflammatory and prothrombotic milieu of thrombocytosis. By inhibiting the equilibrative nucleoside transporter 1 (ENT1), ticagrelor increases circulating adenosine, which exerts anti-inflammatory, vasodilatory, and microvascular protective effects. Elevated platelet counts are frequently reactive to systemic inflammation and are associated with endothelial dysfunction and impaired coronary microcirculation. These adenosine-mediated actions may therefore contribute additional benefit in this high-inflammatory-burden subgroup, complementing the primary antiplatelet effect and further explaining the pronounced ischemic and mortality reductions observed. For instance, ticagrelor has demonstrated potential in improving coronary microvascular function in experimental sepsis [19] and has exhibited satisfactory antiplatelet effects at lower doses compared with clopidogrel [20]. Additionally, ticagrelor and its active metabolites effectively inhibit platelet function [21].
These findings build upon extensive prior research evaluating antiplatelet therapy in STEMI, where ticagrelor has consistently outperformed clopidogrel in broader populations. The ESC guidelines advocate for ticagrelor as the first-line treatment option for patients with STEMI undergoing PCI [18]. Furthermore, post-PCI ticagrelor treatment is preferred for patients with the CYP2C19 loss-of-function allele to mitigate MACCE [22]. Prehospital administration of ticagrelor prior to PCI has yielded improved outcomes in patients with STEMI [23, 24, 25]. In a Korean study [17], ticagrelor was found to reduce the risk of MACCE in patients with AMI and multivascular disease compared to clopidogrel. Notably, the superior efficacy of ticagrelor observed in this study aligns with these prior findings. Although the high prevalence of CYP2C19 loss-of-function alleles in East Asian populations provides a plausible biological explanation for this consistent benefit, this study did not genotype patients, leaving the contribution of pharmacogenetic variations to our findings speculative and warranting further investigation. These benefits remained robust after adjustments for calendar time, site, and PPCI. A nationwide cohort study [26] suggests that ticagrelor may be beneficial in preventing post-myocardial infarction stroke in East Asian patients.
Although the lack of CYP2C19 genotyping is a limitation, admission platelet
count
With regard to safety, observational data comparing ticagrelor with clopidogrel are inconsistent. The PEGASUS–TIMI 54 trial [27] found ticagrelor to significantly reduce the incidence of cardiovascular death, myocardial infarction, and stroke, although it also resulted in an increased risk of major bleeding in patients with a myocardial infarction history extending beyond 1 year. Additionally, transitioning from clopidogrel to ticagrelor significantly improved 1-year clinical outcomes without an increased risk of bleeding [28]. Notwithstanding, most studies have not specifically investigated high platelet counts in patients with STEMI, limiting our understanding of this subgroup. To date, few studies have examined the prognosis of antiplatelet therapy in patients with STEMI and elevated platelet counts.
Regarding safety, the low absolute number of BARC type 3–5 bleeding events
(1.3% versus 0.9%, p = 0.52) precludes definitive conclusions about
bleeding risk and indicates limited statistical power for this low-event
endpoint, with a high risk of Type II error (false negative). However, in this
particularly high-thrombotic-risk cohort (admission platelet count
This study leveraged a vast dataset from 82 secondary and tertiary hospitals in Tianjin City, covering the 2010–2023 period and encompassing a sizable number of patients with AMI. This extensive sample size enhances statistical power and overall reliability. Furthermore, the analysis assessed multiple primary and secondary clinical outcomes, including MACCE, NACE, all-cause mortality, cardiac mortality, recurrent non-fatal myocardial infarction, coronary artery revascularization, stroke, and bleeding events (BARC type 3–5). Such a comprehensive evaluation enabled an in-depth comparison of the efficacy of ticagrelor against that of clopidogrel in patients with STEMI and thrombocytosis.
The observed benefits of ticagrelor—characterized by a significantly lower rate of cardiovascular events than that associated with clopidogrel, with a more pronounced advantage than in previous trials—are attributable to the high-risk patient population, optimized treatment protocols, and rigorous follow-up strategies. Additionally, the high prevalence of CYP2C19 intermediate metabolizers (approximately 40%–45%) within the Han population [29], driven by loss-of-function allele carrier rates of 38.6% for CYP2C192 and 5.2% for CYP2C193, likely enhanced the superiority of ticagrelor, as it circumvents the metabolic limitations of clopidogrel. Although pharmacogenetic data were not directly incorporated, this ethnic-specific context further strengthens the relevance of the findings for East Asian cohorts.
Despite the significantly lower incidence of cardiovascular events associated with ticagrelor than with clopidogrel—potentially attributable to the high-risk thrombocytosis subgroup, optimized protocols, and rigorous follow-up—several limitations warrant consideration.
First, as an administrative database study, endpoint classifications (for example, cardiac death and all-cause mortality) relied solely on ICD codes without independent adjudication of pathological causes, potentially introducing misclassification bias. Furthermore, the database did not capture detailed causes of cardiovascular death (for example, pump failure, reinfarction-related death, stent thrombosis, arrhythmic death, procedure-related death, or unknown cause), limiting the ability to perform sub-classifications and direct comparisons of incidence rates between groups. This constraint hinders a more comprehensive exploration of the factors driving survival benefits, suggesting that future studies should enhance detailed death adjudication.
Second, several non-fatal secondary endpoints exhibited low absolute event counts (for example, recurrent myocardial infarction: 11 versus 15; BARC type 3–5 bleeding: 6 versus 4), thus limiting the statistical power to detect meaningful differences. Additionally, post-PSM sample sizes (n = 461 per group) were modest, potentially yielding insufficient power for rarer outcomes and increasing the risk of false negatives.
Third, all data were sourced from hospitals in Tianjin, where regional variations in medical standards, treatment practices, and population characteristics limit the generalizability of the findings to broader Chinese or international populations. Caution is thus warranted when extrapolating results on a nationwide or global scale.
Fourth, despite stringent inclusion and exclusion criteria, residual selection bias might have persisted owing to patient heterogeneity, variability in treatment strategies, and inconsistencies in follow-up duration. The Killip classification, derived from discharge documentation, may not accurately reflect admission severity; although adjusted for shock proxies (vasopressors, intubation, and intra-aortic balloon pump/extracorporeal membrane oxygenation), residual misclassification remains possible and requires prospective validation. While temporal adjustments increased robustness, residual secular trends are acknowledged as limitations. Moreover, post-discharge medication adherence was unmeasured, and reactive thrombocytosis was not adjusted for owing to the unavailability of markers—factors warranting future exploration via claims data integration and marker assessment. Despite PSM and IPTW, residual confounding may persist, including the slight post-PSM imbalance in primary PCI rate (p = 0.043), which could influence ischemic outcomes favoring ticagrelor. However, the consistency of benefits in IPTW-adjusted models (which included reperfusion variables) and sensitivity analyses mitigates this concern.
Fifth, the database lacks longitudinal outpatient medication dispensing or refill data. As a result, post-discharge adherence to the initially prescribed P2Y12 inhibitor, rates of treatment switching, and discontinuation could not be evaluated. The intention-to-treat analysis assuming persistent exposure to the discharge medication may therefore underestimate or overestimate the true on-treatment effect of ticagrelor versus clopidogrel. Importantly, this limitation most likely introduces a conservative bias that underestimates the true magnitude of ticagrelor’s benefit. In an ITT framework, patients initially prescribed ticagrelor who subsequently discontinued therapy or switched to clopidogrel (e.g., due to dyspnea, cost, or physician preference) would be analyzed in the ticagrelor arm despite receiving reduced or no exposure to the drug. The fact that highly significant reductions in MACCE, all-cause mortality, and cardiac mortality were still observed despite this probable dilution of treatment effect strongly supports a robust biological advantage of ticagrelor in this high-thrombotic-risk population and validates the observed benefits. Future studies incorporating pharmacy claims linkage or prospective follow-up are needed to address adherence and persistence in this high-risk population. Future research should prioritize the assessment of bleeding risks across diverse platelet functional states and implement targeted preventive measures.
Additionally, due to the limited number of events (62 all-cause deaths and 50 cardiac deaths), the full multivariable Cox models that adjusted for nine prespecified covariates yielded a low events-per-variable ratio (approximately 6–7). These analyses are exploratory, and the multivariable-adjusted hazard ratios should therefore be regarded as exploratory and interpreted with caution. The primary evidence for the benefits of ticagrelor derives from the more robust propensity score-matched intention-to-treat comparison and doubly robust IPTW analyses, which are not subject to the same events-per-variable constraint.
Although the subgroup analyses were prespecified and adjusted for multiple comparisons where appropriate, the nominal interactions observed for MACCE (p_interaction = 0.039) and NACE (p_interaction = 0.047) in patients with versus without primary PCI should be interpreted with considerable caution. These interactions are driven by low event counts in several subgroups and composite endpoints that include non-fatal events of lesser clinical severity, rendering them underpowered for detecting true heterogeneity of treatment effect. Accordingly, no definitive claims of subgroup-specific differences are made, and the overall findings remain consistent across the majority of tested subgroups.
To address these limitations, subsequent studies should adopt prospective designs with comprehensive data collection (for instance, detailed death adjudication, genotype profiling, and precise timing of platelet measurements), minimize biases through multicenter recruitment, and enhance generalizability via nationwide cohorts.
In patients with STEMI and elevated admission platelet counts (
Please contact the corresponding authors for access to the data.
Conceptualization: FJJ, XS, TSG; Methodology: XS, TSG, YKZ; Software: TSG, YKZ; Validation: JKZ, XW; Formal Analysis: XS, TSG; Investigation: STH, CJ; Resources: XW, XL; Data Curation: STH, CJ; Writing – Original Draft: All authors; Funding Acquisition: TL, KYC, FJJ. Writing – Review & Editing: FJJ, XS; Visualization: YKZ, CJ; Supervision: SWR, TL, KYC. All authors contributed to the conception in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was conducted in accordance with the guiding principles of the Declaration of Helsinki and received approval from the Second Hospital of Tianjin Medical University (KY2023052-01). Written informed consent for participation was not required for this retrospective analysis in accordance with the national legislation and the institutional requirements.
The authors thank the staff and participants of the Tianjin Health and Medical Big Data Super Platform for their important contributions.
The work was funded by Tianjin Key Medical Discipline Construction Project (TJYXZDXK-3-006B); Key project of Tianjin Natural Science Foundation (21JCZDJC01080); The Tianjin Fourth Central Hospital’s 2023 Outstanding Young Talent Fund (tjdszxyy20230008); The National Science and Technology Innovation 2030, Noncommunicable Chronic Diseases-National Science and Technology Major Project (Grant No. 2024ZD0524300, 2024ZD0524301); The Tianjin Youth Project (No. TJWJ2022QN048).
The authors declare no conflicts of interest.The funders had no role in the design, analysis, interpretation of data, writing of the report, or decision to submit the article for publication. Tong Liu is serving as one of the Editorial Board members and Guest Editors of this journal. We declare that Tong Liu had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Lloyd W. Klein.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/RCM46358.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.