



 , Zhaofeng Zhang 2,*
, Zhaofeng Zhang 2,*
1 Department of Pharmacy, Ganzhou People’s Hospital, 341000 Ganzhou, Jiangxi, China
2 Department of Pharmacology, Ganzhou Dermatosis Hospital, 341000 Ganzhou, Jiangxi, China
Abstract
The C-reactive protein-to-albumin ratio (CAR), a marker of inflammation and nutritional status (calculated as C-reactive protein [CRP]/albumin [ALB]), is associated with increased mortality in congestive heart failure (CHF). However, whether vitamin D modulates the CAR-CHF relationship remains unclear. Using data from the National Health and Nutrition Examination Survey (NHANES), this study aimed to investigate the mediating role of vitamin D in the association between CAR and CHF among older adults, with implications for cardiovascular disease prevention.
Data from NHANES 2001–2010 were analyzed, including adults aged ≥65 years. Multivariate logistic regression was used to assess the independent association of CAR and 25-hydroxyvitamin D [25(OH)D] with CHF. Pearson correlation evaluated bivariate relationships between continuous variables (vitamin D, CAR), while Spearman correlation assessed associations between the dichotomous CHF status and continuous variables (vitamin D, CAR). Mediation analysis (Hayes’ PROCESS Model 4, 5000 bootstrap samples) tested whether 25(OH)D mediated the CAR-CHF link. Subgroup analyses explored effect modification by age, sex, and comorbidities.
A total of 4128 participants (mean age: 70.0 years; 55.81% male) were included, with 247 (5.98%) diagnosed with CHF. Vitamin D deficiency (25(OH)D <20 ng/mL) and insufficiency (20–30 ng/mL) were prevalent (71.2%). Key findings included: Bivariate associations: Lower 25(OH)D correlated with higher CAR (r = –0.12, p = 0.004) and increased CHF risk (Spearman ρ = –0.061, p < 0.01), while CAR was positively correlated with CHF (Spearman ρ = 0.080, p < 0.01). Multivariate analysis: CAR was an independent risk factor for CHF (adjusted OR for highest vs. lowest quartile: 1.96, 95% confidence interval (CI): 1.31–2.95, p < 0.001; p-trend < 0.001. Vitamin D sufficiency (25(OH)D ≥30 ng/mL) was associated with a lower CHF risk compared to deficiency (25(OH)D <20 ng/mL, OR: 0.56, 95% CI: 0.38–0.83, p = 0.003), indicating that deficiency was indirectly linked to higher risk. Mediation effect: 25(OH)D partially mediated the CAR-CHF association, explaining 3.00% of the total effect (indirect effect: 0.002, 95% CI: 0.001–0.005, p = 0.039). Predictive value: CAR had modest accuracy for CHF (area under the curve (AUC) = 0.597, 95% CI: 0.560–0.634), with an optimal cut-off of 0.149 (sensitivity: 59.1%, specificity: 56.4%).
Elevated CAR and vitamin D deficiency are independently associated with increased CHF risk in older adults. Vitamin D partially mediated the association between CAR and CHF, underscoring its role in linking inflammation/nutrition status to cardiovascular risk. Clinicians should monitor both biomarkers in CHF prevention, prioritizing inflammation control and vitamin D repletion in high-risk populations.
Keywords
- vitamin D
- C-reactive protein to albumin ratio (CAR)
- congestive heart failure (CHF)
- mediation effect analysis
- National Health and Nutrition Examination Survey (NHANES)
- cross-sectional study
Congestive heart failure (CHF) is a common cardiovascular disease characterized by symptoms such as dyspnea, malaise (usually manifesting as reduced exercise tolerance) and fluid retention (e.g., peripheral oedema), as well as elevated plasma natriuretic peptide levels [1]. With the rapid aging of the world’s population, CHF has become a growing public health concern, placing a significant burden on the health status and quality of life of the elderly [2]. This condition, characterized by progressive cardiac dysfunction and impaired hemodynamics, highlights the urgent need for improved diagnostic strategies and therapeutic interventions to mitigate its impact on vulnerable aging populations [3].
Traditional risk factors for CHF, including hypertension, smoking, diabetes mellitus, genetic predisposition and obesity, are well established [4, 5, 6]. However, in addition to these well-recognized traditional risk factors, emerging novel risk factors are being identified, which may hold significant prognostic and therapeutic implications. Despite substantial progress in the treatment of CHF, early diagnosis and the identification of factors capable of accurately predicting the risk of developing CHF remain critical for early disease prevention and necessitate further in-depth research.
Inflammatory processes are implicated in every stage of CHF onset, progression, and complication [7, 8]. C-reactive protein (CRP), a well-known archetypal marker of inflammation, has been positively correlated with the risk of CHF. Meanwhile, albumin levels are indicative of the body’s nutritional status, and a decrease in albumin is associated with a poor prognosis in CHF patients. In recent years, the CRP to albumin ratio (CAR), as a novel inflammatory indicator, has garnered significant attention. Studies have shown that elevated CAR levels are closely associated with the development of various chronic diseases [8, 9], particularly cardiovascular diseases [10]. CAR can comprehensively reflect the body’s inflammatory and nutritional status, and changes in its level may indicate the level of risk of cardiovascular diseases, especially CHF [11, 12, 13].
Beyond its established importance in calcium and phosphorus metabolism and bone health, researchers worldwide have conducted numerous investigations into the relationships among vitamin D, CAR, and cardiovascular diseases. An accumulating body of evidence suggests that vitamin D has an effect on the cardiovascular system [14, 15, 16, 17]. Similarly, elevated CAR levels have been recognized as an independent risk factor for cardiovascular diseases [18, 19]. Elevated CAR levels signify the body’s chronic inflammatory state, and inflammatory responses are known to play a pivotal role in the development of cardiovascular diseases. These responses can trigger pathological processes such as atherosclerosis and thrombosis, which are crucial in the progression of cardiovascular disorders. Conducting an in-depth exploration of the role of vitamin D in the relationship between CAR and CHF among the elderly population is highly promising. Such a study could simultaneously help elucidate the underlying pathogenesis of CHF and also provide a solid theoretical basis for formulating effective preventive and therapeutic strategies. This research direction may open up new avenues for understanding the complex mechanisms underlying CHF and contribute to the development of more targeted and efficient interventions for this prevalent disease among the elderly.
Notwithstanding the existing research, the mediating role of vitamin D in the association between CAR and CHF has received relatively scant attention, and the conclusions drawn from previous studies have been inconsistent. Therefore, the present study, which utilizes the nationally representative National Health and Nutrition Examination Survey (NHANES) database, is of great theoretical and practical significance. It aims to comprehensively explore the intricate relationships among vitamin D, CAR, and CHF, potentially shedding new light on the underlying pathological mechanisms of CHF, hopefully contributing to advancing methods of prevention and treatment for this prevalent condition among the elderly population.
The NHANES is a nationally representative continuous health survey project conducted by the National Center for Health Statistics (NCHS) under the Centers for Disease Control and Prevention (CDC). The database covers a wide range of information on demographics, physical measurements, laboratory tests, and health questionnaires, providing a rich data resource for medical research. No additional informed consent or ethical review was required as all study participants provided informed consent and the NCHS Institutional Review Board approved the study. All methods were performed in accordance with relevant guidelines and regulations.
In this study, data from the NHANES database spanning the years 2001–2010 were carefully screened to identify the elderly population aged 60 years or older. The inclusion criteria were designed to ensure the availability of complete data regarding vitamin D levels, the CAR, and disease-related markers of CHF. Conversely, individuals with severe hepatic and renal disorders, malignancies, autoimmune diseases (specifically rheumatoid arthritis), and other conditions that could potentially impact vitamin D metabolism and the inflammatory response were excluded. Following this rigorous screening procedure, a total of 4128 elderly individuals were selected for inclusion in the study. The sample selection process is presented in Fig. 1 through a detailed flowchart, which demonstrates the steps and criteria employed to determine the final study sample.
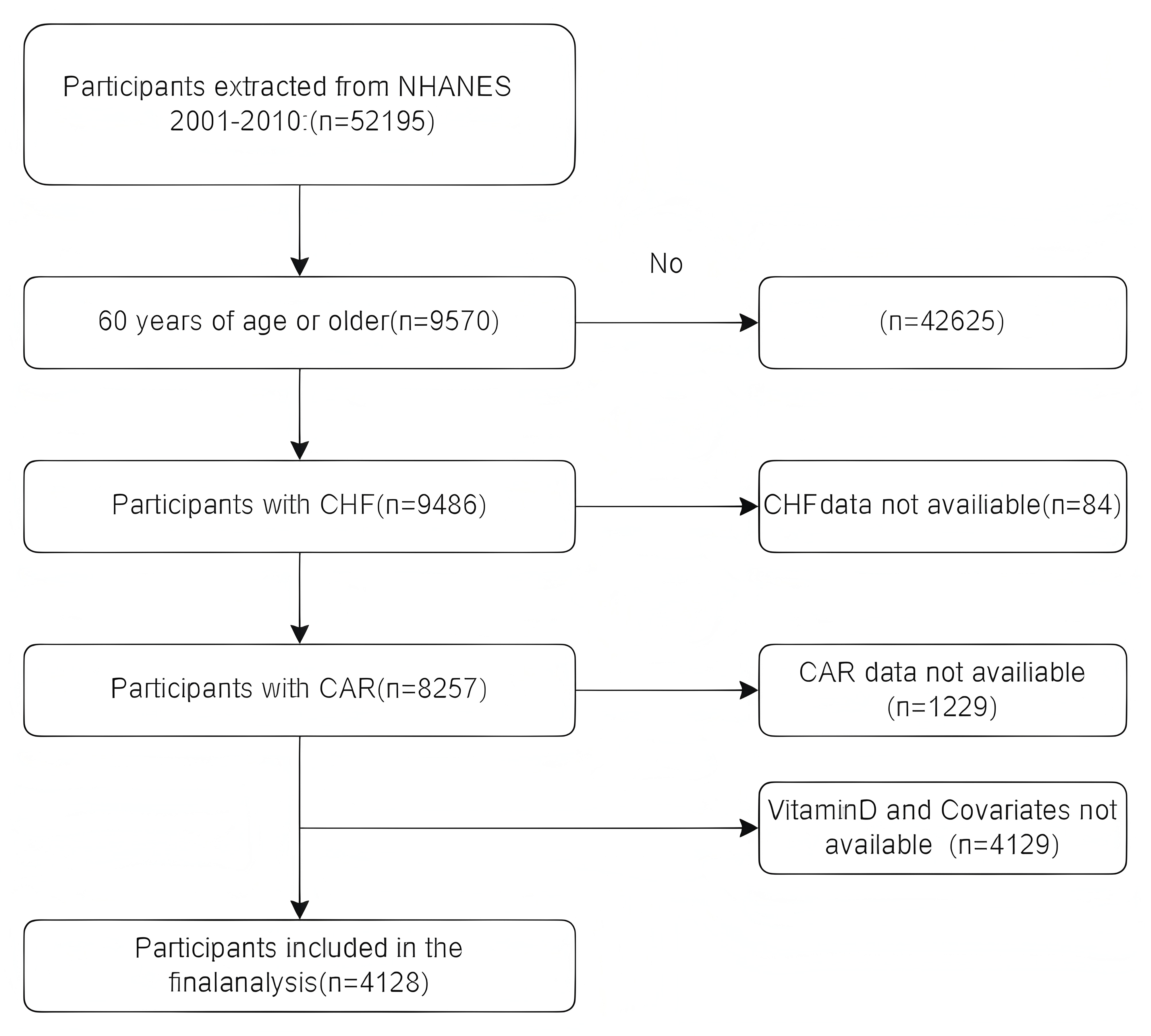 Fig. 1.
Fig. 1.
Flow diagram of selecting populations for analysis. CHF, congestive heart failure; CAR, C-reactive protein to albumin ratio; NHANES, National Health and Nutrition Examination Survey.
Flowchart illustrating the process of selecting study participants aged 60 years and above from the NHANES database between 2001 and 2010, including inclusion and exclusion criteria, and the final inclusion of 4128 individuals.
Serum samples from NHANES 2001–2010 were evaluated by liquid
chromatography-tandem mass spectrometry. Serum total vitamin D levels (nmol/L)
were calculated by totaling the levels of 25-hydroxyvitamin D2 and
25-hydroxyvitamin D3. Vitamin D deficiency was defined as 25(OH)D
CHF disease history was obtained through an interview. Participants were asked, ‘Has a doctor or other health professional ever told you that you have congestive heart failure?’ Patients were considered to have CHF if they answered ‘yes’ to the above question [21].
CAR was defined as serum CRP (mg/dL)/serum albumin (g/dL) and both CRP and albumin (ALB) were collected at a mobile screening center and sent to the laboratory for analysis. Prior to collection, blood samples were screened against specific exclusion criteria [9, 22].
In our study, several potential covariates were considered, including demographic factors, living status variables, disease status indicators, and biochemical indices. Demographic information encompassed sex, age, race, marital status, and educational attainment. Living status variables involved smoking habits, alcohol consumption patterns, and body mass index (BMI). Disease status included hypertension, diabetes mellitus, cancer, hepatic and renal diseases, and autoimmune diseases (specifically rheumatoid arthritis). The information regarding hypertension, diabetes mellitus, cancer, hepatic and renal diseases, and rheumatoid arthritis was obtained through questionnaires. In terms of biochemical indices, total cholesterol (TC) and aspartame nontransferable (AST) were utilized. All data collection and handling processes adhered to a standardized protocol to systematically investigate the potential impact of these covariates on the relationship between the CAR and CHF.
CAR was categorized into quartiles (Q1
Table 1 presents a summary of the baseline characteristics of the study
population, stratified by the presence or absence of CHF. Among the included
elderly adults, 28.78% had vitamin D deficiency, 42.44% had vitamin D
insufficiency, and 28.78% had sufficient vitamin D levels. Further analysis
indicated that the rates of vitamin D deficiency and insufficiency were higher in
men compared to women. Racial disparities were also observed, with non-Hispanic
whites having the highest prevalence of vitamin D deficiency. Out of the 4128
participants, 247 were diagnosed with CHF, resulting in an overall CHF prevalence
of 5.98% in the study population. The mean age of the participants was 70 years.
Regarding gender distribution, 55.81% of the participants were male, and 44.19%
were female. Statistical analyses revealed that men, individuals with higher
educational attainment, drinkers, smokers, those with hypertension, and patients
with vitamin D deficiency had a significantly higher risk of developing CHF
compared to their counterparts (all p
| Characteristics | No-CHF (n = 3881) | CHF (n = 247) | p | |
| Age (years) | 69.0 (63.0, 76.0) | 72.0 (66.0, 80.0) | ||
| BMI (kg/m2) | 28.0 (24.8, 31.5) | 29.5 (26.4, 35.4) | ||
| ALB (g/dL) | 4.2 (4.0, 4.4) | 4.1 (3.8, 4.2) | ||
| AST (U/L) | 24.0 (20.0, 28.0) | 23.0 (19.0, 27.0) | ||
| TC (mg/dL) | 201.0 (173.0, 230.0) | 180.0 (147.0, 215.0) | ||
| CRP (mg/dL) | 0.2 (0.1, 0.5) | 0.3 (0.1, 0.8) | 0.002 | |
| CAR (mg/g) | 0.054 (0.0, 0.1) | 0.077 (0.0, 0.2) | 0.002 | |
| Vitamin D (ng/mL) | 25.3 (19.5, 31.3) | 23.0 (16.0, 28.6) | ||
| Gender, n (%) | ||||
| Male | 2135 (55.01) | 169 (68.42) | ||
| Female | 1746 (44.99) | 78 (31.58) | ||
| Race, n (%) | 0.122 | |||
| Mexican American | 692 (17.83) | 30 (12.15) | ||
| Others | 296 (7.63) | 19 (7.69) | ||
| Non-Hispanic White | 2239 (57.69) | 149 (60.32) | ||
| Non-Hispanic Black | 654 (16.85) | 49 (19.84) | ||
| Education, n (%) | 0.002 | |||
| High school graduate | 1321 (34.04) | 108 (43.72) | ||
| Some college or above | 2560 (65.96) | 139 (56.28) | ||
| Marital status, n (%) | 0.043 | |||
| Have a partner | 2419 (62.33) | 138 (55.87) | ||
| No partner | 1462 (37.67) | 109 (44.13) | ||
| Drinker, n (%) | ||||
| Yes | 618 (15.92) | 67 (27.13) | ||
| No | 3263 (84.08) | 180 (72.87) | ||
| Smoker, n (%) | ||||
| Yes | 2303 (59.34) | 173 (70.04) | ||
| No | 1578 (40.66) | 74 (29.96) | ||
| Hypertension, n (%) | ||||
| Yes | 2100 (54.11) | 185 (74.90) | ||
| No | 1781 (45.89) | 62 (25.10) | ||
| Diabetes, n (%) | ||||
| Yes | 661 (17.03) | 103 (41.70) | ||
| No | 3220 (82.97) | 144 (58.30) | ||
| Vitamin D, n (%) | 0.003 | |||
| 25(OH)D |
1097 (28.30) | 91 (36.84) | ||
| 20 ng/mL |
1647 (42.40) | 105 (42.51) | ||
| 25(OH)D |
1137 (29.30) | 51 (20.65) | ||
Notes: Continuous and categorical variables were displayed individually as mean
Abbreviations: BMI, body mass index; ALB, albumin; AST, aspartate aminotransferase; TC, total cholesterol; CRP, C-reactive protein; CHF, congestive heart failure; CAR, C-reactive protein to albumin ratio.
Clinical baseline characteristics of the study population stratified by the presence or absence of CHF. This includes the distribution of vitamin D levels (deficiency, insufficiency, sufficiency), CHF prevalence, age, gender distribution, and the risk differences of CHF among various demographic and clinical characteristics (e.g., higher risk of CHF in males, higher education, drinkers, smokers, hypertensive patients, and vitamin D deficient individuals).
Table 2 displays the CAR values of the participants stratified into quartiles.
The median CAR value was 0.055. Q1 represents values below 0.0262, Q2 encompasses
values ranging from 0.0262 to 0.055, Q3 includes values from 0.055 to 0.1167, and
Q4 corresponds to values above 0.1167. The level of CAR was found to be
correlated with multiple factors, including age, gender, BMI, smoking status, and
alcohol consumption. Specifically, there was a statistically significant
association between CAR levels and age (p = 0.035), but the trend was
not a simple increase with age. Men exhibited higher CAR levels compared to
women. A positive correlation was detected between BMI and CAR levels, such that
the higher the BMI, the higher the CAR level. Smokers showed a progressive
increase in proportion across higher CAR quartiles (p
| Characteristics | Q1 (n = 1041) | Q2 (n = 1030) | Q3 (n = 1029) | Q4 (n = 1028) | p | |
| Age (years) | 70.0 (64.0, 76.0) | 69.0 (63.0, 76.0) | 70.0 (63.0, 76.0) | 68.0 (63.0, 75.0) | 0.035 | |
| BMI (kg/m2) | 26.3 (23.3, 29.1) | 27.7 (25.0, 31.0) | 28.8 (25.8, 32.2) | 30.1 (26.0, 34.5) | ||
| ALB (g/dL) | 4.3 (4.1, 4.5) | 4.2 (4.1, 4.4) | 4.2 (4.0, 4.4) | 4.0 (3.8, 4.2) | ||
| AST (U/L) | 24.0 (21.0, 28.0) | 24.0 (21.0, 28.0) | 23.0 (20.0, 28.0) | 22.0 (19.0, 26.0) | ||
| TC (mg/dL) | 196.0 (169.0, 224.0) | 200.0 (172.0, 232.0) | 202.0 (174.0, 232.5) | 201.0 (172.0, 230.8) | 0.005 | |
| Vitamin D (ng/mL) | 26.4 (20.7, 32.3) | 25.4 (20.0, 31.1) | 24.6 (18.6, 30.1) | 23.8 (16.8, 30.1) | ||
| Gender, n (%) | ||||||
| Male | 636 (61.10) | 594 (57.67) | 579 (56.27) | 495 (48.15) | ||
| Female | 405 (38.90) | 436 (42.33) | 450 (43.73) | 533 (51.85) | ||
| Race, n (%) | ||||||
| Mexican American | 167 (16.04) | 175 (16.99) | 204 (19.83) | 176 (17.12) | ||
| Others | 97 (9.32) | 75 (7.28) | 67 (6.51) | 76 (7.39) | ||
| Non-Hispanic White | 638 (61.29) | 618 (60.00) | 594 (57.73) | 538 (52.33) | ||
| Non-Hispanic Black | 139 (13.35) | 162 (15.73) | 164 (15.94) | 238 (23.15) | ||
| Education, n (%) | ||||||
| High school graduate | 302 (29.01) | 380 (36.89) | 347 (33.72) | 400 (38.91) | ||
| Some college or above | 739 (70.99) | 650 (63.11) | 682 (66.28) | 628 (61.09) | ||
| Marital status, n (%) | ||||||
| Have a partner | 699 (67.15) | 649 (63.01) | 644 (62.59) | 565 (54.96) | ||
| No partner | 342 (32.85) | 381 (36.99) | 385 (37.41) | 463 (45.04) | ||
| Drinker, n (%) | 0.008 | |||||
| Yes | 137 (13.16) | 182 (17.67) | 185 (17.98) | 181 (17.61) | ||
| No | 904 (86.84) | 848 (82.33) | 844 (82.02) | 847 (82.39) | ||
| Smoker, n (%) | ||||||
| Yes | 571 (54.85) | 606 (58.83) | 642 (62.39) | 657 (63.91) | ||
| No | 470 (45.15) | 424 (41.17) | 387 (37.61) | 371 (36.09) | ||
| Hypertension, n (%) | ||||||
| Yes | 532 (51.10) | 545 (52.91) | 580 (56.37) | 628 (61.09) | ||
| No | 509 (48.90) | 485 (47.09) | 449 (43.63) | 400 (38.91) | ||
| Diabetes, n (%) | 0.154 | |||||
| Yes | 184 (17.68) | 182 (17.67) | 183 (17.78) | 215 (20.91) | ||
| No | 857 (82.32) | 848 (82.33) | 846 (82.22) | 813 (79.09) | ||
| CHF, n (%) | ||||||
| No | 999 (95.97) | 980 (95.15) | 963 (93.59) | 939 (91.34) | ||
| Yes | 42 (4.03) | 50 (4.85) | 66 (6.41) | 89 (8.66) | ||
Notes: Continuous and categorical variables were displayed individually as mean
Pearson correlation analysis showed that vitamin D level was significantly
negatively correlated with CAR (r = –0.12, p = 0.004), i.e., the lower
the level of vitamin D, the higher the level of CAR; Given that CHF is a
dichotomous variable, a Spearman correlation analysis was performed. The results
showed a significant negative correlation between CHF and vitamin D (
The associations between CAR and CHF, as well as vitamin D and CHF, are
presented in Table 3, derived from multivariate logistic regression analyses. In
the unadjusted model, CAR was significantly and positively associated with CHF
(odds ratio (OR) = 2.09, 95% CI: 1.49–2.94, p
| Variables | Model 1 | Model 2 | Model 3 | Model 4 | |||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | ||
| CAR (continuous) | 2.09 (1.49~2.94) | 2.10 (1.49~2.96) | 2.05 (1.45~2.88) | 2.16 (1.51~3.09) | |||||
| CAR (quartile) | |||||||||
| Quartile 1 | Reference | Reference | Reference | Reference | |||||
| Quartile 2 | 1.21 (0.80~1.85) | 0.366 | 1.24 (0.81~1.89) | 0.315 | 1.01 (0.65~1.54) | 0.981 | 1.11 (0.72~1.71) | 0.644 | |
| Quartile 3 | 1.63 (1.10~2.42) | 0.016 | 1.69 (1.13~2.51) | 0.01 | 1.28 (0.85~1.93) | 0.235 | 1.50 (0.99~2.27) | 0.057 | |
| Quartile 4 | 2.25 (1.55~3.29) | 2.50 (1.71~3.67) | 1.72 (1.16~2.57) | 0.008 | 1.96 (1.31~2.95) | 0.001 | |||
| Vitamin D (continuous) | 0.97 (0.96~0.98) | 0.96 (0.95~0.98) | 0.97 (0.96~0.99) | 0.97 (0.95~0.99) | |||||
| Vitamin D (groups) | |||||||||
| 25(OH)D |
Reference | Reference | Reference | Reference | |||||
| 20 ng/mL |
0.77 (0.57~1.03) | 0.076 | 0.69 (0.51~0.94) | 0.018 | 0.76 (0.55~1.03) | 0.081 | 0.76 (0.55~1.05) | 0.095 | |
| 25(OH)D |
0.54 (0.38~0.77) | 0.48 (0.33~0.71) | 0.58 (0.39~0.85) | 0.005 | 0.56 (0.38~0.83) | 0.003 | |||
Notes: Model 1: No adjustment for covariates. Model 2: Adjust: Gender, Age, Race. Model 3: Adjust: Gender, Age, Race, Drinking, Smoking, BMI. Model 4: Adjust: Gender, Age, Race, Drinking, Smoking, BMI, Hypertension, Diabetes, TC.
Abbreviations: OR, odds ratio; 95% CI, 95% confidence interval.
After stratifying CAR into quartiles, the strong correlation between CAR and CHF
was still evident, and the trend test was statistically significant (p
These findings suggest that both vitamin D and CAR are independent risk factors for CHF. This further corroborates the crucial role of vitamin D and CAR in the pathogenesis of CHF, and demonstrates that their effects on CHF remain significant even after controlling for other common risk factors.
The results of the linear regression analyses exploring the relationship between
the CAR and vitamin D are presented in Table 4. In the unadjusted model, CAR was
negatively associated with vitamin D levels (
| Variables | Model 1 | Model 2 | Model 3 | Model 4 | |||||
| p | p | p | p | ||||||
| CAR (continuous) | –1.68 (–2.82~–0.54) | 0.004 | –1.13 (–2.19~–0.07) | 0.037 | –0.65 (–1.71~0.41) | 0.228 | –0.70 (–1.75~0.36) | 0.196 | |
| CAR (quartile) | |||||||||
| Quartile 1 | Reference | Reference | Reference | Reference | |||||
| Quartile 2 | –1.42 (–2.20~–0.63) | –1.25 (–1.98~–0.52) | –0.79 (–1.52~–0.06) | 0.035 | –0.80 (–1.53~–0.06) | 0.033 | |||
| Quartile 3 | –1.99 (–2.77~–1.20) | –1.68 (–2.41~–0.95) | –1.00 (–1.74~–0.25) | 0.008 | –1.03 (–1.77~–0.28) | 0.007 | |||
| Quartile 4 | –2.79 (–3.57~–2.00) | –2.01 (–2.75~–1.27) | –1.02 (–1.79~–0.26) | 0.008 | –1.06 (–1.82~–0.29) | 0.007 | |||
Notes: Model 1: No adjustment for covariates. Model 2: Adjust: Gender, Age, Race. Model 3: Adjust: Gender, Age, Race, Drinking, Smoking, BMI. Model 4: Adjust: Gender, Age, Race, Drinking, Smoking, BMI, Hypertension, Diabetes, TC.
To accurately evaluate the predictive power of the CAR level for CHF, we calculated the AUC of the ROC curve for the study subjects. The results are presented in Fig. 2. Our study findings revealed that the AUC value of the CAR level was 0.597. While this suggests CAR has a marginal predictive ability for CHF compared to random guessing (AUC = 0.5), the modest AUC indicates that CAR alone holds limited clinical predictive value for CHF. These results warrant cautious interpretation, and additional research is needed to explore biomarker combinations or refined models with enhanced predictive accuracy. Through further analysis, the optimal cut-off value of CAR was determined to be 0.149. At this cut-off value, the sensitivity for predicting CHF was 59.1% and the specificity was 56.4% (since specificity = 1 – 0.436), achieving an optimal balance between sensitivity and specificity for prediction.
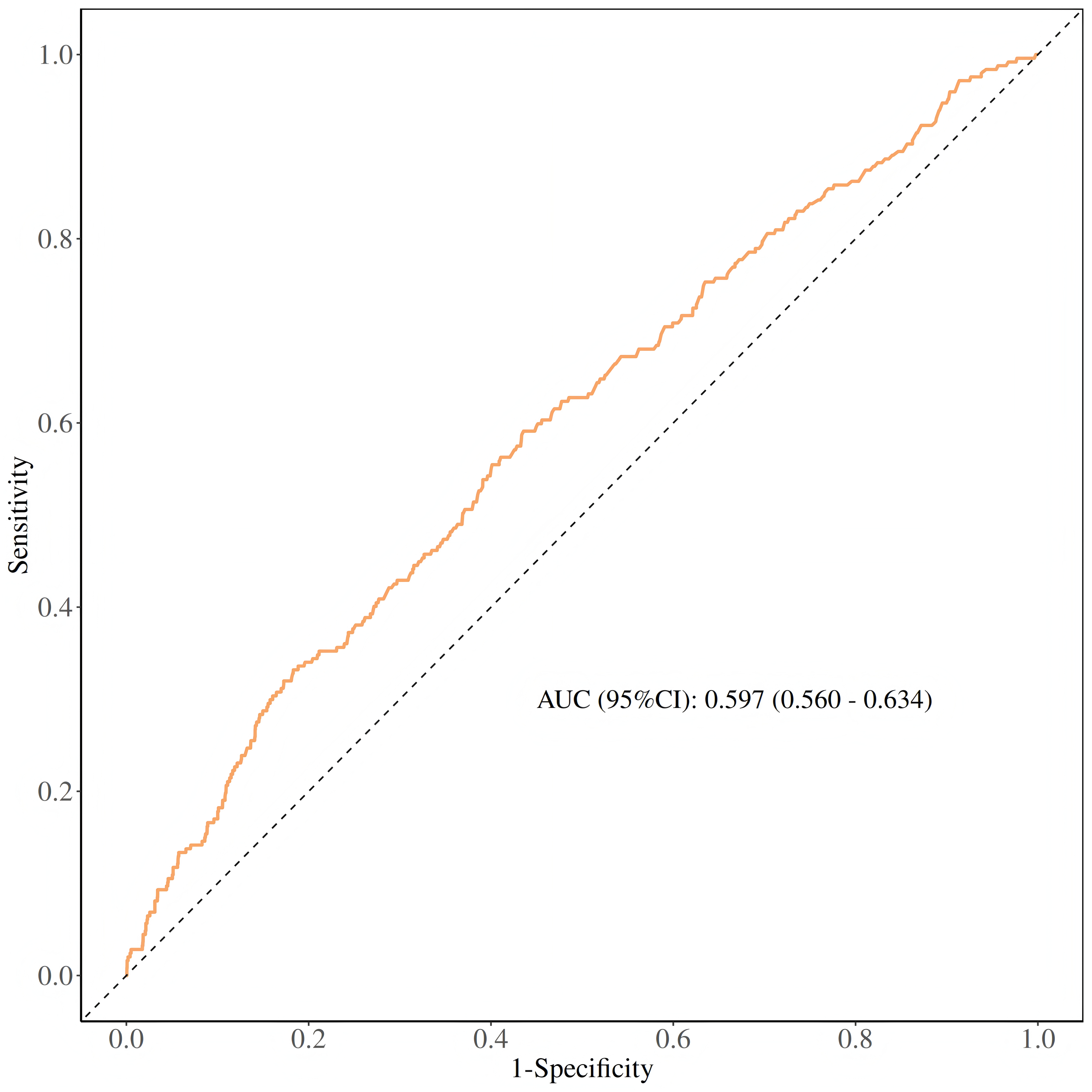 Fig. 2.
Fig. 2.
ROC curves and the AUC values of CAR in diagnosing CHF. AUC, area under the curve; ROC, receiver operating characteristic.
To evaluate the stability of the association between the CAR and CHF and to identify potential differences among different subgroups, we conducted subgroup analyses. The results of these analyses are presented in Table 5. In the sensitivity test, we observed that the ‘p-value for interaction’ was greater than 0.05. This finding indicated that the positive association between CAR and CHF was generally stable and consistent across the overall population.
| Variables | n (%) | OR (95% CI) | p | p for interaction | |
| All patients | 4128 (100.00) | 2.12 (1.50~3.00) | |||
| Gender | 0.082 | ||||
| Male | 2304 (55.81) | 2.71 (1.77~4.14) | |||
| Female | 1824 (44.19) | 1.53 (0.90~2.59) | 0.113 | ||
| Race | 0.313 | ||||
| Mexican American | 722 (17.49) | 3.37 (1.26~9.01) | 0.016 | ||
| Others | 315 (7.63) | 20.65 (1.40~304.80) | 0.027 | ||
| Non-Hispanic White | 2388 (57.85) | 2.13 (1.37~3.31) | |||
| Non-Hispanic Black | 703 (17.03) | 1.30 (0.37~4.53) | 0.680 | ||
| Education | 0.314 | ||||
| High school graduate | 1429 (34.62) | 2.75 (1.52~4.97) | |||
| Some college or above | 2699 (65.38) | 1.88 (1.25~2.81) | 0.002 | ||
| Drinker | 0.357 | ||||
| Yes | 685 (16.59) | 2.54 (1.44~4.49) | 0.001 | ||
| No | 3443 (83.41) | 1.91 (1.25~2.93) | 0.003 | ||
| Smoker | 0.187 | ||||
| Yes | 2476 (59.98) | 1.96 (1.38~2.80) | |||
| No | 1652 (40.02) | 4.98 (1.67~14.90) | 0.004 | ||
| Hypertension | 0.836 | ||||
| Yes | 2285 (55.35) | 2.03 (1.34~3.07) | |||
| No | 1843 (44.65) | 2.18 (1.14~4.17) | 0.019 | ||
| Diabetes | 0.108 | ||||
| Yes | 764 (18.51) | 5.61 (1.50~21.00) | 0.010 | ||
| No | 3364 (81.49) | 1.91 (1.35~2.70) | |||
| Age | 0.422 | ||||
| 60–70 | 2330 (56.44) | 1.76 (0.89~3.47) | 0.106 | ||
| 1798 (43.56) | 2.31 (1.47~3.64) | ||||
Mediation analyses were performed to assess whether vitamin D mediates the
association between CAR and CHF disease occurrence. Mediation analyses were
performed by establishing three pathways. For this purpose, we set up three
pathways: (1) exposure to mediator; (2) mediator to outcome (direct effect); and
(3) exposure to outcome (total effect). The total effect reflects the sum of the
direct and mediated (indirect) effects. The percentage of mediated effects was
calculated using the following formula: (mediated effect/total effect)
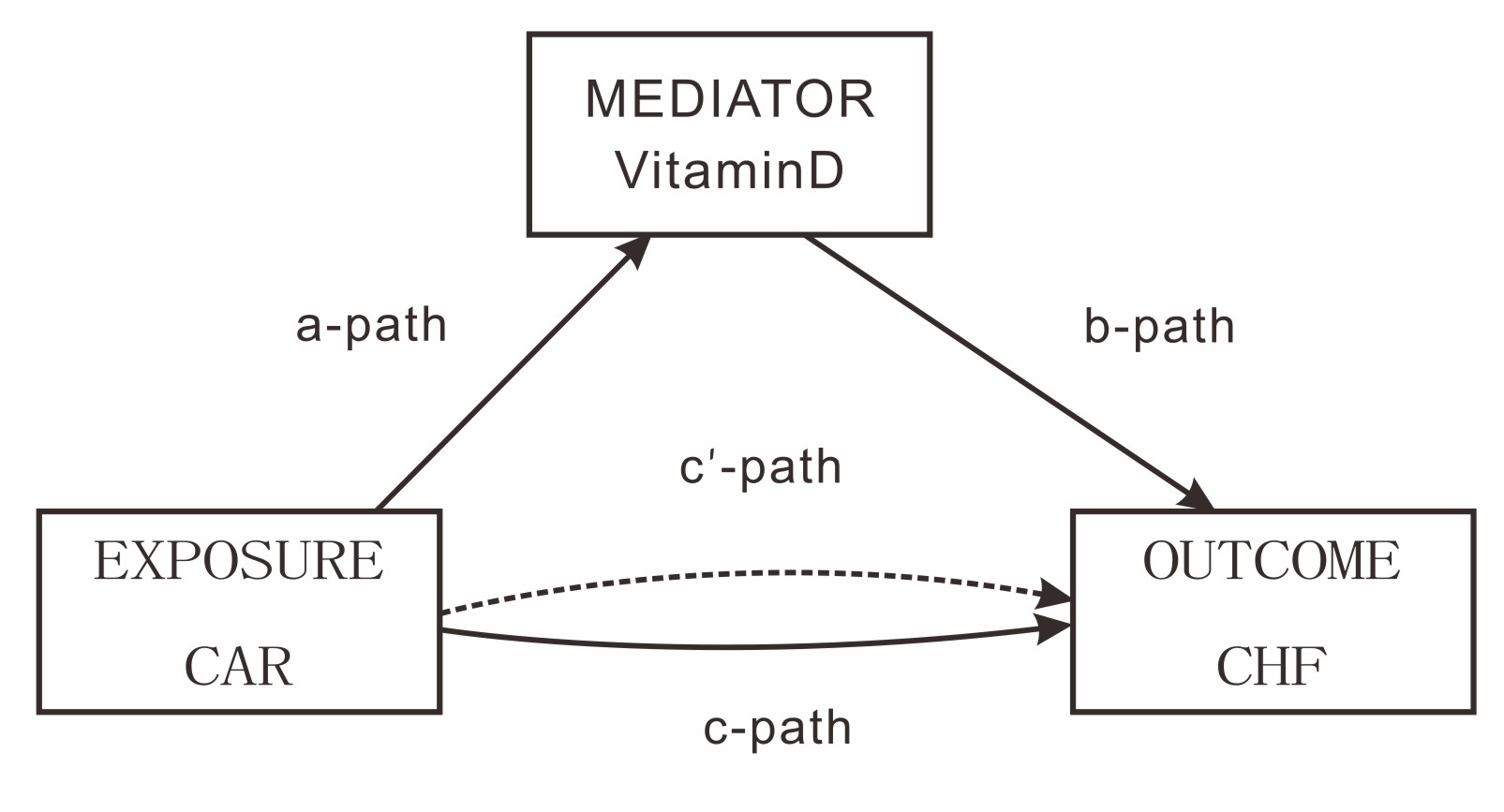 Fig. 3.
Fig. 3.
Path diagram of the mediation analysis models. In the mediation analysis framework, the “c - path” represents the total effect of EXPOSURE (CAR) on OUTCOME (CHF), while the “c’ - path” denotes the direct effect, excluding the influence mediated by vitamin D.
| Independent variable mediator | Mediator | Total effect | Indirect effect | Direct effect | Proportion mediated |
| Coefficient (95% CI) | Coefficient (95% CI) | Coefficient (95% CI) | |||
| CAR | vitamin D | 0.081 (0.052~0.111) | 0.002 (0.001~0.005) | 0.079 (0.05~0.108) | 3.00% |
Note: In mediation analyses, adjustments were made for Gender, Age, Race, Drinking, Smoking, AST, TC.
Mediation effect analysis models and results for the role of vitamin D in the association between CAR and CHF. This includes the total effect of CAR on CHF, the direct effect, the mediating effect of vitamin D, and the proportion of the total effect mediated by vitamin D (3.00%), indicating that vitamin D plays a partial mediating role in the relationship between CAR and CHF.
The results of the mediation effect analysis indicated that the total effect of
the CAR on CHF was significant (
This finding holds significant importance for clinical practice. Physicians can utilize this cut-off value to assess the risk of patients, enabling them to promptly identify individuals at potential risk of CHF and take appropriate preventive and therapeutic measures. For instance, if a patient’s CAR level exceeds this cut-off value, it indicates that the patient is at a high risk of developing CHF, and further in-depth examination and close monitoring of the patient are necessary.
Vitamin D partially mediated the association between CAR and CHF, but its percentage contribution was low (3.00%), but the indirect effect was statistically significant (p = 0.039). Analyzing a sample of 4128 individuals aged 60 years and above, we identified a significant association between CAR and CHF. This finding implies that individuals with elevated CAR levels are more likely to develop CHF. Remarkably, this correlation remained strong even after adjusting for a comprehensive set of covariates in the fully adjusted model (Model 4). Subgroup analyses and sensitivity tests further indicated that the associations were relatively stable across different subgroups, with no significant differences observed. Overall, there was a positive association between CAR and the development of CHF. Simultaneously, vitamin D was found to partially mediate the relationship between CAR and CHF, emphasizing the importance of closely monitoring both the inflammatory levels (represented by CAR) and vitamin D levels. This also highlights the significance of improving the management of patients with low vitamin D levels for the prevention of cardiovascular diseases.
An in-depth exploration of the NHANES database has unveiled the critical role of vitamin D in mediating the relationship between CAR and CHF. CAR, as a novel biomarker, integrates information on inflammation and nutritional status of the organism, providing valuable insights into the mechanistic study of the disease and prognostic assessment of patients. This finding is consistent with previous findings by other scholars and further validates the potential of CAR in clinical applications [24, 25, 26]. Elevated CRP levels signify an augmented inflammatory response [27]. CRP concentration is a strong predictor of the occurrence or exacerbation of heart failure events in patients with heart failure and those at risk [11, 28]. While decreased ALB levels suggest poor nutritional status. Both serum CRP and ALB are important prognostic indicators of the risk of death in patients with CHF.
Our findings are consistent with numerous prior studies [15, 29, 30, 31], indicating that vitamin D deficiency is significantly associated with an increased risk of CHF. As a steroid hormone with a wide range of biological functions, vitamin D exerts complex and diverse effects within the cardiovascular system. On one hand, vitamin D can regulate the renin-angiotensin system (RAS) [32, 33]. By inhibiting the expression of the renin gene, it reduces the production of angiotensin Ⅱ, which ultimately leads to a decrease in blood pressure and a reduction in the pressure load on the vascular wall, thus protecting the cardiovascular system. On the other hand, vitamin D has anti-inflammatory and antioxidant properties [34, 35, 36]. It can suppress the activation of inflammatory cells and the release of inflammatory factors, alleviate oxidative stress damage, and preserve the integrity and function of vascular endothelial cells. These actions collectively contribute to reducing the risk of cardiovascular diseases. In conclusion, both vitamin D deficiency and elevated CAR levels are associated with an increased risk of CHF.
The results of the mediation effect analysis strongly confirm that vitamin D plays a significant mediating role in the relationship between CAR and CHF. This reveals that CAR not only has a direct impact on the occurrence of CHF but also indirectly influences it by modulating vitamin D levels. Specifically, elevated CAR levels may trigger an inflammatory response and disrupt vitamin D metabolism, resulting in decreased vitamin D levels. Vitamin D deficiency, in turn, further diminishes its protective effects on the cardiovascular system, thereby increasing the risk of CHF.
This finding underscores that, in the prevention and treatment of cardiovascular diseases, apart from focusing on the inflammatory and nutritional status reflected by CAR, it is essential to pay close attention to maintaining and regulating vitamin D levels. By doing so, healthcare providers can more effectively control the risk of CHF and potentially improve patient outcomes.
In comparison to previous research, the present study, leveraging a large sample from the NHANES database and applying more rigorous research methodologies and statistical analyses, has further affirmed the associations among vitamin D, CAR, and CHF. Notably, it has, for the first time, clarified the mediating role of vitamin D in the relationship between CAR and CHF. While several prior studies have recognized the association between vitamin D deficiency and CHF, they have not explored its mediating role in the connection between inflammatory markers and CHF. Therefore, this study fills this research gap and provides a novel perspective for a more in-depth understanding of the relationships among vitamin D, CAR, and CHF.
However, this study is not without limitations. First, the NHANES database adopts a cross-sectional study design, inherently restricting the establishment of causal relationships among vitamin D, CAR, and cardiovascular disease. Prospective studies are vital to confirm such causal links. Second, although certain potential confounders were accounted for, unmeasured confounders might still affect the findings. Third, supplementary analyses on the correlation between cardiovascular disease and medications/specific treatments in cardiovascular patients were lacking, which could impact the interpretation of investigated relationships and require further exploration. More importantly, the CHF disease history relied on interviews, potentially introducing recall bias. Additionally, the absence of objective verification via tests (e.g., echocardiography) poses a risk of misdiagnosis. These limitations in CHF diagnosis data collection should be acknowledged.
The present study demonstrated for the first time that vitamin D plays a key
mediating role in the association between CAR and CHF by analyzing data from an
elderly population (mediating effect share 3.00%, p = 0.039).
Cross-sectional analyses showed that vitamin D deficiency (25(OH)D
In clinical practice, combined monitoring of CAR and vitamin D levels may help to identify people at risk for CHF. Prompt supplementation of vitamin D-deficient patients, especially those with elevated CAR, may slow the progression of CHF by reducing the inflammatory load. However, this study was limited by a cross-sectional design, and causality needs to be further validated in a prospective cohort study. Future randomized controlled trials are needed to assess the synergistic effect of vitamin D supplementation combined with anti-inflammatory interventions in the prevention of CHF in order to improve the theoretical basis and guide clinical translation.
Detailed descriptions of NHANES, all data, and guidance on analytical approaches can be found at https://www.cdc.gov/nchs/nhanes/index.htm.
YFW and ZFZ critically revised the manuscript for important intellectual content, were jointly responsible for the conception and design of the research methodology, as well as for the collection, analysis, and interpretation of the data, and wrote the first draft of the manuscript, both making substantial contributions to the manuscript and approving the version submitted for publication. Both authors read and approved the final manuscript. Both authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Not applicable. This study utilized publicly available data from the National Health and Nutrition Examination Survey (NHANES), which was approved by the National Center for Health Statistics Ethics Review Board. All participants provided informed consent at the time of data collection by NHANES.
We would like to thank the National Center for Health Statistics and each of the survey teams and study participants who made this analysis possible.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.