



1 Department of Cardiology, Hospital General Universitario Gregorio Marañón, 28007 Madrid, Spain
2 Medicine Department, Universidad Europea, 28670 Madrid, Spain
3 Medicine Department, Universidad Complutense, 28005 Madrid, Spain
Abstract
With population aging and the subsequent accumulation of cardiovascular risk factors, a growing proportion of patients presenting with acute coronary syndrome (ACS) are octogenarian (aged between 80 and 89). The marked heterogeneity of this population is due to several factors like age, comorbidities, frailty, and other geriatric conditions. All these variables have a strong impact on outcomes. In addition, a high prevalence of multivessel disease, complex coronary anatomies, and peripheral arterial disease, increases the risk of invasive procedures in these patients. In advanced age, the type and duration of antithrombotic therapy need to be individualized according to bleeding risk. Although an invasive strategy for non-ST-segment elevation acute myocardial infarction (NSTEMI) is recommended for the general population, its need is not so clear in octogenarians. For instance, although frail patients could benefit from revascularization, their higher risk of complications might change the risk/benefit ratio. Age alone should not be the main factor to consider when deciding the type of strategy. The risk of futility needs to be taken into account and identification of risk factors for adverse outcomes, such as renal impairment, could help in the decision-making process. Finally, an initially selected conservative strategy should be open to a change to invasive management depending on the clinical course (recurrent angina, ventricular arrhythmias, heart failure). Further evidence, ideally from prospective randomized clinical trials is urgent, as the population keeps growing.
Keywords
- acute coronary syndrome
- octogenarians
- NSTEMI
- frailty
The prevalence of coronary artery disease increases with age. Acute coronary
syndromes (ACS) are common in octogenarians (aged between 80 and 89) and age is
associated with a poor prognosis [1]. Elderly patients have been underrepresented
in ACS clinical trials, particularly in the case of frail patients and those
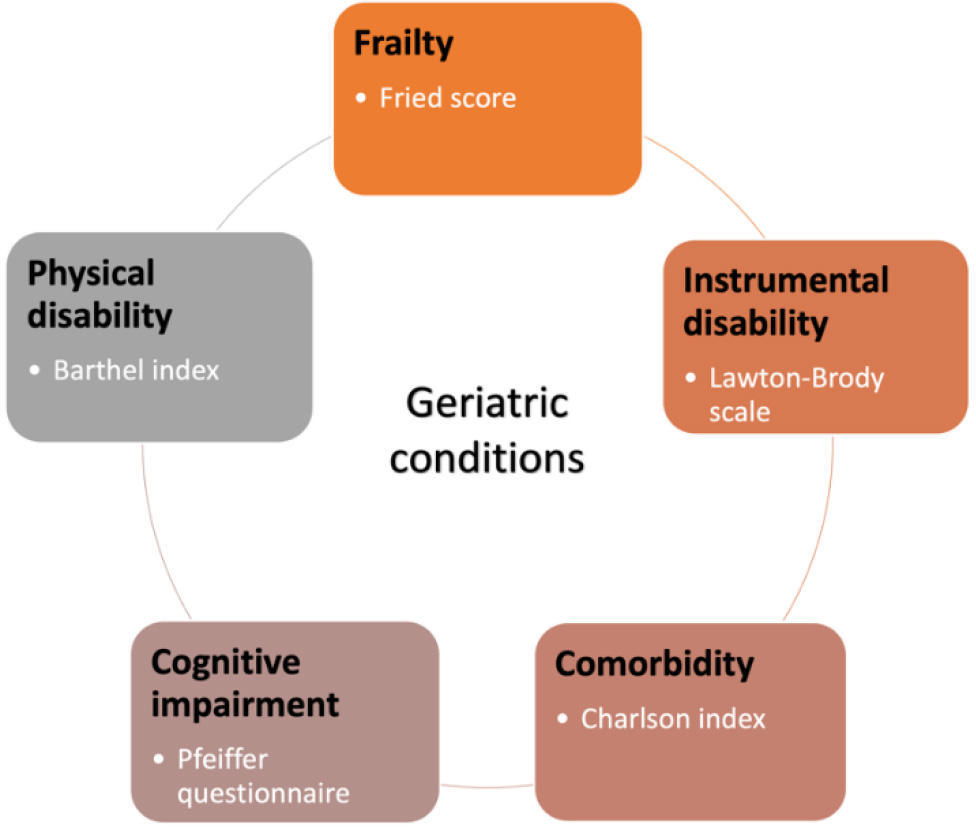 Fig. 1.
Fig. 1.Geriatric conditions. Common geriatric conditions and some simple indexes to assess them.
Cardiovascular changes associated with aging can predispose an individual to coronary artery disease, myocardial ischemia and ACS. The increased stiffness of the aorta and main arteries, frequently seen in the elderly, leads to increased resistance of left ventricular ejection and main systolic blood pressure, with a decrease in diastolic pressure. This causes a compensatory left ventricular hypertrophy, with increased myocardial work and oxygen demand, whereas the loss in diastolic pressure diminishes coronary perfusion pressure, leading to an imbalance in myocardial oxygen demand and supply, which predisposes older adults to type 2 myocardial infarction and NSTEMI. In addition, the combination of endothelial dysfunction and a state of chronic inflammation that is seen in older patients begets atherosclerosis, contributing to coronary artery disease development and progression [5].
NSTEMI clinical presentation in advanced-age patients is frequently atypical. Dyspnea, or even syncope or malaise might be present [6]. The frequent presence of advanced and complex coronary artery disease and comorbidities favor complications of interventional procedures [7].
Age is related to ACS in hospital and long-term mortality [3, 8]. In the
Randomized Intervention Trial of unstable Angina 3 (RITA-3 trial), age was the
strongest predictor of death or myocardial infarction, with more than a doubling
risk for each 10 years of age over 60 years [9]. In-hospital mortality for
elderly patients with ACS ranges between 8–11% [10, 11]. One-year mortality
increases with age (Fig. 2) [12]. High mortalities after percutaneous coronary
intervention in patients
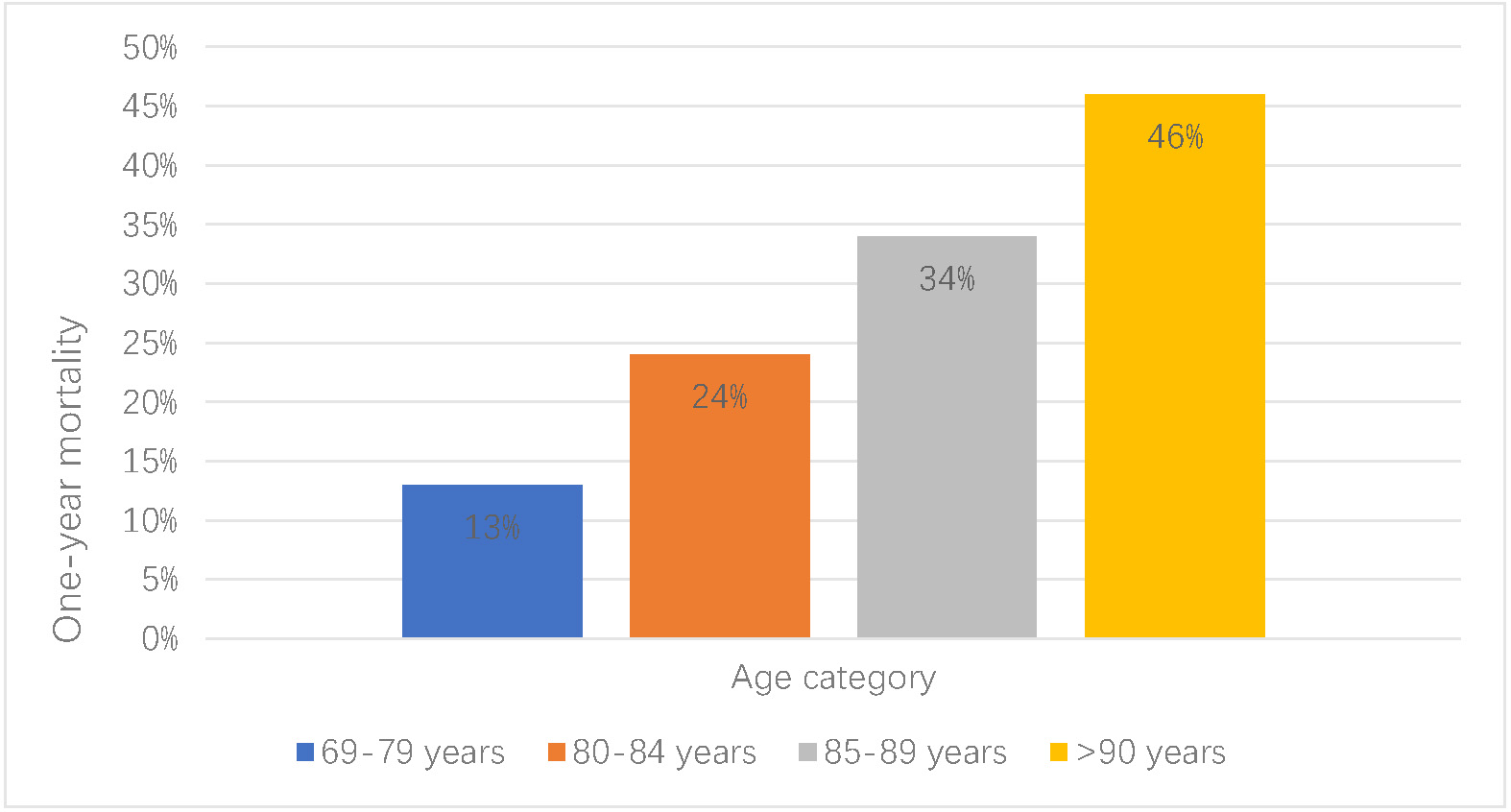 Fig. 2.
Fig. 2.Mortality of acute coronary syndromes (ACS) in the elderly. One-year mortality of acute coronary syndrome increases with age.
Multimorbidity is present in most elderly patients with ACS and can interfere with treatment. Comorbidities can be assessed using the Charlson Comorbidity Index [19], which includes up to 19 conditions. A simplified version with six comorbidities has been proposed for a more accurate assessment of comorbidity in this specific population [20]. They include renal failure, anemia, diabetes mellitus, cerebrovascular disease, peripheral artery disease, and chronic lung disease. Mortality increased with a higher number of comorbidities [20]. Evidence suggests that the benefits or revascularization in older patients diminish with more comorbidity burden [21].
Chronic kidney disease is more prevalent in older patients because of the
progressive loss of kidney function with age [22]. Cardiorrenal syndrome can also
play a role in the severity of kidney injury, which is associated with worse
outcomes [23, 24]. The Impacto de la fragiLidad y Otros síndromes
GEriátricos en el manejo y pronóstico Vital del ancianO con Síndrome
Coronario Agudo sin elevación de segmento ST (LONGEVO-SCA) registry studied
consecutive patients aged
Diabetes is known to be associated with mortality in patients with ACS [26]. In the Elderly-ACS 2 trial, diabetes was associated with an increase in cardiovascular mortality but only due to its association with higher rates of comorbidities and cardiovascular risk profile [27]. In the elderly, diabetes seems to be associated with a higher incidence of events mainly among frail patients, with a similar incidence of mortality or readmission in non-frail patients [28, 29]. The impact of diabetes on prognosis seems to be particularly strong in elderly women [30].
Anemia is a strong predictor of prognosis in ACS, with an increased risk of mortality for hemoglobin levels below 11 g/dL [31]. It is also a predictor of bleeding in older patients undergoing percutaneous coronary intervention, non-inferior than well-known bleeding scores like PREdicting bleeding Complications In patients undergoing Stent implantation and subsEquent Dual Anti Platelet Therapy (PRECISE-DAPT) or CRUSADE [32]. The association between anemia and mortality seems to be more significant in robust patients, whereas frailty leads to a poorer prognosis irrespective of hemoglobin levels [33].
Cognitive impairment is prevalent in the elderly (
Frailty is defined as a clinical syndrome, characterized by a loss of biological
reserves, which can lead to failure of the mechanisms of homeostasis after a
stressor event [35]. Two main models of frailty have been described: the
phenotype model defines frailty as the presence of three or more signs and
symptoms, such as weight loss, self-reported exhaustion, weakness, slow walking
speed, and low physical activity [36]. The cumulative model includes
comorbidities and calculates a frailty score according to the number of
“deficits” present, which can be symptoms, signs, diseases, or disabilities
[37, 38]. The prevalence of frailty is up to 22% in those aged
Frailty is independently associated with mortality in advanced-age patients with ACS [41, 42, 43, 44, 45]. In the LONGEVO-SCA registry [46] the presence of pre-frailty and frailty increased six-month mortality 2.7 and 3.0 times respectively [47] and the association remained significant in long-term follow-up [48]. In addition, frailty is a risk factor for the development of other geriatric syndromes [40].
The prevalence of frailty in the elderly is twice as high in women than in men, and elderly women have a higher incidence of comorbidities, accounting for the increased mortality of frail women after an ACS [49]. In LONGEVO-SCA, the female sex was an independent predictor of death/hospitalization, and frailty was associated with higher mortality in women, but not prefrailty [45].
Functional and sensorial decline, delirium, falls, and polypharmacy are also common in the elderly. The presence of geriatric syndromes may affect the clinical course, prognosis and treatment [2]. Nutritional status is also related to outcomes in advanced-age patients with ACS and the Mini Nutritional Assessment-Short Form (MNA-SF) has been shown to be an independent risk factor for mortality in this population [50].
Delirium is a fluctuating state of confusion with alterations in attention and
cognitive function. Its incidence depends on the setting of the population,
reaching up to 20% in cardiac intensive care units and 17% in elderly
individuals admitted for acute cardiac conditions [51, 52]. Delirium is associated
with mortality and bleeding events and up to 7% of patients
The Comprehensive Geriatric Assessment (CGA) is a multidimensional, interdisciplinary diagnostic process to determine the medical, psychological and functional capacities of advanced-age patients, that enables the elaboration of a personalized integrated and coordinated plan for diagnosis, treatment, and follow-up [54]. Its use has been shown to increase survival and home stay after hospital admission in elderly patients [54].
Compared to younger patients, octogenarians more frequently present with
multivessel disease [55, 56] and revascularization of the culprit lesion is less
frequently achieved, in relation to the higher prevalence of calcification and
tortuosity, complex lesions, need for bifurcation stenting, and ostial lesions
[55, 56, 57]. In addition, the decision of whether to achieve complete
revascularization or restraining the treatment of the culprit lesion remains a
clinical challenge. Although the benefits of complete revascularization seem
clearer in younger patients, there is still conflicting evidence regarding the
elderly [58]. Multivessel percutaneous intervention seems to have better outcomes
than culprit-only revascularization [59]. Coronary imaging and physiology are
increasingly used to guide revascularization [60]. The recently published
Functional versus Culprit-only Revascularization in Elderly Patients with
Myocardial Infarction and Multivessel Disease (FIRE) trial, although done in the
different context of ST-segment elevation, suggests a benefit for
physiology-guided complete revascularization also in patients
Although no clear differences have been encountered between revascularization strategies, a less aggressive percutaneous intervention seems reasonable in old and fragile patients to avoid surgical-related complications [56, 62]. The radial artery approach is feasible and can be used in a similar way as in younger patients [57].
In summary, percutaneous interventions seem safe in octogenarians, with about 10% procedure complications, but all-cause death, cardiac mortality and recurrent myocardial infarction remain high in this population [57]. Preprocedural renal impairment and left ventricular systolic dysfunction are predictive of cardiovascular events [63].
Age is included in most thrombotic and bleeding risk scales as a risk factor,
and recent studies consider age to be a stronger predictor of bleeding than
ischemic events [64]. Comorbidities have also been related to an increased
bleeding risk, as well as frailty although to a lesser extent [65]. Some
strategies to minimize bleeding risk in older patients include blood pressure
control, gastroprotection, appropriate revascularization criteria, avoidance of
pretreatment with purinergic receptor P2Y, G-protein coupled, 12 protein (P2Y12)
inhibitors for NSTEMI, radial arterial access, and modulation of dual
antiplatelet therapy duration [66]. Current guidelines recommend antithrombotic
treatment with prasugrel in preference to ticagrelor or clopidogrel [67].
However, prasugrel is not recommended in patients
In a sub-analysis of the Platelet Inhibition and Patient Outcomes (PLATO) study
comparing clinical outcomes in the elderly, ticagrelor reduced ischemia and
mortality outcomes compared with clopidogrel without increasing bleeding risk
[76]. However, in the Clopidogrel versus Ticagrelor or Prasugrel in Patients Aged
70 Years or Older with Non-ST-Elevation Acute Coronary Syndrome (POPular-AGE)
trial that randomized clopidogrel versus ticagrelor or prasugrel, clopidogrel was
not inferior to ticagrelor for all-cause death, myocardial infarction, stroke and
minor bleeding, with a lower incidence of bleeding [77]. In addition, the Swedish
Web-System for Enhancement and Development of Evidence-Based Care in Heart
Disease Evaluated According to Recommended Therapies (SWEDEHEART) registry found
an increased bleeding risk of ticagrelor compared to clopidogrel in patients
There is some evidence for prasugrel dose reduction from 10 to 5 mg daily as an
option in the elderly, with recent data showing comparable efficacy and safety to
clopidogrel in patients
Current guidelines recommend extending dual antiplatelet therapy beyond 1 year in patients with high ischemic risk. This strategy has been shown to be feasible in older patients, although their benefits seem to be attenuated in this population and therefore the implementation of extended dual antiplatelet therapy should be carefully evaluated [66, 82].
The management of NSTEMI in robust octogenarians should not differ from the one done in younger patients and an invasive strategy is the preferred option [2]. However, the approach to NSTEMI in octogenarians with severe or multiple comorbidities, those with dependence, frailty and/or limited life expectancy is not straightforward and conservative management is frequently an acceptable option [2, 83]. Invasive strategy reduces the risk of composite ischemic endpoints, particularly in high-risk patients but might produce complications [67]. The European Society of Cardiology guidelines recommend a routine invasive strategy for all patients irrespective of age, except for those deemed to be at a very low risk, where a selective invasive strategy is also accepted [67] but a global geriatric assessment might be a reason to change this approach in some octogenarians.
The evidence supporting invasive strategy in the general population comes mainly
from three ACS trials: FRagmin and Fast Revascularisation during InStability in
Coronary artery disease (FRISC) II, RITA-3, and Invasive versus Conservative
Treatment in Unstable Coronary Syndromes (ICTUS) [84]. FRISC II [84] randomized
2457 patients (461
A summary of the main randomized trials in advanced-age patients is shown in
Table 1 (Ref. [89, 90, 91, 92, 93, 94, 95, 96]). Bach et al. [89] found that an invasive
strategy was associated with a reduction in death or myocardial infarction at 6
months in the subgroup of patients
| First author, year | Age (years), mean | N | Primary outcome | Benefits of invasive strategy |
| Bach 2004 [89] | 962 | Mortality, nonfatal MI, rehospitalization, stroke and hemorrhagic complications | 6-months death/MI: 10.8% vs. 21.6% | |
| Savonitto 2012 [90] | 313 | Composite of death, MI, disabling stroke, and repeat hospitalization for cardiovascular causes or severe bleeding | NS | |
| Sanchis 2016 [91] | 106 | Composite of all-cause mortality, reinfarction, and readmission for cardiac cause | NS | |
| Tegne 2016 [92] | 457 | Composite of MI, need for urgent revascularization, stroke, and death | 40.6% vs. 61.4%, HR = 0.53 | |
| Gnanenthiran 2017 [93] | 20,540 | In-hospital mortality, mortality at follow-up, MI, revascularization, rehospitalization for cardiac causes, stroke, major bleeding | Inhospital mortality OR = 0.65, 95% CI: 0.53–0.79 | |
| Ma 2018 [94] | 832,007 | Death at follow-up from 6 months to 5 years | RR = 0.65, 95% CI: 0.59–0.73 | |
| Reaño 2020 [95] | 3768 | All-cause mortality, cardiovascular mortality, MI, stroke, need for revascularization, recurrent angina. | NS | |
| Sanchis 2023 [96] | 167 | Number of days alive and out of the hospital. | NS |
MI, miocardial infarction; NS, non significant; HR, hazard ratio; OR, odds ratio; RR, risk ratio; CI, confidence interval.
Observational studies suggest that an invasive strategy benefit persists in the
elderly but there are conflicting data regarding whether the benefit persists or
is even higher in frail patients [97, 98, 99]. Randomized trials have failed to show
an invasive strategy benefit in frail patients. The Randomized comparison between
the invasive and conservative strategies in comorbid elderly patients with non-ST
elevation myocardial infarction (MOSCA) trial included patients with
Patients’ perspectives, values and opinions are key in the decision-making
process and should be incorporated into the protocolized decision [101]. Some
patients might prefer the option with the lowest risk for harm, even if the
long-term benefit is lower [102]. In addition, expected life expectancy should be
one of the variables that is incorporated in the equation, as conservative
management is probably a better option in patients with life expectancies
NSTEMI is one of the main causes of mortality and morbidity in the elderly. Age alone should not be the main factor to consider when offering an invasive strategy, as the heterogeneity of this population makes it imperative for clinicians to assess other variables like frailty, comorbidities, and other geriatric conditions. The risk of futility needs to be taken into account and an invasive approach should not be a static choice, as some elderly patients might benefit from an initial conservative approach open to subsequent invasive management depending on the clinical course (recurrent angina, ventricular arrhythmias, heart failure). Further evidence, ideally from prospective randomized clinical trials is urgent, as the population keeps growing.
MMS and MJF designed the research study. SÁZ performed the research. SÁZ analyzed the data. SÁZ, MMS and MJF wrote the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest. Manuel Martínez-Sellés is serving as Guest Editor and one of the Editorial Board members of this journal. We declare that Manuel Martínez-Sellés had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Salvatore De Rosa and Leonardo De Luca.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.