



 , Mingjian Lang 1,†, Benjamin Samraj Prakash Earnest 2, Ihab Elsayed Mohamed Ali Abdou 2,*
, Mingjian Lang 1,†, Benjamin Samraj Prakash Earnest 2, Ihab Elsayed Mohamed Ali Abdou 2,*
1 Department of Cardiovascular Medicine (Chengdu Institute of Geriatric Diseases), The Fifth People's Hospital Affiliated to Chengdu University of Traditional Chinese Medicine, 611137 Chengdu, Sichuan, China
2 School of Medicine, Faculty of Health and Medical Sciences, Taylor’s University Lakeside Campus, 47500 Subang Jaya, Selangor Darul Ehsan, Malaysia
†These authors contributed equally.
Abstract
This study aimed to evaluate the effectiveness of left bundle branch-optimized cardiac resynchronization therapy (LOT-CRT) in patients diagnosed with heart failure and reduced ejection fraction due to ischemic cardiomyopathy.
A total of 78 patients with ischemic cardiomyopathy who underwent pacemaker implantation at a single center between March 2020 and March 2022 were randomly assigned to two groups based on different pacing methods: LOT-CRT group (n = 39) and biventricular pacing (BVP) group (n = 35). Pacing threshold, impedance, electrocardiogram QRS wave duration during pacing, ventricular pacing ratio during follow-up, and cardiac ultrasound-related indicators were compared immediately after surgery and at the six-month follow-up.
The two groups were similar regarding baseline characteristics, cardiac ultrasound and magnetic resonance imaging (MRI) parameters, and overall cardiac function. However, the BVP group demonstrated higher pacing thresholds and impedance levels immediately after surgery and at the six-month follow-up (p < 0.001). Moreover, the X-ray exposure time was significantly longer in the BVP group compared to the LOT-CRT group. While no significant differences in QRS duration were observed between the groups preoperatively, the QRS duration in the LOT-CRT group was significantly shorter both immediately after surgery and during follow-up (p < 0.001). No significant differences were found between the groups in terms of the New York Heart Association (NYHA) functional class, left ventricular ejection fraction (LVEF), or left ventricular end-diastolic diameter (LVEDD). Six months post-surgery, both groups showed modest improvements in NYHA class, LVEF, and LVEDD, with the LOT-CRT group demonstrating significant improvements (p < 0.001).
LOT-CRT may be an alternative treatment for patients with heart failure complicated by left bundle branch block due to ischemic cardiomyopathy in whom BVP is ineffective.
Keywords
- ischemic cardiomyopathy
- heart failure
- cardiac resynchronization therapy
- left bundle branch-optimized cardiac resynchronization therapy
Cardiac resynchronization therapy (CRT), which typically involves biventricular pacing (BVP), is a crucial treatment for patients with cardiomyopathy, left bundle branch block (LBBB), and advanced heart failure (HF). However, up to 30% of patients do not respond to BVP, particularly those with ischemic cardiomyopathy (ICM). Consequently, exploring alternative treatments for these patients is essential to improve clinical outcomes. Recent studies indicate that physiological left bundle branch pacing (LBBP) can significantly reduce or even normalize the width of QRS waves and improve clinical outcomes [1, 2, 3, 4, 5]. Furthermore, other studies have shown that left bundle branch-optimized cardiac resynchronization therapy (LOT-CRT) can improve the prognosis for patients with non-ischemic cardiomyopathy (NICM) [6, 7, 8]. However, more comprehensive research is needed to examine the efficacy of LOT-CRT in patients with ICM. Therefore, this study aimed to investigate the therapeutic effect of LOT-CRT and provide a theoretical foundation and valuable insights for applying LOT-CRT in these patients.
This prospective, randomized study was conducted at the People’s Hospital
affiliated with Chengdu University of Traditional Chinese Medicine from March
2020 to March 2022. Patients with ICM who met the following criteria were
eligible for inclusion: age range of 18 to 65 years; conformity with CRT
criteria: New York Heart Association (NYHA) functional classes III–IV,
electrocardiogram showing complete LBBB, QRS interval
During the study period, 78 patients who met the inclusion criteria were randomly assigned to the LOT-CRT (n = 39) and BVP (n = 39) groups using a random number table. Overall, from the originally assigned 39 patients in the BVP group, two patients were reassigned to the LOT-CRT group; one abandoned surgery, and another experienced a surgical failure; thus, 35 patients were included in the BVP group. Comparatively, for the LOT-CRT group, two patients experienced surgical failure and were excluded; however, since two patients were reassigned from the BVP group, the number of patients in the LOT-CRT group remained at 39. This study was approved by the Medical Ethics Committee of the Fifth People’s Hospital, Affiliated with the Chengdu University of Traditional Chinese Medicine (Ethics Number: Ethical review 2022-009 (Section) -01). Written informed consent was obtained from all patients before their enrolment. This study was conducted in accordance with the guidelines of the Declaration of Helsinki. Data were anonymized during analysis and reporting to protect the privacy of participants.
Patients were randomly assigned to either the LOT-CRT or BVP groups using a computer-generated random number table. The allocation was performed in a 1:1 ratio. To ensure anonymity, the randomization process was managed by an independent coordinator not involved in patient care or the follow-up assessment. The assignment was sealed in opaque envelopes and opened after the patient met the inclusion criteria and provided informed consent. This randomization method was implemented to minimize selection bias and ensure comparable baseline characteristics between the two groups.
All patients were treated for chronic HF using angiotensin-converting enzyme
inhibitors (ACEIs)/angiotensin receptor antagonists (angiotensin receptor
blocker, ARB) and
The 3830 pacing lead was positioned in the right anterior oblique 30°
fluoroscopic view via the C315 His sheath. Unipolar pacing was conducted at 2.0
V/0.4 ms to identify the optimal pacing site based on the following criteria: (1)
The pacing QRS duration in lead V1 with the 3830 lead tip should exceed 120 ms
and display a “W” morphology, with a notch observed at either the nadir or
upstroke; (2) The R-wave amplitude at the tip electrode should be at least 5.0
mV. The 3830 lead was then rotated clockwise, approximately five to six turns,
with unipolar pacing applied at each rotation to dynamically assess QRS
morphology, QRS duration (QRSd), pacing impedance, and R-wave amplitude. As the
lead approached the left bundle branch (LBB) region, a marked reduction in QRSd
was observed. The left ventricular peak time was assessed in leads V5 to V6.
Rotation was stopped once the left ventricular peak time significantly shortened
and stabilized across different pacing outputs (
Traditional CRT was performed via the
axillary vein approach. A balloon catheter was inserted, and after retrograde
venography delineated the course of the coronary vein, the left ventricular lead
was advanced through the coronary sinus sheath to the distal lateral or
posterolateral branch of the coronary sinus. After obtaining a satisfactory
threshold and sensing parameters, the pacing was performed at 10 V, with a pulse
width of 1.0 ms to prevent diaphragmatic stimulation. The right ventricular
apical and right atrial leads were then implanted sequentially using conventional
methods. Finally, the pacemaker generator was connected to the leads and placed
into a preformed subcutaneous pocket. The incision was then sutured in layers.
The pocket was closed and covered with a sterile dressing, and local pressure was
applied for six to eight hours using a sandbag (Fig. 1). All patients underwent
transvenous implantation of a biventricular pacemaker, with no cases requiring
open-chest implantation for the left ventricular lead. Postoperative CRT
programming was optimized to the dual-chamber demand (DDD) pacing or dual-chamber
demand rate-adaptive (DDDR) pacing mode, with an atrioventricular (AV) sensing
interval of 100 ms and an AV pacing interval of 130 ms. The lower pacing rate was
adjusted to achieve a BVP ratio of
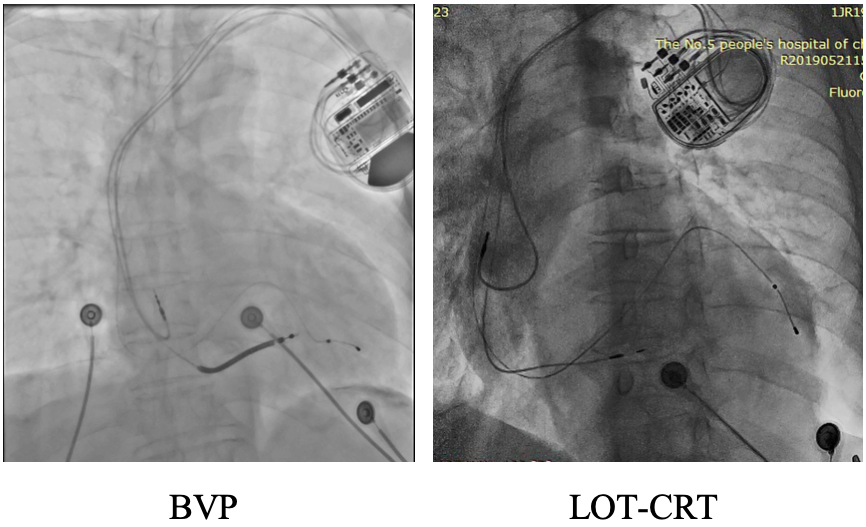 Fig. 1.
Fig. 1.
Representative chest X-rays from the first postoperative day are shown for both groups.
To ensure consistency in surgical techniques across patients, we implemented a comprehensive CRT implantation protocol in this study. All procedures were performed by experienced surgeons who had completed at least 50 LOT-CRT implantations. The surgical team held regular meetings to ensure strict adherence to the established protocol by all participating surgeons. Key steps in the procedure, including accurate positioning of the left bundle branch, control of implantation depth, and intraoperative monitoring and adjustment of QRS duration, were standardized using real-time imaging and electrophysiological evaluation during surgery. Additionally, pacing parameters during follow-up, including pacing threshold, impedance, and QRS duration, were uniformly recorded and analyzed to maintain consistency in postoperative outcomes.
All patients were monitored through follow-up visits at the arrhythmia
outpatient clinic every three months. Diuretics and digitalis were gradually
reduced during these visits if the patient’s HF symptoms
significantly improved. The dosages of
The primary outcome of this study was to analyze the improvement in LVEF at six months post-procedure, chosen due to its strong association with long-term prognosis in heart failure patients.
The secondary outcomes included the following: QRS duration was measured at baseline, immediately after the procedure, and six months post-procedure. NYHA functional class: assessed at baseline and six months post-procedure. The left ventricular end-diastolic diameter (LVEDD) was measured by echocardiography at baseline and six months after the procedure. Plasma NT-proBNP levels were measured at baseline and six months as a marker of the severity of heart failure. The incidence of arrhythmic episodes was monitored throughout the follow-up period. Rehospitalization for heart failure and all-cause mortality were recorded as clinical outcomes at the follow-up.
Statistical analysis was performed using SPSS 19.0 software (IBM Corp., Armonk,
NY, USA). Continuous variables with normal distribution are presented as the mean
The mean age in the LOT-CRT group was 55.8
| BVP (N = 35) | LOT-CRT (N = 39) | p-value | ||
| Age, years | 56.5 |
55.8 |
0.801 | |
| Male, n (%) | 21 (60.0) | 24 (62.0) | 0.703 | |
| NYHA | 2.9 |
2.8 |
0.955 | |
| NYHA II, n (%) | 9 (26.7) | 8 (20.5) | ||
| NYHA III, n (%) | 20 (57.1) | 19 (48.7) | ||
| NYHA IV, n (%) | 6 (17.1) | 12 (30.7) | ||
| Hypertension, n (%) | 12 (34.3) | 11 (28.2) | 0.654 | |
| Diabetes mellitus, n (%) | 6 (17.1) | 8 (20.5) | 0.923 | |
| Atrial fibrillation, n (%) | 9 (25.7) | 8 (20.5) | 0.557 | |
| Baseline QRSd, ms | 173.2 |
175.5 |
0.277 | |
| Left atrium, mm | 43.3 |
42.2 |
0.822 | |
| LVEDD, mm | 70.6 |
71.2 |
0.835 | |
| LVDS, mm | 63.3 |
63.7 |
0.901 | |
| MRA, cm2 | 5.2 |
5.2 |
0.224 | |
| LVESV, mL | 222.3 |
222.5 |
0.463 | |
| LVEDV, mL | 300.6 |
301.8 |
0.367 | |
| LVEF, % | 26.83 |
26.00 |
0.439 | |
| RV, mm | 23.9 |
24.0 |
0.117 | |
| NT-proBNP, pg/mL | 1714.5 (914.7, 2514.3) | 1757.1 (997.2, 2517.0) | 0.532 | |
| Drug therapy | ||||
| Digitalis, n (%) | 23 (66.7) | 27 (69.0) | 0.570 | |
| Diuretics, n (%) | 35 (100.0) | 10 (100.0) | 1.000 | |
| ACEI/ARB, n (%) | 35 (100.0) | 10 (100.0) | 1.000 | |
| Mineralocorticoid receptor antagonist, n (%) | 35 (100.0) | 10 (100.0) | 1.000 | |
| Beta-blocker, n (%) | 32 (91.4) | 31 (79.0) | 0.087 | |
Note: ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BVP, biventricular pacing; LOT-CRT, left bundle branch-optimized cardiac resynchronization therapy; LVEDD, left ventricular end-diastolic diameter; LVEDV, left ventricle end-diastolic volume; LVEF, left ventricular ejection fraction; LVESV, left ventricular end-systolic volume; NYHA, New York Heart Association; RV, right ventricle; QRSd, QRS duration; LVDS, left ventricular diastolic size; MRA, mitral regurgitation area; NT-proBNP, N-terminal pro-brain natriuretic peptide.
At the time of implantation, the mean QRSd in the LOT-CRT group
was significantly shorter than in the BVP group (p
| BVP group | LOT-CRT group | p-value | ||
| Variables | N = 35 | N = 39 | ||
| CRT-D, n (%) | 26 (74.3) | 31 (79.5) | 0.865 | |
| At implantation | ||||
| Threshold, at 0.4 ms, V | 1.28 |
0.83 |
0.002** | |
| Paced QRSd, ms | 157.6 |
128.0 |
||
| X-ray exposure duration (total), min | 40.4 |
32.6 |
||
| Impedance, |
772.8 |
608.2 |
||
| Follow-up | ||||
| VP (%) | 96.1 |
98.3 |
0.265 | |
| Paced QRSd, ms | 151.0 |
114.0 |
||
| Threshold, at 0.4 ms, V | 1.32 |
0.74 |
||
| Impedance, |
726.3 |
562.8 |
||
Note: **p
The LOT-CRT group showed significantly greater LVEF (p
| BVP group | LOT-CRT group | p-value | ||
| Variables | N = 35 | N = 39 | ||
| Echocardiography parameters | ||||
| LVEDD, mm | 62.6 |
47.4 |
||
| LVEF, % | 34.0 |
55.5 |
||
| Echocardiographic response, n (%) | 20 (57.1) | 31 (79.5) | 0.033* | |
| Upper‐response, n (%) | 6 (17.1) | 16 (41.0) | 0.001** | |
| NYHA class | 2.4 |
1.2 |
||
| NYHA I, n (%) | 6 (17.1) | 19 (48.8) | ||
| NYHA II, n (%) | 18 (51.5) | 16 (41.0) | ||
| NYHA III, n (%) | 9 (25.7) | 4 (10.2) | ||
| NYHA IV, n (%) | 3 (8.6) | 0 (0.0) | ||
| NT‐proBNP, pg/mL | 1224.3 (568.5, 2310.7) | 432.9 (210.9, 709.2) | ||
| Clinical response, n (%) | 26 (74.2) | 35 (89.7) | 0.021* | |
Note: *p
Ischemic cardiomyopathy refers to the left ventricular systolic dysfunction caused by coronary artery disease (CAD), which is the most common cause of HF worldwide [15]. The five-year mortality of ICM patients with HF ranges from 50% to 84% [16]. Thus, developing individualized treatment strategies for such patients represents a key challenge in clinical practice.
BVP is an established treatment for patients with LV systolic dysfunction (LVEF
Hence, we conducted a preliminary investigation into the application of LOT-CRT
in patients with ICM-induced HF and compared it with the traditional BVP.
An intention-to-treat analysis at a six-month follow-up revealed
several significant findings: the LOT-CRT group exhibited lower immediate and
follow-up threshold and impedance (p
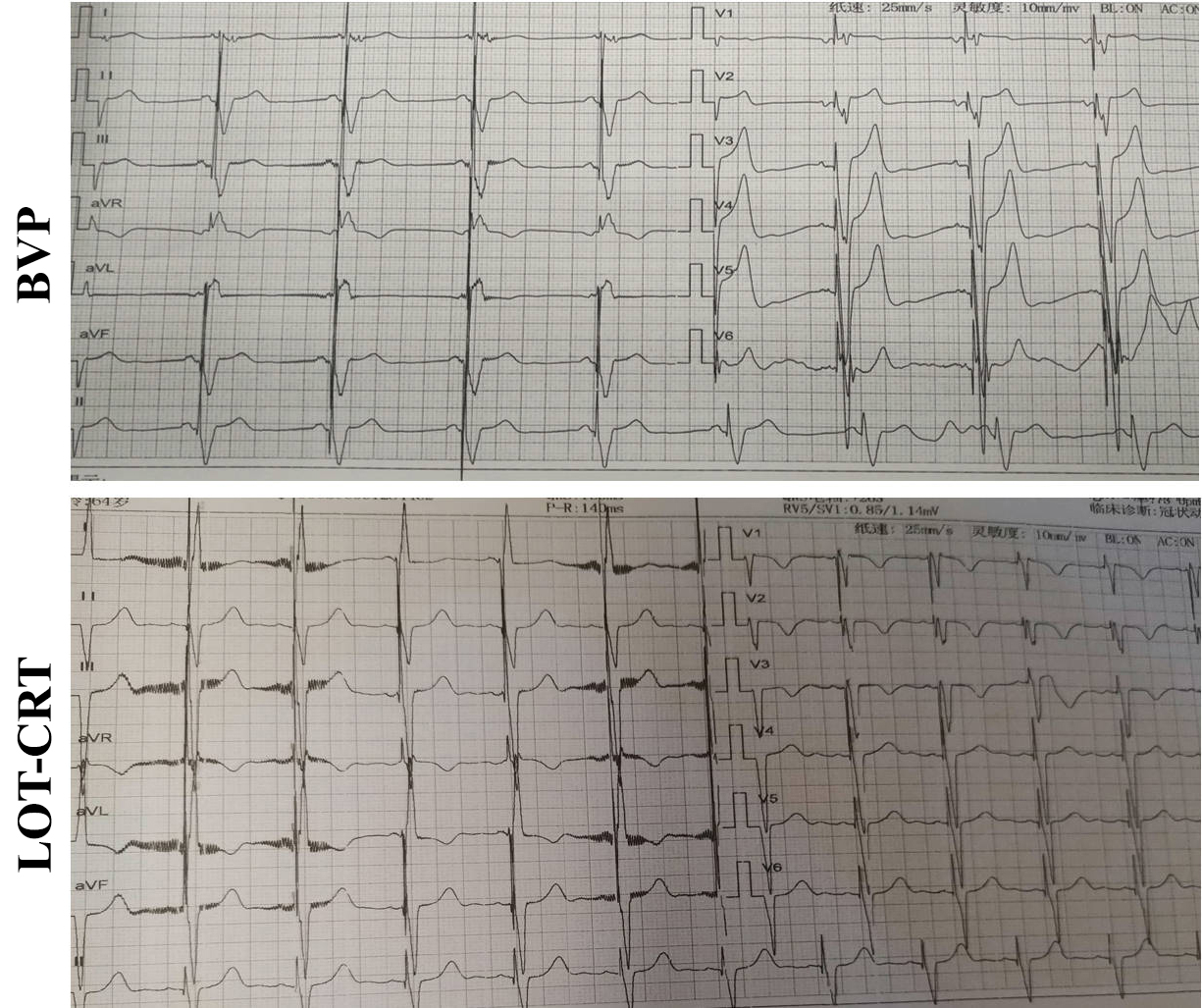 Fig. 2.
Fig. 2.
Typical image of an ECG in the two groups at six months post-surgery.
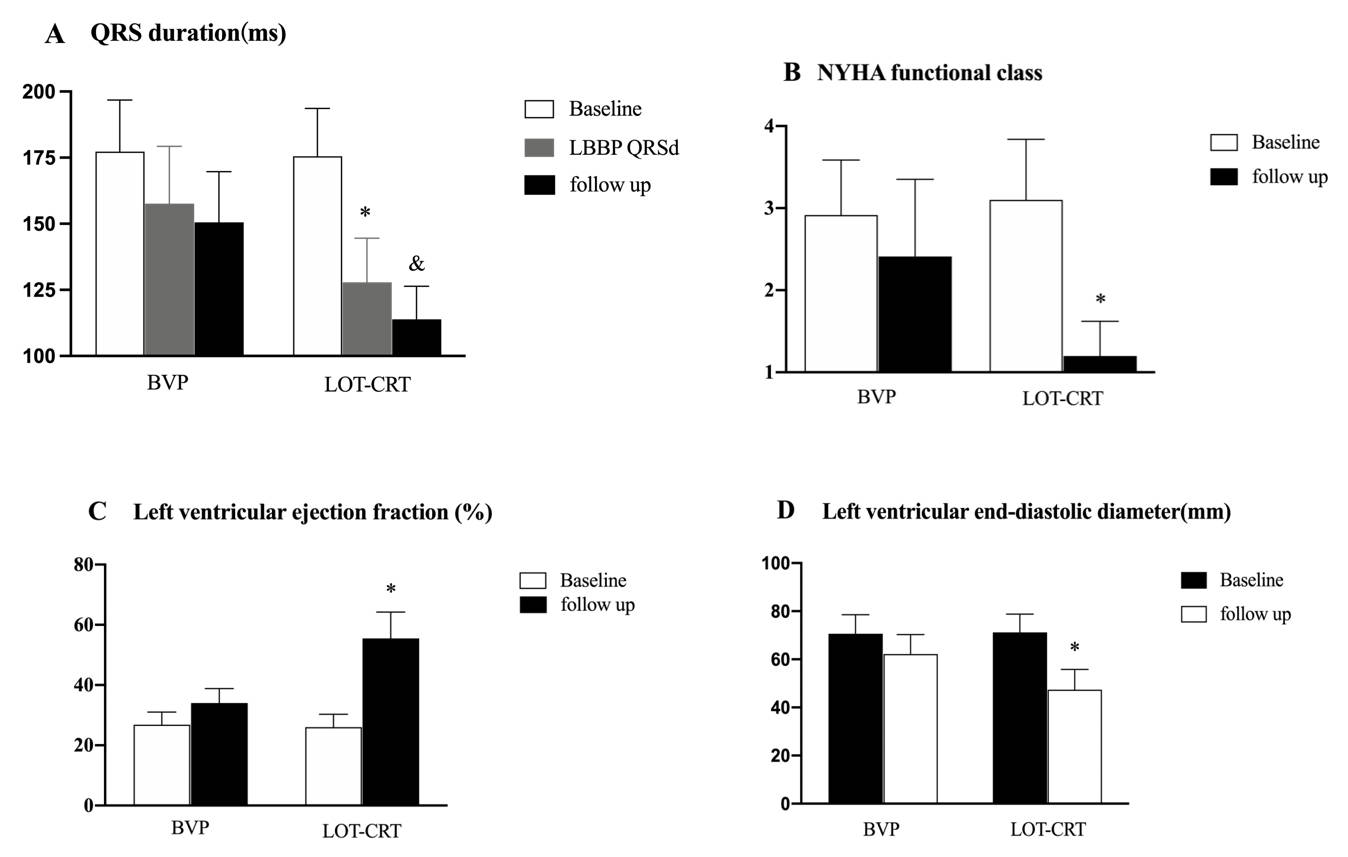 Fig. 3.
Fig. 3.
Comparison of the QRS duration and cardiac function at baseline
and six months follow-up. (A) QRS duration at implantation and six-month
follow-up were significantly shorter in the LOT-CRT group. (B,C) The NYHA cardiac
function grade and LVEF at the six-month follow-up were significantly improved in
the LOT-CRT group. (D) The left ventricular end-diastolic diameter at the
six-month follow-up was significantly lower in the LOT-CRT group.
&p
Furthermore, the results of our study not only demonstrate superior echocardiographic outcomes with LOT-CRT compared to BVP but also suggest the potential for a reduction in arrhythmic episodes. Indeed, it is well-known that improved mechanical synchrony, as indicated by better echocardiographic response, can reduce the burden of arrhythmias in patients with heart failure. Recent studies, such as the one by Compagnucci P, et al. [32], have shown that LOT-CRT is associated with a lower incidence of arrhythmic events, likely due to increased physiological pacing and improved ventricular function. These findings are consistent with our observation that LOT-CRT achieves superior LVEF improvement and greater QRS narrowing, both of which are critical in minimizing arrhythmogenic substrates. Therefore, LOT-CRT may offer a dual benefit of both improving cardiac function and reducing arrhythmia risk, particularly in patients with ischemic cardiomyopathy.
Some limitations of this study warrant consideration. This study was conducted at a single center with a small sample size and a short follow-up period, which may have introduced potential bias. Therefore, more robust, multi-center prospective studies are needed to investigate further the efficacy of LOT-CRT in HF patients with LBBB.
While the results of this study are promising, they should be interpreted in the context of certain limitations. Notably, the follow-up period of six months, while sufficient to observe initial clinical improvements and device integration, may not fully capture long-term outcomes such as survival rates, chronic device complications, or late-stage device optimizations. Subsequently, this relatively short follow-up period limits our ability to generalize the findings to longer-term clinical scenarios where factors such as lead integrity, device longevity, and patient adaptation to the device play a more pronounced role. Therefore, future studies with extended follow-up durations are needed to validate these initial findings and provide a more comprehensive assessment of the long-term benefits and risks associated with LOT-CRT.
In this study, LOT-CRT in patients with ICM-induced HF with LBBB demonstrated superior echocardiographic response and clinical outcome compared to BVP. Our findings indicated that LOT-CRT may be a potential alternative to BVP in these patients. Additional research is essential to establish more definitive evidence.
The data and materials supporting the findings of this study are available from the corresponding author upon reasonable request.
DZ: Conceptualization, methodology, and writing of the manuscript; ML: Data collection and statistical analysis; BSPE and IEMAA: Supervision and review of the manuscript. All authors contributed to the study design, reviewed the manuscript critically for important intellectual content, and approved the final version for submission. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was approved by the Medical Ethics Committee of the Fifth People’s Hospital Affiliated with the Chengdu University of Traditional Chinese Medicine (Ethics Number: Ethical review 2022-009 (Section) -01). Written informed consent was obtained from all patients before their enrolment. This study was conducted in accordance with the guidelines of the Declaration of Helsinki.
We would like to express our gratitude to the staff of Chengdu Fifth People’s Hospital for their support during the study and to Dr. Tang Mingyang for his valuable insights and contributions to the planning and implementation of the research.
Project No. 2023219, Chengdu Municipal Health Commission, Sichuan, China.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.