

 , Xinguang Chen 1,3,†, Yan Dong 1, Qiushi Chen 1, Nishant Yadav 1, Fengxiang Zhang 1,*
, Xinguang Chen 1,3,†, Yan Dong 1, Qiushi Chen 1, Nishant Yadav 1, Fengxiang Zhang 1,*
1 Division of Cardiology, The First Affiliated Hospital of Nanjing Medical University, 210029 Nanjing, Jiangsu, China
2 Division of Cardiology, Xuzhou Central Hospital, 221009 Xuzhou, Jiangsu, China
3 Section of Pacing and Electrophysiology, Division of Cardiology, The First Affiliated Hospital of Gannan Medical University, 341000 Ganzhou, Jiangxi, China
†These authors contributed equally.
Abstract
Atrial fibrillation catheter ablation (AFCA) success rates vary across different phenotypes of hypertrophic cardiomyopathy (HCM). Therefore, we compared long-term outcomes between apical (aHCM) and septal (sHCM) subtypes of HCM.
This retrospective study analyzed patients with HCM who underwent AFCA at the First Affiliated Hospital of Nanjing Medical University between January 2010 and December 2020.
A total of 36 patients with aHCM and 80 patients with sHCM were enrolled. During a median follow-up of 42 months (interquartile range (IQR) 18–83), the overall atrial tachyarrhythmia (ATa) recurrence rate after a single ablation was 42.2% (49/116). The aHCM patients had a higher ATa recurrence rate than the sHCM patients (58.3% vs. 35.0%; χ2 = 5.54; p = 0.019). The ATa recurrence risk increased by 94% in patients with aHCM (hazard ratio (HR) 1.94, 95% confidence interval (CI) 1.10–3.43; log-rank p = 0.021). Subgroup analysis demonstrated pronounced risk elevation in paroxysmal atrial fibrillation (AF) patients (HR 2.85, 95% CI 1.44–5.67; p = 0.003), while no intergroup difference was observed in patients with persistent AF (HR 0.90, 95% CI 0.31–2.62; p = 0.853) (interaction p = 0.080). Multivariate Cox regression analysis identified antiarrhythmic drug (AAD) use (HR 0.22, 95% CI 0.08–0.59; p = 0.003), hypertension comorbidity (HR 2.50, 95% CI 1.21–5.19; p = 0.014), persistent AF type (HR 0.41, 95% CI 0.17–1.00; p = 0.049), and left atrial diameter ≥45 mm (HR 2.55, 95% CI 1.11–5.85; p = 0.028) as independent predictors of postoperative recurrence.
An aHCM subtype predicts higher ATa recurrence after a single ablation versus sHCM. Hypertension, a left atrial enlargement ≥45 mm, and no AAD use are independent predictors of recurrence. Meanwhile, optimizing blood pressure and AAD therapy may improve outcomes.
Keywords
- apical hypertrophic cardiomyopathy
- atrial fibrillation
- catheter ablation
- septal hypertrophic cardiomyopathy
- recurrence
Atrial fibrillation (AF) affects 22.5% of hypertrophic cardiomyopathy (HCM) patients [1, 2]. It increases heart failure risk and mortality [3, 4]. Drug treatment is limited to maintaining sinus rhythm (SR) yet may cause serious adverse effects [5]. Catheter ablation (CA) offers an alternative approach. Prior studies [6, 7] support the feasibility and relative safety of CA for managing AF in HCM. However, success rates differ, and there is a frequent need for repeat procedures [8]. Depending on the predominant localization of segmental myocardial hypertrophy, HCM has distinct subtypes: septal (sHCM) and apical (aHCM) [9]. The potential differential effects of CA for AF among HCM phenotypes are not well established. Given the limited and inconsistent evidence, we directly compared ablation outcomes between these phenotypes.
Patients with HCM and AF who underwent de novo CA at the First
Affiliated Hospital of Nanjing Medical University between January 2010 and
December 2020 were included in this retrospective study. Exclusion criteria: (1)
Individuals with prior CA for AF; (2) Patients presenting with severe
comorbidities; (3) Cases with incomplete peri-procedural documentation; (4) Age
All patients received effective pre-procedural anticoagulation. Transesophageal echocardiography or computerized tomography (CT) excluded cardiac thrombi. This study was conducted by following the Declaration of Helsinki and was approved by the Ethics Committee of the First Affiliated Hospital of Nanjing Medical University (ethics approval number: 2020-SR-494). Informed consent was waived due to the retrospective nature of the study.
AF was categorized as either paroxysmal or persistent based on the established
guidelines [10]. Paroxysmal AF is defined as a continuous episode lasting longer
than 30 seconds but resolving spontaneously or through intervention within seven
days. In contrast, persistent AF lasts longer than seven days but less than one
year in duration. The diagnosis of HCM was made according to the 2011 American
Heart Association (AHA) guidelines [11], which require that the left ventricular
(LV) end-diastolic wall thickness be
All non-amiodarone antiarrhythmic medications were discontinued more than five
half-lives pre-procedure. Local anesthesia was used during the procedures.
Systemic anticoagulation was achieved through intravenous administration of
heparin, maintaining an activated clotting time of 300–350 seconds throughout
the procedure. The standardized Atrial fibrillation catheter ablation (AFCA)
protocol used at our institution has been described in previous studies [13, 14].
A three-dimensional electroanatomical mapping system (CARTO, Biosense Webster)
guided the ablation procedure. Complete circumferential pulmonary veins isolation
(CPVI) was achieved using an Ablation index (AI)-guided approach, producing
continuous circular lesions at a power of 30 to 40 W and contact force of 15
Anticoagulation was recommended for a minimum of three months following ablation in patients with paroxysmal AF and for at least six months in those with persistent AF. Antiarrhythmic drugs (AADs) were resumed but then stopped after a 3-month post-ablation blanking period. Patients with blanking recurrence were treated with AADs and/or cardioversion if needed. All patients underwent scheduled follow-up assessments at our outpatient clinics at 1, 3, 6, 12 months postoperatively, as well as 6 months thereafter. A recurrence of atrial tachyarrhythmia (ATa) was defined as the return of AF/AFL/AT lasting more than 30 s on the standard Electrocardiograph (ECG), or 24-h Holter recording during the follow-up period after the 3-month post-ablation blanking period.
Normally distributed continuous variables were expressed as mean
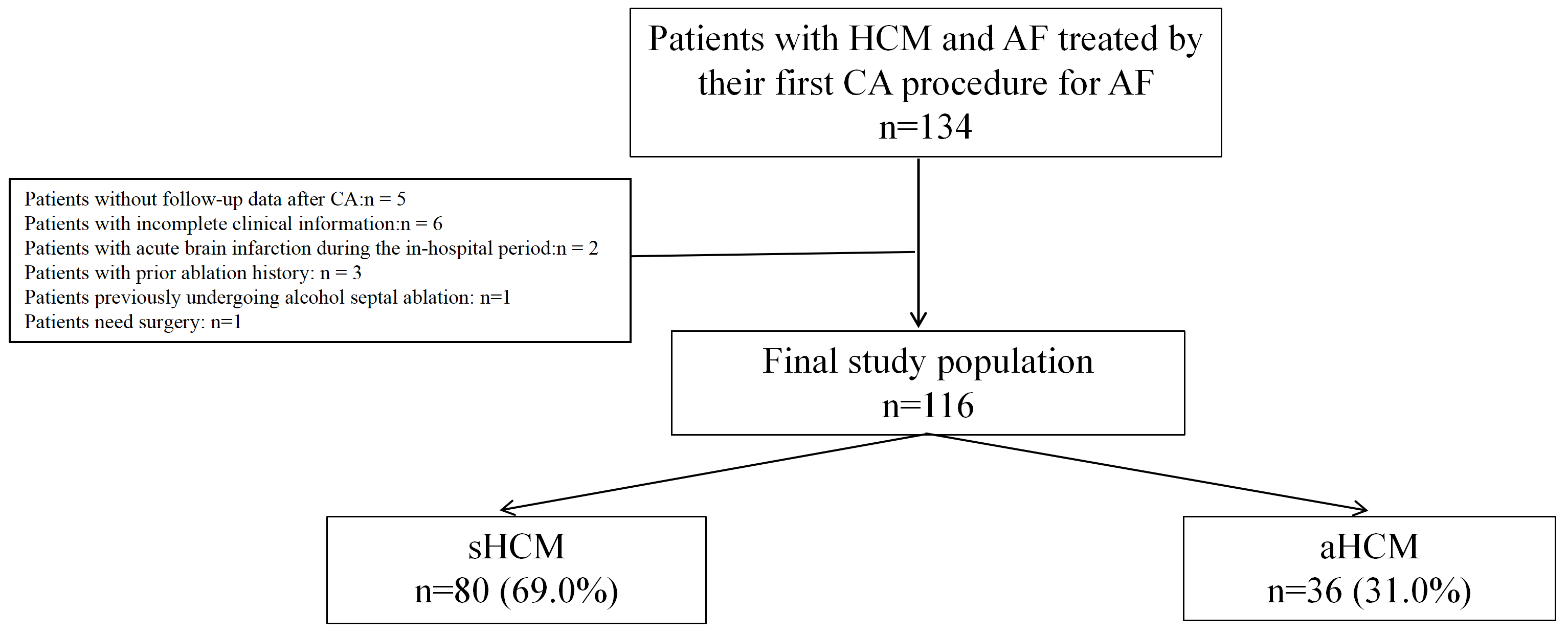
Between January 2010 and December 2020, 134 consecutive patients with HCM and
drug-refractory symptomatic AF undergoing first CA were enrolled. After excluding
five cases who failed to complete follow-up, six with incomplete clinical data,
one who had previously undergone alcohol septal ablation, one who required
surgery, three with prior history of ablation, and two who experienced acute
brain infarction during hospitalization, a total of 116 individuals were included
in the study: 36 aHCM, 80 sHCM (Fig. 1). The mean age was 57.9
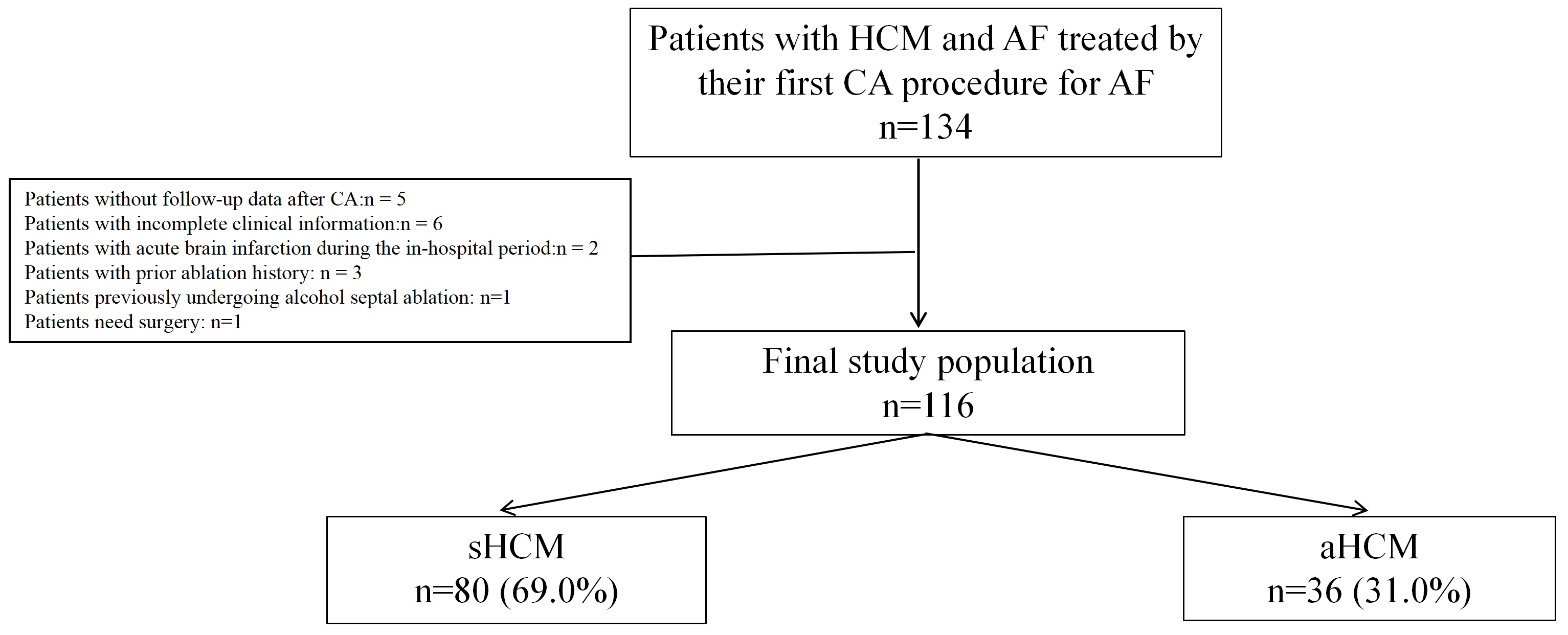 Fig. 1.
Fig. 1.
Flow diagram for this study. HCM, hypertrophic cardiomyopathy; AF, atrial fibrillation; CA, catheter ablation; sHCM, septal hypertrophic cardiomyopathy; aHCM, apical hypertrophic cardiomyopathy.
| Variables | All patients | sHCM | aHCM | p-value |
| (n = 116) | (n = 80) | (n = 36) | ||
| Age (yrs) | 57.9 |
56.3 |
61.4 |
0.024 |
| Male, n (%) | 82 (70.7) | 58 (72.5) | 24 (66.7) | 0.523 |
| Height (cm) | 170.5 |
170.8 |
170.0 |
0.645 |
| Weight (kg) | 70.6 |
70.7 |
70.3 |
0.814 |
| Persistent AF, n (%) | 34 (29.3) | 23 (28.7) | 11 (30.6) | 0.843 |
| AF duration (month) | 36 (12.0, 72.0) | 36 (12.0, 72.8) | 48 (25.5, 72.0) | 0.596 |
| Hypertension, n (%) | 54 (46.6) | 32 (40.0) | 22 (61.1) | 0.035 |
| Diabetes, n (%) | 21 (18.1) | 17 (21.3) | 4 (11.1) | 0.190 |
| CHA2DS2-VASC | 1.7 |
1.5 |
2.0 |
0.122 |
| LAD (mm) | 45.3 |
45.1 |
45.8 |
0.485 |
| RAD (mm) | 36.9 |
36.9 |
36.8 |
0.941 |
| LVEDD (mm) | 47.1 |
46.8 |
47.9 |
0.117 |
| LVEDS (mm) | 30.6 |
30.5 |
30.8 |
0.643 |
| LVEF (%) | 63.5 |
63.0 |
64.7 |
0.037 |
| IVS (mm) | 16.1 |
16.5 |
12.9 |
|
| LVOTO (%) | 9 (7.8) | 9 (11.3) | - | NA |
| LVOTG (mmHg) | - | 31.4 |
- | NA |
| LVPW (mm) | 11.2 |
11.5 |
10.7 |
0.304 |
| AADs, n (%) | 109 (94.0) | 75 (93.8) | 34 (94.4) | 1.000* |
| 90 (77.6) | 66 (82.5) | 24 (66.7) | 0.059 | |
| ACEI/ARB, n (%) | 40 (34.5) | 32 (40.0) | 8 (22.2) | 0.062 |
| Calcium antagonist, n (%) | 17 (14.7) | 8 (10.0) | 9 (25.0) | 0.035 |
| NOACs, n (%) | 39 (33.6) | 25 (31.3) | 14 (38.9) | 0.420 |
| Warfarin, n (%) | 69 (59.5) | 47 (58.8) | 22 (61.1) | 0.811 |
ACEI/ARB, angiotensin-converting enzyme inhibitor/angiotensin II receptor blocker; AF, atrial fibrillation; NOACs, non-vitamin K antagonist oral anticoagulants; LAD, left atrial diameter; RAD, right atrial diameter; LVEDD, left ventricular end-diastolic diameter; LVEDS, left ventricular end-systolic diameter; LVEF, left ventricular ejection fraction; IVS, interventricular septum thickness; LVOTO, left ventricular outflow tract obstruction; LVOTG, left ventricular outflow tract gradient; LVPW, left ventricular posterior wall thickness; AADs, antiarrhythmic drugs; *, Fisher’s exact test; NA, not applicable.
The details of the ablation procedures are summarized in Table 2. CPVI was
achieved in all patients. Substrate modification-encompassing linear ablation
and/or fractionated potential ablation-was performed more frequently in the aHCM
cohort (30.6% vs.15.0%, p = 0.052). Cavotricuspid isthmus isolation and
superior vena cava isolation were similar between groups (8.3% vs. 17.5%; 5.6%
vs. 6.3%, both p
| Variables | All patients | sHCM | aHCM | p-value |
| (n = 116) | (n = 80) | (n = 36) | ||
| PV isolation, n (%) | 116 (100) | 80 (100) | 36 (100) | NA |
| Substrate modification, n (%) | 23 (19.8) | 12 (15.0) | 11 (30.6) | 0.052 |
| CTI isolation, n (%) | 17 (14.7) | 14 (17.5) | 3 (8.3) | 0.197 |
| SVC isolation, n (%) | 7 (6.0) | 5 (6.3) | 2 (5.6) | 0.884 |
| Complications, n (%) | 1 (0.8) | 1 (1.3) | 0 (0.0) | 1.000* |
| Follow-up months | 42 (18, 83) | 43 (23, 85) | 38 (13, 78) | 0.172 |
| ATa recurrence, n (%) | 49 (42.2) | 28 (35.0) | 21 (58.3) | 0.019 |
PV, pulmonary vein; CTI, cavotricuspid isthmus; SVC, superior vena cava; Ata, atrial tachycardias; *, Fisher’s exact test; NA, not applicable.
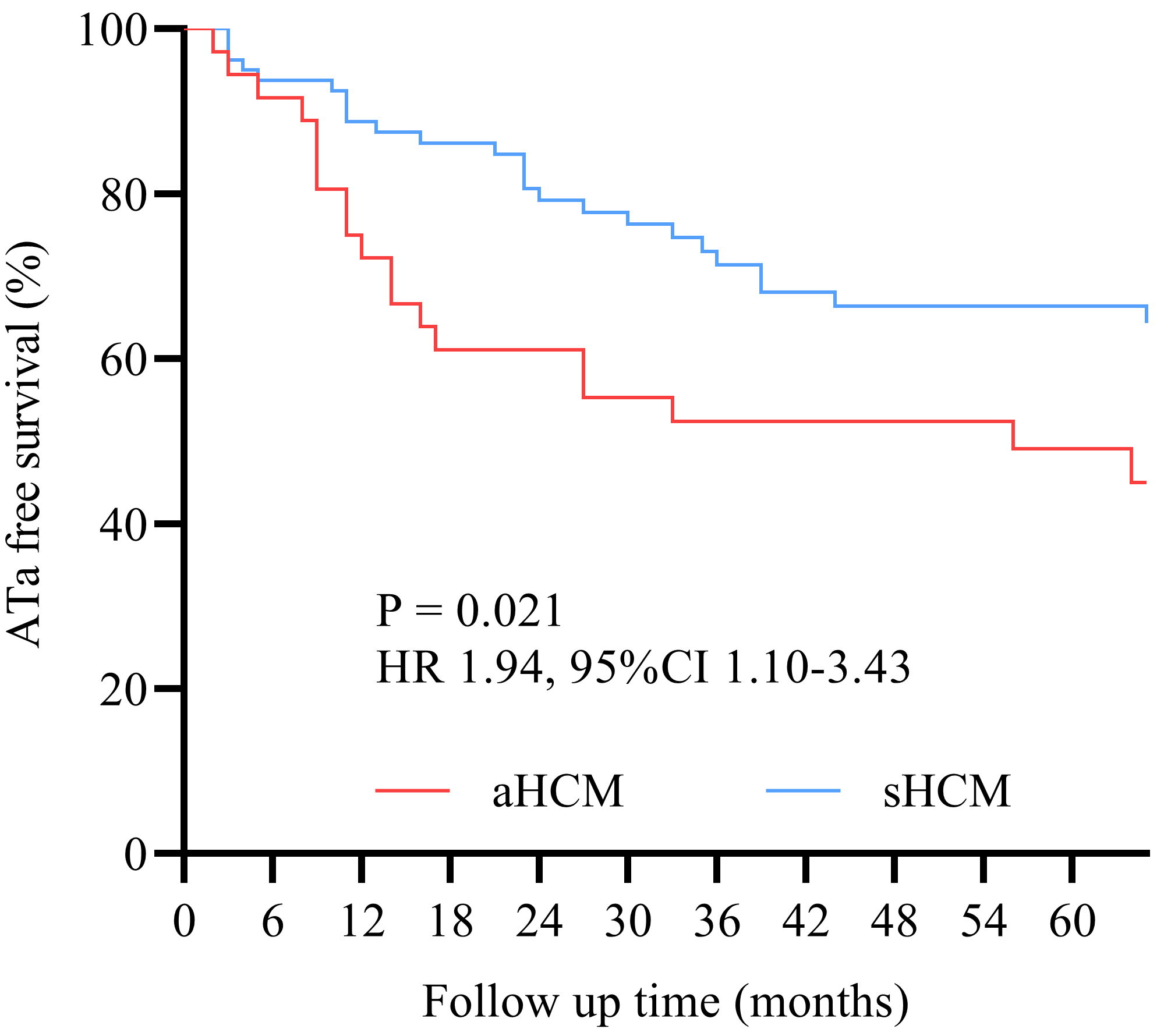
Overall ATa recurrence rate was 42.2% (49/116), after a median follow-up of 42
(18, 83) months. The aHCM group demonstrated significantly higher ATa recurrence
rates than the sHCM group [58.3% (21/36) vs. 35.0% (28/80);
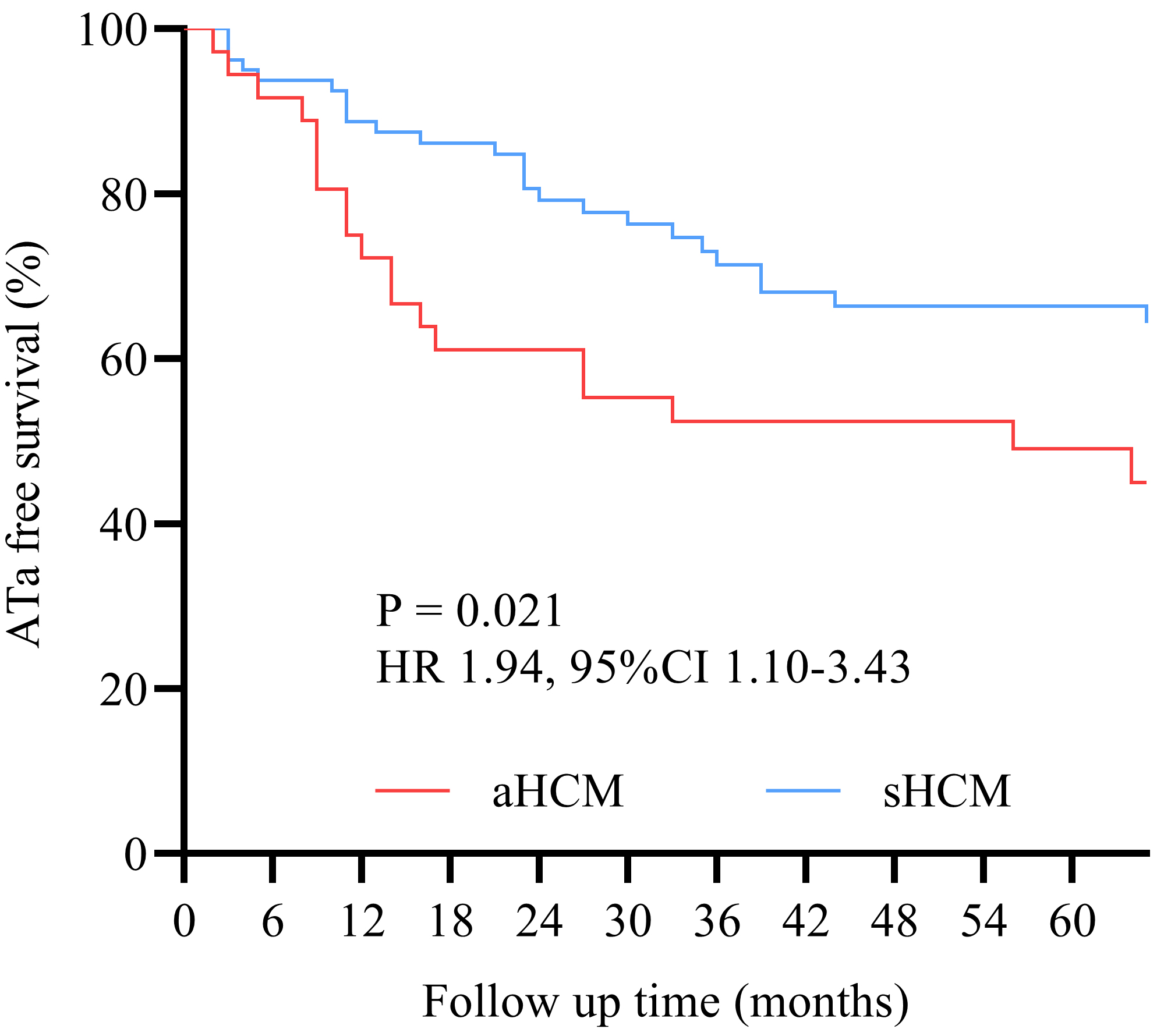 Fig. 2.
Fig. 2.
Kaplan–Meier survival curves. Kaplan–Meier analysis revealed a 94% increased cumulative ATa recurrence risk in the aHCM group compared to the sHCM group (HR 1.94, 95% CI 1.10–3.43; log-rank p = 0.021).
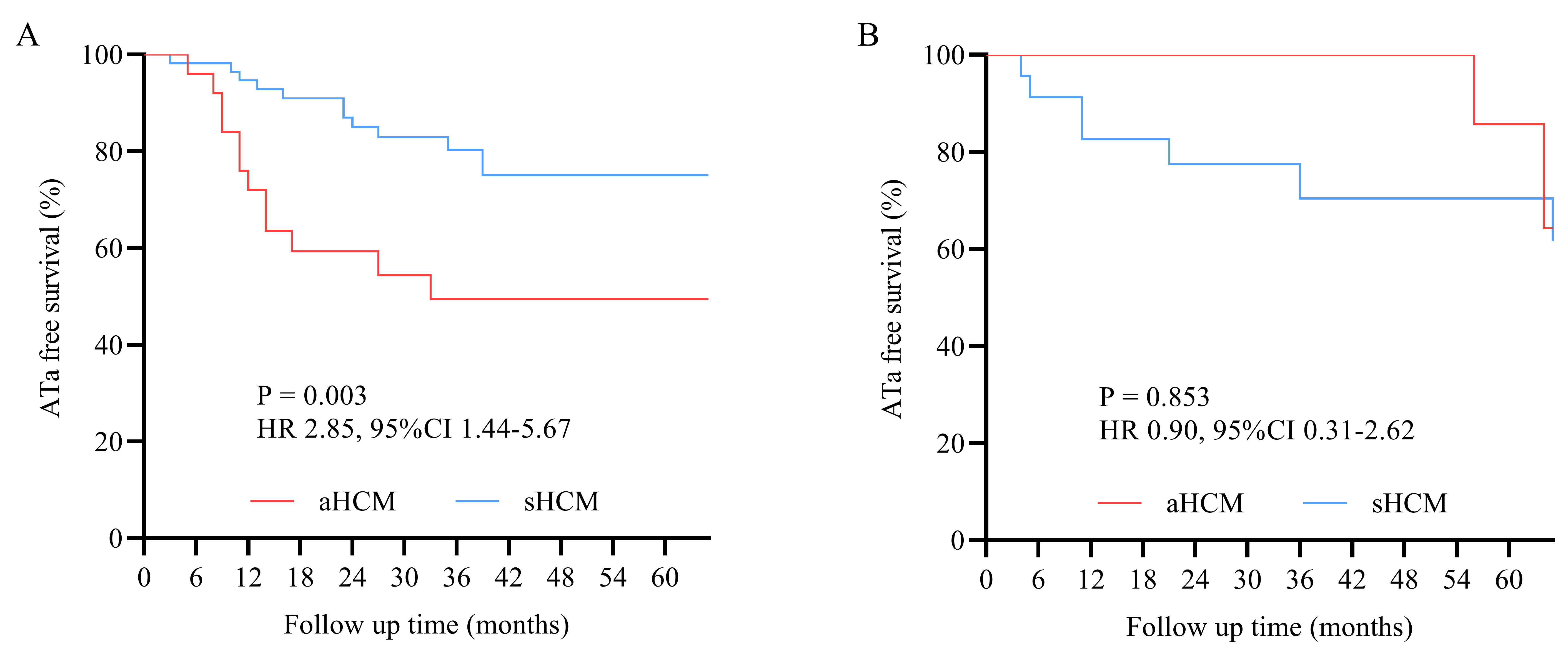 Fig. 3.
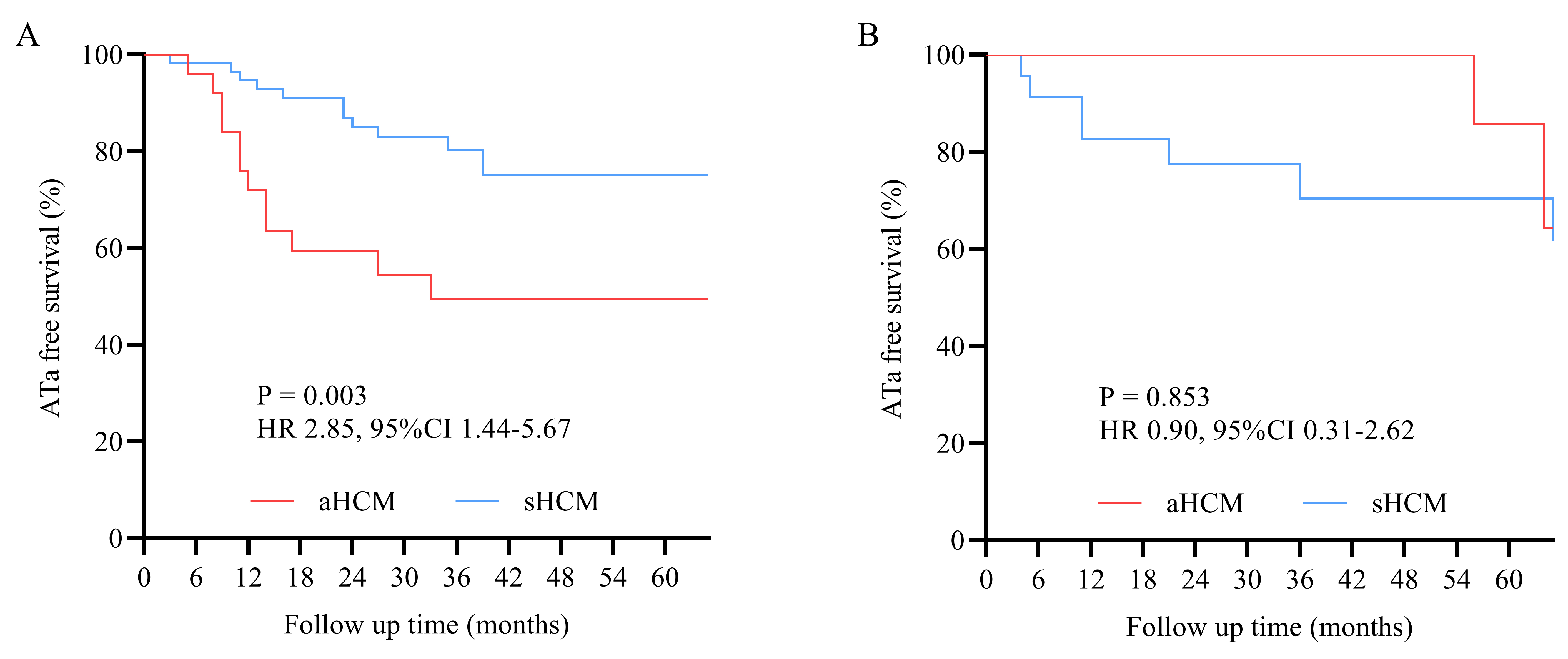
Fig. 3.
Kaplan–Meier survival curves. (A) sHCM demonstrated superior outcomes versus aHCM in paroxysmal AF (p = 0.003). (B) No significant intergroup difference observed in persistent AF (p = 0.853).
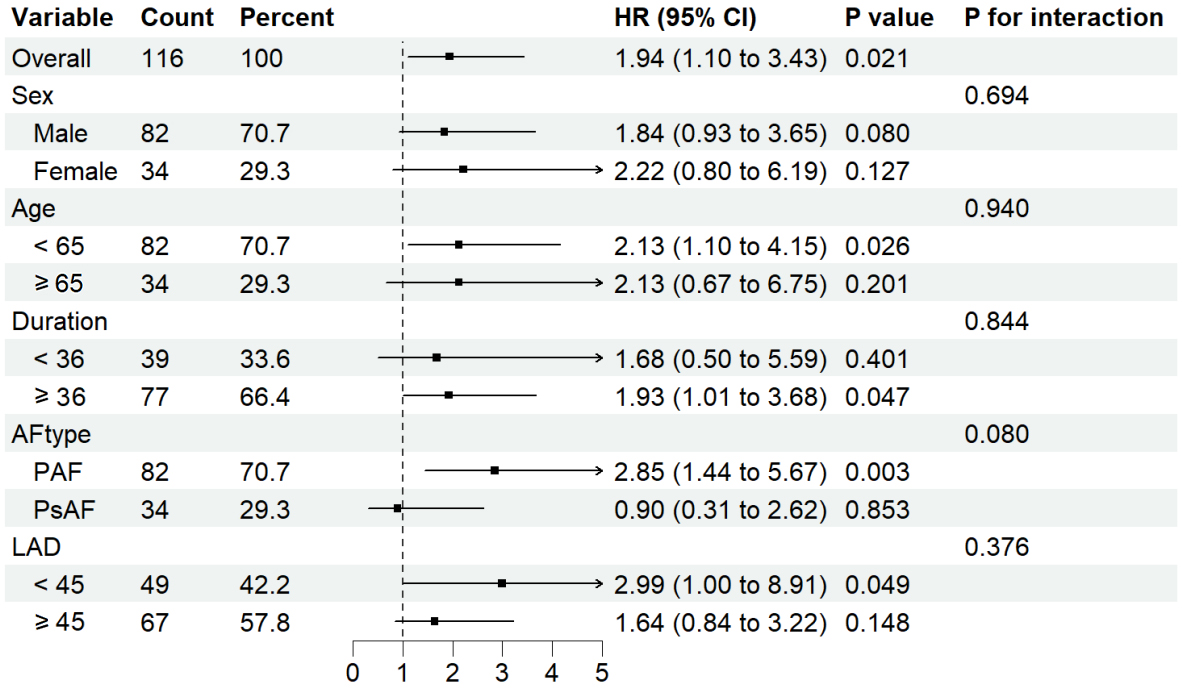
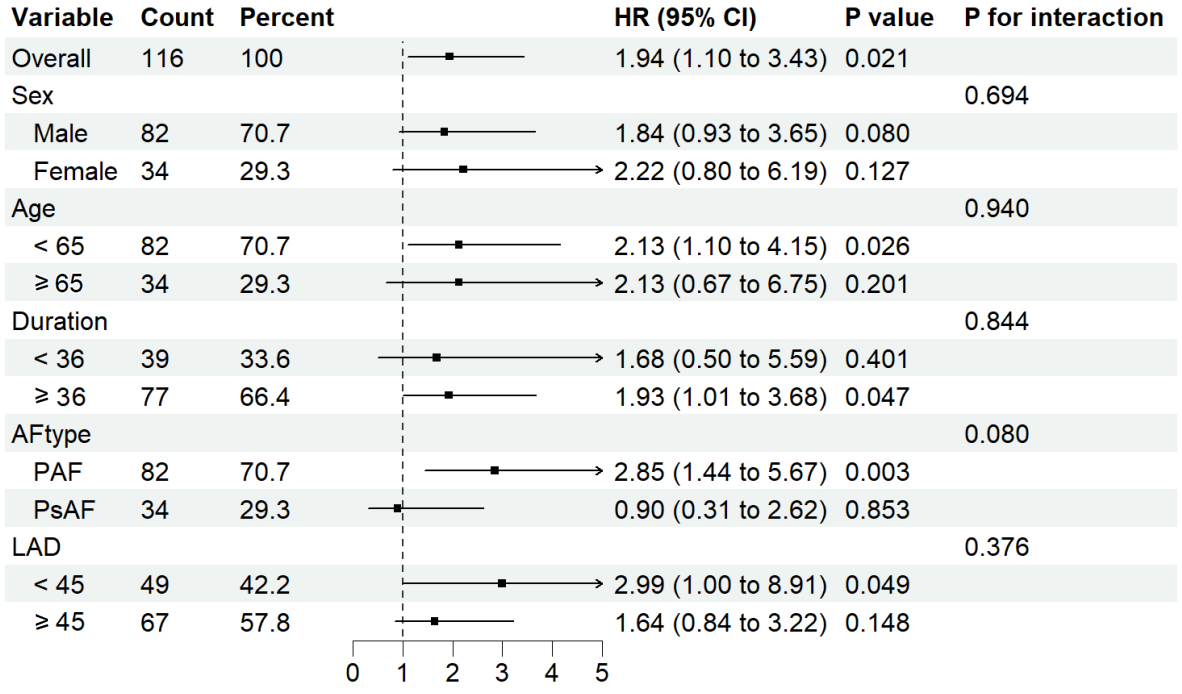 Fig. 4.
Fig. 4.
Subgroup heterogeneity analysis. The forest plot demonstrates a
non-significant interaction effects across prespecified subgroups (p for interaction
Patients with ATa recurrence exhibited longer AF duration, higher prevalence of
hypertension, larger left atrial diameter (
| Variables | With recurrence | Without recurrence | p-value |
| (n = 35) | (n = 81) | ||
| Age (yrs) | 60.2 |
56.9 |
0.096 |
| Male, n (%) | 26 (74.3) | 56 (69.1) | 0.576 |
| Height (cm) | 171.0 |
170.4 |
0.695 |
| Weight (kg) | 71.4 |
70.3 |
0.595 |
| Persistent AF, n (%) | 10 (28.6) | 24 (29.6) | 0.909 |
| AF duration (months) | 67.1 |
53.4 |
0.309 |
| Hypertension, n (%) | 23 (65.7) | 31 (38.3) | 0.007 |
| Diabetes, n (%) | 6 (17.1) | 15 (18.5) | 0.860 |
| LAD |
27 (77.1) | 40 (49.4) | 0.005 |
| RAD (mm) | 36.2 |
37.2 |
0.301 |
| LVEDD |
26 (74.3) | 47 (58.0) | 0.096 |
| LVEDS (mm) | 30.6 |
30.6 |
0.990 |
| IVS (mm) | 16.4 |
16.0 |
0.566 |
| LVEF (%) | 63.5 |
63.5 |
0.928 |
| LVOTO (%) | 7 (8.6) | 2 (5.7) | 0.588 |
| AADs (n) | 29 (82.9) | 80 (98.8) | 0.001 |
| 25 (71.4) | 65 (80.2) | 0.296 | |
| ACEI/ARB, n (%) | 11 (31.4) | 29 (35.8) | 0.649 |
| Calcium antagonist, n (%) | 6 (17.1) | 11 (13.6) | 0.618 |
| NOACs, n (%) | 12 (34.3) | 27 (33.3) | 0.921 |
| Warfarin, n (%) | 23 (65.7) | 46 (56.8) | 0.369 |
| aHCM, n (%) | 15 (42.9) | 21 (25.9) | 0.070 |
| Substrate modification, n (%) | 11 (31.4) | 12 (14.8) | 0.039 |
| CTI isolation, n (%) | 3 (8.6) | 14 (17.3) | 0.223 |
| SVC isolation, n (%) | 0 | 7 (8.6) | 0.173 |
AF, atrial fibrillation; ACEI/ARB, angiotensin-converting enzyme inhibitor/angiotensin II receptor blocker; NOACs, non-vitamin K antagonist oral anticoagulants; LAD, left atrial diameter; RAD, right atrial diameter; LVEDD, left ventricular end-diastolic diameter; LVEDS, left ventricular end-systolic diameter; LVEF, left ventricular ejection fraction; LVOTO, left ventricular outflow tract obstruction; AADs, antiarrhythmic drugs; CTI, cavotricuspid isthmus; SVC, superior vena cava; sHCM, septal hypertrophic cardiomyopathy.
| Variables | HR | 95% CI | p-value |
| AAD | 0.22 | 0.08–0.59 | 0.003 |
| Hypertension | 2.50 | 1.21–5.19 | 0.014 |
| LAD |
2.55 | 1.11–5.85 | 0.028 |
| LVEDD |
0.84 | 0.36–1.97 | 0.690 |
| HCM type (aHCM) | 1.49 | 0.07–3.14 | 0.299 |
| AF duration | 1.00 | 0.99–1.01 | 0.284 |
| AF type (PeAF) | 0.41 | 0.17–1.00 | 0.049 |
| Substrate modification | 0.28 | 0.69–1.57 | 0.590 |
| mitral regurgitation | 1.55 | 0.57–4.21 | 0.395 |
AADs, antiarrhythmic drugs; AF, atrial fibrillation; LAD, left atrial diameter;
LVEDD, left ventricular end-diastolic dimension; sHCM, septal hypertrophic
cardiomyopathy; AF, atrial fibrillation. Bold values: p
This study revealed three principal findings: (1) The overall ATa recurrence after a single procedure was 42.2% over a nearly four-year follow-up period. (2) aHCM patients had a significantly higher recurrence rate than those with sHCM, primarily driven by the presence of paroxysmal AF. (3) Hypertension, left atrial enlargement, and no AAD use were identified as independent predictors of recurrence.
Our overall success rate (57.8%) aligns with prior HCM ablation studies [6, 7, 15, 16, 17]. Notably, despite requiring multiple procedures, success rates in HCM patients remained substantially lower than in non-HCM populations [8], underscoring the impact of HCM-specific myocardial substrate on ablation outcomes. HCM-driven atrial remodeling occurs through two main pathways: first, structural changes such as left atrial wall hypertrophy and pulmonary venous sleeve dysplasia [16, 18]; and second, hemodynamic stress resulting from diastolic dysfunction, which leads to progressive left atrial dilation. Together, these mechanisms contribute to electromechanical remodeling, characterized by low-voltage zones and increased complex fractionated electrograms.
Evidence regarding the outcomes of AF ablation across various subtypes of HCM remains inconsistent and conflicting [19, 20]. Our data show that ATa recurrence is higher in patients with aHCM compared to those with sHCM. We propose three potential explanations for this observation. First, aHCM demonstrates a greater presence of low-voltage zones; our findings support this, showing that substrate modification occurred twice as frequently in aHCM patients (30.6% compared to 15.0% in sHCM). Second, electromechanical dysfunction associated with apical hypertrophy leads to impaired ventricular relaxation, which increases left atrial pressure and exacerbates atrial stretch and electrical instability. Third, the higher prevalence of hypertension in aHCM patients may further compound the risk of recurrence, with hypertension independently predicting recurrence (HR 2.50).
The pronounced risk associated with paroxysmal AF, indicated by a hazard ratio of 2.85, contrasts with persistent AF, which showed no significant difference (p = 0.853), suggesting that triggers may be phenotype-specific. In paroxysmal AF, the condition primarily arises from the pulmonary veins, and the distinct fibrosis creates arrhythmogenic substrates that extend beyond the pulmonary veins, potentially harboring non-pulmonary vein triggers that are resistant to standard ablation techniques. In contrast, persistent AF is influenced by a more diffuse substrate, and both phenotypes exhibit advanced remodeling, which may dilute the differences observed between them. Clinically, this implies that patients with aHCM and paroxysmal AF might benefit from first-line extensive substrate ablation strategies, such as posterior wall isolation and voltage mapping. Our strict criteria for sHCM, focusing on reverse-curve septal hypertrophy, allow for a clearer isolation of phenotype effects.
While left atrial enlargement remains a key predictor of recurrence [21, 22, 23], our
study has identified hypertension (adjusted Hazard Ratio (aHR) 2.50, 95% CI
1.21–5.19) and AAD usage (aHR 0.22, 95% CI 0.08–0.59) as independent risk
modifiers. Hypertension may accelerate fibrosis via RAAS overactivation and
autonomic dysregulation, while the maintenance of AAD usage likely stabilizes
post-ablation substrates. Antihypertensive therapy could reduce both the
incidence of de novo AF and post-cardioversion/ablation recurrence,
particularly when targeting optimal blood pressure control [24]. As hypertension
represents a modifiable risk factor, optimized blood pressure control (target
Performing concomitant AF surgery during septal myectomy effectively eliminates
AF in patients with HOCM [29]. However, this study specifically excluded patients
with more severe forms of HCM that would necessitate surgical intervention. The
majority of our cohort consisted of patients with mild hypertrophy, with an
average septal thickness of 16.1
A significant limitation of this study is the absence of a systematic assessment of late gadolinium enhancement (LGE). CMRI-LGE is considered the gold standard for measuring fibrosis in both the atria and ventricles. This fibrosis has been linked to the complexity of the AF substrate and the ablation outcomes in HCM [30, 31]. Without LGE data, we could not evaluate whether the differences in fibrotic burden contribute to the varying efficacy observed between apical and septal phenotypes. Therefore, future research should incorporate LGE assessments to accurately identify patients who might benefit from additional substrate modification strategies. The study has several additional limitations: First, the single-center retrospective design increases the risk of selection bias and residual confounding, particularly concerning the phenotyping of HCM and the standardization of ablation strategies. Second, the moderate sample size of 116 participants limits the robustness of subgroup analyses. Third, genetic factors such as MYBPC3 and MYH7 mutations were not systematically assessed. Additionally, the absence of left atrial strain parameters and the reliance on left ventricular end-diastolic dimension measurements, rather than volumetric assessments may inadequately characterize diastolic dysfunction in HCM. Furthermore, 24-hour Holter monitoring may underestimate asymptomatic recurrences or intermittent ATa episodes. Lastly, the lack of quantitative symptom assessment restricts our ability to evaluate the clinical benefits of ablation beyond merely measuring arrhythmia recurrence. Previous studies have shown that AF ablation can enhance symptom alleviation even in cases of recurrent ATa [32]. Therefore, future research needs to incorporate patient-reported outcomes to provide a more comprehensive understanding of the treatment’s impact.
Our study indicates that patients with aHCM face a significantly greater risk of ATa recurrence after ablation compared to those with sHCM. This notable difference in recurrence rates for paroxysmal AF underscores the need to recognize the specific vulnerabilities associated with different phenotypes. Consequently, our findings suggest that treatment strategies should be tailored to individual phenotypes. Additionally, maintaining strict control of hypertension, aiming for a blood pressure of less than 130/80 mmHg, along with the use of AADs after the ablation, is essential. Future research should focus on validating the benefits of adjunctive ablation techniques and the use of CMRI to quantify fibrosis, as these approaches could significantly enhance outcomes for this high-risk patient group.
The data presented in this study are available on request from the corresponding author.
FXZ, WD, QSC, and XGC designed the study and conceived the paper and revised the manuscript. WD, XGC, YD, and NY performed statistical analysis and drafted the manuscript. FXZ, QSC, and XGC were responsible for the methodology and investigation. YD, NY, and XGC arranged the data and performed visualization. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was approved by the Ethical Committee of the First Affiliated Hospital of Nanjing Medical University. All participants provided written informed consent as there were no interventions. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the First Affiliated Hospital with Nanjing Medical University (ethics approval number: 2020-SR-494).
We want to thank the patients who participated in this study.
This study was funded by the Chinese Society of Cardiology (CSCF2022A03), the 6th phase 333 project of Jiangsu Province (2022-2-408), Zhongnanshan Medical Foundation of Guangdong Province: ZNSA-2020017, and Clinical Competence Promotion Project Medical Program (JSPH-MA-2022-10).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.