
 , Zsuzsanna Besenyi 2, Viktória Nagy 3, Bence Radics 4, Hajnalka Vágó 5, Zsigmond Jenei 1, Gábor Katona 1, Róbert Sepp 3
, Zsuzsanna Besenyi 2, Viktória Nagy 3, Bence Radics 4, Hajnalka Vágó 5, Zsigmond Jenei 1, Gábor Katona 1, Róbert Sepp 31 Department of Medicine and Hematology, Semmelweis University, 1088 Budapest, Hungary
2 Department of Nuclear Medicine, University of Szeged, 6720 Szeged, Hungary
3 Division of Non-Invasive Cardiology, Department of Medicine, University of Szeged, 6720 Szeged, Hungary
4 Department of Pathology, University of Szeged, 6720 Szeged, Hungary
5 Heart and Vascular Center, Semmelweis University, 1122 Budapest, Hungary
Abstract
Sarcoidosis is an inflammatory multisystemic disease of unknown etiology
characterized by the formation of non-caseating granulomas. Sarcoidosis can
affect any organ, predominantly the lungs, lymphatic system, skin and eyes. While
Keywords
- sarcoidosis
- cardiac sarcoidosis
- granulomatous disease
Sarcoidosis is a systemic inflammatory disease of unknown etiology characterized
by multiorgan involvement and the formation of non-caseating granulomas. It is
thought that exposure to certain environmental antigens (infectious, occupational
or other) results in an exaggerated, dysregulated T-cell-driven immune response
in patients with a genetic predisposition leading to non-necrotic granulomatous
inflammation. Sarcoidosis can affect any organ, predominantly the lungs,
lymphatic system, skin and eyes. While 90% of patients with sarcoidosis have
lung and intrathoracic lymph node involvement, only approximately 5% have
clinically manifest cardiac involvement. Another 20–25% of patients have
asymptomatic, clinically silent cardiac involvement shown in autopsy studies
[1, 2, 3, 4, 5, 6, 7, 8, 9]. Earlier studies [10, 11, 12] showed that most patients with clinically manifest
cardiac sarcoidosis (CS) have minimal extracardiac disease and up to two thirds
have isolated CS, however more recent studies [13, 14] reported a much lower 3.2%
to 9.4% prevalence of isolated CS without evidence of extracardiac disease using
The prevalence of systemic sarcoidosis is between 5 and 64 per 100,000 of the population. A higher prevalence has been reported in Scandinavian countries and among African Americans and the lowest prevalence was found among Asians [21, 22, 23, 24]. Most disease occurs in patients between 25 and 60 years of age and sarcoidosis is unusual in people under the age of 15 or older than 70 years, the disease affects both sexes, with slight predominance in women [4, 5, 8, 25].
The inciting antigen, which might be an infectious agent, environmental antigen
or an autoantigen in individuals with genetic predisposition, and/or certain
human leukocyte antigen (HLA) polymorphisms trigger the formation of
non-necrotizing granulomas. Antigen-presenting cells, such as macrophages and
dendritic cells, process the inciting antigen and induce cell-mediated immune
reaction by activating na
Among the several infectious agents suggested to have a role in the etiology of sarcoidosis Propionibacterium acnes is the only microorganism, which was isolated from sarcoid lesions [10, 27, 28, 29]. There is a familial clustering of cases in sarcoidosis, as the first- and second-degree relatives are more affected than the general population [30]. The Case Control Etiology of Sarcoidosis Study (ACCESS) study showed that patients who are first-degree relatives of patients with sarcoidosis had a five times higher risk of developing sarcoidosis compared to controls [31].
Isolated CS is a more serious disease than CS associated with extracardiac sarcoidosis [11, 32]. Cardiac manifestations of CS include ventricular and atrial arrhythmias, AV or intraventricular conduction disturbance, sinus node dysfunction, heart failure, sudden cardiac death (SCD) and less commonly valvular heart disease, ischemia, pericardial disease with or without pericardial effusion. The most common symptoms of CS related to these cardiac manifestations are palpitation, presyncope, syncope, breathlessness disproportionate to the extent of pulmonary involvement, angina-like chest pain, edema or cardiac arrest, sudden cardiac death as a first presentation of the disease. Approximately 20–25% of patients with CS are asymptomatic [9, 32]. The manifestations of CS mainly depend on the location and extent of granulomas and fibrosis. AV block, bundle branch block (BBB) or sinus node dysfunction can be due to granulomatous inflammation or scar tissue in regions of the conduction system (in the sinus node or basal/mid interventricular septum) or direct involvement of the coronary artery blood supply to the conduction system (sinoatrial and AV nodal arteries) by granulomas and/or scar tissue. AV block occurs in 26–67% of CS patients, BBB has an estimated prevalence of 12–61% with right BBB (RBBB) occurring more frequently than left BBB (LBBB) [32]. Ventricular arrhythmias are mostly due to late-stage scar formation and in some cases due to small ventricular aneurysm formation serving as anatomical substrate for macroreentry, but active inflammation can also cause ventricular arrhythmias by triggered activity, increased automaticity and also by reentry mechanisms. Atrial arrhythmias, such as atrial fibrillation, atrial flutter, atrial tachycardia, are more commonly caused by atrial enlargement due to systolic or diastolic ventricular dysfunction associated with heart failure, or atrial enlargement due to pulmonary sarcoidosis-related pulmonary arterial hypertension, right heart dysfunction, than by direct granulomatous involvement of the atrial myocardium. The mechanisms of atrial arrhythmias are abnormal automaticity, macroreentry and triggered activity [9, 32]. Heart failure develops as a consequence of widespread myocardial infiltration by granulomatous inflammation and fibrosis. Angina-like chest pain, acute coronary syndrome may be due to impaired coronary flow reserve from compression of the myocardial microvasculature, rarely to granulomatous coronary arteritis, or either compression or dissection of a single coronary artery [20]. Granulomas can also involve heart valves resulting in valvular insufficiency, most commonly mitral regurgitation [32].
The diagnosis of sarcoidosis is based on the classic triad of (1) compatible clinical characteristics, (2) histological evidence of non-caseating and non-necrotizing granulomas and (3) the exclusion of other granulomatous diseases [4, 20]. There are two major pathways for the diagnosis of CS: (1) the histological pathway, (2) the clinical diagnosis pathway. The histological pathway can be applied and the diagnosis of CS established by performing endomyocardial biopsy (EMB), which reveals non-caseating granulomas with no alternative underlying cause. Or, if EMB is not attempted or negative, which cannot rule out CS, due to the patchy nature of the disease resulting in a low sensitivity (20–30%) of detection, that despite the application of imaging-, or electroanatomical mapping-guided sampling techniques can improve to modest at best, the clinical diagnosis of CS is probable and can be established, if there is histological evidence of extracardiac sarcoidosis and the simultaneous presence of one or more suggestive cardiac findings (Table 1, Ref. [5]). The histological pathway is recommended by the Heart Rhythm Society (HRS) Expert Consensus statement [33] and the World Association for Sarcoidosis and Other Granulomatous Disorders (WASOG) Guidelines [34] (Table 1). However, the 2016 Japanese Ministry of Health and Welfare guidelines [8] also allow the diagnosis of CS without a biopsy of any affected organ and render possible the clinical diagnosis pathway when in addition to the presence of certain characteristic findings suggesting cardiac involvement, certain characteristic laboratory findings are also present (Table 2, Ref. [8]).
| There are 2 pathways to a diagnosis of cardiac sarcoidosis (CS): |
| 1. Histological diagnosis from myocardial tissue |
| CS is diagnosed if an endomyocardial biopsy shows non-caseating granuloma with no alternative cause for the histological findings identified |
| 2. Clinical diagnosis from invasive and non-invasive studies: |
| CS is probable* if |
| (a) There is a histological diagnosis of extra-cardiac sarcoidosis |
| and |
| (b) One or more of following is present: |
| ➢ Steroid +/- immunosuppressant responsive cardiomyopathy or heart block |
| ➢ Unexplained reduced left ventricular ejection fraction ( |
| ➢ Unexplained sustained (spontaneous or induced) ventricular tachycardia |
| ➢ Mobitz type II, second- or third-degree heart block |
| ➢ Patchy uptake on dedicated cardiac FDG-PET in a pattern consistent with CS |
| ➢ Late Gadolinium Enhancement on CMR consistent with CS pattern |
| ➢ Positive gallium uptake in a pattern consistent with CS |
| and |
| (c) Other causes for the cardiac manifestation(s) have been reasonably excluded |
*In general, “probable involvement” is considered adequate to establish a
clinical diagnosis of CS.
Adapted from [5] with minor modifications. CMR, cardiac magnetic resonance;
FDG-PET, 18F-fluorodeoxyglucose positron emission tomography.
| 1. Histological diagnosis |
| CS is diagnosed when a biopsy (endomyocardial or surgical) shows non-caseating epithelioid granulomas |
| 2. Clinical diagnosis |
| If an endomyocardial biopsy is not performed or is negative, a diagnosis is made clinically. |
| CS is diagnosed clinically (1) when epithelioid granulomas are found in organs other than the heart, and clinical findings strongly suggestive of cardiac involvement by CS are present; or (2) when there is evidence of pulmonary or ophthalmic sarcoidosis and there are |
| Criteria for cardiac involvement |
| Clinical findings that satisfy |
| 1. Major criteria |
| (a) High-grade AV block or fatal ventricular arrhythmia (VF and sustained VT) |
| (b) Basal thinning of the ventricular septum or abnormal ventricular wall anatomy including ventricular aneurysm, thinning of the middle or upper ventricular septum, regional ventricular wall thickening |
| (c) LVEF |
| (d) |
| (e) Cardiac MRI reveals LGE of the myocardium |
| 2. Minor criteria |
| (a) Abnormal ECG findings: ventricular arrhythmias including NSVT, multifocal or frequent PVCs, BBB, axis deviation or abnormal Q waves |
| (b) Myocardial perfusion scintigraphy (SPECT) showing perfusion defects |
| (c) Endomyocardial biopsy showing infiltration with monocytes and moderate to severe myocardial interstitial fibrosis |
| Characteristic laboratory and imaging findings in sarcoidosis |
| A diagnosis of sarcoidosis is established when |
| 1. High serum ACE activity or elevated serum lysozyme levels |
| 2. High serum soluble interleukin-2 receptor levels |
| 3. Increased tracer uptake in |
| 4. A high percentage of lymphocytes in BAL with a CD4/CD8 ratio of |
| 5. Bilateral hilar lymphadenopathy |
| Isolated CS diagnostic guidelines |
| Isolated CS is suspected when: |
| 1. No clinical findings are suggestive of other organ involvement than the heart |
| 2. Absence of increased uptake in |
| 3. A chest CT scan reveals no shadow along the lymphatic tracts in the lungs or no hilar and mediastinal lymphadenopathy |
| Isolated CS is diagnosed with: |
| 1. Histological diagnosis: endomyocardial biopsy or surgical biopsy show non-caseating epitheloid granulomas |
| 2. Clinical diagnosis: isolated CS diagnosis is made when criteria for cardiac involvement 1(d) and |
Adapted from [8] with modifications.
AV, atrioventricular; ACE, angiotensin-converting enzyme; BAL, bronchoalveolar
lavage; BBB, bundle branch block; CS, cardiac sarcoidosis; LGE, late gadolinium
enhancement; LVEF, left ventricular ejection fraction; NSVT, non-sustained
ventricular tachycardia; PVC, premature ventricular complex; VF, ventricular
fibrillation; VT, ventricular tachycardia; ECG, electrocardiogram; MRI,
magnetic resonance imaging; CT, computed tomography; ECG, electrocardiogram;
SPECT, single-photon emission computed tomography; CD4, helper T lymphocytes;
CD8, cytotoxic T lymphocytes; FDG-PET, 18F-fluorodeoxyglucose positron emission
tomography.
There are two scenarios when evaluation of patients for CS should be performed:
(1) screening for cardiac involvement in patients with extracardiac sarcoidosis,
(2) the presence of clinical signs and symptoms raising the suspicion of CS in
patients without known sarcoidosis. All patients with verified extracardiac
sarcoidosis should be screened for CS, irrespective whether they have or haven’t
symptoms suggesting cardiac involvement, because CS is the second leading cause
of mortality in patients affected by sarcoidosis. In these patients a detailed
patient history, physical examination, electrocardiogram (ECG) (probably also
Holter) recording and transthoracic echocardiography should be performed for
initial CS assessment according to the HRS Expert Consensus statement [33, 35].
Patient history should be considered positive if significant palpitations lasting
In
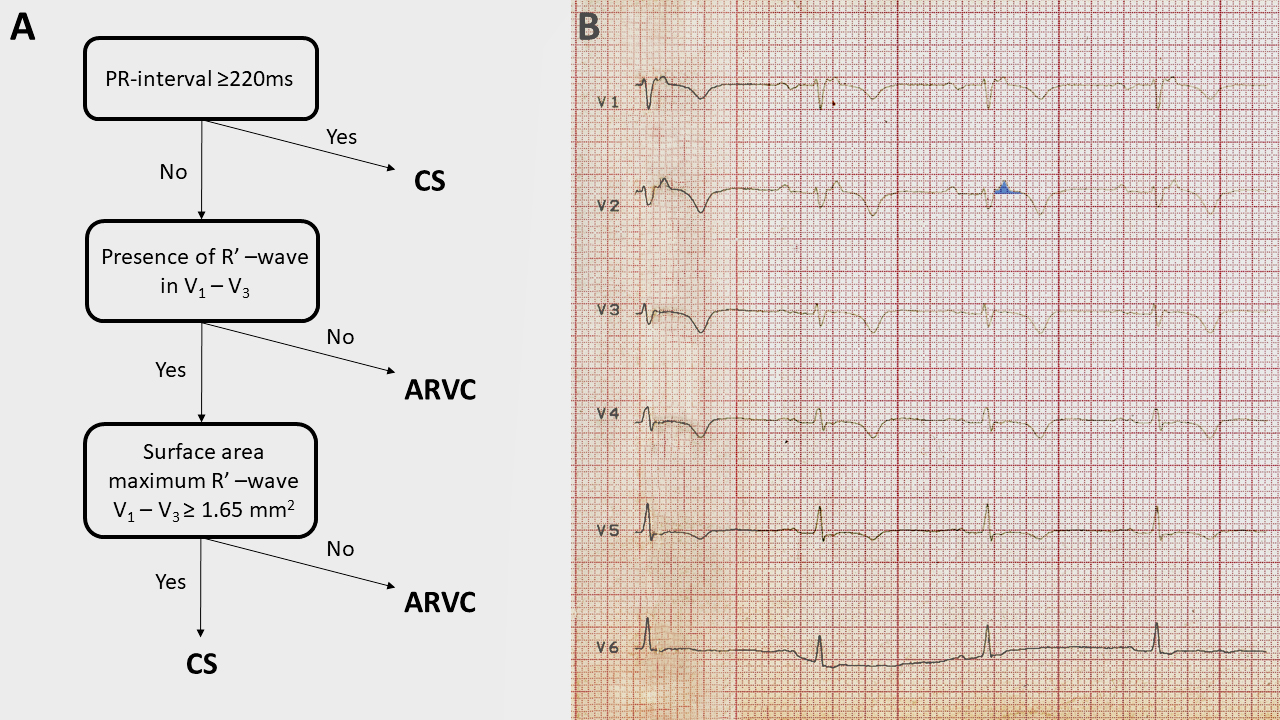 Fig. 1.
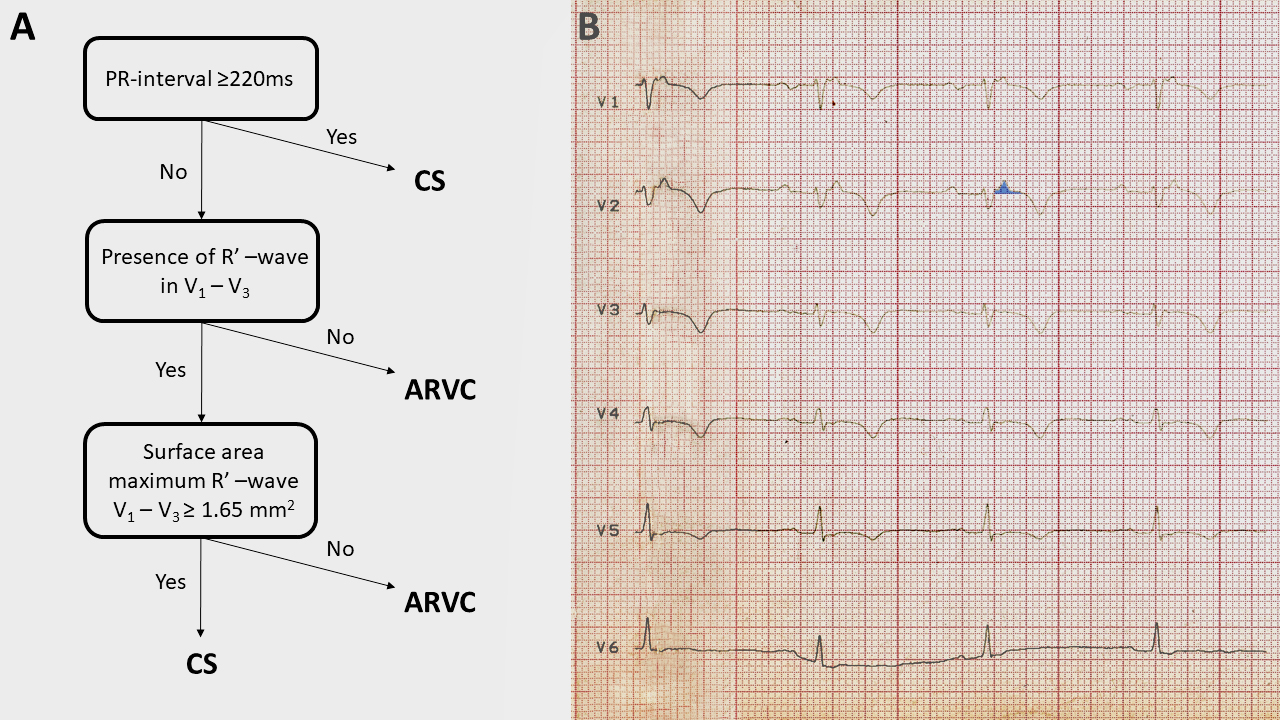
Fig. 1.The algorithm devised to distinguish sarcoidosis with left and
right ventricular involvement from ACM and its application to the ECG of our
patient who had CS mimicking ACM. (A) The ECG algorithm. (B) The application of
the algorithm on our patient’s ECG. The PR interval is 220–230 ms, thus already
the first step of the algorithm suggests CS. The surface area of the maximum R’
wave in lead V
No pathognomonic biomarker of CS exists. Serum angiotensin converting enzyme
(SACE), which is produced by activated macrophages and correlates with granuloma
burden, is elevated in 30–80% of patients with active sarcoidosis, but has
neither sufficient sensitivity nor specificity. SACE levels are decreased in
patients treated with ACE inhibitors. Serum soluble interleukin-2 receptor
(sIL-2R), which is a marker of T-cell activation, is also elevated in patients
with active sarcoidosis, and can be a marker of disease activity, but it is not
specific, and may be significantly elevated in other granulomatous diseases,
hematological malignancies and various autoimmune disorders. Other markers of
macrophage activation, such as lysozyme, neopterin, serum amyloid A,
chitotriosidase may also be elevated in patients with active sarcoidosis and
might be used to assess disease activity rather than as diagnostic markers, due
to their low specificity. Also elevated adenosine deaminase, due to T-lymphocyte
stimulation, might indicate sarcoidosis diagnosis and disease activity [1, 41, 42, 43].
Serum chitotriosidase was verified as a good biomarker of sarcoidosis, which
showed a higher sensitivity and specificity than other biomarkers, and correlated
well with disease activity, severity and multiorgan dissemination [44]. The
presence of lymphocytosis and an increased CD4+/CD8+ cell ratio of
Transthoracic echocardiography is usually the first imaging study performed in
patients with suspected CS, and although not a sensitive and specific examination
for CS, it can provide useful informations. CS can manifest with normal
ventricular function or with dilated or restrictive cardiomyopathy. The most
commonly observed echocardiographic abnormality is dilated cardiomyopathy with
globally hypokinetic left ventricle and secondary mitral regurgitation. During an
early stage of the disease thickening of the septum (usually its basal and
lateral wall), sometimes with increased echogenicity, may be seen. However the
thinning (
If the sceening tests (history, physical examination, ECG, echocardiography,
biomarkers) suggest a clinical suspicion of CS, advanced imaging studies, CMR and
FDG-PET/CT [usually together with resting myocardial perfusion single-photon
emission computed tomography (SPECT) or positron emission tomography (PET)] are
performed to confirm the presence of CS. Usually CMR is the first performed
advanced imaging modality, as it is the study of choice for diagnosing cardiac
involvement in sarcoidosis, due to its accuracy in the assessment of cardiac
structure (capability of detecting morphological abnormalities, such as wall
thinning, thickening, aneurysms) and function and tissue characterization by
detection of small areas of myocardial damage due to scarring or inflammation,
and its high negative predictive value (
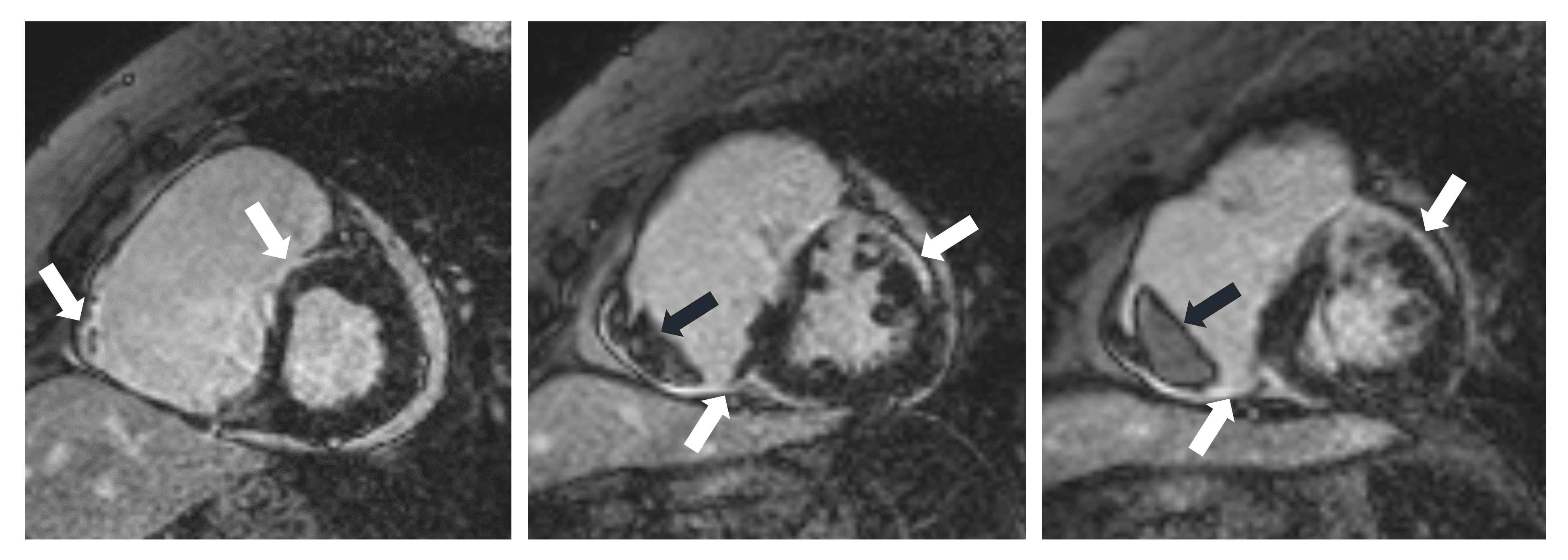
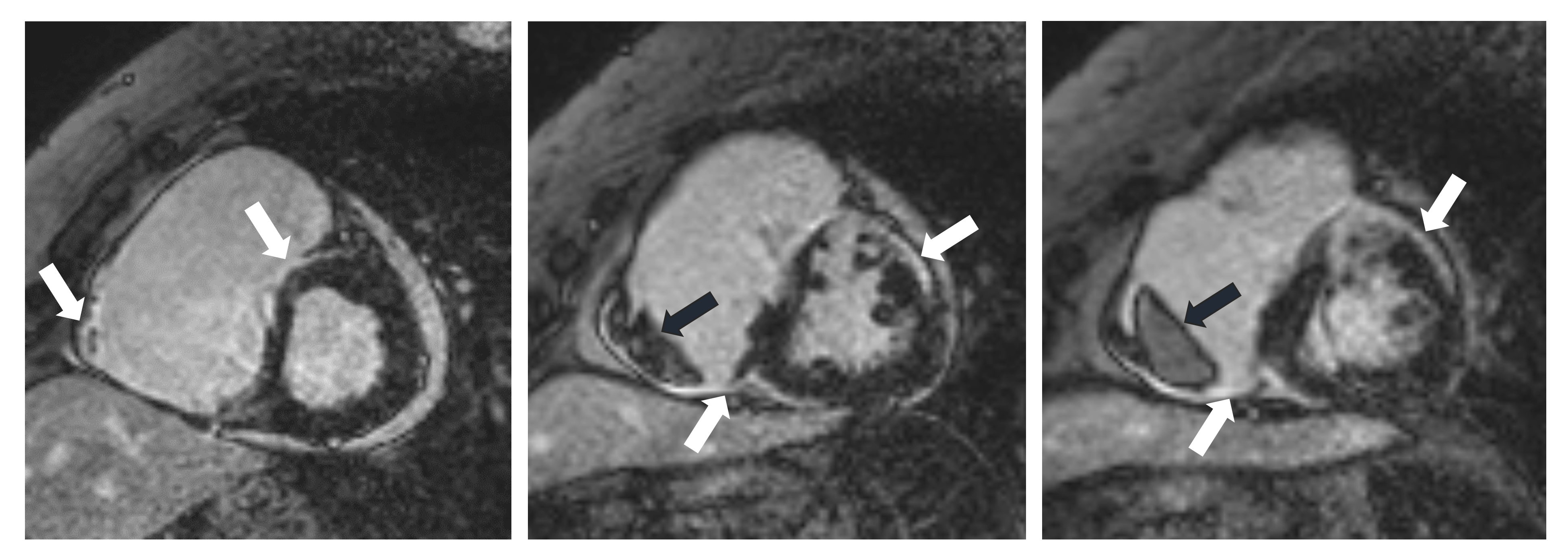 Fig. 2.
Fig. 2.CMR images of a 70-year-old female patient with CS. The delayed contrast enhancement images in short axis planes show biventricular late gadolinium enhancement (LGE) corresponding to fibrotic involvement (white arrows) and right ventricular thrombus formation (black arrows). Subepicardial LGE is present in the anterior septum, LV inferior wall, subepicardial-midmyocardial LGE is seen in the LV anterior wall and LGE is present in the RV myocardium in the vicinity of thrombus. CMR, cardiac magnetic resonance; CS, cardiac sarcoidosis; LV, left ventricle; RV, right ventricle.
Active inflammatory cells have high glycolytic activity and the accumulation of
fluorodeoxyglucose (FDG) in activated macrophages and CD4+ T-lymphocytes is the
underlying mechanism for in vivo visualization of active granulomatous
sarcoid lesions. The physiologic cardiac glucose metabolism should be switched
off by a low carbohydrate/high-fat diet for 12–24 h prior to the scan, followed
by a 12–18 h fasting and in some centers the use of 50 IU/kg intravenous
unfractionated heparin approximately 15 min prior to
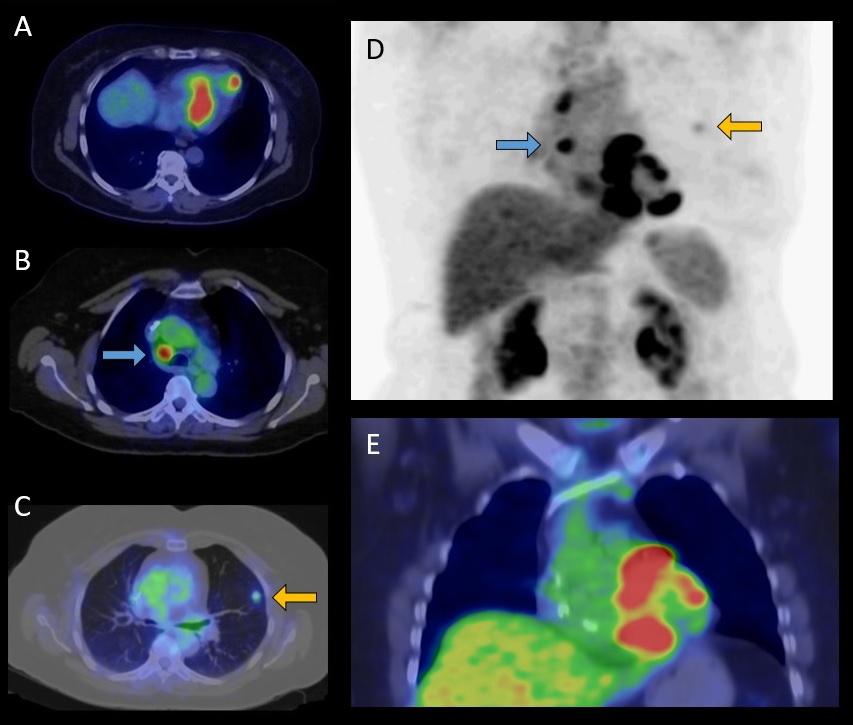
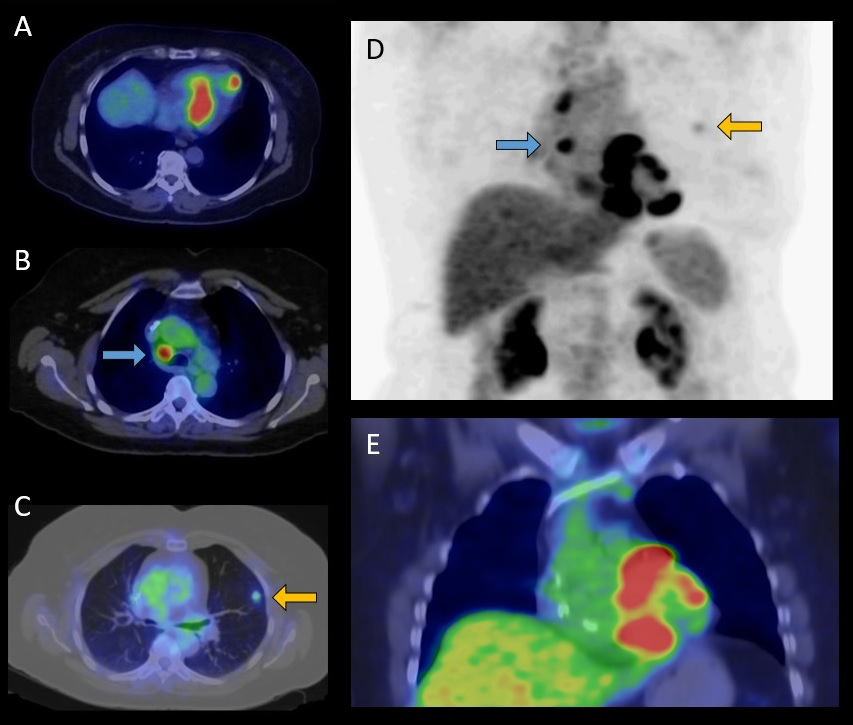 Fig. 3.
Fig. 3.FDG-PET/CT examination of a 65-year-old female patient with histologically (EMB) proven sarcoidosis. Axial fused (A,B,C) and coronal fused (E) PET/CT images and maximum intensity projection (MIP) PET image (D) show increased multifocal FDG uptake in the left ventricular myocardium (A,E) as cardiac involvement, high focal lymph node uptake ((B,D) marked by blue arrows) and pulmonary uptake ((C,D) marked by yellow arrows) indicative for extracardiac manifestation of sarcoidosis. FDG-PET/CT, 18F-fluorodeoxyglucose positron emission tomography/computed tomography; EMB, endomyocardial biopsy.
A standard FDG-PET/CT is usually performed in conjunction with resting myocardial perfusion imaging to confirm the presence of CS. Both SPECT (99mTc labelled tracers) and PET (rubidium or ammonia) myocardial perfusion imaging methods are acceptable, based on the availability of different radiotracers, although the spatial resolution of PET is significantly higher compared to SPECT [64]. A “mismatch pattern” with FDG accumulation within and in the surrounding areas of a perfusion defect is highly suggestive of CS, as granulomas may impair coronary microcirculation leading to perfusion defects in non-coronary distribution, which can be reversible on treatment, but replacement fibrosis in the chronic stage causes irreversible perfusion defects, that can be associated with segmental wall motion abnormalities. The following combined FDG and myocardial perfusion imaging patterns can be present: (1) “early” (only FDG positive), (2) “progressive inflammatory” (FDG positive without major perfusion defects), (3) “peak active” (high FDG uptake with small perfusion defects), (4) “progressive myocardial impairment” (high FDG uptake with large perfusion defects), and (5) “fibrosis predominant” (perfusion defects without FDG uptake). It is mandatory to rule out coronary artery disease as an alternative diagnosis by cardiac CT or coronary angiography, if perfusion defects are present [45]. In a meta-analysis the pooled sensitivity was 89% and the specificity was 78% of FDG-PET in the detection of CS [65, 66]. In the future cardiac PET studies using tracers that work without dietary preparation, such as somatostatin analogs, and hybrid PET/CMR imaging may further improve diagnostic accuracy [20, 67]. It should be noted that abnormal FDG uptake is not specific for CS, it can also be present in ACM, Lamin A-mutation related cardiomyopathy, myocarditis (giant cell myocarditis), hibernating myocardium, connective tissue, and rheumatic disease with cardiac involvement. The absence of extracardiac uptake decreases the specificity of FDG-PET for CS [20, 47]. It is important that FDG-PET can also be used to detect extracardiac sarcoidosis. Atrial FDG uptake predicts atrial tachyarrhythmia. FDG-PET has also prognostic implications. A “mismatch pattern” and RV uptake are the key predictors of cardiac events [66, 68, 69].
Due to the insufficient sensitivity and associated risk of endomyocardial
biopsy, the diagnosis in the majority of CS cases is based on findings of
extracardiac tissue biopsy combined with the patient’s clinical presentation and
advanced cardiac imaging findings. Chest CT or whole-body FDG-PET scan can
identify lung tissue and mediastinal or hilar lymphadenopathy suitable for
extracardiac tissue biopsy. Endobronchial ultrasound-guided biopsy is preferable
over mediastinoscopy for lymph node biopsy and provides a higher yield, has a
better sensitivity and lower procedural risk than endomyocardial biopsy
[1, 20, 35]. Due to the patchy distribution of non-caseating granulomas in CS,
endomyocardial biopsy (EMB) performed as a non-targeted RV biopsy has a poor
diagnostic yield and a low 20–30% sensitivity. This can be improved by
performing CMR or FDG-PET or electroanatomical mapping guided EMB, if a clear
involvement of the RV or the interventricular septum can be verified, and by
taking more, 10–15 heart muscle samples. By using these methods the sensitivity
of EMB can be increased to 50–77% [15, 33, 70, 71]. Potential complications of EMB
include rupture of the RV free wall causing tamponade, conduction disturbance,
arrhythmias, pneumothorax, tricuspid valve regurgitation and pulmonary embolism.
The risk of complications is relatively low,
The hallmark histological finding in CS is non-caseating, non-necrotizing
granulomas composed of aggregates of tightly clustered epithelioid macrophages
often with multinucleated giant cells with or without surrounding
lymphocytic/granulocytic infiltration combined with myocardial fibrosis, sharply
demarcated areas of involvement, but no extensive eosinophilia or myocyte
necrosis (Fig. 4). However, the typical non-caseating granulomas are seldom
observed in the EMB specimen, therefore diagnostic confirmation of CS is often
difficult. A combination of some novel surrogate histological findings, such as
microgranulomas, increased number of dendritic cells, the accumulation of
pro-inflammatory M1 (CD68
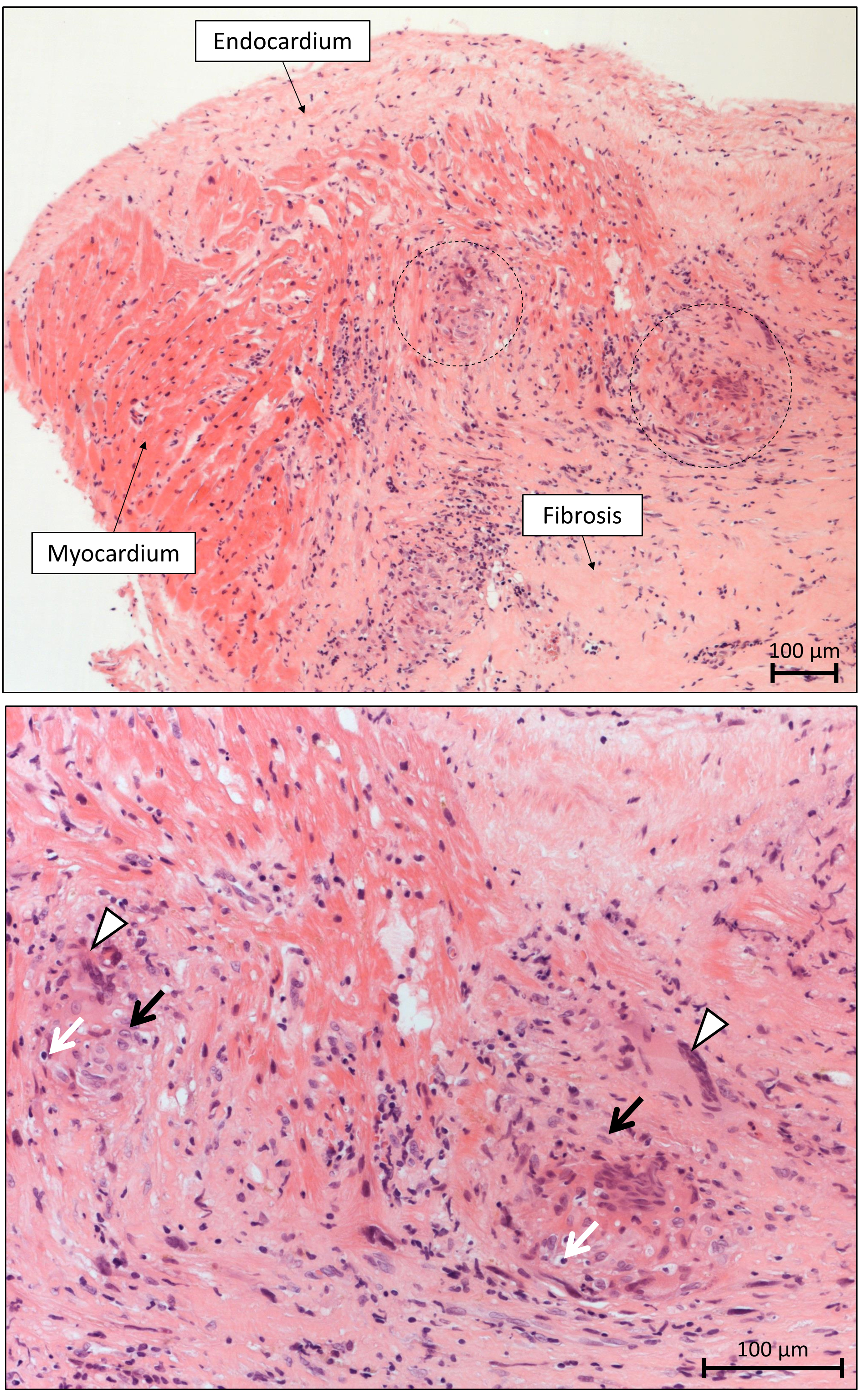
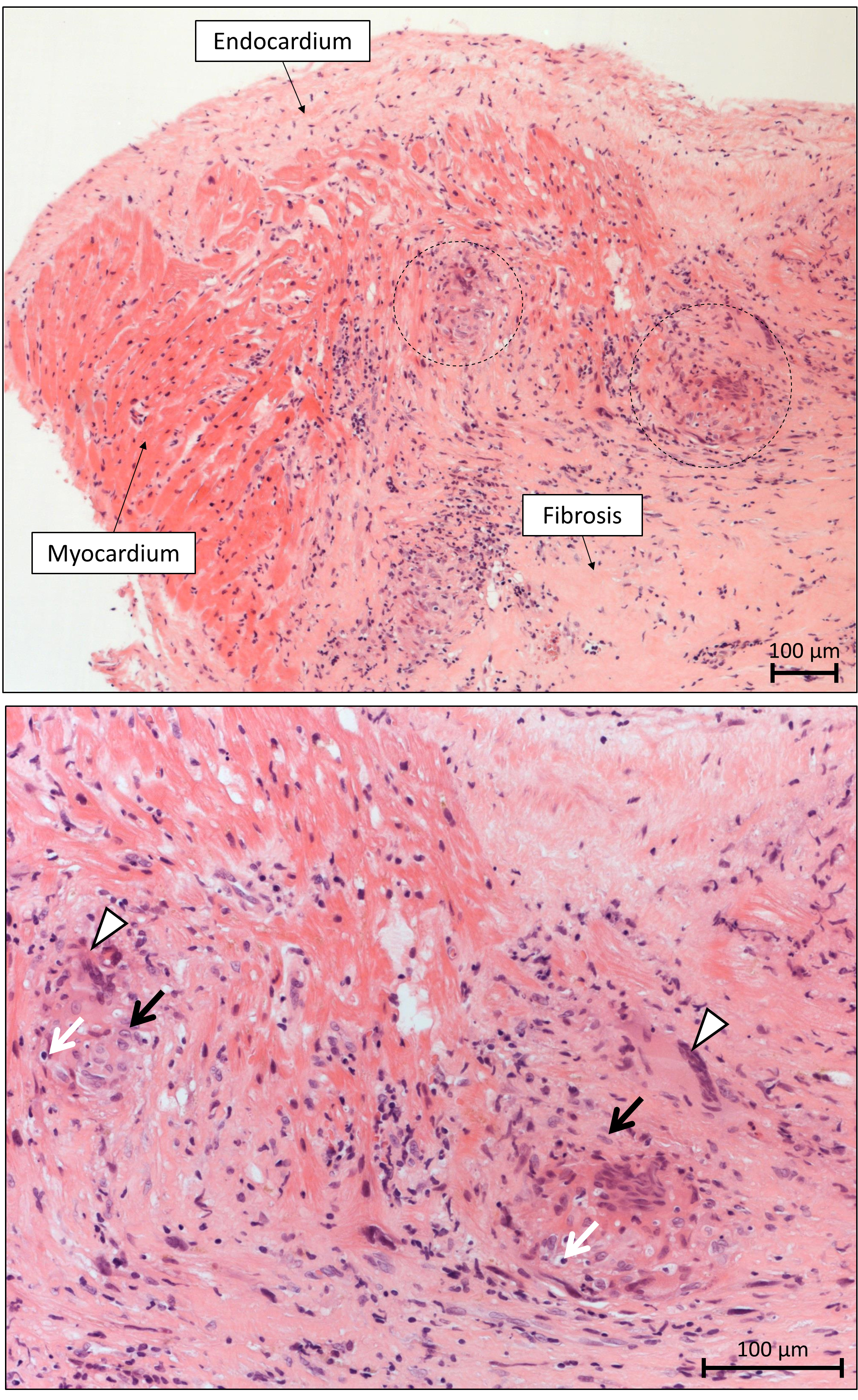 Fig. 4.
Fig. 4.Microscopic appearance of sarcoidosis in the endomyocardial
biopsy specimen. Top: The non-necrotizing granulomatous inflammation of the
myocardium is sharply demarcated, and it is typically surrounded by diffuse
fibrosis. The granulomas (- - -) are scattered and typically well circumscribed
in sarcoidosis. Diffuse necrosis of cardiomyocytes is absent (H&E staining,
10(
In the differential diagnosis of CS ACM, desmoplakin cardiomyopathy,
lymphocytic, eosinophilic and giant cell myocarditis, non-ischemic dilated
cardiomyopathy or ischemic cardiomyopathy, restrictive cardiomyopathy, some
genetic cardiomyopathies and granulomatous infections should be mostly considered
[20, 26]. The difficulty in distinguishing CS from other cardiac diseases is
indicated by the fact that the classification of CS is not yet fully determined.
In the 2023 ESC Cardiomyopathy Guideline CS is classified as a dilated
cardiomyopathy, in a review article as a restrictive cardiomyopathy, and in the
2022 ESC Guideline on ventricular arrhythmias and SCD neither as dilated nor as
restrictive cardiomyopathy, but as an inflammatory cardiac disease [77, 78, 79]. CS
can perfectly mimic ACM with biventricular involvement fulfilling its all
diagnostic criteria, however presentation of symptoms at an older age, negative
family history, AV conduction abnormalities (any degree of AV block), the
presence of R’ wave and the surface area of the maximum R’ wave in leads V
Patients with clinically manifest symptomatic CS are treated with immunosuppressive therapy. However, there is no evidence and therefore no consensus whether treatment should be started based on the presence of active lesions or based on the presence of clinical symptomatology. Whether immunosuppressive therapy should be initiated in patients with asymptomatic, metabolically active CS on FDG-PET and normal ventricular function without conduction disturbance and ventricular arrhythmias is less clear, because there is no unequivocal evidence from randomized studies for the benefit of immunosuppression in these patients. Therefore some experts recommend individualized treatment of these patients based on the consideration of the extent of myocardial inflammation, systemic involvement and potential risks of therapy. But many other experts recommend the immunosuppressive treatment of these asymptomatic patients in order to prevent disease progression to fibrosis and later severe cardiovascular complications [10, 20, 26]. Sarcoidosis experts agree on the treatment of CS with immunosuppressive therapy for the following clinical scenarios: LV dysfunction, ventricular arrhythmias, hypermetabolic activity on cardiac FDG-PET, presence of conduction defects, LGE on CMR, or RV dysfunction in the absence of pulmonary hypertension [45]. Isolated CS has a poorer prognosis than CS associated with systemic sarcoidosis, because it presents with lower LVEF and frequent ventricular arrhythmias and SCD. Therefore its treatment might be more indicated, even in asymptomatic cases [46, 93, 94].
Immunosuppression with corticosteroids is the first-line treatment of patients
with CS. A review of 34 clinical reports involving 1297 patients concluded that
corticosteroids improve AV conduction in 40% of patients and may prevent the
deterioration of LV function, whereas their effect on ventricular arrhythmias and
mortality remains ambiguous due to poor data quality [20, 95]. There are
contradictory results whether corticosteroid therapy is beneficial in patients
with severe LV dysfunction (LVEF
Second-line immunosuppressive agents, including methotrexate, azathioprine, mycophenolate mofetil, leflunomide, cyclophosphamide, are used in patients with refractory disease, or if the dose of corticosteroid needs to be reduced to prevent or diminish its adverse effects. The most commonly used second-line agent is methotrexate used in a weekly dose of 10–20 mg. Azathioprine, which is also used frequently, is applied in a 1–2 mg/kg body weight/day dose. Both need follow-up to check for adverse effects, including bone marrow suppression, infections, hepatotoxicity, renal failure, gastrointestinal complications, interstitial pneumonitis, pulmonary fibrosis, and teratogenicity. There are some data supporting combination therapy from the very beginning, but there is not yet a good evidence for improved outcome achieved by this combined therapy compared with only corticosteroid treatment. However, due to the multiple significant side effects of corticosteroid therapy, many centers consider the initial use of combined therapy with medium to low dose of corticosteroids in association with a sparing immunosuppressive agent, such as methotrexate [20, 101].
Biological therapy using TNF-
The Cardiac Sarcoidosis Multicenter Randomized Trial (CHASM CS-RCT) that tests the hypothesis that low-dose prednisone-methotrexate combination is as effective as a standard dose of prednisone is expected to publish the results in approximately 3 years. The Japanese Antibacterial Drug Management for CS (J-ACNES) trial is a randomized, multicenter trial comparing corticosteroid therapy given alone or together with antibiotics (chlarithromycin and doxycycline) based on the assumed pathogenetic role of Propionibacterium acnes. The Interleukin-1 Blockade for Treatment of CS (MAGIC-ART) is a randomized trial comparing standard care alone with standard care+IL-1 blocker (anakinra) treatment in CS. The RESOLVE-Heart trial is investigating the efficacy, safety and tolerability of namilumab, a monoclonal antibody, targeting the granulocyte macrophage colony stimulating factor in active CS [20, 46].
In many centers repeated FDG-PET studies are performed as a gold standard test
to determine the extent, presence or absence of myocardial inflammation and its
response to therapy and to tailor treatment accordingly. It was shown that
reduction of myocardial inflammation was associated with an improvement in LVEF
[26, 46, 47, 102]. Several studies indicated that serial FDG-PET is feasible to
determine the extent of disease activity and to quantitatively assess the
response of CS to therapy [103, 104]. To evaluate response to treatment baseline
and follow-up cardiac FDG-PET scans are performed. The therapeutic response is
analyzed visually and quantitatively, the widely used quantitative parameters are
the maximum and mean standardized uptake values (SUV
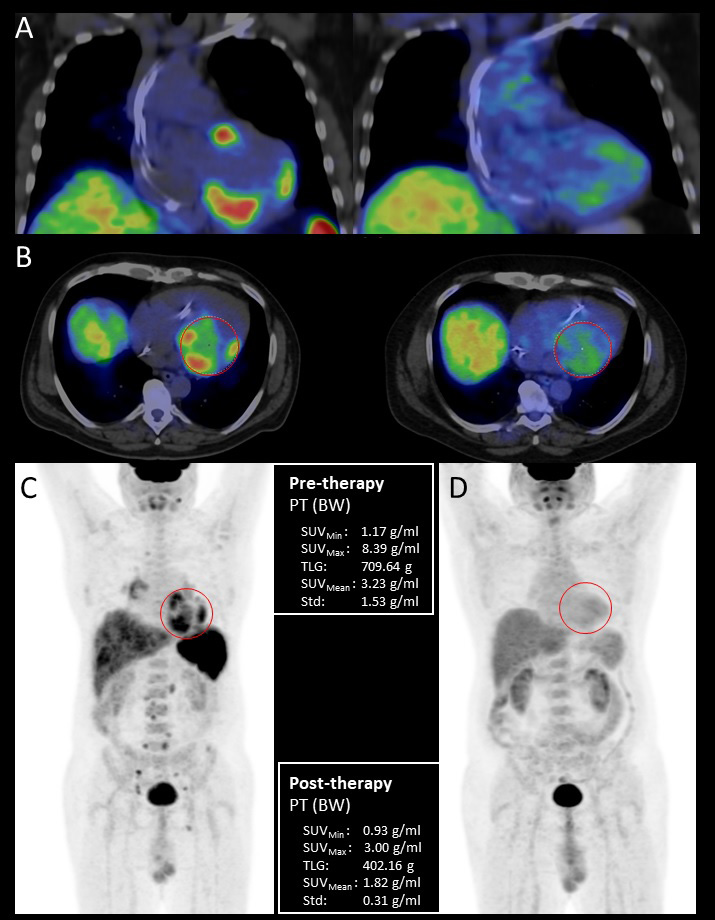 Fig. 5.
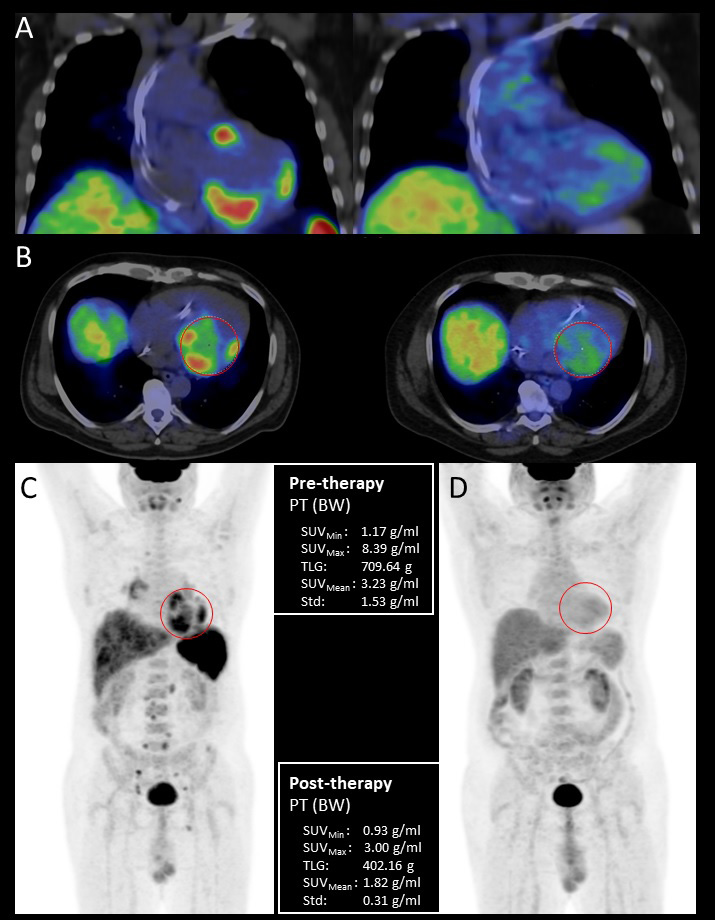
Fig. 5.Pre- and posttreatment FDG-PET/CT examination of a 44-year-old male patient with histologically (EMB) proven sarcoidosis. Coronal fused pretreatment and posttreatment (A) and axial fused (B) PET/CT images with volume of interest (VOI) and maximum intensity projection (MIP) PET images before (C) and after immunosuppressive therapy (D) with quantitative parameters. Pretreatment scans show increased multifocal FDG uptake in the left and right ventricular myocardium as cardiac involvement, the presence of high focal supra- and infradiaphragmatic lymph node uptake is indicative of extracardiac sarcoidosis. Posttreatment scans do not show pathological FDG uptake confirming complete treatment response. EMB, endomyocardial biopsy; BW, body weight; FDG-PET/CT, 18F-fluorodeoxyglucose positron emission tomography/computed tomography; PT, positron emission tomography; SUV, standardized uptake values; TLG, total glycolytic activity.
In the case of active inflammation corticosteroid treatment is recommended for the treatment of ventricular arrhythmias together with antiarrhythmic drugs, mainly amiodarone or sotalol for VT. If medical therapy is not effective, and the ventricular arrhythmia is felt scar based, catheter ablation can be considered. In contrast to AV block, which primarily develops in CS during the acute, inflammatory phase, sustained VT more commonly develops in the advanced stage of CS, due to a scar-related substrate. VT ablation can help to control VT storm or incessant VTs, which have a relatively high incidence in CS. In cases refractory to medical and catheter ablation therapy bilateral cardiac sympathectomy may be considered [10, 20, 32, 35, 77, 105].
SCD is considered responsible for the majority of deaths in CS, patients with
clinically manifest CS having a 10% risk of SCD over 5 years of follow-up
[10, 106]. Table 3 (Ref. [35]) and Fig. 6 (Ref. [79]) summarizes the
recommendations given by the HRS [33], the ACC/AHA/HRS consortium [107] and the
ESC [79] guidelines. General implantable cardioverter defibrillator (ICD) indications for secondary prevention, such as
documented sustained VT, prior aborted cardiac arrest, are also applicable for
patients with CS. In a patient with CS and LVEF
| Indications for ICD in CS class of recommendation | |
| Documented sustained VT, prior aborted cardiac arrest or LVEF |
I |
| LVEF |
IIa |
| History of syncope/near syncope compatible with arrhythmia-related etiology | IIa |
| Inducible sustained ventricular arrhythmia at PES | IIa |
| LVEF |
IIa |
| LVEF 36–49% and RVEF |
IIb |
Adapted with modifications from [35].
CS, cardiac sarcoidosis; GDMT, guideline directed medical therapy; ICD,
implantable cardioverter- defibrillator; LGE, late gadolinium enhancement; PES, programmed electric stimulation; VT, ventricular tachycardia;
LVEF, left ventricular ejection fraction; PET,
positron emission tomography; CMR, cardiac magnetic resonance; RVEF, right
ventricular ejection fraction.
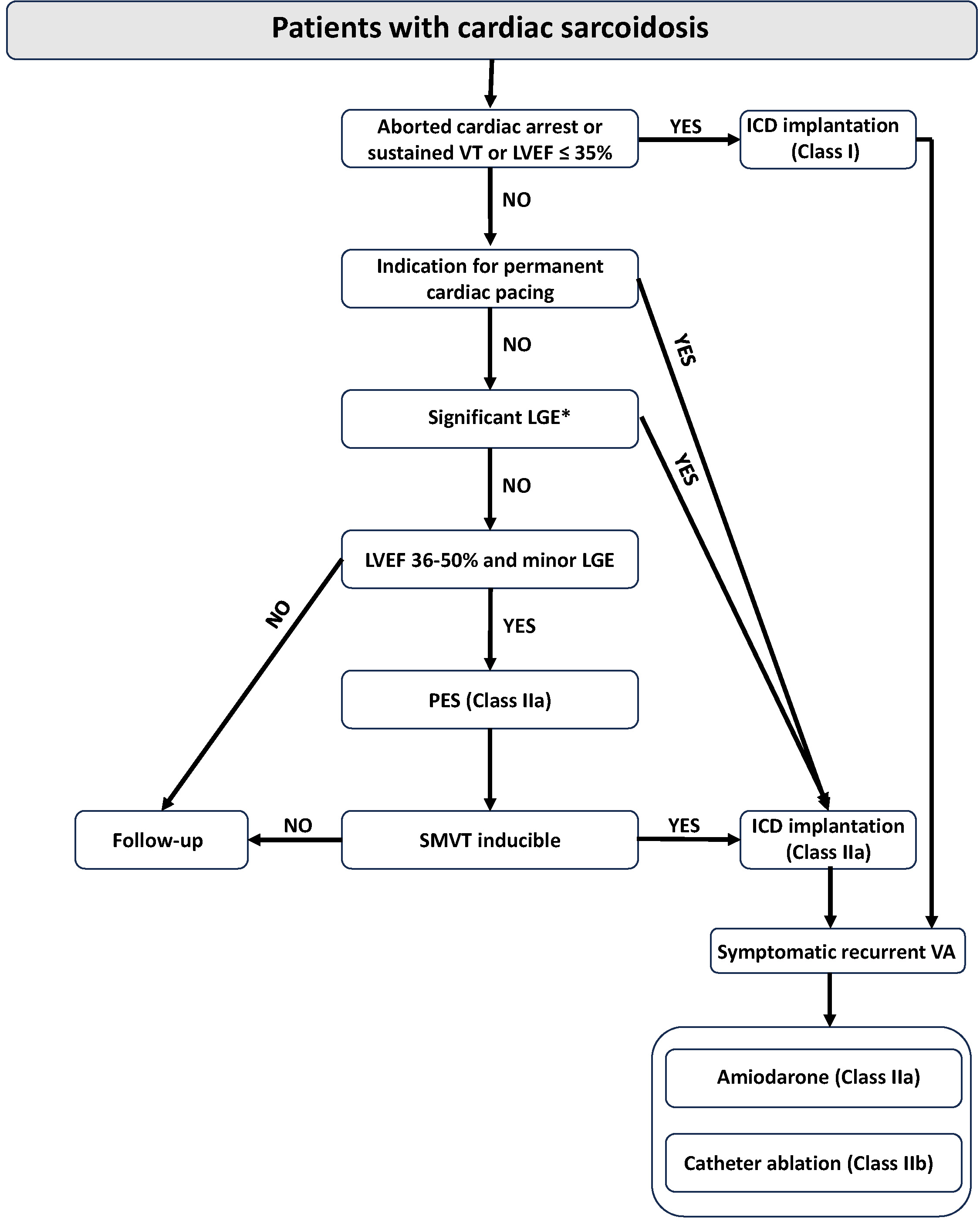 Fig. 6.
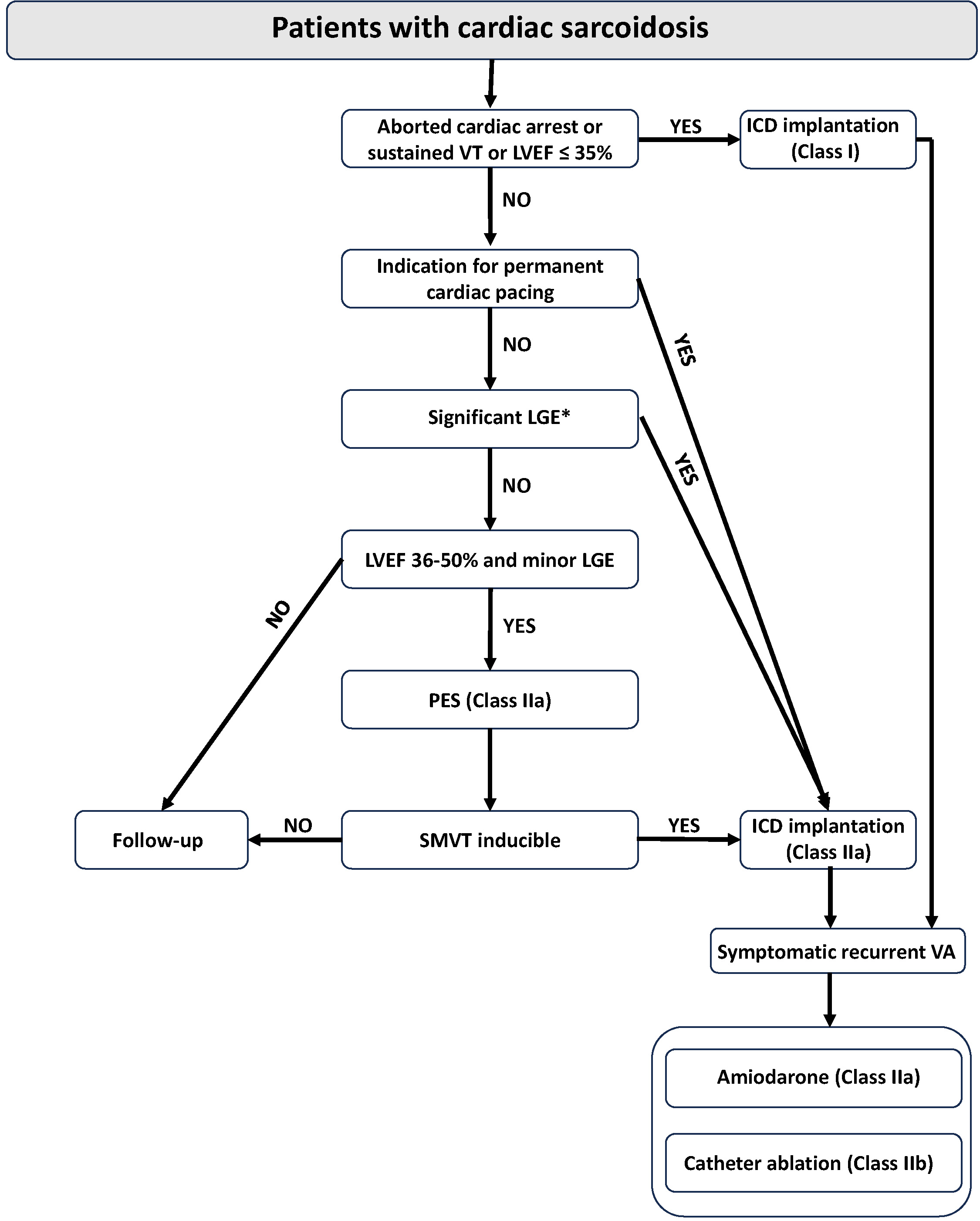
Fig. 6.Algorithm for sudden cardiac death prevention and treatment of
ventricular arrhythmia in patients with cardiac sarcoidosis. ICD, implantable
cardioverter defibrillator; LGE, late gadolinium enhancement; LVEF, left
ventricular ejection fraction; PES, programmed electrical stimulation;
SMVT, sustained monomorphic ventricular tachycardia; VA, ventricular arrhythmia;
VT, ventricular tachycardia. *LGE affecting
In the rare cases of CS-related fulminant myocarditis aggressive immunosuppressive therapy and mechanical circulatory support may be necessary. In CS patients with heart failure and ventricular dyssynchrony rather CRT-D, than cardiac resynchronization therapy with a-pacemaker (CRT-P) is recommended. In patients with end-stage CS mechanical circulatory support (LV assist device) and cardiac transplantation can be considered. Patients with CS have a similar post-transplant survival and risk of late complications as other transplant recipients. Recurrence of CS in the allograft is rare and not resulted in transplant failure [20, 114, 115, 116].
The prognosis of CS patients is less favorable than the prognosis of patients
with sarcoidosis without cardiac involvement [5]. Contemporary data show improved
prognosis of patients with CS compared with earlier data, due to modern heart
failure management and an increasing use of ICDs. A Finnish study of biopsy
verified CS patients found a 92.5% transplant-free 10-year survivals and other
studies showed
Although CS is increasingly recognized, it remains a diagnostic and therapeutic
challenge requiring a multidisciplinary approach. Its timely recognition and
treatment has utmost importance since it is the second most frequent cause of
death from sarcoidosis, and its early treatment may prevent life-threatening
arrhythmias, SCD and heart failure. CS should be considered in all patients with
extracardiac sarcoidosis, even if they have no symptoms suggesting cardiac
involvement, and in all
AV prepared and wrote up the greatest part of the manuscript and managed some of the patients with cardiac sarcoidosis. ZB, BR, and HV are experts of nuclear medicine, pathology and cardiac MRI respectively, and contributed significantly to these parts of the manuscript and to the work-up of patients with cardiac sarcoidosis. VN, ZJ, GK participated in the management of patients with cardiac sarcoidosis and in the preparation of the manuscript. RS is an expert of cardiomyopathies, who contributed significantly to the preparation and critical review of the manuscript and management of patients. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.