







1 Department of Endocrinology, The Third Affiliated Hospital of Anhui Medical University (Hefei First People’s Hospital), 230022 Hefei, Anhui, China
2 Department of Cardiology, The Third Affiliated Hospital of Anhui Medical University (Hefei First People’s Hospital), 230022 Hefei, Anhui, China
Abstract
The association between the platelet to high-density lipoprotein cholesterol ratio (PHR) and the risk of a heart disease event remains unclear. This study aims to determine whether the PHR can identify individuals at high risk for heart disease events, with a particular focus on middle-aged and elderly Chinese individuals.
The retrospective cohort study encompassed 7188 middle-aged and elderly participants (>45 years) sourced from the China Health and Retirement Longitudinal Study (CHARLS) database. This research utilized longitudinal data from 5 follow-up visits spanning 2011 to 2020, which encompassed the collection of demographic profiles and pertinent blood biomarkers. Kaplan-Meier survival analysis was conducted based on PHR quartiles, with differences assessed using the log-rank test. The Cox proportional hazards model evaluated PHR’s hazard ratio (HR) as a predictor of outcome events, with trend tests applied. Restrictive cubic splines (RCS) were employed to explore associations. Subgroup analyses were performed to validate the robustness of the findings.
Baseline comparisons across quartiles of the PHR revealed a progressive increase in PHR values (133.16 vs 202.09 vs 267.04 vs 388.24), which corresponded to ascending incidence rates of heart disease (18.20% vs 18.64% vs 18.86% vs 21.59%) (p < 0.05). The Kaplan-Meier survival analysis of PHR quartile groups revealed a notable elevation in the incidence of cardiovascular events in Q4 compared to Q1, Q2, and Q3 throughout the follow-up period (log-rank p < 0.05). Upon adjustment for age, gender, stroke history, drinking, smoking, body mass index (BMI), white blood cell (WBC) count, fasting plasma glucose (FPG), creatinine (Cr), and triglyceride (TG), the Q4 group continued to exhibit a significantly elevated HR relative to Q1 (HR = 1.203, p = 0.023). Furthermore, RCS affirmed a linear association between PHR and heart disease events (Adjusted: Overall p = 0.014, Nonlinear p = 0.588). When analyzing by gender, high PHR was a risk factor for males (Q4: HR = 1.352, p = 0.019), but not for females (Q4: HR = 1.158, p = 0.166). Subgroup analysis indicates a significant association between higher PHR levels and increased risk of cardiac events compared to lower levels.
Our study reveals a positive correlation between PHR levels and the incidence of heart disease events in middle-aged and elderly men in China. However, no such correlation was observed in female patients.
Keywords
- platelets to high density lipoprotein cholesterol ratio
- heart disease events
- CHARLS
Cardiovascular disease (CVD) currently accounts for approximately one-third of all global deaths, with a notable increase of 12.5% over the past decade [1], which was the primary cause of mortality among both urban and rural residents in China. The 2022 China Cardiovascular Health and Disease Report emphasizes the widespread impact of CVD, estimating 330 million cases. This includes 11.39 million cases of coronary heart disease (CHD), 8.9 million cases of heart failure, as well as significant numbers of other conditions such as pulmonary heart disease, atrial fibrillation, rheumatic heart disease, and congenital heart disease [2]. Risk factors such as smoking, sedentary lifestyle, and aging contribute to the increasing incidence and mortality of CVD in China. Projections based on a Maldivian computer simulation model suggest a more than 50% annual increase in CVD events in China from 2010 to 2030, underscoring the urgent need for effective preventive measures [3]. As global management of heart disease transitions to prevention, it is crucial to identify reliable indicators of high cardiovascular risk.
The platelet to high-density lipoprotein cholesterol ratio (PHR) has emerged as a promising biomarker for assessing inflammatory and lipid metabolic health, which is essential for maintaining the balance between clotting and anti-inflammatory processes in the bloodstream. Its effectiveness is primarily attributed to the significant roles of platelets and high-density lipoprotein cholesterol (HDL-C) in vascular health and the immune system. Excessive or aberrantly activated platelets may contribute to the development of atherosclerosis, thereby increasing the risk of thrombosis. HDL-C, often referred to as “good cholesterol”, facilitates the removal of excess cholesterol from arteries and possesses antioxidant and anti-inflammatory properties, thereby safeguarding arterial health. In contrast to isolated platelet counts or HDL-C levels, PHR offers a more comprehensive assessment of the balance between thrombus formation and arterial health by integrating data from both metrics. Notably, PHR not only reflects the anti-inflammatory and antioxidant capabilities of the vasculature but also serves as an indicator of systemic inflammatory responses. Under inflammatory conditions, platelet activation is enhanced, while HDL-C levels decrease. Consequently, PHR can act as a more sensitive marker for monitoring the progression of inflammatory diseases, such as atherosclerosis and myocarditis. Additionally, the total cholesterol-to-HDL-C ratio is commonly utilized for evaluating cardiovascular health; however, this approach overlooks the role of platelets. By incorporating both platelets and HDL-C, PHR provides a more comprehensive evaluation of potential thrombotic risk. Preliminary research suggests that elevated PHR levels may correlate with an increased risk of atherosclerosis, thrombosis, and metabolic syndrome [4]. Furthermore, PHR has shown promise in predicting the severity of coronary artery stenosis and the prognosis of patients with CHD [5, 6]. Nevertheless, the capacity of PHR to effectively predict future heart disease risk remains uncertain and requires further investigation [7].
Currently, there is a lack of studies exploring the predictive value of PHR specifically for heart disease occurrence in middle-aged and elderly populations. This study aims to address this gap using data from the CHARLS database, focusing on middle-aged and elderly Chinese individuals. Its objective is to determine whether PHR can identify high-risk individuals for heart disease events, potentially informing targeted preventive strategies in these high-risk groups.
The China Health and Retirement Longitudinal Study (CHARLS) is a comprehensive national longitudinal social survey database encompassing middle-aged and elderly individuals in China [8]. Initiated in 2011, CHARLS is a collaborative effort between the Institute of Economics at the Chinese Academy of Social Sciences and the China Center for Economic Research at Peking University, with funding from the National Institutes of Health (NIH), the National Science Foundation (NSF), among others. This database integrates various data modalities, including structured questionnaires, physiological measurements, and biological samples, spanning urban and rural regions nationwide, and ensuring national representativeness.
This research utilized longitudinal data from 5 follow-up visits spanning 2011
to 2020, capturing demographic profiles and pertinent blood biomarkers. Exclusion
criteria were applied to remove entries lacking essential baseline indicators or
definitive heart disease status. The retrospective cohort study encompassed 7188
middle-aged and elderly participants (
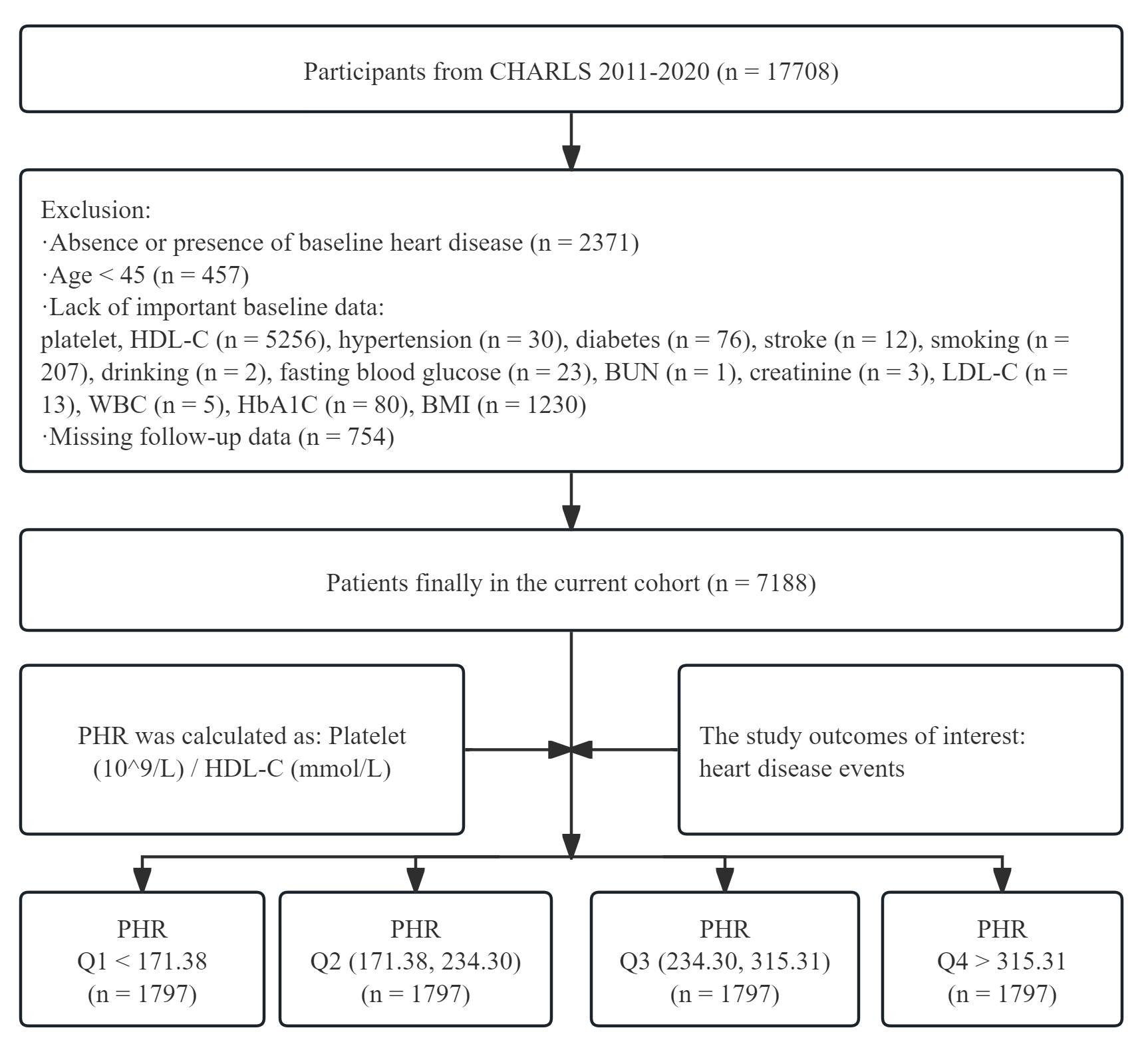 Fig. 1.
Fig. 1.
Flow chart for inclusion of participants. CHARLS, China Health and Retirement Longitudinal Study; HDL-C, high density lipoprotein cholesterol; BUN, blood urea nitrogen; LDL-C, low density lipoprotein cholesterol; HbA1C, glycosylated hemoglobin; BMI, body mass index; PHR, platelets to high density lipoprotein cholesterol ratio; WBC, white blood cell; Q1, quartile 1 of PHR; Q2, quartile 2 of PHR; Q3, quartile 3 of PHR; Q4, quartile 4 of PHR.
In this study, PHR was defined as the ratio of platelet count
(
This study utilized data was analyzed with the use of the statistical packages R
(The R Foundation; http://www.r-project.org; version 4.2.0) and EmpowerStats
(http://www.empowerstats.net/, X&Y solutions, Inc. Boston, MA, USA) for
statistical analyses. The study cohort was stratified into four groups based on
quartiles of the PHR: Q1 (n = 1797, PHR
In this study, a total of 7188 subjects were enrolled, with a median follow-up
period of 108 months. Among them, 1389 participants (19.32%) experienced a
cardiovascular event. Baseline comparisons across quartiles of the PHR revealed a
progressive increase in PHR values (133.16 vs 202.09 vs 267.04 vs 388.24)
corresponding to ascending incidence rates of heart disease (18.20% vs 18.64%
vs 18.86% vs 21.59%) (Table 1). Significant differences (p
| Variables | Total (n = 7188) | Q1 ( |
Q2 (171.38, 234.30) | Q3 (234.30, 315.31) | Q4 ( |
p | |
| (n = 1797) | (n = 1797) | (n = 1797) | (n = 1797) | ||||
| Age (years), Mean |
58.77 |
60.11 |
59.19 |
58.07 |
57.69 |
||
| Time (month), M (Q1, Q3) | 108.00 (84.00, 108.00) | 108.00 (84.00, 108.00) | 108.00 (84.00, 108.00) | 108.00 (84.00, 108.00) | 108.00 (84.00, 108.00) | 0.122 | |
| WBC ( |
6.25 |
5.69 |
6.06 |
6.41 |
6.83 |
||
| PLT ( |
207.00 (162.00, 255.00) | 139.00 (111.00, 170.00) | 192.00 (165.00, 222.00) | 226.00 (197.00, 260.00) | 273.00 (237.00, 311.00) | ||
| Cr (mg/dL), Mean |
0.78 |
0.79 |
0.77 |
0.77 |
0.77 |
0.209 | |
| UA (mg/dL), Mean |
4.41 |
4.41 |
4.35 |
4.41 |
4.48 |
0.016 | |
| BMI (kg/m2), Mean |
23.45 |
22.51 |
22.88 |
23.80 |
24.62 |
||
| TC (mmol/L), Mean |
3.39 |
3.41 |
3.40 |
3.40 |
3.36 |
0.119 | |
| TG (mmol/L), Mean |
2.22 |
1.67 |
1.94 |
2.18 |
3.08 |
||
| HDL-C (mmol/L), Mean |
0.90 |
1.12 |
0.96 |
0.85 |
0.68 |
||
| LDL-C (mmol/L), Mean |
2.05 |
1.99 |
2.07 |
2.12 |
2.02 |
||
| HbAlC (%), Mean |
5.27 |
5.19 |
5.24 |
5.30 |
5.34 |
||
| FPG (mmol/L), M (Q1, Q3) | 5.67 (5.24, 6.22) | 5.61 (5.21, 6.08) | 5.64 (5.25, 6.16) | 5.65 (5.22, 6.23) | 5.78 (5.30, 6.45) | ||
| CRP (mg/L), M (Q1, Q3) | 0.98 (0.54, 2.08) | 0.82 (0.48, 1.73) | 0.87 (0.49, 1.86) | 1.01 (0.54, 2.10) | 1.30 (0.70, 2.63) | ||
| PHR, M (Q1, Q3) | 234.30 (171.38, 315.31) | 133.16 (109.39, 154.15) | 202.09 (186.64, 218.79) | 267.04 (250.04, 289.34) | 388.24 (346.01, 461.48) | ||
| Heart event, n (%) | 0.043 | ||||||
| No | 5799 (80.68) | 1470 (81.80) | 1462 (81.36) | 1458 (81.14) | 1409 (78.41) | ||
| Yes | 1389 (19.32) | 327 (18.20) | 335 (18.64) | 339 (18.86) | 388 (21.59) | ||
| Stroke, n (%) | 0.081 | ||||||
| No | 7037 (97.90) | 1757 (97.77) | 1771 (98.55) | 1760 (97.94) | 1749 (97.33) | ||
| Yes | 151 (2.10) | 40 (2.23) | 26 (1.45) | 37 (2.06) | 48 (2.67) | ||
| Gender, n (%) | 0.027 | ||||||
| Female | 3859 (53.69) | 917 (51.03) | 969 (53.92) | 966 (53.76) | 1007 (56.04) | ||
| Male | 3329 (46.31) | 880 (48.97) | 828 (46.08) | 831 (46.24) | 790 (43.96) | ||
| Drinking, n (%) | |||||||
| No | 4754 (66.14) | 1094 (60.88) | 1150 (64.00) | 1215 (67.61) | 1295 (72.06) | ||
| Yes | 2434 (33.86) | 703 (39.12) | 647 (36.00) | 582 (32.39) | 502 (27.94) | ||
| Smoking, n (%) | 0.093 | ||||||
| No | 5009 (69.69) | 1217 (67.72) | 1248 (69.45) | 1258 (70.01) | 1286 (71.56) | ||
| Yes | 2179 (30.31) | 580 (32.28) | 549 (30.55) | 539 (29.99) | 511 (28.44) | ||
| Hypertension, n (%) | |||||||
| No | 3903 (54.30) | 1010 (56.20) | 1026 (57.10) | 968 (53.87) | 899 (50.03) | ||
| Yes | 3285 (45.70) | 787 (43.80) | 771 (42.90) | 829 (46.13) | 898 (49.97) | ||
| Diabetes, n (%) | |||||||
| No | 6135 (85.35) | 1595 (88.76) | 1556 (86.59) | 1528 (85.03) | 1456 (81.02) | ||
| Yes | 1053 (14.65) | 202 (11.24) | 241 (13.41) | 269 (14.97) | 341 (18.98) | ||
SD, standard deviation; M, median; PHR, platelets to high density lipoprotein cholesterol ratio; WBC, white blood cell; PLT, platelet; Cr, creatinine; UA, uric acid; BMI, body mass index; TC, total cholesterol; TG, triglyceride; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; HbA1C, glycosylated hemoglobin; FPG, fasting plasma glucose; CRP, C-reactive protein; Q1, quartile 1 of PHR; Q2, quartile 2 of PHR; Q3, quartile 3 of PHR; Q4, quartile 4 of PHR.
Based on the Kaplan-Meier survival analysis of PHR quartile groups, the
incidence of cardiovascular events was notably elevated in Q4 compared to Q1, Q2,
and Q3 throughout the follow-up period (log-rank p
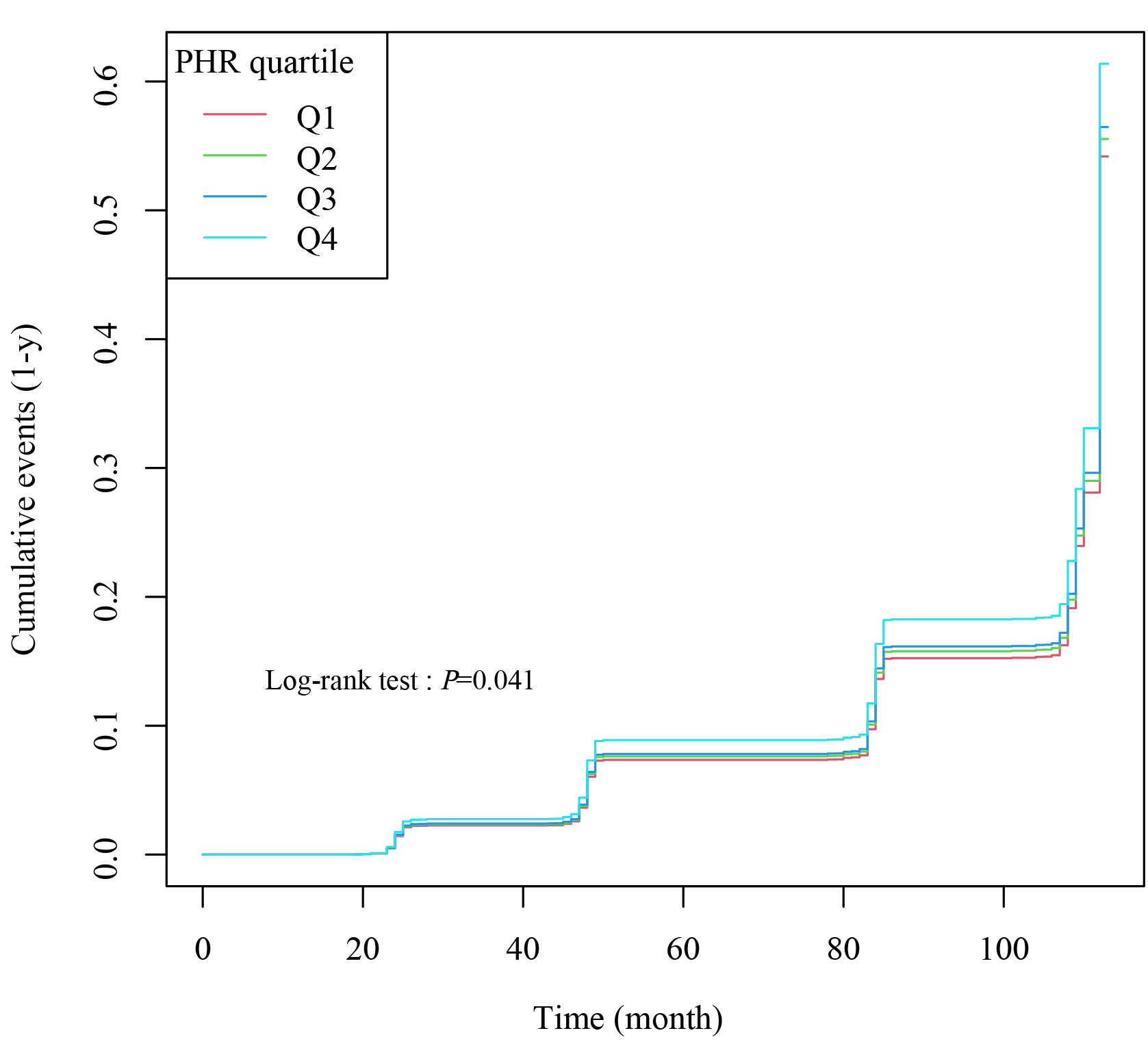 Fig. 2.
Fig. 2.
Kaplan-Meier cumulative risk curve for cardiac events. PHR, platelets to high density lipoprotein cholesterol ratio; Q1, quartile 1 of PHR; Q2, quartile 2 of PHR; Q3, quartile 3 of PHR; Q4, quartile 4 of PHR.
Using group Q1 as the reference, a Cox proportional hazards
model was employed to assess the association between PHR and incidents of heart
disease. Initially, without adjusting for pertinent risk factors, the hazard ratio (HR) in the
Q4 group significantly exceeded that of Q1, underscoring a notable association
between elevated PHR and heightened susceptibility to heart disease events (Q4:
HR = 1.214, p = 0.009) (Table 2). Upon adjustment for age, gender,
stroke history, drinking, smoking, BMI, WBC, FPG Cr, and TG,
the Q4 group continued to exhibit a significantly elevated HR relative to Q1 (Q4:
HR = 1.203, p = 0.023) (Table 2). When treating PHR as a continuous
variable, each interquartile range increase was associated with a 4.4% rise in
the risk of new heart events (HR = 1.044, p
| Exposure | Non-adjusted | Adjust I | Adjust II | ||||
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | ||
| PHR | 1.041 (1.019, 1.064) | 1.049 (1.027, 1.072) | 1.044 (1.019, 1.070) | ||||
| PHR quartile | |||||||
| Q1 | 1.0 | 1.0 | 1.0 | ||||
| Q2 | 1.036 (0.889, 1.206) | 0.652 | 1.048 (0.900, 1.221) | 0.545 | 1.051 (0.902, 1.226) | 0.522 | |
| Q3 | 1.056 (0.907, 1.230) | 0.481 | 1.103 (0.947, 1.284) | 0.208 | 1.056 (0.904, 1.235) | 0.490 | |
| Q4 | 1.214 (1.048, 1.407) | 0.009 | 1.276 (1.101, 1.479) | 0.001 | 1.203 (1.025, 1.412) | 0.023 | |
| PHR for trend | 1.064 (1.015, 1.115) | 0.010 | 1.083 (1.033, 1.135) | 0.001 | 1.058 (1.005, 1.114) | 0.032 | |
| Male | |||||||
| Q1 | 1.0 | 1.0 | 1.0 | ||||
| Q2 | 0.982 (0.767, 1.258) | 0.886 | 1.033 (0.806, 1.323) | 0.800 | 1.052 (0.820, 1.350) | 0.691 | |
| Q3 | 1.028 (0.805, 1.314) | 0.825 | 1.100 (0.860, 1.406) | 0.449 | 1.076 (0.838, 1.381) | 0.566 | |
| Q4 | 1.305 (1.035, 1.646) | 0.025 | 1.434 (1.135, 1.812) | 0.003 | 1.352 (1.050, 1.742) | 0.019 | |
| Female | |||||||
| Q1 | 1.0 | 1.0 | 1.0 | ||||
| Q2 | 1.103 (0.909, 1.337) | 0.321 | 1.108 (0.914 1.344) | 0.298 | 1.087 (0.895, 1.320) | 0.399 | |
| Q3 | 1.044 (0.858, 1.269) | 0.669 | 1.086 (0.893 1.321) | 0.408 | 1.022 (0.836, 1.250) | 0.834 | |
| Q4 | 1.186 (0.981, 1.434) | 0.078 | 1.243 (1.028 1.504) | 0.065 | 1.158 (0.941, 1.426) | 0.166 | |
Non-adjusted model adjust for: None.
Adjust I model adjust for: Age; Gender.
Adjust II model adjust for: Age; Gender; Stroke; Drinking; Smoking; BMI; WBC; FPG; Cr; TG; LDL-C; CRP; HbA1C; UA; Hypertension; Diabetes.
PHR for trend: trend test of PHR and cardiac events.
PHR, platelets to high density lipoprotein cholesterol ratio; HR, hazard ratio; CI, confidence interval; BMI, body mass index; WBC, white blood cell; FPG, fasting plasma glucose; Cr, creatinine; TG, triglyceride; LDL-C, low density lipoprotein cholesterol; CRP, C-reactive protein; HbA1C, glycosylated hemoglobin; UA, uric acid; Q1, quartile 1 of PHR; Q2, quartile 2 of PHR; Q3, quartile 3 of PHR; Q4, quartile 4 of PHR.
To evaluate the linearity of the relationship between PHR and heart
disease events, a bar chart was constructed. This graphical representation
illustrates a progressive increase in heart disease events as PHR values ascend
from Q1 to Q4 (Fig. 3). Furthermore, RCS analysis affirmed a linear association
between PHR and heart disease events, maintaining significance across adjusted
and non-adjusted models (Non-adjusted: Overall p
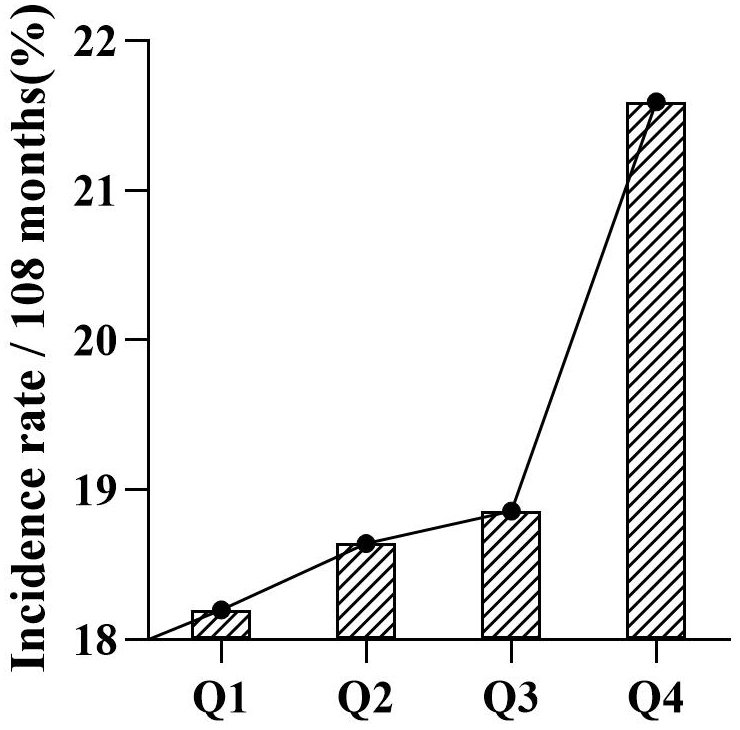 Fig. 3.
Fig. 3.
Comparison of the incidence of cardiac events in the PHR quartile population. PHR, platelets to high density lipoprotein cholesterol ratio.
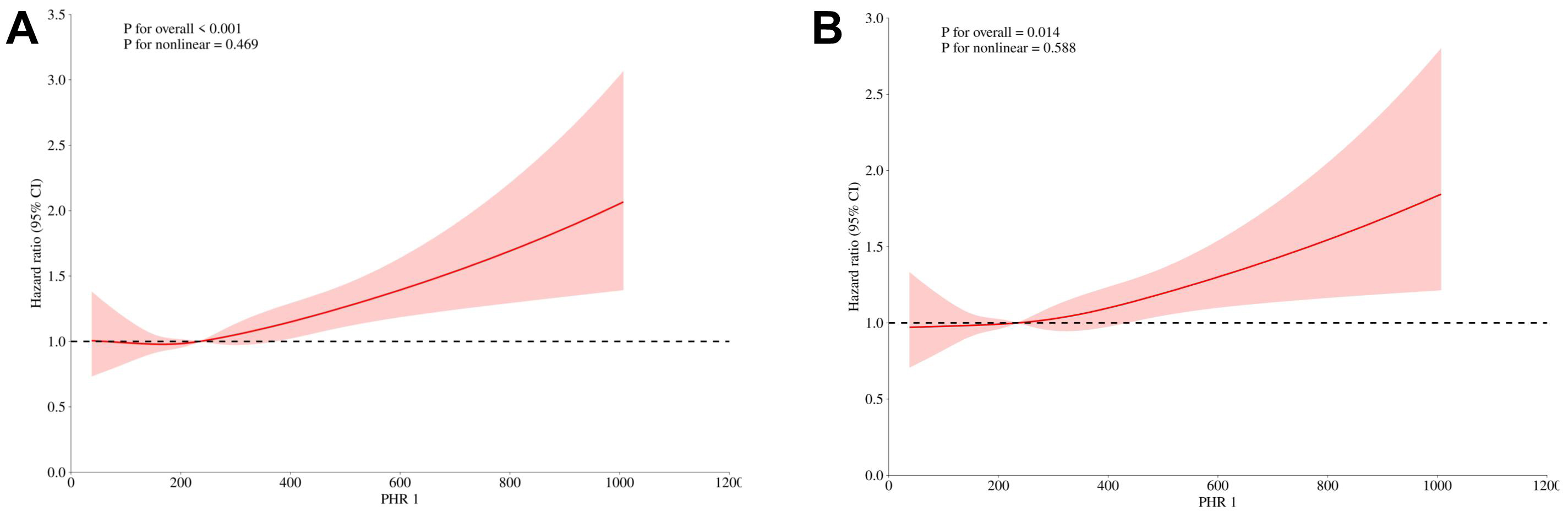 Fig. 4.
Fig. 4.
Restricted cubic spline curve for PHR hazard ratio (A: Non-adjusted. B: Adjusted for: Age; Gender; Stroke; Drinking; Smoking; Hypertension; Diabetes). CI, confidence interval; PHR, platelets to high density lipoprotein cholesterol ratio.
To assess the robustness of the association between elevated PHR and the
incidence of heart disease events, and to examine potential subgroup variations
in this association, we categorized PHR into quartiles and stratified by common
risk factors: age (
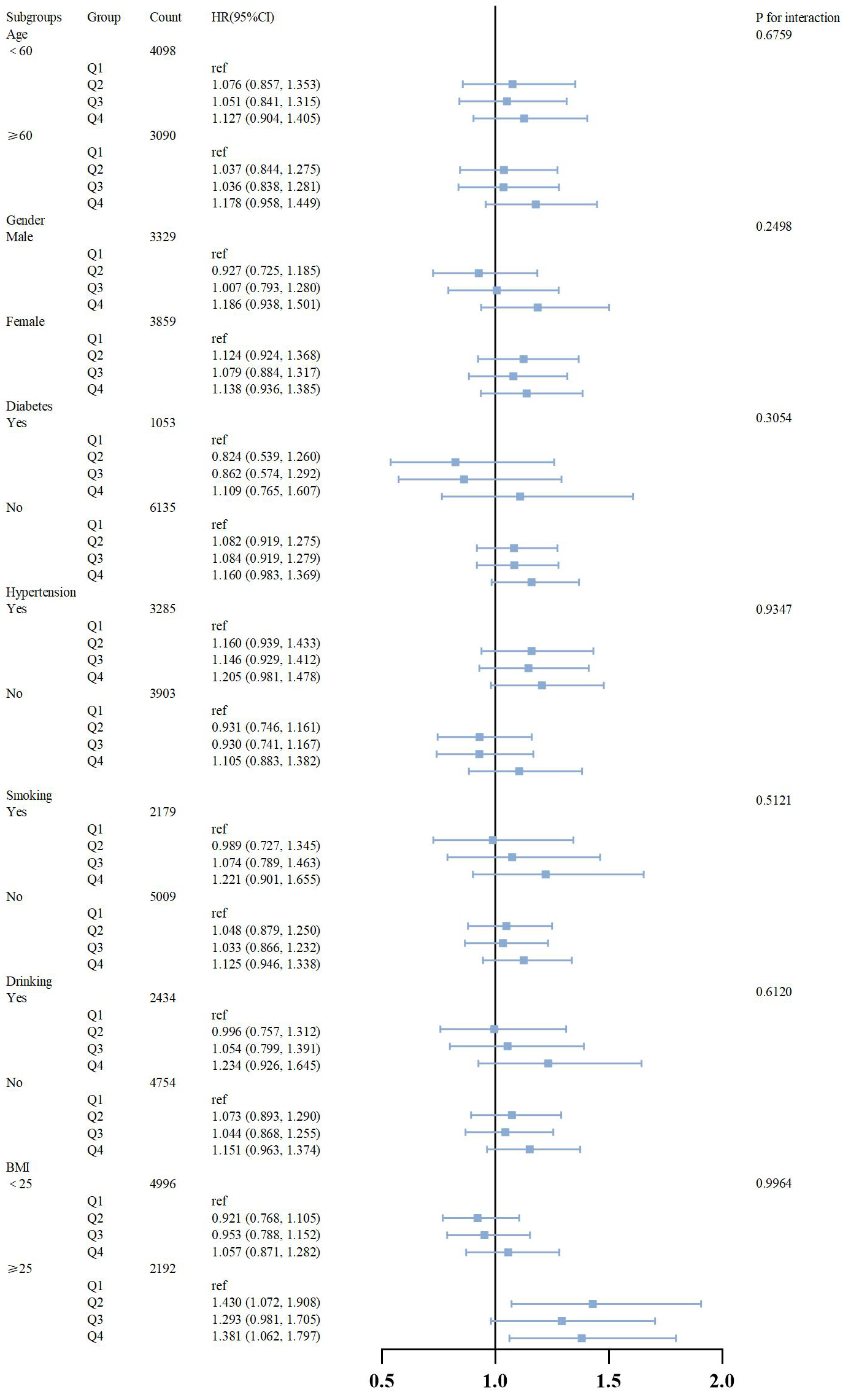 Fig. 5.
Fig. 5.
Subgroup analysis of outcomes from cardiac events. HR, hazard ratio; CI, confidence interval; BMI, body mass index; Q1, quartile 1 of PHR; Q2, quartile 2 of PHR; Q3, quartile 3 of PHR; Q4, quartile 4 of PHR.
Previous studies have shown associations between PHR and patient outcomes in metabolic syndrome, stroke, and cardiovascular disease [4, 5, 6]. However, the specific relationship between PHR and heart disease requires further elucidation. This retrospective cohort study analyzed data from 7188 participants in the CHARLS database spanning 2011 to 2020, with a median follow-up of 108 months. Controlling for pertinent confounders, our findings indicate a significant association between PHR and incident cardiac events. Furthermore, employing RCS regression revealed a linear trend, underscoring an incremental risk of heart disease events with higher PHR values. These results suggest that PHR holds promise as a prognostic indicator for heart disease occurrence.
PHR has been demonstrated to possess both inflammatory and lipid metabolic properties. Consequently, it is currently regarded as a reliable marker of inflammation. Previous research has extensively explored the relationship between PHR and lipid metabolic disorders as well as CVDs. A cohort study utilizing the 2005–2018 the National Health and Nutrition Examination Survey (NHANES) data has revealed a correlation between PHR and CVD mortality risk in stroke survivors [9]. However, this study was limited in scope, as it was conducted exclusively with stroke survivors, which limits the extent to which its findings can be generalized. This study builds upon previous research by examining the relationship between PHR and cardiac disease, with a particular focus on middle-aged and older populations, who are at elevated risk for cardiac disease and may potentially benefit from this investigation in a significant clinical manner. Moreover, a real-world study of coronary artery disease patients with type 2 diabetes mellitus (T2DM) revealed an association between PHR and long-term adverse outcomes [5]. This study’s narrow focus on coronary artery disease limits its applicability and primarily examines prognosis, whereas our research emphasizes the preventive aspects of PHR in cardiac disease. Furthermore, a study of patients with depression indicated a potential correlation between PHR and cardiovascular mortality in this population [10]. However, the focus of this study on prognosis contrasts with our focus on the risk of incident disease. Previous research has also investigated PHR in relation to metabolic syndrome risk factors such as hypertension, diabetes, and obesity, all of which are known risk factors for cardiac events. Nonetheless, direct associations between PHR and cardiac events have not been reported [4]. Furthermore, our study reveals that PHR shows a stronger association with cardiac events in men, whereas no significant correlation was observed in females. This could potentially be due to the higher estrogen levels in women, which reduce platelet activity compared to males.
Platelets, which originate from megakaryocytes, serve as crucial participants in
hemostasis, thrombosis, and various physiological processes. They are
increasingly being recognized as non-traditional risk factors in the context of
CVD [7]. Recent studies indicate that platelets influence the development of CVD
by modulating the properties of vascular endothelial cells, thereby promoting
monocyte and lymphocyte infiltration into artery walls [11, 12, 13, 14, 15]. This
platelet-mediated influence on endothelial cells is tightly regulated by
receptors such as
Numerous epidemiological studies have consistently identified low HDL-C as a significant risk factor for CVD, particularly in patients with early-onset coronary artery disease. The incidence of CVD is inversely proportional to HDL-C concentration [24]. Each 1 mg/dL increase in HDL-C is associated with a 2% to 3% lower risk of CVD [25]. HDL-C plays a crucial role in the reduction of atherosclerosis through cholesterol reverse transport, whereby HDL-C particles act as vehicles for the removal of cholesterol from peripheral tissues and its subsequent excretion in the liver [26]. The precise mechanisms underlying HDL-C’s regulatory and protective effects on endothelial function remain incompletely understood. Recent research has demonstrated that reconstituted HDL-C (rHDL-C) particles containing apolipoprotein A-I and phospholipids stimulate nitric oxide (NO) production in endothelial cells, inhibit apoptosis, and promote endothelial cell migration and re-endothelialization [27, 28, 29].
HDL-C and platelets engage in complex interactions that collectively regulate the onset and progression of CVD. HDL-C has been identified as an independent predictor of acute platelet thrombosis. It exerts antiplatelet effects by inhibiting processes such as platelet aggregation, fibrinogen binding, granule secretion, and thromboxane A2 release [30, 31]. Furthermore, HDL-C facilitates vascular dilation, enhancing blood flow and restraining platelet inflammatory activation and thrombosis through endothelial cell signaling pathways. Activation of protein kinase B (PKB), mitogen-activated protein kinase (p42/44MAPK), Ca2+ calmodulin-dependent protein kinase, and adenosine monophosphate (AMP)-activated protein kinase (AMPK) collectively promote the release of vasodilator factors and the production of endothelial NO, thereby further inhibiting platelet activation, atherosclerosis, and thromboinflammatory responses [32, 33, 34, 35, 36]. Additionally, HDL-C enhances prostacyclin (PGI2) synthesis and acts in conjunction with NO to inhibit platelet activation, thus reducing thrombotic risk and the incidence of CVD [37, 38, 39, 40, 41]. Conversely, platelets facilitate the formation of foam cells by enhancing cholesterol ester formation and accumulation in monocyte-derived macrophages which are circulating in the periphery, thereby promoting atherosclerosis and elevating the risk of CVD [42, 43].
PHR emerges as a composite marker reflecting both inflammation and lipid metabolism, offering a straightforward, cost-effective assessment readily applicable in clinical settings. A substantial body of research has underscored the correlation between PHR and cardiovascular diseases. For instance, Jialal and colleagues [4] demonstrated a correlation between PHR and atherosclerosis risk, indicating its potential as a marker for assessing metabolic syndrome and cardiovascular risk. Similarly, a prospective study involving 56,316 patients identified PHR as a promising tool for identifying high-risk individuals among those with CHD and diabetes [5]. Nevertheless further definitive assessments of the association between PHR and cardiovascular risk remain limited. PHR has been proposed as a metabolic indicator for predicting cardiac disease risk, yet definitive evidence supporting its role in identifying future cardiovascular disease risks is lacking and requires further investigation [7].
In this study, significant differences were observed in LDL-C levels among the four groups (Q1 to Q4). Notably, LDL-C levels gradually increased from Q1 to Q3, while a decline was observed in Q4. Previous studies have generally established that a substantial elevation in LDL-C is a primary cause of atherosclerosis. However, numerous observational and experimental studies contradict Bradford-Hill’s causality criteria, failing to establish a clear association between elevated LDL-C levels and the development of atherosclerosis [44]. Furthermore, no controlled, randomized cholesterol-lowering trials in patients with familial hypercholesterolemia (FH) have demonstrated positive outcomes. Additionally, research has suggested that oxidized low density lipoprotein (LDL) promotes platelet activation and arterial thrombosis through scavenger receptors that are constitutively expressed. These receptors transmit lipid-induced stress associated with atherosclerosis to platelets, thereby activating complex signaling pathways that influence thrombus formation and may trigger acute cardiovascular events [45]. This indicates that factors contributing to thrombosis may represent a more significant risk in hyperlipidemia than LDL-C levels alone. Notably, a study has shown that individuals who die prematurely often have elevated levels of lipoprotein(a) [Lp(a)], factor VIII, and/or fibrinogen compared to those with normal life expectancy, while their LDL-C levels do not differ significantly. This suggests that certain FH patients may inherit other genetic risk factors which are more crucial than elevated LDL-C [46].
This study aims to address these gaps by investigating whether PHR can effectively identify individuals at high risk of heart events among middle-aged and elderly adults. Our research, to our knowledge, represents the first attempt to correlate PHR with the incidence of new heart events in this demographic. This investigation could potentially aid in identifying high-risk individuals early, facilitating targeted preventive measures and ultimately extending life expectancy among middle-aged and elderly populations.
Several limitations are inherent in this study. Firstly, it relies on self-reported data from the study subjects, potentially leading to inaccuracies due to inadequate understanding of their own health conditions, including diabetes, hypertension, and heart disease. Such inaccuracies could affect the reliability of questionnaire responses. Secondly, PHR was assessed only at baseline during the initial follow-up, without capturing dynamic changes over time. Therefore, the relationship between dynamic changes in PHR and the incidence of heart disease remains unknown. Thirdly, this study focused on overall heart disease events without distinguishing between specific types such as heart failure, coronary heart disease, and atrial fibrillation. Future research may benefit from examining these distinctions more closely. Fourthly, as a sampling study, there is a possibility of sampling errors which limit generalizability to the broader population. Lastly, this study did not differentiate between ethnic or national populations in relation to PHR and heart disease events. Future multicenter prospective studies should explore these factors to provide a more comprehensive understanding.
In conclusion, our study demonstrates a positive correlation between PHR levels and the incidence of heart disease events among middle-aged and elderly individuals in China. Specifically, higher PHR levels correspond to an increased risk of heart disease events, illustrating a linear relationship between PHR and heart disease risk.
PHR, platelet-to-high-density lipoprotein cholesterol ratio; HDL-C, high-density lipoprotein cholesterol; CHARLS, The China Health and Retirement Longitudinal Study; CVD, cardiovascular disease; CHD, coronary heart disease; NIH, national Institutes of Health; NSF, national Science Foundation; BMI, body mass index; CI, confidence interval; DM, diabetes mellitus; HR, hazard ratios; WBC, white blood cell count; PLT, platelet count; UA, uric acid; BMI, body mass index; TG, triglycerides; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; HbA1C, hemoglobin Alc; FBG, fasting blood-glucose; CRP, C-reactive protein; NO, nitric oxide; RCS, restricted cubic splines; ROS, reactive oxygen species; ICBP, international blood pressure consortium; SD, standard deviation; rHDL-C, reconstituted HDL-C; PGI2, prostacyclin; PKB, protein kinase B; MAPK, mitogen-activated protein kinase; AMPK, AMP-activated protein kinase; Lp(a), lipoprotein(a).
The datasets generated for this study are available on request to the corresponding author.
YH and XH conducted research implementation, performed statistical analysis of data, created figures and tables, and drafted the manuscript. FL and ZG designed the study and revised the manuscript. All authors have reviewed and approved the final version for publication. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Each round of CHARLS investigation was approved by the Biomedical Ethics Committee of Peking University. The field work plan of this round of household questionnaire survey has been approved, and the approval number is IRB00001052-11015. Ethical review and approval were waived for this study since secondary analysis did not require additional institutional review board approval. During the field survey, each respondent who agreed to participate was required to sign two informed consent forms. One copy was kept by the respondent, and the other was stored in the CHARLS office and scanned in PDF format. Therefore, all participants in this project have given informed consent.
The authors thank the Institute of Economics at the Chinese Academy of Social Sciences and the China Center for Economic Research at Peking University for their efforts in creating the data for the CHARLS.
This study was supported by the Young Scientists Fund of Anhui Medical University in 2022 (2022xkj106).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.