





1 Department of Physical Education, Tongji University, 200092 Shanghai, China
2 Physical Education Department of Shanghai International Studies University, 201620 Shanghai, China
3 School of Sports and Health of Shanghai Lixin University of Accounting and Finance, 201209 Shanghai, China
Abstract
Background: This meta-analysis aimed to evaluate the impact of aerobic
exercise on Peak VO2 (Oxygen Consumption) in postoperative patients with
congenital heart disease (CHD). Besides this, we also tried to discover whether
the improvement was influenced by patient ages, modes of supervision, types of
exercise, the total dose of exercise, intervention periods, and types of CHD.
Methods: Following the Population Intervention Comparison Outcome Study
Design (PICOS) principle, a comprehensive search of the PubMed, Web of Science,
Embase and Cochrane Library databases was conducted for randomized controlled
trials (RCTs) evaluating the intervention effects of aerobic exercise on
cardiopulmonary function in postoperative CHD patients until December 2023. This
meta-analysis and publication bias tests were conducted using Stata 17.0, and the
mean differences (MDs) with 95% confidence intervals (CIs) were used as effect
sizes in statistics. Results: A total of 15 RCTs (762 cases) were
included in this meta-analysis, with 407 cases in the experimental group and 355
cases in the control group. Meta-analysis showed that aerobic exercise had a
positive effect on Peak VO2 in postoperative CHD patients (MD = 2.14, 95%
CI (1.34, 2.94), p
Keywords
- aerobic exercise
- congenital heart disease
- Peak VO2
- cardiopulmonary function
- meta-analysis
Congenital heart disease (CHD), caused by abnormal fetal cardiovascular development, is one of the most common congenital abnormalities [1]. According to 2020 European Society of Cardiology (ESC) Guidelines for the Management of Adult Congenital Heart Disease issued by Association for European Paediatric and Congenital Cardiology (AEPC) and International Society for Adult Congenital Heart Disease (ISACHD), approximately 9 out of every 1000 newborns worldwide are affected by CHD [2]. Being a condition present at birth, CHD leads to impaired blood supply to tissues and organs of the body, resulting in tissue hypoxia, which greatly hampers the growth and development of affected children. Moreover, hemodynamic abnormalities will exacerbate cardiac workload, predisposing patients to malignant arrhythmias and sudden cardiac death [3]. With substantial advancements in cardiac surgery and perioperative management techniques, approximately [1] 90% of CHD patients can survive to adolescence and adulthood through surgical intervention. Nevertheless, postoperative patients with CHD often encounter long-term issues such as hypoxia and reduced exercise endurance [4, 5]. These challenges directly impact patients’ oxygen supply capacity and exercise endurance, posing an urgent need for effective strategies to enhance postoperative cardiopulmonary function of CHD patients.
In the United States and Europe, the guidelines for CHD patients suggest that moderate and sustained aerobic exercise will enhance the contraction and relaxation abilities of the myocardium, promote blood circulation, increase coronary blood flow, and elevate functional capacity of the heart [6, 7]. Studies have found a range of positive effects during aerobic exercise, such as increased respiratory rate and depth, expanded lung capacity, and improved endurance, all of which can enhance the function of postoperative CHD patients, thereby improving their quality of life [8, 9, 10].
Cardiopulmonary Exercise Test (CPET) serves as a cornerstone for health
evaluation and exercise prescription, and is deemed as the “gold standard” for
diagnosing CHD patients’ cardiopulmonary functions [11]. Relevant indicators such
as the cardiorespiratory reserve function and exercise endurance of CHD patients
can be assessed by CPET. Peak oxygen consumption (VO2) represents the oxygen uptake when CHD
patients reach their maximum exercise load during CPET, reflecting the body’s
maximal aerobic metabolism and cardiorespiratory reserve capacity. As a result,
it is the optimal indicator for assessing aerobic metabolic capacity. The
prognostic significance of Peak VO2 for mortality and morbidity rates in CHD
patients has been proven [12, 13, 14, 15]. Multiple studies have shown that there is an
inverse relationship between Peak VO2 and the risk of cardiovascular events,
and a direct correlation between Peak VO2 and cardiopulmonary functions in
CHD patients [11, 16, 17]. Laukkanen et al. (2016) [18] demonstrated
through their studies that for every increase of 1 mL/kg/min in Peak VO2,
there is a 9% reduction in relative risk of all-cause mortality (hazard ratio =
0.91; 95% CI, 0.87–0.95), emphasizing the importance of maintaining good
cardiopulmonary function. Study results from Opotowsky et al. (2018)
[19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29] indicated that aerobic exercise can increase Peak VO2 in
postoperative CHD patients. An RCT by Westhoff-Bleck et al. (2013) [26]
showed that exercise for 24 weeks at a heart rate of 110.3
A review of prior research reveals inconsistent findings regarding the effect of aerobic exercise on Peak VO2 in postoperative CHD patients. The meta-analysis results by Xu C et al. (2020) [30] indicated that exercise has no significant impact on Peak VO2, a conclusion also reached by Klausen et al. (2016) [31]. However, studies by Opotowsky et al. (2018) [19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29] suggested that aerobic exercise provides substantial benefits for Peak VO2 in postoperative CHD patients. The disparities in these findings may be due to the small sample sizes in each experiment and remarkable age differences among participants in these studies. Furthermore, we also found that previous studies have not clarified whether different exercise elements have an effect on Peak VO2 in postoperative CHD patients. Thus, this study, harnessing the methodology of evidence-based medicine, aims to systematically evaluate and analyze whether aerobic exercise can effectively improve Peak VO2 in CHD patients. We also tried to figure out whether the effectiveness is influenced by factors such as patient age, modes of supervision, types of exercise, and the types of CHD. Moreover, this study observed whether the duration, frequency, and intervention period of aerobic exercise present a dose-response effect for improving CHD patients’ condition. In conclusion, this study aims to identify the potential dose-response effect of aerobic exercise on Peak VO2 in postoperative CHD patients, ascertain the optimal exercise regimen for enhancing Peak VO2 in postoperative CHD patients, and provide evidence-based clinical support.
Regarding the selection and utilization of research methods, this study adhered to the PRISMA writing guidelines for meta-analysis [32], and has been registered on INPLASY No.202440016 (https://inplasy.com).
The research framework is based on 2020 ESC Guidelines for the management of adult congenital heart disease [2] issued by AEPC and ISACHD. It involves an analysis of patient information including age, modes of supervision, types of exercise, the dose of exercise, intervention periods, and types of CHD. This study aims to analyze the intervention effects of exercise on the cardiorespiratory function and exercise endurance of postoperative CHD patients by observing the changes in Peak VO2. Additionally, we aim to investigate potential dose-effects of aerobic exercise on the optimal intervention period, the dose of exercise, types of exercise, and modes of supervision for postoperative CHD patients. The Population Intervention Comparison Outcome Study Design (PICOS) framework for this systematic review is presented in Table 1.
| PICOS | Inclusion criteria |
| Population | Patients diagnosed with CHD, excluding those with conditions such as pregnancy or history of sudden death, and those with abnormal exercise test results. |
| Intervention | The experimental group undergoes exercise training as an intervention. In addition to routine care, this includes aerobic exercise, resistance training, or unsupervised home-based exercise through electronic health education. |
| Comparison | The control group undergoes non-exercise interventions, including routine care and health education. |
| Outcome | Peak VO2 |
| Study design | Randomized controlled trials |
CHD, congenital heart disease; PICOS, Population Intervention Comparison Outcome Study Design; VO2, oxygen consumption.
Two retrieval personnel searched PubMed, Embase, Web of Science, and Cochrane databases respectively to collect randomized controlled trials (RCTs) about the effects of aerobic exercise on cardiopulmonary function and exercise endurance in postoperative CHD patients. The retrieval period extended from the establishment of each database to December 31, 2023. Additionally, manual searches of previously written reviews were conducted, included in relevant literature to acquire full-text articles. The literature was searched using the following words “Heart Defects, Congenital”[Mesh] OR “congenital heart disease”[Title/Abstract] OR “atrial septal defect”[Title/Abstract] OR “ventricular septal defect”[Title/Abstract] OR “cardiac function”[Title/Abstract] OR “pulmonary hypertension”[Title/Abstract] AND “Exercise”[Mesh] OR “motion”[Title/Abstract] OR “movement”[Title/Abstract] OR “sport”[Title/Abstract] OR “physical activity”[Title/Abstract] OR “rehabilitation training”[Title/Abstract] OR “high intensity interval training”[Title/Abstract] OR “moderate intensity exercise”[Title/Abstract] OR “aerobic training”[Title/Abstract] OR “resistance exercise”[Title/Abstract] AND “Cardiorespiratory function”[Mesh] OR “exercise endurance”[Title/Abstract] OR “peak oxygen uptake”[Title/Abstract] AND “randomized controlled trial”[Publication Type] (Take PubMed as an example).
(1) The subjects included in study were diagnosed as postoperative CHD patients
by the hospital. (2) The experimental group took aerobic exercise as an
intervention in addition to routine postoperative care, with the intervention
period being
(1) Patients with contraindications for exercise, conditions such as pregnancy or history of sudden death, and those with abnormal exercise test results. Exercise contraindications also include patients with acute illnesses such as acute heart, liver, gallbladder, pancreas, stomach, intestine, and kidney diseases, early-stage viral myocarditis, acute viral hepatitis, acute phase of pulmonary tuberculosis, etc.; patients with hemorrhagic diseases such as leukemia, hemophilia, thrombocytopenic purpura, etc.; patients with malignant tumor metastasis; and patients with coronary artery disease, etc. (2) Duplicated publications. (3) Unclear experimental data descriptions, inconsistent baselines, lack of pre-test data, and no response from authors, making it impossible to calculate or extract data. (4) Inappropriate interventions or mismatched outcomes.
After retrieving the relevant literature, they would be further deduplicated in Endnote. Two researchers selected studies and extracted data independently in a double-blind trial. Extracted data were inputted into RevMan 5.4.1 (The Cochrane Collaboration, 11-13 Cavendish Square, London W1G 0AN, UK), and their accuracy was double-checked. In case of discrepancies, a third researcher would be consulted to decide whether to include the data. Extracted data included the first author’s name, publication year, publication country, baseline information of the study subjects (age, gender, and stages of recovery), interventions and outcomes.
The methodological quality of included studies was evaluated using the Physiotherapy Evidence Database (PEDro)
scale [33], which includes 10 items: “random allocation” “concealed
allocation” “similarity at baseline” “subject blinding” “therapist
blinding” “assessor blinding” “
Evidence for the quality of outcomes was evaluated using the GRADEpro evidence rating system, which categorizes evidence quality as high, moderate, low, or very low. Quality assessment was conducted by two researchers respectively, and in case of discrepancies, a third researcher would be involved in the discussion until a consensus was reached.
RevMan 5.4.1 software was used for heterogeneity assessment of all outcomes in
the included studies. The sample sizes as well as the mean and standard
difference of the improvement values before and after interventions were
assessed. The included outcomes were all continuous variables. For outcomes with
the same measurement method and unit, mean difference (MD) was
used, and for those with different measurement methods or units, the standard
mean difference (SMD) was used. We used a threshold of p less than 0.05
and I
A total of 3807 relevant pieces of literature were identified through searches in PubMed, Embase, Web of Science, and Cochrane databases. Additionally, 2 articles were manually retrieved from other sources. After removing duplicates and preliminary screening based on titles and abstracts, 66 articles were selected. Following a full-text assessment and exclusion of articles that failed to meet the eligibility, a final set of 12 articles were included, comprising 15 RCTs for our meta-analysis (Fig. 1).
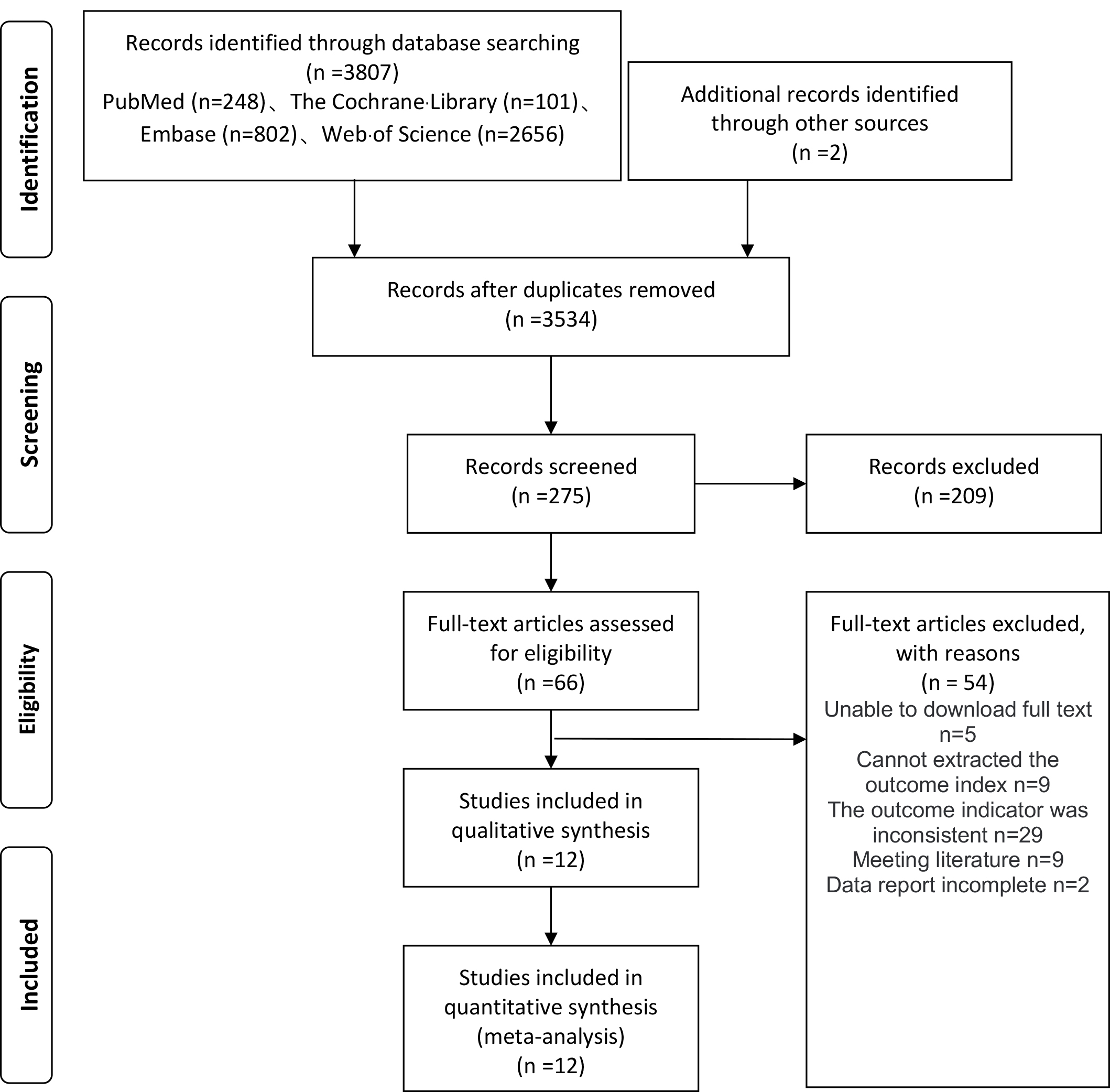 Fig. 1.
Fig. 1.
Process of Study selection.
Table 2 (Ref. [19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 31]) presents the basic information of included studies, comprising 12 articles [19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 31] with 15 studies (762 participants). The subjects were all postoperative CHD patients with ages ranging from 8 to 43 years old. The interventions all involved aerobic exercise with exercise frequencies ranging from 2 to 5 times per week and intervention periods ranging from 10 to 52 weeks.
| Study | Country | Location | Sample size (T/C) | Age (year) (T/C) | Intervention (T/C) | Intensity of exercise interventions | Frequency (times/week) | Period (week) | Dose (min) | Super-vison (Y/N) | Outcome [mL/kg/min] |
| Opotowsky et al. 2018 [19] | America | Rehabilitation center | 28 (13/15) | 47.5 |
②/③ | 2 | 12 | 1440 | Y | Peak VO2 | |
| Sandberg et al. 2018 [20] | Swedan | Home | 23 (13/10) | 31.1 |
①/③ | THR75%–80% | 3 | 12 | 1116 | N | Peak VO2 |
| Morrison et al. 2013 [21] | Northern Ireland | Home and laboratory | 143 (72/71) | 15.24/15.89 | ①/③ | 24 | Y | Peak VO2 | |||
| Ávila et al. 2016 [22] | Canada | Institute and activity center | 17 (13/4) | 35 |
②/③ | HRmax70%–80% | 2 | 12 | Y | Peak VO2 | |
| Therrien et al. 2003 [23] | Canada | Rehabilitation center | 17 (9/8) | 35.0 |
①/③ | Peak VO260%–85% | 3 | 12 | 1880 | Y | Peak VO2 |
| Fredriksen et al. 2000 [24] | Norway | Rehabilitation center and sports center | 93 (55/38) | 12.4 |
①/③ | HRmax65%–80% | 2 | 20 | Y | Peak VO2 | |
| Klausen et al. 2016 [31] | Denmark | Home | 158 (81/77) | 13–16 | ①/③ | 52 | N | Peak VO2 | |||
| Rhodes et al. 2006 [25] | America | Laboratory | 33 (15/18) | 11.9 |
②/③ | 2 | 12 | 1440 | Y | Peak VO2 | |
| Westhoff-Bleck et al. 2013 [26] | Germany | Home | 48 (24/24) | 29.9 |
①/③ | Peak VO250% | 3–5 | 24 | 2550 | N | Peak VO2 |
| Winter et al. 2012 [27] | The Netherlands | Home | 54 (28/26) | 31 |
①/③ | HRmax75%–90% | 3 | 10 | 1260 | Y | Peak VO2 |
| Duppen et al. 2015 [28] | The Netherlands | Hospital or rehabilitation center | 90 (53/37) | 15 |
①/③ | RHR60%–70% | 2–3 | 12 | 1800 | Y | Peak VO2 |
| Novaković et al. 2018 [29] | Slovenia | Hospital or rehabilitation center | 27 (18/9) | 38.5 |
①/③ | HRmax50%–80% | 2–5 | 12 | 1260 | N | Peak VO2 |
Notes: T, treatment group; C, control group; Y, yes; N, no; Intervention, ① Aerobic exercise; ② Aerobic exercise combined with resistance training; ③ Routine care; THR, training heart rate; HRmax, maximum heart rate; RHR, resting heart rate; VO2, oxygen consumption.
All 12 articles included in this study employed an RCT or quasi-RCT design.
Additionally, they all met the criteria of “similarity at baseline”
“intention-to-treat analysis” “between-group statistical comparison” and
“point and variability measures”. Additionally, 11 studies employed “random
allocation”; 4 studies met the criterion of “concealed allocation”; 5 studies
met the criterion of “subject blinding”; 3 studies met the criterion of
“therapist blinding”; 2 studies met the criterion of “assessor blinding”; and
9 studies met the criterion of “
| Random allocation | Concealed allocation | Similarity at baseline | Subject blinding | Therapist blinding | Assessor blinding | Intention-to-treat analysis | Between-group statistical comparison | Point and variability measures | Total points | ||
| Opotowsky et al. 2018 [19] | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Sandberg et al. 2018 [20] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 |
| Morrison et al. 2013 [21] | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 5 |
| Ávila et al. 2016 [22] | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Therrien et al. 2003 [23] | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Fredriksen et al. 2000 [24] | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 |
| Klausen et al. 2016 [31] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 8 |
| Rhodes et al. 2006 [25] | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Westhoff-Bleck et al. 2013 [26] | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 5 |
| Winter et al. 2012 [27] | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Duppen et al. 2015 [28] | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 8 |
| Novaković et al. 2018 [29] | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
The results are shown in Fig. 2, indicating that aerobic exercise effectively
enhanced Peak VO2 in postoperative CHD patients [MD = 2.14, 95% CI (1.34,
2.94), p
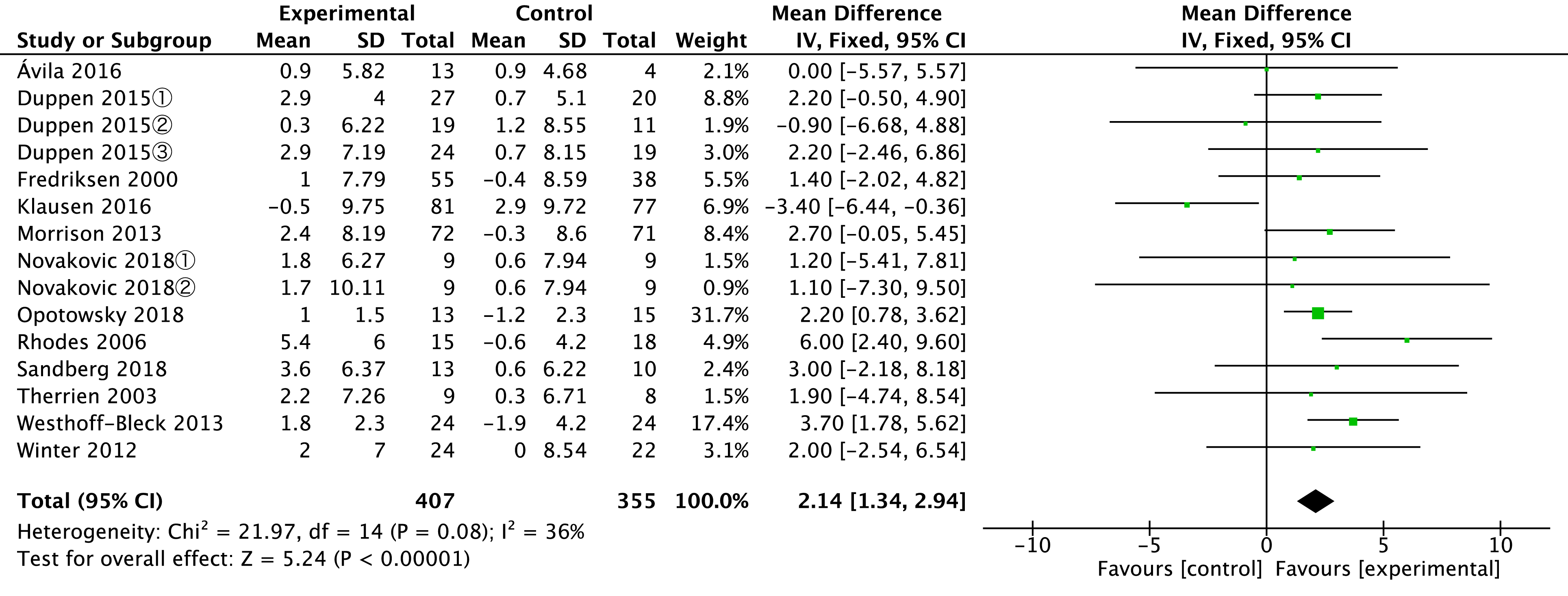 Fig. 2.
Fig. 2.
Forest-plot: the effects of aerobic exercise on Peak VO2 [mL/kg/min] in postoperative CHD patients. SD, standard deviation; IV, inverse variance; CI, confidence interval; Chi2, Chi-square; df, Degrees of Freedom; I2, I-squared; VO2, oxygen consumption; CHD, congenital heart disease. Duppen 2015①, Mixed patients group; Duppen 2015②, Fontan patients group; Duppen 2015③, ToF (Tetralogy of Fallot) patients group; Novakovic 2018①, Interval training group; Novakovic 2018②, Continuous training group.
Heterogeneity tests were conducted to examine if there was significant heterogeneity among the studies. The results showed that all studies were within the range of [–2, +2], which indicated good homogeneity and a certain level of stability and reliability among the studies. See Fig. 3.
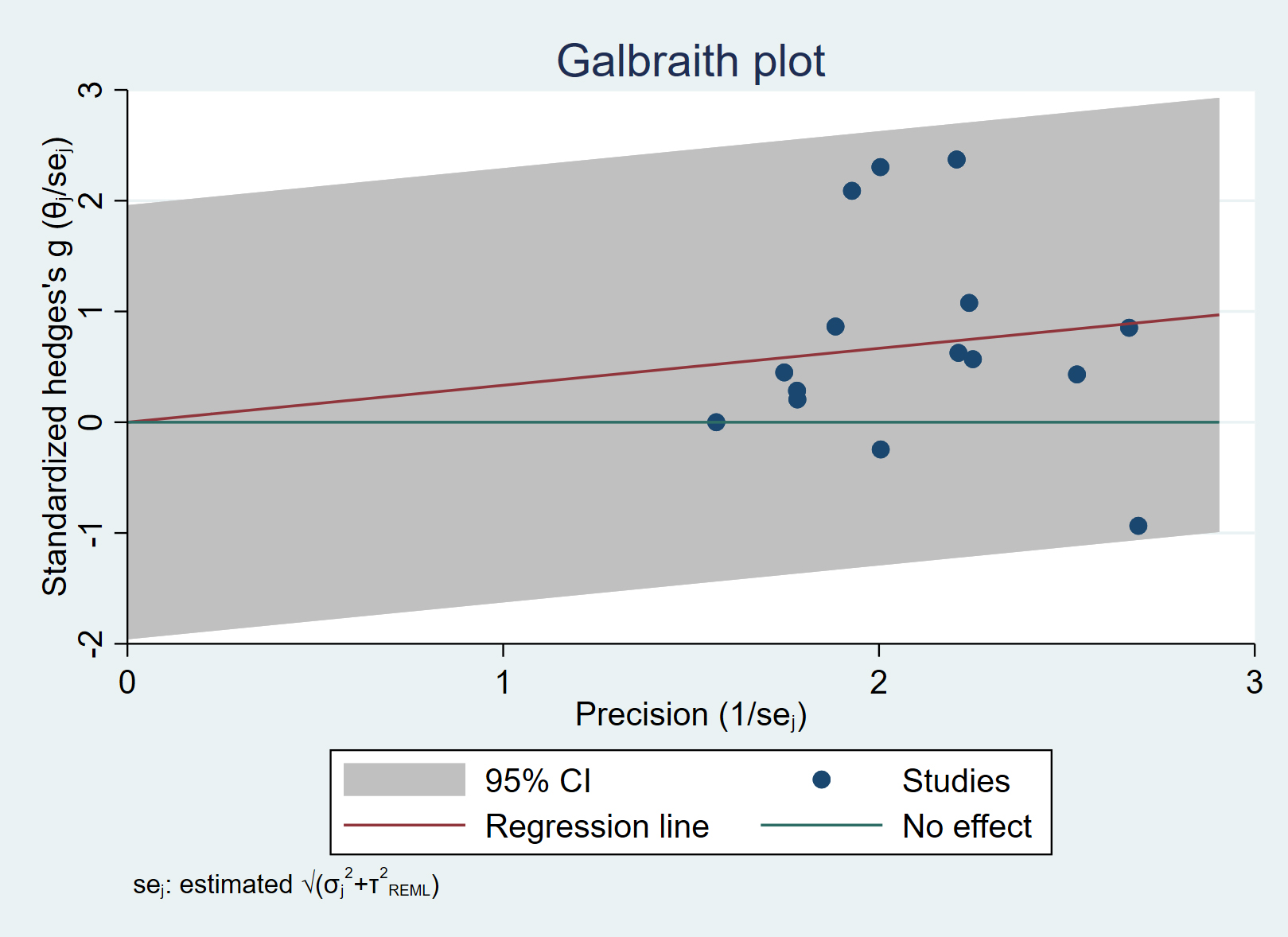 Fig. 3.
Fig. 3.
Galbraith plot. CI, confidence interval; se, standard error; REML, restricted maximum likelihood.
To explore potential sources of heterogeneity, this study analyzed outcome in
subgroups, as presented in Table 4 (Ref. [19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 31]). The impact of aerobic
exercise on Peak VO2 [mL/kg/min] in postoperative CHD patients may be
associated with factors such as age, modes of supervision, types of exercise, the
total dose of exercise (frequency of exercise time, unit: minutes), intervention
periods, and the types of CHD. We categorized age into two subgroups:
| Outcome | Number of included studies | I2/% | Result of meta-analysis | ||
| MD (95% CI) | p | ||||
| Age | 8 (215) [19, 20, 22, 23, 26, 27, 29] | 0 | 2.53 (1.5, 3.56) | ||
| 7 (547) [21, 24, 25, 28, 31] | 62 | 1.63 (0.36, 2.91) | 0.01000 | ||
| Mode of supervision | Supervised | 12 (413) [19, 20, 22, 23, 24, 25, 27, 28, 29] | 0 | 2.23 (1.26, 3.21) | |
| Unsupervised | 3 (349) [21, 26, 31] | 85 | 2.06 (0.66, 3.46) | 0.00400 | |
| Type of exercise | Aerobic exercise | 10 (684) [20, 21, 23, 24, 26, 27, 28, 29, 31] | 34 | 1.87 (0.84, 2.89) | 0.00030 |
| Aerobic exercise combined with resistance training | 3 (78) [21, 26, 31] | 56 | 2.57 (1.28, 3.85) | ||
| Total dose of exercise | 4 (105) [20, 27, 29] | 0 | 2.05 (–0.8, 4.9) | 0.16000 | |
| 5 (181) [19, 25, 28] | 23 | 2.45 (1.33, 3.58) | |||
| Intervention period | 10–12 weeks | 11 (320) [19, 20, 22, 23, 25, 27, 28, 29] | 0 | 2.31 (1.29, 3.33) | |
| 4 (442) [21, 24, 26, 31] | 78 | 1.97 (0.67, 3.26) | 0.00300 | ||
| Type of CHD | ToF | 5 (113) [22, 23, 28, 29] | 0 | 1.36 (–1.33, 4.05) | 0.32000 |
| Mixed | 8 (572) [19, 20, 21, 24, 25, 26, 27, 31] | 61 | 2.34 (1.45, 3.23) | ||
I2, I-squared; MD, mean difference; CI, confidence interval; ToF, Tetralogy of Fallot; VO2, oxygen consumption; CHD, congenital heart disease.
Subgroup analysis results in Table 4 (Ref. [19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 31]) indicate that when the
total dose of exercise is
To investigate whether the heterogeneity among studies was caused by certain
studies, this study conducted a sensitivity analysis by excluding individual
studies one by one to analyze the combined effect, as shown in Table 5. After
excluding the study by Klausen et al. (2016) [31], the combined effect
was MD = –3.4, 95% CI (–6.44, –0.36), and I
| Outcome | Excluded study | Effect size | 95% CI | p (Combined effect) | I2/% |
| Peak VO2 | Ávila et al. 2016 [22] | 0 | –5.57, 5.57 | 39 | |
| Duppen et al. 2015① [28] | 2.2 | –0.50, 4.90 | 41 | ||
| Duppen et al. 2015② [28] | –0.9 | –6.68, 4.88 | 38 | ||
| Duppen et al. 2015③ [28] | 2.2 | –2.46, 6.86 | 41 | ||
| Fredriksen et al. 2000 [24] | 1.4 | –2.02, 4.82 | 40 | ||
| Klausen et al. 2016 [31] | –3.4 | –6.44, –0.36 | 0 | ||
| Morrison et al. 2013 [21] | 2.7 | –0.05, 5.45 | 40 | ||
| Novaković et al. 2018① [29] | 1.2 | –5.41, 7.81 | 41 | ||
| Novaković et al. 2018② [29] | 1.1 | –7.30, 9.50 | 41 | ||
| Opotowsky et al. 2018 [19] | 2.2 | 0.78, 3.62 | 41 | ||
| Rhodes et al. 2006 [25] | 6 | 2.40, 9.60 | 25 | ||
| Sandberg et al. 2018 [20] | 3 | –2.18, 8.18 | 41 | ||
| Therrien et al. 2003 [23] | 1.9 | –4.74, 8.54 | 41 | ||
| Westhoff-Bleck et al. 2013 [26] | 3.7 | 1.78, 5.62 | 31 | ||
| Winter et al. 2012 [27] | 2 | –2.54, 6.54 | 41 |
CI, confidence interval; I2, I-squared; VO2, oxygen consumption. Duppen 2015①, Mixed patients group; Duppen 2015②, Fontan patients group; Duppen 2015③, ToF (Tetralogy of Fallot) patients group; Novakovic 2018①, Interval training group; Novakovic 2018②, Continuous training group.
The funnel plot of the intervention effects of aerobic exercise on Peak VO2
in postoperative CHD patients shows symmetrical distribution. Egger’s Test
yielded a result of t = –0.64, p
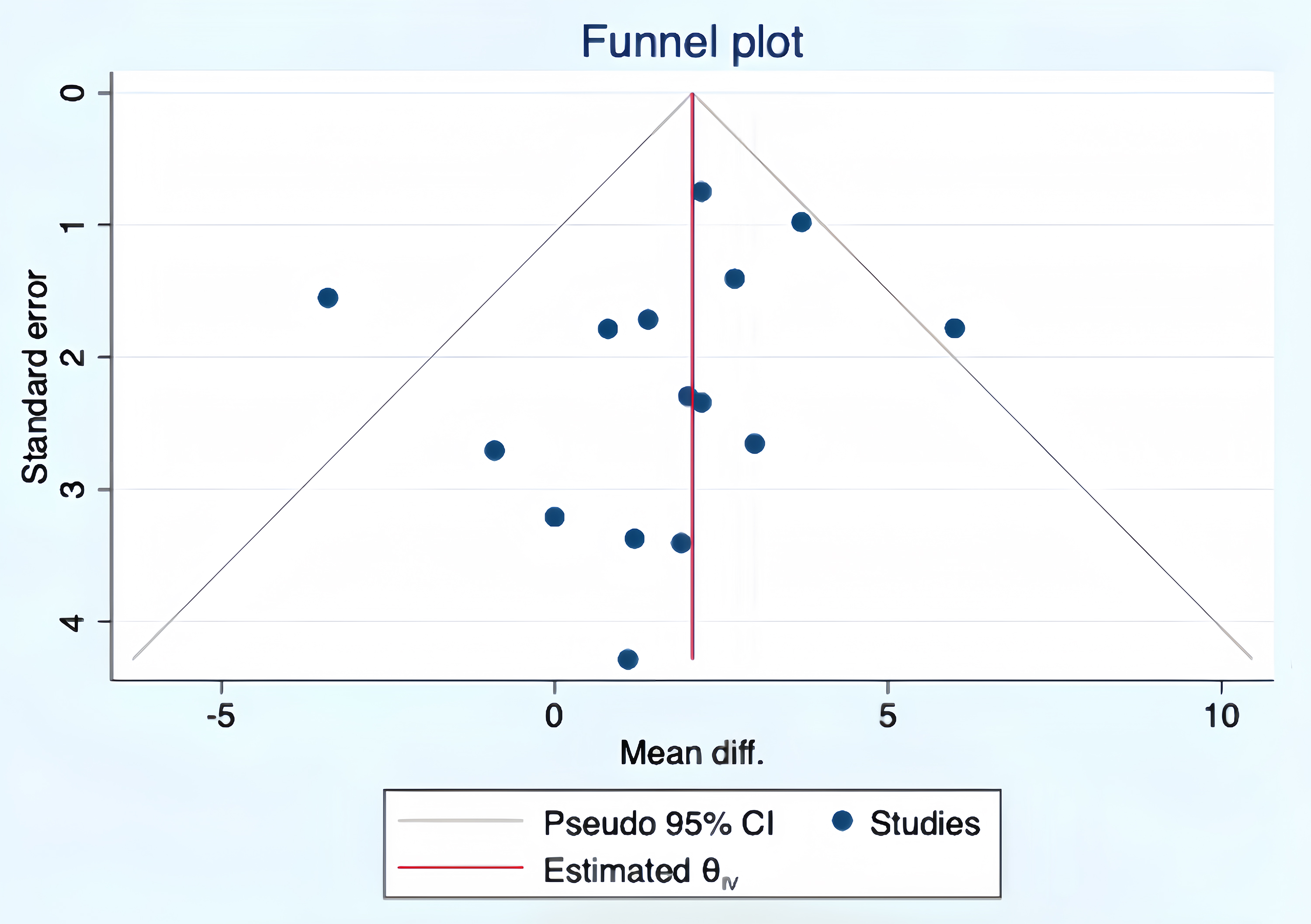 Fig. 4.
Fig. 4.
Funnel plot of the intervention effects of aerobic exercise on Peak VO2 in postoperative CHD patients. CI, confidence interval; IV, inverse variance; diff, difference; VO2, oxygen consumption; CHD, congenital heart disease.
According to GRADEPro, there were no deductions in terms of limitations, inconsistency, indirectness, imprecision, and publication bias of this study. Therefore, the quality of evidence was graded as high (Table 6). The above results suggested that the intervention effects of aerobic exercise on Peak VO2 in postoperative CHD patients is likely close to reality.
| Outcome | Included studies | Quality of evidence assessment | Quality | ||||
| Limitation | Inconsistency | Indirectness | Imprecision | Publication bias | |||
| Peak VO2 | 15 | Not serious | Not serious | Not serious | Not serious | Not serious | High |
GRADE, Grading of Recommendations, Assessment, Development and Evaluation; VO2, oxygen consumption.
In the study by Sandberg et al. 2018 [20], one participant experienced discomfort and arrhythmia during exercise training, leading to the cessation of exercise. However, no arrhythmia was observed in subsequent exercise tests and dynamic electrocardiograms. Apart from this event, no other exercise-related adverse events occurred.
The results of this study showed that aerobic exercise can improve Peak VO2 in postoperative CHD patients. A MD of 2.14 in Peak VO2 was observed. This change indicated that even a slight increase in Peak VO2 may signify a significant improvement in cardiopulmonary function and exercise capacity in CHD patients [21]. Therefore, the increase of Peak VO2 not only provides clinicians with a valuable indicator for assessing patient prognosis but also offers valuable guidance for developing personalized treatment plans and exercise prescriptions. The meta-analysis results of Li et al. 2019 [34] also supported this conclusion (MD = 1.96). Additionally, the result validated the study by Gomes-Neto et al. 2016 [34, 35], indicating the effectiveness of aerobic exercise intervention on Peak VO2 in child, adolescent, or adult postoperative CHD patients. Meyer et al. 2020 [36] suggested that unsupervised home-based aerobic exercise can improve Peak VO2 in postoperative CHD patients, aligning with the results of this study. Although the mechanism by which exercise increases Peak VO2 remains unclear, exercise has been proven to improve peripheral muscle function [37], enhance autonomic nervous system regulation, increase vagal activity, inhibit sympathetic activation, and reduce levels of angiotensin and renin, thereby improving cardiopulmonary function [34].
Our study included a total of 15 RCTs (762 patients) for a systematic review and analysis of the intervention effects of aerobic exercise on Peak VO2 in postoperative CHD patients. Included studies were quality-assessed by the PEDro scale, with an average score of 6.75 points. There were no low-quality studies found, indicating satisfactory quality of the overall included studies. There appeared to be no noticeable publication bias. I2 = 36%, after subgroup analysis, it was found that the patients’ age, modes of supervision, types of exercise, the total dose of exercise, intervention periods, and types of CHD might be sources of heterogeneity; sensitivity analysis revealed that intervention periods and modes of supervision could be sources of heterogeneity. The quality of evidence evaluation had no deductions for limitations, inconsistency, indirectness, imprecision and publication bias. Overall, the intervention effects of aerobic exercise on Peak VO2 in postoperative CHD patients were classified under high quality evidence. In addition, this study has certain limitations. There was certain heterogeneity among exercises with different types, frequencies, intensities, durations, and periods, which may affect the overall effect size and subgroup analyses. Besides, it was difficult to implement complete blinding in exercise interventions, and there was diversity in the patients’ conditions and stages of recovery.
In this study, it was found that for adult patients aged 18 and above,
supervised aerobic exercise combined with resistance training, implemented for
10–12 weeks with a total dose of exercise
The results of this study also demonstrated that there was no significant difference in intervention effects of aerobic exercise on the ToF subgroup. Williams et al. (2020) [40], in their meta-analysis, arrived at the same conclusion. However, among included studies, results of 4 RCTs by Ávila et al. (2016) [22, 23, 28, 29] all indicated a significant intervention effect of aerobic exercise on Peak VO2 in postoperative ToF patients, with only Novaković et al. (2018) [29] expressing disagreement. The reason for the non-significant intervention effect of aerobic exercise on the ToF subgroup in this study may be attributed to insufficient sample size, necessitating further high-quality RCTs for clarification.
In summary, aerobic exercise could significantly improve Peak VO2 in postoperative CHD patients. For patients aged 18 and above, a 10–12 weeks supervised intervention integrating aerobic exercise with resistance training, with a total exercise dosage of at least 1440 minutes, yielded better results. Current evidence of included studies suggests that aerobic exercise is significant and safe for enhancing Peak VO2 in postoperative CHD patients. Despite certain limitations, our study provided evidence-based medicine for the exercise rehabilitation of postoperative CHD patients. Finally, we look forward to further research in this area to explore the intervention effects and mechanisms of exercise on postoperative CHD patients with different conditions and at different stages of recovery.
CHD, congenital heart disease; RCTs, randomized controlled trials; MD, mean difference; SMD, standard mean difference; CI, confidence interval; AEPC, Association for European Paediatric and Congenital Cardiology; ISACHD, International Society for Adult Congenital Heart Disease; ToF, Tetralogy of Fallot; CPET, Cardiopulmonary Exercise Test.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
XG, YS, LY, and HL designed the research study. XG and LY performed the research. YS and LY acquired and interpreted the data. LY and HL analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.