



 , YunDai Chen 1,2,*
, YunDai Chen 1,2,*1 School of Medicine, Nankai University, 300071 Tianjin, China
2 Department of Cardiology, The First Medical Center, Chinese PLA General Hospital, 100853 Beijing, China
†These authors contributed equally.
Abstract
Background: There is controversy regarding the effectiveness the of
jailed wire technique (JWT) and jailed balloon technique (JBT) in preserving the
side branch (SB) during treatment. This study compares the protective effect of
JBT versus JWT on the SB ostium area in coronary bifurcation lesions using
three-dimensional optical coherence tomography (3D-OCT). Methods: We
obtained data from coronary heart disease patients who received OCT-guided
percutaneous coronary intervention (PCI) for bifurcation lesions. The SB
protection strategies were divided into JWT and JBT, with the latter further
subdivided into active JBT (A-JBT) and conventional JBT (C-JBT). The primary
endpoint was the SB ostium area difference measured by 3D-OCT before and after
PCI. Partial correlation analysis and propensity score matching (PSM) was used to
mitigate confounding biases. Results: A total of 207 bifurcation lesions
from 191 patients were analyzed, including 136 lesions treated with JWT and 71
lesions treated with JBT. The SB ostium area was significantly greater in the JBT
group compared to the JWT group (0.41
Keywords
- optical coherence tomography
- jailed balloon technique
- jailed wire technique
- bifurcation lesion
Bifurcation lesions account for 20% of all percutaneous coronary interventions (PCI), with provisional stenting being the predominant strategy for treating de novo coronary bifurcation lesions [1, 2]. The process of stent placement in the main vessel (MV) may lead to plaque redistribution or carina shift, subsequently impacting the side branch (SB) [3]. This can escalate into SB complications ranging from ostial stenosis deterioration to complete SB occlusion, potentially resulting in perioperative myocardial infarction and adverse long-term outcomes [4, 5]. Previous studies have shown that SB ostial stenosis is an independent predictor of acute SB occlusion following MV stenting [6, 7]. Therefore, it is crucial to address SB ostium stenosis during bifurcation lesion interventions.
The jailed balloon technique (JBT) and jailed wire technique (JWT) are key strategies for protecting the SB and mitigating SB occlusion risk in complex bifurcation lesions [8, 9]. Despite their widespread use, comparative data on JBT and JWT is limited and has yielded mixed results [10, 11]. Studies indicate JWT was associated with fewer instances of SB occlusion following MV stenting in cases of severe stenosis at the SB or MV [10]. In contrast, the CIT-RESOLVE study showed that JBT provided superior SB protection compared to JWT [12], a finding contested by another research group [13]. This discrepancy underscores the need for further investigation to clarify the comparative efficacy of these techniques.
The evaluation of SB complications often relies on immediate angiographic results. However, accurately assessing SB ostial stenosis is challenging due to factors such as vessel overlap, angulations, stent struts obstructing the branch view, and image foreshortening [14]. These inherent limitations complicate the clarity of assessments.
Three-dimensional (3D) optical coherence tomography (OCT) has emerged as a sophisticated intravascular imaging tool, offering detailed insights into the coronary lumen and vessel wall. It facilitates an indirect yet precise assessment of the SB ostium area, overcoming the drawbacks of traditional imaging techniques [15, 16]. The effectiveness of 3D-OCT in accurately measuring the SB ostium area has been demonstrated, positioning it as a reliable alternative to direct OCT pullback examinations of the SB [15]. Given its potential, this imaging method is poised to significantly influence the interventional treatment of bifurcation lesions. To our knowledge, no studies have utilized 3D-OCT to assess the protective effect of JBT and JWT on the SB.
Therefore, the objective of this study was to evaluate the protective effects of JBT and JWT on the SB ostium using 3D-OCT. By employing this innovative approach, we anticipate the ability to provide more comprehensive data on the efficacy of JBT and JWT, thereby aiding in the clinical decision-making process.
Between September 2019 and March 2022, we conducted a retrospective screening of the coronary artery OCT imaging database at a national high-volume tertiary referral center. The inclusion criteria were as follows: (ⅰ) high quality OCT pullbacks obtained from the main branch. (ⅱ) Availability of OCT pullback data both before and after PCI. (ⅲ) The presence of at least one side branch affected by stent deployment in the main vessel. (ⅳ) The side branch ostium being sufficiently large to allow for three-dimensional visualization. The exclusion criteria were as follows: (ⅰ) Poor image quality (e.g., incomplete flushing) or image artifacts (e.g., guidewire shadow) that impeded 3D rendering and visualization of the SB ostium. (ⅱ) Inability to match the OCT image of the SB with coronary angiography. Patients were then categorized into either the JWT or the JBT group based on the side branch protection strategy employed.
All procedures were performed by experienced interventional clinicians following standard techniques at our institution. The choice of intervention strategy was left to the discretion of the physician. Prior to the intervention, all patients received a loading dose of aspirin (300 mg) and either clopidogrel (600 mg) or ticagrelor (180 mg) at least 24 hours in advance. Additionally, all patients received unfractionated heparin at a rate of 100 mg/kg to achieve an activated clotting time of 250–350 seconds. After intracoronary injection of 100–200 µg nitroglycerin, coronary angiography was conducted via the radial or femoral approach.
For the JWT procedure, coronary guidewires were placed distally in the MV and SB respectively. The MV lesions were routinely prepared, and the preparation of SB lesions was based on the operator’s discretion. The wire for SB protection was kept in place, and MV stents were deployed with a size optimized for the distal MV.
In the JBT procedure, the use of guidewires and the preparation of MV or SB
lesions were similar to that of JWT. A jailed balloon with a diameter of 1.5 mm
to 2.5 mm was advanced over the guide wire and positioned at the SB ostial site.
The proximal protrusion of the balloon was adjusted to the MV by approximately 2
mm. The MV stents were deployed with a size optimized for the distal MV. Note
that A-JBT refers to simultaneous dilation of the main branch stent and the SB
jailed balloon, while C-JBT refers to dilation of the main branch stent without
dilation of the SB jailed balloon. The dilation pressure of the jailed balloon
was clustered on 4 atm and the diameter clustered on 2 mm. A low dilation
pressure of the jailed balloon was defined as
The OCT image acquisition was conducted using two different systems: the commercially available C7-XRTM OCT intravascular image acquisition system (St Jude/LightLab Imaging, Inc., Westford, MA, USA) with a Dragonfly catheter (St Jude /LightLab Imaging, Inc., Westford, MA, USA) (N = 126, L = 132), and the CornarisTM system (Vivolight Corporation, Shenzhen, China) with a Pathfinder164 catheter (Vivolight Corporation, Shenzhen, China) (N = 65, L = 75). The OCT catheter was advanced over the guide wire and positioned at least 10 mm distal to the target lesion in the tested artery. Automated OCT pullback was performed at a speed of 20 mm/s while continuously injecting contrast medium (Iodixanol 370, Visipaque TM, GE HealthCare, Ireland) through the guiding catheter at a rate of 3–4 mL/s. The OCT images were analyzed offline by two experienced investigator (QHJ and JGC) who were blinded to the information. The analysis was performed according to a predefined standard operating procedure using available software (Vivolight Imaging Systems, Shenzhen, China). The SB ostium area was measured using a cut-plane analysis based on a 3D model [15]. Plaque types were classified based on criteria from previous studies, and were divided into fibrous plaques, lipid-rich plaques, and fibrocalcific plaques. A normal vessel wall was defined as having mild intimal hyperplasia or a typical three-layer structure of the intima, media, and adventitia [17].
The primary efficacy endpoint was the difference in SB ostium areas, while the safety endpoint was the quantification of SB protection procedure related complications. The area of the SB ostium was measured using Vivolight OCT software in a 3D model before and after single stenting of the MV. The SB ostium area difference was calculated as the post-PCI SB ostium area minus the pre-PCI SB ostium area. Complications related to JBT or JWT were defined as SB dissection, entrapment of guidewires, or entrapment of balloons.
Continuous variables with a normal distribution were reported as mean
To mitigate confounding biases linked to an intention-to-treat analysis,
propensity score matching (PSM) was applied. Factors influencing outcomes or
those significantly differing between groups—such as bifurcation angle,
bifurcation carina angle, plaque type, branching point to carina tip length,
minimal lumen area at bifurcation, classification of bifurcation as true or
non-true, SB ostium area, and the mean, minimal, and maximal diameter at the
carina level in the main vessel (MV)—served as covariates for calculating the
propensity score. The SB protection strategy was marked as the group indicator.
For PSM, a 1:1 nearest neighbor approach with a caliper of 0.2 standard deviation
of logit was used. The analysis was performed using SPSS 25.0 (IBM, Chicago, IL,
USA). A two-tailed p-value of
In the current study, a total of 1032 patients who underwent PCI and OCT examinations were initially screened for eligibility, out of which 841 were excluded due to various criteria. Consequently, the final dataset comprised 207 bifurcation lesions in 191 patients, forming the final dataset for investigation (Fig. 1).
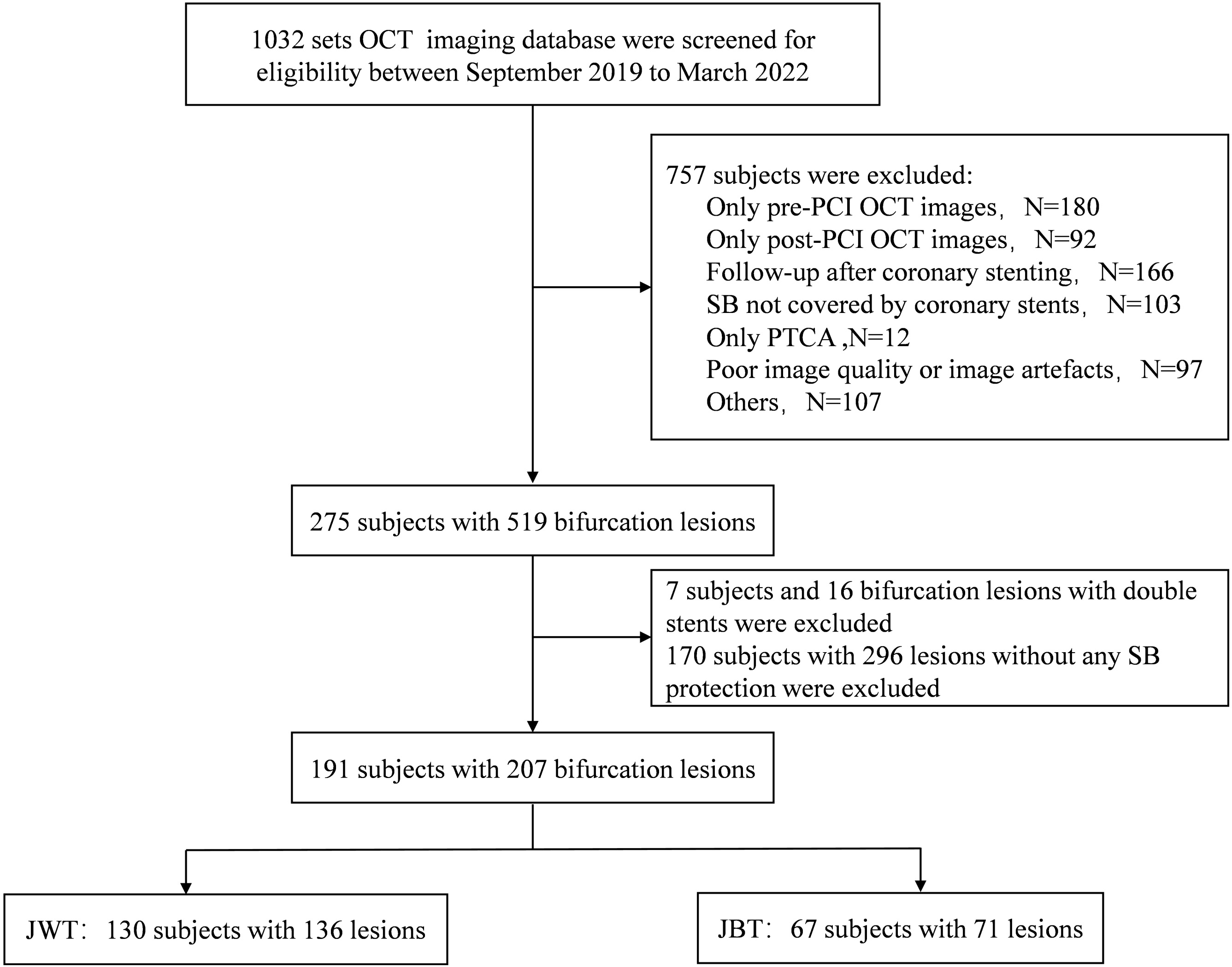 Fig. 1.
Fig. 1.
Patient selection and lesion treatment overview in bifurcation lesions. This figure outlines the screening and inclusion process of patients undergoing PCI and OCT, detailing the distribution of bifurcation lesions treated with the JBT and JWT. Specifically, four patients with two bifurcation lesions were treated with JBT simultaneously, while three patients with two lesions were treated with JWT simultaneously. Additionally, three patients with two lesions were each treated with both JBT and JWT. In another case, one patient received JBT for one lesion and JWT for two others. OCT, optical coherence tomography; PCI, percutaneous coronary intervention; PTCA, percutaneous transluminal coronary angioplasty; SB, side branch; JBT, jailed balloon technique; JWT, jailed wire technique.
In the study, the prevalence of true bifurcation lesions was significantly
elevated in the JBT treatment cohort when compared to the JWT treatment cohort
(73.2% vs. 47.1%, p
| Characteristics | JWT | JBT | p | |
| Bifurcation location, n (%) | 0.535 | |||
| Left main | 22 (16.2) | 10 (14.1) | ||
| LAD diagonal | 96 (70.6) | 56 (78.9) | ||
| LCX-OM | 14 (10.3) | 4 (5.6) | ||
| RCA-PDA | 4 (2.9) | 1 (1.4) | ||
| Medina classification, n (%) | 0.000 | |||
| True bifurcation | 64 (47.1) | 52 (73.2) | ||
| 0, 1, 1 | 13 (9.6) | 11 (15.5) | ||
| 1, 0, 1 | 7 (5.1) | 2 (2.8) | ||
| 1, 1, 1 | 44 (32.4) | 39 (54.9) | ||
| Non-true bifurcation | 72 (52.9) | 19 (26.8) | ||
| 0, 0, 1 | 2 (1.5) | 3 (4.2) | ||
| 1, 1, 0 | 17 (12.5) | 6 (8.5) | ||
| 0, 1, 0 | 36 (26.5) | 8 (11.3) | ||
| 1, 0, 0 | 17 (12.5) | 2 (2.8) | ||
| Plaque type | 0.040 | |||
| Normal | 2 (1.5) | 1 (1.4) | ||
| Fibrous plaques | 66 (48.5) | 20 (28.2) | ||
| Lipid-rich plaques | 37 (27.2) | 25 (35.2) | ||
| Fibrocalcific plaques | 31 (22.8) | 25 (35.2) | ||
| Bifurcation angle (°) | 52.50 (41.81, 69.38) | 52.75 (35.57, 63.58) | 0.256 | |
| Bifurcation carina angle (°) | 53.72 (34.08, 75.75) | 54.29 (32.90, 71.16) | 0.607 | |
| Minimum diameter of bifurcation (mm) | 1.90 (1.54, 2.40) | 1.67 (1.44, 2.00) | 0.011 | |
| Maximum diameter of bifurcation (mm) | 2.52 (2.17, 3.08) | 2.31 (1.90, 2.61) | 0.007 | |
| Mean diameter of bifurcation (mm) | 2.24 (1.93, 2.79) | 2.15 (1.76, 2.37) | 0.026 | |
| MV area of bifurcation (mm2) | 3.74 (2.69, 5.69) | 3.23 (2.20, 4.26) | 0.009 | |
| MLA in bifurcation (mm2) | 1.72 (1.27, 2.25) | 1.52 (1.09, 2.10) | 0.076 | |
| Branching point- carina tip length (mm) | 1.60 (1.10, 2.08) | 1.40 (1.20, 1.80) | 0.177 | |
| SB ostium area pre-PCI (mm2) | 3.09 (1.81, 4.55) | 2.40 (1.69, 3.26) | 0.002 | |
All values are presented as n (%), mean
The JBT was utilized in 71 bifurcation lesions, with active JBT (A-JBT) employed
in 62 cases. The balloons in the procedures had a mean diameter of 2.01
The application of this technique resulted in successful outcomes in all patients. Notably, there were no cases of entrapment or fracture of the guidewire in either group, nor were there any incidents of jailed balloon entrapment in the JBT group. However, a single case of type B coronary artery dissection, as determined by the National Heart, Lung, and Blood Institute (NHLBI) criteria, was observed in the JBT group [18]. Based on the operator’s discretion, no further interventions were performed for this patient as they did not exhibit significant ischemic symptoms and there was no progression in the dissection’s severity.
We determined the JBT group experienced a significantly greater SB ostium area
increase compared to the JWT group (0.41
| SB ostium area difference (mm2) | |||||||||
| Groups | JWT | JBT | p | JWT | A-JBT | p | JWT | C-JBT | p |
| Total | –0.25 |
0.41 |
0.001 | –0.25 |
0.50 |
0.001 | –0.25 |
–0.17 |
0.862 |
| True bifurcation | –0.10 |
0.38 |
0.023 | –0.10 |
0.47 |
0.011 | –0.10 |
–0.18 |
0.859 |
| Non-true bifurcation | –0.38 |
0.49 |
0.034 | –0.38 |
0.56 |
0.030 | –0.38 |
–0.14 |
0.833 |
Note: Lesion level.
All values are presented as the mean
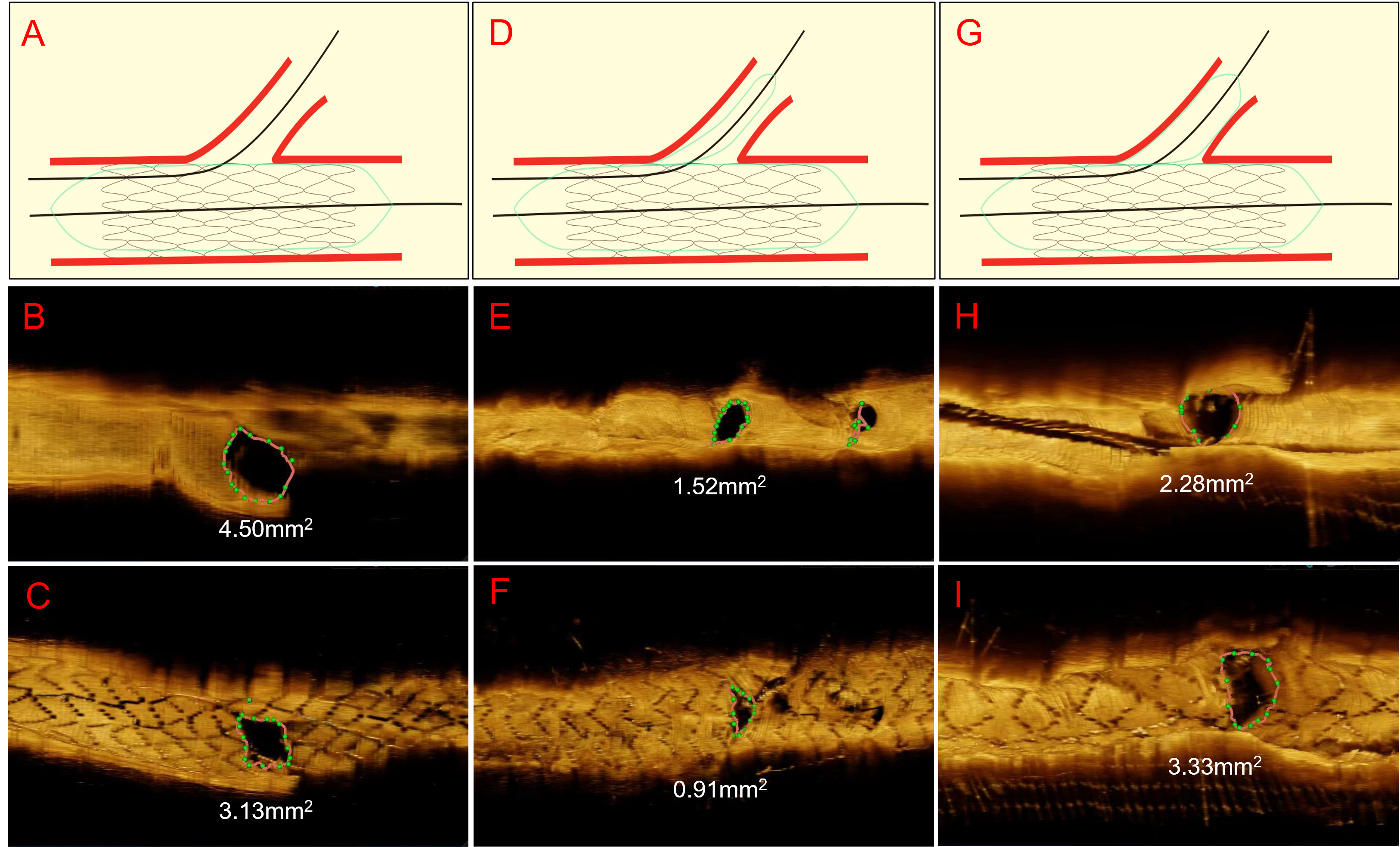 Fig. 2.
Fig. 2.
Representative cases of OCT imaging pre- and post-PCI. This
figure presents a visual comparison of the SB ostium area before and after stent
placement in coronary artery bifurcation lesions, as captured through OCT
imaging. The figure is divided into three main sections, each depicting a
different stenting technique: JWT, C-JBT, and A-JBT. The first
section (A,B,C) includes a schematic of the JWT, followed by OCT images
showcasing the SB ostium area (as green dotted lines) before (B) and after (C)
PCI. In this JWT case, the area of the SB ostium decreases from 4.5 mm
After propensity score matching (PSM), to equalize the coronary vascular
structural factors between groups, no significant difference in SB ostium
protection was observed between JBT and JWT, although JBT showed a
non-significant trend towards better outcomes (0.28
Assessing the relationship between jailed balloon characteristics and the resulting changes to the SB ostium area led to the following findings. The correlation coefficient between jailed balloon pressure and the change in SB ostium area was 0.118 (p = 0.327), indicating a lack of significant correlation. Conversely, a significant correlation was found between the jailed balloon diameter and the SB ostium area difference, with a coefficient of 0.307 (p = 0.009) (Supplementary Fig. 1). There was a significant positive partial correlation between the diameter of the jailed balloon and the SB ostium area difference (r = 0.296, p = 0.013) suggesting that larger balloon diameters are associated with greater increases in the SB ostium area. However, no significant correlation was observed between the jailed balloon pressure and the SB ostium area difference (r = 0.083, p = 0.495).
After dividing the A-JBT group into two subgroups based on the dilation pressure
(
| SB ostium area difference (mm2) | ||||||
| Groups | Low pressure ( |
High pressure ( |
p | Small diameter ( |
Large diameter ( |
p |
| Total | 0.59 |
0.46 |
0.713 | 0.22 |
1.44 |
0.002 |
| True bifurcation | 0.32 |
0.52 |
0.639 | 0.30 |
1.74 |
0.037 |
| Non-true bifurcation | 1.10 |
0.36 |
0.267 | –0.11 |
1.32 |
0.019 |
Note: Lesion level.
All values are presented as the mean
To the best of our knowledge, this study is the first to compare the protective effect of the JBT and the JWT in bifurcation lesions using 3D-OCT. The key findings of this study can be summarized as follows: (1) The protective effect of JBT primarily stems from the impact of A-JBT. (2) The larger diameter of the jailed balloon, rather than the higher pressure, provides greater protection for the SB.
While SB ostium stenosis may worsen due to plaque or carina shift following MV stenting, adopting a single stent technique with SB stenting is still the recommended approach for treating coronary bifurcation lesions [19]. This clinical approach is justified by evidence showing that a smaller SB ostium area is associated with decreased fractional flow reserve values [20]. This correlation suggests that compromised SB integrity is a significant concern, and is likely to result in adverse clinical outcomes in PCI bifurcation [20]. Consequently, considerable efforts have been made to identify patients at risk for SB compromise following MV stent implantation [6, 8, 10, 21, 22, 23, 24]. Although the JBT and JWT techniques are established methods for preventing SB occlusion during bifurcation lesion treatment, their effectiveness in protecting against SB occlusion remains controversial [10, 11, 12, 13]. Previous studies have suggested that JBT is more effective than JWT in preventing SB occlusion, but these studies relied on visual assessment of coronary angiography or quantitative coronary angiography [8, 12]. However, visual estimation based on angiography or quantitative coronary angiography is not reliable for assessing the severity of SB lesions [14, 25]. Therefore, more accurate tools are needed to measure the extent of SB ostial stenosis.
As a state-of-the-art imaging modality, OCT plays a critical role in measuring the side branch ostium [16]. The accuracy of SB ostial area measurements using 3D-OCT in MV closely matches that of SB OCT pullback, suggesting that 3D-OCT guidance for optimal SB treatment is a viable and effective solution [15, 26]. Therefore, this study aimed to evaluate the impact of JBT versus JWT on the SB ostial area in bifurcation lesions treated with the single-stent approach. When considering all bifurcation lesions, JBT was associated with a relatively larger absolute SB ostium area compared to JWT. In the subgroup analysis, JBT demonstrated a superior protective effect, primarily attributed to A-JBT. In contrast, C-JBT did not show any discernible advantage over JWT. Previous studies have shown that A-JBT can prevent SB occlusion, and even improve SB functional blood flow compared to JWT [11, 27, 28]. This superiority of JBT over JWT was consistent across both true and non-true bifurcation lesion subgroups. Furthermore, PSM analysis was utilized to compensate for potential selection bias in retrospective observational studies and to facilitate an intention-to-treat analysis. Although no statistical difference was observed, there was a trend suggesting that the increase in SB ostium area may be greater in the JBT group compared to the JWT group.
Carina and plaque shifts are the primary mechanisms leading to SB ostial
compromise at the SB following MV stent implantation [29]. The protective effect
of JBT on SB ostium may be attributed to its capacity to mitigate these shifts.
We have demonstrated that the utilization of a large diameter jailed balloon and
A-JBT provide superior protection in true bifurcation lesions. Subgroup analysis
revealed that a larger jailed balloon diameter (
Several studies have assessed the protective effect of JBT on SB through coronary angiography, finding JBT superior to JWT in reducing branch occlusion, but not in long-term patient outcomes [11, 12]. Our study aligns with these findings to an extent, confirming that JBT, particularly A-JBT, offers more effective protection of the SB ostium area compared to JWT. Nonetheless, the difference in the increase of the SB ostium area between the JBT and JWT groups was modest, at an average of 0.66 mm2 in the JBT group compared to the JWT group (0.41 mm2 vs. –0.25 mm2). This relatively small disparity in SB ostium area enlargement may explain the absence of observed significant differences in the long-term prognosis of patients treated with either technique [11].
The JBT group was characterized by a smaller initial SB ostium area and a greater incidence of true bifurcation cases, which aligns with observations from clinical practice. Despite the strategic use of JBT, the extent of SB ostium enlargement following PCI in the JBT group was modest, with a mean difference of 0.41 mm2. This finding suggests that A-JBT, particularly when utilizing larger diameter balloons, may be more suitable for treating relatively large SBs with ostial stenosis [31]. Such scenarios include bifurcations of the non-left main trunk and the left main trunk when associated with a smaller left circumflex artery [31]. However, the implementation of A-JBT necessitates a careful consideration of potential risks, including SB dissection, the entrapment of devices, and stent deformation, which could complicate the procedure [32, 33]. In our study, balloons ranging from 1.5–2.5 mm were used for SB treatment via JBT, and no significant complications were reported, suggesting a cautious yet effective application for this technique.
This study has several limitations that merit acknowledgment. Firstly, its retrospective design inherently carries the risk of introducing various certain biases into the findings. Secondly, the selection of patients and procedural techniques was subject to the operating clinician’s subjective preferences, potentially leading to selection bias. However, it’s noteworthy that the basic demographic and clinical characteristics, such as age, sex, and clinical diagnosis were similar across the groups, somewhat mitigating concerns related to selection bias. Thirdly, the initial SB ostium area was smaller in the JBT group compared to the JWT group before undergoing PCI. To counteract these confounding factors, PSM was employed, aiming to equalize these variables and reduce the impact of biases on the study’s outcomes.
Based on the analysis of the series OCT imaging database, A-JBT was found to be superior to JWT in preserving SB ostial area in single stent procedures. Notably, the efficacy of protection afforded to the SB was more strongly associated with the diameter of the jailed balloon than with the pressure applied during dilation. Therefore, when using the provisional stenting technique for bifurcation lesions, utilizing a larger diameter balloon and ensuring its protection with A-JBT appears to be a preferable strategy for SB preservation. Nonetheless, the validation of these findings necessitates further investigation through prospective studies and randomized clinical trials to solidify the evidence base supporting this approach.
OCT, optical coherence tomography; SB, side branch; MV, main vessel; 3D, three-dimensional; JWT, jailed wire technique; JBT, jailed balloon technique; PCI, percutaneous coronary intervention; PSM, propensity score matching.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
JC and QJ designed the research study. JC, XW and QJ performed the research. JC analysed the data. JC wrote the manuscript. YC conceived of the study and participated in supervising data quality. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study protocol was approved by the Institutional Review Board of the General Hospital of Chinese People’s Liberation Army (No. S2020-196–01), and it adheres to the Helsinki Declaration. All patients provided written consent for the use of their imaging data.
All authors gratefully acknowledge the staff at the Chinese People’s Liberation Army General Hospital’s Department of Cardiology and Cardiac catheterization room for their contributions to this study.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.