





 , Maurizio Taramasso 3,*
, Maurizio Taramasso 3,*
1 Instituto de Ciências Biológicas e da Saúde, Universidade Federal do Rio Grande do Sul, 90046-900 Porto Alegre, Brazil
2 Cardiac Surgery Department, Hospital Mãe de Deus, 90880-481 Porto Alegre, Brazil
3 Clinic of Cardiac Surgery, HerzZentrum Hirslanden Zurich, 8008 Zurich, Switzerland
Abstract
Tricuspid regurgitation, once considered a relatively benign condition, has now gathered significant attention due to new evidence showing its impact on both short- and long-term follow-up. While surgical intervention remains the established standard approach for treating severe tricuspid regurgitation, current guidelines provide Class I indication for intervention in only a limited set of scenarios. This review delves into the present and future perspectives of surgical tricuspid regurgitation management, examining aspects such as disease prognosis, surgical indications, outcomes, and a comprehensive overview of past and upcoming clinical trials.
Keywords
- tricuspid valve
- tricuspid regurgitation
- surgery
- heart failure
- right ventricle
Tricuspid regurgitation (TR), once deemed a relatively benign condition, has now received significant attention due to its impact on both prognosis and quality of life. Consequently, dedicated congress sessions and task forces have been established to discuss TR prognosis and management. Additionally, numerous studies on new TR interventional approaches have been published.
Despite this, the role of TR surgical intervention remains limited, with only a few scenarios receiving a Class I indication for intervention according to current guidelines [1, 2]. The restricted number of patients undergoing TR surgery, especially for isolated TR, can be attributed to two main factors:
(1) The poor post-operative prognosis, which has remained consistently stable over the last few decades even with ongoing surgical improvements;
(2) The advanced disease stage in which patients with TR are referred for surgery, often in the presence of multi-organ failure.
These factors have compelled the scientific community to explore new technologies capable of addressing TR with a lower procedural risk, providing less invasive alternatives for high surgical risk patients. In this setting, transcatheter tricuspid valve intervention (TTVI) has not only provided a novel alternative for critically ill patients but has also given rise to an entirely new field of research. This includes the development of new clinical trial definitions, disease severity classification, and tailored risk scoring systems [3, 4].
This review addresses the current and future landscape of TR surgical management, focusing on disease prognosis, surgical indications, outcomes, and past and forthcoming clinical trials.
Since the early 1950s, a distinction between organic and functional TR has been established [5]. According to this classification, organic or primary TR (PTR) arises from primary abnormalities in the tricuspid valve (TV) apparatus in the absence of significant left-sided heart disease or pulmonary hypertension (PH) [6]. PTR can be further categorized into degenerative, congenital or acquired etiologies.
Functional or secondary TR (STR) accounts for over 85% of cases and is characterized by tricuspid annular (TA) dilatation and/or leaflet tethering in the setting of right ventricle (RV) remodeling due to pressure and/or volume overload [7, 8] with left-sided heart disease and/or PH being the most prevalent etiologies [9, 10]. A subgroup of patients presents isolated TR due to TA dilation probably attributed to atrial fibrillation (AF) [1].
Besides this standard classification, the Tricuspid Valve Academic Research Consortium (TVARC) document suggested dividing STR into three subcategories as presented in Table 1 (Ref. [11]).
| Causative Disease Process | Etiology | TV/RV Morphology | |
| Primary TR (5%–10%) | |||
| Degenerative disease | Prolapse or flail leaflet | Abnormal leaflet mobility, normal RV | |
| Congenital | Apical displacement of leaflet attachment (i.e., Ebstein’s anomaly) | Abnormal leaflet position, atrialized RV | |
| Acquired (i.e., tumors, trauma, carcinoid, RHD, radiation) | Leaflet injury (i.e., tumor, trauma, biopsy, lead extraction) or infiltration/fibrosis (i.e., carcinoid, rheumatic disease, radiation valvulopathy) | Abnormal leaflet morphology/mobility, normal RV | |
| Secondary TR (80%) | |||
| Ventricular secondary TR | |||
| LV disease | Postcapillary PH (HFpEF, HFrEF) | RV dilatation (spherical remodeling)/dysf- unctional | |
| Left heart valvular disease | Postcapillary PH | ||
| Pulmonary disease | Pre-capillary PH (chronic lung disease, CTEPH, PAH) | ||
| RV dysfunction/remodeling | RV dilatation and dysfunction (i,e., RV infarct, RV dysplasia) | ||
| Atrial secondary TR | |||
| RA/TA dilatation | RA/TA dilatation (i.e., related to age, AF, HFpEF) | RA dilatation/dysfunction | |
| CIED-related TR (10%–15%) | |||
| LTR-A (causative) | Leaflet impingement, perforation, valvular/subvalvular adhesions/restriction | Tricuspid leaflet tethering/adhesions | |
| LTR-B (incidental) | CIED present without TV apparatus interference | Morphology dependent on primary disease process | |
CTEPH, Chronic thromboembolic pulmonary hypertension; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; LTR-A, lead-associated tricuspid regurgitation type A; LTR-B, lead-associated tricuspid regurgitation Type B; LV, left ventricle; PAH, pulmonary arterial hypertension; PH, pulmonary hypertension; RHD, rheumatic heart disease; RA, right atrial; RV, right ventricular; TA, tricuspid annular; TR, tricuspid regurgitation; STR, Functional or secondary TR; TVARC, Tricuspid Valve Academic Research Consortium; TV, tricuspid valve; AF, atrial fibrillation; CIED, cardiac implantable eletronic device. Adapted from Hahn et al. [11]
A community-based study by Topilsky et al. [12] revealed that
significant (at least moderate) TR is present in 0.55% of the population, with a
higher prevalence in the female sex. TR prevalence significantly increased with
age, reaching approximately 4% in patients over 75 years old [12]. These
findings reinforced previous data from the Framingham Heart Study, which
demonstrated that for
In patients with degenerative mitral regurgitation (MR), the prevalence of
hemodynamically significant TR was reported to be around 30% at the time of
mitral valve (MV) surgery. Additionally, up to a third of patients with
significant mitral stenosis exhibit TR. Nonetheless, up to 40% of patients
undergoing MV surgery develop significant TR late after surgery. The
pre-existence of TA dilation (diameter
Severe TR is associated with a dismal prognosis, leading to progressive RV dysfunction, renal and liver failure, chronic right HF, and the need for increasing doses of diuretics [11].
It has been suggested that the clinical impact of TR is directly proportional to
its degree, with moderate/severe TR associated with a 2-fold increase in
mortality compared to no/mild TR, irrespective of pulmonary pressures and right
HF [20]. In a retrospective study involving 5223 patients, Nath et al.
[6] demonstrated that
Similarly, in another retrospective analysis, individuals with moderate and
severe TR exhibited a 2.0- to 3.2-fold increased risk of all-cause long-term
mortality, even after adjusting for age and sex, compared to those with
no/trivial TR (p
From a clinical standpoint, TR patients often exhibit progressive signs of right HF, such as peripheral edema, fatigue, exercise intolerance, weight gain, hepatic dysfunction, ascites, and cardiac cachexia, irrespective of the underlying condition [22].
Identifying predictors of outcomes and discriminating patients who are responders or non-responders to TR intervention is of paramount importance in guiding the decision-making process for TR surgical management [23].
Indications for TR surgical intervention, according to current American and European guidelines, are presented in Fig. 1 (Ref. [1, 2]). Selected patients should receive a TV repair at the time of the left-sided valve lesions surgery to address severe TR or to prevent later severe TR development in the presence of progressive TR. The rationale behind this recommendation is the understanding that severe TR may not reliably improve after left-sided lesion treatment and RV afterload reduction. In this context, a combined intervention would not increase the operative risk and could promote RV reverse remodeling and improved functional status, especially in the presence of TA dilatation. As an isolated procedure, TV surgery should be considered for selected patients with PTR or STR attributed to TA dilation, in the absence of PH or dilated cardiomyopathy. For PTR, surgery is recommended for symptomatic patients with severe regurgitation. In selected asymptomatic or mildly symptomatic patients deemed suitable for surgery, intervention should also be contemplated when RV dilatation or declining RV function is observed [1, 2].
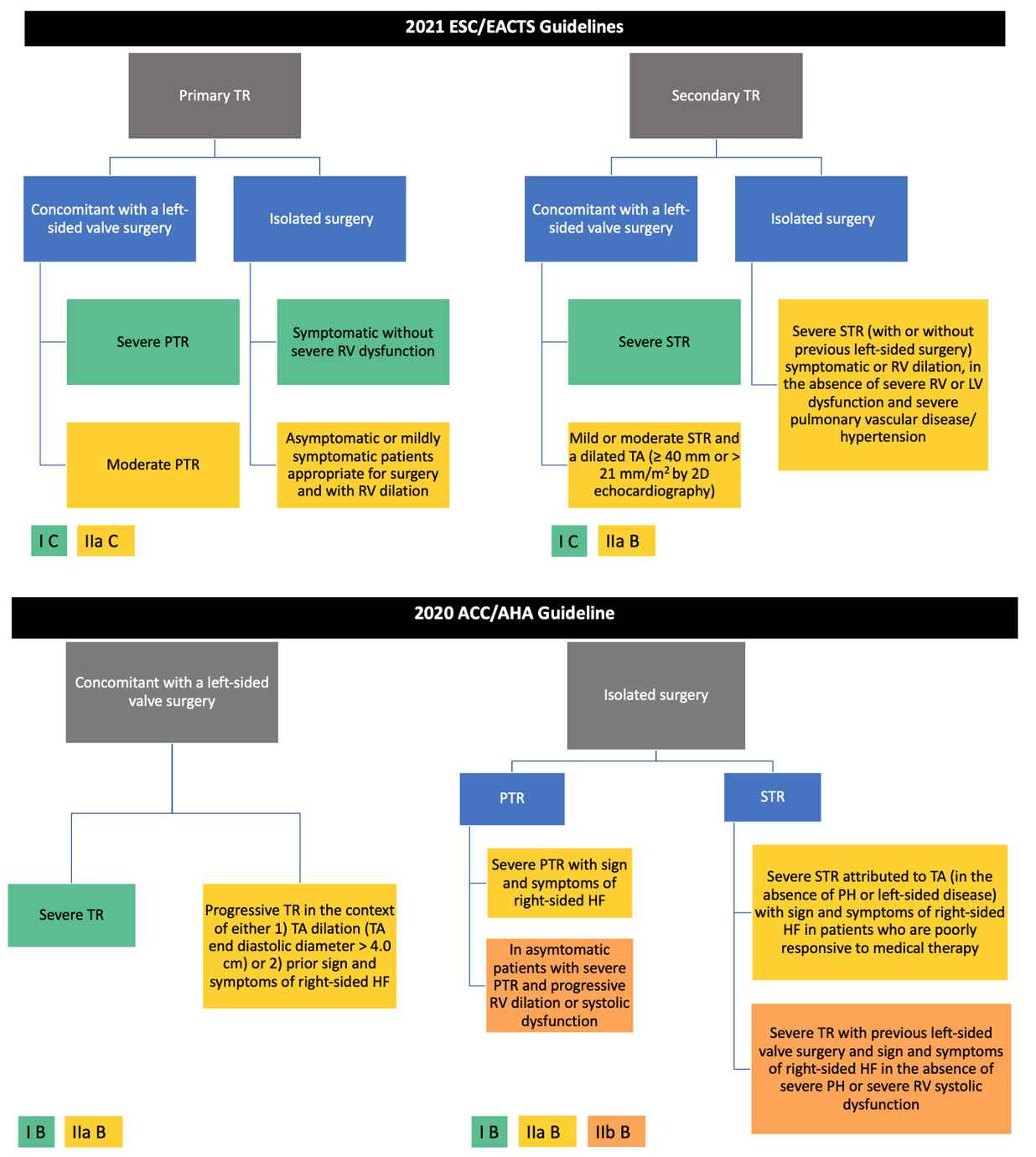 Fig. 1.
Fig. 1.Current indication for TR surgical intervention according to European and American guidelines [1, 2]. ESC, European Society of Cardiology; EACTS, European Association for Cardiothoracic Surgery; ACC/AHA, American College of Cardiology/American Heart Association; TR, tricuspid regurgitation; PTR, primary tricuspid regurgitation; RV, right ventricle; LV, left ventricle; STR, secondary tricuspid regurgitation; TA, tricuspid annular.
TV reoperation for new-onset or worsening STR after left-sided surgery carries a high procedural risk, possibly due to late referral and subsequent poor clinical condition. The perioperative mortality rate for reoperation in the presence of severe, isolated TR after left-sided valve surgery is reported to be between 10% and 25% [1]. The surgical treatment should be considered if there are signs of RV dilatation or decline in RV function, after excluding left-sided valve dysfunction, severe RV or LV dysfunction, and severe pulmonary vascular disease/PH [1].
Although this article primarily delves into the surgical management of acquired TR, it is worth mentioning that in cases of congenitally dysplastic TVs, the Cone’s reconstruction technique, as described by da Silva et al. [24], stands as the standard approach for treating both pediatric patients and adults with Ebstein’s anomaly.
Severe isolated TR surgery historically carries a high mortality rate, ranging from 8% to 20% [25]. To improve these numbers and avoid operating on patients in a late disease stage, there has been a renewed interest in earlier surgery for patients with severe isolated TR before the onset of severe RV dysfunction or end-organ damage.
According to Sala et al. [26], patients who underwent isolated TV
surgery in early disease stages (Stages 2 and 3, see Fig. 2 (Ref. [26])), without
prominent symptomatology, RV dilation or dysfunction, and organ involvement, were
more likely to receive TV repair than replacement. They exhibited lower
in-hospital mortality, fewer postoperative complications, shorter postoperative
lengths-of-stay, and also experienced a 100% 5-year survival with no further HF
rehospitalizations. Conversely, patients in advanced disease stages (Stages 4 and
5) had higher in-hospital mortality (15.3%), higher postoperative complications
rate (acute kidney injury: 3.7–10% vs. 44–100%, p
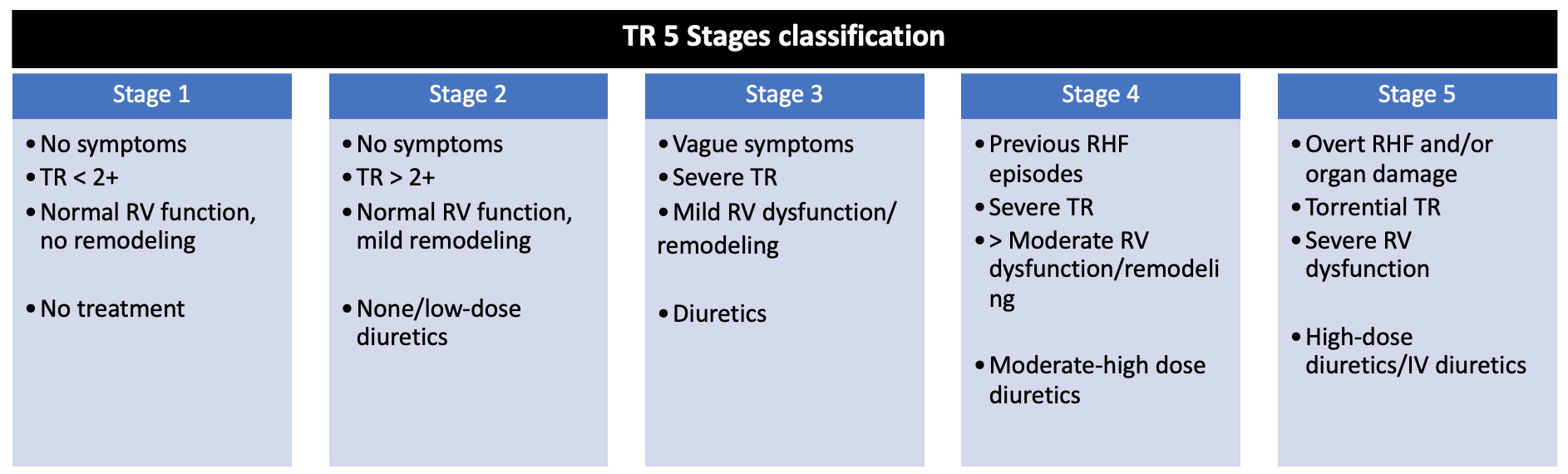 Fig. 2.
Fig. 2.TR 5 stages classification. Adapted from Sala et al. [26]. IV, intravenous; RHF, right heart failure; RV, right ventricle; TR, tricuspid regurgitation.
In the context of STR, Dreyfus et al. [15] proposed a comprehensive
approach considering not only TR severity but also TA dilation, the mode of
tricuspid leaflet coaptation, and tricuspid leaflet tethering. Recommendations
for intervention would vary according to the disease stage. In Stage 1 (no or
mild TR, TA 40 mm, and normal leaflet coaptation), TR intervention would not be
indicated. In Stage 2 (mild or moderate TR, TA
To better evaluate the role of concomitant TR intervention based on TA dilation,
a sequence of randomized clinical trials (RCT) were conducted (Table 2, Ref.
[19, 29, 30, 31]). In the first trial, Benedetto et al. [19] showed that
patients with
| Study | Publication year | Number of patients | Patient population | Primary endpoint | Follow-up | Main results |
| Benedetto et al. [19], RCT | 2012 | 44 patients (22 concomitant intervention vs. 22 control group) | MV surgery indication with |
Moderate to severe ( |
1-year | New onset of moderate to severe STR: 0% vs. 28%, p = 0.02; |
| TR absent: 71% vs. 19%, p = 0.001; | ||||||
| 6-minute walk test: +115 | ||||||
| 30-day mortality: 4.4% vs. 4.4% | ||||||
| Song et al. [29], RCT | 2016 | 100 patients (50 concomitant intervention vs. 50 control group) | MV replacement indication with mild TR | TR degree; | 2-year | TR absent: 35 vs. 20 cases; Mild TR: 13 vs. 21 cases; Mild-to-moderate TR: 2 vs. 3 cases; |
| Survival | Moderate TR: 0 vs. 6 cases, p | |||||
| Survival rate: 97.0% vs. 85.6%, p | ||||||
| Pettinari et al. [30], Single-center RCT | 2019 | 106 patients (53 concomitant intervention vs. 53 control group) | MV surgery indication and less-than severe STR (vena contracta |
Freedom from |
5-year | Freedom from |
| Freedom from severe TR; | Freedom from severe TR: 100% vs. 87.4%, p | |||||
| TR progression (increase |
TR progression: 0% vs. 17.6%, p | |||||
| Freedom from cardiac-related mortality: 94.1% vs. 89.7%, p = 0.9 | ||||||
| Gammie et al. [31], Multicentre RCT | 2022 | 401 patients | Degenerative severe MR with moderate or less-than-moderate TR and TA dilatation ( |
TR reoperation, TR progression by 2 grades from baseline or the presence of severe TR, or death | 2-year | Combined endpoint: 3.9% vs. 10.2%, p = 0.02; |
| (198 concomitant intervention vs. 203 control group) | Mortality: 3.2% vs. 4.5%; | |||||
| TR progression: 0.6% vs. 6.1% |
RCT, randomized clinical trial; MV, mitral valve; TV, tricuspid valve; TR, tricuspid regurgitation; TA, tricuspid annular; STR, secondary tricuspid regurgitation.
Despite these initial promising results, Pettinari et al. [30] suggested that in patients with less-than severe STR submitted to a TV repair at the time of MV surgery, long-term TR recurrence occurred irrespective of baseline TA dilation. Several echo parameters such as functional capacity, RV ejection fraction, RV end-systolic volume, and RV end-diastolic volume also remained similar in patients who underwent or not have a TV repair [29]. In this same line, another RCT conducted by The Cardiothoracic Surgical Trials Network (CTSN) investigators showed that in patients with severe degenerative MR and moderate or less-than-moderate TR with TA dilatation, the primary composite endpoint occurred almost exclusively in patients with moderate TR at baseline and not in those with less-than-moderate TR and TA dilatation. Nevertheless, concomitant TV surgery increased cardiopulmonary bypass time by an average of 34 minutes and resulted in a high permanent pacemaker implantation rate (14.1%) due to iatrogenic atrioventricular block [31].
In an attempt to better understand the impact of leaving
Following these trials, two meta-analysis showed that in patients with
TV surgical technique should be tailored to individual patient characteristics, disease stage, and anatomical considerations.
For STR treatment, Kay et al. [35] introduced a repair technique in 1965 using a 1–0 silk suture placed through the posterior leaflet, resulting in this leaflet exclusion. This technique, known as ‘bicuspidization’, had a high TR recurrence as it did not address the tendency of the anterior annulus to dilate. Seeking to stabilize the TA, De Vega proposed a suture semicircular annuloplasty technique, aiming to reduce the amount of intracardiac prosthetic material, enhance annular flexibility, and minimize the risk of conduction system injury [36]. Some years later, Carpentier introduced the concept of a prosthetic ring to reinforce the TA [37]. Annuloplasty rings offer several technical advantages over suture annuloplasty, including better tension distribution in the suture line, more standardized annular reduction, and the ability to differentially plicate an asymmetrically dilated annulus. Moreover, ring annuloplasty is easier to master and more reproducible, resulting in less residual or recurrent TR. The ring’s size is generally chosen by measuring the distance from the anteroseptal to the posteroseptal commissures and is implanted starting posteriorly (at the midpoint of the septal leaflet) and, then, proceeding counterclockwise.
Currently, three main devices are employed during TV annuloplasty: standard rigid rings, which were predominant in the 1990s; flexible bands, increasingly employed from the early 2000s; and 3-dimensional (3D) rigid rings in recent years [38]. Flexible bands allow for the natural physiological motion of the TA throughout the cardiac cycle, offering improved flexibility, a simpler design and implantation technique, and lower risks of device breakages and tricuspid stenosis. They also better preserve RV function and assist in RV functional recovery after surgery [39, 40, 41]. In contrast, 3D rings are designed to accommodate the saddle-shaped TV annulus. Another technique that may be applied in case of severe TA dilatation associated with leaflet tethering is anterior leaflet pericardial patch augmentation [42].
Fig. 3 (Ref. [43, 44]) and Fig. 4 (Ref. [45]) show different techniques used to surgically repair STR [43, 44] or isolated TR [45].
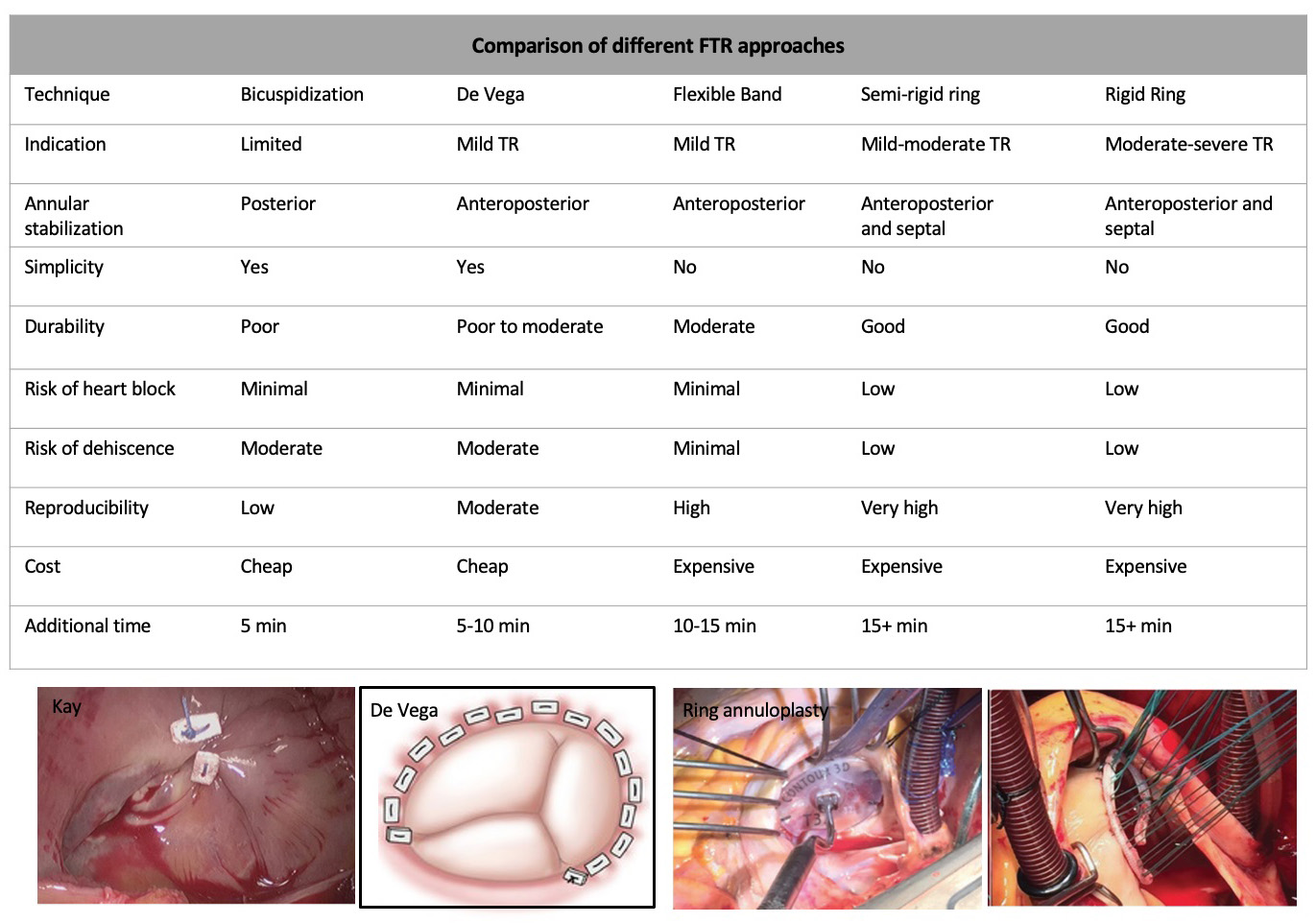 Fig. 3.
Fig. 3.Different approaches to treat STR. Modified from Chikwe et al. [43, 44]. STR, Secondary tricuspid regurgitation; FTR, functional tricuspid regurgitation; TR, tricuspid regurgitation.
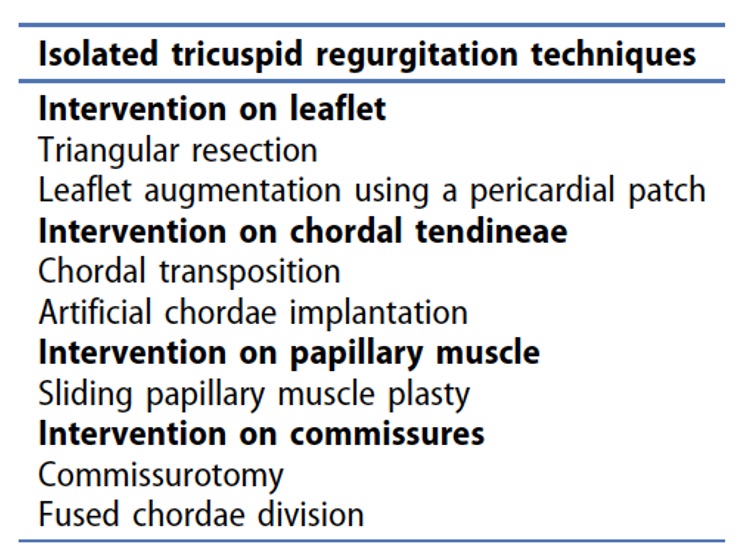 Fig. 4.
Fig. 4.Additional techniques for the treatment of isolated TR, which include intervention on the different components of the tricuspid valve, including the leaflets, chordal tendineae, papillary muscle and the commissures. Modified from Belluschi et al. [45]. TR, tricuspid regurgitation.
In 1985 Rivera et al. [46] conducted the first RCT comparing the
Carpentier tricuspid annuloplasty with the De Vega technique in 159 patients with
moderate to severe TR. Over an average follow-up of 64 months, the ring
annuloplasty group exhibited a significantly lower incidence of moderate or
severe TR (14/41 De Vega vs. 4/40 Carpentier, p
Regarding the best annuloplasty device, an RCT compared rigid rings versus flexible bands in 380 patients who underwent MV surgery concomitant with TV repair for STR. No difference was found in freedom from recurrent TR (97.3% in rigid ring vs. 96.2% in flexible band, p = 0.261), early mortality, overall survival, and freedom from TV reoperation. Notably, the flexible band demonstrated an advantage in restoring regional RV function, as evidenced by Doppler-derived systolic velocities of the annulus (S) and TA plane systolic excursion (TAPSE) at a 12-month follow-up [48].
Two meta-analyses also evaluated the TV annuloplasties technique. In the first,
3141 patients (1893 flexible band vs. 1248 rigid ring) were enrolled. There was
no difference in in-hospital mortality (6.9% flexible band vs. 7.3% rigid
ring), stroke (1.7% flexible band vs. 1.3% rigid rings), reoperation
(p = 0.232), and survival (p = 0.086). On the other hand, the
rigid ring had significantly better freedom from grade
Whenever possible, TV annuloplasty is preferable to valve replacement, which should only be considered when there is extensive leaflet destruction, severe tethering of TV leaflets, and significant TA dilation. When cardiac implantable electronic device leads interfere with the TV, the surgical technique should be adapted based on the patient’s condition and the surgeon’s experience [2].
In cases where replacement is indicated, a biological prosthesis is typically preferred over a mechanical one, as mechanical valves are more prone to thrombosis due to lower pressure and flow rate across the TV [51, 52]. For this same reason, the durability of a bioprosthesis in the TV position seems to be superior compared to the durability in the MV or aortic valve position. Additionally, with the emergence of TTVI, a bioprosthesis may offer the option for a future tricuspid transcatheter valve-in-valve therapy [53].
Regarding outcomes, a study by Zack et al. [25], which evaluated
national trends and outcomes of isolated TV surgery in the United States, found
that TV replacement was associated with a higher 30-day mortality rate (OR 1.91,
95% CI 1.18–3.08), an increased blood transfusion rate (39.3% vs. 33.2%,
p
TV surgery through a right mini-thoracotomy, as opposed to conventional sternotomy, has demonstrated favorable midterm outcomes. This approach is associated with reduced wound infection, lower bleeding, less pain, and a quicker return to normal life [54, 55]. Right mini-thoracotomy can be used for combined MV and TV intervention, yielding a 5-year estimated survival of 81.3%, and a 5-year freedom from reoperation rate of 100% [56]. It can also be used in patients with previous cardiac surgery with a 5-year survival rate of 72.2% [57].
Beyond minimally invasive access, isolated TV repair can also be performed
through a beating heart procedure. In a multicenter study, TV-beating heart
surgery was associated with a lower rate of acute renal failures and stroke
compared with the arrested heart strategy. Patients undergoing a beating heart
approach presented a 30-day mortality of 5%; with a 6-year survival and freedom
from cardiac death of 78%
Considering that both the Society of Thoracic Surgeons (STS) and logistic
EuroSCORE/EuroSCORE II were not proposed to predict TV intervention outcomes, the
TRI score was developed as a dedicated TV risk score model. The TRI-SCORE was
validated in a study based on a large consecutive cohort of 466 patients who
underwent isolated TV surgery for severe TR at 12 French tertiary centers. The
final risk score ranged from 0 to 12 points and incorporated 8 parameters, as
shown in Fig. 5 (Ref. [59]). The final simplified risk score model presented a
good discrimination performance (area under the ROC curve (AUROC) 0.808). Observed and predicted in-hospital
mortality rates increased from 0% to 60% and from 1% to 65%, respectively, as
the score increased from 0 up to
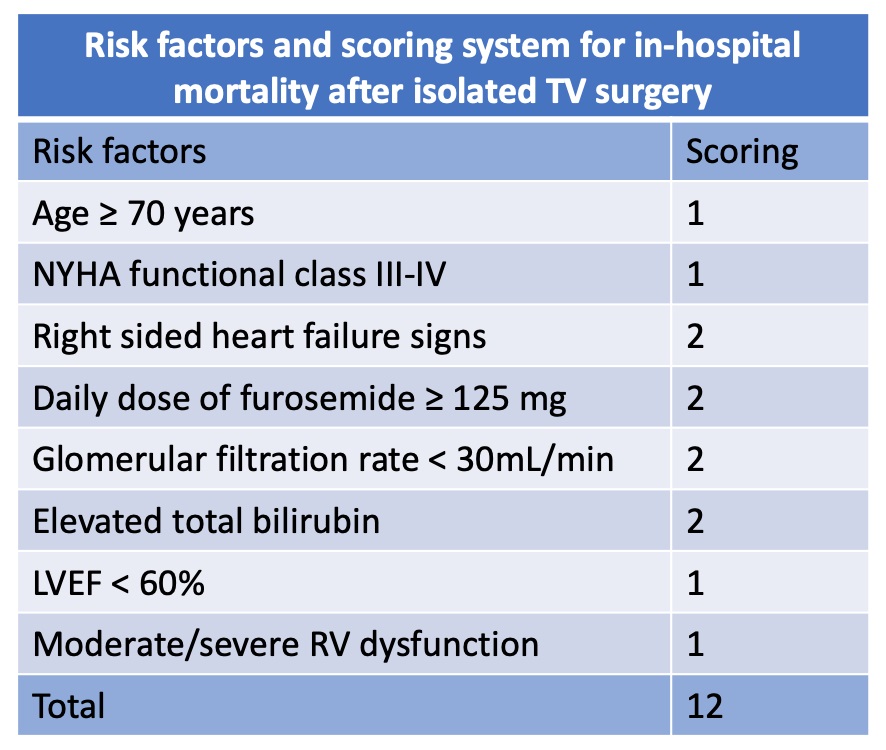 Fig. 5.
Fig. 5.TRI-SCORE variables. Adapted from Dreyfus et al. [59]. LVEF, left ventricle ejection fraction; NYHA, New York Heart Association; RV, right ventricle; TV, Tricuspid valve.
The TVARC consensus [11], besides the proposal STR subclassification presented above, provided important outcome definitions that could be useful to standardize TR trials, leading to more homogenous reports, accurate adjudication, and appropriate comparisons of clinical research studies.
According to TVARC Steering Committee [11], the timing of assessing endpoints is crucial for interpreting periprocedural, early, and later risks and benefits of TR therapy. The duration of follow-up must be sufficient to ascertain device durability, ensuring it is acceptable for the intended patient population and comparable to alternative therapies. Clinical outcomes should be reported at in-hospital, 30-day, and 1-year follow-up. Common safety endpoints might be assessed at in-hospital and 30-day, while less common safety endpoints and device failures may occur only after a longer follow-up. Imaging efficacy endpoints should be reported at post-procedure or predischarge, 30 days, and 1 year at a minimum, with yearly reporting up to 5 years in premarket studies.
In terms of endpoints, clinical trials should report both all-cause hospitalizations and cardiovascular and HF hospitalizations. Hospitalizations should also be adjudicated as valve, both native or device, and/or procedure-related. Commonly disease-specific instruments for HF patients include the Kansas City Cardiomyopathy Questionnaire (KCCQ) and the Minnesota Living with HF Questionnaire. Objective performance measures, which are not true patient-reported outcomes, can also be used to further quantify a patient’s physical function and health status. This includes the 6-minute walk test (6MWT), with a 25-to-50-meter increase in the 6MWT being considered a clinically significant improvement for an individual patient. Safety endpoints, including device-related complications and success endpoints should also be considered. These may involve TV reintervention, bleeding, vascular, access-related, cardiac injury, conduction disturbances, complications involving cardiac implantable electronic devices, neurological events, pulmonary embolism, deep vein thrombosis, and device- and procedure-related complications. Standardizing the reporting of these outcomes is crucial for the understanding and management of TR.
Even though a comprehensive discussion regarding current TTVI options and
outcomes falls beyond the purview of this surgical review, there are few reports
comparing TTVI with conventional surgical approaches that are worth mentioning.
In this line, Wang et al. [61] analyzed demographic characteristics,
complications, and outcomes of 92, 86, and 84 TR patients who underwent TR
surgical repair (STVr) or replacement (STVR), and transcatheter repair (TTVr),
respectively, using real-world data from the National Inpatient Sample (NIS)
database. The study found that TTVr patients were significantly older than STVr
(65.03 years in STVr, 66.3 years in STVR, 71.09 years in TTVr, p
Last but not least, a retrospective observational multicentre study by Wilde
et al. [62] showed that, despite a trend toward lower 30-day mortality
with the tricuspid transcatheter edge-to-edge repair (T-TTER) (2.8% vs. 10.7%,
p = 0.07), MIC-TVS led to a significantly more efficient TR reduction
(p
Despite the growing recognition that TR has received due to its prognostic role and the emergence of new interventions, TR management is still neglected. Clinical factors such as advanced stage of the disease, presence of multiple comorbidities, and high surgical risk contribute to the suboptimal outcomes associated with TR surgical interventions. These factors, along with the anatomical challenges inherent to TV, must be contemplated not only to determine the optimal timing for intervention but also to choose the most suitable surgical technique (Table 3). Therefore, addressing the neglected aspects of TR management, especially in light of its prognostic role, requires a comprehensive understanding of both clinical factors and anatomical intricacies. By doing so, we can enhance the effectiveness of interventions and improve patient outcomes.
| TV surgical candidates | ||
| Clinical and epidemiological factors | ||
| Age | Old patients | |
| Comorbidities | High frequent | |
| Surgical risk | High surgical risk | |
| Preferable surgical technique | Repair | |
| Multiple valve disease | Frequently associated with left-sided valve disease | |
| Entities | PTR and STR (predominant cause) | |
| Anatomical factors | ||
| Components of the valve | Tricuspid valve, RA, RV, subvalvular apparatus | |
| Configuration of the valve | Asymmetrical – 3 leaflets | |
| Morphology of the annulus | 3D saddle-shaped annulus | |
| Dimensions of the annulus | Large annulus dimension | |
| Calcification | Less frequent | |
| Structures in proximity | Right coronary artery, coronary sinus, conduction system | |
PTR, primary tricuspid regurgitation; RA, right atrial; RV, right ventricle; STR, secondary tricuspid regurgitation; TV, tricuspid valve.
AF, atrial fibrillation; A-STR, atrial secondary tricuspid regurgitation; CI, confidence interval; CTEPH, chronic thromboembolic pulmonary hypertension; FAC, fractional area change; HF, heart failure; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; HR, hazard ratio; KCCQ, Kansas City Cardiomyopathy Questionnaire; LTR, lead-associated tricuspid regurgitation; LTR-A, lead-associated tricuspid regurgitation type A; LTR-B, lead-associated tricuspid regurgitation type B; LV, left ventricle; LVEF, left ventricle ejection fraction; MIC-TVS, minimally invasive tricuspid valve surgery; MR, mitral regurgitation; MV, mitral valve; OR, odds ratio; PAH, pulmonary arterial hypertension; PASP, pulmonary artery systolic pressure; PH, pulmonary hypertension; PTR, primary tricuspid regurgitation; RA, right atrial; RCT, randomized clinical trials; RHD, rheumatic heart disease; RR, relative risk; RV, right ventricle; STS, Society of Thoracic Surgeons; STR, secondary tricuspid regurgitation; 6MWT, 6-minute walk test; STVr, surgical tricuspid valve repair; STVR, surgical tricuspid valve replacement; TA, tricuspid annular; TAPSE, tricuspid annular plane systolic excursion; TR, tricuspid regurgitation; TTVI, transcatheter tricuspid valve intervention; T-TTER, transcatheter edge-to-edge repair; TTVr, transcatheter tricuspid valve repair; TV, tricuspid valve; TVARC, Tricuspid Valve Academic Research Consortium; 3D, 3-dimensional; V-STR, ventricular secondary tricuspid regurgitation.
APT and MT designed the research study, performed the research and wrote the manuscript. Both authors contributed to editorial changes in the manuscript. Both authors read and approved the final manuscript. Both authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
Dr. Tagliari has received speaking fees from Biotronik, Boston Scientific and Meril Life. Dr Taramasso has been a consultant or the recipient of consultancy fees from Abbott, Edwards Lifesciences, Boston Scientific, Shenqi Medical, CoreMedic, 4tech, Simulands, MTEx, Cardiovalve, and MEDIRA. The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.