


1 Department of Cardiology, Xiangtan Central Hospital, 411100 Xiangtan, Hunan, China
Abstract
Diabetes mellitus (DM) and left ventricular (LV) systolic dysfunction are common in patients who receive percutaneous coronary intervention (PCI) for chronic total occlusion (CTO). This study aimed to investigate the clinical outcomes of LV systolic dysfunction patients who had successful PCI for CTO over two years, with or without DM.
This cohort included 185 patients with LV systolic dysfunction undergoing successful PCI for CTO. A comparative analysis was performed on individual data and clinical outcomes among patients with and without DM after a two-year follow-up.
DM was identified in 99 (53.5%) patients who exhibited a higher incidence of chronic kidney disease (CKD), elevated serum creatinine levels, increased hemoglobin A1c, and reduced estimated glomerular filtration rates (p < 0.05). Patients with diabetes also experienced increased multi-vessel disease, a higher number of lesions per patient, as well as elevated multicenter chronic total occlusion registry in Japan (J-CTO) and Synergy between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery (SYNTAX) scores (p < 0.05). During the two-year follow-up, the DM group showed a greater occurrence of major adverse cardiovascular events (MACEs) compared with the non-DM group (24.2% versus 12.8%, p < 0.001). The DM group also had higher rates of all-cause mortality (9.1% versus 3.5%, p < 0.002), cardiac death (8.1% versus 1.2%, p < 0.001), and target vessel revascularization (18.2% versus 7.1%, p < 0.001). Multivariable logistic regression analysis demonstrated that the presence of DM is not an independent predictor of MACEs (hazard ratio (HR): 0.58; 95% confidence interval (CI): 0.32 to 1.03; p = 0.260). Moreover, the multi-vessel disease (HR: 1.69; 95% CI: 1.21 to 2.36; p = 0.002), CKD (HR: 1.38; 95% CI: 1.08 to 1.78; p = 0.011) and complete revascularization (HR: 0.36; 95% CI: 0.14 to 0.88; p = 0.026) had a significant association with MACEs.
In patients with LV systolic dysfunction who underwent successful CTO-PCI, those with diabetes exhibited a higher trend toward the incidence of MACEs over two years.
Keywords
- chronic total occlusion
- percutaneous coronary intervention
- diabetes mellitus
- major adverse cardiac events
- left ventricular systolic dysfunction
Approximately 30%–50% of individuals receiving coronary angiography with the diagnosis of coronary artery disease (CAD) exhibit chronic total occlusion (CTO) [1]. Previous retrospective research has shown that effective percutaneous coronary intervention (PCI) for CTO can improve ventricular function and decrease the symptoms of angina and dyspnea compared to failed attempts at revascularization [2, 3]. Studies have shown that diabetes mellitus (DM) is common in patients with CAD [4] and a risk factor for the occurrence of CTO [5, 6]. Research also revealed that 27% to 45% of patients undergoing CTO revascularization have DM [5, 7, 8]. Currently, there is controversy regarding the effect of DM on clinical results after successful revascularization with PCI. The research findings are still controversial: some studies have reported that the incidence of major adverse cardiac events (MACEs) is higher in diabetic patients [8, 9, 10], whereas others have observed no significant differences in MACE rates between diabetic and non-diabetic patients [11, 12, 13]. Left ventricular ejection fraction (LVEF) is an important predictor of cardiovascular events in CAD patients [14]. Evidence suggests that in patients with reduced LVEF, the presence of CTO correlates with poorer clinical outcomes [14]. However, CTO-PCI can potentially relieve angina symptoms in these patients and also improve LVEF in carefully selected cases [15].
Many physicians in clinical practice hesitate to undertake PCI for CTO lesions in patients suffering from left ventricular (LV) systolic dysfunction and DM because of concerns about safety during the procedure and unknown long-term benefits. Insufficient data exists concerning the long-term clinical impacts of successful PCI for CTO on LV systolic dysfunction in patients with DM. This study sought to assess the clinical results for successful PCI for CTO in individuals with LV systolic dysfunction over two years.
This single-center, observational, retrospective study was conducted in Xiangtan
Central Hospital, which included patients who underwent PCI for CTO between
January 1, 2016, and July 31, 2021. The inclusion criteria of the study were that
the patient had to have at least one CTO in a main coronary artery, stable vital
signs, a LVEF of 40% or less, and a successful revascularization via PCI. All
patients who received the treatment for CTO revascularization had symptoms
suggestive of stable angina and/or noninvasive imaging for functional ischemia
preference. The criteria for exclusion included (1) severe coagulation
abnormalities, malignant tumors, unstable hemodynamics, cardiogenic shock with a
projected life span of less than one year, or other terminal conditions; (2)
acute myocardial infarctions included ST-segment elevation
myocardial infarction (STEMI) and non-STEMI; (3) a previous history of coronary
artery bypass grafting (CABG); (4) unsuccessful CTO-PCI; (5) an LVEF
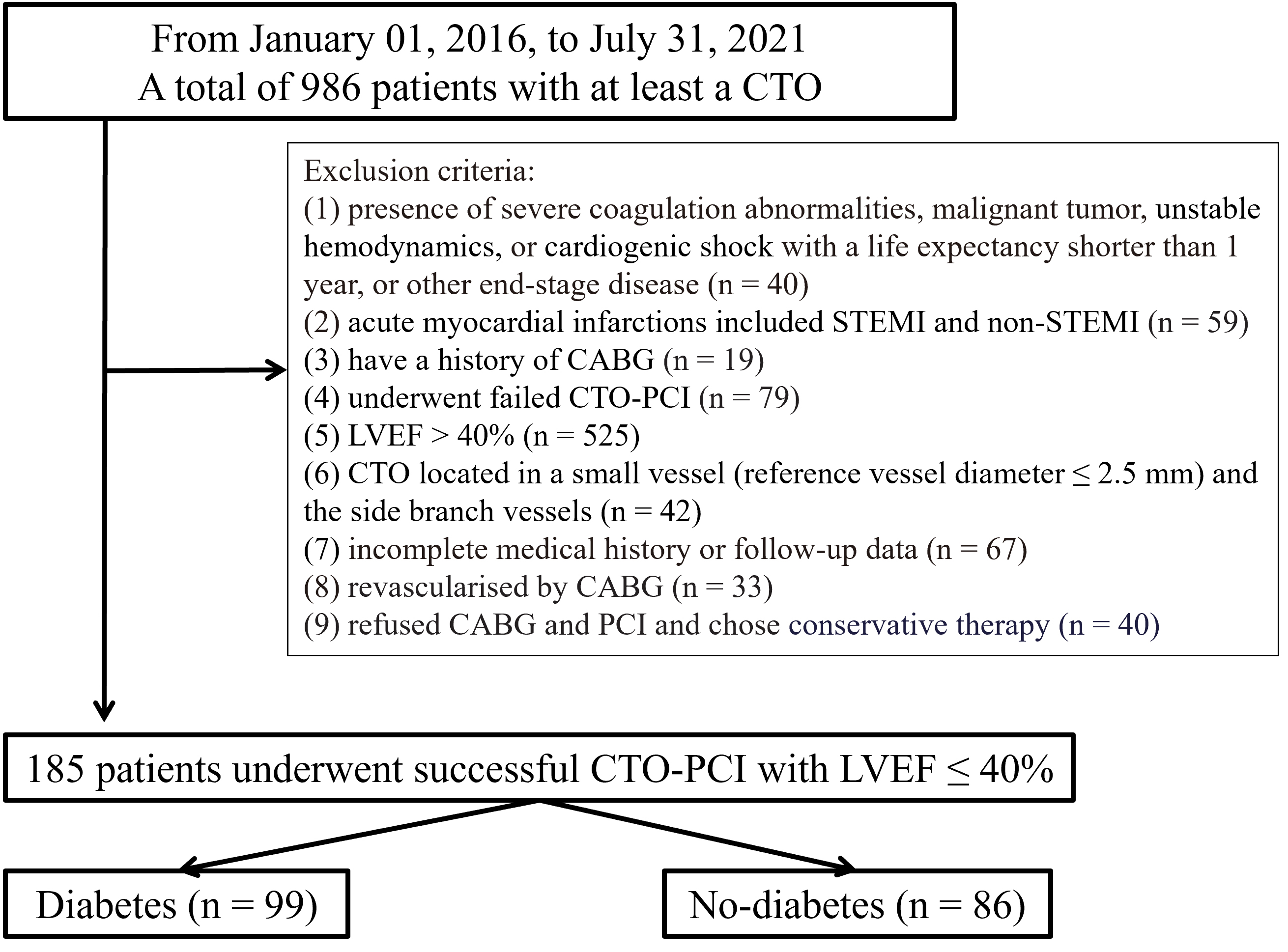
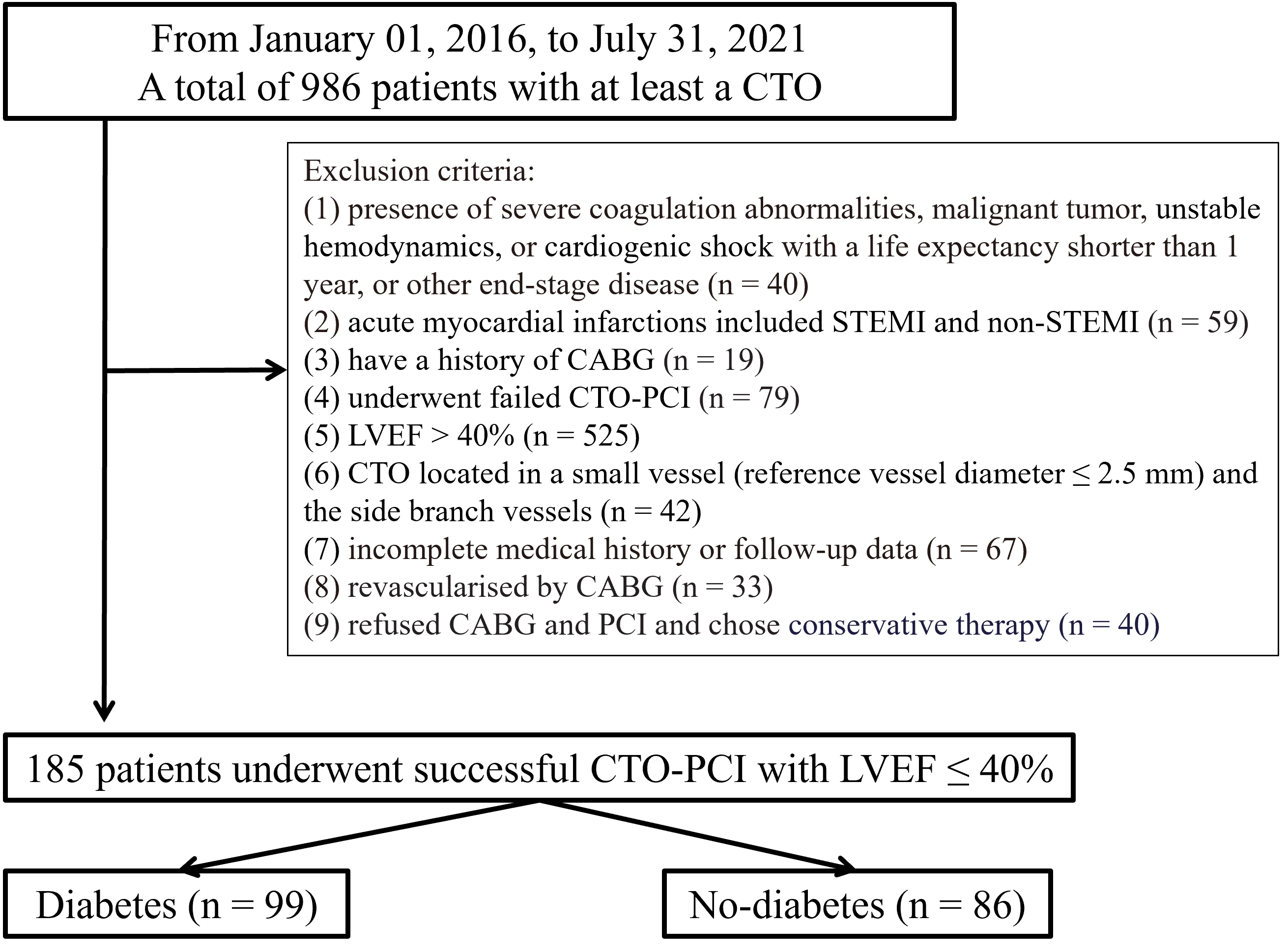 Fig. 1.
Fig. 1.
Study flowchart. CABG, coronary artery bypass grafting; CTO, chronic total occlusion; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction; LVEF, left ventricular ejection fraction.
A diagnosis of CTO was made when angiographic evidence revealed a thrombolysis
in myocardial infarction (TIMI) flow grade of 0 in an occluded artery segment
that was present for more than three months [16]. We classified non-CTO lesions
as having a stenosis diameter of 50% for the left main (LM) artery and 70% for
non-LM CAD within vessels with a diameter of at least 2.5 mm [17]. DM was
identified by the administration of oral hypoglycemic agents or insulin, a
fasting plasma glucose level of
We selectively performed PCI on symptomatic patients suffering from non-CTO lesions. For the CTO-PCI procedure, standard methods and guidelines were used, including bilateral injections, the hybrid algorithm, tapered-tip guidewires, stiff wires, parallel wires, microcatheters, and the retrograde method upon availability [25]. After a previous balloon angioplasty procedure, drug-eluting stents were inserted, and anticoagulant medication was administered during the PCI. Dual antiplatelet therapy for a minimum of one year and cardiovascular drugs, such as beta-blockers, calcium channel blockers, inhibitors of the renin–angiotensin–aldosterone inhibitors system, and statins, was also administered during the follow-up period.
MACEs were defined as cardiac death, myocardial infarction, target vessel revascularization, and all-cause mortality [26]. Meanwhile, in-hospital MACEs, including the above clinical adverse events, were assessed before hospital discharge. The primary endpoint was a MACE, with cardiac mortality as the secondary endpoint. Patients were evaluated at one-, six-, and twelve months post-PCI and annually after that for a maximum of 24 months through hospital record reviews, telephone interviews, and outpatient visits conducted by research coordinators.
The categorical variables were analyzed using either the Chi-square or Fisher’s
exact tests, with results presented as frequencies and percentages. Continuous
variables were expressed as the mean
A total of 185 patients underwent successful PCI for CTO, of which 99 (53.5%)
had DM. The clinical features of patients are listed in Table 1. Chronic kidney
disease was significantly increased in patients with DM compared to those without
DM (29.3 vs. 18.6%, p
| Characteristic | DM (n = 99) | Non-DM (n = 86) | p-value | |
| Males, n (%) | 82 (82.8) | 69 (80.2) | 0.551 | |
| Age, y | 62.3 |
63.2 |
0.546 | |
| BMI, kg/m2 | 27.1 |
26.6 |
0.204 | |
| Smoker or previous smoker, n (%) | 50 (50.5) | 43 (50.0) | 0.945 | |
| Hypertension, n (%) | 77 (77.8) | 60 (70.0) | 0.189 | |
| Cerebrovascular disease, n (%) | 26 (26.3) | 19 (22.1) | 0.583 | |
| Peripheral artery disease, n (%) | 18 (18.2) | 19 (22.1) | 0.441 | |
| Previous MI, n (%) | 26 (26.3) | 24 (27.9) | 0.609 | |
| Previous PCI, n (%) | 18 (18.2) | 20 (23.3) | 0.340 | |
| Chronic pulmonary disease, n (%) | 4 (4.0) | 5 (5.8) | 0.737 | |
| Family history of CHD, n (%) | 6 (6.1) | 7 (8.1) | 0.617 | |
| Chronic kidney disease, n (%) | 29 (29.3) | 16 (18.6) | ||
| CCS score, n (%) | 0.384 | |||
| I | 6 (6.1) | 7 (8.1) | ||
| II | 18 (18.2) | 11 (12.8) | ||
| III | 26 (26.3) | 26 (30.2) | ||
| IV | 18 (18.2) | 21 (24.4) | ||
| NYHA functional class, n (%) | 0.271 | |||
| I | 27 (27.3) | 22 (25.6) | ||
| II | 45 (45.5) | 41 (47.7) | ||
| III | 21 (21.2) | 19 (22.0) | ||
| IV | 6 (6.1) | 4 (4.7) | ||
| LVEF at baseline | 36.2 |
37.1 |
0.772 | |
| LVEF after PCI | 44.2 |
46.2 |
0.361 | |
| ICD | 15 (15.2) | 16 (18.6) | 0.411 | |
| Homocysteine, µmol/L | 18.0 |
14.0 |
0.315 | |
| Lactate, mmol/L | 2.3 |
2.6 |
0.220 | |
| Serum creatinine, µmol/L | 147.2 |
93.8 |
||
| eGFR, mL/min/1.73 m2 | 66.9 |
83.2 |
||
| Hemoglobin A1c | 7.9 |
5.8 |
||
| Total cholesterol, mmol/L | 4.1 |
4.0 |
0.557 | |
| Triglycerides, mmol/L | 2.2 |
2.1 |
0.312 | |
| HDL-c, mmol/L | 0.9 |
0.9 |
0.400 | |
| LDL-c, mmol/L | 2.5 |
2.5 |
0.997 | |
| Drug treatment | ||||
| Aspirin, n (%) | 99 (100) | 86 (100) | 1.000 | |
| Clopidogre, n (%) | 98 (99.0) | 84 (97.7) | 0.962 | |
| Ticagrelor, n (%) | 1 (1.0) | 2 (2.3) | 0.901 | |
| ACEI, n (%) | 24 (24.2) | 47 (54.7) | ||
| ARB, n (%) | 18 (18.2) | 25 (29.1) | 0.010 | |
| Beta-blocker, n (%) | 82 (82.8) | 70 (81.4) | 0.566 | |
| Calcium channel blocker, n (%) | 25 (25.3) | 27 (31.4) | 0.408 | |
| Diuretic, n (%) | 51 (51.5) | 46 (53.5) | 0.753 | |
| Nitrate, n (%) | 34 (34.3) | 25 (29.1) | 0.383 | |
| Statin, n (%) | 94 (94.9) | 84 (97.7) | 0.580 | |
BMI, body mass index; MI, myocardial infarction; CHD, coronary atherosclerotic heart disease; CCS, Canadian Cardiovascular Society; NYHA, New York Heart Association; PCI, percutaneous coronary intervention; LVEF, left ventricular ejection fraction; ICD, implantable cardioverter defibrillator; eGFR, estimated glomerular filtration rate; HDL-c, high-density lipoprotein cholesterol; LDL-c, low-density lipoprotein cholesterol; ACEI, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blocker; DM, diabetes mellitus.
Table 2 displays the angiographic details and procedure features. Patients with
DM exhibited a significantly higher prevalence of multi-vessel disease compared
to those with no DM (85.9% vs. 73.3%, p = 0.017). Patients with DM
exhibited a greater number of lesions per patient (2.61
| Characteristic | DM (n = 99) | Non-DM (n = 86) | p-value | |
| Vascular lesion, n (%) | ||||
| LM | 14 (14.1) | 10 (11.6) | 0.571 | |
| LAD | 81 (81.8) | 65 (75.6) | 0.189 | |
| LCX | 57 (57.6) | 52 (60.5) | 0.206 | |
| RCA | 76 (76.8) | 65 (75.6) | 0.645 | |
| Non-CTO target vessel, n (%) | ||||
| LM | 10 (10.1) | 8 (8.1) | 0.303 | |
| LAD | 61 (61.6) | 59 (68.6) | 0.792 | |
| LCX | 29 (29.3) | 23 (26.7) | 0.622 | |
| RCA | 55 (55.6) | 49 (57.0) | 0.814 | |
| Multi-vessel disease, n (%) | 85 (85.9) | 63 (73.3) | 0.017 | |
| Number of lesions per patient | 2.61 |
2.20 |
0.001 | |
| Vessels with CTO | ||||
| LAD | 32 (32.3) | 35 (35.4) | 0.848 | |
| LCX | 36 (36.4) | 28 (32.6) | 0.510 | |
| RCA | 53 (53.5) | 38 (44.2) | 0.055 | |
| Multi-CTO lesion, n (%) | 29 (29.3) | 24 (27.9) | 0.631 | |
| Number of CTO per patient | 1.40 |
1.34 |
0.087 | |
| Location of CTO | ||||
| Proximal | 55 (55.6) | 48 (55.8) | 0.806 | |
| Mid | 43 (43.4) | 33 (38.4) | 0.690 | |
| Distal | 23 (23.2) | 20 (23.2) | 0.995 | |
| Ostial location, n (%) | 10 (10.1) | 8 (9.3) | 0.727 | |
| In-stent occlusion, n (%) | 7 (7.1) | 10 (11.6) | 0.069 | |
| Lesion length, mm | 28.39 |
27.85 |
0.672 | |
| Lesion length |
68 (68.7) | 55 (64.0) | 0.130 | |
| Blunt stump, n (%) | 66 (66.7) | 60 (70.0) | 0.169 | |
| Tortuosity |
28 (28.3) | 24 (27.9) | 0.801 | |
| Calcification, n (%) | 32 (32.3) | 25 (29.1) | 0.693 | |
| Reattempt, n (%) | 9 (9.1) | 8 (9.3) | 0.723 | |
| J-CTO score | 2.48 |
2.01 |
0.015 | |
| SYNTAX score | 23.64 |
21.17 |
0.041 | |
| Complete revascularization | 79 (79.8) | 74 (86.0) | 0.077 | |
| Success of PCI for CTO | 84 (84.8) | 78 (90.7) | 0.151 | |
| Contrast amount, mL | 250 |
240 |
0.473 | |
| Procedural time, min | 119.14 |
117.21 |
0.667 | |
DM, diabetes mellitus; LAD, left anterior descending artery; LCX, left circumflex artery; LM, left main artery; CTO chronic total occlusion; J-CTO, multicenter CTO registry in Japan; RCA, right coronary artery; PCI, percutaneous coronary intervention; SYNTAX, Synergy between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery.
Table 3 shows the clinical outcomes between patients with and without DM
in-hospital and two years. No significant differences in in-hospital MACEs were
detected between the DM and non-DM groups. During the two-year follow-up, 35
(18.9%) patients experienced MACEs, and death occurred in 12 patients (6.5%).
The DM group had higher incidences of MACEs (24.2 vs. 12.8%, p
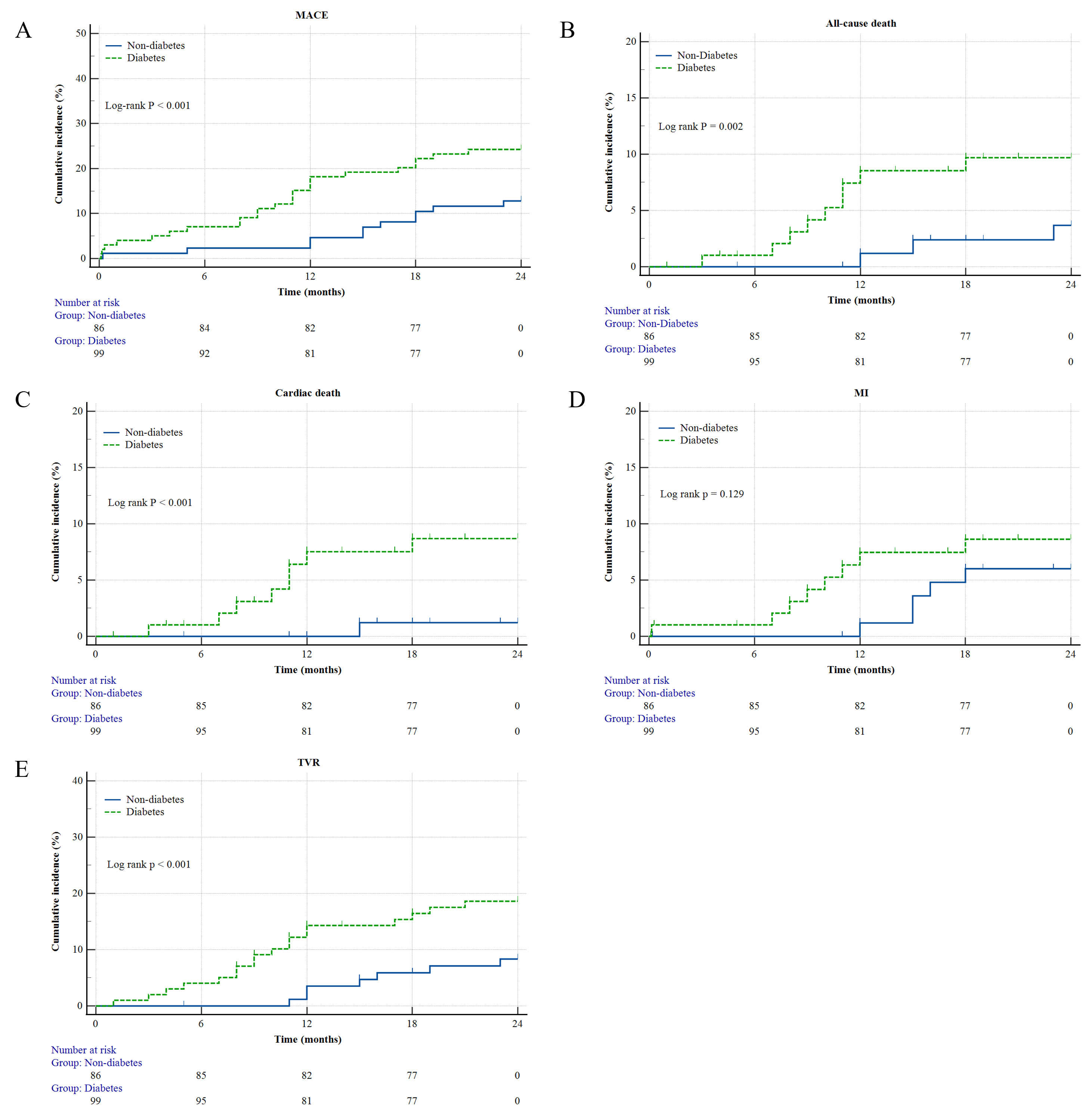
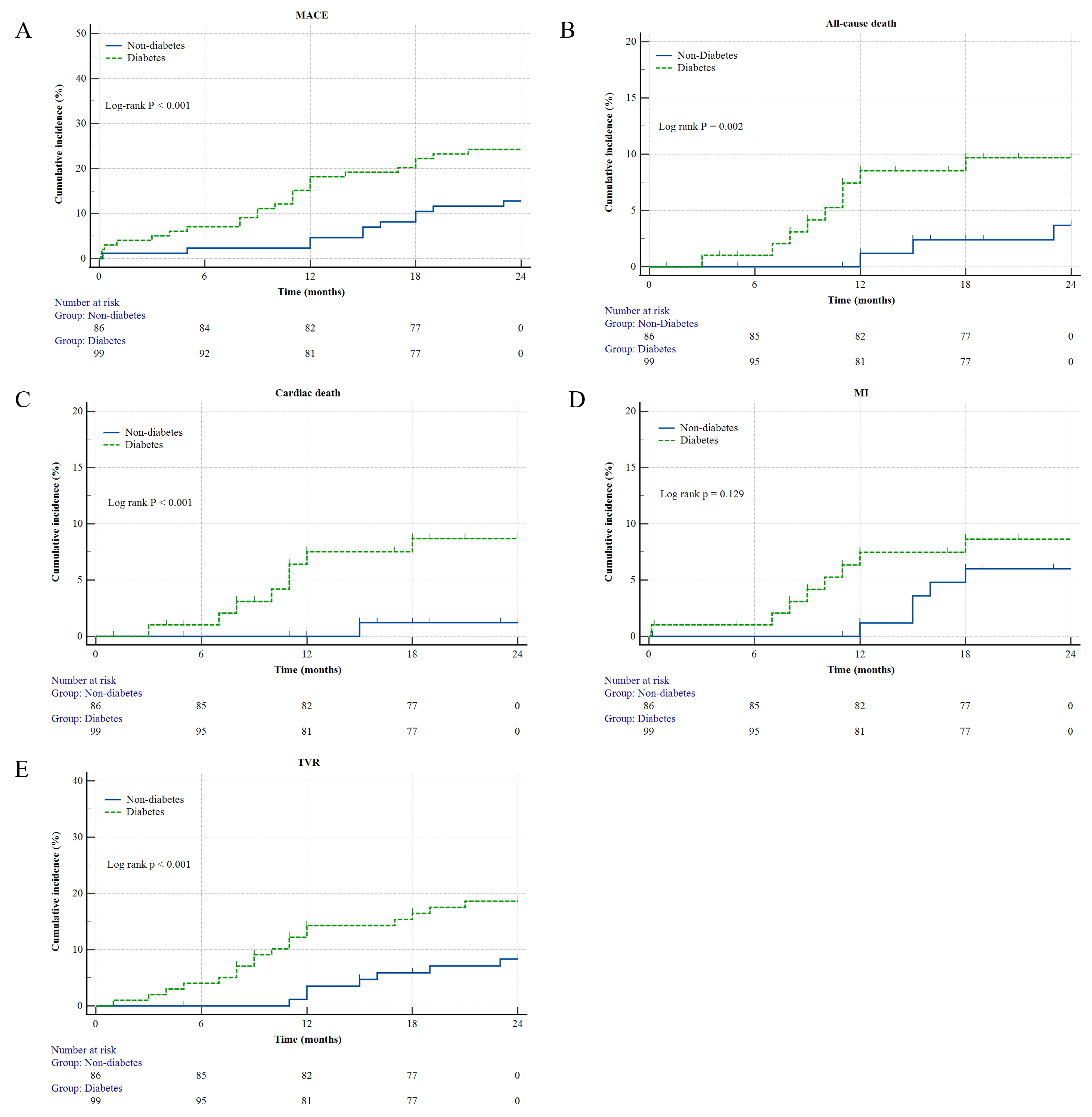 Fig. 2.
Fig. 2.
Kaplan–Meier survival curves for 2 years. (A) MACEs. (B) All-cause death. (C) Cardiac death. (D) MI. (E) TVR. MACEs, major adverse cardiac events; MI, myocardial infarction; TVR, target vessel revascularization.
| Characteristic | DM (n = 99) | Non-DM (n = 86) | p-value |
| In-hospital MACEs | 1 (1.0) | 3 (3.5) | 0.300 |
| All-cause death | 0 | 0 | - |
| Cardiac death | 0 | 0 | - |
| Myocardial infarction | 3 (3.5) | 1 (1.0) | 0.300 |
| Target vessel revascularization | 0 | 0 | - |
| 2-year total MACEs | 24 (24.2) | 11 (12.8) | |
| All-cause death | 9 (9.1) | 3 (3.5) | 0.002 |
| Cardiac death | 8 (8.1) | 1 (1.2) | |
| Myocardial infarction | 8 (8.1) | 5 (5.8) | 0.129 |
| Target vessel revascularization | 18 (18.2) | 7 (7.1) |
DM, diabetes mellitus; MACEs, major adverse cardiac and cerebrovascular events.
The univariate and multivariate regression analyses in Table 4 indicated that the presence of DM is not an independent predictor of MACEs (HR: 0.58; 95% CI: 0.32 to 1.03; p = 0.260); meanwhile, multi-vessel disease (HR: 1.69; 95% CI: 1.21 to 2.36; p = 0.002) and CKD (HR: 1.38; 95% CI: 1.08 to 1.78; p = 0.011) were independent predictors of MACEs and complete revascularization was associated with a reduced incidence of MACEs (HR: 0.36; 95% CI: 0.14 to 0.88; p = 0.026).
| HR (95% CI) | p-value | ||
| Univariate | |||
| Age (per year increment) | 0.98 (0.95–1.01) | 0.296 | |
| Male | 0.99 (0.93–1.06) | 0.863 | |
| Hypercholesterolemia | 0.69 (0.31–1.34) | 0.261 | |
| Hypertension | 0.98 (0.56–1.77) | 0.968 | |
| The presence of DM | 1.88 (1.09–3.28) | 0.024 | |
| Smoking | 1.40 (0.81–2.41) | 0.237 | |
| CKD | 3.59 (1.89–6.84) | ||
| LVEF at baseline | 0.85 (0.42–1.62) | 0.621 | |
| Prior MI | 1.99 (0.26–12.2) | 0.475 | |
| Multi-vessel disease | 2.26 (1.33–3.91) | 0.003 | |
| CTO target vessel | 1.11 (0.39–2.83) | 0.838 | |
| RCA | 4.96 (2.18–11.8) | ||
| LAD | 0.61 (0.14–1.95) | 0.437 | |
| LCX | 1.18 (0.68–2.04) | 0.552 | |
| Total CTO length (mm) | 1.95 (0.85–4.30) | 0.117 | |
| SYNTAX score | 1.68 (0.50–5.05) | 0.387 | |
| J-CTO score | 4.48 (1.28–28.3) | 0.020 | |
| Complete revascularization | 0.29 (0.108–0.755) | 0.012 | |
| Blunt stump | 1.64 (0.73–3.54) | 0.231 | |
| Tortuosity |
1.20 (0.48–2.77) | 0.689 | |
| Calcification | 1.08 (0.43–2.46) | 0.864 | |
| Reattempt | 0.82 (0.31–1.92) | 0.662 | |
| Multivariate | |||
| CKD | 1.38 (1.08–1.78) | 0.011 | |
| The presence of DM | 0.58 (0.32–1.03) | 0.260 | |
| CTO vessel (RCA) | 1.16 (0.11–11.53) | 0.893 | |
| J-CTO score | 3.41 (0.20–16.88) | 0.341 | |
| Multi-vessel disease | 1.69 (1.21–2.36) | 0.002 | |
| Complete revascularization | 0.36 (0.14–0.88) | 0.026 | |
DM, diabetes mellitus; MI, myocardial infarction; MACEs, major adverse cardiac and cerebrovascular events; CTO, chronic total occlusion; LAD, left anterior descending coronary artery; LCX, left circumflex coronary artery; RCA, right coronary artery; J-CTO, multicenter CTO registry in Japan; CKD, chronic kidney disease; HR, hazard ratio; 95% CI, 95% confidence interval; LVEF, left ventricular ejection fraction; SYNTAX, Synergy between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery.
This is the first study to assess the clinical outcomes after a successful PCI for CTO in patients with and without DM who have LV systolic dysfunction over two years. The results revealed several key findings: (1) the presence of DM is not an independent risk factor for MACEs. In addition, multi-vessel disease and CKD were independent predictors of MACEs, whereas complete revascularization was associated with a decreased incidence of MACEs. (2) patients with DM had an increased incidence of CKD, higher serum creatinine and hemoglobin A1c levels, and lower eGFR. Patients with DM were less likely to utilize angiotensin-converting enzyme inhibitors medications and angiotensin receptor blockers than those without DM. (3) patients with DM exhibited an increased incidence of multi-vessel CAD, a greater number of lesions per patient, and elevated J-CTO and SYNTAX scores than non-DM patients. (4) DM was associated with decreased long-term survival benefits regarding MACEs following a successful CTO-PCI.
In this study, 53.5% (99 out of 185) of patients with LV systolic dysfunction undergoing CTO-PCI were diagnosed with DM. This finding aligns with previous studies reporting a 27–45% DM prevalence among CTO patients [5, 7, 8]. It has been consistently observed that patients with DM exhibit a more accelerated progression of atherosclerotic burden and more widespread coronary atherosclerosis compared to non-DM individuals [4, 27]. In addition, previous research has shown that DM patients are more likely to experience hypertension, previous PCIs, and strokes [10]. Our findings further indicate that DM patients have higher rates of chronic kidney disease, elevated serum creatinine and hemoglobin A1c levels, and reduced eGFR. Patients with DM are more prone to have complex and severe CAD. This condition frequently involves the presence of multi-vessel disease, diffuse narrowing, and calcifications in the coronary arteries [28]. This study also revealed that diabetic patients more often present with multi-vessel disease, higher J-CTO scores, and SYNTAX scores compared to non-diabetic patients, as reported in earlier studies [5, 8, 10]. In patients suffering from complex or multi-vessel CAD who have PCI, the occurrence of CTO was demonstrated to have a negative impact on the extent of revascularization and long-term clinical outcomes, including death, repeat revascularization, and stent thrombosis [29]. This impact is notably more pronounced in DM patients, who exhibit a two-fold higher prevalence of CTOs than non-diabetic individuals [30]. Furthermore, while DM significantly worsens the prognosis in CAD patients undergoing coronary revascularization, other cardiovascular risk factors, and comorbidities that adversely affect outcomes are also more prevalent in this group [31]. As a result, diabetic patients who have CTO-PCI have a greater cardiovascular risk profile compared to those without diabetes [6].
Patients suffering from DM had a higher incidence of CTOs [30]. However, diabetic patients undergo PCI for CTO less often compared to non-diabetic patients [7, 32]. This phenomenon, known as the treatment-risk paradox, reflects the less frequent intervention in high-risk compared to lower-risk patients within the PCI population [4]. Patients with diabetes continue to have an increased risk of long-term MACEs following PCI, even with the use of newer-generation drug-eluting stents. This is mainly because they are more likely to require repeat procedures to reopen the blocked blood vessels, regardless of the severity of their underlying CAD [33]. Guo et al. [8] revealed a significant increase in MACEs among diabetes patients after a successful PCI for CTO. Similarly, Sanguineti F et al. [9] reported elevated MACE rates in diabetic CTO patients during a 4.2-year follow-up period. Systematic reviews have consistently indicated that diabetic patients undergoing successful CTO-PCI have an increased risk of adverse clinical outcomes compared to non-diabetic patients [34, 35]. Zhu et al. [36] found that diabetic patients experienced higher rates of MACEs following successful CTO-PCI, particularly within follow-up periods shorter than three years. Wang et al. [37], analyzing 5-year outcomes in 719 patients post-successful CTO-PCI (316 diabetic and 403 non-diabetic), noted that non-diabetic patients showed superior long-term survival benefits in terms of MACEs contrasted with diabetic patients. However, in several studies, there were no statistically significant variations in MACE rates involving diabetic and non-diabetic patients over follow-up periods ranging from 1.7 to 5 years [11, 12, 13]. In these present studies, MACEs were consistently increased in diabetic patients compared to non-diabetic patients following successful CTO-PCI.
Patients with DM are more prone to developing cardiomyopathy associated with LV systolic dysfunction, potentially leading to significant decreases in the viability of myocardium downstream from a CTO [9, 38]. Furthermore, the presence of a CTO in a myocardial infarction-affected artery often results in a significant scar and, notably, a larger area surrounding the scar [39]. This larger border zone is associated with an increased incidence of arrhythmias and sudden cardiac death [39]. Revascularizing the viable or ischemic myocardium in the CTO region can improve survival by reducing scar tissue formation after a heart attack [39]. Our research sample found no significant disparities in the rates of complete revascularization between the diabetic and non-diabetic cohorts. A Study has shown that performing complete myocardial revascularization is associated with lower mortality rates, a reduced incidence of MI, and a decreased need for repeat revascularization [40]. DM patients who undergo incomplete revascularization are at a higher risk of long-term MACEs, including death, MI, stroke, or the need for repeat revascularization [41]. Our study indicates that LV systolic dysfunction patients with DM may experience more unfavorable long-term clinical outcomes following successful CTO PCI because of multiple contributing factors. DM, which is a well-known risk factor for CAD, is associated with more negative angiographic and clinical features [6, 31]. Moreover, patients with DM typically present with an increased number of lesions per patient, potentially increasing the risk of adverse outcomes [42]. Secondly, DM may exacerbate the risk of adverse outcomes by negatively affecting post-procedure blood glucose levels, lipid metabolism, insulin resistance, susceptibility to coronary plaque formation, and vascular endothelial function [43, 44]. The increased amount of platelet aggregation among DM patients and hypo-responsiveness to anti-platelet drugs such as aspirin and clopidogrel result in increased adverse outcomes. The impaired coronary collateralization seen in DM patients might also play a role in their unfavorable prognosis [45].
Consistent with previous studies, our findings corroborate that multi-vessel disease is linked to increased risks of MACEs [35]. Although the prevalence of CTOs was comparable across coronary territories between the two groups, in our CTO cohort, diabetic patients exhibited a higher rate of multi-vessel disease, which could predispose them to elevated long-term mortality and MACEs. Previous studies also found a strong link between CKD and a higher frequency of MACEs. Previous studies have identified renal insufficiency as a strong independent predictor of poor clinical outcomes post-PCI for CTO [11, 13]. The influence of CKD on patients with CTO requires further investigation to determine whether the observed adverse outcomes are attributable solely to the additional risk posed by CKD in conjunction with DM or if CKD alone constitutes an independent risk variable that contributes to negative cardiovascular findings within patients suffering from CTO lesions. In our research, complete revascularization was independently associated with a decreased risk of MACEs. Our results suggest that complete revascularization might mitigate future coronary events by alleviating the burden on non-CTO arteries in patients with DM. This is because the myocardial territory supplied by a CTO artery receives collateral blood flow from other coronary arteries [46]. Our results indicate that all patients exhibited multi-vessel disease, involving at least half of the coronary system. Therefore, complete revascularization could alleviate the functional burden on non-CTO arteries. Moreover, in the event of subsequent coronary incidents, the revascularized CTO artery could potentially support the affected artery [47, 48]. Similar to the results of previous studies [11, 13], our research has shown that DM was not an independent predictor for MACEs. This result may be due to the evolution of equipment, new application techniques, and the accumulation of recent CTO-PCI experience.
This research has several limitations. First, its retrospective design may introduce selection and information biases. Second, the research findings, performed at a single center, might not be generalizable to a wider population. It is imperative, therefore, to validate these results through multi-center clinical trials. Third, the limited sample size may impede the research’s ability to identify substantial disparities between the cohorts. Fourth, the absence of a medically treated comparison group precluded a comprehensive outcome comparison. Only successful CTO PCI cases were included, excluding failed procedures, which could affect the validity of the conclusions. Fifth, data collection relied on hospital information systems and telephone follow-ups, potentially introducing unknown confounding factors that could skew the results. Specific data, such as coronary collateral scoring and glycemic control during the extended follow-up, were lacking, possibly compromising the precise assessment of future adverse event risks in CTO patients. Additionally, the selection criteria could also influence the long-term outcome, unmatched baseline characteristics (such as the rate of multi-vessel coronary disease, complete revascularization and CKD and baseline renal function and SYNTAX and J-CTO score), and treatment choice (such as angiotensin-converting enzyme inhibitors and angiotensin receptor blocker). Finally, 19 patients had a history of CABG, and 15 patients rejected PCI for main coronary artery CTO and chose optimal medical therapy. The other four patients chose revascularization for left internal thoracic artery graft or saphenous vein graft and rejected PCI for main coronary artery CTO. Thus, the present research excluded post-CABG patients.
Our registry found that LV systolic dysfunction patients with DM who underwent successful CTO revascularization had increased rates of MACEs over a two-year follow-up compared to patients without DM. However, the presence of DM is not an independent risk factor for MACEs. Moreover, multi-vessel disease and CKD significantly increased the incidence of MACEs, whereas complete revascularization was associated with a reduced risk. Further large-scale, rigorously designed, randomized controlled trials with extended follow-ups are essential to corroborate these findings.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
XW and LW had the idea for the paper, reviewed and edited it critically for important intellectual content. HBH and HH performed the literature search and analysis. XW, MXW, LW, QL, ZL and HH substantially contributed to the conception of the paper, drafted and critically revised the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The present research was carried out in accordance with the tenets mentioned in the Helsinki Declaration and was approved by the Ethical Board of Xiangtan Central Hospital (approval number: X201781019-1). Prior to the commencement of the research, our team obtained written informed consent from each patient.
Not applicable.
This work was supported by Natural Science Foundation of Hunan Province (No. 2022JJ30575) and Health Research Project of Hunan Provincial Health Commission (No. 20233486).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.