

1 Chinese Academy of Medical Sciences, Peking Union Medical College, National Center for Cardiovascular Diseases, Fuwai Hospital, 100037 Beijing, China
†These authors contributed equally.
Abstract
Backgrounds: Hematocrit is found an independent risk factor for acute
kidney injury (AKI) in certain patients, but this effect in patients with acute
myocardial infarction (AMI) is unclear. We aim to identify the relationship
between hematocrit and AKI in patients with AMI. Methods: The patient
data for the discovery and validation cohorts were extracted from the electronic
Intensive Care Unit database and the Medical Information Mart for Intensive Care
III database, respectively, to identify the relationship between hematocrit and
AKI. With normal hematocrit as the reference, patients were divided into five
groups based on the initial hematocrit value. The primary outcome was AKI during
hospitalization. A multivariable logistic regression and a marginal effect
analysis were used to evaluate the relationship between hematocrit and AKI.
Results: In this study, a total of 9692 patients diagnosed with AMI were
included, with 7712 patients in the discovery cohort and 1980 patients in the
validation cohort. In the discovery cohort, hematocrit in 30–33%, 27–30% or
Keywords
- acute myocardial infarction
- acute kidney injury
- hematocrit
- logistic regression
- marginal effect
Acute kidney injury (AKI) frequently arises as a complication during the hospitalization of patients experiencing acute myocardial infarction (AMI) [1]. Numerous studies have elucidated a robust correlation between cardiac and renal function, underscoring AKI as an independent risk factor for mortality in AMI patients [2, 3, 4]. Regrettably, as of now, no established therapeutic interventions have demonstrated efficacy in improving outcomes for patients afflicted with AKI [5]. While renal replacement therapy (RRT) serves as a crucial intervention for severe AKI, its application is hindered by potentially life-threatening complications and limited accessibility in certain regions and healthcare settings [6]. Consequently, there is an imperative need to identify opportunities for preventing AKI within this clinical context.
Hematocrit (HCT) is a vital parameter that quantifies the percentage of red blood cells in the total blood volume, which plays a pivotal role in determining blood viscosity and regulating blood flow [7]. Previous investigations have elucidated an inverse correlation between HCT levels and the incidence of AKI among patients undergoing on-pump cardiac surgery [8, 9, 10]. Moreover, a reduced HCT has been recognized as an independent predictor of deterioration in renal function [11]. However, the association between HCT and AKI in individuals with AMI remains unexplored. The objective of this study was to assess whether reduced HCT was associated with an increased risk of AKI in patients with AMI.
The discovery cohort for our study consisted of patients selected from the electronic Intensive Care Unit Collaborative Research Database (eICU, version 2.0), which is a comprehensive database containing detailed information from multiple intensive care units (ICUs). The database includes data from over 200,000 ICU admissions that took place between 2014 and 2015 in 208 hospitals across the United States [12]. The validation cohort data were obtained from the Medical Information Mart for Intensive Care III (MIMIC-III, version 1.4), which is an extensive database containing the medical records of 60,000 intensive care unit (ICU) patients treated at the Beth Israel Deaconess Medical Center in Boston, Massachusetts, USA, from 2001 to 2012 [13]. In the context of routine clinical activities, all data are systematically acquired by computerized means, obviating the direct involvement of medical personnel in the data collection process. One author (LL) completed a web course titled “Protecting Human Research Subjects” offered by the National Institutes of Health, and obtained the corresponding certificate (ID: 35965741). Possessing the requisite qualifications, LL is duly authorized to initiate inquiries into the information repositories. It is noteworthy that the establishment of the databases received explicit approval from the Massachusetts Institute of Technology, granted under an exemption for informed consent.
We analyzed data from consecutive patients aged 18 years or older who were
diagnosed with AMI. All patients received Guideline-Directed Medical Therapy. The
definition of AMI was based on the clinical practice guideline [14]. AKI was
diagnosed using the criteria proposed by Kidney Disease: Improving Global
Outcomes. These criteria include an increase in serum
creatinine (SCr) by
Patients’ data, including demographics (age, gender, race, weight), vital signs (temperature, blood pressure, heart rate, respiratory rate, UO), common comorbidities (congestive heart failure, hypertension, diabetes, chronic pulmonary obstructive disease, sepsis, renal disfunction, hepatic disfunction, stroke, cancer), and laboratory tests results (white blood cell count, red blood cell count, HCT, hemoglobin, platelet count, serum sodium, serum potassium, serum calcium, serum chloride, serum glucose, serum creatine kinase, serum aniongap, serum bicarbonate, SCr, blood urine nitrogen) were included in the initial analysis. In the two public databases, for patients with multiple ICU admissions, only the data from the first ICU admission were selected for analysis.
The principal determinant examined in this analysis was the initial HCT level
upon hospitalization. The categorization of HCT was performed in accordance with
the World Health Organization’s definition of anemia [16], stratifying it into
five groups: (1) normal range (HCT
We aimed to identify the relationship between HCT and renal dysfunction in patients with AMI. The main outcome of interest was AKI during hospitalization. The secondary outcomes included RRT and hospital mortality.
The assessment of data normal distribution was conducted utilizing the
Kolmogorov-Smirnov test. Continuous variables were presented as mean
Multivariable logistic regression analysis employing stepwise backward selection
methodology was employed for covariate adjustment, incorporating variables
identified to exhibit marginal association (p
The discovery cohort consisted of a total of 7712 AMI patients. Among them, 950
patients (12.3%) experienced AKI during hospitalization (Supplementary
Table 1). In short, mean age was 65.0
| Variables | Discovery cohort (n = 7712) | Validation cohort (n = 1980) | |||||
| AKI | Non-AKI | p value | AKI | Non-AKI | p value | ||
| (n = 950) | (n = 6762) | (n = 279) | (n = 1701) | ||||
| Age, years | 68.4 |
64.5 |
72.3 |
67.1 |
|||
| UO, mL/kg/h | 0.87 |
1.13 |
0.87 |
1.18 |
|||
| RR, bpm | 21 |
19 |
20 |
18 |
|||
| MAP, mmHg | 76.9 |
78.5 |
74.6 |
77.8 |
|||
| Heart rate, bpm | 94 |
85 |
88 |
84 |
|||
| SpO |
96.4 |
97.0 |
96.8 |
97.2 |
0.028 | ||
| AMI | |||||||
| STEMI | 266 (28.0) | 3678 (54.4) | 105 (37.5) | 899 (52.8) | |||
| NSTEMI | 684 (72.0) | 3084 (45.6) | 174 (62.5) | 802 (47.2) | |||
| Invasive strategy | |||||||
| PTCA + CAG | 201 (21.2) | 3251 (48.1) | 89 (31.9) | 755 (44.4) | |||
| CAG | 116 (12.2) | 1310 (19.4) | 31 (11.1) | 336 (19.8) | |||
| CHF, % | 264 (27.8) | 685 (10.1) | 158 (56.6) | 558 (32.8) | |||
| VA, % | 79 (8.3) | 319 (4.7) | 42 (15.1) | 299 (17.6) | 0.301 | ||
| COPD, % | 111 (11.7) | 357 (5.3) | 41 (14.7) | 182 (10.7) | 0.050 | ||
| Sepsis, % | 328 (34.5) | 419 (6.2) | 52 (18.9) | 83 (4.9) | |||
| CKD, % | 215 (22.6) | 552 (8.2) | 40 (14.3) | 70 (4.1) | |||
| Anemia, % | 432 (45.5) | 1336 (19.7) | 111 (39.8) | 392 (23.0) | |||
| WBC, × 10 |
14.2 |
11.6 |
13.8 |
12.4 |
|||
| Potassium, mmol/L | 4.52 |
4.06 |
4.33 |
4.19 |
0.006 | ||
| SCr, mg/dL | 2.40 |
1.27 |
1.89 |
1.16 |
|||
| BUN, mg/dL | 41.3 |
21.1 |
39.5 |
21.3 |
|||
| Hematocrit, % | 36.4 |
39.5 |
31.7 |
33.7 |
|||
| HCT |
109 (11.5) | 270 (4.0) | 47 (16.8) | 164 (9.6) | |||
| 27 |
89 (9.4) | 270 (4.0) | 45 (16.1) | 185 (10.9) | |||
| 30 |
123 (12.9) | 457 (6.8) | 44 (15.8) | 250 (14.7) | |||
| Mild reduction | 217 (22.8) | 1240 (18.3) | 82 (29.4) | 268 (33.4) | |||
| Normal | 412 (43.3) | 4525 (66.9) | 61 (21.9) | 534 (31.4) | |||
AKI, acute kidney injury; UO, urine output; RR, respiratory rate; MAP, mean
aortic pressure; SpO
A multivariable logistic regression analysis was conducted to
investigate the correlation between HCT and AKI. In the unadjusted model,
low HCT was found to be significantly associated with an
increased risk of AKI in AMI patients, with OR of 1.876 (95% CI: 1.572–2.238,
p
| Variables | Non-adjusted | Model 1 | Model 2 | ||||
| OR | p value | OR | p value | OR | p value | ||
| Discovery cohort | |||||||
| Normal | Ref. | Ref. | Ref. | ||||
| HCT |
4.399 (3.446–5.615) | 2.828 (2.088–3.828) | 2.502 (1.467–4.266) | 0.001 | |||
| 27 |
3.592 (2.770–4.657) | 2.051 (1.460–2.880) | 1.802 (1.115–2.911) | 0.016 | |||
| 30 |
2.933 (2.346–3.665) | 2.023 (1.527–2.680) | 1.739 (1.178–2.566) | 0.005 | |||
| Mild reduction | 1.876 (1.572–2.238) | 1.484 (1.192–1.848) | 1.334 (0.998–1.783) | 0.051 | |||
| Validation cohort | |||||||
| Normal | Ref. | Ref. | Ref. | ||||
| HCT |
2.509 (1.651–3.813) | 1.843 (1.182–2.873) | 0.007 | 1.613 (1.022–2.552) | 0.039 | ||
| 27 |
2.129 (1.399–3.240) | 1.818 (1.173–2.818) | 0.007 | 1.660 (1.051–2.618) | 0.030 | ||
| 30 |
1.541 (1.017–2.335) | 0.042 | 1.120 (0.771–1.867) | 0.420 | 1.078 (0.654–1.802) | 0.699 | |
| Mild reduction | 1.263 (0.889–1.797) | 0.192 | 1.240 (0.862–1.785) | 0.246 | 1.182 (0.782–1.767) | 0.401 | |
Model 1: age, respiratory rate, mean aortic pressure, heart rate, saturation of pulse oxygen; Model 2: age, urine output, respiratory rate, mean aortic pressure, heart rate, saturation of pulse oxygen, ventricular arrhythmia, chronic obstructive pulmonary disease, sepsis, chronic kidney disease, anemia, white blood cell, potassium, creatinine, blood urea nitrogen, coronary angiography. OR, odds ratios; HCT, hematocrit.
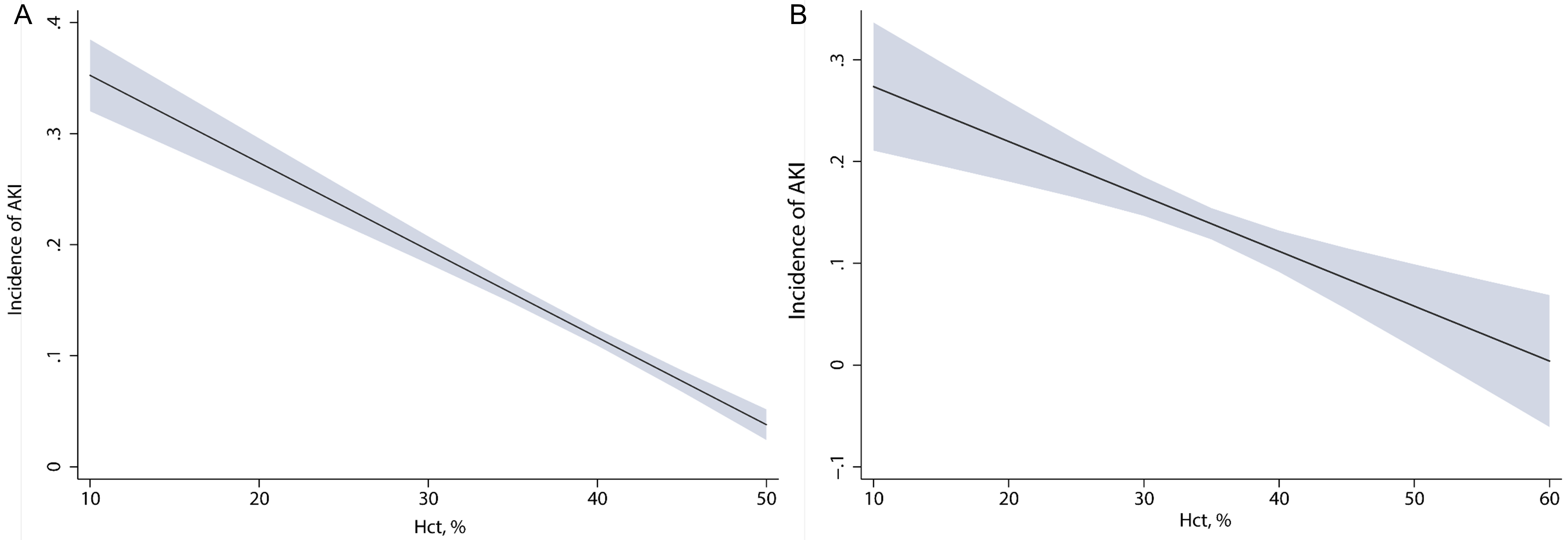
The marginal effect analysis was employed to evaluate the association between HCT and AKI. Our findings revealed a clear negative linear correlation between HCT and AKI (Fig. 1A). With an increase in the initial HCT upon ICU admission, there was a linear decline in the probability of AKI. In the validation cohort, the linear relationship between HCT and AKI was also found in the marginal effect analysis (Fig. 1B).
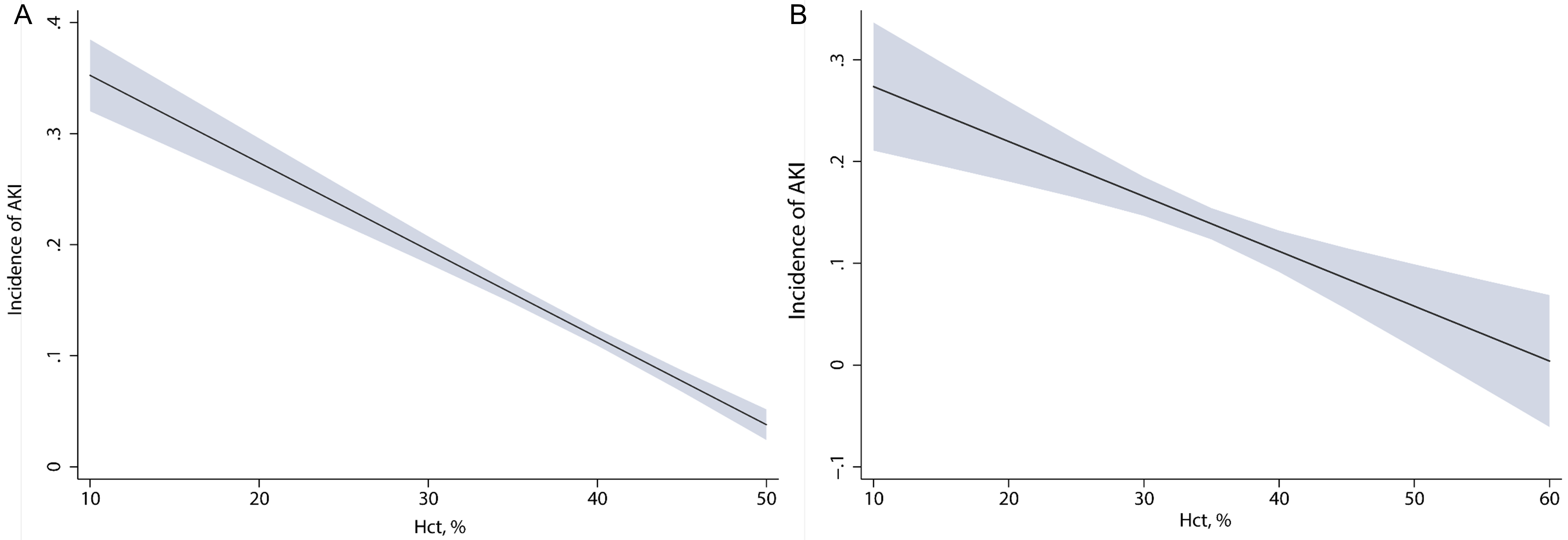 Fig. 1.
Fig. 1.Relationship between initial HCT and risk of AKI evaluated by marginal effect analysis in patients with AMI. (A) Marginal effect in the discovery cohort. (B) Marginal effect in the validation cohort. HCT, hematocrit; AKI, acute kidney injury; AMI, acute myocardial infarction.
As shown in Supplementary Fig. 1, after adjusting for the 17 variables
in the logistic model, low HCT was found to be significantly associated with
hospital mortality. The OR for HCT between 27–30% and below 27% were 1.557
(95% CI: 1.007–2.407, p = 0.047) and 1.755 (95% CI: 1.169–2.634, p = 0.007),
respectively. Furthermore, in the multivariate logistic model, there was a
significant association between low HCT and the need for RRT during
hospitalization. The OR for HCT levels in mild reduction, 30–33%, 27–30%, and
below 27% were 2.353 (95% CI: 1.510–3.670, p
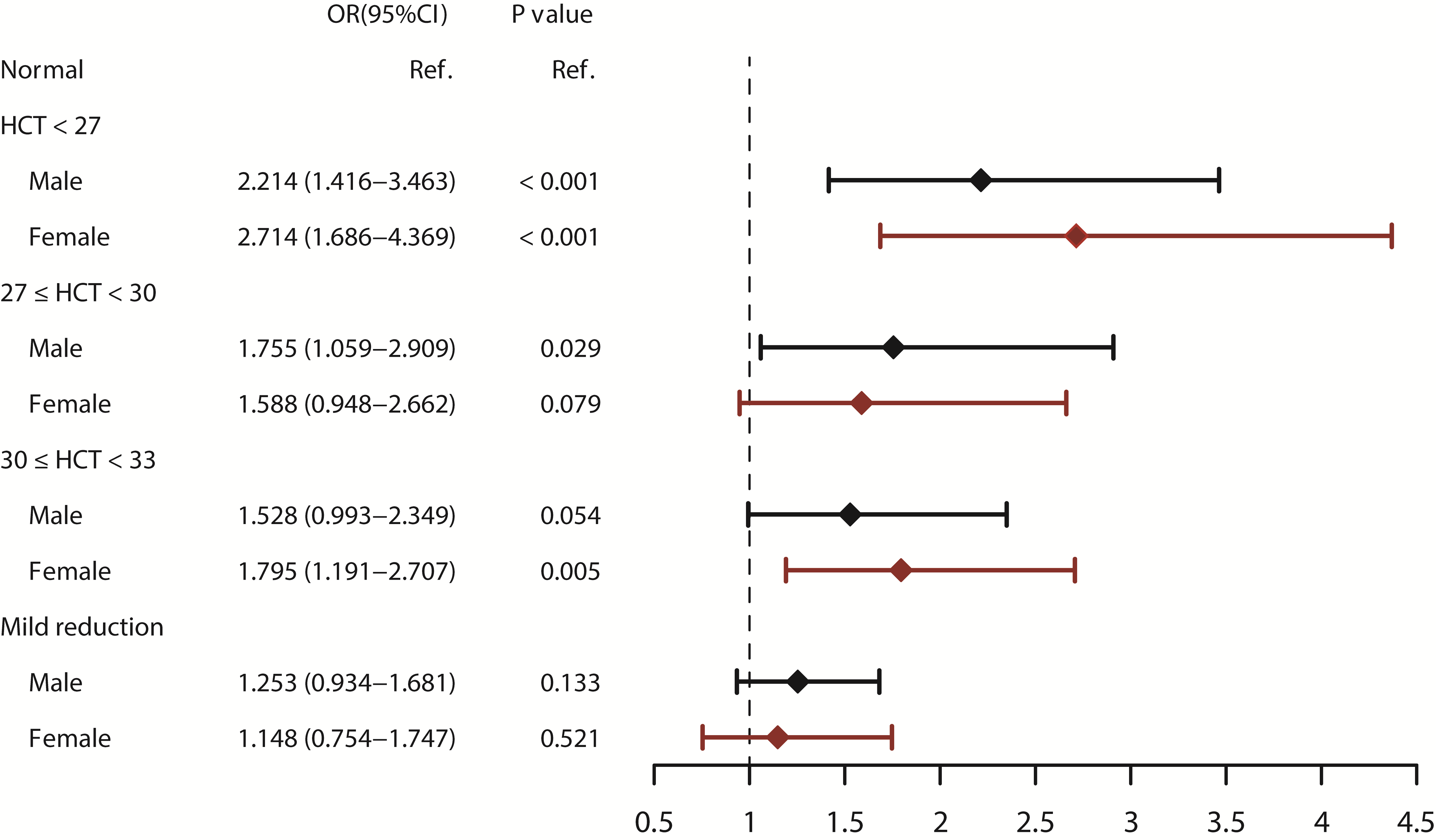
In order to reduce a possible sex stratification effect, we performed a subgroup
analysis separated by sex. After adjusting for other variables
in the multivariate logistic model, HCT below 27% was independently associated
with an increased risk of AKI in both male and female patients. The OR in male
patients was 2.214 (95% CI: 1.416–3.463, p
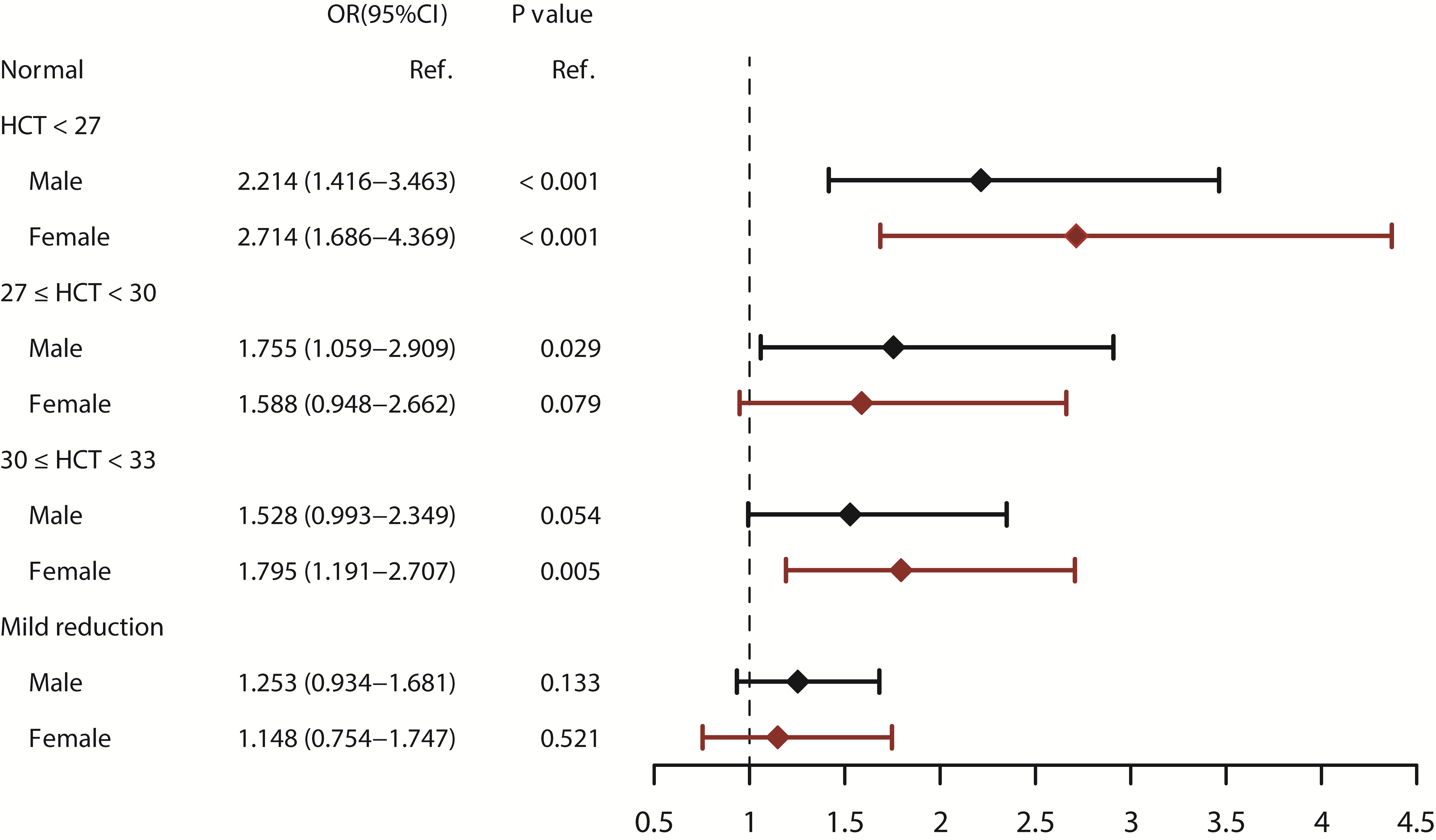 Fig. 2.
Fig. 2.Subgroup analysis of sex on the relationship between HCT and AKI assessed by the multivariate logistic regression. HCT, hematocrit; AKI, acute kidney injury.
This study aimed to investigate the association between HCT and the occurrence of AKI in AMI patients. We found that HCT was negatively associated with AKI, and the correlation was approximately linear. Furthermore, this correlation was consistent across genders, as low HCT was strongly associated with AKI in both male and female patients. Additionally, low HCT was found to be an independent risk factor for RRT during hospitalization and hospital mortality.
HCT, defined as the percentage of blood volume comprised of red blood cells, serves as a pivotal factor influencing various physiological parameters. It significantly contributes to the regulation of whole blood viscosity, blood pressure, venous return, cardiac output, and platelet adhesiveness [18, 19, 20]. As HCT rises, the blood viscosity increases rapidly, and vice versa. Therefore, HCT could be used as a reference for fluid infusion. Additionally, HCT is considered one of the most precise methods of determining the degree of anemia [21].
From a pathophysiological perspective, the etiology of AKI can be categorized into three overarching classifications: prerenal, characterized by diminished renal perfusion; intrinsic renal, stemming from pathological processes within the glomeruli and tubules; and postrenal, resulting from obstructive conditions in the urinary tract [22]. Prerenal AKI is the predominant form globally [22], and is correlated with diminished renal perfusion and glomerular filtration rate (GFR), attributable to intravascular volume depletion stemming from hypovolemia, peripheral vasodilation, reduced arterial pressures, and compromised cardiac function, culminating in a reduction of cardiac output. Patients with AMI are characterized as acute myocardial ischemia which significantly affects cardiac pump function. Therefore, renal hypoperfusion is common in patients with AMI because of a low cardiac output state, which is also called cardiorenal syndrome [23].
Given the above evidence, low HCT could reflect the reduced effective
circulatory volume, which significantly reduces renal perfusion and induces
prerenal AKI in patients with AMI. Habib et al. [24] have demonstrated that HCT
of cardiopulmonary bypass
Prior investigations have elucidated a sexual dimorphism in the context of HCT
and AKI. Female patients demonstrated a heightened propensity
to experience reduced hematocrit levels compared to their male counterparts,
consequently manifesting an augmented overall susceptibility to AKI following
meticulous adjustment for risk factors [9]. Kang et al. [28] attributed this
phenomenon to the protective effect of estrogen against ischemic injury.
Furthermore, Mehta et al. [8] proposed that menstruation, coupled with its
concomitant blood loss, may afford women the capacity to optimize oxygen
extraction and delivery to tissues even at reduced systemic HCT levels. However,
Brescia et al. [10] found no sex-related differences in the effect of HCT on AKI
in patients who underwent coronary artery bypass grafting. The effect of sex on
the relationship between HCT and AKI is still controversial. In the present
study, we conducted a subgroup analysis stratified by sex, and the results showed
that HCT
While this study represents a comprehensive analysis based on a large-scale cohort and has undergone external validation to substantiate its primary findings, it is essential to acknowledge certain limitations inherent in the current investigation. Firstly, the potential influence of unmeasured confounding factors cannot be definitively excluded. Rigorous methodologies, such as risk adjustment, were employed to address discernible variations in hospital admission characteristics. However, it is imperative to note that the analysis of potential AKI risk factors was confined to the data accessible in the public database. Secondly, due to the presence of missing and extreme data points in the public database, pivotal variables with a notable degree of missing data, including left ventricular ejection fraction and the use of contrast, were regrettably excluded from the analysis. Furthermore, specific imputation methods were applied to address missing data, potentially impacting the robustness of the results. Lastly, it is crucial to recognize the retrospective nature of this cohort study. While external validation provides support for the findings, prospective clinical trials are indispensable to further substantiate and generalize the results. The necessity for prospective investigations is paramount to establish a causal relationship and enhance the clinical applicability of the observed associations.
HCT was an independent risk factor for AKI and hospital mortality in patients with AMI. The relationship between HCT and AKI was negatively linear, and was gender-independent. In addition, HCT was also found an independent risk factor for RRT in these patients.
The datasets used during the current study are available from the corresponding author on reasonable request.
This study was designed by SS and LKZ. ZXZ, YLX, ZHZ, ZH and LL were responsible for data collation and statistical analysis. SS, LKZ, ZXZ and YLX wrote the first draft. ZHZ, ZH, LL and YY reviewed it critically for important intellectual content. YY interpretated the data and reviewed the work. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Given that our research involved a third party, anonymized, and publicly accessible database with prior institutional review board (IRB) consent, there was no need for additional IRB approval from our side and no additional patient’s informed consent is required.
Not applicable.
This research was funded by Clinical and Translational Medicine Research Project of Chinese Academy of Medical Sciences, grant number 2022-LC04.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.