



 , Mingxing Xie 1,2,3,*
, Mingxing Xie 1,2,3,*1 Department of Ultrasound Medicine, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, 430022 Wuhan, Hubei, China
2 Clinical Research Center for Medical Imaging in Hubei Province, 430022 Wuhan, Hubei, China
3 Hubei Province Key Laboratory of Molecular Imaging, 430022 Wuhan, Hubei, China
†These authors contributed equally.
Abstract
Mitral regurgitation is the second most prevalent valvular disease, with primary mitral regurgitation (PMR) accounting for 61%–67% of cases. Chronic PMR can result in progressive left ventricular remodeling and dysfunction, ultimately leading to heart failure or other adverse cardiac events. This, in turn, necessitates frequent referrals, hospitalizations, and cardiac surgeries. The optimal timing for PMR surgery has been a subject of ongoing debate and remains a controversial issue. Presently, it is recommended that patients with chronic PMR undergo earlier mitral valve surgery to enhance post-operative outcomes. For example, the recommendation of European and American guidelines about left ventricular end-systolic diameter for surgery has been altered from 45 mm to 40 mm. Echocardiographic parameters are regarded as noteworthy indicators for intervention in patients with PMR. Extensive research has been undertaken in the field of echocardiography to identify more effective indicators that can propose the optimal timing for surgery, encompassing both conventional and novel echocardiography parameters. However, some parameters are not known to clinicians and the cut-off values for these parameters have shown some variations. Furthermore, a comprehensive review of this topic is currently missing. Consequently, this review aims to provide a thorough summary and elucidation of the prognostic significance of various echocardiographic measurements and their corresponding cut-off values, to help the clinical decision-making and further improve the outcomes of patients with PMR.
Keywords
- echocardiology
- primary mitral regurgitation
- surgery
- prognosis
Mitral regurgitation (MR) is the second most prevalent valvular disease [1, 2], with primary mitral regurgitation (PMR) accounting for 61%–67% [1, 2]. Chronic PMR can result in progressive left ventricular (LV) remodeling and dysfunction, ultimately leading to heart failure or other adverse cardiac events [3]. This, in return, necessitates frequent referrals, hospitalizations, and cardiac surgery [4]. Besides, the burden of PMR is expected to rise with population aging [5]. The optimal timing for PMR surgery has been a subject of ongoing debate and remains a contentious issue. Presently, it is recommended that patients with chronic PMR undergo earlier mitral valve surgery to enhance post-operative outcomes. For example, the patients would be better off undergoing surgery when their left ventricular end-systolic diameter (LVESD) reaches 40 mm rather than waiting until 45 mm [6, 7, 8]. Current guidelines recommend the presentation of symptoms and left ventricular dysfunction as Class I indications for intervention in patients with PMR [7, 9]. However, left ventricular ejection fraction (LVEF) and LVESD are dependent on LV geometry, heart rate, and volume status [10], and can overestimate the LV systolic function in patients with PMR, although the value of these parameters has been suggested [11, 12, 13, 14, 15, 16]. As a result, more precise and sensitive measures for determining optimal intervention timing are needed.
Furthermore, extensive research has been undertaken in the field of echocardiology to identify more effective indicators that can propose the optimal timing for surgery, encompassing both conventional and novel echocardiographic parameters. However, the question lies in that substantial new parameters and cut-off values were not used in clinical practice, because some variations existed in the published trials and no review has analyzed those results systematically, making it hard to impact decision making.
Consequently, in order to help the clinical decision-making and further improve the outcomes of patients with PMR, this review aims to provide a comprehensive summary and elucidation of the published evidences concerning the prognostic significance of these parameters and their cut-off values (Fig. 1).
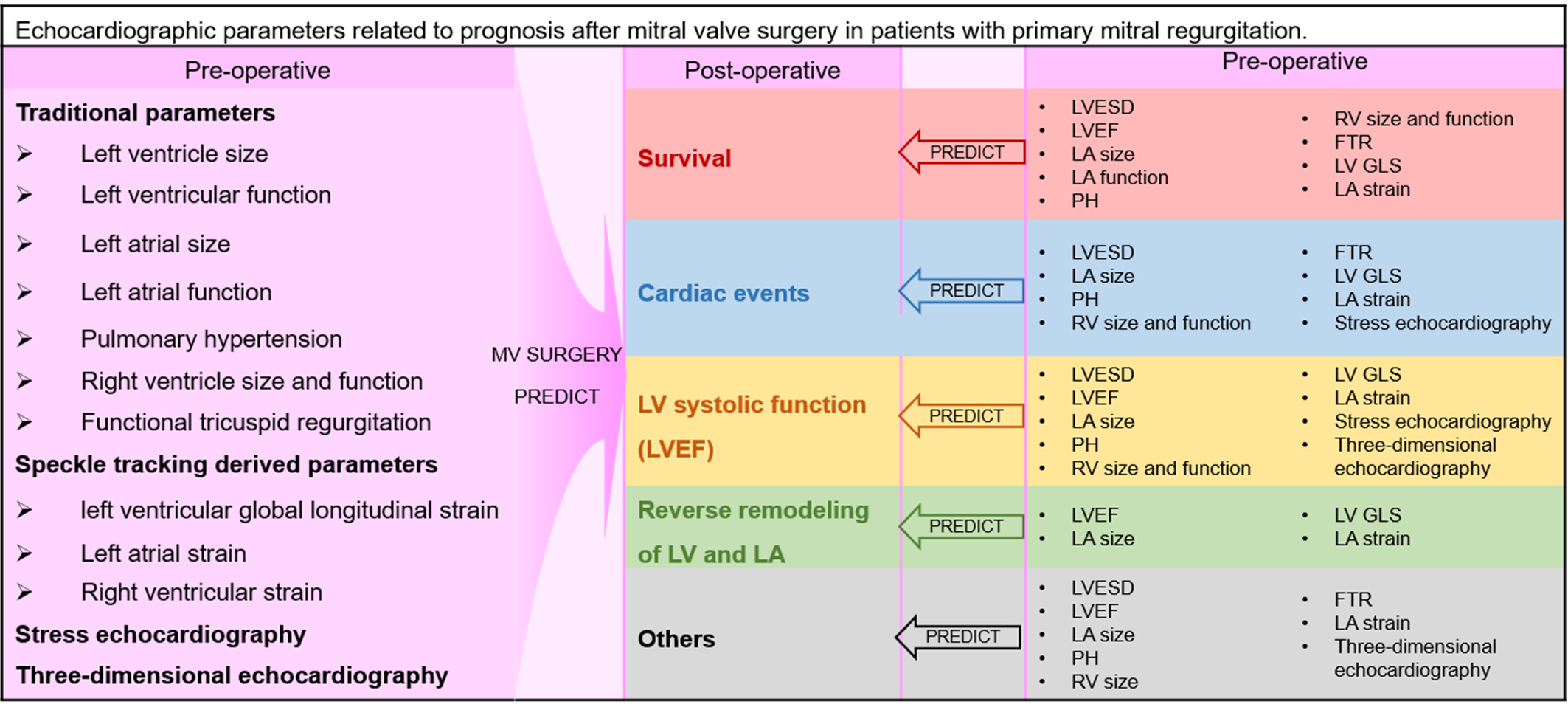 Fig. 1.
Fig. 1.
Echocardiographic parameters related to prognosis after mitral valve surgery in patients with primary mitral regurgitation. Please note that colors from Fig. 1 are used in all supplementary tables, and different colors are used to distinguish particular post-operative prognosis (red, survival; blue, cardiac events; gold, LVEF; green, reverse remodeling of LV and LA; grey, other post-operative outcomes). LVEF, left ventricular ejection fraction; LV, left ventricle; LA, left atrium; LVESD, left ventricular end-systolic diameter; PH, pulmonary hypertension; FTR, functional tricuspid regurgitation; LV GLS, left ventricular global longitudinal strain; RV, right ventricle; MV, mitral valve.
LVESD was a well-recognized prognostic parameter for post-operative LV performance in patients who underwent mitral valve (MV) surgery [17]. It is demonstrated that pre-operative LVESD was useful for predicting various outcomes, including LV dysfunction [18, 19, 20, 21, 22, 23], LVEF deterioration [14], cardiac events [23], as well as mortality [15, 16] during follow-up (Supplementary Table 1).
Based on previous studies of the predictive value of LVESD [15, 20, 21],
American College of Cardiology/American Heart Association (ACC/AHA) have
recognized LVESD
However, some studies have reported different cut-off values for LVESD. For
instance, Tribouilloy et al. [22] found a cut-off value of 37 mm to
predict LV dysfunction, while Kitai et al. [19] identified 39 mm as a
predictor for LV dysfunction. These values differ from the guideline-recommended
40 mm. Additionally, Li et al. [14] discovered that in patients with PMR
and LV systolic dysfunction (LVEF
Other parameters reflecting LV size have also been studied for their predictive
value. Left ventricular end-systolic diameter index was demonstrated to be
predictive of LV dysfunction six months after surgery, with a cut-off value of 22
mm/m2 [21]. Left ventricular end-systolic volume index (LVESVi) was
identified as the best marker of LV impairment one year after operation, with an
optimal cut-off of 36.3 mL/m2 (area under curve (AUC) 0.738 [0.56–0.71])
[24]. Furthermore, left ventricular end-diastolic diameter (
LVEF is a classical parameter to assess LV systolic function. It has been demonstrated that pre-operative LVEF holds prognostic value in predicting post-operative LV dysfunction [13, 19, 22, 23, 25, 26], a reduction in LVEF [14], left atrial reverse remodeling (LARR) [27], recurrent MR [16], and mortality [12, 16] during follow up (Supplementary Table 2). This indicates the importance of assessing LVEF prior to surgery as it can provide valuable insights into the potential outcomes and complications that may arise after the procedure.
Based on previous studies [25, 26], LVEF
However, the cut-off values of LVEF reported by some studies are different, such
as 63% suggested by Kitai et al. [19] and 64% suggested by Tribouilloy
et al. [22]. In addition, for PMR patients with LVEF
LV Tei index (myocardial performance index) serves as a measure of both systolic and diastolic function, but its predictive value has shown inconsistency across various studies. In a study by Mabrouk-Zerguini et al. [31] involving 25 patients who underwent MV repair, the Tei index was found to be capable of predicting immediate post-operative LV fractional area change. This predictive ability was noted to assist in identifying patients who might encounter challenges during the weaning process from cardiopulmonary bypass. However, a study by Mukherjee et al. [32], which included 130 patients undergoing MV repair, revealed that pre-operative Tei index was not able to predict left ventricular function immediately after surgery.
While the predictive value of diastolic function in PMR has been explored, the
existing research is limited. One study reported that late diastolic tissue
Doppler imaging a′ (a′-TDI) wave of the septal apical wall (
Left atrial (LA) size plays a crucial role in patients with chronic PMR because
LA can adapt to the volume overload resulting from regurgitation [35]. LA size
can be measured by LA dimension, area, and volume [36, 37]. Many related studies
showed associations between pre-operative enlarged LA and post-operative adverse
outcomes [13, 37, 38, 39, 40, 41, 42, 43], such as atrial fibrillation (AF) [40, 43], all-cause
mortality [37, 38, 39], cardiac events [39] and LV dysfunction [13]
(Supplementary Table 3). The current ESC/EACTS guideline recommends that
enlarged LA (volume index
However, Song et al. [44] showed that pre-operative LAVi was negatively
associated with post-operative LARR (
Except for emerging data about the prognostic value of LA volume in PMR, LA
function assessment has also started to be concerned [47]. LA coupling index is a
clinically achievable parameter that couples LA volumetric and mechanical
characteristics, calculated as the ratio of LAVi to a′-TDI at the mitral
annulus. Through analysis of a large cohort of PMR patients, Essayagh et al. [48] demonstrated that higher LA coupling index was associated with higher
mortality (HR 1.13 [1.00–1.24], p = 0.04 per 3 units), and LA coupling
index has significant incremental predictive power over LAVi (p
AF occurs around in 30–42% of PMR patients at diagnosis [45, 49, 50]. AF was confirmed to be an independent predictive factor of worse outcomes, including excess long-term mortality [50, 51] and post-operative LV dysfunction [19, 20, 45, 49, 50], although AF is associated with older age, severity of PMR and LA size [49, 50]. AF is considered a prompt trigger for intervention regardless of patients’ symptoms [19, 20, 45, 50].
A series of downstream changes can occur following chronic PMR. Volume overload caused by PMR leads to a sustained increase in LA volume and pressure. Consequently, it is transmitted backward into the pulmonary veins and then PH occurs [52]. Then the elevated right ventricular (RV) afterload can lead to right heart remodeling, functional tricuspid regurgitation (FTR), and finally RV dysfunction or failure [52]. The interactions among PH, RV size and function, and FTR remain complex and their prognostic value have been studied.
It is reported that approximately 20%–30% of patients with severe PMR were
present with significant PH (systolic pulmonary arterial pressure [SPAP]
What’s more, Le Tourneau et al. [54] reported that SPAP cut-off value
of 50 mmHg could predict all-cause mortality with a sensitivity of 61% and a
specificity of 72% (AUC 0.7, p
Additionally, although cardiac catheterization is the gold standard for PH diagnosis, echocardiology is the most convenient and commonly used tool to evaluate SPAP in clinical practice, it is worthy paying more attention to the prognostic value of echocardiology-derived PH in patients with PMR.
Generally, dilated RV size and impaired RV function are often indicative of a more advanced stage of disease progression [52]. The prognostic significance of RV size and function in patients with PMR has been the subject of investigation, with various parameters used to evaluate the RV, including RV size, RV fractional area change (RV FAC), right ventricular ejection fraction (RV EF), tissue Doppler–derived tricuspid lateral annular systolic velocity (s′-TDI), tricuspid annular plane systolic excursion (TAPSE), and RV index of myocardial performance (RV MPI) [62].
Studies have shown significant associations between RV parameters and clinical
outcomes in patients undergoing MV surgery (Supplementary Table 5). For
instance, Gackowski et al. [28] reported that right ventricular
end-diastolic diameter (RVEDD) was independently predictive of a prolonged ICU
stay after MV replacement, with the cut-off value being 35 mm. Haddad et al. [63] pointed out that a smaller RV FAC was linked to in-hospital mortality
or circulatory failure (odds ratio [OR] 0.001 [
FTR is not uncommon in patients requiring MV surgery, with the prevalence
ranging from 25% to 59% [68, 69], and the prevalence of moderate or greater FTR
ranging from 8% to 45% [70, 71]. The studies concerning the effects of FTR were
summarized in Supplementary Table 6. It is demonstrated that increasing
grades of pre-operative FTR was associated with poorer post-operative survival
[69, 70, 72, 73, 74], congestive heart failure [69, 70] or FTR progression [69] during
long-term follow up. Given these poor prognoses associated with FTR, concomitant
surgical or transcatheter treatments of FTR have been more frequent in recent
years [75]. Current ESC/EACTS and ACC/AHA guidelines recommended that, for FTR
attributed to left-sided valve diseases, tricuspid valve surgery be performed in
patients with severe FTR undergoing concomitant left-sided valve surgery (Class
I) [9], or in patients with progressive FTR and tricuspid annulus end-diastolic
diameter
The benefits and risks of tricuspid valve surgery in patients with mild or moderate FTR need to be further investigated and considered.
Most studies consistently indicate that impaired pre-operative left ventricular global longitudinal strain (LV GLS) serves as a prognostic indicator for adverse outcomes in patients with PMR [18, 20, 21, 24, 30, 39, 80, 81, 82, 83, 84, 85, 86] as shown in Supplementary Table 7. The cut-off values for LV GLS predicting worse outcomes typically ranged from –17.9% to –20.5%. Additionally, the incremental value of LV GLS over traditional parameters has been underscored [20, 39, 80, 83, 84, 87]. However, there are some divergent findings in the literature. For instance, Pandis et al. [87] noted that an LV GLS better than –20.5% was associated with a greater reduction of LVEF, and an LV GLS better than –17.9% was associated with LVEF reduction of more than 10% and resultant LVEF below 50%. Song et al. [23] did not find any association between pre-operative LV GLS and LV dysfunction at 1 week and 3 months post-operation possibly due to unstable hemodynamics immediately following surgery and the inclusion of a heterogeneous patient population.
Twist, another parameter derived from speckle tracking echocardiography, has also been investigated. Candan et al. [18] examined 59 asymptomatic severe MR patients who underwent surgery and discovered that pre-operative twist was associated with post-operative LVEF (r = 0.42, p = 0.001) and independently predicted post-operative LV function (OR 0.8 [0.64–0.96], p = 0.02).
In summary, impaired pre-operative LV GLS could significantly predict negative outcomes but the cut-off values varied within a relatively narrow range because of differences in vendor-specific software.
LA strain indices are of increasing value to assess LA function [88]. Studies have shown that decreased pre-operative LA reservoir strain was one of the independent and incremental predictors of poorer outcomes after MV surgery [42, 84, 85, 89, 90] in terms of mortality, cardiac events, LV dysfunction, and functional capacity (Supplementary Table 8). An LA reservoir strain worse than cut-off value 21% may predict higher risk of post-operative cardiac events [90]. An LA reservoir strain worse than 22% could predict long-term post-operative all-cause mortality [85]. Besides, Cameli et al. [91] reports that LA strain impairment may appear earlier than LV strain because LA is the most susceptible chamber due to its’ thinner wall and MR-induced volume overload. In the future, studies about LA strain should take the thin walls of LA and the lack of normal values across various vendor-specific software into account [92].
Study concerning the predictive value of RV longitudinal strain in patients after MV surgery for PMR were scarce. Kislitsina et al. [84] reported that worse RV free wall longitudinal strain was associated with post-operative LV dysfunction (OR 1.171 [1.015–1.351]), and incremental prognostic value of strain (LV GLS, RV free wall longitudinal strain, LA reservoir strain) on top of demographics and other echocardiography parameters was demonstrated, but on multivariable Cox survival analysis, RV free wall longitudinal strain was not shown to be significantly associated with mortality (HR 1.078 [0.952–1.231], p = 0.243). More investigations about the predictive value of RV dysfunction in patients with PMR are needed.
Stress echocardiography has emerged as a valuable tool for identifying latent ventricular dysfunction [7, 9], which may present as deteriorated echocardiographic measurements or limited contractile reserve in pharmaceutical or exercise stress echocardiography [86, 93, 94, 95, 96]. Concerning PMR, stress echocardiography plays a crucial role in guiding clinical decisions for patients with discrepancies in regurgitation severity, symptoms, or LV function at rest [7, 9].
Studies investigating the prognostic utility of stress echocardiography have
highlighted several key findings, as outlined in Supplementary Table 9.
Exercise-induced parameters such as LVEF (with a cut-off value of 68%) [96],
LVESVi (cut-off value 25 cm3/m2) [96], and LV GLS normalized for LVESD
(cut-off value –5.7%/cm) [86, 95] have been identified as predictors of
post-operative LVEF. Additionally, exercise-induced PH (SPAP
In conclusion, exercise echocardiography offers valuable insights in PMR cases where resting two-dimensional echocardiography results are inconclusive or ambiguous. However, despite its clinical significance, the widespread adoption of exercise echocardiography in PMR patients is hindered by its time-consuming and labor-intensive nature. Further research and advancements are needed to streamline and optimize the clinical application of exercise echocardiography in the management of PMR.
Significant advancements in three-dimensional (3D) echocardiography have revolutionized the visualization of pathomorphological features of heart valves in real-time [100], as well as the precise quantification of chamber dimensions and regurgitation volumes [101], thereby enhancing its clinical utility in MV disease [102]. When compared with two-dimensional echocardiology, 3D echocardiology allows for more accurate pathomorphological characterization and function evaluation.
Studies have indicated that 3D echocardiography is valuable in predicting
post-operative outcomes in patients with PMR. Yingchoncharoen et al.
[103] found that 3D LVESVi independently predicted the post-operative development
of AF or LV dysfunction (OR 1.06 [1.04–1.16], p
While the scientific literature and clinical applications of 3D echocardiography are expanding, its primary use remains in transesophageal echocardiography. Transthoracic 3D echocardiography is limited by lower frame rates and spatial resolution. Future advancements in technology may address these limitations, potentially enhancing the role of 3D echocardiography in routine clinical practice.
This review offers a detailed overview of published evidences regarding the
prognostic relevance of pre-operative echocardiographic parameters in patients
undergoing MV surgery for PMR. Key prognostic indicators are a LVESD
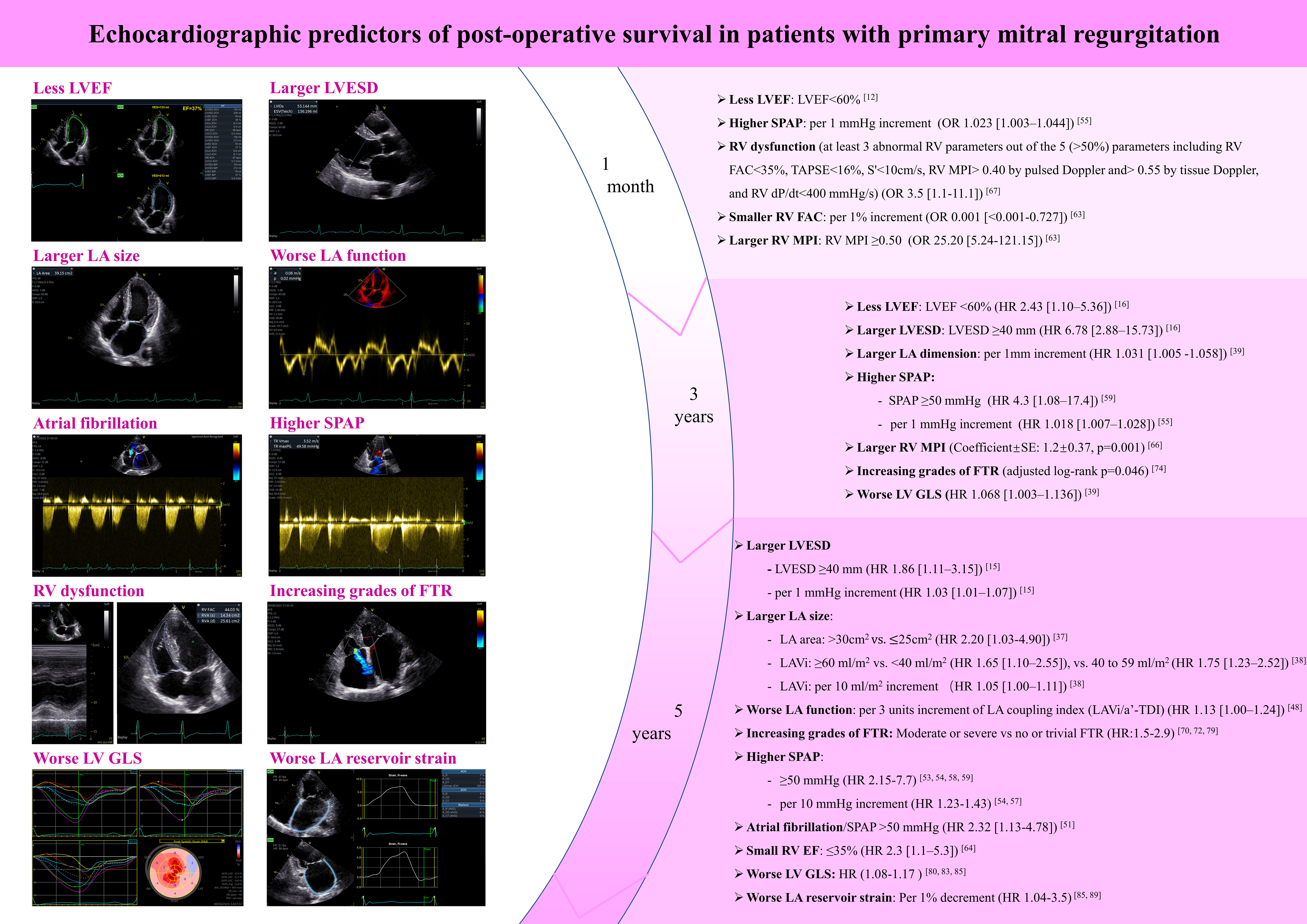 Fig. 2.
Fig. 2.
Echocardiographic predictors of post-operative survival in patients with primary mitral regurgitation. LVEF, left ventricular ejection fraction; LVESD, left ventricular end-systolic diameter; LA, left atrium; SPAP, systolic pulmonary arterial pressure; RV, right ventricle; FTR, functional tricuspid regurgitation; LV GLS, left ventricular global longitudinal strain; RV FAC, RV fractional area change; RV MPI, RV index of myocardial performance; LAVi, left atrial volume index; RV EF, RV ejection fraction; a′-TDI, late diastolic tissue Doppler imaging a′; OR, odds ratio; HR, hazard ratio; TAPSE, tricuspid annular plane systolic excursion; CH, chamber; VES,volume in end-systole; VED, volume in end-diastole; EF, ejection fraction; LVVES, left ventricular volume in end-systole; LVVED, left ventricular volume in end-diastole; LVSV, left ventricular stroke volume; LVEF, left ventricular ejection fraction; LVLs, left ventricular length at systole; LVLd, left ventricular length at diastole; HR, heart rate; LVCO, left ventricular cardiac output; BiP, biplane; LVIDs, left ventricular internal diameter at systole; ESV, end-systolic volume; f, frequency; P, power; AG, amplitude gain; Compr, compression; DDP, depth dependent gain; D, depth; FPS, frames per second; G, gain; PFR, pulse repetition frequency; SV, sample volume; Rej, reject; SVD, stress velocity diastolic; ACE, angle correction enabled; TR, tricuspid regurgitation, RV FAC, right ventricular fractional area change; RVA(s), right ventricular area at the end of systole; RVA(d), right ventricular area at the end of diastole; AVC, aortic valve closure; APLAX, apical long-axis view; ANT, anterior; SEPT, septal; INF, inferior; LAT, lateral; POST, posterior; GLPS, global longitudinal peak strain; LAX, long-axis; A4C, apical four-chamber view; A2C, apical two-chamber view; AVG, average; AVC_STORED, stored aortic valve closure; FR, frame rate; PSD, post-systolic duration; S_R, left atrial reservoir strain; S_CD, left atrial conduit strain; S_CT, left atrial contraction strain; LAV, left atrial volume; PreA, the time point before the mitral late filling-wave. “V” in the images in an image marking, the position of this marking corresponds to the marking on the transducer, helping physicians identify the orientation in the image.
Echocardiography plays a critical role in patients with PMR, the prognostic value of echocardiographic parameters was comprehensively summarized and elucidated in this review, including the traditional parameters and novel parameters. This review may help facilitate the integration of these parameters into the clinical decision-making process and further improve the outcomes of patients with PMR. In the future, further larger, multi-centered, prospective studies and randomized clinical trials are still required to clarify and strengthen their precise values.
YY, LYF, WQW, HL, LH, MWL, LZ, YLY, QL, YML, JW, and MXX contributed to the study’s conception and design. Literature search and the first draft of the manuscript were performed by YY and LYF. YY and LYF were responsible for the design of the figure/tables. JW and MXX commented on previous versions of the manuscript and critically revised the work. The final work was revised and approved by all authors. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
We would like to express our gratitude to all those who helped us during the writing of this manuscript. Thanks to all the peer reviewers for their opinions and suggestions.
This work was supported by grants from the National Natural Science Foundation of China [grant numbers 82230066, 82211530116].
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/j.rcm2511414.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.