

 , Shi-Yue Zheng 1, Fei Guo 1, Chun-Hui He 1, Jing Lin 1, Hao Fu 1, Xin Du 1, Jian-Zeng Dong 1,*
, Shi-Yue Zheng 1, Fei Guo 1, Chun-Hui He 1, Jing Lin 1, Hao Fu 1, Xin Du 1, Jian-Zeng Dong 1,*
1 Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, 100029 Beijing, China
Abstract
The efficacy of beta-blockers in stable coronary artery disease (CAD) patients with preserved left ventricular function remains controversial. We aimed to evaluate the cardiovascular associations of beta-blocker therapy in this population through a comprehensive meta-analysis.
We conducted a systematic review and meta-analysis following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, searching PubMed, EMBASE, Web of Science, Scopus, Google Scholar, and Cochrane databases from inception to May 2025, updating and extending the previous meta-analysis. We included observational studies comparing beta-blocker therapy versus control in stable CAD patients, defined as those without acute coronary syndrome manifestations for a sufficient period (typically >6 months) to ensure clinical stability, with preserved left ventricular ejection fraction (left ventricular ejection fraction >50%). Primary outcome was cardiac death. Secondary outcomes included all-cause mortality, heart failure, myocardial infarction (MI), and stroke. Random-effects models were used for all analyses. Subgroup analyses were conducted for cardiac and all-cause death stratified by propensity score matching status and prior beta-blocker use exclusion criteria. Publication bias was assessed using funnel plots and Peter's test.
Nine observational studies encompassing 903,870 patients (616,645 beta-blocker users vs. 287,225 controls) were included. Beta-blocker therapy showed no significant association with the primary endpoint: cardiac death (hazard ratio (HR) 0.98, 95% CI: 0.93–1.04, p = 0.54). Secondary outcomes similarly demonstrated no significant associations: all-cause mortality (HR 0.98, 95% CI: 0.91–1.05, p = 0.49), MI (HR 1.02, 95% CI: 0.93–1.11, p = 0.72), stroke (HR 1.02, 95% CI: 0.97–1.08, p = 0.43), and heart failure (HR 1.10, 95% CI: 0.95–1.27, p = 0.20). Substantial heterogeneity was observed for all-cause death (I2 = 87%) and heart failure (I2 = 95%). Subgroup analyses failed to identify populations with clear associations between beta-blocker therapy and improved outcomes.
Beta-blocker therapy was not significantly associated with cardiovascular benefits in stable CAD patients with preserved left ventricular function. These findings provide additional contemporary evidence supporting current guideline recommendations from both American Heart Association (AHA)/American College of Cardiology (ACC) and European Society of Cardiology (ESC) regarding beta-blocker use in this population. Clinicians should conduct individualized risk-benefit assessments rather than adopting routine prescribing patterns.
CRD420251141812, https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=1141812.
Keywords
- beta-blockers
- stable coronary artery disease
- meta-analysis
- cardiovascular outcomes
- preserved left ventricular function
Coronary artery disease (CAD) remains the leading cause of cardiovascular mortality worldwide, affecting millions of patients and significantly impacting their quality of life and prognosis [1]. Stable CAD, characterized by coronary artery stenosis resulting in myocardial ischemia while maintaining relatively stable clinical presentation without acute coronary syndrome manifestations, remains a significant clinical challenge [1, 2]. Despite remarkable progress in revascularization strategies and pharmacological interventions, patients with stable CAD continue to experience considerable risks of major adverse cardiovascular events (MACE), encompassing myocardial infarction (MI), stroke, and cardiovascular mortality [3]. Therefore, identifying effective pharmacological intervention strategies to improve long-term outcomes in this patient population holds substantial clinical significance.
Beta-blockers, as one of the cornerstones of cardiovascular pharmacotherapy,
exert cardioprotective effects through blockade of
The most comprehensive evaluation to date was a 2021 meta-analysis by Arero et al. [8], which pooled six observational studies (n = 774,089) and found no significant reduction in MACE MI, or cardiovascular mortality with beta-blocker therapy. These results questioned the widespread use of beta-blockers in stable CAD and underscored a critical gap between clinical practice and evidence-based recommendations. However, in 2023, Godoy et al. [9] published a large population-based cohort study in the Journal of the American College of Cardiology that challenged these findings. Using a rigorous new-user design in 28,039 patients with angiographically confirmed stable CAD, they demonstrated an 8% relative risk reduction in the composite of all-cause death and hospitalization for heart failure (HF) or MI (HR 0.92, 95% CI: 0.86–0.98, p = 0.006). This contradiction in recent evidence highlighted the ongoing uncertainty regarding beta-blocker efficacy in this population. Therefore, this systematic review and meta-analysis aims to update and expand upon the existing evidence by integrating all available studies to clarify the role of beta-blockers in stable CAD and guide contemporary therapeutic decision-making.
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines. https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=1141812 (or equivalent view link for CRD420251141812).
We conducted a systematic literature search of PubMed, EMBASE, Web of Science, Scopus, Google Scholar, and Cochrane Controlled Trials Register from database inception to May 24, 2025, to identify studies evaluating the effects of beta-blockers on cardiovascular outcomes in patients with stable CAD. Search terms included “beta-blockers”, “beta blockers”, “beta antagonists”, “adrenergic beta-antagonists”, “stable coronary artery disease”, “stable CAD”, “ischemic heart disease”, “major adverse cardiovascular events”, “MACE”, “cardiovascular death”, “myocardial infarction”, and “stroke”.
For the purpose of this meta-analysis, stable CAD was defined as coronary artery
stenosis without acute coronary syndrome manifestations for a sufficient period
to ensure clinical stability. This included patients with significant coronary
stenosis without prior MI, patients stabilized after elective Percutaneous
Coronary Intervention (PCI) or CABG (generally
The inclusion criteria were as follows: (1) studies involving patients with stable CAD or stable ischemic heart disease as defined above; (2) comparison of beta-blocker therapy versus control (placebo or no beta-blocker treatment); (3) reporting of at least one cardiovascular outcome of interest (all-cause death, cardiac death, HF, MI, or stroke); (4) Follow-up duration of at least 12 months. The exclusion criteria were as follows: (1) studies focusing on patients with AMI or left ventricular dysfunction; (2) animal studies; (3) case reports, editorials, comments, reviews, and meta-analyses; (4) studies published in languages other than English; (5) conference abstracts without full-text availability; (6) studies with insufficient data for analysis. The primary outcome was cardiac death. Secondary outcomes included all-cause death, HF, MI, and stroke.
Two investigators independently screened all retrieved records by title and abstract, followed by full-text review of potentially eligible studies. Disagreements were resolved through discussion with a third reviewer.
Data extraction was performed independently by two reviewers using a standardized data extraction form. The following information was extracted: study characteristics (first author, publication year, study design, location, sample size, follow-up duration), patient demographics (age, sex, body mass index, diabetes, hypertension, hypercholesterolemia, stroke history, smoking status), procedural characteristics (percutaneous coronary intervention, coronary artery bypass grafting), concomitant medications (statins, aspirin, angiotensin converting enzyme (ACE) inhibitors/angiotensin receptor blockers, calcium channel blockers), confounding control methods (propensity score matching or multivariate adjustment), and outcome data (risk ratios or hazard ratios with 95% confidence intervals for each cardiovascular outcome).
The methodological quality and risk of bias of included studies were assessed using the Risk Of Bias In Non-randomized Studies - of Interventions (ROBINS-I) tool.
All analyses were performed using R statistical software (version 4.3.0, R Foundation for Statistical Computing, Vienna, Austria) with the meta package and RevMan (version 5.4). HR with 95%
confidence intervals (CI) were calculated for all outcomes. Statistical
heterogeneity between studies was assessed using the I2 statistic and
Cochran’s Q test. According to Higgins et al. [10], I2 values of
Random-effects models (using the DerSimonian-Laird method with REML tau2
estimation) were applied for all analyses. Additionally, due to the relatively
small number of included studies (
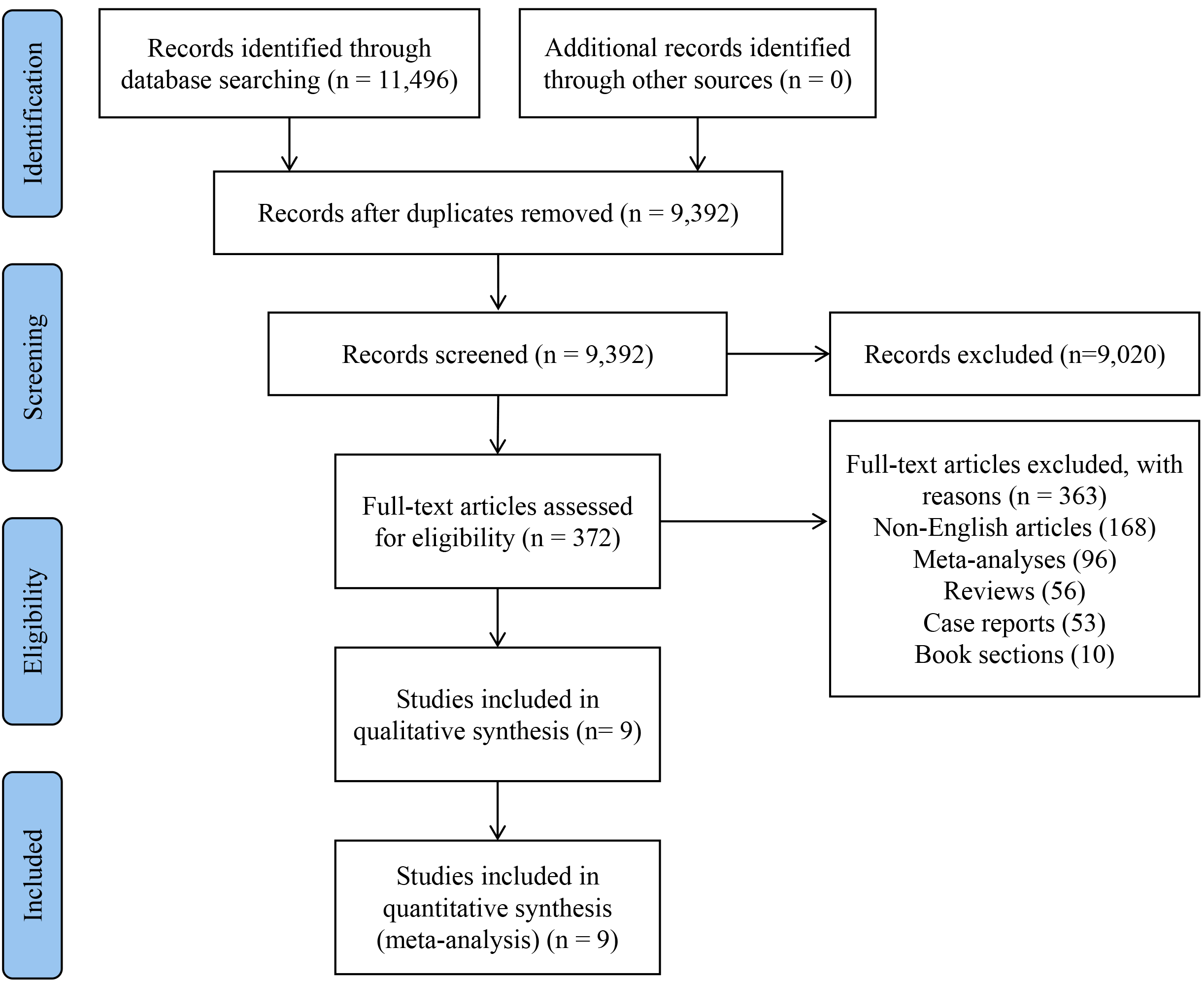
We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart to describe the screening and selection of articles (Fig. 1). After a comprehensive search, we identified 11,496 potentially relevant articles from database searching. After removing 2104 duplicates, 9392 records were screened by title and abstract, and 372 studies were selected for full-text review. After applying the inclusion and exclusion criteria, 9 studies published between 2005 and 2025 were finally analyzed [9, 10, 11, 12, 13, 14, 15, 16, 17].
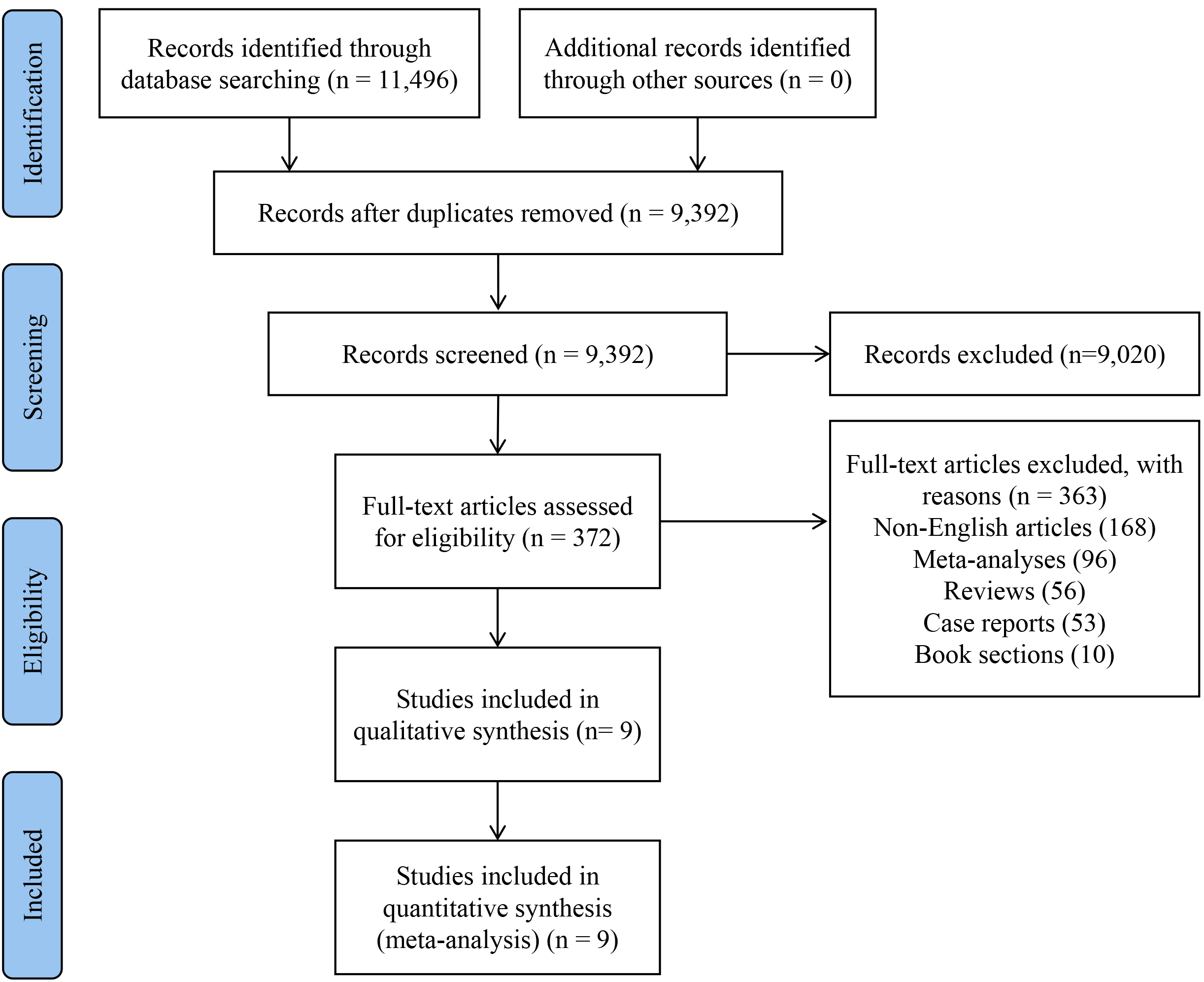 Fig. 1.
Fig. 1.
Flow diagram of meta-analysis.
The 9 studies comprised 903,870 patients with stable CAD, of whom 616,645 patients received beta-blocker therapy and 287,225 patients served as controls. The baseline characteristics of the included studies are presented in Table 1 (Ref. [9, 11, 12, 13, 14, 15, 16, 17, 18]), and the baseline characteristics of the patients are shown in Table 2 (Ref. [9, 11, 12, 13, 14, 15, 16, 17]). The studies were conducted across various locations including the United States, international multi-center settings, Taiwan, Japan, South Korea, and Canada. Six studies were retrospective in design, while 3 were prospective. The median follow-up duration ranged from 3 to 5.4 years. Propensity score matching was employed in 6 studies, while 3 studies used multivariate adjustment to control for confounding factors. Only 2 studies explicitly excluded patients with prior beta-blocker use, while the remaining 7 studies did not specify or exclude patients with previous beta-blocker exposure.
| Studies | Location | Study periods | Control for confounding | Timing of the study | Follow-up periods, median (year) | Without prior BB use | Total cohort | BB | no BB | Primary outcomes | Secondary outcomes |
| Bunch et al., 2005 [12] | Single center, USA | 1993−2002 | Multivariate | Prospective | 3 | No | 4304 | 1024 | 3280 | All-cause death | All-cause death, MI |
| Bangalore et al., 2012 [11] | Multi centers, International | 2003–2009 | PS matched | Prospective | 3.6 | No | 7198 | 3599 | 3599 | Cardiac death, nonfatal MI, or nonfatal stroke | Cardiac death, nonfatal MI, nonfatal stroke, hospitalization for atherothrombotic events, and revascularization |
| Li et al., 2013 [13] | Single center, Taiwan | 1997–2003 | Multivariate | Prospective | 5.4 | No | 607 | 243 | 364 | All-cause death, cardiac death, non-cardiac death | - |
| Ozasa et al., 2013 [15] | Multi centers, Japan | 2005–2007 | PS matched | Prospective | 3 | No | 5288 | 1117 | 4171 | Cardiac death, MI | All-cause death, cardiac death, MI, revascularization |
| Motivala et al., 2016 [14] | Multi centers, USA | 2005–2013 | Multivariate | Retrospective | 3 | No | 755,215 | 539,521 | 215,694 | All-cause death | Revascularization, hospitalization for MI, HF, or stroke |
| Tsujimoto et al., 2017 [16] | Multi centers, International | 2001–2005 | PS matched | Retrospective | 5 | No | 1477 | 1019 | 458 | All-cause death | All-cause death, MI or stroke |
| Lee et al., 2022 [17] | Multi centers, South Korea | 2005–2015 | PS matched | Retrospective | 5 | No | 78,380 | 45,746 | 32,634 | MACE: composite of cardiac death, MI, HF, and hospitalization for 5 years after PCI with 6 months quarantine | All-cause death and the individual MACE components |
| Godoy et al., 2023 [9] | Single center, Canada | 2009–2019 | PS matched | Retrospective | 5.2 | Yes | 28,039 | 12,695 | 15,344 | All-cause death and hospitalization for HF or MI | All-cause death and hospitalization for HF or MI, cardiac death, revascularization, hospitalization for stroke or unstable angina |
| Khan et al., 2025 [18] | Multi centers, USA | 2009–2024 | PS matched | Retrospective | 5 | Yes | 23,362 | 11,681 | 11,681 | All-cause death | Hospitalization for MI, stroke, HF, and AF |
Abbreviation: BB, Beta-blocker; PS, production sequence; MI, myocardial infarction; HF, heart failure; MACE, major adverse cardiovascular events; AF, atrial fibrillation; PCI, Percutaneous Coronary Intervention.
| Studies | Total cohort | Age (years), mean | Men, (%) | BMI (kg/m2), mean | Diabetes, (%) | Hypertension, (%) | Hypercholesterolaemia, (%) | Stroke, (%) | Smoking, (%) | PCI, (%) | CABG (%) | Statins, (%) | Aspirin, (%) | ACEi/ARB, (%) | CCB, (%) |
| Bunch et al., 2005 [12] | 4304 | 65 | 75 | - | 16 | 60 | 55 | - | 23 | 30 | 20 | 18 | - | 43 | - |
| Bangalore et al., 2012 [11] | 7198 | 69 | 66 | 28 | 39 | 81 | 73 | 12 | 9 | - | - | 71 | 74 | 44 | 42 |
| Li et al., 2013 [13] | 607 | 67 | 70 | 26 | 34 | 75 | - | 8 | 27 | 56 | 23 | 19 | - | 38 | 54 |
| Ozasa et al., 2013 [15] | 5288 | 68 | 72 | 24 | 37 | 83 | - | 10 | 25 | - | - | 52 | 99 | 46 | 56 |
| Motivala et al., 2016 [14] | 755,215 | 65 | 64 | 30 | 35 | 82 | - | - | 19 | 30 | - | - | - | - | - |
| Tsujimoto et al., 2017 [16] | 1477 | 62 | 69 | - | 100 | 83 | 81 | - | 11 | - | - | 72 | 87 | - | - |
| Lee et al., 2022 [17] | 78,380 | 64 | 65 | - | 34 | 78 | - | - | - | - | - | - | 57 | 58 | - |
| Godoy et al., 2023 [9] | 28,039 | 73 | 66 | - | 35 | 77 | - | - | 10 | - | - | 87 | - | 74 | - |
Abbreviation: BB, Beta-blocker; BMI, Body Mass Index; PCI, Percutaneous Coronary Intervention; CABG, Coronary Artery Bypass Grafting; ACEi/ARB, Angiotensin-Converting Enzyme inhibitor/Angiotensin Receptor Blocker; CCB, Calcium Channel Blocker.
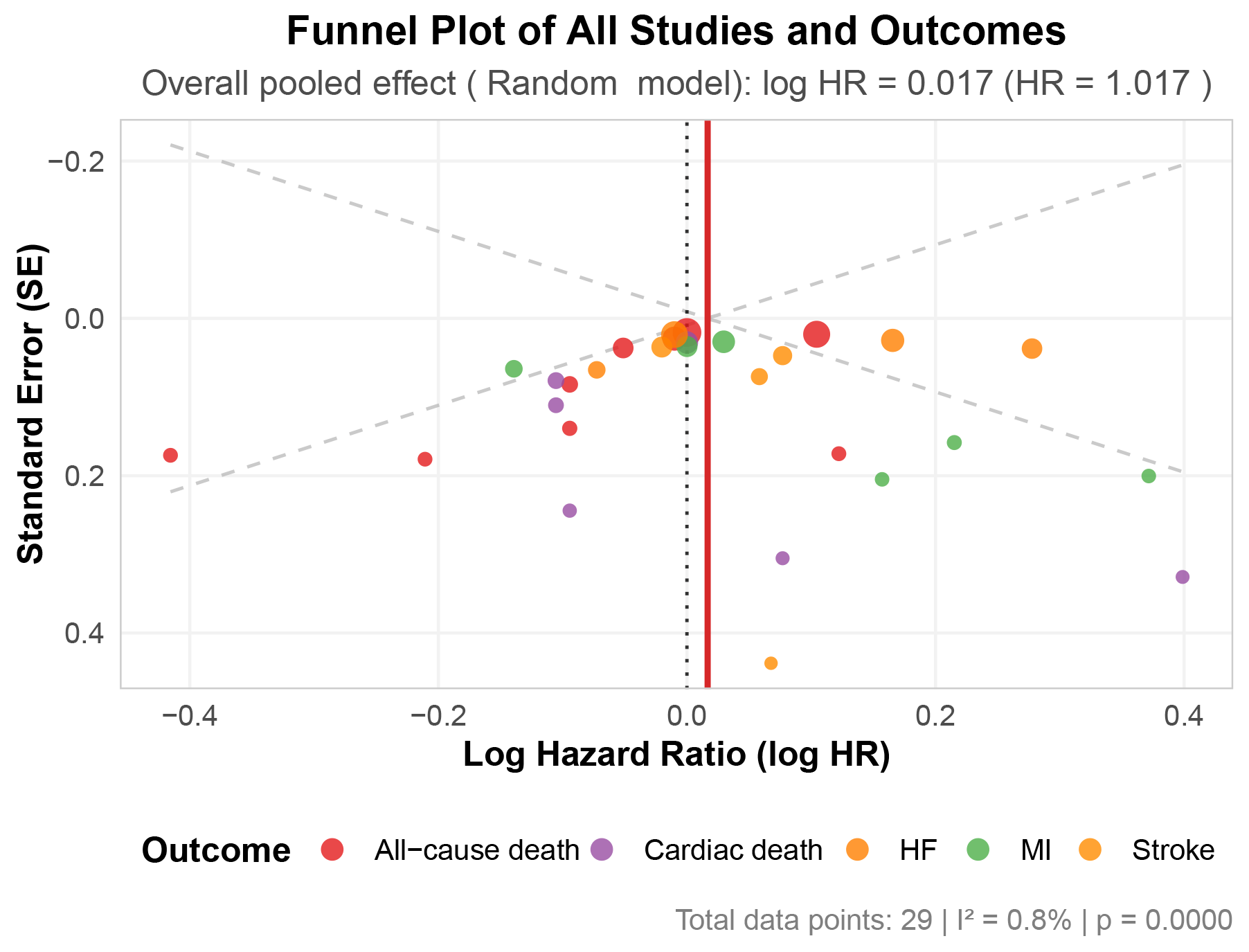
Publication bias was assessed using funnel plots and Egger’s regression test
(Fig. 2). The funnel plot, which included 37 data points representing all
cardiovascular outcomes across the included studies, appeared relatively
symmetric around the overall pooled effect estimate (HR = 1.022; 95% CI:
0.982–1.062). Egger’s test showed no evidence of significant publication bias
(p = 0.975). The overall heterogeneity across all outcomes was minimal
(I2 = 0.8%, p
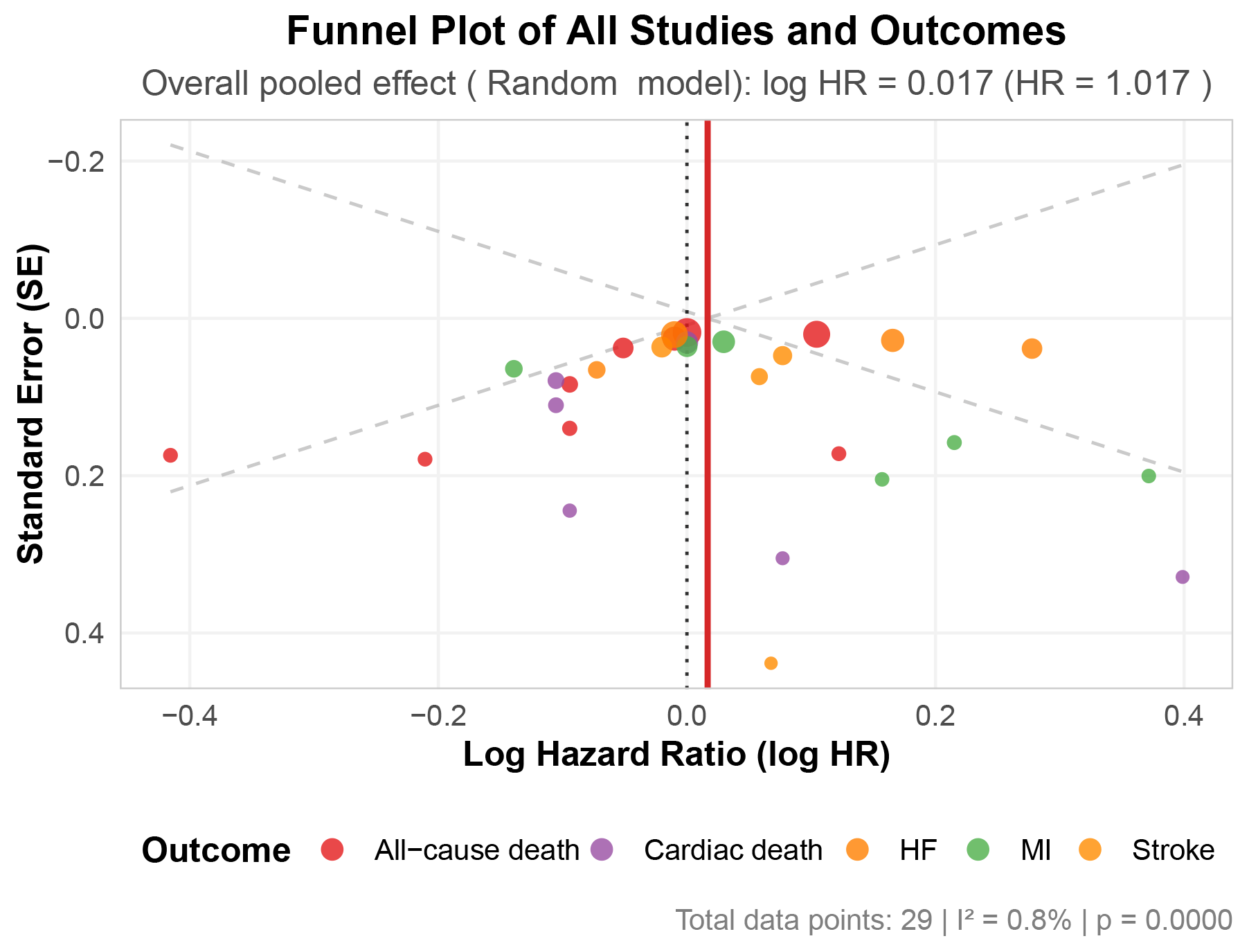 Fig. 2.
Fig. 2.
Funnel plot. Abbreviation: HF, heart failure; MI, myocardial infarction.
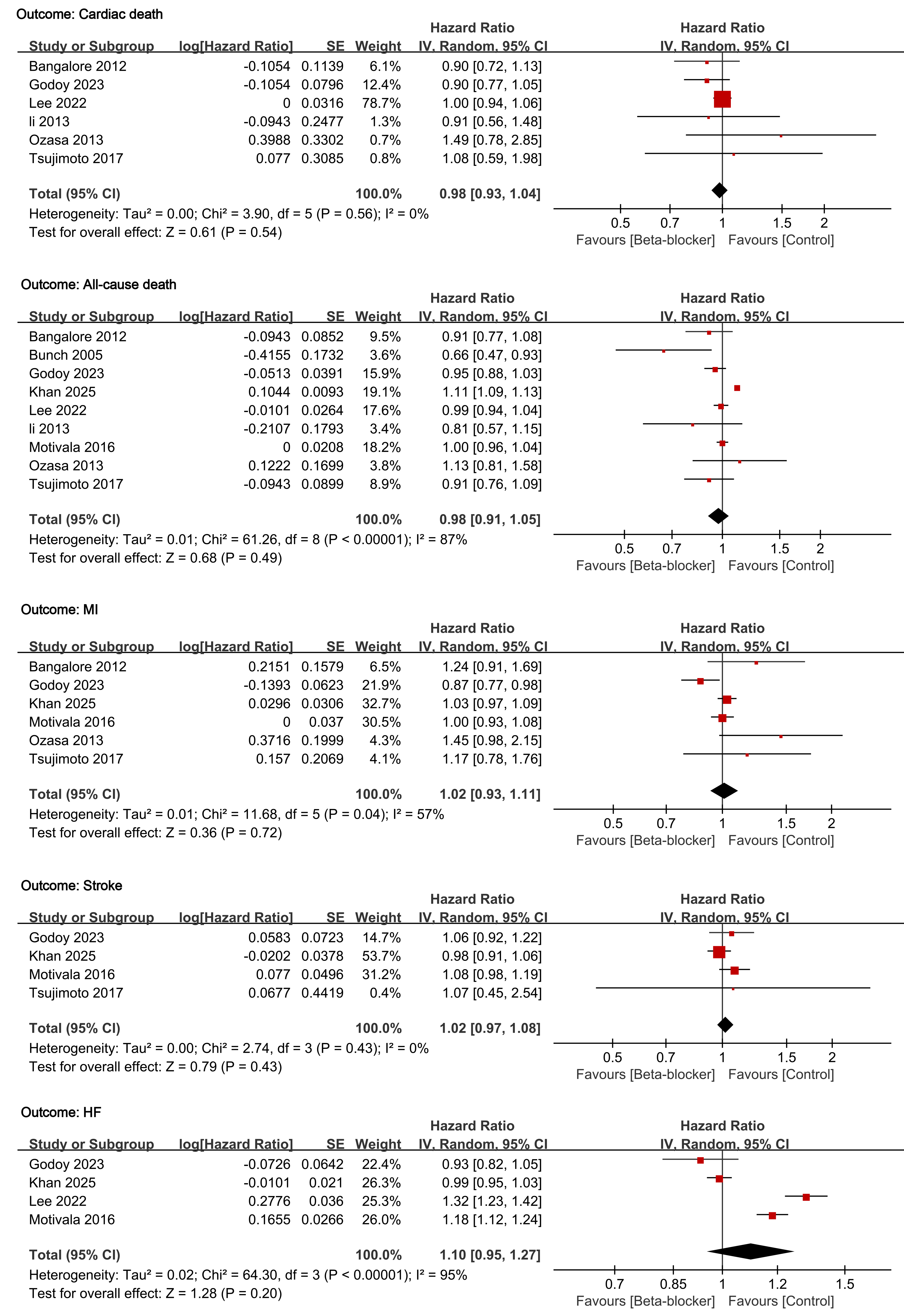
The cardiovascular effects of beta-blocker therapy across five outcomes are presented in Fig. 3. Beta-blocker treatment demonstrated no significant benefit for the primary endpoint of cardiac death (HR 0.98; 95% CI: 0.93–1.04; p = 0.54). Secondary outcomes similarly demonstrated no significant effects: all-cause death (HR 0.98; 95% CI: 0.91–1.05; p = 0.49), MI (HR 1.02; 95% CI: 0.93–1.11; p = 0.72), stroke (HR 1.02; 95% CI: 0.97–1.08; p = 0.43), and HF (HR 1.10; 95% CI: 0.95–1.27; p = 0.20). All confidence intervals crossed unity, indicating no statistically significant effects. Heterogeneity analysis revealed substantial variation across outcomes. High heterogeneity was observed for all-cause death (I2 = 87%) and HF (I2 = 95%), while moderate heterogeneity was present for MI (I2 = 57%). Conversely, cardiac death and stroke demonstrated no heterogeneity (I2 = 0% for both).
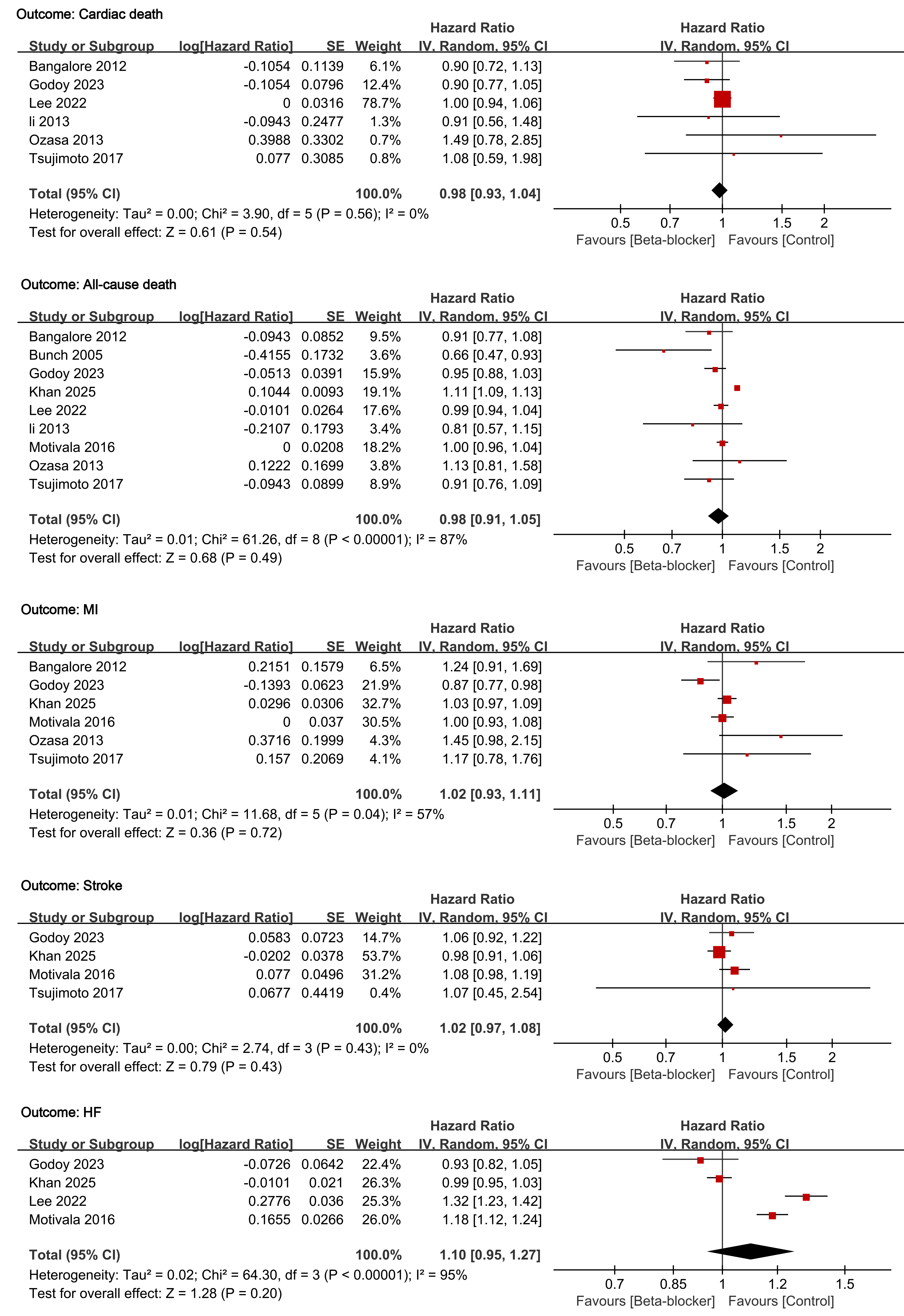 Fig. 3.
Fig. 3.
Forest plots of the effects of beta-blockers on cardiovascular outcomes in patients with stable ischemic heart disease.
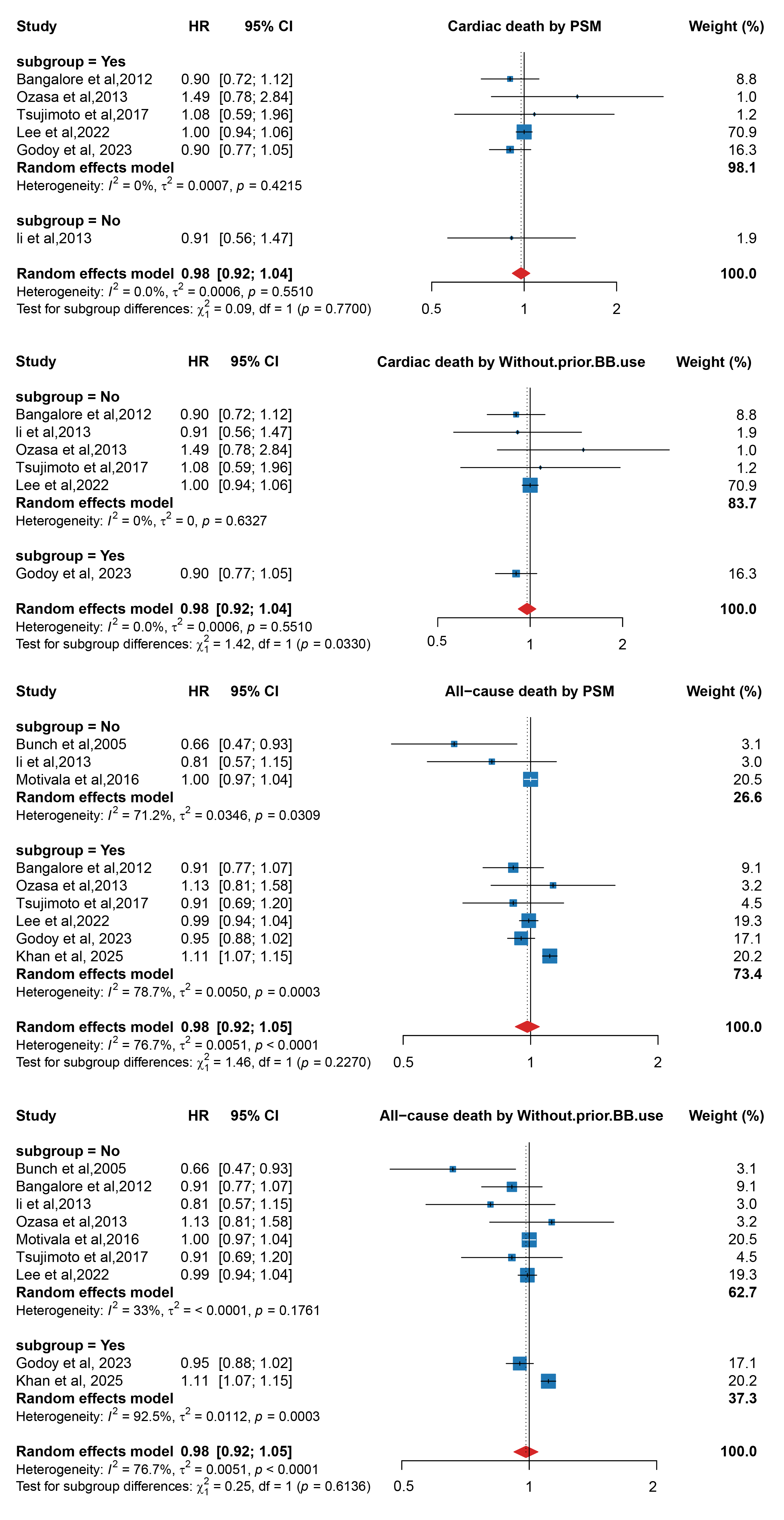
To explore potential sources of heterogeneity and identify patient populations who might derive differential benefits from beta-blocker therapy, we conducted subgroup analyses according to two predefined variables: propensity score matching status and explicit exclusion of patients with prior beta-blocker use (Fig. 4). For cardiac death, when stratified by propensity score matching status, no significant differences were observed between subgroups (p = 0.77). Studies employing propensity score matching showed neutral effects (HR = 0.98, 95% CI: 0.92–1.04), while studies using multivariate adjustment demonstrated similar neutral effects (HR = 0.91, 95% CI: 0.56–1.47). When stratified by prior beta-blocker use exclusion criteria, a statistically significant subgroup difference was detected (p = 0.03). Studies that did not explicitly exclude patients with prior beta-blocker use showed neutral effects (HR = 1.00, 95% CI: 0.94–1.06), whereas the single study that explicitly excluded prior users demonstrated a trend toward benefit, although not statistically significant (HR = 0.90, 95% CI: 0.77–1.05). For all-cause death, when stratified by propensity score matching status, no significant differences were observed between subgroups (p = 0.23). Studies without propensity score matching demonstrated a slight protective trend (HR = 0.85, 95% CI: 0.71–1.02), while studies with propensity score matching showed neutral effects (HR = 1.00, 95% CI: 0.94–1.07). When stratified by prior beta-blocker use exclusion criteria, no significant subgroup difference was found (p = 0.61). Studies that did not explicitly exclude patients with prior beta-blocker use showed neutral effects (HR = 0.99, 95% CI: 0.94–1.04), while studies that explicitly excluded prior users showed similar neutral effects (HR = 0.98, 95% CI: 0.91–1.05). Overall, subgroup analyses failed to identify specific patient populations that would clearly benefit from beta-blocker therapy.
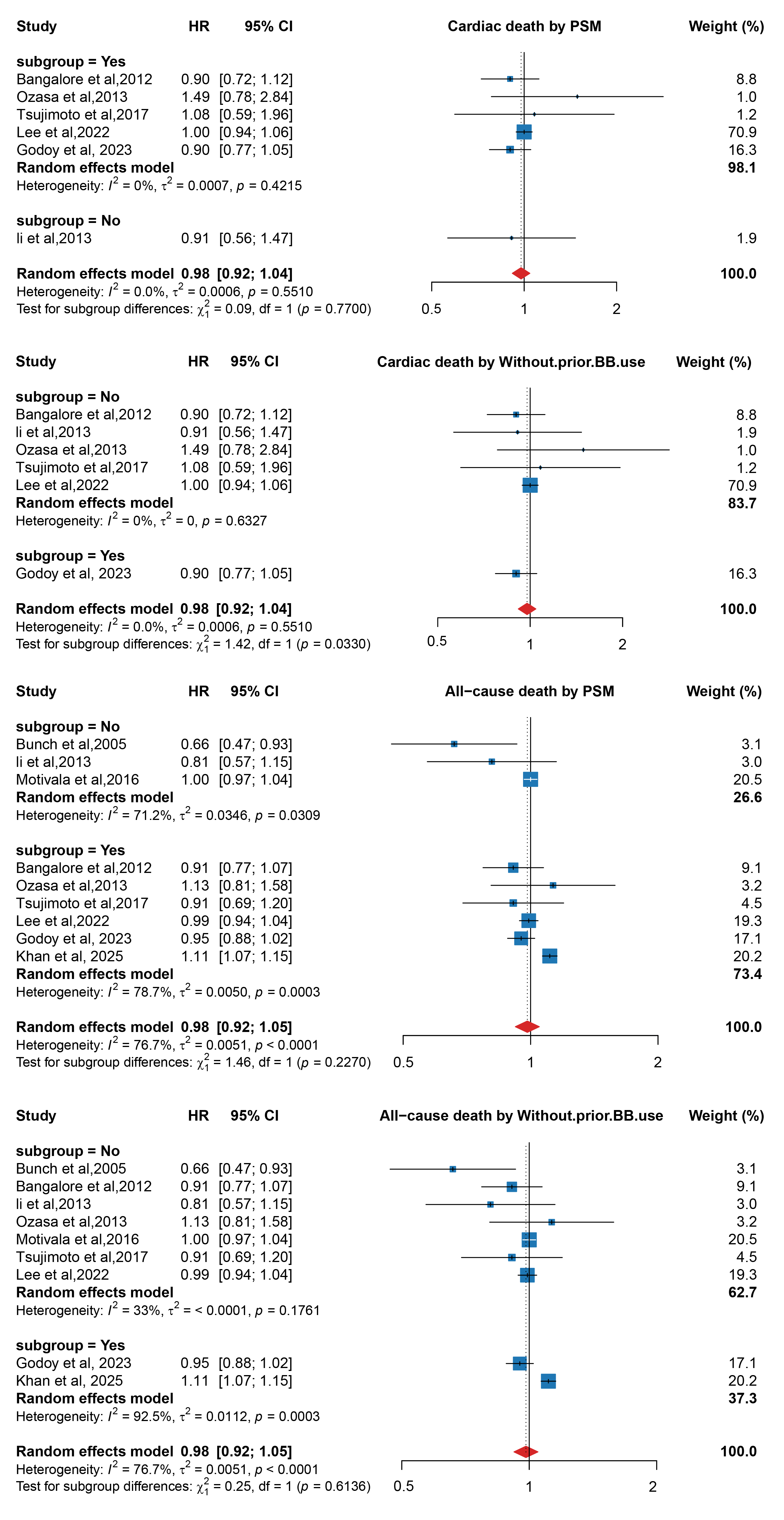 Fig. 4.
Fig. 4.
Subgroup analyses of beta-blockers effects on all-cause death and MACE stratified by PSM status and prior beta-blocker use. Abbreviation: BB, Beta-blocker; MACE, major adverse cardiovascular events; PSM, propensity score matching.
This systematic review and meta-analysis demonstrates that beta-blocker therapy was not significantly associated with cardiovascular endpoints in patients with stable CAD and preserved left ventricular function. These findings contribute to an evolving and contradictory body of evidence regarding beta-blocker efficacy in this population.
Current clinical practice guidelines have increasingly questioned the routine
use of beta-blockers in stable CAD patients without prior MI or left ventricular
dysfunction. The most recent 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the
Management of Patients with Chronic Coronary Disease made significant changes to
beta-blocker recommendations, stating that “long-term beta-blocker therapy is
not recommended to improve outcomes in patients with chronic coronary disease in
the absence of MI in the past year, left ventricular ejection fraction
Our comprehensive meta-analysis, incorporating all available evidence including
the Godoy study, found no significant benefit for cardiac death (HR 0.98, 95%
CI: 0.93–1.04, p = 0.539), suggesting that the overall evidence remains
insufficient to support routine beta-blocker use in stable CAD patients. Although
our subgroup analyses did not identify specific patient populations that
consistently benefit from beta-blocker therapy, examining potential explanatory
factors for the divergent results between studies may generate important
hypotheses for future research. The divergent results from the Godoy study may
stem from several key factors: First, their new-user design with a 1-year washout
period specifically included only beta-blocker-naïve patients, designed to
eliminate confounding from prior exposure and capture the true effects of
beta-blocker initiation. However, our subgroup analysis of studies that
explicitly excluded patients with prior beta-blocker use still failed to
demonstrate significant benefits for cardiac death (p = 0.2330),
suggesting that even in treatment-naïve populations, beta-blocker efficacy
remains uncertain. Second, strict patient selection criteria created a unique
study population—patients
Our meta-analysis revealed substantial heterogeneity, particularly for all-cause death (I2 = 87%) and HF (I2 = 95%). Beyond the factors discussed in our subgroup analyses and exploration of the Godoy study, several additional elements likely contributed to this variability. Geographic diversity across studies (spanning North America, East Asia, and international settings) introduced differences in healthcare systems and practice patterns. The specific beta-blockers used varied from predominantly cardioselective agents in some studies to more diverse pharmacological profiles in others. Background therapy levels also differed markedly, with variations in contemporary evidence-based therapies potentially creating different contexts for beta-blocker efficacy. Methodological differences in follow-up durations and approaches to confounding control further contributed to the observed heterogeneity. These multiple sources of clinical and methodological variability may help explain the absence of significant associations between beta-blocker therapy and cardiovascular outcomes in our analysis.
Despite our overall null findings, it would be premature to conclude that beta-blockers provide no benefit in stable CAD patients. The divergent results between studies, particularly the positive findings in Godoy’s carefully selected elderly population with high-risk anatomical features, suggest that patient heterogeneity may be the key factor determining treatment response. Rather than reflecting true inefficacy, our results may highlight the limitations of current research methodologies in identifying the optimal candidates for beta-blocker therapy. The challenge lies in developing robust clinical criteria to identify patients who would truly benefit from therapy. Future research should focus on establishing individualized treatment algorithms rather than pursuing blanket recommendations, with careful consideration of individual patient characteristics, comorbidities, and risk profiles.
This study has several important limitations to consider. First, all included studies were observational, and despite employing advanced confounding control methods, residual and unmeasured confounding cannot be completely excluded. Second, significant methodological heterogeneity existed between studies, including differences in exposure definitions, follow-up times, endpoint definitions, and statistical methods, potentially affecting result comparability. Third, we could not obtain individual patient data for more refined subgroup analyses, limiting precise identification of benefiting populations. Fourth, the relatively small number of included studies (n = 9) limits the robustness of publication bias assessment using funnel plots, although we supplemented this with Peter’s test to strengthen our evaluation. Fifth, most studies came from developed countries’ healthcare systems, potentially limiting global applicability to developing countries or different healthcare resource settings. Finally, rapid evolution of medical practice during observation periods, particularly introduction of novel antiplatelet agents and proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, may have affected assessment of beta-blockers’ relative therapeutic value.
In conclusion, we conducted a meta-analysis of 9 observational studies investigating the effects of beta-blocker therapy on cardiovascular endpoints in stable CAD patients. Our meta-analysis showed no significant association between beta-blockers and reduced cardiac death incidence in stable CAD patients. These findings provide additional contemporary evidence supporting current guideline recommendations from both AHA/ACC (Class III: No Benefit) and ESC regarding beta-blocker use in this population. Although Godoy et al.’s [9] study showed positive signals in specific subgroups, overall evidence suggests that routine use of beta-blockers in this population may require careful reconsideration. Clinicians should conduct risk-benefit assessments based on individual patient characteristics rather than adopting “one-size-fits-all” prescribing patterns. To clarify beta-blocker indications in this patient subset and identify truly benefiting populations, rigorously designed randomized controlled trials are needed to improve evidence quality, particularly prospective studies targeting elderly patients with high-risk anatomical features.
In this meta-analysis of contemporary studies, beta-blocker therapy did not significantly reduce the incidence of cardiovascular events in stable CAD patients with preserved left ventricular function without other indications for beta-blockers. These findings provide additional contemporary evidence supporting current guideline recommendations from both AHA/ACC and ESC regarding beta-blocker use in this population. Clinicians should conduct individualized risk-benefit assessments rather than adopting routine prescribing patterns.
The data used to support the results of this study are available from the corresponding author upon request.
JXL, SYZ, and FG designed and performed the research study. CHH, JL, HF, XD, and JZD provided design and advice. JX L analyzed the data and drafted the manuscript. All authors contributed to the critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/RCM44520.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.