






 , Yongtai Gong 1, Yiqun Zhang 2, Danghui Sun 1, Yue Li 1,3,4,5,6,*
, Yongtai Gong 1, Yiqun Zhang 2, Danghui Sun 1, Yue Li 1,3,4,5,6,*
1 Department of Cardiology, The First Affiliated Hospital, Harbin Medical University, 150001 Harbin, Heilongjiang, China
2 The Vivolight Medical Device & Technology Co., Ltd., 518000 Shenzhen, Guangdong, China
3 NHC Key Laboratory of Cell Translation, Harbin Medical University, 150001 Harbin, Heilongjiang, China
4 Key Laboratory of Hepatosplenic Surgery, Harbin Medical University, Ministry of Education, 150001 Harbin, Heilongjiang, China
5 Key Laboratory of Cardiac Diseases and Heart Failure, Harbin Medical University, 150001 Harbin, Heilongjiang, China
6 Heilongjiang Key Laboratory for Metabolic Disorder & Cancer Related Cardiovascular Diseases, 150081 Harbin, Heilongjiang, China
Abstract
Precise coronary stent implantation is crucial for ostial and partial bifurcation lesions during percutaneous coronary intervention (PCI). Conventional post-dilation coronary stent implantation often causes longitudinal stent deformation (LSD); meanwhile, even a small area of protrusion into the proximal main branch (MB) can lead to severe problems. This study aimed to introduce a novel post-dilation technique, the proximal anchoring technique (PAT), and evaluate the associated feasibility and efficacy in achieving precise stent implantation and preventing LSD.
This bench study was performed in a tapered silicon vessel model, in which 3.5 × 28 mm-sized everolimus-eluting stents (Xience Xpedition™; Abbot, USA) were deployed at a nominal pressure. Post-dilation was conducted using two different strategies: the proximal anchor followed by distal post-dilation group (PAT group) and the conventional post-dilation group (dilation from distal to proximal) (D-P group). After each step, the subsequent changes in stent length were measured by optical coherence tomography (OCT). Additionally, three clinical PCI cases in which PAT and conventional post-dilation were employed are presented.
The longitudinal elongation of stents was significantly increased in the D-P group compared with the PAT group (p < 0.001). The OCT measurements showed that the stents were elongated during every step of the procedure in the D-P group (29.35 ± 0.10 mm vs. 29.65 ± 0.10 mm; p = 0.0054), but only slightly elongated in the first step of the post-dilation in the PAT group (28.73 ± 0.12 mm vs. 28.87 ± 0.12 mm; p = 0.2262).
We present a novel technique, PAT, to assist in more precise coronary stent implantation by preventing LSD for partial ostial and bifurcation lesions during PCI.
Keywords
- stent elongation and shortening
- post-dilation
- percutaneous coronary intervention
During percutaneous coronary interventions (PCI), complex coronary lesions, including aortic ostial lesions and partial bifurcation lesions (such as Medina 0,1,0 and 0,1,1 and 0,0,1), require precise stent deployment [1, 2]. Currently, there are several techniques to help accurate stent placement in the ostium including multiple angiographic views assist, the aorta flowing wire technique, the Szabo technique (anchor wire), and intra-luminal imaging assist [3, 4, 5]. However, the low accuracy, complex operation steps, high economic costs and increased complications have limited the clinical application of these methods [6].
Longitudinal stent deformation (LSD) is a relatively common complication during PCI procedures, which is defined as the distortion of a stent in the longitudinal axis [7, 8, 9, 10]. Although LSD is mainly described as focal or overall longitudinal stent shortening, recent studies have shown that longitudinal stent elongation was over four times more common than stent shortening in clinical practice [11, 12]. During aorta ostial lesion interventions, longitudinal stent elongation causes strut damage induced by the guiding catheter or the post-dilation balloon. This becomes a potential nidus for thrombus formation, plus difficulties with ostial catheter engagement and wire advancement during future catheterizations. Stents that are implanted too proximally in the side branch (SB) could cause struts to protrude into the main branch (MB), which may complicate future revascularization or lead to episodes of acute thrombosis. The problem of unintentional stent elongation and the accurate location of the proximal stent edge during PCI remains unresolved.
In this report, we introduce the proximal anchoring technique (PAT), which consists of the proximal portion of the stent with a non-compliant balloon size ratio 1:1 with the proximal reference vessel followed by distal sequential post-dilation. We evaluate the safety and effectiveness of the PAT in a series of clinical PCI cases, to achieve precise stent implantation and prevent the conventional post-dilation induced LSD.
Bench testing was performed for the PAT in a three dimensional (3D) printed, double-sided polished, pure saline-filled silicone tapered vessel phantoms (Shonankasei Co., Kanagawa, Japan). The procedures were performed by operators who had sufficient practical (human and bench) experience with PCI. Although clinically drug eluting stents (DES) and bioabsorbable scaffolding stents (BVS) are associated with more fractures than bare metal stents, the drug coating does not alter the potential for fracture of a stent platform on the bench [13, 14]. The Xience Xpedition™ everolimus-eluting coronary stent (Abbott, Abbott Park, IL, USA) was used for the experiments. The distal carina site of the vertical side branch was used as a marker to calculate the proximal length of stent elongation. The exact parameters of the tapered vessel phantom are shown in Supplementary Fig. 1.
After the PAT, optical coherence tomography (OCT) imaging was systematically performed to evaluate the relative length of stent elongation [15]. Pullback runs were performed at 20 mm/s with a Dragonfly™ Duo OCT catheter (Abbott Vascular, Temecula, CA, USA) and analysis was performed using a dedicated workstation (C7-XR™ OCT intravascular imaging system; Abbott Vascular). Images were recorded at 100 frames per second. The measurement parameters of the tapered vessel phantom by OCT are shown in Supplementary Fig. 2.
PAT was investigated both in a bench model and clinically in patients undergoing
PCI, with stents implanted precisely, followed by post-dilation of PAT. In this
in vitro model, a 3.5
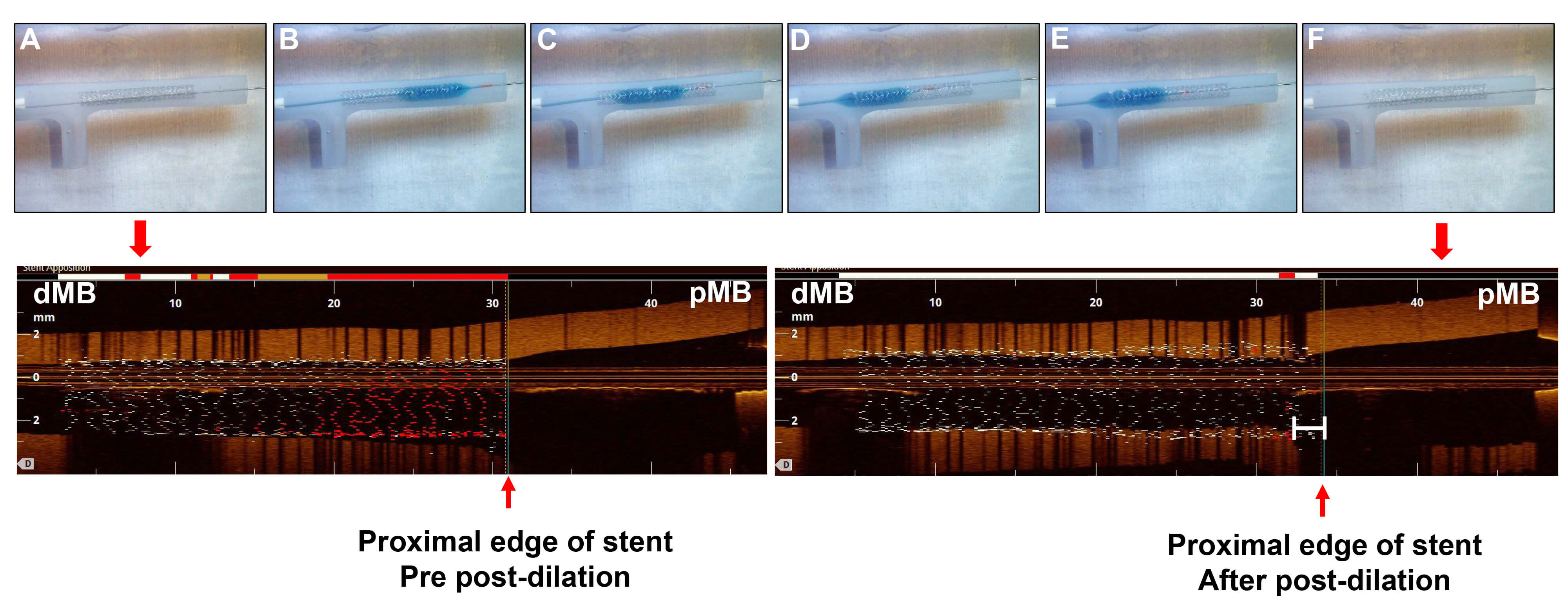 Fig. 1.
Fig. 1.
Study procedure of post-dilation from distal to proximal
direction. Upper panel: (A) A 3.5
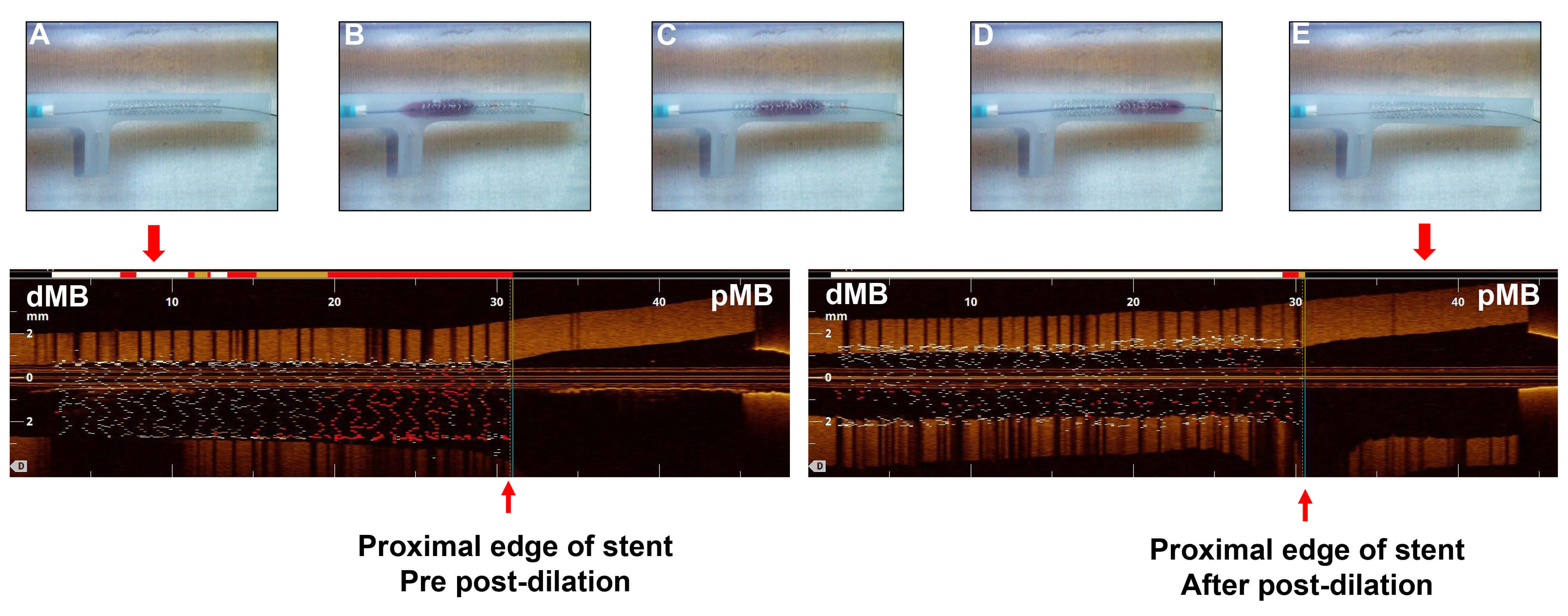 Fig. 2.
Fig. 2.
Study procedure of post-dilation from proximal to distal
direction. Upper panel: (A) A 3.5
In this group, after the precise stent placement at the ostium was performed,
the stent length and malposition were measured by OCT scans. Next, post-dilation
was performed from the distal to proximal stent at 12 atm, 15 atm, and 18 atm
respectively using a 3.5 mm
In this group, after the precise stent placement at the ostium was performed,
the stent length and malposition were measured by OCT scans. Post-dilation was
performed from the proximal to distal direction. First, post-dilation was
performed at the proximal edge of the stent by using a 4.0 mm
Every step of post-dilation was performed for 20 s. Each group’s bench test will undergo 3-4 repeated operations to ensure stable results. At the end of the procedure, the OCT scan was repeated to measure the stent length and to determine if there was any malposition.
The distribution of continuous variables was examined using the Shapiro–Wilk
test. The paired Student’s t-test was used to compare the stent length
before and after stent post-dilation during each step of the procedure.
Student’s t-test was used to compare the differences in the percentage
change of stent length during post-dilation between the D-P and PAT groups. All
calculations were performed using R software version 4.3.0 (https://www.r-project.org/) and Figures were
drawn using GraphPad Prism version 10.1.2 (GraphPad Software LLC, San Diego, CA, USA). A
p-value of
In the bench test, there were no differences in stent length between two groups immediately after stent deployment. In the D-P group, the stents were significantly elongated during the first and second post-dilations. However, in the PAT group, the stents were slightly elongated during the first post-dilation, whereas it was not significantly elongated during the second post-dilation (Table 1). In addition, the stent length after first and second post-dilation of PAT group were significantly shorter than that in D-P group (Table 1). Compared to the D-P group, the distance of the stent length proximally was significantly reduced in the PAT group after the first post-dilation, and the elongated distance was not statistically different after the second post-dilation between the two groups (Table 2). The total elongated distance was significantly shorter in PAT group than that in D-P group (Fig. 3).
| Nominal stent length (mm) | Immediately after stent deployment (mm) | p value (Nominal vs. Immediately) | After 1st post-dilation (mm) | p value (Immediately vs. 1st) | After 2nd post-dilation (mm) | p value (1st vs. 2nd) | |
| D-P group (n = 4) | 28.0 | 28.08 |
0.1586 | 29.35 |
29.65 |
0.0054 | |
| PAT group (n = 3) | 28.0 | 28.13 |
0.0750 | 28.73 |
0.0036 | 28.87 |
0.2262 |
D, distal; P, proximal; n, number of repetitions for the bench test; PAT, proximal anchoring technique. A p-value of statistical significance is shown in bold. **p
| After 1st dilation stent lengthened toward the proximal (mm) | p value (D-P vs. PAT) | After 2nd dilation stent lengthened toward the proximal (mm) | p value (D-P vs. PAT) | |
| D-P group (n = 4) | 1.28 |
0.0018 | 0.30 |
0.2534 |
| PAT group (n = 3) | 0.60 |
0.13 |
D, distal; P, proximal; n, number of repetitions for the bench test. A p-value of statistical significance is shown
in bold. ***p
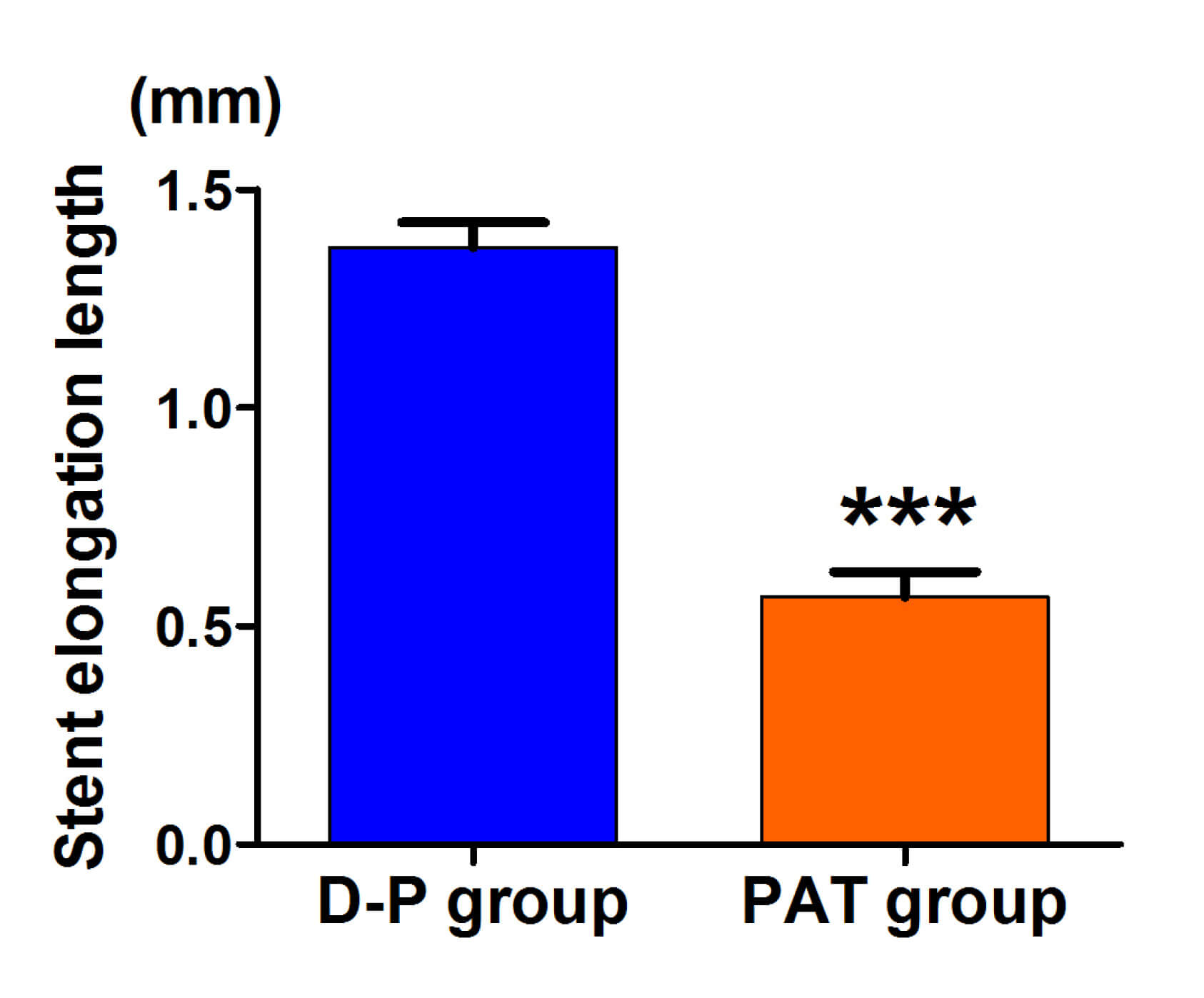 Fig. 3.
Fig. 3.
Stent elongation length in the PAT group and conventional post-dilation group. ***p
We describe clinical cases performed with precise stent location and followed by
PAT or conventional techniques distal to proximal post-dilation. The first
patient presented with left main (LM) moderate stenotic lesions and diffuse
moderate stenotic lesions of the left anterior descending (LAD) artery. After
pre-dilatation, two DES were sequentially implanted at the middle of the LAD to
the LM, and the proximal edge of stent was precisely located at the ostium of
aorta-to-coronary which was achieved by the flowing wire technique (Fig. 4A,B).
Then, sequential post-dilation was performed with PAT using a 4.0
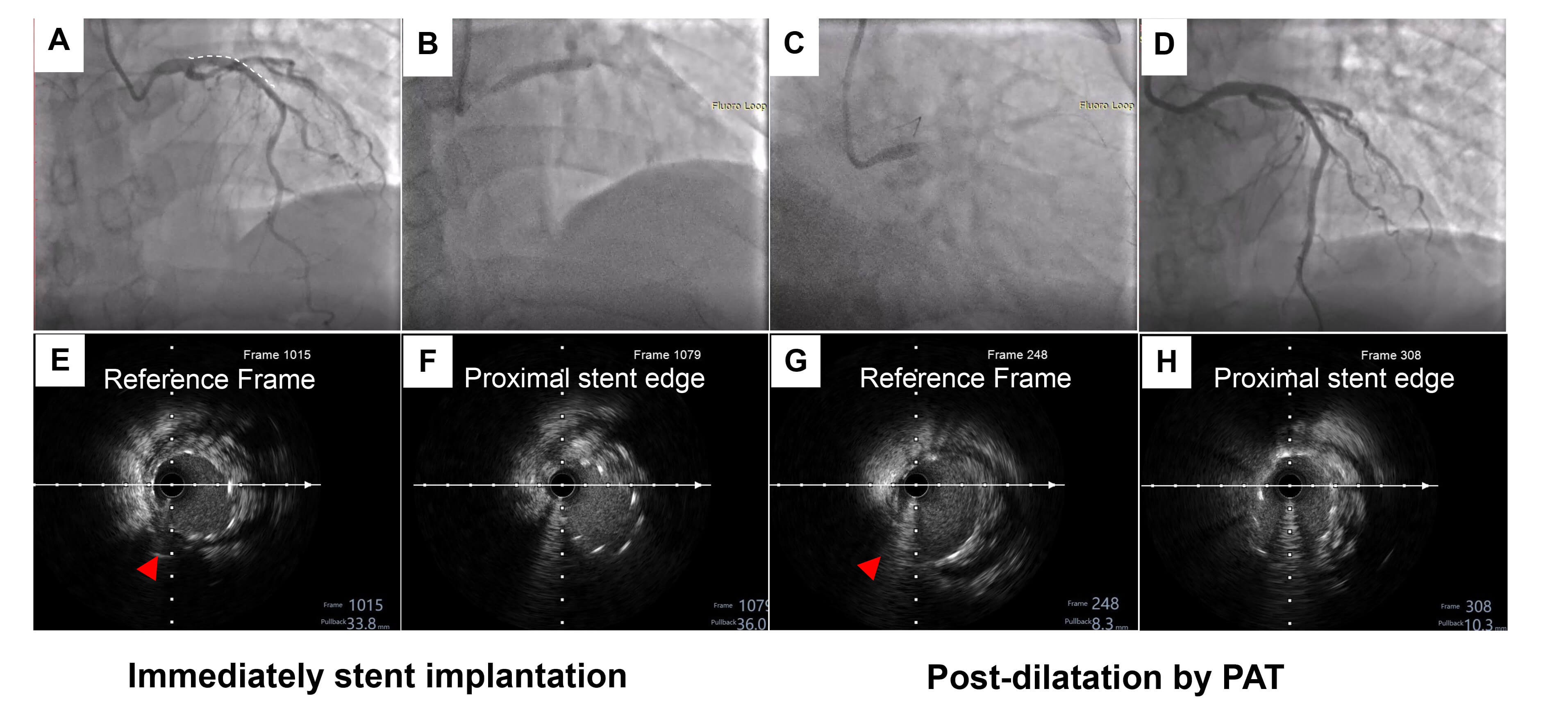 Fig. 4.
Fig. 4.
The first representative case of PAT. (A) Angiography showed a
moderate ostial LM stenotic lesion and diffuse moderate stenosis lesions of the
LAD. (B) Two drug eluting stents, a 2.75
The coronary angiography of another patient who was undergoing PAT showed an
isolated lesion at the ostium of the LAD, with plaques extending to the
mid-segment of the LAD (Fig. 5A). Since IVUS showed no significant stenosis at
the root of the LM or ostium of the LCX, precise stent positioning was required
(Medina 0,1,0). A 3.0
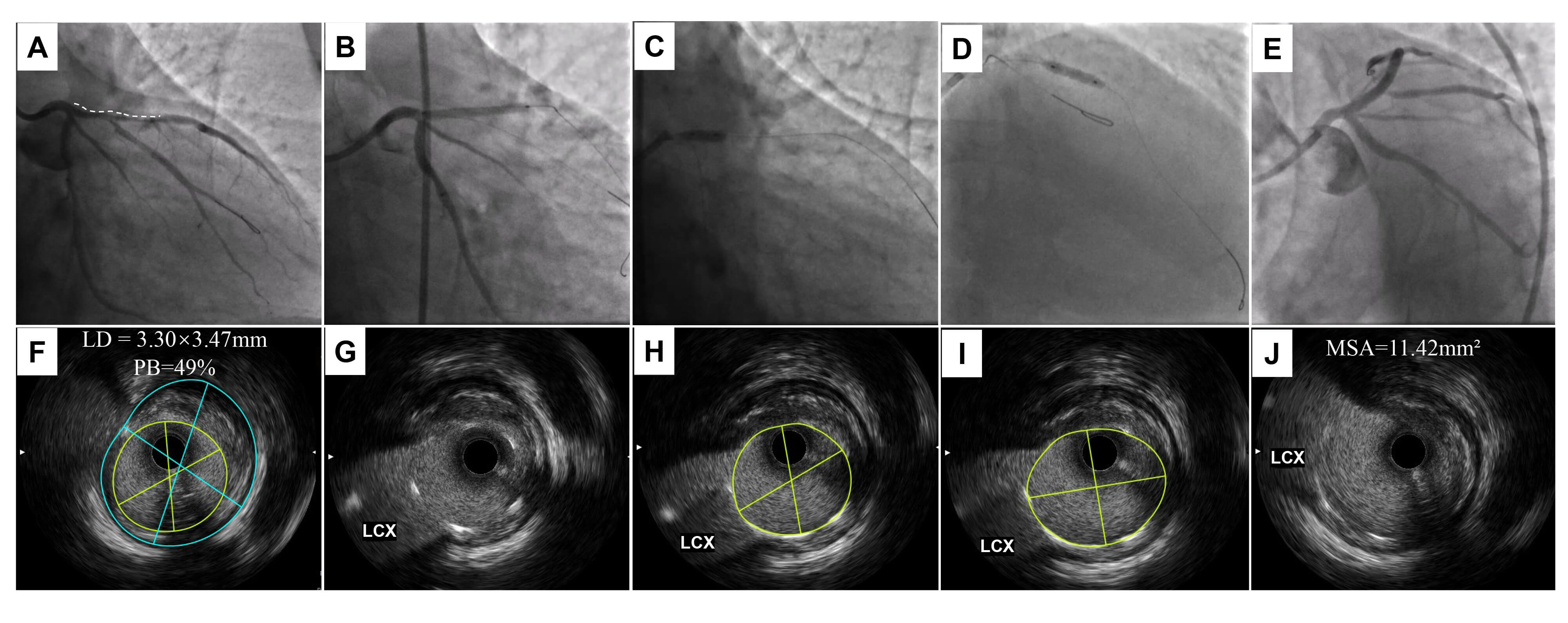 Fig. 5.
Fig. 5.
The second representative case of PAT. (A) Angiography showed a
severe stenotic lesion from the ostium to the middle of the LAD. (B) A 3.0
The third patient presented with diffuse severe stenosis from the proximal to mid LAD. The IVUS check confirmed plaque extension into the polygon of confluence (POC). In order to avoid missing the geography, we decided to crossover the stent from the LAD to LM. A pre-dilation balloon was used to treat the LAD lesions, which was followed by three DES implanted at the mid LAD to LM. Sequential post-dilation was then performed using conventional techniques from the distal to proximal direction (Fig. 6A–D). Longitudinal stent deformation during each step of the procedure was checked by IVUS. Compared with immediate stent implantation (Fig. 6H–J), IVUS showed that the length was longitudinally extended 2.3 mm to the proximal portion of the LAD after post-dilation (Fig. 6E–G).
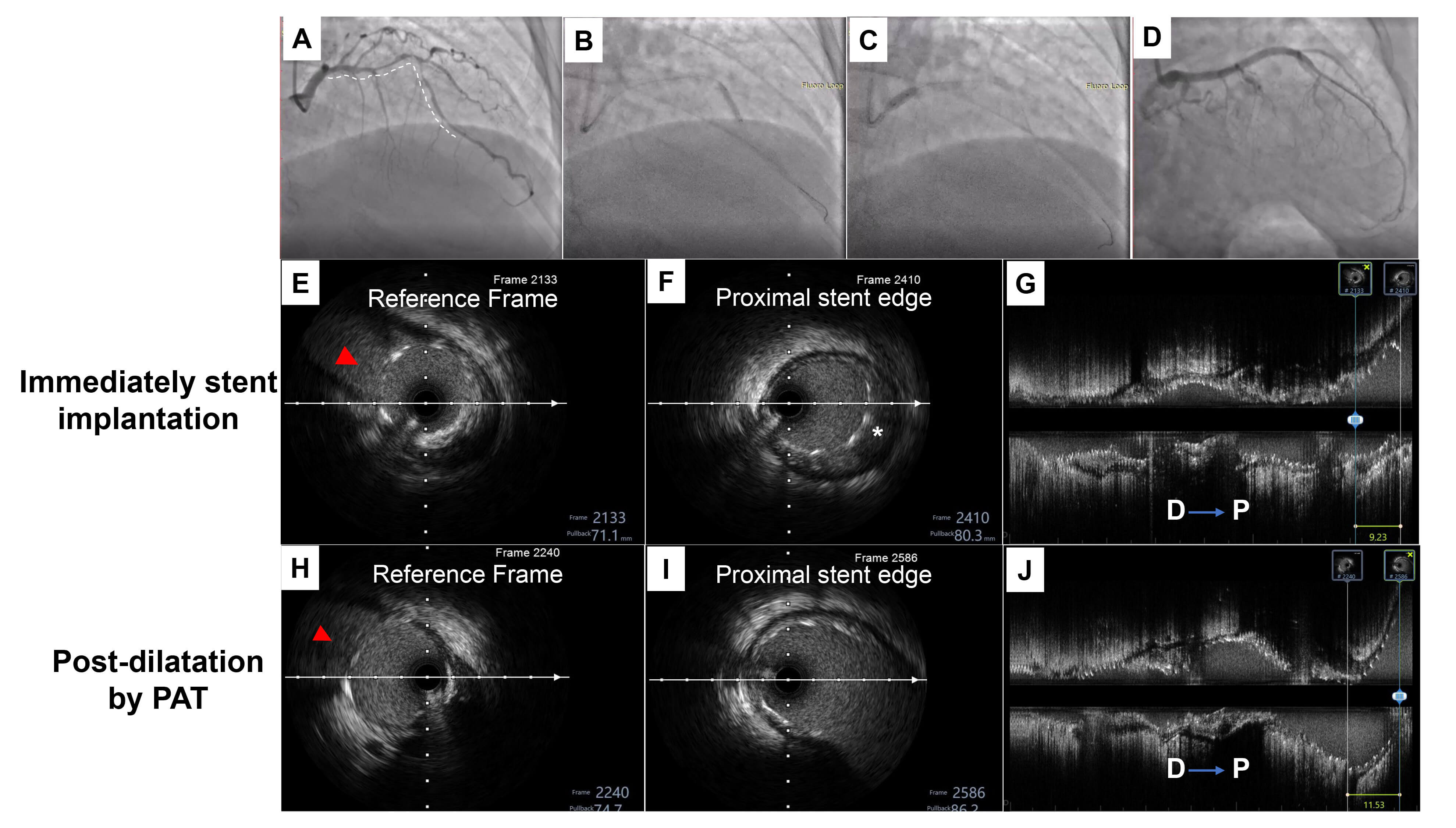 Fig. 6.
Fig. 6.
A representative case of conventional post-dilation distal to
proximal. (A) Angiography showed diffuse severe stenosis from the proximal to
the middle of left anterior descending (LAD). (B) Three drug eluting stents, a
2.25
In this study, we have described the PAT, a novel proximal post-dilation technique that aims at preventing the LSD. By utilizing bench modeling and the analysis of clinical cases, we provide novel insights into stent deformation related to post-dilation direction. We found that the D-P group showed a significant elongation in stent longitudinal length compared with the PAT group in the bench testing model. In addition, we found the PAT would help minimal proximal elongation and not affect the precise ostium stent implantation by analysis derived from clinical cases.
LSD has been described as longitudinal elongation or shortening of the stent in the longitudinal axis [7, 16]. Algowhary and Abdelmegid [11] analyzed 102 consecutively deployed stents by IVUS and found that 67.6% of implanted stents became elongated compared with the box-stated length. We know that even small changes in stent length can cause severe problems, especially in stents used for the treatment of aorta-ostial or some bifurcation lesions (Medina 0,1,0 and 0,1,1 and 0,0,1). Although there are several methods to help accurately locate the stent edge, such as multiple view angiography, the Szabo technique and the floating wire, the precise proximal location of the stent can be changed due to post-dilation ballooning [17].
Previous studies demonstrated that withdrawal of the device through deployed stents and extrinsic compression are involved in the longitudinal stent elongation [8, 18]. Matsuda et al. [19] retrospectively evaluated the effectiveness of post-dilation balloons on LSD in 103 stents using OCT, and found that stent elongation length was significantly longer in the mal-apposed group than in the well-apposed group. Most coronary arteries are anatomically shaped, however, the size of the stent often selected depends on the diameter of the distal reference vessel, which leads to mal-apposition of the proximal edge of the stent immediately upon placement. Stents performed with the proximal optimization technique (POT) increase the frictional force between the stent struts and the vessel wall to prevent the stent from elongating into the proximal direction. We hypothesize that PAT had a positive impact on preventing proximal stent elongation which may underlie the similar mechanisms with POT.
PAT has different indications than with POT. The latter is considered to be mandatory in true bifurcation lesions (Medina 1,1,0 and 1,1,1) which need to be performed with crossover or two-stent implantation techniques. However, the PAT is indicated for ostial or some bifurcation lesions (Medina 0,1,0 and 0,0,1) which always need precise stent placement. Second, the POT aims to complete circular correction of expected proximal strut mal-apposition [20, 21], to facilitate stent apposition in the proximal MB, to optimize strut clearance across the jailed side branch ostium, and to correct instrumentation-related stent deformation. The PAT is a novel post-dilation strategy with a different post-dilation direction using reference size non-compliant balloons according to the proximal lumen to avoid the LSD. Third, Toth et al. [6] recently found that POT with excessive overexpansion would cause significant proximal stent longitudinal elongation. They assumed that the overexpansion with tight ‘balloon-to-strut’ interaction results in longitudinal stretching of crowns and connectors, and that the POT balloon slides backwards during opening which pulls stent struts back from the distal portion of the ostium of the main branch. In consideration of these differences between POT and PAT, we advise that these two post-dilation methods should not be substituted for each other.
In addition, some studies showed that the post-dilation direction also impacts the stent longitudinal elongation, which is where the initial design of PAT originates. In a previous bench study, Sumi et al. [22] found that the distal to proximal post-balloon dilatation showed linear elongation during each step of the post-balloon dilatation. In contrast, during the proximal to distal post-balloon dilatation, the most significant change was observed in the first step of post-dilation and only slight changes were observed thereafter. Similar to these results, we found that the PAT group only had extended after the first post-dilation, but no further elongation thereafter, which is very crucial since these lesions need accurate location of the proximal stent edge.
There are some important details related to the use of PAT. First, the PAT balloon should be positioned with its proximal marker accurately located at the proximal end of the stent. Second, only non-compliant balloons (diameter of balloon was 1~1.2:1 ratio to the proximal reference vessel) are used for the PAT, to ensure accurate strut apposition and avoid excess overexpansion (always smaller than or equal to 16 atm). The balloons should always be completely deflated first and removed under visual control in order to avoid any stent entrapment when pulling back the deflated balloon catheter. Potential proximal elongation should be considered before stent implantation. Since PAT has minimal effect on stent elongation, the stent should be positioned slightly away from the ostium of the lesion.
Despite the promising findings from our bench testing and initial clinical experience, this study has several limitations that should be acknowledged. First, the bench test was conducted using a single stent platform. Different stent platforms vary in their cell design, connector type, and material composition, which may influence their susceptibility to longitudinal deformation. Therefore, the generalizability of our results to other contemporary stent platforms requires further validation. Second, the use of a static silicone phantom, while valuable for a controlled initial assessment, cannot fully replicate the complex biomechanical environment of a human coronary artery, including pulsatile flow, vascular tortuosity, and the dynamic interaction with atherosclerotic plaques. Future studies utilizing more sophisticated biomechanical models or animal studies could provide further insights. Third, the clinical evidence is based on a small number of illustrative cases from a single center without a control group for direct comparison. The limited number of patients precludes any definitive conclusions regarding the clinical efficacy and safety of PAT. Furthermore, we did not provide long-term follow-up data to assess the durability of the technique and its impact on clinical endpoints such as target lesion revascularization or stent thrombosis. Finally, the operators in both the bench and clinical studies were not blinded to the post-dilation strategy, which could introduce observation bias. A larger-scale, prospective, randomized controlled trial is warranted to confirm the benefits of PAT over conventional techniques and to establish its role in contemporary PCI practice.
We present a novel technique—PAT—to assist in preventing LSD. It has the potential to optimize current practices with stent implantation of ostial lesions and partial bifurcation lesions (Medina 0,1,0 and 0,1,1 and 0,0,1), which need massive over-dilation and accurate stent placement. In this study, only bench testing and clinical case series were reported. The long-term outcomes require further investigation in a prospectively designed study.
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
SZ and YTG and YQZ performed the statistical analyses. YL and YTG designed the research study and helped draft the manuscript. SZ and DHS interpreted the results and prepared the manuscript with inputs from all authors. All authors contributed to critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Analysis of the IVUS image recordings of clinical cases series was approved by the Ethics Committee of the First Affiliated Hospital of Harbin Medical University (ethics number: 2025505), and all procedures were performed in compliance with Helsinki declaration. Clinical case series were included after the written consent was signed by the patients.
We are grateful to the staff in the Department of Cardiology and Catheterization Laboratory at The First Affiliated Hospital of Harbin Medical University.
This research received no external funding.
Yiqun Zhang is an employee of Vivolight Medical Device & Technology Co., Ltd. The company had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. No financial or material support for the research was provided by Vivolight Medical Device & Technology Co., Ltd. All authors declare no other competing interests.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/RCM44250.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.