



 , Yanjuan Lin 1,2,3,*
, Yanjuan Lin 1,2,3,*1 Department of Nursing, Union Hospital, Fujian Medical University, 350122 Fuzhou, Fujian, China
2 Department of Cardiovascular Surgery, Union Hospital, Fujian Medical University, 350122 Fuzhou, Fujian, China
3 Key Laboratory of Cardio-Thoracic Surgery (Fujian Medical University), Fujian Province University, 350122 Fuzhou, Fujian, China
Abstract
Background: This cross-sectional study explores postoperative kinesiophobia in patients with acute type A aortic dissection (AAAD), an understudied area. The occurrence of postoperative kinesiophobia and its relation to various factors were investigated. Methods: Patients diagnosed with AAAD and undergoing surgical treatment from January 2019 to December 2021 were selected through continuous sampling. Kinesiophobia levels were assessed using the Tampa Scale for Kinesiophobia Heart (TSK-SV-HEART). Univariate and multivariate regression analyses were employed to determine factors influencing kinesiophobia. Results: Out of 264 included patients, the mean postoperative kinesiophobia score was 38.15 (6.66), with a prevalence of 46.2%. Multivariate logistic regression revealed that education level, general self-efficacy, family care index, and facing style reduced kinesiophobia, while avoidance style and yielding style increased it. Conclusions: Postoperative kinesiophobia prevalence in AAAD patients is high and associated with diverse factors. Medical staff should remain vigilant to potential kinesiophobia during postoperative rehabilitation.
Keywords
- acute type A aortic dissection
- movement
- kinesiophobia
- influencing factor
Acute type A aortic dissection (AAAD) is a dangerous condition that usually presents with sudden and severe chest, back and abdominal pain wherein the typical initial symptoms are such that patients feel tearing or impending doom, and undergo shock in severe cases; the detection rate and number of cases have been increasing annually [1]. Advances in medical technology have improved the survival rate of patients with AAAD, and the 1-year survival rate was 94%, and the 2-year survival rate was 92.2% [2]. A database from the International Registry of Acute Aortic dissection (IRAD) [3] revealed that 54.9% of patients with type A dissection lacked physical activity after surgery, and the number showed a gradually increasing trend. Patients with AAAD are still at high risk of postoperative aortic lesions and related cardiovascular events, and their quality of life is lower than that of the normal population [4]. Studies have shown that over 50% of patients with AAAD experience new depression due to lack of physical activity, and more than one-third of patients have reported disability at work [4]. Studies have demonstrated that exercise is a key factor in cardiac rehabilitation (CR), and CR reduces cardiac mortality and risk of hospitalization [5], and improves oxygen uptake and mental health [6, 7]. A study on kinesiophobia in hospitalized patients with acute cardiovascular events also reported that 83% of patients had kinesiophobia [8], which reduced the CR attendance rate [9]. The European Society of Cardiology emphasizes that exercise at a safe level is feasible for patients with heart disease [10]. However, Pasadyn et al. [11] investigated 132 postoperative patients with AAAD and found that 36% did not participate in CR treatment, exhibiting low participation and compliance. Studies have shown that high levels of kinesiophobia are associated with a decline in health-related quality of life, muscle strength and physical activity levels [12].
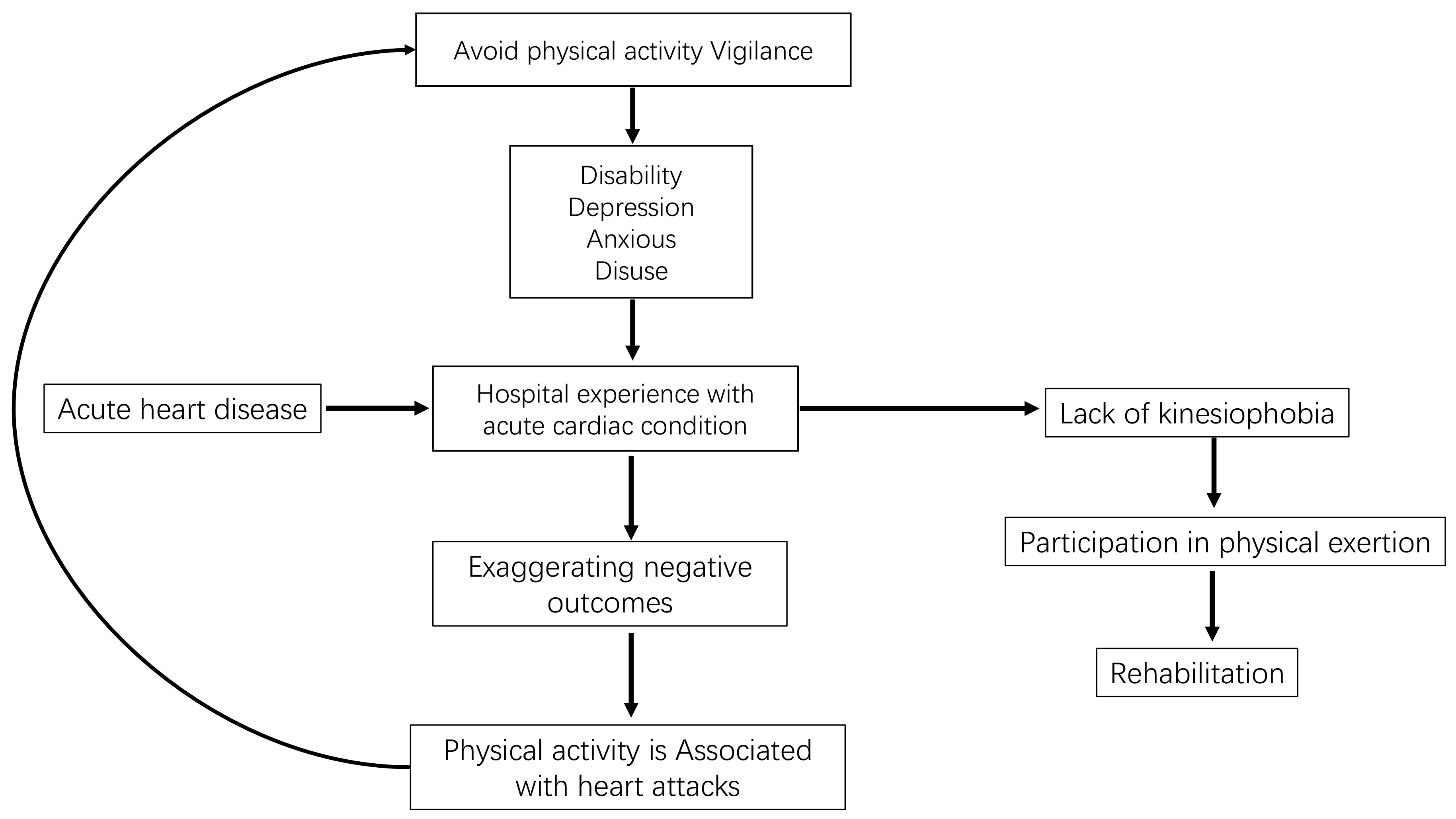
Kinesiophobia was originally proposed by Kori et al. [13] and refers to an “excessive, unreasonable and debilitating fear of movement and activity”. Sports phobia has been shown to have an important negative impact on the outcome of rehabilitation, so it is important to study its clinical occurrence [14, 15]. Fear and associated avoidance behavior are typical psychological responses in the early stages after an acute cardiovascular event. Avoidance, as a form of self-protection, can reduce the possibility of adverse reactions caused by stressful events in the short term, while excessive fear of injury may lead to ineffective coping strategies [16]. Based on clinical experience, some AAAD patients may be concerned about the adverse consequences of physical activity after surgery, leading to re-dissection of the aorta, or may be concerned about other complications caused by exercise. Such fears cause patients to be highly vigilant in avoiding exercise that leads, in the long term, to adverse outcomes such as muscle disuse, disability, anxiety and depression. In turn, these physical and psychological symptoms will aggravate the individual’s fear experience of exercise, thus forming a vicious cycle (avoidance strategy), as shown in Fig. 1 (Ref. [16]).
According to the theory of stress process [17], stressors can act on individuals through mediating effects such as family support, coping style and personality characteristics, thus leading to different physiological, psychological and behavioral responses and further affecting the health or disease of individuals. The painful experience caused by symptoms of AAAD is the most common stressor for AAAD patients. Therefore, this study aims to investigate the current situation of exercise fear and related influencing factors of AAAD patients under the guidance of the theory of stress process, so as to provide theoretical reference for improving exercise fear, exercise endurance and disease prognosis of AAAD patients.
A continuous sampling method was used to identify patients who were first
diagnosed with type A aortic dissection in our hospital from January 2019 to
December 2021 and successfully implanted with ascending aorta and semi-arch
replacement combined with improved three-stent implantation [18]. The surgical
details of modified three-branch stenting (MTBSG) have been described in detail
before [18], which simply involves the use of modified three-branch stenting to
reconstruct the aortic arch, brachiocephalic artery, left common carotid artery,
left subclavian artery, and descending aorta. A professional investigator called
the patient and informed them of the study. If the patient agreed to participate
in the study, a review was scheduled and the relevant questionnaires and tests
were completed. Inclusion criteria: ① Age
The study was approved by the Ethics Committee of Fujian Medical University Affiliated Union Hospital ([2020] Union Hospital Ethics Review No. 080) and conducted in accordance with the Declaration of Helsinki. We also received written informed consent from subjects or their legal counsels before research commencement.
Sociodemographic and clinical data, including age, sex, marital status, intraoperative conditions and underlying diseases, retrieved from hospital databases. Other data were collected on site, such as education status, living habits, occupational status, regular exercise habits, medical coping style scale, family care index scale, etc. Two trained investigators conducted a questionnaire survey one-on-one. In the questionnaire, the patients made their choices independently, and the researchers accurately recorded each answer. When the patients were unable to fill in the questionnaire by themselves due to factors such as education level, the researchers explained the items for the patients and filled in the questionnaire, and timely remedied the problems such as lack of data filling.
To ensure data collection accuracy, the data collectors were the same members of the research team. On the day of follow-up, one investigator explained the purpose and use of the grip strength test and pedometer to the patients, and two other investigators performed the grip strength test and pedometer correction. Data from grip strength tests were collected during the visit and patients were told to wear pedometers for seven days, after which pedometer data was collected.
Based on the purpose of the study, through literature research, and expert consultation, a general information questionnaire was prepared for the investigation, including items regarding demographic data, disease history, and hospitalization related medical information.
The TSK-SV-Heart was adapted by Bäck et al. [12] from Sweden based
on the Exercise fear Scale (Tampa Scale for Kinesiophobia, TSK) for chronic pain
patients, and its Cronbach’s
Grip strength is a good indicator of an individual’s overall muscle strength
[19]. In this study, a uniform hand-held grip strength device (Olli 2.26,
specification: 15
Walking is one of the most basic, simple and popular physical activities [20]. In this study, a step-counting App was downloaded on the smartphone of each participant. The accuracy of the pedometer was verified in advance to reduce measurement errors. The average number of steps per day = the sum of steps per week/7.
When patients were admitted to hospital, they were instructed to use the numerical rating scale (NRS) to assess their pain [21]. The NRS scoring method divides a straight line into 10 segments, with 0 indicating no pain and 10 indicating severe pain. Patients choose a number to represent their degree of pain according to their own feelings, with 1–3 indicating mild pain, 4–6 indicating moderate pain and 7–10 indicating severe pain.
Designed by Smilkstein [22], its Cronbach’s
The MCMQ, designed by Feifel et al. [23], is used to judge the characteristics of coping strategies selected by patients in the face of diseases. There were 20 items in the scale, and the total score was 60, including 3 dimensions, namely, facing, avoidance and yielding. The Likert 4 grading method was adopted. Among the 20 items, items 1, 4, 9, 10, 12, 13, 18 and 19 were scored backwards, and the remaining items were scored forward. The reliability of face, avoidance and yield were 0.69, 0.6 and 0.76, respectively.
The GSES was compiled by Schwarzer et al. [24] and translated and
revised by Wang et al. [25]. The Chinese version of the General
Self-efficacy Scale is used to measure the self-efficacy of subjects. Cronbach’s
SPSS 26.0 statistical software (SPSS 26.0: SPSS; Chicago, IL, USA) was used for
statistical analysis of the data. The counting data were described using
frequency and percentage, and the measurement data were described by mean
Among the 312 patients post-AAAD, 280 fulfilled the inclusion criteria
(89.74%), 264 questionnaires were filled out validly (84.6%) (Fig. 2), and the
average age of patients was 53.33+/–11.85 years. The investigation showed that
122 patients had kinesiophobia, with a prevalence of kinesiophobia post-AAAD of
46.2%, the mean score of postoperative kinesiophobia was 38.15 (6.66) (Fig. 3).
Physical activity measurement 6 months after surgery revealed that the pedometer
results of patients with kinesiophobia 4275.37 (1067.11)/day were significantly
different from those of patients without kinesiophobia 5665.52 (1660.42)/day
(p
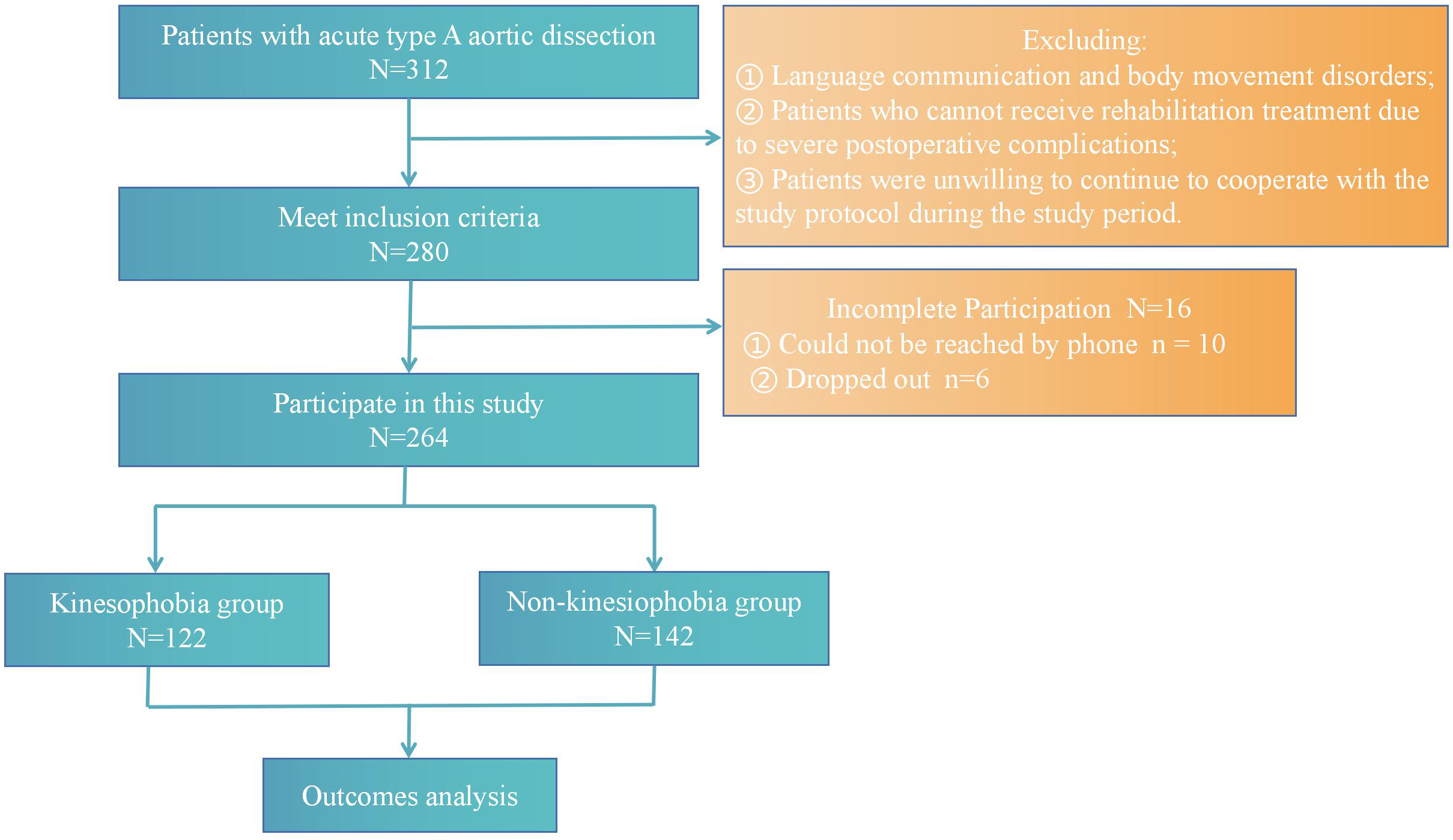 Fig. 2.
Fig. 2.
Flow diagram of the screening and enrollment of study patients.
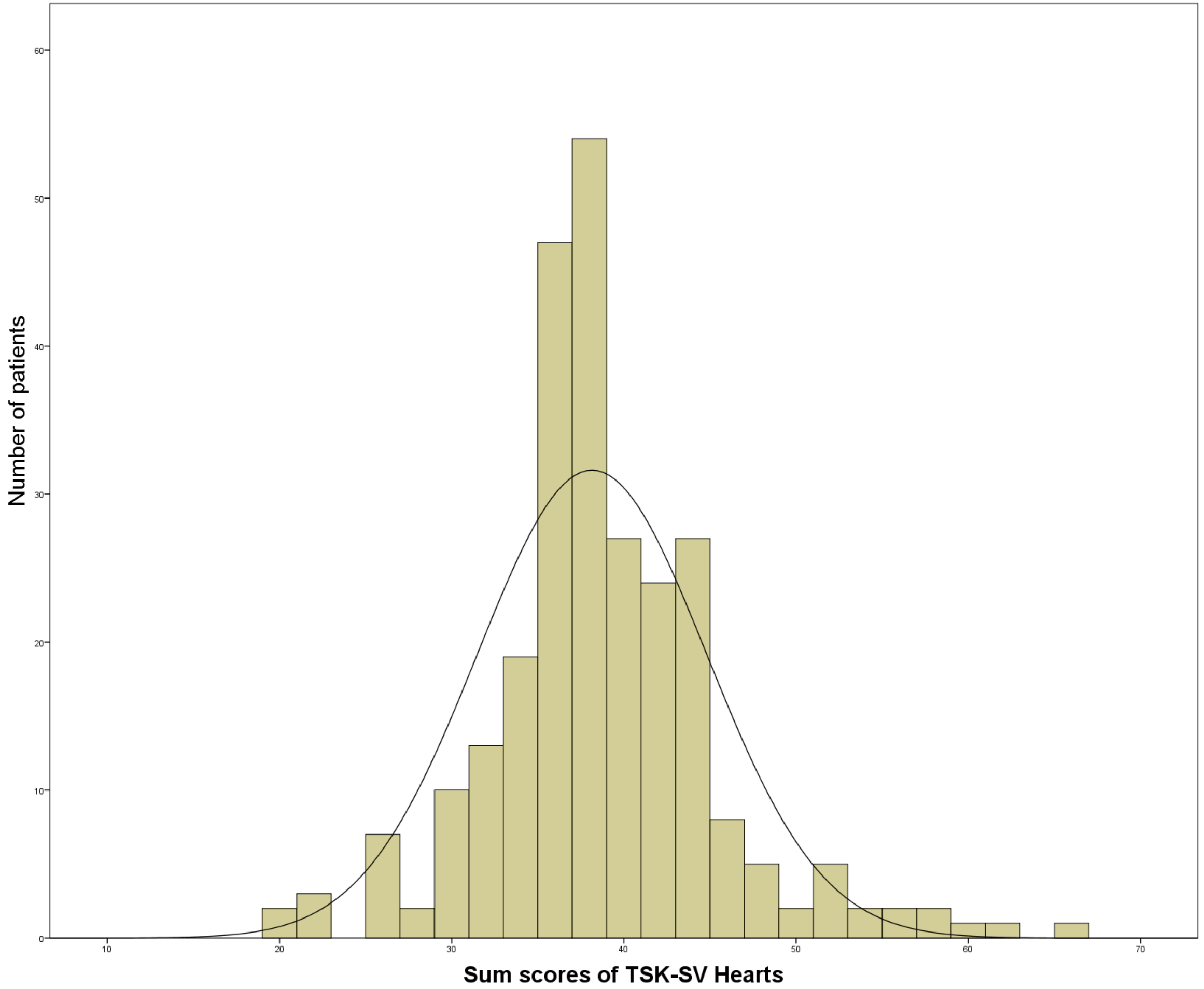 Fig. 3.
Fig. 3.
Frequency distribution of sum scores (17–68 points) of Tampa Scale for Kinesiophobia (TSK-SV) heart in patients with acute type A aortic dissection (AAAD) (N = 264).
| Variable | Kinesiophobia (n = 122) | Non-kinesiophobia (n = 142) | p value | |
| Age ( |
48 (39.3) | 32 (22.5) | 0.003 | |
| Gender (Male), n (%) | 95 (77.9) | 117 (82.4) | 0.36 | |
| BMI (kg/m2) ( |
69 (56.6) | 66 (46.5) | 0.10 | |
| Marital status (Married), n (%) | 112 (93.3) | 134 (94.4) | 0.41 | |
| Education levels (Middle school or under), n (%) | 47 (38.5) | 87 (61.3) | ||
| Medical insurance Payment Method (Self-supporting), n (%) | 12 (9.8) | 10 (7.0) | 0.21 | |
| Residence (Rural), n (%) | 71 (58.2) | 75 (52.8) | 0.38 | |
| Current smoking, n (%) | 19 (15.6) | 19 (13.4) | 0.61 | |
| Current drinking, n (%) | 29 (23.8) | 40 (28.2) | 0.42 | |
| Pain, n (%) | 107 (87.7) | 125 (88.0) | 0.94 | |
| NRS score (SD) | 7.76 (3.13) | 7.98 (3.18) | 0.58 | |
| Steps/day (pedometer) (SD) | 4275.37 (1067.1) | 5665.52 (1660.4) | ||
| Grip strength test | ||||
| Left hand grip strength test (kg) (SD) | 29.80 (6.6) | 32.54 (7.3) | 0.002 | |
| Right hand grip strength test (kg) (SD) | 31.84 (8.6) | 35.46 (8.6) | 0.001 | |
| Occupational status | ||||
| Preoperative physical labor | 51 (51.5) | 48 (48.5) | 0.566 | |
| Postoperative physical labor | 33 (42.9) | 44 (57.1) | 0.483 | |
| Exercise habits | ||||
| Regular exercise before surgery | 22 (50.0) | 22 (50.0) | 0.581 | |
| Regular exercise after surgery | 28 (53.8) | 24 (46.2) | 0.218 | |
| Diabetes mellitus, n (%) | 6 (4.9) | 10 (7.0) | 0.47 | |
| Hypertension, n (%) | 84 (68.9) | 94 (66.2) | 0.65 | |
| Hyperlipidemia, n (%) | 17 (13.9) | 10 (7.0) | 0.07 | |
| Marfan syndrome, n (%) | 2 (1.64) | 5 (3.5) | 0.34 | |
| Heart failure, n (%) | 3 (1.1) | 2 (1.4) | 0.53 | |
| Hemoglobin (g/L) (SD) | 127.10 (13.8) | 125.46 (15.4) | 0.37 | |
| EF (%) (SD) | 61.9 (6.1) | 61.99 (7.5) | 0.89 | |
| MCMQ | ||||
| Facing | 19.2 (2.5) | 22.4 (3.3) | ||
| Avoidance | 19.5 (2.4) | 16.3 (2.7) | ||
| Yielding | 11.9 (2.2) | 9.5 (1.8) | ||
| APGAR | 6.4 (1.1) | 7.9 (1.3) | ||
| GSES | 22.1 (3.1) | 24.2 (4.2) | ||
BMI, body mass index; NRS, numerical rating scale; EF, left ventricular ejection fraction; MCMQ, Medical Coping Modes Questionnaire; APGAR, adaptation, partnership, growth, affection and resolve, family care index scale; GSES, general self-efficacy scale; SD, standard deviation. Continuous normally distributed variables were expressed as mean (standard deviation) and categorical data are given as the counts and percentage (n, %).
Although most patients still had residual abdominal aortic dissection, no
significant abdominal aortic enlargement was observed compared to preoperative
findings. The prevalence of cerebral complications was low due to the short time
of circulatory stop and low-flow cerebral perfusion, with 10 cases of temporary
neurological dysfunction (3.8%). Other basic characteristics and
surgical data are shown in Tables 1,2. There was no significant
difference in medical variables between the two groups (p
| Valuables | Kinesiophobia (n = 122) | Non-kinesiophobia (n = 142) | p value | |
| Surgical data | ||||
| ICU treatment days (SD) | 3.6 (1.34) | 3.88 (1.64) | 0.14 | |
| Intraoperative time | ||||
| Operative time (min) (SD) | 304.5 (56.8) | 308.2 (51.9) | 0.58 | |
| Cardiopulmonary bypass time (min) (SD) | 148.4 (31.6) | 146.5 (37.1) | 0.66 | |
| Aortic clamp time (min) (SD) | 55.1 (16.7) | 54.3 (15.9) | 0.69 | |
| Low flow cerebral perfusion time (min) (SD) | 16.7 (4.3) | 16.4 (5.9) | 0.64 | |
| Concomitant arotic root procedure | ||||
| Bentall (%) | 22 (18.0) | 29 (20.4) | 0.62 | |
| Aortic valve replacement (%) | 2 (1.6) | 3 (2.1) | 0.86 | |
| Coronary artery bypass surgery (%) | 9 (7.4) | 11 (7.7) | 0.91 | |
| David (%) | 3 (2.5) | 4 (2.8) | 0.83 | |
| Valsalva sinus forming (%) | 25 (20.5) | 28 (19.7) | 0.88 | |
| Temporary neurologic dysfunction (%) | 3 (2.5) | 7 (4.9) | 0.30 | |
| Last Follow-Up data | ||||
| EF (%) (SD) | 62.01 (7.75) | 63.23 (6.20) | 0.16 | |
| Aortic insufficiency (yes), n (%) | 1 (0.8) | 3 (2.1) | 0.39 | |
| False lumen thrombus (yes), n (%) | 116 (95.1) | 138 (97.2) | 0.37 | |
EF, left ventricular ejection fraction; SD, standard deviation; ICU, intensive care unit. Continuous normally distributed variables were expressed as mean (standard deviation) and categorical data are given as the counts and percentage (n, %).
Descriptive results and the differences between high versus low levels of kinesiophobia for each variable are presented in Tables 1,2.
In order to facilitate the interpretation of the results in Table 1, the
relationships between kinesiophobia and AAAD variables were reported as
correlations. The Spearman correlation analysis results showed that there is a
correlation between postoperative APGAR (Adaptation, Partnership, Growth,
Affection and Resolve), MCMQ (Medical Coping Modes Questionnaire), GSES (General
Self-efficacy Scale), and kinesiophobia levels in AAAD patients. (p
| Variable | Score | R value | p value | |
| MCMQ | ||||
| Facing | 20.92 (3.36) | –0.43 | ||
| Avoidance | 17.76 (3.01) | 0.51 | ||
| Yielding | 10.60 (2.30) | 0.50 | ||
| APGAR | 7.2 (1.43) | –0.42 | ||
| GSES | 23.23 (3.85) | –0.25 | ||
MCMQ, Medical Coping Modes Questionnaire; APGAR, adaptation, partnership, growth, affection and resolve, family care index scale; GSES, general self-efficacy scale. Continuous normally distributed variables were expressed as mean (standard deviation).
Considering the existence of fear of motility as a dependent variable, the
related variables conforming to p
| Independent variables | B | S.E. | Wald | p | Exp (B) | Lower 95% CI for Exp (B) | Upper 95% CI for Exp (B) | |
| Age ( |
0.48 | 0.64 | 0.55 | 0.46 | 1.61 | 0.46 | 5.7 | |
| Hyperlipidemia | 0.20 | 2.10 | 0.01 | 0.92 | 1.22 | 0.02 | 69.3 | |
| Education levels (Middle school or under) | 1.38 | 0.58 | 5.62 | 0.02 | 3.97 | 1.27 | 12.39 | |
| Left hand grip strength test (kg) | 0.01 | 0.03 | 0.22 | 0.64 | 1.01 | 0.96 | 1.07 | |
| Right hand grip strength test (kg) | –0.02 | 0.03 | 0.43 | 0.51 | 0.98 | 0.93 | 1.03 | |
| Steps/day (pedometer) | –0.00 | 0.00 | 16.51 | 0.10 | 0.10 | 1.0 | ||
| APGAR | –1.30 | 0.29 | 20.03 | 0.27 | 0.16 | 0.48 | ||
| Facing | –0.37 | 0.11 | 12.66 | 0.70 | 0.56 | 0.85 | ||
| Avoidance | 0.50 | 0.11 | 19.75 | 1.65 | 1.32 | 2.05 | ||
| Yielding | 0.74 | 0.15 | 26.42 | 2.10 | 1.58 | 2.80 | ||
| GSES | –0.30 | 0.09 | 11.44 | 0.001 | 0.74 | 0.63 | 0.88 | |
Age:
The cross-sectional results of this study found that 46.2% of patients who survived AAAD exhibited varying degrees of kinesiophobia after successful surgery, with high levels of patients with kinesiophobia with lower education levels, negative coping styles, lower family care indices and generally lower self-efficacy were associated with postoperative kinesiophobia.
In our study, 46.2% of patients with AAAD suffered from kinesiophobia, which was higher than the results of Bäck et al. [12] on the prevalence of kinesiophobia in 332 patients with coronary heart disease (20%). The disparate results may be explained by the different nature of the disease. In the present study, 87.9% of the patients had severe pain at the time of disease onset, which easily resulted in traumatic fear memories. Many patients were unable to cope with their fear, leading to long-term avoidance of physical activities and exercise. According to relevant literature, even if surgical intervention is performed at an early stage, the mortality rate of recurrence and the prevalence of surgical complications are high [26]. Some patients avoid physical activity and exercise for fear of disease recurrence caused by activities. The specific psychological process of fear of exercise in patients with AAAD could be explored by qualitative studies in the future.
Patients with a fear of movement exhibited lower postoperative muscle strength
and physical activity compared with patients without kinesiophobia (p
Our results showed a significant difference between the two groups in terms of
self-reported activity (number of steps), p
Our study showed that general postoperative self-efficacy was negatively correlated with kinesiophobia in AAAD patients (Table 3). The results of multifactor logistic regression logic analysis showed that general self-efficacy was the influencing factor for the occurrence of kinesiophobia in postoperative AAAD patients. People with higher self-efficacy were more likely to start and continue activities conducive to recovery, while the opposite was true for people with lower self-efficacy [32]. Studies have shown that self-efficacy is positively correlated with long-term adherence to physical activity during post-discharge CR [33]. Another study [25] showed that self-efficacy is an important risk factor for sports phobia after total knee replacement [OR = 1.4]. Zelle et al. [15] also believe that self-efficacy is closely related to sports phobia and may be an important factor in the relationship between sports phobia and physical activity. Therefore, this study found that the influence of exercise fear on physical activity can be explained by a low sense of self-efficacy to a large extent [34]. Positive and healthy self-efficacy beliefs can make patients more confident to regulate emotions and induce compliance with brain movements. Meanwhile, in this study, 81.1% of the subjects were in junior high school or below, and their ability to accept, understand and actively acquire disease knowledge was low. The more adverse consequences they had of their illness, the lower their levels of self-efficacy. Second, self-efficacy can influence physical activity behaviors through the development and use of self-regulating behaviors. Patients with low self-efficacy have more difficulty facing painful traumatic memories and are more likely to adopt negative coping strategies to cope with the stress caused by kinesiophobia, leading to further fear of physical activity. Given this, it is necessary for healthcare providers to consider self-efficacy as a contributing factor to exercise phobia and establish self-efficacy enhancement strategies to increase the chances of physical activity in postoperative AAAD patients.
We also found that negative coping styles are a significant risk factor for dyskinesia. The stress coping model proposed by Feifel et al. [23] shows that coping styles play an important role in disease outcomes in addition to patients and disease characteristics. This result is consistent with the results of Worm [35], who found that negative coping was associated with kinesiophobia and increased rates of long-term disability and depression. Somers et al. [36] also concluded that individuals who experience pain-related fears are likely to engage in avoidance behaviors, especially avoiding sports and physical activities. Although these patients had successful surgery and improved function after surgery, they still struggled to erase traumatic memories, leading to anxiety and other difficult mood changes. In addition, patients are concerned about the risk of elevated blood pressure due to exercise during CR because they are uncertain about their future health and safe level of exercise after surgery. Thus, more negative coping strategies can be used to deal with the stress caused by sports phobia, leading to higher pain intensity and further fear of physical activity.
In addition to the above risk factors, we found that less family support was associated with an increased prevalence of kinesiophobia and that APGAR was significantly negatively associated with kinesiophobia scores. Multivariate analysis suggested that APGAR was a protective factor for postoperative kinesiophobia in AAAD patients. Birtwistle et al. [37] also demonstrated that family support is closely related to physical activity (PA) behavior. Earlier studies have found that family support is associated with greater anxiety, depression and reduced mobility in people with CABG (Coronary Artery Bypass Grafting). Family members can communicate CR information to patients, encourage positive behaviors, and provide partner-based forms of PA to facilitate PA participation [37]. High levels of family support are associated with higher CR attendance and even longer survival rates; More family support predicted positive changes in mental health, while low levels of family support were associated with poorer perceptual status and physical dysfunction [38, 39]. Early studies have confirmed that integrating the family into CR helps promote physical actively-related interactions [37] and reduces the occurrence of sports kinesiophobia. Therefore, there is strong evidence that family support is a key factor in PA and can reduce the prevalence of sports kinesiophobia. However, there are some challenges within the family, including the family’s “over-involvement” and the family’s own health beliefs, which can negatively affect patients, and the role of family caregivers in AAAD patients requires further efforts.
The main strength of this study is that it produced cross-sectional findings showing the influence of related factors on kinesiophobia in AAAD patients. The study found that exercise phobia was present in 46.2% of AAAD patients. In addition, the impact on recovery outcomes in AAAD patients was determined by clinical variables that represent components of the theory of processes of stress action. In light of these findings, kinesiophobia needs to be considered in the rehabilitation of AAAD patients and given priority in future studies.
The following limitations were also considered in this study. Firstly, this was a single-center study with a limited sample size, which may affect the statistical results. Future research directions should involve larger sample sizes and employ a more rigorous multi-center design to further validate our conclusions. Secondly, recall bias may occur in remote telephone collection of questionnaire information. More rigorous data collection methods should be developed for subsequent studies, such as face-to-face interviews or real-time online surveys. Thirdly, our study only examined some factors that may affect kinesiophobia, but did not take into account the influence of preoperative factors, particularly anxiety and sleep state, which have been proven in other studies to increase patients’ perception of pain or the occurrence of kinesiophobia [40, 41]. In summary, we advocate for future studies to build upon these identified limitations, utilizing more comprehensive and diverse research approaches to strengthen the reliability and applicability of our conclusions.
Patients with AAAD exhibit a high prevalence of postoperative kinesiophobia. Patients’ education level, medical coping style, family care index and general self-efficacy are related to the occurrence of postoperative kinesiophobia. Therefore, the existence of kinesiophobia should be considered in the CR of patients with AAAD.
AAAD, Acute type A aortic dissection; AAD, Acute aortic dissection; CR, Cardiac rehabilitation; MTBSG, Modified Triple-Branched Stent Graft; AD, Aortic dissection; TSK-SV-Heart, The Tampa Scale for kinesiophobia Heart; PA, Physical activity; NRS, Numerical Rating Scale; GSES, General Self-efficacy Scale; MCMQ, Medical Coping Modes Questionnaire; APGAR, Adaptation, Partnership, Growth, Affection and Resolve, Family care index scale.
The data that support the findings of this study are available from Fujian Cardiac Medical Center but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Fujian Cardiac Medical Center.
YJL and LWC conceived and designed the study, and critically revised the manuscript for significant intellectual content. YQC prepared the first draft of the manuscript, conducted the literature review, and made significant contributions to the design of the work. YCP jointly made substantial changes to the manuscript and participated in the design of the work. XZH collected and analyzed data together, and drafted the manuscript. All authors read and approved the final manuscript. All authors have actively participated in the work and are accountable for all aspects of it.
The study was approved by the Ethics Committee of Fujian Medical University Affiliated Union Hospital ([2020] Union Hospital Ethics Review No. 080) and conducted in accordance with the Declaration of Helsinki. We also received written informed consent from subjects or their legal counsels before research commencement.
Not applicable.
This work was funded by the research project of science and technology Innovation think tank of Fujian Province University, Fujian Provincial Center for Cardiovascular Medicine Construction Project (NO.2021-76) and Joint Funds for the innovation of science and Technology, Fujian province (2021Y0023).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.