

 , Danqing Hu 4,†, Hong Zheng 1,2,3, Long Chen 5, Mingming Hu 5, Lianglong Chen 1,2,3,*
, Danqing Hu 4,†, Hong Zheng 1,2,3, Long Chen 5, Mingming Hu 5, Lianglong Chen 1,2,3,* , Wei Cai 1,2,3,*
, Wei Cai 1,2,3,*1 Department of Cardiology, Fujian Medical University Union Hospital, Fujian Medical University, 350001 Fuzhou, Fujian, China
2 Fujian Heart Medical Center, Fujian Medical University Union Hospital, Fujian Medical University, 350001 Fuzhou, Fujian, China
3 Fujian Institute of Coronary Artery Disease, Fujian Medical University Union Hospital, Fujian Medical University, 350001 Fuzhou, Fujian, China
4 School of Health, Fujian Medical University, 350122 Fuzhou, Fujian, China
5 Shanghai Pulse Medical Technology, Inc, 200030 Shanghai, China
†These authors contributed equally.
Abstract
The clinical impact of changes in the bifurcation angle throughout the cardiac cycle (BAC) after percutaneous coronary intervention (PCI) for left main coronary bifurcation lesions (LMCBLs) remains controversial, and the associated long-term evolution post-stenting remains unknown. Therefore, this study aimed to evaluate temporal changes in the BAC and the related impact on lesion progression in patients undergoing single- or dual-stenting.
Proximal (PBAC) and distal (DBAC) bifurcation angles were quantified throughout the cardiac cycle using two-dimensional quantitative coronary angiography at optimal views before the procedure, immediately after, and at long-term follow-up. These measurements represented the absolute difference between the end-diastolic and end-systolic angles for the left main (LM) to the left circumflex (LCX) and for the left anterior descending (LAD) to the LCX. Lesion progression was assessed from increases in diameter stenosis percentage (iDS%) from post-procedure to follow-up.
A total of 284 patients underwent single-stenting (LM-LAD), and 84 underwent dual stenting (LM-LAD-LCX). Changes in the PBAC were unaffected by interventional strategies or time. The DBAC was narrowed post-stenting in all patients, but rebounded to pre-procedural levels during follow-up in the single-stenting group. In contrast, the DBAC remained at post-procedural levels in the dual-stenting group. Lesion progression was more pronounced in patients with dual stenting, particularly in the LCX. The pre-procedural PBAC correlated linearly with the iDS%-LCX metric in the dual stenting.
The PBAC remained stable over time and across strategies, whereas the DBAC decreased post-stenting. During follow-up, the DBAC rebounded in the single-stenting group but remained low in the dual-stenting group. The pre-procedural PBAC represents an independent anatomical risk marker for future LCX progression in patients with dual-stented LMCBLs.
Keywords
- coronary artery disease
- anatomy
- cardiac cycle
- disease progression
- stents
Percutaneous coronary intervention (PCI) for left main coronary bifurcation lesion (LMCBL) is becoming increasingly common, as has been proven to be a reasonable option to coronary artery bypass grafting (CABG) surgery, especially in patients with a lower Syntax score [1, 2]. However, it remains inferior to CABG in the interventional treatment of complex LMCBL, primarily due to a higher rate of target lesion revascularization [3, 4]. Part of this challenge may stem from limitations in the angiographic classification systems used for procedural planning. The Medina classification, while widely adopted, does not incorporate the bifurcation angle (BA)—a fundamental anatomical characteristic. This omission limits its utility for comparing complex lesions and may contribute to clinical ambiguity and research stagnation [5].
Recognizing this gap, the Movahed classification was proposed as a more anatomically descriptive system that specifically includes the BA [6]. The development of this angle-inclusive classification underscores a growing consensus on the physiological importance of the BA. Indeed, substantial evidence links both the static BA and its change throughout the cardiac cycle (BAC) in LMCBL to an increased risk of restenosis, particularly after dual stenting [7, 8, 9, 10, 11]. Nevertheless, the precise prognostic value of BA/BAC remains inconsistent. For instance, a substudy of the SYNTAX trial found that post-procedural systolic-diastolic distal BA (between left anterior descending (LAD) and left circumflex (LCX)) was associated with higher 5-year event rates [12], whereas pre-procedural distal BA showed no significant correlation with outcomes at 12 months or 5 years [12, 13]. These highlight a key gap: the longitudinal evolution of BAC after stenting and its relationship with lesion progression are poorly understood.
Consequently, we performed this study to determine the temporal changes in BAC (pre-procedure, post-procedure and long-term follow-up) in LMCBL patients, who underwent PCI using either a single stenting or dual stenting technique, and the relation between BAC and lesion progression.
This retrospective study was conducted at Fujian Medical University Union
Hospital between January 2013 and December 2021. We consecutively enrolled
patients with LMCBL who had undergone PCI and had completed follow-up coronary
angiography at a minimum of 6 months. Eligible patients needed to have angiograms
available for BAC analysis at three time points: pre-procedure, immediately
post-procedure, and at long-term follow-up, covering both left main (LM) to LAD
single stenting and LM-LAD-LCX dual stenting techniques. Key exclusion criteria
were: (1) a history of CABG; (2) an excessively short LM length (
In view of the disparity between the three-dimensional (3D) angiographic reconstruction and the actual coronary artery in LMCBL, and given that our study’s target variable is the range of BA between diastole and systole in LMCBL patients over time, our study performed the BAC analysis from the two-dimensional (2D) optimal view of left main bifurcation angiogram at the three specified time points, maintaining consistent optimal views throughout (pre-procedure, post-procedure, and long-term follow-up). Experienced analysts conducted BAC and quantitative coronary angiography (QCA) measurements of the LMCBL from these optimal angiograms at the aforementioned three time points using AngioPlus software (Ver. 2.0, Pulse Medical Imaging Technology, Shanghai, China).
The BA in LMCBL was presented in accordance with the European Bifurcation Club consensus [14]. The proximal bifurcation angle (PBA) in LMCBL was defined as the angle between LM and LCX, while the distal bifurcation angle (DBA) in LMCBL was delineated between LAD and LCX. Angles at end-diastole and end-systole, both before and immediately after the interventional procedure, as well as during long-term follow-up, were concurrently evaluated. The ranges of PBA and DBA throughout the cardiac cycle were expressed as PBAC and DBAC, representing the absolute difference between the end-diastolic and end-systolic angle values.
Long-term lesion progression was determined by the change in percent diameter stenosis (DS%) from post-procedure to long-term follow-up. This was expressed as an increase in DS% (iDS%) across three segments of the LMCBL.
All statistical analyses were performed with SPSS (version 24; SPSS Inc,
Chicago, IL, USA). Continuous variables were tested for normality using the
Shapiro-Wilk test and were presented as mean
The reproducibility of pre-procedural bifurcation angle measurements was assessed by evaluating both intra- and inter-observer variability. A randomly selected sample of 40 patients (20 from each stenting group) was used for this analysis. Measurements were performed by the primary observer and an independent observer following standardized procedures. Reliability was quantified using the Intraclass Correlation Coefficient (ICC) with a two-way random-effects model for absolute agreement.
Hierarchical multiple linear regression was performed to investigate whether BAC was a significant predictor for iDS%, after accounting for the predictive contribution of previously identified arteriosclerosis-related demographic and interventional variables. The regression model consisted of three separate blocks of variables, with categorical variables being transformed into dummy variables. In the regression model, age, gender, the time of follow-up, body mass index (BMI), diabetes mellitus, hypertension, current smoking, dyslipidemia, low-density lipoprotein cholesterol (LDL-C), left ventricular ejection fraction (LVEF), the use of intravascular ultrasound (IVUS) or optical coherence tomography (OCT), and the DS% immediately post-procedure were entered in the first block. Interventional strategies, including single stenting and dual stenting in LMCBL, were entered in the second block. Next, BAC (PBAC and DBAC) measured before and immediately after the procedure were entered in the third block. The R2 changed for each block was tested.
The analytical framework of this study distinguished between descriptive comparisons and the core, pre-specified inferential analyses. Comparisons of baseline and follow-up characteristics were primarily descriptive and exploratory, whereas the study’s main conclusions were based strictly on the hierarchical multiple regression and associated correlation analyses.
A total of 368 LMCBL patients were included in this study, stratified according
to the interventional strategies, with 284 patients undergoing PCI using a single
stent from the LM to the LAD (single stenting group), and 84 patients undergoing
PCI with dual stenting in the LM-LAD-LCX (dual stenting group). There were no
significant differences in baseline characteristics between the two groups,
except for the percentage of dyslipidemia, as shown in Table 1. Second-generation
drug-eluting stents were implanted in all included patients. The population was
predominantly male (299 patients, 81.3%) and had a mean age of 65.3
| All patients (n = 368) | Single stenting (n = 284) | Dual stenting (n = 84) | p value | |
| Age at baseline, years | 65.3 |
65.3 |
65.6 |
0.820 |
| Male gender, n (%) | 299 (81.3%) | 232 (81.7%) | 67 (79.8%) | 0.691 |
| BMI, kg/m2 | 24.2 (22.1–26) | 24.2 (22.1–26.2) | 24.1 (22.1–25.4) | 0.393 |
| Prior myocardial infarction, n (%) | 58 (15.8%) | 43 (15.1%) | 15 (17.9%) | 0.548 |
| Diabetes mellitus, n (%) | 133 (36.1%) | 109 (38.4%) | 24 (28.6%) | 0.100 |
| Hypertension, n (%) | 242 (65.8%) | 189 (66.5%) | 53 (63.1%) | 0.558 |
| Dyslipidemia, n (%) | 132 (35.9%) | 110 (38.7%) | 22 (26.2%) | 0.035 |
| Current smoking, n (%) | 127 (34.5%) | 99 (34.9%) | 28 (33.3%) | 0.796 |
| Total cholesterol, mmol/L | 3.9 (3.3–4.9) | 4 (3.3–4.9) | 3.9 (3.4–4.6) | 0.999 |
| LDL-C, mmol/L | 2.5 (2–3.3) | 2.5 (2–3.4) | 2.4 (2–3.1) | 0.751 |
| HDL-C, mmol/L | 1 (0.8–1.1) | 1 (0.8–1.1) | 1 (0.9–1.1) | 0.490 |
| Serum creatinine, μmol/L | 80 (69–93.8) | 80 (70–94) | 78.5 (67–92.8) | 0.369 |
| LVEF, % | 64 (56.3–68.8) | 63 (56.1–68.7) | 65.3 (57.4–69.6) | 0.203 |
| Follow-up, days | 379 (361–439.8) | 381 (361–461.3) | 378 (359.3–419.3) | 0.407 |
| Intermediate coronary artery, n (%) | 51 (13.9%) | 46 (16.2%) | 5 (6%) | 0.017 |
| IVUS/OCT, n (%) | 115 (31.3%) | 91 (32%) | 24 (28.6%) | 0.547 |
| Rotational Atherectomy, n (%) | 18 (4.9%) | 13 (4.6%) | 5 (6%) | 0.822 |
Values were n (%), mean
BMI, body mass index; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; LVEF, left ventricular ejection fraction; IVUS/OCT, intravascular ultrasound/optical coherence tomography.
The morphologies observed in LMCBL were not comparable, with fewer occurrences of the intermediate coronary artery in the dual stenting group. However, the usage of intracoronary imaging devices (IVUS/OCT) was similar between groups, as was the incidence of severe calcification lesions requiring rotational atherectomy.
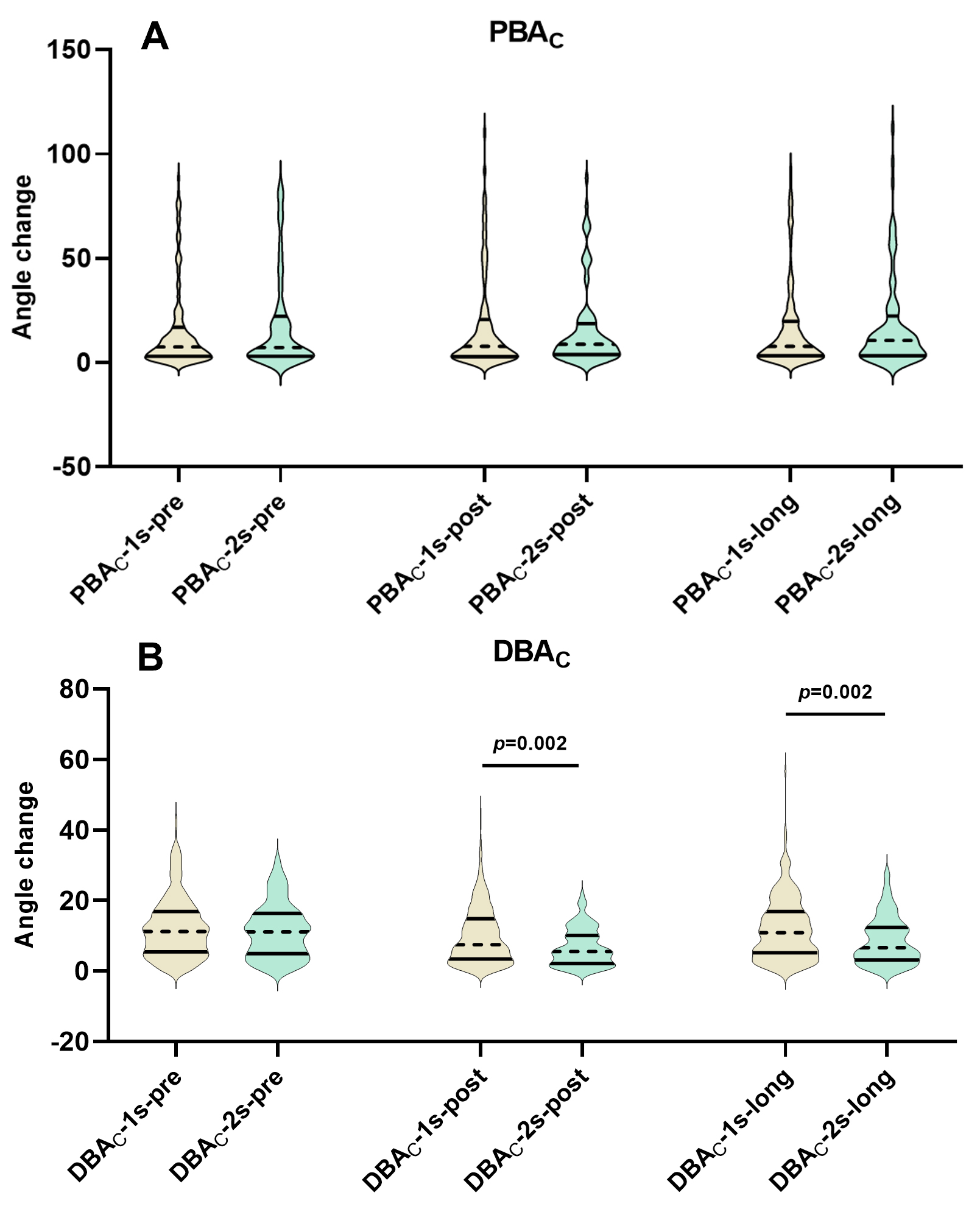
The analysis demonstrated excellent reproducibility for BAC measurements. The intra-observer ICC was 0.99 (95% CI: 0.99–1.00) for pre-procedural PBAC and 0.97 (95% CI: 0.94–0.98) for pre-procedural DBAC. The inter-observer ICC was 0.99 (95% CI: 0.99–1.00) for PBAC and 0.98 (95% CI: 0.97–0.99) for pre-procedural DBAC. The details of PBAC and DBAC between the two groups were shown in Tables 2,3. Regarding PBAC, whether before procedure (PBAC-pre), post-procedure (PBAC-post), or during long-term follow-up (PBAC-long), there were no differences in terms of single or dual stenting in LMCBL, shown in Fig. 1A. The PBAC in the LMCBL using the single stenting technique, as well as the LMCBL with the dual stenting technique, were not subject to changes due to stent implantation and over time, as indicated in Fig. 2A.
| All patients (n = 368) | Single stenting (n = 284) | Dual stenting (n = 84) | p value | |
| Diastolic PBA-pre | 141.8 (102.3–165.5) | 143.1 (103–165.8) | 136.1 (94.7–164.5) | 0.408 |
| Systolic PBA-pre | 136.6 (106.4–162.1) | 137.4 (105.4–162.7) | 134.4 (108.6–159.2) | 0.929 |
| PBAC-pre | 7.4 (3.1–18.1) | 7.5 (3.1–17) | 7.2 (3–22.2) | 0.602 |
| Diastolic PBA-post | 126 (99.4–166) | 131.6 (101.7–166.9) | 113.6 (94.4–156.4) | 0.073 |
| Systolic PBA-post | 126.6 (106.4–163.3) | 130.9 (107.9–164.3) | 118.4 (103.8–155.1) | 0.159 |
| PBAC-post | 8.2 (3–19.7) | 7.8 (2.9–20.6) | 8.8 (3.8–18.7) | 0.720 |
| Diastolic PBA-long | 130.3 (101.1–162.8) | 131 (101–165.12) | 127.6 (101–157.8) | 0.455 |
| Systolic PBA-long | 130.9 (110.1–163.3) | 132.8 (110.7–164.1) | 123.4 (106.9–158.2) | 0.091 |
| PBAC-long | 8.4 (3.3–20.2) | 7.8 (3.3–19.8) | 10.6 (3.3–22.3) | 0.553 |
| Diastolic DBA-pre | 85.8 (68.8–101.4) | 86.1 (71–102.8) | 81.5 (63.3–96.8) | 0.029 |
| Systolic DBA-pre | 74.7 (60.7–90.2) | 75.5 (61.7–91.8) | 69.3 (56.2–87.3) | 0.028 |
| DBAC-pre | 11.2 (5.3–16.7) | 11.2 (5.5–16.9) | 11.1 (4.9–16.4) | 0.462 |
| Diastolic DBA-post | 81.3 (68.3–97.7) | 83.8 (70.9–100.3) | 73.8 (59.6–85.7) | |
| Systolic DBA-post | 73.6 (62.6–88.9) | 75.8 (63.5–90.5) | 70.1 (55.7–79.6) | |
| DBAC-post | 7.1 (3.1–13.2) | 7.5 (3.4–14.8) | 5.6 (2.1–10.1) | 0.002 |
| Diastolic DBA-long | 79 (67.6–96.6) | 82.8 (69.9–98.8) | 73 (57.7–84.2) | |
| Systolic DBA-long | 70.6 (59.8–83.1) | 72.1 (61.6–84.7) | 65 (56.6–77.3) | |
| DBAC-long | 9.9 (4.4–16.3) | 10.8 (5.2–16.9) | 6.7 (3.2–12.4) | 0.002 |
| DS%-pre in LM | 48.8 (28.1–64.1) | 47.3 (26.3–62.1) | 54 (34–69.7) | 0.004 |
| DS%-pre in LAD | 62.8 (54.1–68.9) | 62.4 (53.7–68.6) | 63.8 (54.8–70.2) | 0.495 |
| DS%-pre in LCX | 25.4 (16.4–46.1) | 20.4 (13.9–29.6) | 54.5 (46.2–60.8) | |
| DS%-post in LM | 2.8 (0–5.5) | 3 (0–5.7) | 2.2 (0–4.9) | 0.086 |
| DS%-post in LAD | 5.9 (3.2–8.8) | 5.7 (3.1–8.7) | 6.7 (3.6–10.1) | 0.179 |
| DS%-post in LCX | 22.7 (14.9–32) | 25.8 (19.6–34.5) | 10.7 (5.8–16.3) | |
| DS%-long in LM | 7 (4.9–11.1) | 6.8 (4.7–10.9) | 7.9 (5.3–11.7) | 0.217 |
| DS%-long in LAD | 10.2 (6.4–15.9) | 9.6 (6–14.9) | 12.2 (7.4–18.1) | 0.008 |
| DS%-long in LCX | 30.7 (21.9–40.9) | 31.6 (22.7–40.7) | 26 (17–43.9) | 0.040 |
| iDS%-LM | 3.4 (1.2–6.9) | 3.1 (1.1–6.5) | 4.7 (1.9–8.8) | 0.013 |
| iDS%-LAD | 2.9 (1.3–7.3) | 2.8 (1.2–6.5) | 4.2 (1.6–9.2) | 0.016 |
| iDS%-LCX | 2.6 (0.9–12.6) | 2.2 (0.7–6.5) | 15.6 (2.5–28.6) |
Note: p-values were for descriptive/exploratory purposes only, not for inferential testing of causality or efficacy. The study’s primary conclusions were based on pre-specified regression and correlation analyses. Values were median (interquartile range).
PBA, proximal bifurcation angle; DBA, distal bifurcation angle; PBAC, PBA change throughout the cardiac cycle; DBAC, DBA change throughout the cardiac cycle; PBA/DBA-pre, PBA/DBA-post and PBA/DBA-long, PBA/DBA pre-procedure, post-procedure, and at long-term follow-up; PBAC/DBAC-pre, PBAC/DBAC-post and PBAC/DBAC-long, PBAC/DBACpre-procedure, post-procedure, and at long-term follow-up; DS%, percent diameter stenosis; iDS%, increase in DS%; DS%-pre, DS%-post and DS%-long, DS% pre-procedure, post-procedure, and at long-term follow-up; LM, left main; LAD, left anterior descending; LCX, left circumflex; iDS%-LM, iDS%-LAD, and iDS%-LCX, iDS% in LM, LAD and LCX.
| Before procedure | Post procedure | Long-term follow-up | p value | |
| PBAC-all | 7.4 (3.1–18.1) | 8.2 (3–19.7) | 8.4 (3.3–20.2) | 0.453 |
| PBAC-single stenting | 7.5 (3.1–17) | 7.8 (2.9–20.6) | 7.8 (3.3–19.8) | 0.374 |
| PBAC-dual stenting | 7.2 (3–22.2) | 8.8 (3.8–18.7) | 10.6 (3.3–22.3) | 0.965 |
| DBAC-all | 11.2 (5.3–16.7) | 7.1 (3.1–13.2) | 9.9 (4.4–16.3) | |
| DBAC-single stenting | 11.2 (5.5–16.9) | 7.5 (3.4–14.8) | 10.8 (5.2–16.9) | |
| DBAC-dual stenting | 11.1 (4.9–16.4) | 5.6 (2.1–10.1) | 6.7 (3.2–12.4) |
Note: p-values were for descriptive/exploratory purposes only, not for inferential testing of causality or efficacy. The study’s primary conclusions were based on pre-specified regression and correlation analyses. Values were median (interquartile range).
PBAC, proximal bifurcation angle change throughout the cardiac cycle; DBAC, distal bifurcation angle change throughout the cardiac cycle; PBAC/DBAC-all, PBAC/DBAC in all included patients; PBAC/DBAC-single stenting, PBAC/DBAC in the single stenting group; PBAC/DBAC-dual stenting, PBAC/DBAC in the dual stenting group.
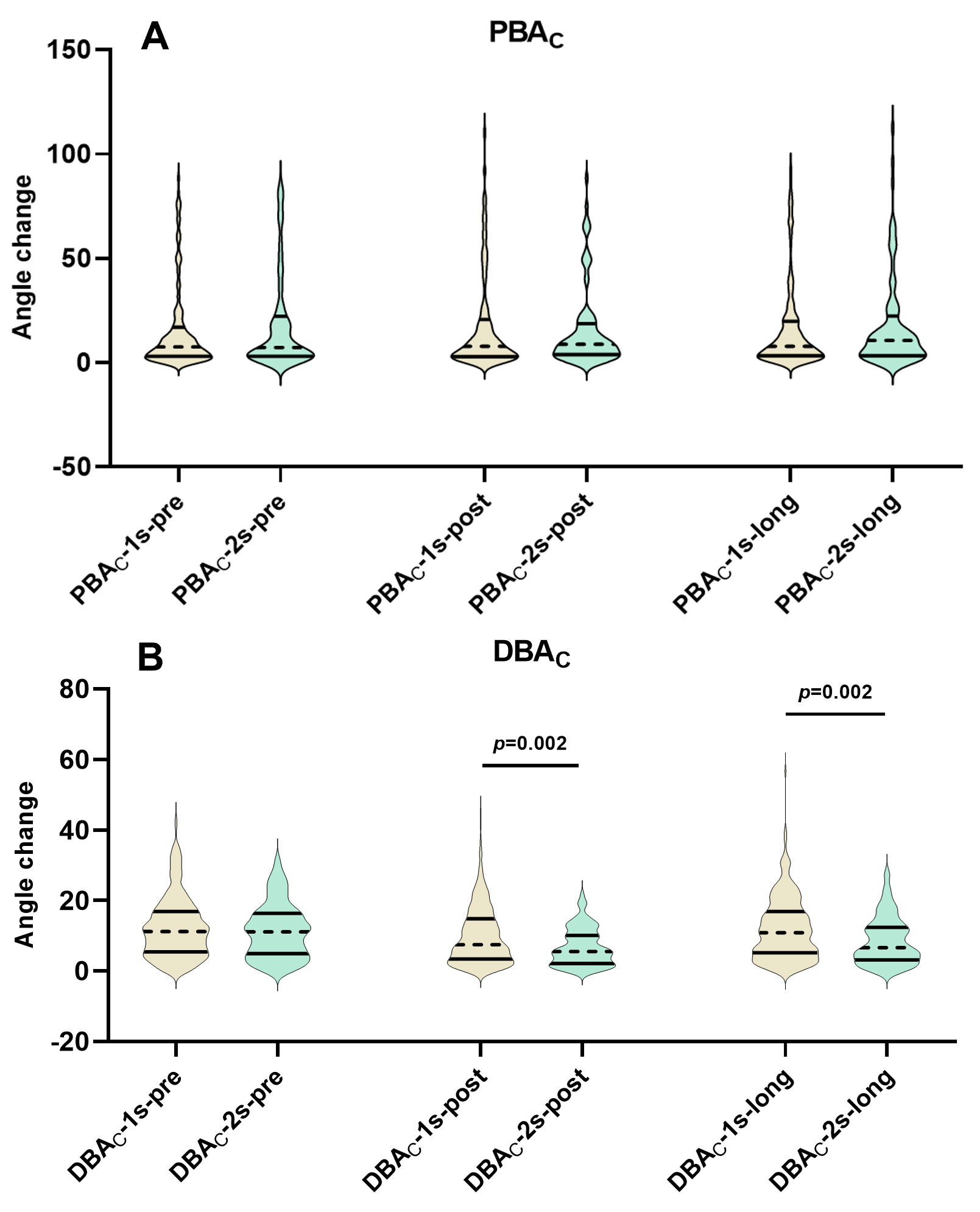 Fig. 1.
Fig. 1.
Temporal changes in PBAC and DBAC following single versus dual stenting. (A) Comparison of PBAC among pre-procedure, post-procedure and long-term follow-up assessments between the single and dual stenting strategies. (B) Comparison of DBAC among pre-procedure, post-procedure and long-term follow-up assessments between the single and dual stenting strategies. PBAC, proximal bifurcation angle change throughout the cardiac cycle; DBAC, distal bifurcation angle change throughout the cardiac cycle; PBAC/DBAC-1s-pre, PBAC/DBAC-1s-post and PBAC/DBAC-1s-long, PBAC/DBAC pre-procedure, post-procedure, and at long-term follow-up in distal left main bifurcation patients treated with single stenting; PBAC/DBAC-2s-pre, PBAC/DBAC-2s-post and PBAC/DBAC-2s-long, PBAC/DBAC pre-procedure, post-procedure, and at long-term follow-up in distal left main bifurcation patients treated with dual stenting.
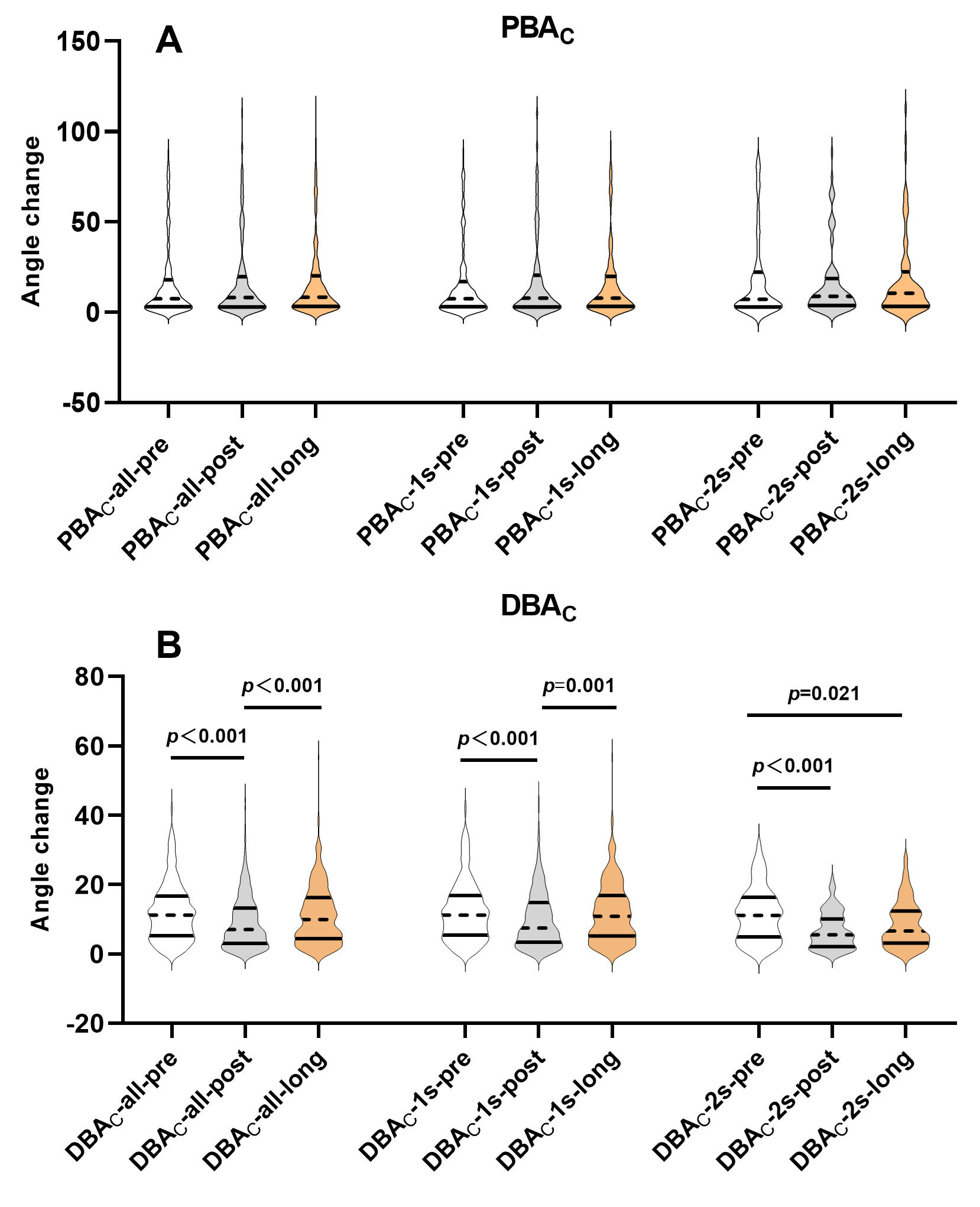 Fig. 2.
Fig. 2.
Temporal trends of PBAC and DBAC within single versus dual stenting groups. (A) PBAC compared across pre-procedural, post-procedural, and long-term follow-up time points within the single stenting group and separately within the dual stenting group. (B) DBAC compared across pre-procedural, post-procedural, and long-term follow-up time points within the single stenting group and separately within the dual stenting group. PBAC compared across pre-procedural, post-procedural, and long-term follow-up time points within the single stenting group and separately within the dual stenting group. PBAC, proximal bifurcation angle change throughout the cardiac cycle; DBAC, distal bifurcation angle change throughout the cardiac cycle; LMCBL, left main coronary bifurcation lesion; PBAC/DBAC-all-pre, PBAC/DBAC-all-post and PBAC/DBAC-all-long, PBAC/DBAC pre-procedure, post-procedure, and at long-term follow-up in all included patients; PBAC/DBAC-1s-pre, PBAC/DBAC-1s-post and PBAC/DBAC-1s-long, PBAC/DBAC pre-procedure, post-procedure, and at long-term follow-up in distal left main bifurcation patients treated with single stenting; PBAC/DBAC-2s-pre, PBAC/DBAC-2s-post and PBAC/DBAC-2s-long, PBAC/DBAC pre-procedure, post-procedure, and at long-term follow-up in distal left main bifurcation patients treated with dual stenting.
DBAC changes over time were displayed in Table 3 and Fig. 2B, indicating a
tendency for DBAC to narrow immediately post-stenting and subsequently widen
over time. This change was mainly observed in the single stenting group, which
exhibited similar DBAC-pre and DBAC-long values but lower
DBAC-post values (pre-procedure 11.2 (5.5–16.9) vs. post-procedure 7.5
(3.4–14.8) vs. long-term follow-up 10.8 (5.2–16.9), p
Furthermore, as depicted in Fig. 1B, when compared to the single stenting group, the dual stenting group exhibited a narrower DBAC-post (5.6 (2.1–10.1) vs. 7.5 (3.4–14.8), p = 0.002) and DBAC-long (6.7 (3.2–12.4) vs. 10.8 (5.2–16.9), p = 0.002), but with similar DBAC-pre (11.1 (4.9–16.4) vs. 11.2 (5.5–16.8), p = 0.462).
The QCA characteristics of LMCBL were presented in Tables 2,4. The dual
stenting techniques were applied to patients with more complex bifurcation
disease, particularly those with higher pre-procedural DS% in LM and LCX.
However, the progression across the three segments of LMCBL following stenting
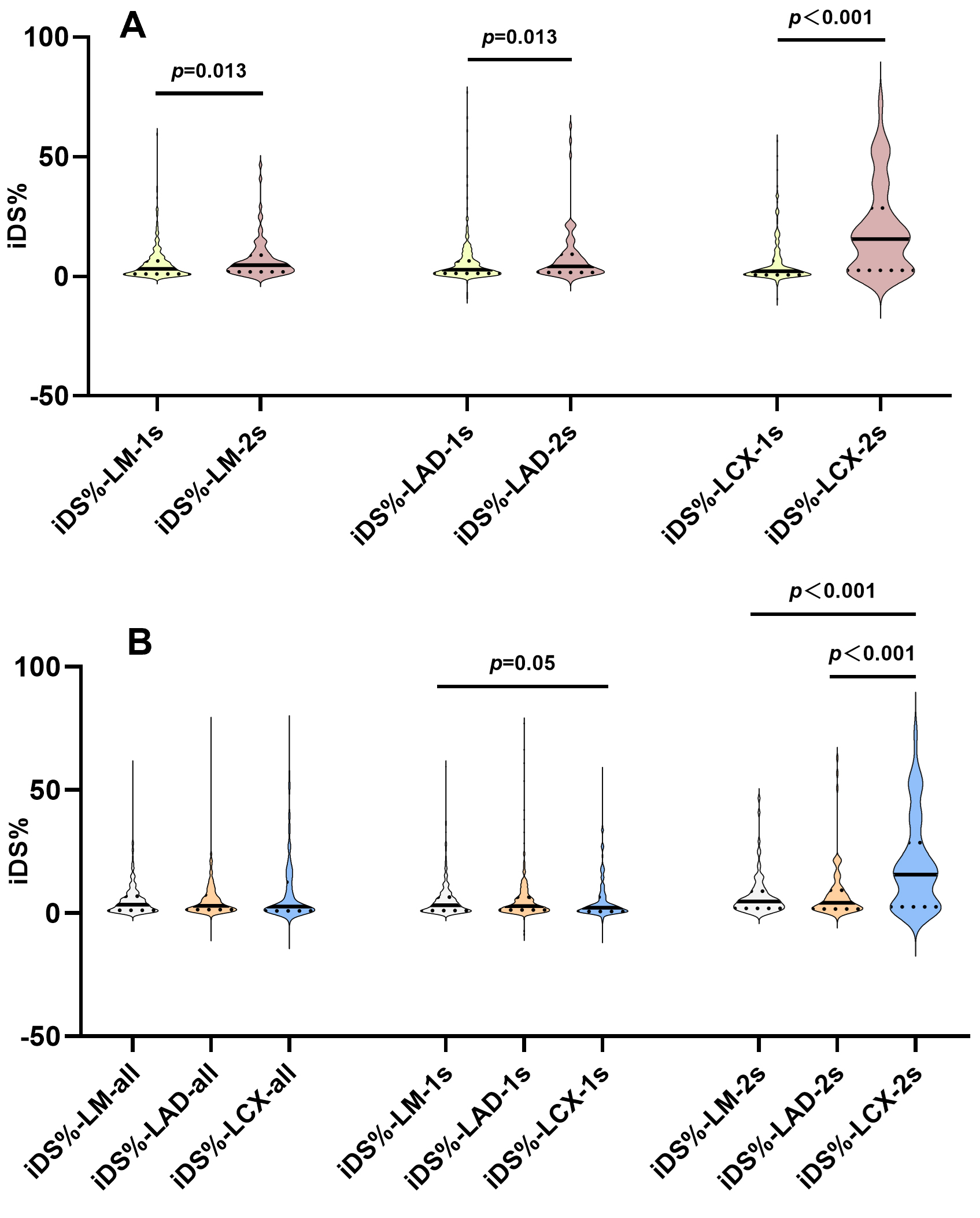
was more pronounced in patients treated with dual stenting technique (Fig. 3A),
especially in the LCX (single stenting: 2.2 (0.7–6.5) vs. dual stenting: 15.6
(2.5–28.6), p
| LM | LAD | LCX | p value | |
| iDS%-all | 3.4 (1.2–6.9) | 2.9 (1.3–7.3) | 2.6 (0.9–12.6) | 0.899 |
| iDS%-single stenting | 3.1 (1.1–6.5) | 2.8 (1.2–6.5) | 2.2 (0.7–6.5) | 0.027 |
| iDS%-dual stenting | 4.7 (1.9–8.8) | 4.2 (1.6–9.2) | 15.6 (2.5–28.6) |
Values were median (interquartile range).
iDS%, increase in percent diameter stenosis; LM, left main; LAD, left anterior descending; LCX, left circumflex; iDS%-all, iDS% in all included patients; iDS%-single stenting, iDS% in the single stenting group; iDS%-dual stenting, iDS% in the dual stenting group.
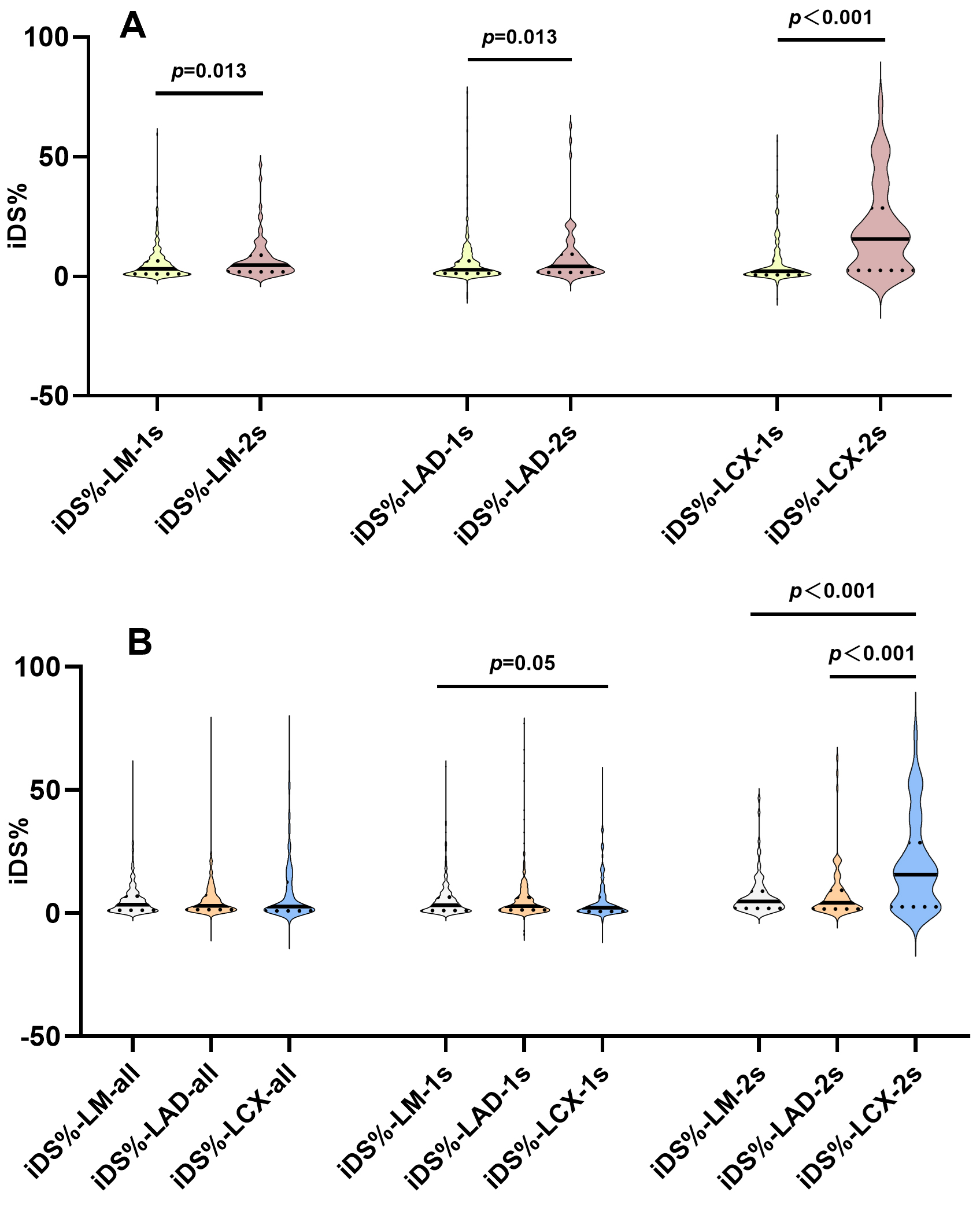 Fig. 3.
Fig. 3.
iDS% across bifurcation segments by stenting strategy. (A) Comparisons among iDS% in LM, LAD and LCX between the single and dual stenting groups. (B) Comparisons of iDS% in LM, LAD and LCX both in the single and dual stenting groups. iDS%, increase in percent diameter stenosis; LMCBL, left main coronary bifurcation lesion; LM, left main; LAD, left anterior descending; LCX, left circumflex; iDS%-LM-1s, iDS%-LAD-1s, and iDS%-LCX-1s, iDS% in LM, LAD and LCX in distal left main bifurcation patients treated with single stenting; iDS%-LM-2s, iDS%-LAD-2s, and iDS%-LCX-2s, iDS% in LM, LAD and LCX in distal left main bifurcation patients treated with dual stenting; iDS%-LM-all, iDS%-LAD-all, and iDS%-LCX-all, iDS% in LM, LAD and LCX in all included patients.
In the distinct individual iDS% across the three segments of LMCBL under the
two interventional strategies, we also compared the differences of iDS% among
the LM, LAD and LCX. As illustrated in Fig. 3B, in the single stenting group, the
discrepancy was attributed to the lower iDS%-LCX compared to iDS%-LM (2.2
(0.7–6.5) vs. 3.1 (1.1–6.5), p = 0.05). But in the dual stenting
group, the iDS%-LCX was significantly higher than both iDS%-LM (15.6
(2.5–28.6) vs.4.7 (1.9–8.8), p
Hierarchical multiple linear regression analysis (Table 5 and Supplementary Fig. 1) was conducted to
explore the factors associated with iDS%-LCX (the dependent variable), which was
prominent in the progression of LMCBL. Regression diagnostics confirmed that
model assumptions were reasonably met. One outlier with a standardized residual
slightly exceeding
| Variables predicting iDS%-LCX | B | SE | t | VIF | R | R2 | ||
| Block 1 | 0.327 | 0.107 | 0.107*** | |||||
| F = 3.554*** | ||||||||
| Age | –0.086 | 0.073 | –0.063 | –1.167 | 1.142 | |||
| Male | –0.251 | 1.892 | –0.007 | –0.133 | 1.215 | |||
| Female (Ref.) | ||||||||
| Follow-up | 0.002 | 0.001 | 0.058 | 1.131 | 1.032 | |||
| BMI | –0.118 | 0.239 | –0.026 | –0.493 | 1.111 | |||
| Diabetes mellitus | –0.519 | 1.450 | –0.019 | –0.358 | 1.082 | |||
| Hypertension | –1.453 | 1.495 | –0.052 | –0.972 | 1.123 | |||
| Current smoking | –0.010 | 1.545 | 0.000 | –0.006 | 1.203 | |||
| Dyslipidemia | –3.618 | 1.600 | –0.130 | –2.261* | 1.314 | |||
| LDL-C | 0.291 | 0.712 | 0.023 | 0.409 | 1.257 | |||
| LVEF | 0.004 | 0.063 | 0.004 | 0.071 | 1.035 | |||
| IVUS/OCT | 0.048 | 1.467 | 0.002 | 0.033 | 1.030 | |||
| DS%-post in LCX | –0.304 | 0.057 | –0.276 | –5.349*** | 1.059 | |||
| Block 2 | 0.469 | 0.220 | 0.113*** | |||||
| F = 7.684*** | ||||||||
| Age | –0.122 | 0.069 | –0.089 | –1.778 | 1.148 | |||
| Male | 0.326 | 1.772 | 0.010 | 0.184 | 1.218 | |||
| Female (Ref.) | ||||||||
| Follow-up | 0.001 | 0.001 | 0.044 | 0.912 | 1.034 | |||
| BMI | –0.089 | 0.223 | –0.020 | –0.397 | 1.111 | |||
| Diabetes mellitus | –0.483 | 1.357 | –0.017 | –0.356 | 1.082 | |||
| Hypertension | –0.744 | 1.403 | –0.026 | –0.530 | 1.128 | |||
| Current smoking | –0.013 | 1.446 | 0.000 | –0.009 | 1.203 | |||
| Dyslipidemia | –2.573 | 1.505 | –0.092 | –1.709 | 1.326 | |||
| LDL-C | 0.036 | 0.668 | 0.003 | 0.055 | 1.261 | |||
| LVEF | –0.018 | 0.059 | –0.015 | –0.306 | 1.038 | |||
| IVUS/OCT | 0.101 | 1.373 | 0.003 | 0.073 | 1.030 | |||
| DS%-post in LCX | –0.053 | 0.064 | –0.048 | –0.830 | 1.520 | |||
| LMCBL with single stenting (Ref.) | ||||||||
| LMCBL with dual stenting | 13.028 | 1.794 | 0.409 | 7.156*** | 1.484 | |||
| Block 3 | 0.483 | 0.233 | 0.013 | |||||
| F = 6.255*** | ||||||||
| Age | –0.118 | 0.069 | –0.086 | –1.713 | 1.162 | |||
| Male | 0.020 | 1.773 | 0.001 | 0.011 | 1.226 | |||
| Female (Ref.) | ||||||||
| Follow-up | 0.001 | 0.001 | 0.050 | 1.036 | 1.046 | |||
| BMI | –0.085 | 0.224 | –0.019 | –0.378 | 1.123 | |||
| Diabetes mellitus | –0.584 | 1.357 | –0.021 | –0.430 | 1.087 | |||
| Hypertension | –0.774 | 1.409 | –0.028 | –0.549 | 1.143 | |||
| Current smoking | –0.168 | 1.456 | –0.006 | –0.115 | 1.227 | |||
| Dyslipidemia | –2.511 | 1.506 | –0.090 | –1.667 | 1.334 | |||
| LDL-C | 0.103 | 0.669 | 0.008 | 0.153 | 1.274 | |||
| LVEF | –0.020 | 0.059 | –0.016 | –0.334 | 1.050 | |||
| IVUS/OCT | –0.143 | 1.377 | –0.005 | –0.104 | 1.043 | |||
| DS%-post in LCX | –0.051 | 0.064 | –0.046 | –0.795 | 1.528 | |||
| LMCBL with single stenting (Ref.) | ||||||||
| LMCBL with dual stenting | 12.915 | 1.837 | 0.406 | 7.029*** | 1.521 | |||
| PBAC-pre | 0.069 | 0.031 | 0.109 | 2.23* | 1.089 | |||
| DBAC-pre | –0.066 | 0.080 | –0.042 | –0.823 | 1.159 | |||
| PBAC-post | –0.028 | 0.028 | –0.048 | –1.004 | 1.059 | |||
| DBAC-post | 0.052 | 0.087 | 0.030 | 0.603 | 1.151 | |||
Note: Dependent variables was Y. “*p
iDS%, increase in percent diameter stenosis; LCX, left circumflex; iDS%-LCX, iDS% in LCX; BMI, body mass index; LDL-C, low-density lipoprotein cholesterol; LVEF, left ventricular ejection fraction; IVUS/OCT, intravascular ultrasound/optical coherence tomography; DS%-post, percent diameter stenosis post procedure; LMCBL with single stenting, LMCBL patients treated with single stenting technique; LMCBL with dual stenting, LMCBL patients treated with dual stenting technique; PBAC/DBAC-pre and PBAC/DBAC-post, PBAC/DBAC before and post procedure.
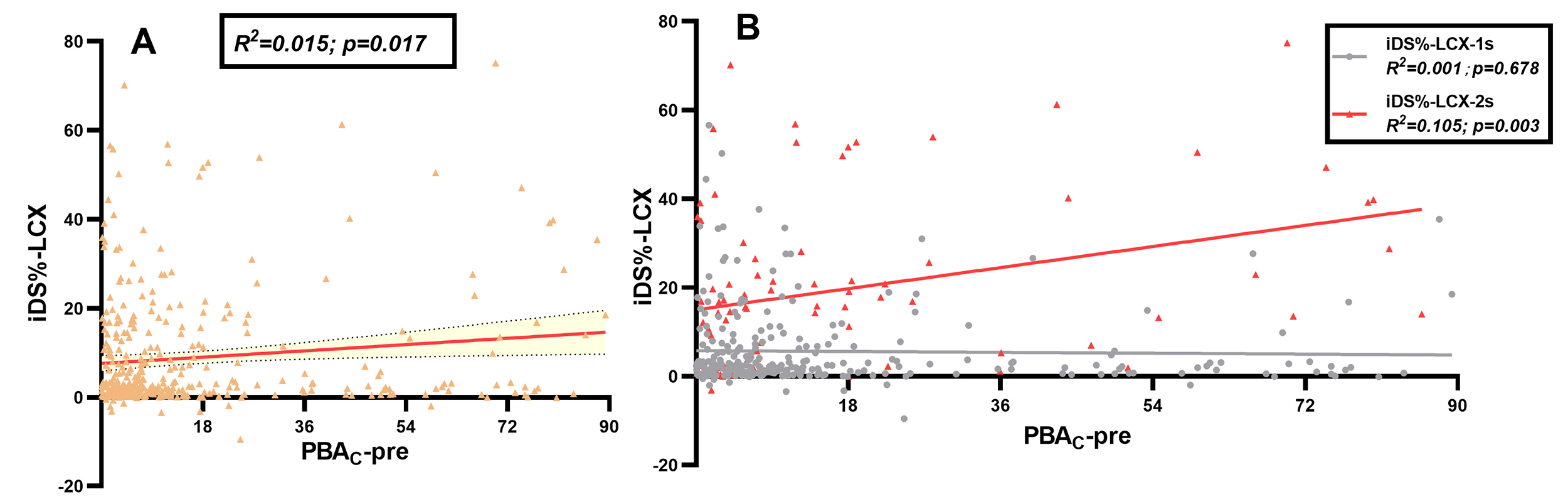
Moreover, as shown in Fig. 4A, the PBAC-pre exhibited a linear correlation with iDS%-LCX (R2 = 0.015, p = 0.017). Upon stratification by interventional strategies (Fig. 4B), it was observed that only the dual stenting technique exhibited a meaningful linear correlation (R2 = 0.105, p = 0.003). To assess the potential influence of sample size on our key finding, a post-hoc power analysis was performed. The result (power = 0.87) was statistically consistent with the observed significant p-value (p = 0.003), suggesting a low risk of a Type II error (i.e., missing an association of this magnitude) under the sample conditions of our study.
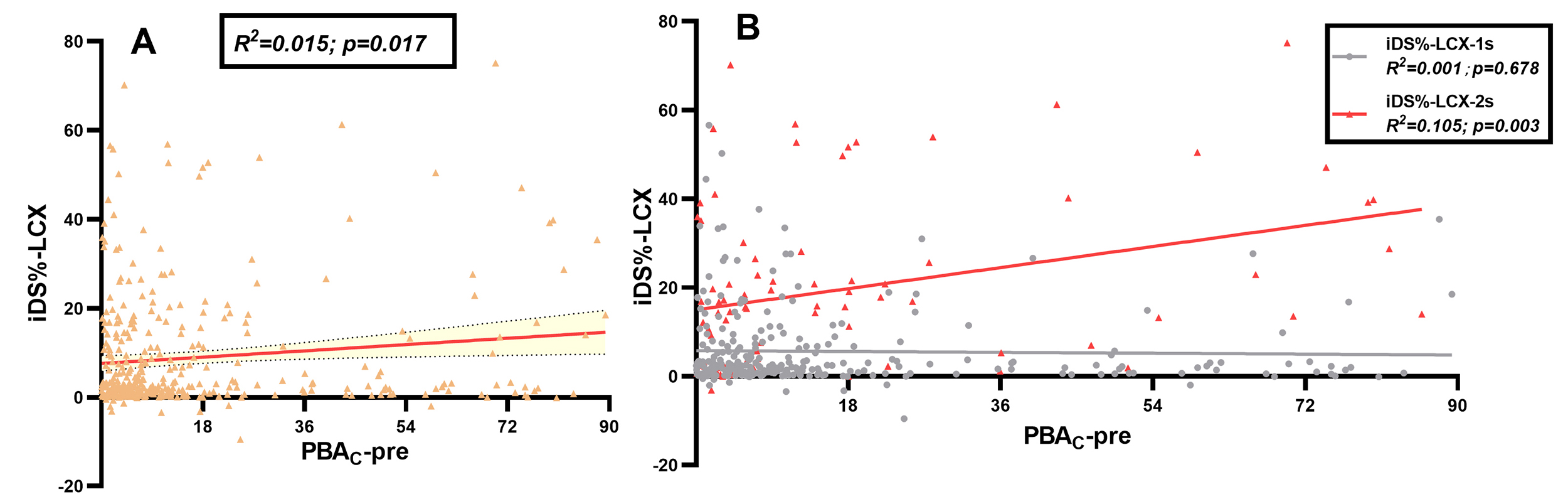 Fig. 4.
Fig. 4.
Correlation of pre-procedural PBAC with iDS% in LCX. (A) Correlation of iDS% in LCX and pre-procedural PBAC in all included patients. (B) Correlation of iDS% in LCX and pre-procedural PBAC, stratified by single and dual stenting. iDS%, increase in percent diameter stenosis; LCX, left circumflex; PBAC, proximal bifurcation angle change throughout the cardiac cycle; PBAC-pre, PBAC before procedure; iDS%-LCX, iDS% in LCX; iDS%-LCX-1s, iDS% in LCX in distal left main bifurcation patients treated with single stenting; iDS%-LCX-2s, iDS% in LCX in distal left main bifurcation patients treated with dual stenting.
Our study revealed several key findings: (1) In LMCBL patients, the temporal changes in PBAC were similar across the pre-procedural, post-procedural, and long-term follow-up assessments. Moreover, PBAC values did not differ significantly between patients who underwent single and dual stenting. (2) The DBAC among LMCBL patients who underwent single stenting showed a tendency to narrow immediately post-stenting and subsequently widened over time to the level of before procedure. However, in LMCBL patients treated with dual stenting, the DBAC remained at a reduced level during long-term follow-up, similar to that post-procedure. The extent of stent-induced DBAC reduction in LMCBL was more pronounced in the dual stenting group. (3) The progressions of lesions following stenting were notably pronounced in LMCBL patients subjected to dual stenting technique, especially in the LCX. (4) The pre-procedural PBAC was identified as an independent anatomical risk marker of future LCX progression in LMCBL patients treated with dual stenting technique.
Previous studies revealed that stent implantation in LMCBL could decrease the BA cyclic range, especially with the dual stenting technique. In the substudy of the SYNTAX trial, Girasis et al. [13] found that the diastolic DBA and DBA range through the cardiac cycle had decreased following stenting. Watanabe et al. [7, 11] had also found this trend in complex dual stenting. In the studies by Wang et al. [8], the restriction of cyclic angulation range for both BALM-LCX (defined as 180∘-PBA) and DBA had been detected among patients undergoing dual stenting. Our study confirmed the findings of prior research regarding DBAC, documenting a narrow tendency in LMCBL patients regardless of whether they were treated with the single or dual stenting. Furthermore, a more marked reduction in DBAC post-stenting was observed in LMCBL patients who received dual stenting compared to those undergoing single stenting. However, DBAC values were different during long-term follow-up, with a rebound to pre-procedural levels in the single stenting group and remaining at post-procedural levels in the dual stenting group.
The decrease in DBAC following stent implantation was attributed to the longitudinal straightening effect, which aligned with the myocardial motion during systole and contrasted during diastole, resulting in a reduction of the DBA throughout the cardiac cycle post-stent implantation [8]. However, in our study, we found that the most significant impact on DBAC was the side branch stenting, which not only caused a more significant decrease in the range of DBAC, but also disrupted the reverting effect during the long-term follow-up. The phenomenon of the reverting effect in DBAC following stenting occurred as the epicardial coronary arteries attempted to return to their original geometry by exerting periodic, repetitive strain on the metallic stent. Stent endothelialization and compression, or even fracture at the stent hinge point, might play a critical role in the process of reverting the effect in DBAC. However, in the dual stenting technique, the reverting effect was compromised due to the restriction of the side branch throughout the cardiac motion, and the change in bifurcation geometric shape was more pronounced. The excessive metal stent struts in the bifurcation core area might be the key factor preventing the bifurcation geometry from reverting to its preoperative state.
Conversely, the longitudinal straightening effect following stenting and the reverting effect over the long term were not statistically significant for PBAC. The temporal changes in PBAC differed from those of DBAC. At pre-procedural, post-procedural, and long-term follow-up assessments, values were similar in LMCBL patients regardless of whether they were treated with single or dual stenting. No difference was detected between the two interventional strategies. The distinction between DBAC and PBAC might be clarified by Torrent-Guasp’s spiral myocardial band theory [15, 16]. This theory suggested that myocardial contraction and relaxation did not occur as the inflation and deflation of a balloon. Instead, they originated at the base of the heart and propagated along the myocardial band, causing various parts of the heart to contract sequentially, similar to “twisting a towel in a spiral”. The near-multiple difference in the thickness of the left and right ventricular walls, resulting from the myocardial band wrapping around either once or twice, led to uneven strain on the PBAC and DBAC in LMCBL. The stent implantation, including dual stents, was unable to counteract the robust strain of myocardial contraction and relaxation, which might explain why PBAC maintains a comparable effect over time.
In our study, when compared to the single stenting group, the dual stenting group exhibited more severe lesion progression in the LM, LAD, and LCX. Furthermore, the iDS% in LCX was far exceeded those in the LM and LAD. The fastest progression for the single stenting group occurred in the LM, not in the LCX. These findings might indicate that the stent itself might serve as a predictor of lesion progression [17].
Regarding BAC, previous studies had failed to reach a consensus on clinical adverse events. Some suggested that pre-procedural DBAC contributed to the target lesion failure in LMCBL, others supported post-procedural DBAC, and still others believed that PBAC also played an important role. The hypothesis was that a larger BAC served as a surrogate for the greater hinge motion of coronary arteries, moving in step with cardiac motion. The implanted stents in LMCBL with larger BAC were exposed to more compression, torsion, kinking, elongation, bending, and shear stress due to cardiac contractions, which were associated with stent-related adverse events [7, 18].
When compared to the single stenting group, the extent of decreased DBAC post-stenting was more prominent in the dual stenting group, mainly driven by the multiple overlaps of metal stent struts at the ostium of side branches. The excessive overlap of metal stent struts in bifurcation core area was usually linked to clinical adverse events [19, 20]. Therefore, to some extent, the reported correlation between DBAC and target lesion failure could be transformed into the relationship between the overlap extent of metal stent struts in dual stenting approach and lesion progression.
However, in our study, except for pre-procedural PBAC in patients using the dual stenting, the DBAC was not associated with lesion progression, regardless of whether it was performed with a single or dual stenting technique. This seemed to contradict the aforementioned studies. The endpoints selected in our study were angiographic lesion progression, as assessed by QCA, whereas other studies chose target lesion failure or revascularization as their endpoints. The degree of lesion progression in other studies was much greater than in our study, which might be why previous studies were able to achieve positive results with a comparable sample size.
Our analysis identified a significant yet modest association between pre-procedural PBAC and lesion progression (iDS%-LCX) in the dual stenting group, accounting for approximately 10.5% of the variance. This finding aligned with the insights from Wang et al. [8], reinforcing the role of bifurcation anatomy in mechanistic environmental perturbations. Furthermore, the hierarchical regression demonstrated that pre-procedural PBAC provided independent predictive value beyond traditional atherosclerotic risk factors, which were not consistently correlated with progression in our model. This suggested that mechanical factors inherent to the bifurcation, partly captured by PBAC, played a distinct role. However, the mechanistic interpretation of these findings was limited by the absence of intracoronary imaging (IVUS/OCT), which precluded definitive insights into underlying factors such as stent expansion, apposition, or the extent of strut overlap [21, 22].
The identification of pre-procedural PBAC as an independent anatomical risk marker opened new avenues for future investigation. Prospective studies should aim to validate this association and explore whether combining pre-procedural PBAC with hemodynamic metrics (e.g., FFR), biomarkers, or advanced imaging modalities (e.g., IVUS/OCT) could lead to the development of a risk stratification model with greater predictive power (higher R2) and clinical utility. In this context, integrating PBAC assessment with intracoronary imaging represented a particularly promising path. Future studies could investigate the synergy whereby baseline PBAC informed anatomical planning, while IVUS/OCT provided direct verification of optimal stent deployment [23, 24], potentially enhancing the paradigm for optimizing left main bifurcation intervention.
This study had several limitations. First, it was retrospective and observational, with a limited sample size. Second, while selection bias due to the requirement for complete angiographic follow-up limited the external validity of our findings, it did not logically break the mechanistic link between variables within the studied cohort. Therefore, the internal validity of the association between pre-procedural PBAC and iDS%-LCX remained robust. Third, it was unclear whether the angiographic follow-up was routine or symptom-directed. However, our study detailed the angiographic restenosis in the LMCBL, which would more clearly exhibit lesion progression, rather than symptom-directed angiographic follow-up potentially driven by other vessels outside the LMCBL. Fourth, our study concentrated exclusively on the progression of lesions within three segments of the LMCBL, not investigating those outside the LMCBL. Furthermore, the correlations between BAC and clinical outcomes were not evaluated in our study. Fifth, the low utilization rate of intracoronary imaging devices meant that IVUS/OCT data were not obtained, which precluded a more mechanistic interpretation of the results. The potential impact of detailed interventional strategies should be specifically clarified in future studies, such as with or without a branch ostial optimization technique in the single stenting group, as well as provisional T, Culotte, and Crush techniques in the dual stenting group. Finally, a direct comparison between alternative techniques for assessing the cyclic BA range in LMCBL was not performed. This included, for instance, a comparison of 3D reconstruction against 2D consistent optimal view measurements across the pre-procedural, post-procedural, and long-term follow-up phases. Further studies are needed to explore the mechanism behind changes in BAC, thereby elucidating the correlation between BAC changes and lesion progression or adverse clinical events. In vitro dynamic bench tests and the application of intracoronary imaging devices could help to understand the relation between BAC changes and the overlap extent of metal stent struts in bifurcation core area.
The PBAC in LMCBL remained unaltered by interventional strategies and over time, whereas the DBAC significantly decreased immediately following stenting, particularly in the dual stenting approach. However, during long-term follow-up, it rebounded to pre-procedural levels in the single stenting group and remained at post-procedural levels in the dual stenting group. The pre-procedural PBAC emerged as an independent anatomical risk marker for lesion progression in the LCX following dual stenting. This exploratory finding warrants future prospective validation and may open new avenues for research into anatomical risk stratification.
PCI, Percutaneous coronary intervention; LMCBL, left main coronary bifurcation lesion; CABG, coronary artery bypass grafting; BA, bifurcation angle; LAD, left anterior descending; LCX, left circumflex; BAC, BA change throughout cardiac cycle; LM, left main; 3D, three-dimensional; 2D, two-dimensional; QCA, quantitative coronary angiography; PBA, proximal bifurcation angle; DBA, distal bifurcation angle; PBAC, PBA change throughout the cardiac cycle; DBAC, DBA change throughout the cardiac cycle; DS%, percent diameter stenosis; iDS%, increase in DS%; ICC, Intraclass Correlation Coefficient; BMI, body mass index; LVEF, left ventricular ejection fraction; LDL-C, low-density lipoprotein cholesterol; IVUS, intravascular ultrasound; OCT, optical coherence tomography; PBAC-pre, PBAC before procedure; PBAC-post, PBAC post-procedure; PBAC-long, PBAC during long-term follow-up; DBAC-pre, DBAC before procedure; DBAC-post, DBAC post-procedure; DBAC-long, DBAC during long-term follow-up; iDS%-LM, iDS% in LM; iDS%-LAD, iDS% in LAD; iDS%-LCX, iDS% in LCX.
All data reported in this paper are available from the corresponding author on reasonable request.
WC, LLC and EC conception and design of the study; EC, DQH, HZ, LC and MMH acquisition, analysis, and interpretation of data; HZ, LC and MMH quality control; WC and LLC critical revision of the manuscript for important intellectual content; EC and DQH drafting of the manuscript; HZ, LC and MMH reviewed, revised, and provided substantial intellectual input to the data-related sections of the manuscript. All authors give final approval of the version to be published. All authors agree to be accountable for all aspects of the work.
The research was conducted in compliance with the Declaration of Helsinki and the Ethical Review Measures for Life Sciences and Medical Research Involving Human Subjects. Additionally, the study was reviewed and approved by the Ethics Committee of Fujian Medical University Union Hospital (No. 2025KY120), and the informed consent was waived due to its retrospective nature.
Not applicable.
This study was funded by the National Natural Science Foundation of China (Grant No. 82170333 and 8201001030), Natural Science Foundation of Fujian Province (Grant No. 2021J01758) and Fujian provincial health technology project (Grant NO. 2020QNA035).
LC and MMH are employees of Shanghai Pulse Medical Technology and have a financial relationship with the company. However, the company had no role in the handling or conduct of the study. The authors had full access to all data in the study and take full responsibility for the integrity of the data and the accuracy of the data analysis. All other authors declare no potential conflicts of interest.
During the preparation of this work the authors used WPS AI in order to check spell and grammar. After using this tool, the authors reviewed and edited the content as needed and takes full responsibility for the content of the publication.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/RCM45495.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.