



 , Seok Jin Ryu 1,2,†, Byung Kook Lee 1,2,*
, Seok Jin Ryu 1,2,†, Byung Kook Lee 1,2,* , Yong Hun Jung 1,2, Kyung Woon Jeung 1,2, Hyo Jin Bang 3, Hyo Jeong Kwon 4, Joo Suk Oh 5, In Soo Cho 6
, Yong Hun Jung 1,2, Kyung Woon Jeung 1,2, Hyo Jin Bang 3, Hyo Jeong Kwon 4, Joo Suk Oh 5, In Soo Cho 61 Department of Emergency Medicine, Chonnam National University Medical School, 61469 Gwangju, Republic of Korea
2 Department of Emergency Medicine, Chonnam National University Hospital, 61469 Gwangju, Republic of Korea
3 Department of Emergency Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, 06591 Seoul, Republic of Korea
4 Department of Emergency Medicine, Asan Medical Center, University of Ulsan College of Medicine, 05505 Seoul, Republic of Korea
5 Department of Emergency Medicine, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, 06591 Seoul, Republic of Korea
6 Department of Emergency Medicine, KEPCO Medical Center, 01450 Seoul, Republic of Korea
†These authors contributed equally.
Abstract
The association between elevated perfusion pressure and neurological outcomes in out-of-hospital cardiac arrest (OHCA) survivors remains unclear. Specifically, to our knowledge, no studies have currently investigated whether the duration of elevated perfusion pressure influences neurological prognosis following OHCA. Thus, this study aimed to examine the association between the duration of a mean arterial pressure (MAP) >80 mmHg during the first 48 hours after return of spontaneous circulation (ROSC) and neurological outcomes in OHCA survivors.
This observational study included adult patients (≥18 years) with OHCA treated between January 2019 and May 2021. The cumulative duration of a MAP >80 mmHg was recorded during the 0–24, 25–48, and 0–48 hour intervals following ROSC. The primary outcome was the neurological status at 6 months, with good outcomes defined as Cerebral Performance Category (CPC) scores of 1 or 2.
Among the 468 patients with OHCA, 132 (28.2%) achieved good neurological outcomes. The duration of a MAP >80 mmHg over 0–48 hours was significantly longer in the good outcome group compared with the poor outcome group (35 (26–42) vs. 28 (16–39) hours; p < 0.001). In the multivariable analysis after adjusting for confounders, longer durations of a MAP >80 mmHg at 0–48 hours (odds ratio (OR): 1.047, 95% confidence interval (CI): 1.021–1.073) and 25–48 hours (OR: 1.086, 95% CI: 1.042–1.131), but not at 0–24 hours, were associated with good neurological outcomes at 6 months.
The duration of a MAP >80 mmHg during the 0–48 and 25–48 hour periods after ROSC was associated with good neurological outcomes at six months in OHCA survivors.
Keywords
- cardiac arrest
- neurological outcomes
- mean arterial pressure
- targeted temperature management
Even after the return of spontaneous circulation (ROSC) in patients with out-of-hospital cardiac arrest (OHCA), comprehensive post-cardiac arrest care is critical to mitigating ongoing ischemia–reperfusion injury [1, 2, 3]. Maintaining arterial pressure (AP) above a certain threshold is essential to ensure adequate organ and tissue perfusion. In the post-ROSC phase, mean AP (MAP) plays a key role in supporting cerebral perfusion and has been associated with overall patient prognosis [4, 5]. Adequate MAP is crucial for preserving oxygen delivery to the brain and other vital organs, minimizing secondary ischemic damage, and facilitating neurological recovery.
To ensure sufficient tissue perfusion, preserve renal function (urine output),
and stabilize metabolic processes (e.g., lactate clearance), current
international guidelines recommend maintaining MAP at
The present study quantified the duration of MAP
The Korean Hypothermia Network (KORHN) established a prospective, multicenter
registry of comatose adult (
A retrospective analysis was conducted using data from the KORHN-PRO registry. Eligible participants were comatose adult OHCA patients who received TTM. Patients were excluded if they lacked data on Sequential Organ Failure Assessment (SOFA) scores, rCAST scores, blood pressure recordings for more than six hours within the first 48 hours post-ROSC, or 6-month neurological outcomes.
All enrolled comatose OHCA survivors received TTM. A feedback-controlled cooling
system was employed to maintain a target temperature of 33–36 °C for 24
hours. To prevent shivering and provide sedation, patients received propofol,
midazolam, or remifentanil for analgosedation. Following the maintenance phase,
rewarming was initiated at a controlled rate of 0.25 °C per hour. All
other aspects of post-arrest care were managed according to institutional
protocols, consistent with international guidelines [14]. Systolic and diastolic
blood pressures were measured via invasive arterial catheters, with continuous
arterial pressure monitoring. MAP was calculated, and vasopressors and fluids
were administered to maintain MAP
The following data were extracted from the registry: age, sex, body mass index, preexisting comorbidities, witnessed arrest status, presence of bystander cardiopulmonary resuscitation, initial cardiac rhythm, cardiac arrest etiology, time from collapse to ROSC, SOFA score within 24 hours post-ROSC [15], arterial pH, Glasgow Coma Scale motor response score, serum lactate concentration after ROSC, systolic and diastolic blood pressure (measured hourly post-ROSC), and 6-month outcomes based on the Cerebral Performance Category (CPC) scale.
The duration for which MAP exceeded 80 mmHg during the first 48 hours after ROSC
was calculated and stratified into three intervals: 0–24 hours, 25–48 hours,
and 0–48 hours. The rCAST score was computed based on previously described
clinical variables [11, 12], and patients were classified into low (
Neurological outcomes were assessed at 6 months post-arrest using the CPC scale, via structured telephone interviews with the patient, or when this was not feasible, with a caregiver or legal proxy. CPC outcomes were categorized as follows: CPC 1 (good performance), CPC 2 (moderate disability), CPC 3 (severe disability), CPC 4 (vegetative state), and CPC 5 (brain death or death) [16].
Categorical variables are presented as frequencies with corresponding percentages, and comparisons between neurological outcome groups were performed using the chi-square test or Fisher’s exact test, as appropriate. Continuous variables are reported as medians with interquartile ranges (IQRs). Given that all continuous variables were non-normally distributed, the Mann–Whitney U test was applied for comparisons between groups.
To explore the association between the duration of MAP
Of the 617 OHCA survivors recorded in the registry, patients were excluded if SOFA scores could not be assessed (n = 2), rCAST scores could not be calculated (n = 22), blood pressure recordings were unavailable for more than 6 hours within the first 48 hours after ROSC (n = 119), or 6-month CPC scores were missing (n = 6). Ultimately, 468 patients were included in the final analysis (Fig. 1). Supplementary Table 2 shows the results of comparison of characteristics between the excluded and included patients. There were significant differences in proportion of malignancy between the included and excluded patients (4.7% vs. 10.1%; p = 0.027). There was no significant difference in the time from neurologic outcome between the two groups.
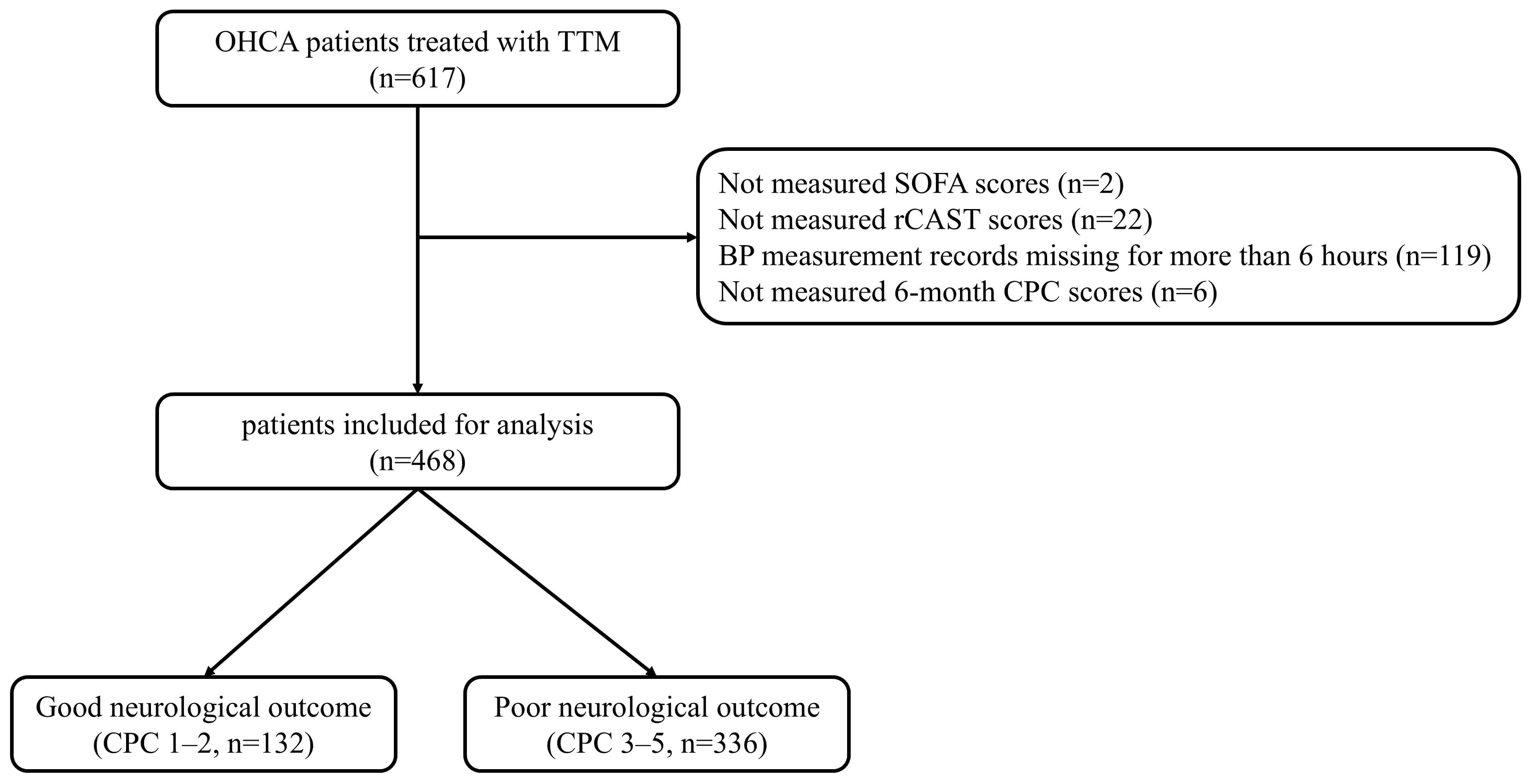 Fig. 1.
Fig. 1.
Flow diagram of patient inclusion. OHCA, out-of-hospital cardiac arrest; TTM, targeted temperature management; SOFA, Sequential Organ Failure Assessment; rCAST, revised post-Cardiac Arrest Syndrome for Therapeutic hypothermia score; CPC, Cerebral Performance Category.
Patients were stratified into good (n = 132, 28.2%) and poor (n = 336, 71.8%)
neurological outcome groups based on CPC scores at 6 months (Table 1). Compared
with those in the poor outcome group, patients in the good outcome group were
younger, more frequently male, and had higher body mass indexes. They also had a
greater prevalence of coronary artery disease and a lower prevalence of diabetes.
Regarding cardiac arrest characteristics, the good outcome group exhibited higher
rates of witnessed arrests and shockable rhythms, as well as shorter times from
collapse to ROSC. Additionally, this group had lower post-ROSC lactate levels,
SOFA scores, and rCAST scores. The duration of MAP
| Variables | Total (n = 468) | Good (n = 132) | Poor (n = 336) | p | |
| Demographics | |||||
| Age (years), median (IQR) | 61.3 (49.3–71.8) | 56.2 (47.6–65.5) | 64.0 (50.1–75.2) | ||
| Male, n (%) | 331 (70.7) | 111 (84.1) | 220 (65.5) | ||
| Body mass index (kg/m2), median (IQR) | 23.5 (21.3–25.6) | 24.2 (22.4–26.3) | 23.1 (20.5–25.2) | ||
| Preexisting illness, n (%) | |||||
| Coronary artery disease | 60 (12.8) | 26 (19.7) | 34 (10.1) | 0.005 | |
| Arrhythmia | 24 (5.1) | 9 (6.8) | 15 (4.5) | 0.420 | |
| Congestive heart failure | 21 (4.5) | 5 (3.8) | 16 (4.8) | 0.834 | |
| Hypertension | 202 (43.2) | 51 (38.6) | 151 (44.9) | 0.256 | |
| Diabetes | 142 (30.3) | 25 (18.9) | 117 (34.8) | ||
| Stroke | 41 (8.8) | 8 (6.1) | 33 (9.8) | 0.266 | |
| Previous pulmonary disease | 38 (8.0) | 5 (3.8) | 33 (9.8) | 0.050 | |
| Previous renal disease | 42 (9.0) | 7 (5.3) | 35 (10.4) | 0.118 | |
| Liver cirrhosis | 8 (1.7) | 1 (0.8) | 7 (2.1) | 0.451 | |
| Malignancy | 22 (4.7) | 6 (4.5) | 16 (4.8) | 0.999 | |
| Cardiac arrest characteristics | |||||
| Witnessed collapse, n (%) | 302 (64.5) | 96 (72.7) | 206 (61.3) | 0.027 | |
| Bystander CPR, n (%) | 321 (68.6) | 97 (73.5) | 224 (66.7) | 0.187 | |
| Shockable rhythm, n (%) | 161 (34.4) | 98 (74.2) | 63 (18.8) | ||
| Cardiac etiology, n (%) | 257 (54.9) | 106 (80.3) | 151 (44.9) | ||
| Time from collapse to ROSC (min), median (IQR) | 29.0 (17.0–46.0) | 17.0 (12.0–27.0) | 35.0 (20.0–50.0) | ||
| Lactate after ROSC (mmol/L), median (IQR) | 9.2 (5.9–12.2) | 6.7 (4.0–9.5) | 10.2 (6.9–12.9) | ||
| SOFA score | 11 (9–13) | 10 (8–12) | 12 (10–13) | ||
| rCAST | 13 (8–16) | 7 (3–10) | 15 (12–16) | ||
| Duration of MAP |
|||||
| During 0–48 h (hour), median (IQR) | 30 (18–40) | 35 (26–42) | 28 (16–39) | ||
| During 0–24 h (hour), median (IQR) | 16 (11–20) | 17 (13–21) | 15 (10–20) | 0.009 | |
| During 25–48 h (hour), median (IQR) | 14 (6–21) | 18 (13–22) | 12 (5–20) | ||
IQR, interquartile range; CPR, cardiopulmonary resuscitation; ROSC, return of spontaneous circulation; SOFA, Sequential Organ Failure Assessment; rCAST, revised post-Cardiac Arrest Syndrome for Therapeutic hypothermia score; MAP, mean arterial pressure.
Fig. 2 shows hourly MAP values during the first 48 hours after ROSC. Patients with good neurological outcomes exhibited consistently higher MAPs throughout the 48-hour period compared with those with poor outcomes. The difference in MAP between the two groups became more pronounced during the 25–48 hour interval after ROSC (Fig. 2).
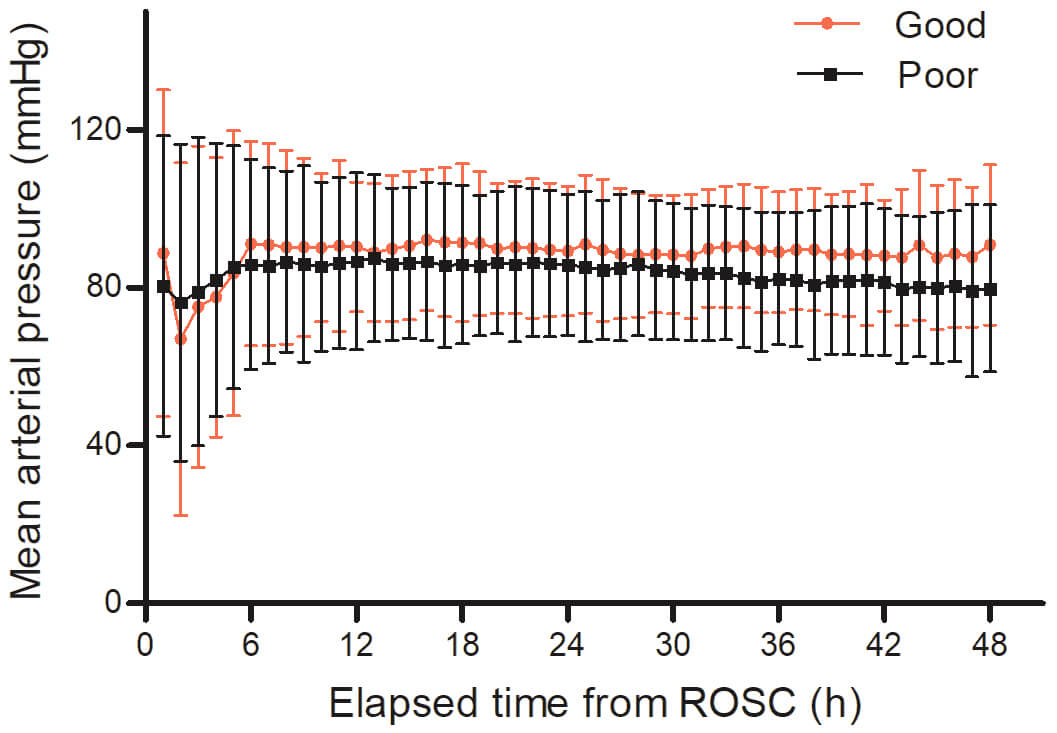 Fig. 2.
Fig. 2.
Hourly MAP within 48 hours after ROSC based on neurological outcomes. MAP, mean arterial pressure; ROSC, return of spontaneous circulation.
Based on rCAST severity, patients were categorized into low (n = 71, 15.2%),
moderate (n = 215, 45.9%), and high (n = 182, 38.9%) severity groups (Table 2).
Statistically significant differences were observed across the three groups with
respect to sex distribution, prevalence of coronary artery disease, witnessed
collapse, bystander cardiopulmonary resuscitation, shockable rhythm, cardiac
etiology, time from collapse to ROSC, lactate levels, SOFA scores, and rCAST
scores. However, no significant differences were found in the duration of MAP
| Variables | Low severity (n = 71) | Moderate severity (n = 215) | High severity (n = 182) | p | |
| Demographics | |||||
| Age (years), median (IQR) | 58.5 (48.8–65.8) | 63.1 (51.3–74.3) | 61.9 (46.9–72.0) | 0.148 | |
| Male, n (%) | 58 (81.7) | 153 (71.2) | 120 (65.9) | 0.046 | |
| Body mass index (kg/m2), median (IQR) | 23.7 (21.6–25.6) | 23.4 (21.3–25.7) | 23.7 (20.6–25.5) | 0.935 | |
| Preexisting illness, n (%) | |||||
| Coronary artery disease | 14 (19.7) | 33 (15.3) | 13 (7.1) | 0.007 | |
| Arrhythmia | 4 (5.6) | 10 (4.7) | 10 (5.5) | 0.882 | |
| Congestive heart failure | 5 (7.0) | 12 (5.6) | 4 (2.2) | 0.127 | |
| Hypertension | 23 (32.4) | 103 (47.9) | 76 (41.8) | 0.064 | |
| Diabetes | 14 (19.7) | 69 (32.1) | 59 (32.4) | 0.102 | |
| Stroke | 5 (7.0) | 23 (10.7) | 13 (7.1) | 0.462 | |
| Previous pulmonary disease | 4 (5.6) | 18 (8.4) | 16 (8.8) | 0.762 | |
| Previous renal disease | 1 (1.8) | 25 (11.6) | 16 (8.8) | 0.019 | |
| Liver cirrhosis | 2 (2.8) | 2 (0.9) | 4 (2.2) | 0.337 | |
| Malignancy | 4 (5.6) | 12 (5.6) | 6 (3.3) | 0.484 | |
| Cardiac arrest characteristics | |||||
| Witnessed collapse, n (%) | 65 (91.5) | 154 (71.6) | 83 (45.6) | ||
| Bystander CPR, n (%) | 51 (71.8) | 167 (77.7) | 103 (58.6) | ||
| Shockable rhythm, n (%) | 57 (80.3) | 80 (37.2) | 24 (13.2) | ||
| Cardiac etiology, n (%) | 58 (81.7) | 132 (61.4) | 67 (36.8) | ||
| Time from collapse to ROSC (min), median (IQR) | 16.0 (12.0–20.0) | 24.0 (15.0–39.0) | 42.0 (30.0–54.3) | ||
| Lactate after ROSC (mmol/L), median (IQR) | 4.6 (3.5–7.9) | 8.0 (5.6–10.4) | 12.1 (9.8–15.0) | ||
| SOFA score | 10 (7–11) | 11 (9–13) | 12 (10–13) | ||
| rCAST | 3 (2–5) | 11 (9–13) | 16 (16–18) | ||
| Duration of MAP |
|||||
| During 0–48 h (hour), median (IQR) | 32 (22–40) | 30 (19–39) | 30 (17–41) | 0.315 | |
| During 0–24 h (hour), median (IQR) | 16 (11–20) | 16 (10–20) | 16 (11–20) | 0.828 | |
| During 25–48 h (hour), median (IQR) | 17 (10–22) | 14 (6–21) | 13 (5–22) | 0.130 | |
| Poor neurologic outcome, n (%) | 14 (19.7) | 148 (68.8) | 174 (95.6) | ||
IQR, interquartile range; CPR, cardiopulmonary resuscitation; ROSC, return of spontaneous circulation; SOFA, Sequential Organ Failure Assessment; rCAST, revised post-Cardiac Arrest Syndrome for Therapeutic hypothermia score; MAP, mean arterial pressure.
In subgroup analyses based on outcome, patients in the low severity group with
good outcomes had a longer MAP
After adjusting for confounders, multivariable logistic regression analysis
revealed that the duration of MAP
| Variables | Adjusted OR (95% CI) a | p | |
| Duration of MAP |
|||
| During 0–48 h, hour | 1.047 (1.021–1.073) | ||
| During 0–24 h, hour | 1.041 (0.989–1.097) | 0.125 | |
| During 25–48 h, hour | 1.086 (1.042–1.131) | ||
Each variable was individually entered into the final model and analyzed separately.
aAdjusted for age, male sex, cardiac etiology, SOFA score, and rCAST score.
MAP, mean arterial pressure; OR, odds ratio; CI, confidence interval; SOFA, Sequential Organ Failure Assessment; rCAST, revised post-Cardiac Arrest Syndrome for Therapeutic hypothermia score.
Table 4 presents stratified multivariable analyses of MAP
| Variables | Low severity (n = 71) | Moderate severity (n = 215) | High severity (n = 182) | ||||
| Adjusted OR (95% CI) a | p | Adjusted OR (95% CI) b | p | Adjusted OR (95% CI) c | p | ||
| Duration of MAP |
|||||||
| During 0–48 h, hour | 1.043 (0.987–1.103) | 0.137 | 1.044 (1.011–1.079) | 0.008 | 1.074 (0.999–1.154) | 0.055 | |
| During 0–24 h, hour | 1.074 (0.959–1.202) | 0.218 | 1.038 (0.976–1.103) | 0.237 | 1.110 (0.953–1.294) | 0.179 | |
| During 25–48 h, hour | 1.075 (0.978–1.182) | 0.132 | 1.094 (1.036–1.154) | 1.103 (0.991–1.227) | 0.072 | ||
a Adjusted by body mass index, presence of stroke, and presence of previous pulmonary disease.
b Adjusted by age, male, diabetes, cardiac etiology, and rCAST score.
c Adjusted by age and presence of coronary artery disease.
MAP, mean arterial pressure; rCAST, revised post-cardiac arrest syndrome for therapeutic hypothermia score; OR, odds ratio; CI, confidence interval.
This study demonstrated that the duration of MAP
Previous research has reported that cerebral autoregulation is often impaired in
patients with post-cardiac arrest, with a rightward shift in the lower limit of
autoregulation. Specifically, patients resuscitated from cardiac arrest exhibited
a significantly higher threshold for maintaining cerebral perfusion (114 mmHg)
compared to healthy controls (76 mmHg) [17]. These findings suggest that a
higher-than-normal MAP may be required to ensure adequate cerebral perfusion in
this population. Additional studies using brain tissue regional oxygen saturation
identified mean optimal MAP thresholds exceeding 76 mmHg [18] and 89 mmHg [19].
Kilgannon et al. [7] further reported a threshold effect, wherein MAP
values above 70 mmHg were associated with favorable neurological outcomes.
Similarly, an observational study identified the MAP range of 76–86 mmHg as
optimal for maximizing survival in cardiac arrest survivors [8], while another
study linked a MAP
In our study, the threshold of MAP
Our findings demonstrate an association between the duration of MAP
Our multivariable analysis revealed strong independent associations between male
sex (OR: 2.427, 95% CI: 1.220–4.827) and cardiac etiology (OR: 2.495, 95% CI:
1.290–4.825) with good neurological outcomes. The association between male sex
and good neurological outcomes reflects multifactorial biological and clinical
mechanisms. Recent meta-analyses encompassing over 1.2 million patients
demonstrate that males present with shockable rhythms more frequently (39.6% vs.
25.7% in females), with meta-regression analysis showing initial shockable
rhythm as a significant predictor of survival outcomes (p
The association between cardiac etiology and good neurological outcomes in our study is consistent with established pathophysiological mechanisms. Unlike non-cardiac causes that involve prolonged hypoxia before arrest, cardiac arrests result from acute coronary occlusion with immediate circulatory cessation, limiting the extent of anoxic brain injury. The therapeutic reversibility of cardiac etiology is crucial—Dumas et al. [31] demonstrated that successful PCI in patients with significant coronary lesions improved survival from 31% to 51%. This finding is supported by nationwide data from Japan showing five-fold better neurological outcomes in cardiac versus non-cardiac origin OHCA (5.0% vs. 1.2%) among 547,153 patients [32]. These mechanisms—electrically reversible rhythms, shorter ischemic time, and treatable coronary pathology—collectively explain why cardiac etiology emerges as a powerful predictor of favorable neurological outcome, supporting aggressive interventional approaches in these patients.
Determining the optimal MAP target for post-cardiac arrest care remains challenging due to the complex interplay of ischemic brain injury, cerebral metabolic demands, and impaired autoregulation. This complexity may explain why recent randomized controlled trials have not demonstrated significant differences in neurological outcomes between patients managed with higher versus lower MAP thresholds [10, 20, 33]. Notably, these trials enrolled only patients with OHCA of presumed cardiac origin and excluded individuals with non-cardiac etiologies, who have worse prognoses [10, 20, 33]. By contrast, our study encompassed a broader patient population, with lower proportions of cardiac etiologies (54.9% vs. 100%) and shockable rhythms (34.4% vs. 100%, 66.7%, and 84.8%) compared with previous trials [10, 20, 33]. This wider inclusion likely contributed to the higher incidence of poor neurological outcomes observed in our cohort (71.8% vs. 35.0%, 63.2%, and 33.0%) [10, 20, 33]. These strict inclusion criteria in the randomized controlled trials (RCTs)—particularly the exclusion of non-cardiac etiologies and unwitnessed arrests—likely selected patients with relatively preserved cerebral autoregulation. Our broader inclusion criteria captured patients with more heterogeneous pathophysiology, where the therapeutic window for MAP optimization may be more relevant. This explains why the association between MAP duration and outcomes was most apparent in our moderate-severity subgroup, while previous RCTs with more homogeneous populations showed neutral results. Given the heterogeneity of our study population, including variations in cardiac arrest etiology and severity, we utilized the rCAST score to stratify injury severity and better evaluate the impact of MAP on neurological outcomes in OHCA survivors. The rCAST score has been extensively validated as a reliable prognostic tool in diverse OHCA populations. In a single-center U.S. validation study (n = 505), Kim et al. [34] demonstrated that the rCAST score achieved excellent discrimination for predicting poor neurological outcome (area under the curve [AUC]: 0.815; 95% CI: 0.763–0.867) and mortality (AUC: 0.799; 95% CI: 0.751–0.847), significantly outperforming the Pittsburgh Cardiac Arrest Category score for mortality prediction (p = 0.017). Similarly, in the multicenter study involving 658 patients across 24 intensive care units (ICUs), Lascarrou et al. [35] reported that rCAST maintained good performance (AUC: 0.82; 95% CI: 0.78–0.85), though it did not significantly outperform Utstein criteria (p = 0.16). Nevertheless, the authors emphasized the clinical utility of rCAST, noting its ease of calculation and rapid bedside determination as key advantages for routine implementation [35].
Our analysis showed that the association between the duration of MAP
In patients with low severity, relatively intact cerebral autoregulation may render additional MAP elevation unnecessary. However, individuals with moderate severity are more likely to have impaired autoregulation and borderline cerebral perfusion, placing them within a physiological range where elevated MAP may meaningfully enhance oxygen delivery and mitigate secondary brain injury. Conversely, patients with high severity often have extensive, irreversible brain damage, limiting the potential benefit of elevated MAP. These observations underscore the value of tailoring post-resuscitation hemodynamic management based on individual injury severity. Identifying patients in the moderate injury category who may benefit from higher MAP targets could facilitate more personalized and effective post-cardiac arrest care.
This study had several limitations. First, as a retrospective observational study, it cannot establish causality between MAP duration and neurological outcomes. Second, although the use of a multicenter registry enhances generalizability, approximately 25% of patients were excluded due to missing data, potentially introducing selection bias. Third, MAP was recorded hourly rather than continuously. This intermittent sampling may have failed to capture transient hypotensive episodes between measurements, potentially contributing to secondary brain injury. While continuous monitoring would provide a more granular assessment of hemodynamic stability, our use of hourly data from a large, multicenter registry represents a pragmatic and methodological advance over many prior studies that relied on less frequent, averaged values. Fourth, our analysis did not account for other hemodynamic parameters that may influence cerebral perfusion and outcomes, a notable limitation of this study. Specific data on the dose and duration of vasopressors or inotropes, as well as on net fluid balance, were not included in our analysis. These interventions are significant potential confounders. For instance, higher vasopressor doses may indicate more severe post-cardiac arrest shock, an independent predictor of poor outcomes, while fluid management can affect both MAP and cerebral edema. Although our multivariable models adjusted for overall illness severity using SOFA and rCAST scores, these scores may not fully capture the influence of these specific pharmacologic interventions was not assessed in the current analysis, and the potential for residual confounding remains. Fifth, the primary outcome was assessed through telephone interviews with patients or proxies. This method may be less sensitive than direct examination for detecting subtle cognitive deficits. Proxy reporting is also susceptible to recall bias, potentially overestimating favorable outcomes. While this approach is pragmatic for multicenter studies, such misclassification could influence the observed associations. Finally, cerebral perfusion pressure was not measured, precluding direct assessment of its relationship with MAP.
In this study, duration of MAP
All data generated or analyzed during this study are included in this article and its supplementary material files. Further enquiries can be directed to the corresponding author.
DHL, SJR: Conceptualization, Data curation, Investigation, Writing - original draft, Writing - review & editing. BKL: Conceptualization, Formal analysis, Methodology, Project administration, Software, Writing - original draft, Writing - review & editing. YHJ, KWJ: Conceptualization, Data curation, Investigation, Writing - review & editing. HJB, HJK, JSO: Data curation, Resources, Validation, Writing - review & editing. ISC: Data curation, Resources Supervision, Writing - review & editing. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was approved by each participating hospital institutional review board including the Chonnam National University Hospital Institutional Review Board (CNUH-2021-017). Written informed consent was obtained from all patients or their legally authorized representatives, in accordance with national regulations and the principles outlined in the Declaration of Helsinki.
We thank all Korean Hypothermia Network (KORHN) investigators.
This study was supported by a grant (BCRI24052) of Chonnam National University Hospital Biomedical Research Institute. And this research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: RS-2024-00335934).
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/RCM42733.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.