


 , Xiaotian Chang 2,*,†
, Xiaotian Chang 2,*,†1 Department of Critical Medicine, The Affiliated Hospital of Qingdao University, 266000 Qingdao, Shandong, China
2 Medical Research Center of the Affiliated Hospital of Qingdao University, 266000 Qingdao, Shandong, China
†These authors contributed equally.
Abstract
Both acute myocardial infarction (AMI) and its salvage treatment, venoarterial-extracorporeal membrane oxygenation (VA-ECMO), may lead to the production of proinflammatory cytokines and further aggravate tissue damage. Xuebijing (XBJ) may modulate cytokine production involved in the inflammatory response. We aimed to determine the efficacy of XBJ in cardiogenic shock patients on VA-ECMO.
This was a prospective, randomized trial carried out in an intensive care unit of a tertiary teaching hospital. Patients with cardiogenic shock after acute myocardial infarction undergoing percutaneous coronary intervention (PCI) with VA-ECMO support were randomly divided into a Xuebijing group and a control group. Cytokines, inflammatory factors and left ventricular ejection fraction (LVEF) were compared between the groups.
41 patients were enrolled in the study, with 21 in the Xuebijing group and 20 in the control group. 28 (68.3%) were male, and the average age was 64.71 ± 8.18 years old. There was no difference in APACHEII (acute physiology and chronic health evaluation II) score, LVEF, or cytokine and inflammatory factors collected before extracorporeal membrane oxygenation (ECMO) between the two groups. The levels of interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α) in the Xuebijing group were lower than those in the control group in the first 24 hours, 48 hours and 72 hours after ECMO (p < 0.05). The LVEF in the Xuebijing group was higher than that of the control group at 48 hours (31.57 ± 3.43 vs. 28.35 ± 4.42, p = 0.013). This trend persisted at 72 hours. The duration of ECMO support in the Xuebijing group was 5.57 ± 2.11 days, which was shorter than that in the control group (p = 0.033).
Xuebijing injection can reduce the inflammatory response and improve cardiac function in patients with acute myocardial infarction treated with VA-ECMO to a certain extent.
Chinese Clinical Trial Registry (ChiCTR), ChiCTR2100054069, Registered 8, December 2021, https://www.chictr.org.cn/showproj.html?proj=142869.
Keywords
- Xuebijing injection
- venous-arterial extracorporeal membrane oxygenation
- cardiogenic shock
- acute myocardial infarction
- inflammation storm
- cytokine
Venoarterial-extracorporeal membrane oxygenation (VA-ECMO) is a life-saving therapy, which can provide circulatory and respiratory support for patients with severe cardiac and/or respiratory failure [1]. Acute myocardial infarction (AMI) is the most common cause of cardiogenic shock (CS), named acute myocardial infarction with cardiogenic shock (AMICS). It is a class of clinical syndromes in which the cardiac output is significantly reduced due to acute myocardial infarction, resulting in tissue hypoperfusion. It may manifest as recurrent or progressive ischemic symptoms that are difficult to control with drugs, accompanied by hemodynamic instability, life-threatening arrhythmias, cardiac arrest, and acute heart failure [2]. The use of VA-ECMO is becoming increasingly popular in the treatment of cardiogenic shock as a salvage therapy. However, with improvement of extracorporeal membrane oxygenation (ECMO) circuits, advances in catheterization technology and management of ECMO treatment, the survival rate of ECMO has not increased significantly. Less than half of the patients supported with VA-ECMO failed to survive to hospital discharge [1].
In patients with AMI, the expression of cytokines significantly increases both
in the infarct and border zone. This is followed by the activation of the
complement system, which mediates humoral and cellular responses, leading to
further expansion of the inflammatory response [3]. Cardiomyocyte necrosis
induces both a systemic response and a local reaction. The recruitment of
circulating inflammatory cells in the necrotic area removes dead cells and matrix
debris. Cytokines such as interleukin-1 (IL-1), tumor necrosis factor-alpha
(TNF-
Xuebijing (XBJ) injection, a drug derived from Chinese herbs, has been approved to treat severe infections including sepsis (China Food and Drug Administration; Beijing, China, Number Z20040033). It is widely used in China and has been used in critically ill patients for more than 10 years. XBJ is composed of five Chinese herbal extracts including Carthami flos, Paeoniae radix rubra, Chuanxiong rhizoma, Salviae miltiorrhizae, and Angelicae Sinensis radix. The dominant components of XBJ that have been monitored include hydroxysafflor yellow A, oxypaeoniflorin, senkyunolide I, and benzoylpaeoniflorin [9]. The incidence and influencing factors of side effects of Xuebijing differ among studies, mainly allergic reaction. Adverse reactions to Xuebijing injections were correlated with vehicle type, dosage, age, and drug combination [10].
It has been demonstrated that XBJ may regulate the production of cytokines,
especially pro-inflammatory factors such as TNF-
In clinical studies, there are many anti-inflammatory strategies for ECMO patients, including glucocorticoids, monoclonal antibodies, blood purification technology, but the efficacy remains uncertain [13, 14, 15]. A multi-target approach targeting multiple intracellular signaling pathways may be a more effective strategy for cardiac protection. Accordingly, this prospective, randomized study was conducted to determine the efficacy of XBJ in addition to standard care for cardiogenic shock patients on VA-ECMO.
This was a prospective, randomized trial carried out in a critical care department of a tertiary teaching hospital, which can independently perform about 100 ECMO cases per year, including more than 70 VA-ECMO cases. It is a single-center, prospective, randomized, double-blinded trial. The trial was approved by Qingdao University Affiliated Hospital (No. qyfykyll 912111920) and registered in the Chinese Clinical Trial Registry (ChiCTR2100054069). Written informed consent was obtained from legally authorized representatives of patients. Enrollment of patients started in December 2021 and ended in December 2022; follow-up finished in June 2023.
Patients who met the following criteria were eligible for inclusion: (1) 18–75 years old; (2) diagnosed as AMICS and treated with VA-ECMO.
Patients were excluded if: (1) they had a history of allergy to XBJ; (2) were in a confirmed or suspected immunosuppressive or immunodeficiency state; (3) with known or suspected infection; (4) failure to open a critical stenotic coronary artery vessel; (5) continuous renal replacement therapy (CRRT) was required; (6) acute or chronic hepatic insufficiency.
Randomization was performed by generating random numbers using a computer, where the XBJ group and the control group were allocated in a 1:1 ratio. The participants received the solvent only (normal saline, 200 mL, q12hr (every 12 hours)) in the placebo group and the solvent plus XBJ (normal saline 100 mL + XBJ 100 mL, q12hr) in the XBJ group. The treatment duration of the study lasted 7 days. All patients received peripheral VA-ECMO catheterization, with the right femoral vein and right femoral artery being preferred, followed by the left femoral vein and left femoral artery. A distal perfusion tube was routinely inserted. Other treatments, including sedative and analgesic management, vasoactive drug administration, ventilator management, and anticoagulant therapy, were performed by the same team according to the guidelines.
As there are no relevant studies on Xuebijing in acute myocardial infarction, we
conducted a prior experiment. 10 patients were randomly assigned to the Xuebijing
group or the control group, with 5 in each group, and IL-6 was measured 3 days
later. The IL-6 levels in the Xuebijing group and the control group were 50.28
Data on (1) Patient information: age, sex, body mass index (BMI), comorbidities, time from
admission to recanalization (hour), APACHEII (acute physiology and chronic health
evaluation II) score, SOFA (Sequential Organ Failure Assessment) score and
survival after VA-ECMO (SAVE) score. (2) cytokine and inflammatory factors
including IL-6, IL-8, IL-10, TNF-
Normal distribution of all data was checked by the Shapiro-Wilk normality test.
Normally distributed data are expressed as the mean and standard deviation.
Non-normally distributed data are presented as the median and interquartile range
(IQR) and were analyzed using the non-parametric Mann–Whitney U test.
Categorical variables are expressed as quantities and percentages and are
compared with the chi-square test or Fisher’s exact test. The results are
expressed as the p value and OR with the 95% CI. p
A total of 1012 patients were screened, 105 patients were diagnosed with AMICS, 64 patients selected VA-ECMO treatment, and were randomly divided into the XBJ group and the control group. 41 patients were finally enrolled in the study, 21 in the XBJ group and 20 in the control group. The flow chart of patient enrollment was shown in Fig. 1.
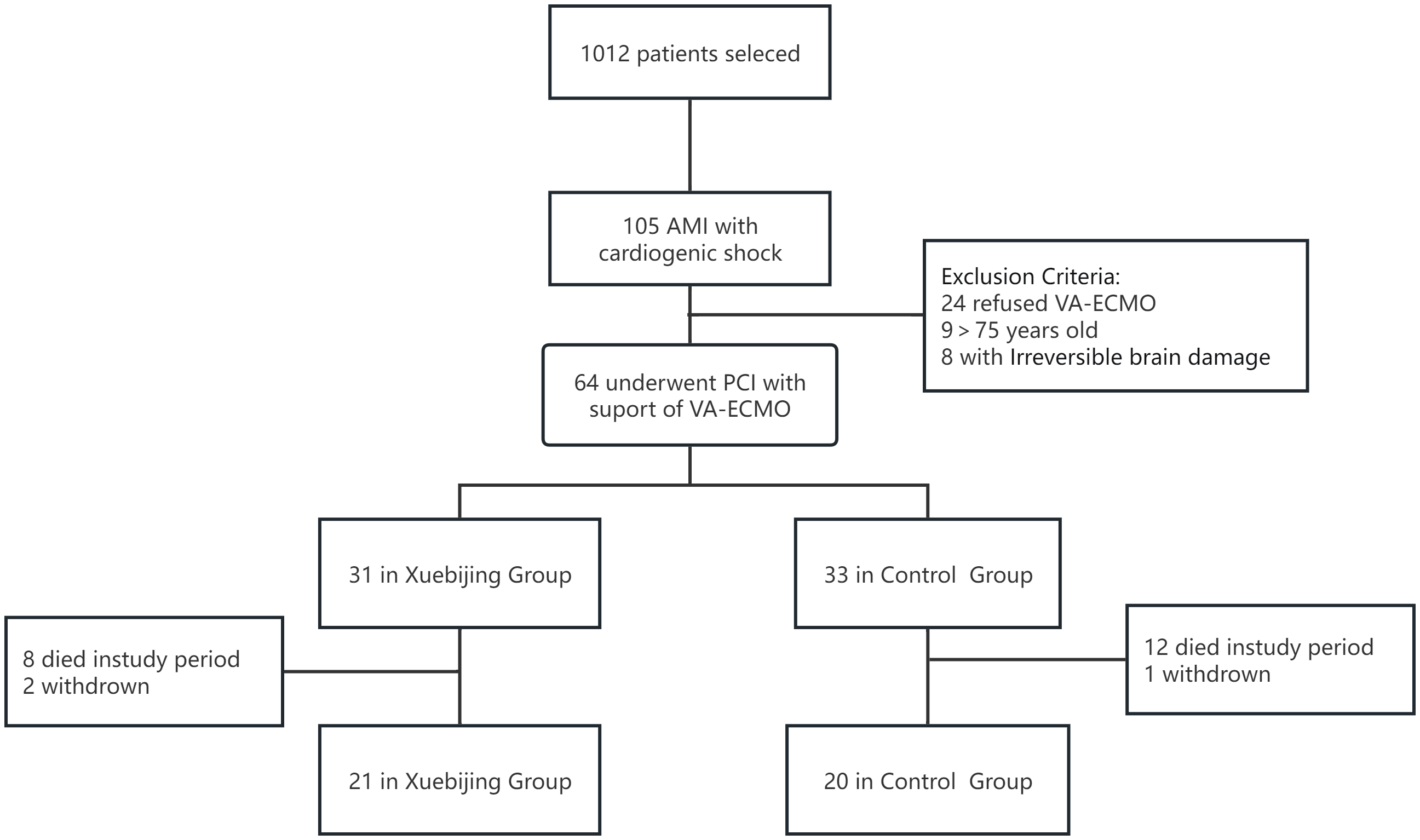 Fig. 1.
Fig. 1.
The flow chart of patient enrollment. AMI, acute myocardial infarction; VA-ECMO, venoarterial-extracorporeal membrane oxygenation; PCI, percutaneous coronary intervention.
Among the 41 patients, 28 (68.3%) were male, and the average age was 64.71
| XBJ group | Control group | p | ||
| N = 21 | N = 20 | |||
| Age (year) | 64.05 |
65.40 |
0.603 | |
| Sex (male) | 14 | 14 | 1.000 | |
| BMI (kg/m2) | 24.98 |
23.79 |
0.082 | |
| Co-morbidities | ||||
| Hypertension | 14 | 14 | 1.000 | |
| Diabetes mellitus | 3 | 6 | 0.277 | |
| Cerebral infarction | 2 | 4 | 0.410 | |
| Coronary atherosclerotic heart disease | 8 | 7 | 0.547 | |
| Peripheral vascular diseases | 3 | 3 | 0.654 | |
| Chronic pulmonary disease | 2 | 6 | 0.104 | |
| Time from onset to blood flow recanalization (hour) | 8.43 |
8.30 |
0.878 | |
| APACHEII score | 21.43 |
22.20 |
0.551 | |
| SOFA score | 4.52 |
4.35 |
0.751 | |
| SAVE score | –1.10 |
–1.15 |
0.941 | |
| Left ventricular ejection fraction (%) | 25.86 |
26.10 |
0.901 | |
| Culprit vessels | ||||
| Right coronary artery | 3 | 3 | 0.845 | |
| Left main coronary artery | 4 | 3 | ||
| Left anterior descending branch | 9 | 11 | ||
| Left circumflex artery | 5 | 3 | ||
APACHEII score, Acute Physiology and Chronic Health Status score II; SOFA score, Sequential Organ Failure Assessment score; XBJ, Xuebijing; BMI, body mass index; SAVE score, Survival After Veno-arterial Extracorporeal Membrane Oxygenation score. An online calculator is available at https://www.evidencio.com/models/show/1001.
Data on cytokines and inflammatory factors were collected before ECMO and did
not differ between the two groups (Table 2). In the first 24 hours, the levels of
cytokines were higher than those before ECMO, but the levels of IL-6 and
TNF-
| XBJ group | Control group | p | |
| N = 21 | N = 20 | ||
| Troponin I (ng/mL) | 0.91 |
0.99 |
0.560 |
| Interleukin-6 (pg/mL) | 110.14 |
109.70 |
0.931 |
| Interleukin-10 (pg/mL) | 8.84 |
8.56 |
0.680 |
| Tumor necrosis factor |
1.21 |
1.20 |
0.818 |
| Interleukin-8 (pg/mL) | 10.23 |
10.84 |
0.437 |
| Hemoglobin (g/L) | 144.48 |
140.5 |
0.322 |
| Platelet ( |
216.05 |
211.45 |
0.730 |
| C reactive protein (mg/L) | 1.17 |
1.34 |
0.380 |
| D-Dimer (ng/mL) | 286.62 |
274.20 |
0.365 |
ECMO, extracorporeal membrane oxygenation; XBJ, Xuebijing.
| XBJ group | Control group | p | ||
| N = 21 | N = 20 | |||
| 24 hours after ECMO | ||||
| Interleukin-6 (pg/mL) | 171.43 |
213.20 |
0.001 | |
| Tumor necrosis factor |
1.81 |
2.20 |
0.014 | |
| Interleukin-8 (pg/mL) | 4.78 |
5.55 |
0.071 | |
| Interleukin-10 (pg/mL) | 2.03 |
2.06 |
0.735 | |
| Hemoglobin (g/L) | 125.43 |
113.25 |
0.002 | |
| Platelet ( |
174.10 |
152.15 |
0.043 | |
| D-Dimer (ng/mL) | 1055.95 |
1348.95 |
0.000 | |
| C reactive protein (mg/L) | 78.90 |
89.15 |
0.113 | |
| 48 hours after ECMO | ||||
| Interleukin-6 (pg/mL) | 75.19 |
130.10 |
0.000 | |
| Tumor necrosis factor |
1.13 |
1.64 |
0.000 | |
| Interleukin-8 (pg/mL) | 2.52 |
3.11 |
0.105 | |
| Interleukin-10 (pg/mL) | 1.01 |
1.07 |
0.343 | |
| Hemoglobin (g/L) | 113.90 |
100.00 |
0.000 | |
| Platelet ( |
135.19 |
118.10 |
0.008 | |
| D-Dimer (ng/mL) | 1388.10 |
1968.0 |
0.000 | |
| C reactive protein (mg/L) | 94.71 |
107.70 |
0.008 | |
| 72 hours after ECMO | ||||
| Interleukin-6 (pg/mL) | 57.47 |
103.70 |
0.000 | |
| Tumor necrosis factor |
1.20 |
1.73 |
0.000 | |
| Interleukin-8 (pg/mL) | 2.46 |
3.38 |
0.000 | |
| Interleukin-10 (pg/mL) | 1.31 |
1.27 |
0.518 | |
| Hemoglobin (g/L) | 98.95 |
84.75 |
0.001 | |
| Platelet ( |
120.00 |
95.80 |
0.000 | |
| D-Dimer (ng/mL) | 1547.62 |
2349.35 |
0.000 | |
| C reactive protein (mg/L) | 114.19 |
131.45 |
0.019 | |
| Average ECMO flow on day 1 (L/min) | 2.85 |
2.88 |
0.768 | |
| Average ECMO flow on day 2 (L/min) | 2.88 |
2.80 |
0.362 | |
| Average ECMO flow on day 3 (L/min) | 2.14 |
2.38 |
0.044 | |
ECMO, extracorporeal membrane oxygenation; XBJ, Xuebijing.
After 48 hours, IL-6 and TNF-
In terms of cardiac function, the difference between the two groups began to
appear at 48 hours. The ejection fraction in the XBJ group was higher than that
of the control group at 48 hours (31.57
| XBJ group | Control group | p | ||
| N = 21 | N = 20 | |||
| Left ventricular ejection fraction (%) | ||||
| Before ECMO | 25.86 |
26.10 |
0.901 | |
| At 24 hours | 28.71 |
27.25 |
0.364 | |
| At 48 hours | 31.57 |
28.35 |
0.013 | |
| At 72 hours | 33.62 |
30.70 |
0.016 | |
| 28 days after ECMO | 42.29 |
40.15 |
0.175 | |
| Duration of ECMO (days) | 5.57 |
7.25 |
0.033 | |
| Length of stay (days) | 12.62 |
16.20 |
0.096 | |
| Bleeding (n) | 0 | 0 | ||
| Thrombosis (n) | 2 | 4 | 0.663 | |
| SOFA score at day 28 | 0 (0, 1) | 1 (0, 2) | 0.205 | |
ECMO, extracorporeal membrane oxygenation; SOFA score, Sequential Organ Failure Assessment score; XBJ, Xuebijing.
The duration of ECMO in the XBJ group was 5.57
The prospective randomized study showed that XBJ could reduce the inflammatory response and improve cardiac function in patients with cardiogenic shock caused by AMI treated with ECMO, but there was no significant difference in cardiac function at 28-day follow-up. To our knowledge, this is the first study of XBJ in patients treated for cardiogenic shock.
AMI remains one of the common causes of hospitalization and death worldwide [16]. Re-perfusion strategies such as thrombolysis and PCI have limited myocardial damage, reduced infarct size, and improved overall prognosis. However, patients with AMI are still confronted with a higher risk of short- and long-term heart failure and even death [17]. The onset of acute myocardial ischemia results in local necrosis, inducing an initial pro-inflammatory response. Circulatory inflammatory cells recruit and remove dead cells and tissues from the MI zone. Myocardial re-perfusion exacerbates proinflammatory response, which is characterized by infiltration of neutrophils resulting in development of necrotic and apoptotic cell death from 6 to 24 hours post-re-perfusion and apoptotic cell death between 48 to 72 hours post-re-perfusion which is associated with large macrophage infiltration and contributes to cardiomyocyte death and oxidative stress [18, 19].
Endothelial dysfunction is more likely to occur in inflammatory states,
resulting in increased permeability, subcutaneous accumulation of lipoproteins,
leukocyte recruitment, and platelet activation. Macrophages derived from
recruited monocytes secrete pro-inflammatory factors, including IL-1
VA-ECMO is an established treatment for cardiogenic shock, providing both time
and perfusion to save heart function. But its complications, whether mechanical,
pump-related, or secondary, are common and often lead to morbidity and mortality.
After the initiation of ECMO, a rapid rise in pro-inflammatory cytokines, which
in severe cases can lead to end-organ dysfunction and death, is thought to be
related to the innate immune response [15]. Frerou et al. [21] have
shown in their prospective study that pro-inflammatory cytokines such as IL-6,
IL-8 and TNF-
Xuebijing, a drug used for the treatment of severe community-acquired pneumonia
and sepsis, also plays an important role in the treatment of coronavirus disease 2019 (COVID-19) [23]. The
multiple active components, multiple targets, and multiple pathways of XBJ
injection also provide a new perspective for the study of cardiac shock with ECMO
treatment. XBJ has anti-inflammatory and anticoagulation effects, regulates
immune responses, protects the vascular endothelium and prevents oxidative
stress, which may inhibit the chronic inflammatory response caused by
atherosclerosis [24]. Recent studies have shown that XBJ injection can attenuate
the excessive production of various inflammatory mediators such as IL-6,
TNF-
Although the levels of cytokines decreased in the XBJ group, there was no effect on cardiac function at 28-day follow-up. This may result from ventricular remodeling due to a persistent chronic inflammatory state, basic heart function and the patients’ condition.
This study has several limitations that have to be acknowledged. Although this was a prospective randomized controlled study, blinding was difficult due to the characteristics of XBJ. The strict inclusion and exclusion criteria meant that only few patients could be included. Secondly, as there are no relevant studies on Xuebijing in AMI, the sample size was calculated from our prior experiment. Only 41 patients have been included over a year period. The small size of both groups undoubtedly limits the value of our results. Lastly, the outcome of patients is greatly affected by the experience of ECMO center, which may vary among centers. Therefore, larger multicenter trials are needed to confirm the reliability and effectiveness of XBJ.
Although no long-term improvement in cardiac function was shown, Xuebijing injections can reduce the inflammatory response, thereby improving short-term cardiac function and promoting ECMO weaning in patients with acute myocardial infarction to a limited extent. However, larger scale multi-center trials are needed to confirm the reliability and effectiveness of Xuebijing.
The data are available from the corresponding author on reasonable request.
ZY: Formal analysis and Writing—original draft; YL: Design and Formal analysis, drafting the manuscript. FW: Investigation and revising; XH: Acquisition of data, Methodology and Writing—review & editing; ZD: Design, interpretation and Writing—review & editing; JX: Conception ,Supervision and Writing—review & editing; XC: Supervision, Design and Writing—review & editing. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The trial was approved by Qingdao University Affiliated Hospital (No. qyfykyll 912111920). All participants provided written informed consent before enrollment.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.