
 , Xiang-Qing Kong 1,2,*
, Xiang-Qing Kong 1,2,*1 Department of Cardiology, Gusu School, Nanjing Medical University, 215008 Suzhou, Jiangsu, China
2 Department of Cardiology, The First Affiliated Hospital of Nanjing Medical University, 210000 Nanjing, Jiangsu, China
†These authors contributed equally.
Abstract
We explore the association between leucocyte telomere length (LTL) and all-cause and cardiovascular disease (CVD)-specific death in CVD patients.
We acquired 1599 CVD patients from a nationally representative US population survey for this study. We applied Kaplan–Meier curves, adjusted weighted Cox regression models, and restricted cubic spline to investigate the association between LTL and all-cause death. Additionally, we employed competing risk regression to assess the impact of LTL on cardiovascular-specific death, setting non-cardiovascular death as a competing event.
The overall mortality rate was 31.0% after a median follow-up of 13.9 years. Patients with shorter LTL exhibited a higher risk of all-cause death, with an adjusted hazard ratio (HR) of 1.25 (95% confidence interval (CI): 1.05–1.48). Restricted cubic spline illustrated a linear dose-response relationship. In gender-specific analyses, female patients with shorter LTL showed a higher risk of death (weighted HR, 1.79; 95% CI, 1.29–2.48), whereas this association was not observed in males (weighted HR, 0.90; 95% CI, 0.61–1.32). The Fine–Gray competing risk model revealed no significant relationship between LTL and cardiovascular-specific mortality but a significant association with non-cardiovascular death (adjusted HR, 1.24; 95% CI, 1.02–1.51).
LTL is inversely associated with all-cause death in female CVD patients. The significant correlation between reduced LTL and increased all-cause mortality emphasizes LTL as a potential marker for tertiary prevention against cardiovascular disease.
Keywords
- telomere length
- cardiovascular-specific death
- all-cause mortality
- Fine–Gray competing risk model
Telomeres, composed of tandem repetitive DNA sequences at eukaryotic chromosome termini, are essential for maintaining genomic stability and integrity during cell division [1, 2]. Accumulating evidence suggests that telomere lengths act as a dependable biomarker of cellular aging, serving as a mitotic clock reflecting cell division history [3, 4, 5]. Telomere length is influenced by various factors, such as age, sex, diseases, genetic variation, physiological stress, and lifestyle [6, 7]. Notably, telomere length is inversely correlated with age, and its shortening can lead to chromosomal end instability and genetic information loss [8, 9, 10].
Despite continuous efforts, cardiovascular disease (CVD) remains a major cause of mortality globally, with it responsible for 32% of deaths worldwide in 2019 [11]. Inflammation and oxidative stress have been well demonstrated as primary contributors to CVD [12, 13, 14]. Telomere shortening may exacerbate oxidative stress, leading to DNA damage, inflammation, and cellular dysfunction [15, 16, 17].
In epidemiological studies, peripheral leukocyte DNA is widely used to measure telomere length owing to the simplicity of blood sample collections [4]. Emerging research indicates that reduced leukocyte telomere length (LTL) is significantly associated with elevated mortality risk in the general population [18, 19, 20]. A study examining the general U.S. population revealed an inverse relationship between LTL and the risk of CVD [21]. Moreover, a meta-analysis has drawn attention to the link between shortened LTL and increased all-cause mortality across a broader population [22]. Recently, Xiong et al. [23] reported increased rates of both all-cause and CVD-related death in metabolic syndrome patients who exhibited shorter LTLs. However, the relationship between the LTL and specific outcomes for CVD patients remains uncertain. Accordingly, we explore the association between LTL and both all-cause and CVD-specific death among CVD patients in this study.
The NHANES is a national cross-sectional survey evaluating the health status of U.S. individuals. The NHANES has been conducting biennial national surveys since 1999, each encompassing about 5000 nationally representative participants. The NHANES provides a comprehensive collection of demographic, physical examinations, laboratory indicators, and questionnaire information [24, 25, 26]. This study focused on only the 1999–2000 and 2001–2002 NHANES cycles, as LTL measurements were only available during these periods.
The National Death Index (NDI) database is a central repository for death records, facilitating the investigation of associations between health factors and mortality. The NDI database provides information until death or the censoring date (December 31, 2015).
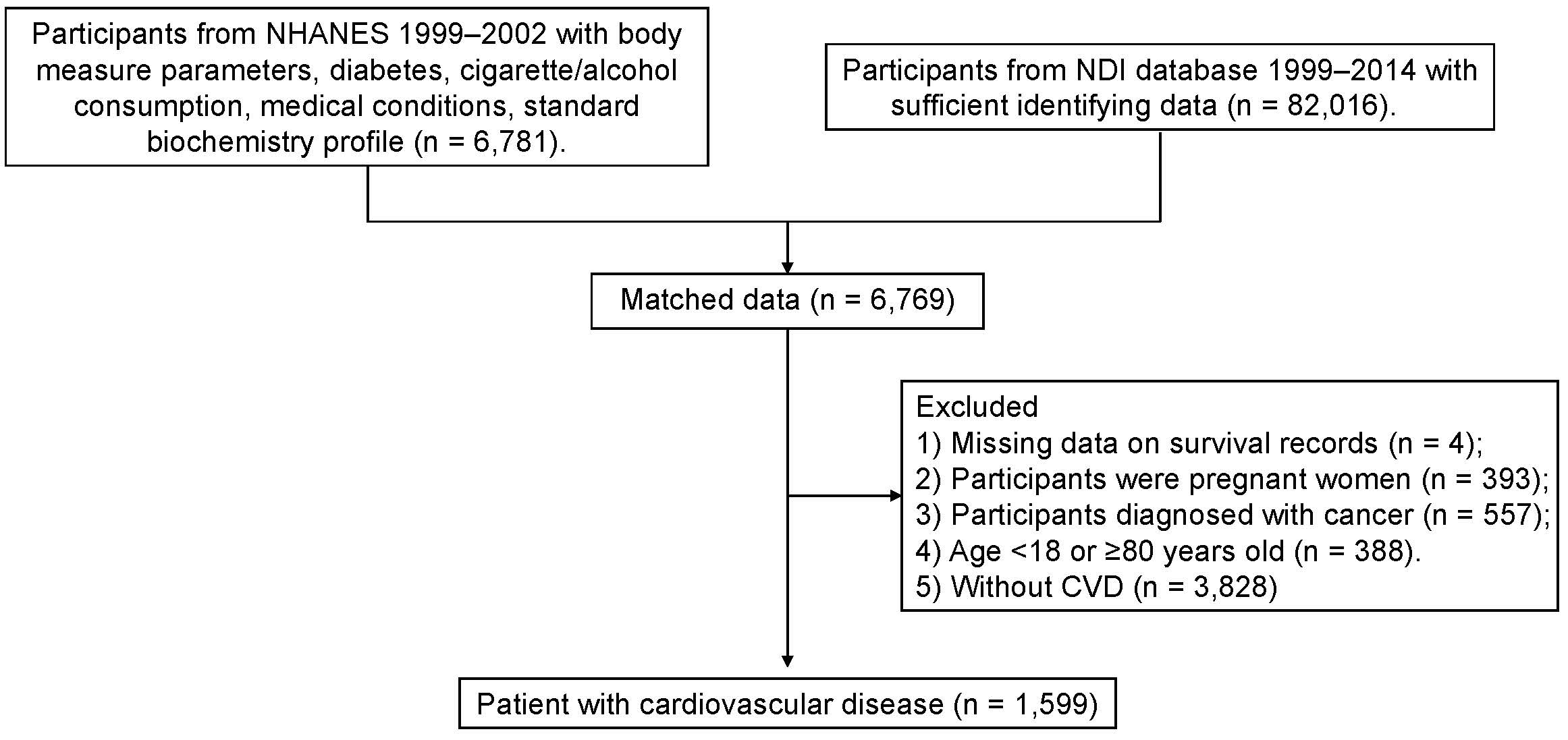
Fig. 1 provides the flowchart for participant selection. This research included participants from the 1999–2002 NHANES cycles who had records on body measurements, diabetes, cigarette/alcohol use, medical conditions, and standard biochemistry profiles. Exclusion criteria were: (1) incomplete survival record data; (2) pregnancy; (3) cancer diagnosis; (4) age under 18 or over 79; (5) absence of CVD. Ultimately, 1599 individuals diagnosed with CVD were enrolled in the study. NHANES survey was approved by the Ethics Review Committee of the National Center, and all participants provided written informed consent.
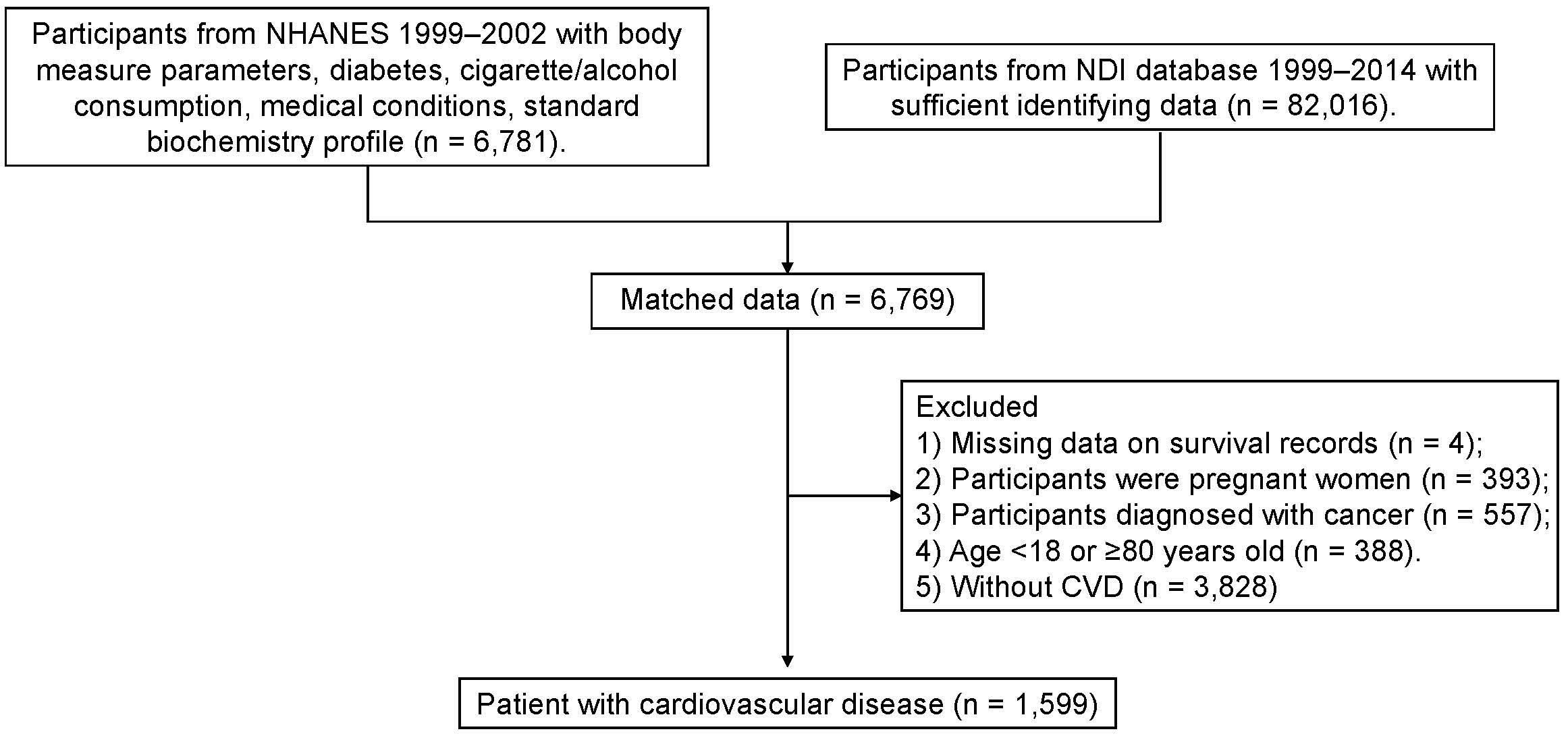 Fig. 1.
Fig. 1.
Flow chart for participant selection. This diagram outlines the criteria and steps to select eligible study participants from the NHANES database and the subsequent mortality tracking using the NDI. NHANES, National Health and Nutrition Examination Survey; NDI, National Death Index; CVD, cardiovascular disease.
The methodology for telomere length measurement has been reported in previous
studies [21, 27, 28]. Genomic DNA was extracted from peripheral blood samples
using QIAamp 96 DNA Blood kits (Qiagen, Valencia, CA, USA). The NHANES utilized a
multiplex quantitative PCR method to determine relative telomere length. This
technique measures the telomere repeat copy number (T) ratio to a single-copy
gene number for albumin (S), compared against a standardized reference sample. To
ensure measurement consistency and accuracy, duplicate samples were assayed using
the average of duplicates taken for final analysis per individual. Analytical
precision was maintained by calculating mean T/S ratio values and identifying
outliers by marking the highest and lowest T/S ratios. Telomere length in base
pairs was converted using the following formula: kbp = 3274 + 2413
In this research, CVD encompasses a range of conditions, including coronary heart disease, myocardial infarction, angina pectoris, heart failure, stroke, and hypertension. These diseases were identified based on participant responses to specific questions in the NHANES questionnaires. Participants were queried with the following questions: “Have you ever been told that you had a heart attack (myocardial infarction), angina pectoris, coronary heart disease, stroke, heart failure, or hypertension?” Additionally, they were asked whether they had been advised to take prescribed medication for hypertension. Affirmative responses to these questions were used as criteria to classify participants as having CVD.
All-cause mortality was the primary outcome, while CVD-specific mortality was designated as the secondary outcome. Individual death statuses were obtained from the NDI database, with causes of death recorded using the International Classification of Diseases, Tenth Revision (ICD-10) [29]. Within the NDI database, the ‘MORTSTAT’ variable records the final determination of vital status, and participants coded as ‘1’ under final mortality status were considered deceased. CVD-specific death was defined as deaths resulting from heart disease (ICD codes 054-064) or cerebrovascular disease (ICD codes 070) [30]. All other causes of death were classified as non-cardiovascular.
Covariates, including demographic characteristics, anthropometric measures, lifestyle factors, and medical history, were incorporated to reduce potential bias in the study [21].
Demographic information was gathered from the NHANES questionnaire, including continuous data on age and categorical data on sex (male or female), ethnicity, and educational level. Anthropometric variables included body mass index (BMI) and waist circumference. Assessed lifestyle variables included smoking status, determined by whether participants had smoked more than 100 cigarettes during their lifetime, and alcohol consumption, defined as consuming at least 12 alcoholic drinks every year. Medical comorbidities and biomarkers, such as triglycerides and diabetes, were also collected. Diabetes was defined according to the positive response to this question: “Has a doctor ever told you that you have diabetes?”
We first imputed missing covariates via multivariate imputation to enhance
statistical robustness [31, 32]. Normally distributed continuous variables were
presented as mean
The relationship between the LTL and overall survival was examined using the Kaplan–Meier curve for telomere length tertiles, with the Bonferroni–Holm method applied for survival comparison adjustments among groups [33, 34]. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated by weighted Cox regression, both unadjusted and adjusted for potential confounders. LTL was both analyzed as a continuous variable and categorized into tertiles to explore its association with all-cause mortality. Model 1 was unadjusted. Model 2 was adjusted for age, sex, ethnicity, and education. Model 3 additionally considered BMI, waist circumference, triglycerides, diabetes, smoking status, and alcohol consumption alongside the Model 2 variables [30, 35]. Additionally, we utilized a weighted restricted cubic spline (RCS) with 4 knots to illustrate the correlation between LTL and all-cause death. We also performed subgroup analyses based on Cox regression, including age, gender, and diabetes.
It is important to note that Cox regression accounts for no competing risks,
which could potentially lead to overestimation of absolute risks for
cause-specific death. We used the Fine–Gray competitive risk regression to
accurately assess the risk of LTL-related CVD-specific death, considering
non-cardiovascular death as a competing outcome [36, 37]. Statistical analyses
were conducted using R software (version 3.6.1, R Foundation for Statistical
Computing, Vienna, Austria), with significance established at p
The average age was 59.0 years, and 50.2% of participants were males. After a median follow-up of 13.9 years, 31.0% were noted as deceased. Table 1 summarizes the demographic characteristics, anthropometric measures, behavioral factors, medical history, and plasm biomarkers of the participants, categorized by LTL tertiles.
| T1 (N = 528) | T2 (N = 527) | T3 (N = 544) | p | ||
| Leukocyte telomere length (kbp) | 5.1 (4.9, 5.3) | 5.6 (5.5, 5.7) | 6.2 (6.0, 6.6) | ||
| Age (years) | 65.0 (54.0, 72.0) | 60.0 (47.0, 66.0) | 52.0 (42.0, 63.0) | ||
| Gender (male, n, %) | 288 (54.5%) | 264 (50.1%) | 251 (46.1%) | 0.023 | |
| Race (n, %) | |||||
| Non-Hispanic White | 277 (52.5%) | 240 (45.5%) | 228 (41.9%) | ||
| Non-Hispanic Black | 116 (22.0%) | 117 (22.2%) | 181 (33.3%) | ||
| Mexican American | 103 (19.5%) | 123 (23.3%) | 88 (16.2%) | ||
| Other Hispanic | 21 (4.0%) | 27 (5.1%) | 31 (5.7%) | ||
| Other races | 11 (2.1%) | 20 (3.8%) | 16 (2.9%) | ||
| Education (n, %) | 0.098 | ||||
| Below high school | 229 (43.4%) | 213 (40.4%) | 192 (35.3%) | ||
| High school | 119 (22.5%) | 120 (22.8%) | 142 (26.1%) | ||
| Above high school | 180 (34.1%) | 194 (36.8%) | 210 (38.6%) | ||
| BMI (kg/m2) | 29.5 (26.1, 34.1) | 29.6 (26.4, 33.9) | 29.9 (26.1, 34.5) | 0.866 | |
| Waist circumference (cm) | 102.8 (93.6, 114.4) | 104.0 (94.5, 112.2) | 102.5 (92.8, 111.6) | 0.401 | |
| All-cause mortality (Yes, n, %) | 234 (44.3%) | 137 (26.0%) | 125 (23.0%) | ||
| Triglycerides (mg/dL) | 136.5 (96.0, 191.0) | 137.0 (97.0, 201.0) | 128.0 (87.8, 185.0) | 0.106 | |
| Diabetes (Yes, n, %) | 105 (19.9%) | 95 (18.0%) | 94 (17.3%) | 0.527 | |
| Smoking (Yes, n, %) | 284 (53.8%) | 286 (54.3%) | 268 (49.3%) | 0.193 | |
| Drinking (Yes, n, %) | 99 (18.8%) | 93 (17.6%) | 108 (19.9%) | 0.652 | |
| HF (Yes, n, %) | 54 (10.2%) | 33 (6.3%) | 32 (5.9%) | 0.011 | |
| CAD (Yes, n, %) | 77 (14.6%) | 43 (8.2%) | 43 (7.9%) | ||
| Stroke (Yes, n, %) | 46 (8.7%) | 46 (8.7%) | 32 (5.9%) | 0.133 | |
| Angina pectoris (Yes, n, %) | 77 (14.6%) | 41 (7.8%) | 40 (7.4%) | ||
| Heart attack (Yes, n, %) | 89 (16.9%) | 45 (8.5%) | 48 (8.8%) | ||
| Hypertension (Yes, n, %) | 463 (87.7%) | 486 (92.2%) | 515 (94.7%) | ||
T1, 4.21–5.37 kbp; T2, 5.37–5.85 kbp; T3, 5.85–8.98 kbp. BMI, body mass index; HF, heart failure; CAD, coronary artery disease.
There is a significant difference across the tertiles (T1–T3) in age, race,
gender, and prevalence of CVD (p
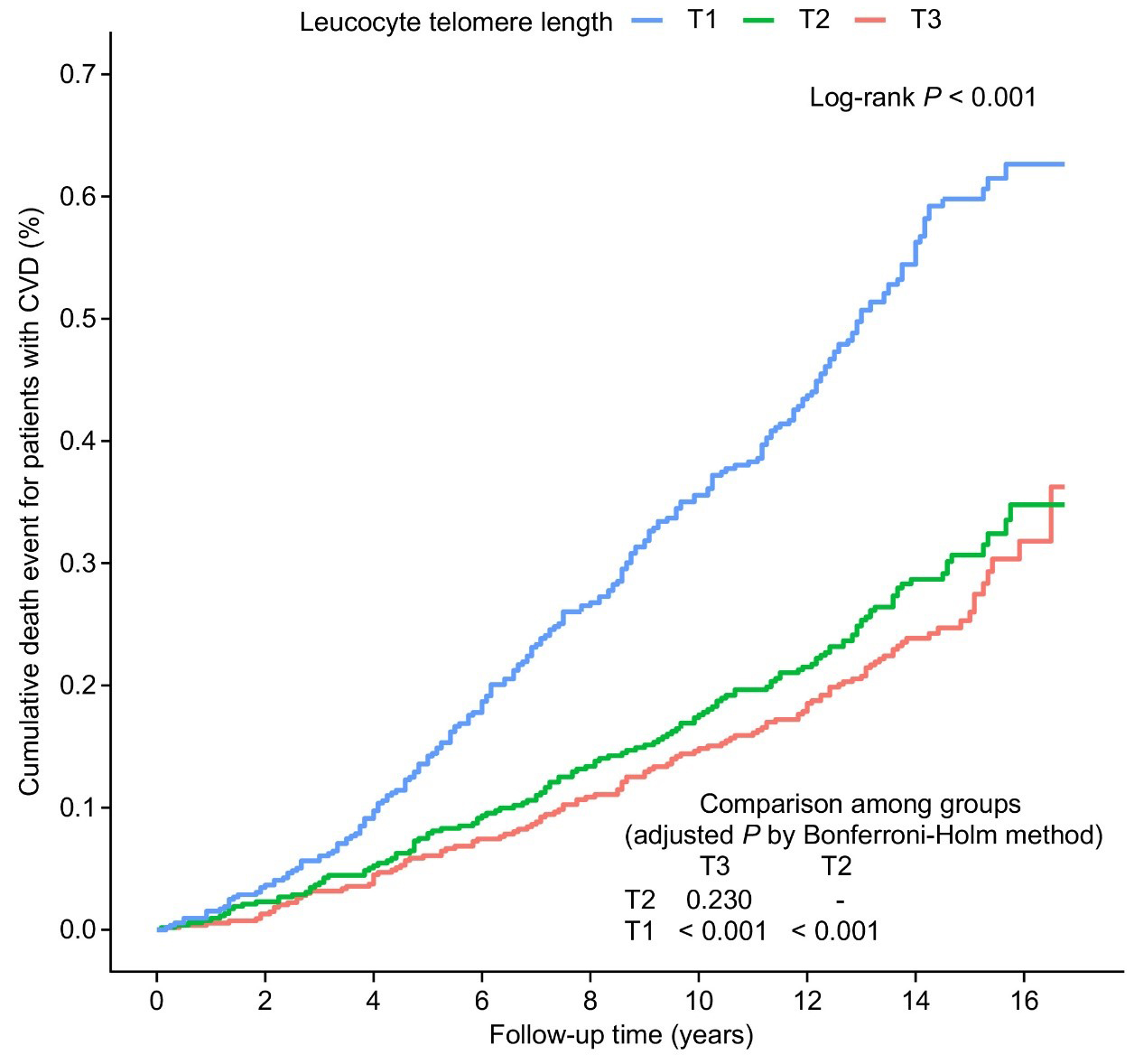
Kaplan–Meier curve analysis revealed significant differences in all-cause
mortality among the LTL tertiles (log-rank p
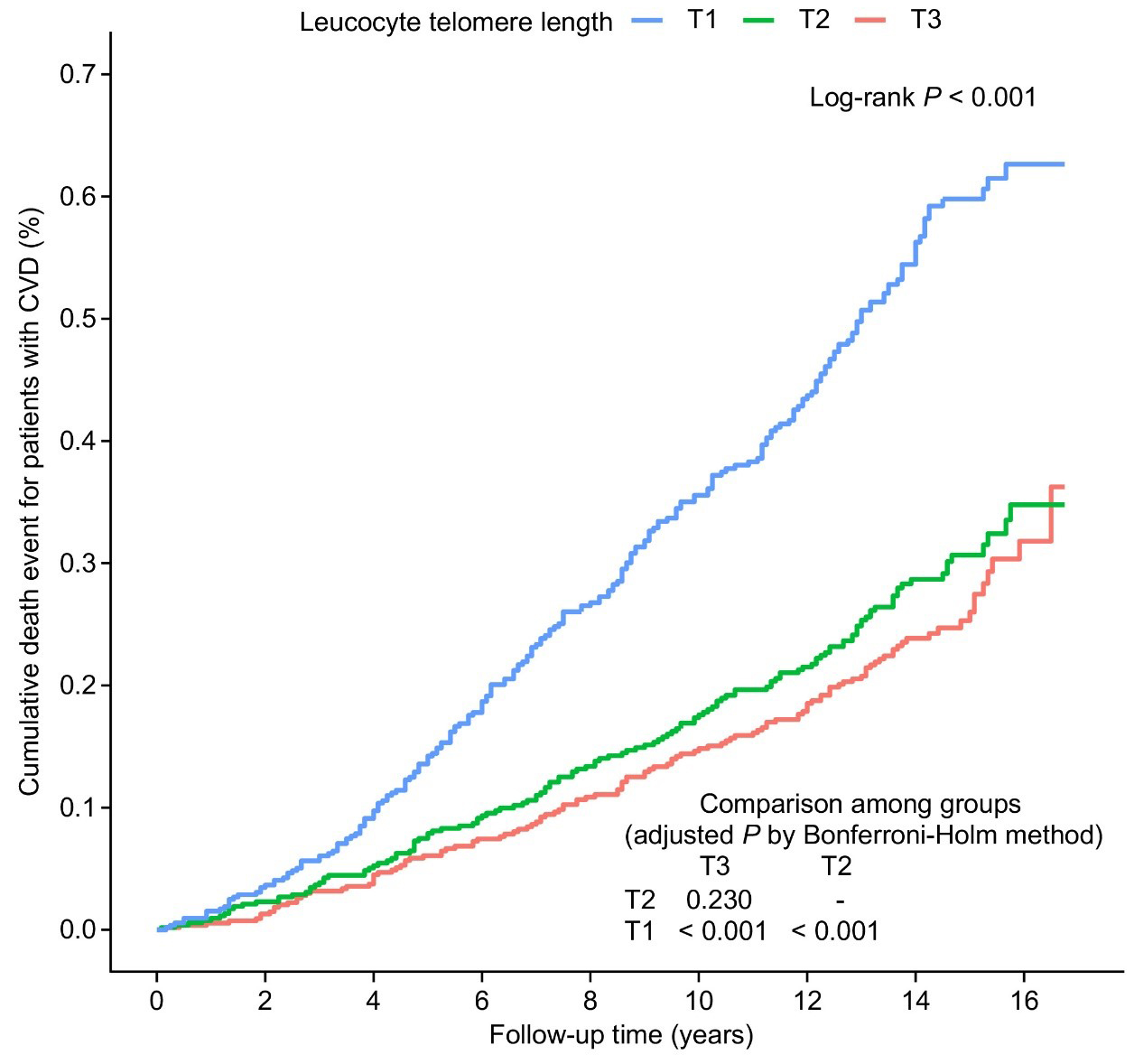 Fig. 2.
Fig. 2.
Kaplan–Meier curves by LTL tertiles in patients with CVD. The
LTL tertiles, based on the entire CVD patient cohort, are T1 (
LTL significantly correlates with all-cause mortality across all models (Table 2). Specifically, HRs with 95% CIs were 2.00 (1.68–2.37) for Model 1, 1.27 (1.07–1.51) for Model 2, and 1.25 (1.05–1.48) for Model 3. In the categorical analysis (non-adjusted, Model 2, and Model 3), an increased risk of all-cause death was observed with decreasing LTL categories. In Model 3, participants in the lowest LTL tertile (T1) showed a 1.29-fold increased risk of death than the highest tertile (T3). However, we observed no significant difference in death risk between the middle tertile (T2) and the highest tertile (T3) (p = 0.196).
| Model 1 | Model 2 | Model 3 | |||||
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | ||
| LTL (per 1 kbp decrease) | 2.00 (1.68, 2.37) | 1.27 (1.07, 1.51) | 0.007 | 1.25 (1.05, 1.48) | 0.011 | ||
| Categories | |||||||
| T3 ( |
Reference | Reference | Reference | ||||
| T2 (5.37–5.85 kbp) | 1.16 (0.91, 1.48) | 0.232 | 0.87 (0.68, 1.11) | 0.259 | 0.85 (0.66, 1.09) | 0.196 | |
| T1 ( |
2.24 (1.80, 2.78) | 1.30 (1.04, 1.63) | 0.023 | 1.29 (1.03, 1.62) | 0.028 | ||
HR, hazard ratio; LTL, leucocyte telomere length; CI, confidence interval; T1, tertile 1; T2, tertile 2; T3, tertile 3.
The dose-response association of LTL with all-cause death was further explored using RCSs, with the median LTL serving as the reference point. As illustrated in Supplementary Fig. 1, all-cause death was elevated with decreasing LTLs after adjusting for covariates such as age, sex, race, and educational attainment.
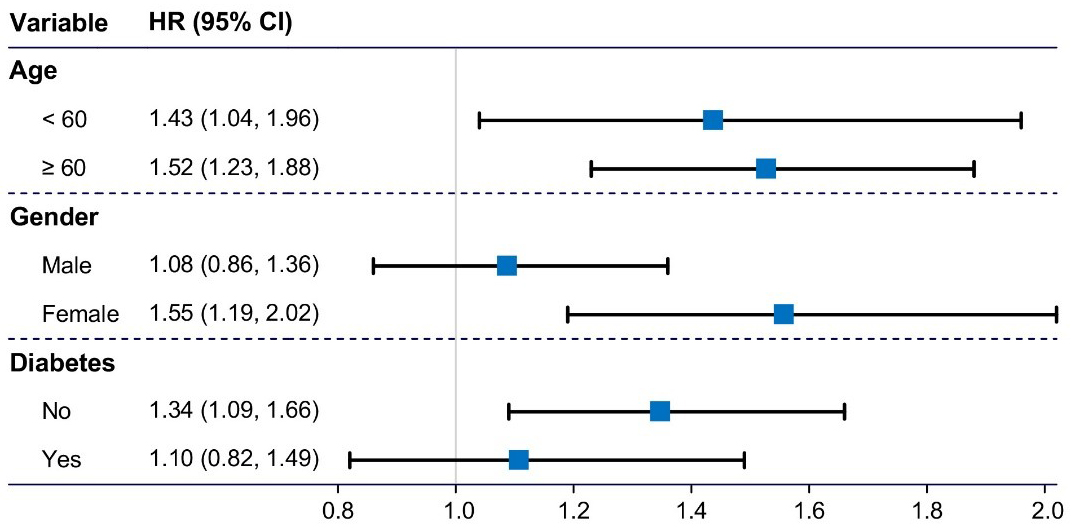
As shown in Fig. 3, the association between LTL and all-cause death remained
robust regardless of age (
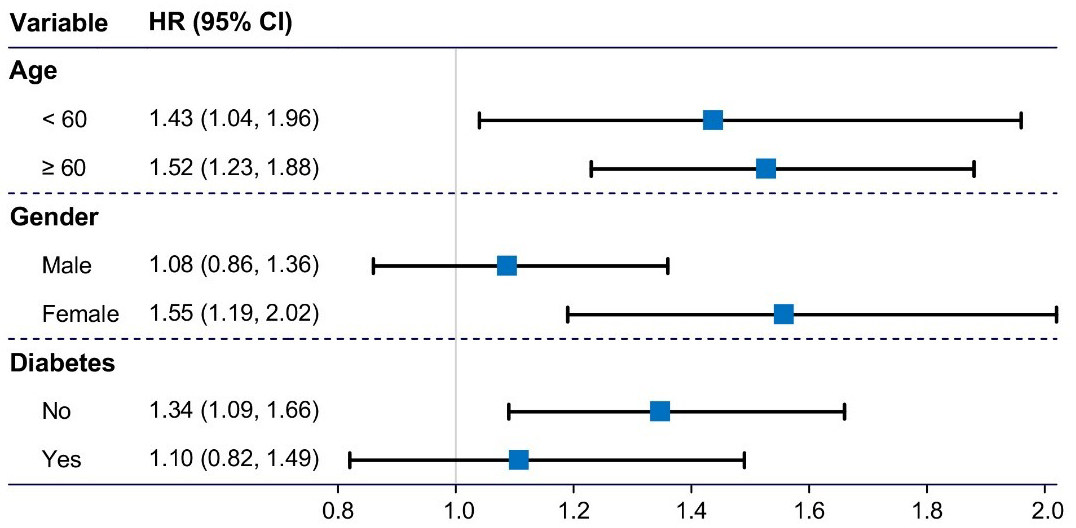 Fig. 3.
Fig. 3.
Subgroup analysis on the associations of LTL with all-cause death across age, gender, or diabetes. The associations were adjusted for age, race, education, body mass index, waist circumference, triglycerides, diabetes, and smoking and drinking statuses. The related covariate was removed from the model when the group was divided based on this covariate. HR, hazard ratio; CI, confidence interval; LTL, leucocyte telomere length.
| HR (95% CI) | p | |||
| Male | ||||
| LTL (per 1 kbp decrease) | 0.90 (0.61, 1.32) | 0.591 | ||
| Categories | ||||
| T3 ( |
Reference | |||
| T2 (5.37–5.85 kbp) | 0.64 (0.40, 1.00) | 0.051 | ||
| T1 ( |
0.94 (0.66, 1.34) | 0.722 | ||
| Female | ||||
| LTL (per 1 kbp decrease) | 1.79 (1.29, 2.48) | |||
| Categories | ||||
| T3 ( |
Reference | |||
| T2 (5.37–5.85 kbp) | 0.78 (0.57, 1.07) | 0.917 | ||
| T1 ( |
1.28 (0.94, 1.74) | 0.004 | ||
We adjusted for age, race/ethnicity, education level, body mass index, waist circumference, triglycerides, diabetes, and smoking and drinking statuses.
Abbreviations: HR, hazard ratio; CI, confidence interval; LTL, leucocyte telomere length.
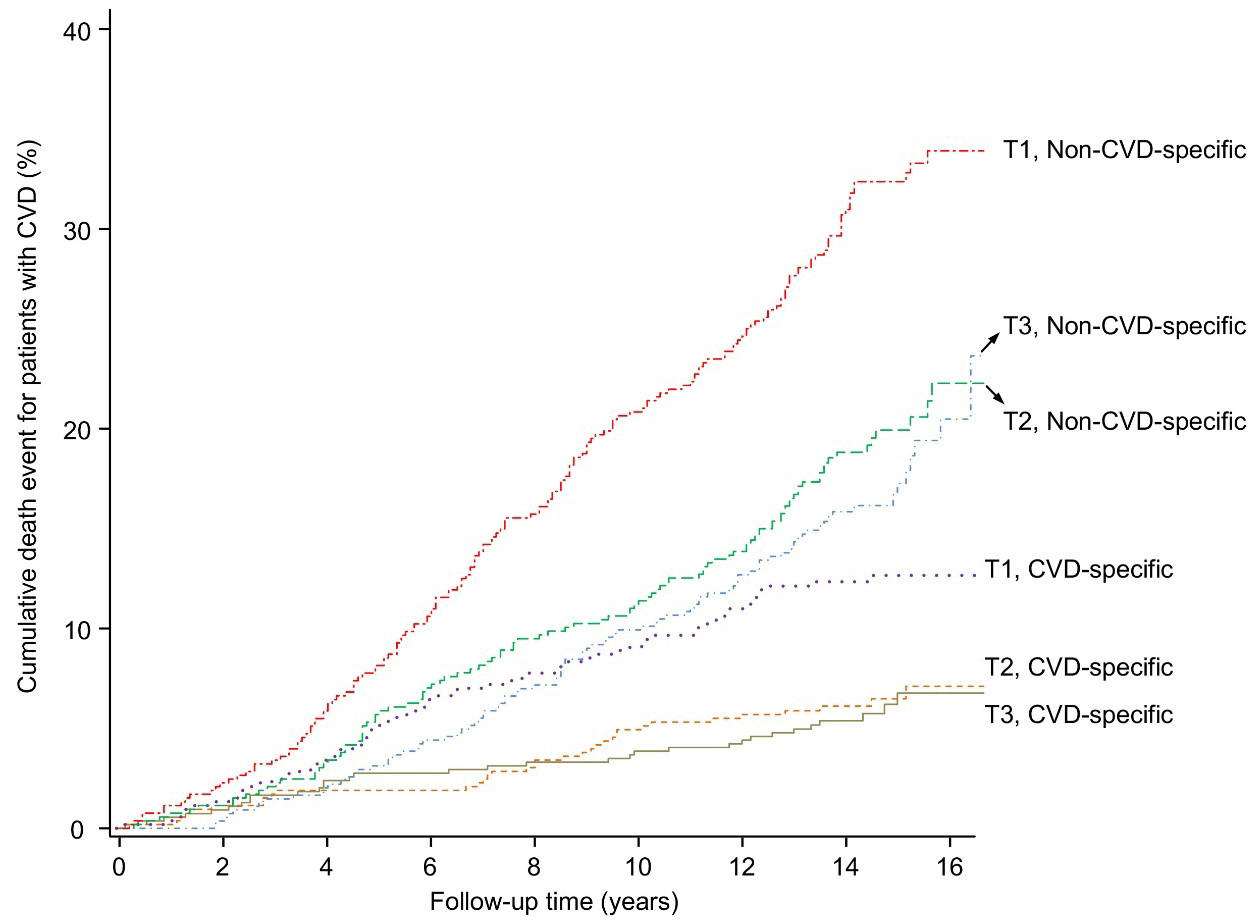
The cumulative incidence of cause-specific death in the LTL tertiles is shown in Fig. 4.
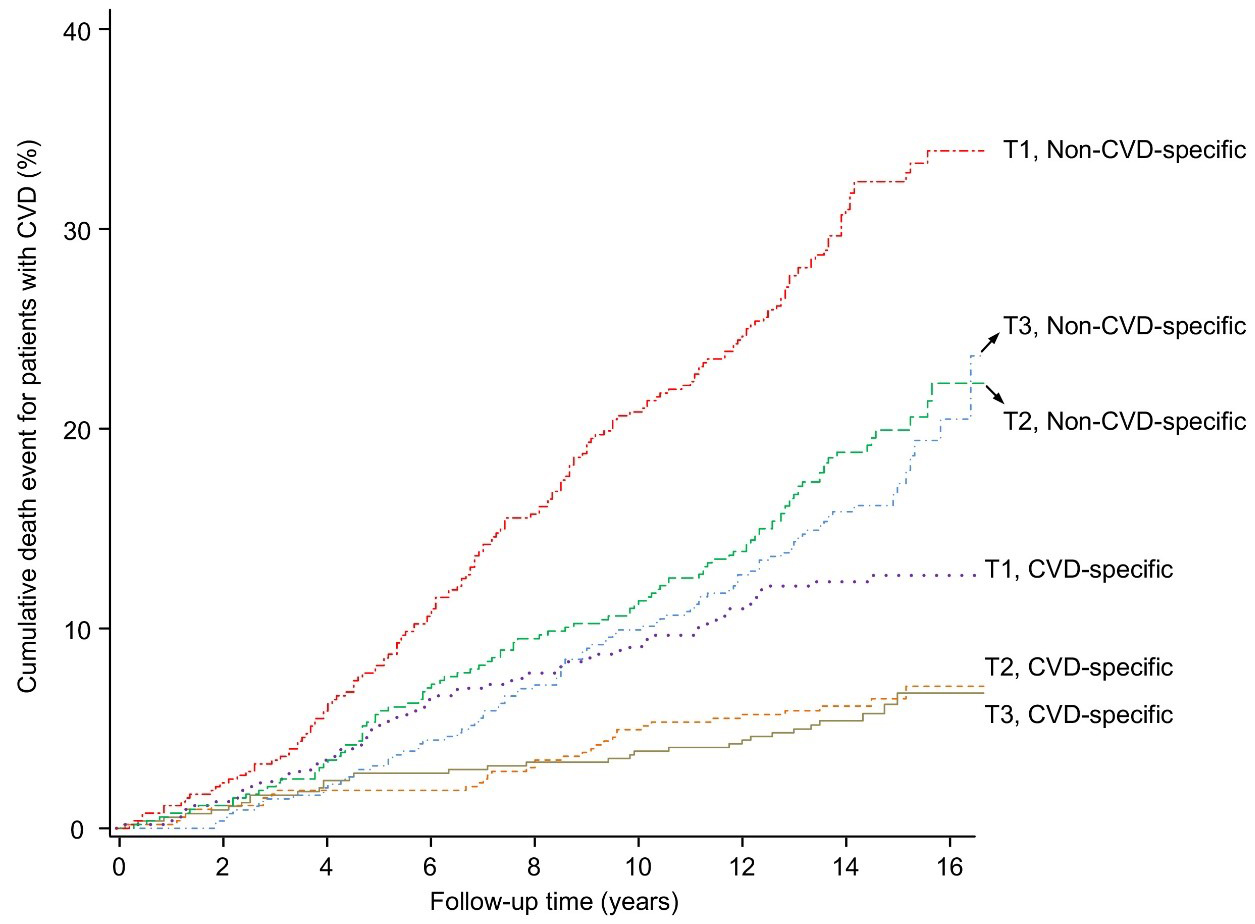 Fig. 4.
Fig. 4.
Cumulative incidence of cause-specific death in LTL tertiles.
Cumulative incidence of both CVD-specific and non-CVD-specific mortality across
different LTL tertiles in CVD patients. The LTL tertiles, based on the entire CVD
patient cohort, are T1 (
After integrating LTL into the Fine–Gray competing risk model, we initially observed a significant association between LTL and both cardiovascular and non-cardiovascular mortality. Specifically, for cardiovascular death, the HR was 2.01 with a 95% CI of 1.37–2.93; for non-cardiovascular death, the HR was 1.84 (95% CI, 1.51–2.24), without adjusting for covariates.
However, after adjusting for covariates, the association between LTL and CVD-specific mortality was no longer significant (adjusted HR, 1.21; 95% CI, 0.85–1.74). In contrast, the association between LTL and non-CVD death remained statistically significant even after adjustments, with an adjusted HR of 1.24 (95% CI, 1.02–1.51).
Telomeres shorten with each cell division, eventually becoming critically short and fragile after numerous divisions [3, 38]. LTL serves as a biomarker, indicative of the overall telomere length in an organism. CVD encompasses a spectrum of heart and blood vessel disorders, including hypertension, atherosclerosis, myocardial infarction, and so forth [11], and it remains a major cause of mortality from non-communicable diseases [39].
In our investigation, which included 1599 CVD patients from the
1999 to 2002 NHANES, we examined the relationship between LTL and the prognosis
of CVD. Notably, individuals in the low LTL group displayed an increased
all-cause death than those in the high LTL group. Kaplan–Meier curve analyses
revealed a marked difference in all-cause mortality across LTL tertiles (log-rank
p
Numerous studies have examined the length of telomere and survival outcomes [19, 20, 40]. A recent meta-analysis involving 121,749 individuals found a short LTL correlated with increased all-cause mortality in the general population [22]. Schneider et al. [10] observed a similar association between shortened LTL and all-cause, circulatory, and respiratory mortality based on 472,432 participants from UK Biobank. Recently, Xiong et al. [23] observed increased all-cause and CVD-specific mortality in patients with metabolic syndrome who had shorter LTL. However, the specific association between LTL and mortality in patients with CVD needs to be clarified.
Our study corroborates these findings and extends them to individuals with CVD, demonstrating that shorter LTL is associated with higher all-cause mortality, even considering multiple demographic and clinical factors. The long follow-up of our study highlights the important role of LTL as a prognostic biomarker in clinical practice, particularly for identifying high-risk groups among CVD patients.
Interestingly, our findings regarding CVD-specific mortality align with several previous studies [41, 42, 43] in demonstrating no significant association between LTL and cardiovascular mortality risk. Mons et al. [41] reported no correlation between telomere length and CVD-specific death in 12,199 participants from two population-based prospective cohort studies. In contrast, Xiong et al. [23] revealed that LTL was independently associated with CVD-specific mortality. This discrepancy between studies may stem from several factors. It should be noted that oxidative stress plays a critical role in telomere shortening and potentially impacts our findings. Oxidative stress leads to oxidative DNA damage, including telomere attrition, which is a key factor in aging and the pathogenesis of various diseases, including CVD [14, 44]. However, our research adjusted for multiple covariates that influence oxidative stress (e.g., age, sex, race, BMI, and lifestyle), although other potential covariates remain to be considered. Second, there is a discrepancy in the research population. Xiong et al. [23] focused on individuals with metabolic syndrome, whereas our study population comprised patients with CVD. Third, previous analysis employed the Cox regression model to examine cause-specific mortality, which may not adequately account for biases introduced by competing outcomes, potentially leading to overestimating the risk of CVD-specific death [23]. Our study utilized the competing risk regression, which sets non-cardiovascular death as a competing event, potentially providing a more accurate assessment of cardiovascular mortality risk. These findings indicate the complexity of telomere biology and its implications for disease. Therefore, additional research is necessary to clarify the relationship between LTL and cause-specific mortality. This could involve more extensive studies with diverse populations and methodologies, ensuring a comprehensive understanding of how LTL influences mortality risks in various contexts of cardiovascular health.
Moreover, our research found that LTL is inversely related to all-cause death in female patients with CVD, which was not observed in males. Males and females often experience varying aging rates, leading to differences in life expectancy between genders [45]. Females possess, on average, longer telomeres and a higher life expectancy than males of equivalent age [9, 45]. In humans, males live shorter lives and experience more rapid telomere shortening, leading to speculation in medical research that gender-specific telomere reduction might be a contributing factor to the differences in gender-specific death [45]. However, Xiong et al. [23] did not observe consistent results, and gender variables in subgroup analyses did not significantly alter the association between telomere length and risk of all-cause or CVD-specific death. Apart from the difference in the study population, their neglect of weighted study design is another possible cause, potentially leading to a conclusion containing selection bias.
Despite the novel perspectives on LTL and the prognosis of CVD, the limitations of this study should be mentioned. Firstly, while comprehensive, focusing on a nationally representative sample from the United States does not account for variations in physical activity, dietary, genetic factors, and other potential covariates. Moreover, the generalizability of our conclusion to populations in different regions, such as China and Europe, still needs to be determined due to the lack of representative data from these areas. These limitations suggest that more research should be performed to validate and expand our findings, ideally incorporating more diverse and global populations and a broader range of covariates.
Our study demonstrates that telomere length is inversely related to all-cause mortality in individuals with CVD. This finding reveals that shorter LTL correlates with an elevated mortality risk from all causes. However, this relationship does not relate to CVD-specific mortality. The significant link between reduced LTL and all-cause death underlines the importance of considering telomere length as a biomarker in managing CVD. By identifying patients with shorter LTLs, healthcare providers can potentially implement more targeted interventions and monitoring strategies, aiming to improve overall outcomes and reduce mortality risks in individuals with CVD.
All the data used in this study were acquired from the NHANES survey (https://wwwn.cdc.gov/nchs/nhanes/Default.aspx).
JYS, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing — original draft, Writing — review & editing. QX, Formal analysis, Validation, Writing — review & editing. HS, Formal analysis, Methodology, Validation, Writing — original draft, Writing — review & editing. WH, Validation, Writing — review & editing. QQ, Methodology, Validation, Writing — original draft, Writing — review & editing. WS, Formal analysis, Investigation, Methodology, Project administration, Validation,Visualization, Supervision, Writing — original draft, Writing — review & editing. XQK, Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Supervision, Writing — original draft, Writing — review & editing. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This research has been conducted using the National Health and Nutrition Examination Survey (https://www.cdc.gov/nchs/nhanes/index.htm). The ethical approval number is Protocol #98-12. This research was approved by the Ethics Review Committee of the National Center and was performed following the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All participants gave written informed consent.
We sincerely acknowledge the US National Center for Health Statistics for conducting the survey.
This work was supported by the National Key Research and Development Program of China (2019YFA0210104).
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/j.rcm2509333.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.