


1 Department of Vascular Surgery, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, 100005 Beijing, China
2 Peking University Fifth School of Clinical Medicine, 100005 Beijing, China
3 Department of Vascular Surgery, The First Affiliated Hospital of Nanjing Medical University, 210029 Nanjing, Jiangsu, China
4 Peking Union Medical College, Chinese Academy of Medical Science, 100006 Beijing, China
†These authors contributed equally.
Abstract
The operation rate for different involved arteries and the manifestation of vessel involvement of patients with Takayasu arteritis undergoing open or endovascular operations remain unclear. We aimed to investigate the clinical characteristics, vessel involvement, angiographic classification and operations information in a large cohort of patients with Takayasu arteritis undergoing open or endovascular operations at a single centre in China.
From January 2017 to October 2022, a total of 153 consecutive patients undergoing open or endovascular operations were recruited from the Department of Vascular Surgery of Beijing Hospital. The demographic characteristics, clinical presentations, pattern of vascular involvement and operation information were collected and analysed.
The majority of patients were female (128/153, 83.7%). The most common vascular finding was hypertension (66.7%). The subclavian (74.2%), carotid (70.1%) and renal (68.9%) arteries were the most commonly involved arteries. Type V (40.5%) was the most common angiographic classification pattern. A total of 296 open or endovascular operations were performed, including 73 percutaneous transluminal angioplasties (PTAs), 50 stent placements and 173 bypass graft operations. Patients with renal (83.3%) or carotid (65.2%) artery involvement had markedly higher rates of undergoing operations.
The subclavian and carotid arteries, as well as the type V (40.5%) pattern, exhibited the highest frequency of involvement among patients with Takayasu arteritis who underwent open or endovascular operations. Variations in angiographic features can result in differences in clinical manifestations and significantly impact the possibility and modality of operations.
Keywords
- angiography manifestation
- clinical characteristics
- surgery
- Takayasu arteritis
Takayasu arteritis (TA) is a rare chronic granulomatous vasculitis that mainly involves the aorta and its primary branches [1]. The disease is reported all over the world, but a high incidence and prevalence of TA were found in East Asia and Turkey [2]. Typically, TA predominantly affects young females under forty years of age [3]. In the early phases of TA, nonspecific constitutional symptoms and signs include fever, general fatigue, neck pain, weight loss and headache/dizziness. Subsequently, inflammation and fibrosis of involved vessels progress, leading to segmental stenosis, occlusion, aneurysm, and even ischemia of involved organs [4, 5].
To date, the pathogenesis of TA is not well understood. Numerous studies have demonstrated that the combination of glucocorticoids (GCs) with various immunosuppressants can effectively control inflammation and active disease [2, 6, 7, 8, 9]. Accumulating evidence has also shown the clinical efficacy of biologic agents, including infliximab (IFX), tocilizumab and B-cell depletion, for TA [10, 11, 12]. Unfortunately, despite an appropriate course of immunosuppressive therapy, persistent active diseases remain common [13].
In cases where medical treatment cannot improve the manifestations, open or endovascular operations seem to be the only choice. Multiple studies have shown that these operations not only improve ischemic symptoms caused by cardiovascular malformations (i.e., stenosis or aneurysm) but also may increase long-term survival in patients with TA [14, 15, 16]. However, the operation rate for different involved arteries and the manifestation of vessel involvement of patients with Takayasu arteritis undergoing open or endovascular operations remain unclear. Here, we performed a retrospective study with a large sample size to investigate the clinical features, imaging findings and operation information for Chinese patients with TA undergoing open or endovascular operations, and conducted a comparison of our data with primarily medicine-treated groups reported in existing literature.We present information to determine the involved vessels that are more commonly in need of these operations to better recognize patients who may need a higher level of surveillance in cases where these operations are inevitable.
Between January 2017 and October 2022, a total of
153 consecutive patients were
recruited from the Department of Vascular
Surgery of Beijing Hospital. Subjects meeting all of the following criteria were
eligible for the study: (1) diagnosed with TA by two expert rheumatologists
according to the 1990 American College of Rheumatology (ACR) criteria and (2) met
at least one of the following operation indication: (i) severe stenosis
(
Subjects with one or more of the following conditions were excluded: (1) comorbidity with other rheumatic diseases or cancer or infectious disease (except tuberculosis); (2) inability to tolerate anaesthesia and trauma due to poor cardiorespiratory function; (3) mental or other cognitive impairment or refusal to cooperate with necessary experiments; and (4) pregnancy.
The demographic characteristics, clinical presentations, laboratory examination, pattern of vascular involvement and operation information were retrospectively collected and analysed. The angiographic involvement pattern was based on criteria established by Hata et al. [17], and the angiographicresults were analysed. Each patient underwent at least one blood vessel examination to assess the extent of blood vessel involvement, which includes catheter angiography, computed tomography angiography (CTA) and ultrasound.
We conducted a search on PubMed for articles using the keywords ‘Takayasu’s arteritis’ and ‘cohort study’ to obtain the clinical characteristics of patients with TA in other studies. Given the low incidence of TA, studies including more than 50 patients were included in this research, and all patients involved in these studies fulfilled the 1990 ACR criteria for TA. Comparisons were conducted between the current study and the studies identified through the literature search.
Each patient underwent blood vessel examinations using either catheter angiography, computed tomography angiography (CTA), or ultrasound, at least once, in order to assess the extent of blood vessel involvement. Stenosis was determined by measuring the ratio between the diameter of the narrowest segment and the diameter of a normal segment of the artery. Restenosis was defined as a target artery narrowing of more than 50% in diameter. Occlusion was defined as an absence of flow in the treated segment. The reporting standards of patency status were defined by the Society for Vascular Surgery.
SPSS 20.0 software (SPSS Inc., Chicago, IL, USA) was used to perform all statistical analyses. Continuous variables are presented as median (Q1, Q3). Categorical data are expressed as the number (percentage).
The clinical features are presented in Table 1. The majority of patients were female (128/153, 83.7%). The most common vascular finding was hypertension (66.7%). This could be a result of hypertension failing to be controlled by appropriate medical therapy being the main leading cause of renal vascular operations for patients with TA and a huge portion of operations performed in this study involved the renal arteries. Cardiovascular risk factors such as diabetes or hyperlipidemia were rare in these patients. Dizziness (37.9%) was the most common neurological manifestation, followed by visual disturbances or loss of vision (18.3%) and headache (12.4%). The median erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) level, WBC count, and creatinine (Cr) level were all evaluated (Table 1).
| Clinical characteristic | No. or value | Proportion (%) | |
| Sex | |||
| Female | 128 | 83.7 | |
| Male | 25 | 16.3 | |
| Age (years) | 30.3 | ||
| Inflammatory symptoms | |||
| Fever | 4 | 2.6 | |
| Neck pain | 2 | 1.3 | |
| Fatigue | 3 | 2.0 | |
| Vascular findings | |||
| Hypertension | 102 | 66.7 | |
| Weak pulse | 14 | 9.2 | |
| Upper limb weakness | 10 | 6.5 | |
| Lower limb weakness | 12 | 7.8 | |
| Cardiovascular risk factors | |||
| Diabetes | 0 | 0 | |
| Hyperlipidaemia | 7 | 4.6 | |
| Hyperhomocysteinaemia | 7 | 4.6 | |
| Neurological manifestations | |||
| Dizziness | 58 | 37.9 | |
| Headache | 19 | 12.4 | |
| Visual disturbance or loss | 28 | 18.3 | |
| TIA | 4 | 2.6 | |
| Stroke | 10 | 6.5 | |
| History of tuberculosis | 16 | 10.5 | |
| Laboratory tests | |||
| ESR (mm/h) | 8.0 (5.0, 13.0) a | ||
| CRP (mg/dL) | 0.3 (0.1, 0.8) a | ||
| WBC (109/L) | 8.8 (6.0, 10.3) a | ||
| Cr (µmol/L) | 59.0 (50.0, 74.0) a | ||
a median (Q1, Q3).
ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; WBC, white blood cell; Cr, creatinine; TA, Takayasu arteritis; TIA, transient ischemic attack.
The details of vessel involvement are shown in Table 2. Among them, the subclavian (74.2%), carotid (70.1%) and renal (68.9%) arteries were the most commonly involved arteries, and their occurrences of involvement were all above 50%. We found another 4 cohort studies from different geographic areas that also described the details of the involved vessels. The details are shown in Table 3 (Ref. [5, 18, 19, 20]). The occurrence rates of carotid artery and subclavian artery involvement were similarly high, but our study had a relatively higher rate of renal artery involvement than the 4 other studies. Obvious differences in occurrence rates were also found in the aorta between the 5 studies.
| Artery | Patients with imaging, n | Any arterial lesion | Any arterial lesion% | Stenosis% | Occlusion% | Aneurysm% | |
| Carotid artery | 127 | 89 | 70.1 | 19.7 | 48.8 | 1.6 | |
| Left | 127 | 87 | 68.5 | 29.9 | 38.6 | 0.0 | |
| Right | 127 | 78 | 61.4 | 29.9 | 29.9 | 1.6 | |
| Innominate artery | 122 | 44 | 36.1 | 31.1 | 4.9 | 0.0 | |
| Subclavian artery | 128 | 95 | 74.2 | 25.0 | 49.2 | 0.0 | |
| Left | 128 | 91 | 71.1 | 30.5 | 40.6 | 0.0 | |
| Right | 128 | 61 | 47.7 | 21.1 | 26.6 | 0.0 | |
| Vertebral artery | 124 | 59 | 47.6 | 26.6 | 21.0 | 0.0 | |
| Left | 124 | 45 | 36.3 | 22.6 | 13.7 | 0.0 | |
| Right | 124 | 36 | 29.0 | 18.5 | 10.5 | 0.0 | |
| Ascending aorta | 98 | 11 | 11.2 | 10.2 | 0.0 | 1.0 | |
| Aortic arch | 118 | 18 | 15.3 | 12.7 | 0.0 | 2.5 | |
| Abdominal aorta | 102 | 61 | 59.8 | 48.0 | 6.9 | 4.9 | |
| AA above RA | 102 | 46 | 45.1 | 41.2 | 0.0 | 3.9 | |
| AA beneath RA | 102 | 34 | 33.3 | 25.5 | 6.9 | 1.0 | |
| Thoracic aorta | 108 | 38 | 35.2 | 34.3 | 0.0 | 0.9 | |
| Renal artery | 122 | 84 | 68.9 | 37.7 | 30.3 | 0.8 | |
| Left | 122 | 65 | 53.3 | 39.3 | 13.1 | 0.8 | |
| Right | 122 | 62 | 50.8 | 30.3 | 20.5 | 0.0 | |
| Mesenteric artery | 89 | 37 | 41.6 | 29.2 | 12.4 | 0.0 | |
| Superior mesenteric artery | 85 | 36 | 42.4 | 30.6 | 11.8 | 0.0 | |
| Inferior mesenteric artery | 67 | 3 | 4.5 | 3.0 | 1.5 | 0.0 | |
| Iliacfemoral artery | 92 | 13 | 14.1 | 7.6 | 6.5 | 0.0 | |
| Left | 92 | 11 | 12.0 | 6.5 | 5.4 | 0.0 | |
| Right | 92 | 12 | 13.0 | 7.6 | 5.4 | 0.0 | |
RA, renal artery; AA, abdominal aorta.
| Artery | This study (n = 153) | Li et al. (n = 411) [18] | Lee et al. (n = 204) [19] | Mwipatayi et al. (n = 272) [20] | Schmidt et al. (n = 126) [5] | ||||||
| Left | Right | Left | Right | Left | Right | Left | Right | Left | Right | ||
| Carotid artery | 68.5% | 61.4% | 79.1% | 72.1% | 63.7% | 30.5% | 50.9% | 41.7% | |||
| Stenosis | 29.9% | 29.9% | 58.6% | 33.3% | 32.3% | 21.7% | 41.7% | 37.0% | |||
| Occlusion | 38.6% | 29.9% | 24.8% | 21.1% | 9.8% | 10.2% | 5.6% | ||||
| Dilatation | ND | ND | 3.9% | 1.0% | 1.5% | ND | ND | ND | |||
| Aneurysm | 0 | 1.4% | 0.5% | 6.3% | 0.9% | 0.9% | |||||
| Innominate artery | 36.1% | 19.7% | 46.8% | 10.5% | 25.5% | ||||||
| Stenosis | 31.1% | 14.8% | 16.3% | 8.1% | 18.9% | ||||||
| Occlusion | 4.9% | 3.9% | 3.0% | 6.6% | |||||||
| Dilatation | ND | 1.9% | 4.0% | ND | ND | ||||||
| Aneurysm | 0 | 0.2% | 5.9% | 0.9% | |||||||
| Subclavian artery | 71.1% | 47.7% | 79.8% | 67.1% | 55.2% | ND | 66.3% | 41.0% | |||
| Stenosis | 30.5% | 21.1% | 56.4% | 26.0% | 24.6% | ND | 43.3% | 36.2% | |||
| Occlusion | 40.6% | 26.6% | 31.6% | 34.8% | 14.3% | ND | 29.8% | 4.8% | |||
| Dilatation | ND | ND | 2.7% | 0.5% | 4.4% | ND | ND | ND | |||
| Aneurysm | 0 | 0 | 1.2% | ND | 0 | 1.0% | |||||
| Vertebral artery | 36.3% | 29.0% | 28.7% | ND | ND | 18.5% | 13.0% | ||||
| Stenosis | 22.6% | 18.5% | 20.0% | ND | ND | 15.7% | 9.3% | ||||
| Occlusion | 13.7% | 10.5% | 11.2% | ND | ND | 2.8% | 3.7% | ||||
| Dilatation | ND | ND | 2.4% | ND | ND | ND | ND | ||||
| Aneurysm | 0 | 0 | 0.2% | ND | ND | 0 | 0 | ||||
| Ascending aorta | 11.2% | 9.5% | 47.8% | 23.9% | 9.1% | ||||||
| Stenosis | 10.2% | 0.7% | 0 | 5.5% | 2.7% | ||||||
| Dilatation | ND | 9.0% | 25.4% | ND | ND | ||||||
| Aneurysm | 1.0% | 0.5% | 15.8% | 2.7% | |||||||
| Aortic arch | 15.3% | 7.8% | 37.9% | 33.1% | 4.5% | ||||||
| Stenosis | 12.7% | 6.1% | 0.5% | 16.5% | 2.7% | ||||||
| Dilatation | ND | 1.7% | 3.4% | ND | ND | ||||||
| Aneurysm | 2.5% | 0.2% | 13.2% | 1.8% | |||||||
| Abdominal aorta | 45.1%a | 33.3%b | 38.4% | 63.2% | 68.4% | 23.7%a | 27.4%b | ||||
| Stenosis | 41.2% | 25.5% | 32.6% | 38.3% | 42.3% | 20.4% | 25.3% | ||||
| Occlusion | 0 | 6.9% | 2.9% | 4.0% | 1.1% | 2.1% | |||||
| Dilatation | ND | ND | 0 | 6.0% | ND | ND | ND | ||||
| Aneurysm | 3.9% | 1.0% | 1.4% | 15.1% | 2.2% | 1.1% | |||||
| Thoracic aorta | 35.2% | 17.5% | 57.2% | 58.1% | 19.1% | ||||||
| Stenosis | 34.3% | 17.5% | 22.9% | 36.0% | 18.2% | ||||||
| Occlusion | 0 | 0 | 0 | 0 | |||||||
| Dilatation | ND | ND | 3.4% | 3.0% | ND | ND | |||||
| Aneurysm | 0.9% | 0.5% | 14.0% | 0.9% | |||||||
| Renal artery | 53.3% | 50.8% | 48.9% | 32.2% | 31.7% | ND | 18.7% | 20.9% | |||
| Stenosis | 39.3% | 30.3% | 44.3% | 25.2% | 25.2% | ND | 16.5% | 19.8% | |||
| Occlusion | 13.1% | 20.5% | 10.5% | 6.0% | 4.5% | ND | 4.4% | 2.2% | |||
| Dilatation | ND | ND | 1.5% | 0 | 0 | ND | ND | ND | |||
| Aneurysm | 0.8 | 0 | 0.5% | ND | 0 | 0 | |||||
| Mesenteric artery | 42.4%c | 4.5%d | 29.7% | 22.8%c | 3.5%d | 37.1% | 24.7%c | 6.9%d | |||
| Stenosis | 30.6% | 3.0% | 21.9% | 14.4% | 0.5% | 33.8% | 18.0% | 2.3% | |||
| Occlusion | 11.8% | 1.5% | 8.0% | 5.9% | 2.0% | 6.7% | 4.6% | ||||
| Dilatation | ND | ND | 0.2% | 1.0% | 1.0% | ND | ND | ND | |||
| Aneurysm | 0 | 0 | 0 | 3.3% | 0 | 0 | |||||
aSuprarenal aorta.
bInfrarenal aorta.
cSuperior mesenteric artery.
dInferior mesenteric artery.
ND, no data.
Seven studies that also detailed the angiographic involvement pattern based on the classification of Hata et al. [17] were selected to compare the angiographic classification between the previous literature and the present study. The details are shown in Table 4 (Ref. [5, 18, 19, 21, 22, 23, 24]). In the 7 studies (including the present study), the type V pattern was the most common and had a similarly high prevalence. However, one study from China showed that type I was the most common pattern [5, 18, 19, 21, 22, 23, 24]. This study had the highest proportion of individuals with Type IV compared to other studies.
| This study | He et al. [21] | Sun et al. [22] | Danda et al. [23] | Chen et al. [24] | Li et al. [18] | Lee et al. [19] | Schmidt et al. [5] | |
| Total (n) | 153 | 240 | 81 | 585 | 97 | 411 | 204 | 126 |
| Type I (%) | 24.2 | 22.9 | 11.1 | 20.9 | 34.0 | 22.1 | 11.1 | 20 |
| Type IIa (%) | 4.6 | 3.8 | 8.6 | 0.5 | 21.7 | 3.9 | 8.6 | 6 |
| Type IIb (%) | 4.6 | 4.6 | 6.2 | 3.6 | 7.2 | 3.9 | 14.1 | 7 |
| Type III (%) | 4.6 | 2.9 | 13.6 | 5.5 | 2.1 | 2.9 | 4.0 | 5 |
| Type IV (%) | 21.6 | 19.2 | 9.9 | 18.3 | 5.2 | 6.3 | 7.6 | 5 |
| Type V (%) | 40.5 | 46.7 | 50.6 | 51.3 | 29.9 | 60.8 | 54.5 | 57 |
A total of 296 open or endovascular operations, including 73 percutaneous transluminal angioplasties (PTAs) (24.7%), 50 stent placements (16.9%) and 173 bypass graft operations (58.4%), were performed in 153 patients. The details are shown in Table 5. Operation rates for different involved vessel are ranked and showed in Fig. 1.
| PTA | Stent | Bypass | Total | Patients underwent operations | Patients with involvement | Operation rate for involved vessel (%) | ||
| Supraaortic branches | 20 | 14 | 82 | 116 | ||||
| Carotid | 13 | 9 | 69 | 91 | 58 | 89 | 65.2 | |
| Vertebral | 0 | 2 | 6 | 8 | 6 | 59 | 10.2 | |
| Subclavian | 7 | 3 | 7 | 17 | 14 | 95 | 14.7 | |
| Aorta | 11 | 18 | 20 | 49 | ||||
| Thoracic | 4 | 7 | 10 | 21 | 16 | 38 | 42.1 | |
| Abdominal | 7 | 11 | 10 | 28 | 23 | 61 | 37.7 | |
| Renal | 39 | 11 | 58 | 108 | 70 | 84 | 83.3 | |
| Iliacfemoral | 1 | 4 | 8 | 13 | 7 | 13 | 53.8 | |
| Mesenteric | 2 | 3 | 5 | 10 | 8 | 37 | 21.6 | |
PTA, percutaneous transluminal angioplasty.
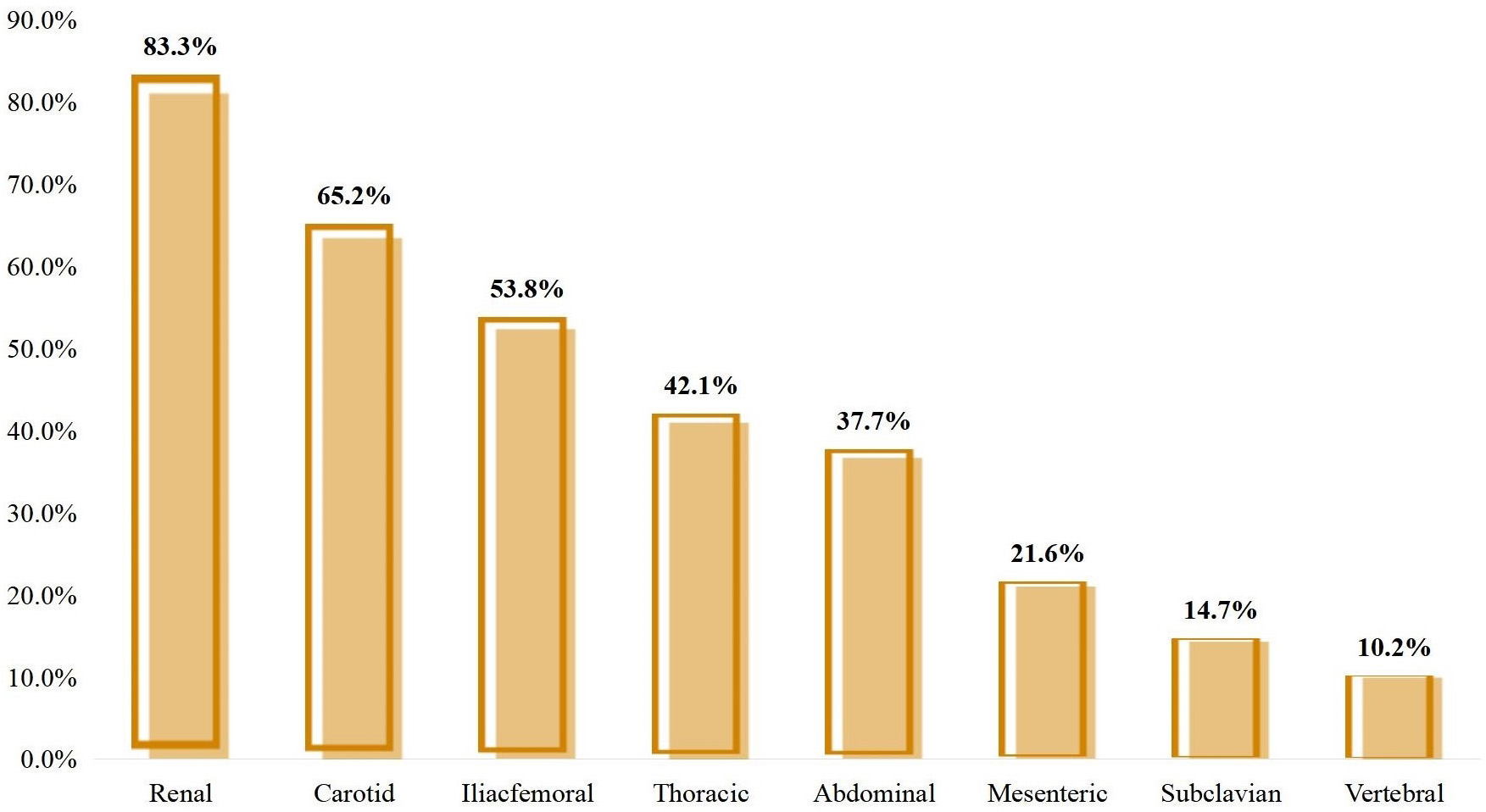 Fig. 1.
Fig. 1.
Operation rate for different involved vessel.
Large differences in the number of operations and the rate of individuals undergoing operations were found between the different involved arteries. As shown in Table 2, carotid and renal arteries were the most commonly involved arteries. We found that not only were these two arteries more commonly involved, but they were also more commonly in need of revascularisation operations. There were 84 patients with renal artery involvement in this study, 70 of them underwent operations to revascularise the renal artery. This figure was 58 out of 89 for patients with carotid artery involvement. The operation rates in renal and carotid arteries were 83.3% (70/84) and 65.2% (58/89), respectively. Although subclavian arteries were also commonly involved, only 14 patients underwent operations to revascularise their subclavian arteries. This means only 14.7% of patients with subclavian artery involvement underwent operations in this study. Operation rates for the vertebral artery (10.2%) in patients with vessel involvement were relatively low, while for the thoracic aorta (42.1%) and abdominal aorta (37.7%), they were relatively higher. The modalities of these operations also varied for the different involved arteries. PTAs were more common in renal artery operations (39/108, 36.1%) compared to general (24.7%). Unlike renal artery operations, bypass graft operations (69/91, 75.8%) were more common than general (58.4%) in carotid operations. Compared to operations involving the thoracic aorta, operations involving the abdominal aorta had a higher proportion of endovascular operations.
The vertebral artery (16.7%) was the most common vessel involved when more than one operation was required to revascularise for restenosis, followed by the renal artery (14.3%) and abdominal aorta (13.0%).
In this article, we demonstrate the clinical characteristics, vessel involvement, angiographic classification and operation information in a large cohort of patients with TA undergoing open or endovascular operations at a single centre in China. To the best of our knowledge, this is the largest series of patients with TA who were admitted to a department of vascular surgery requiring open or endovascular operations. Past studies were usually focused on patients who were admitted to a department of rheumatology or a department of cardiology where operations, especially bypass graft operations, were not the main modality of treatment; notably, previous reports have shown that surgical bypass has superior patency to endovascular treatments [25]. Multiple studies have shown that open or endovascular operation can improve ischaemic symptoms and increase long-term survival in patients with TA. Limited studies from vascular surgery departments have failed to show the operation rate and modality for different involved arteries in detail with a large series of patients.
Clinical characteristics in patients with TA may vary on the basis of geographic region. The demographic characteristics of the cohort study described in this article are similar to those previously described in East Asia [18, 19, 26]. Patients were mainly women and relatively young. The most common vascular finding in this study was hypertension (66.7%). This could be a result of hypertension failing to be controlled by appropriate medical therapy being the main leading cause of renal vascular operation for patients with TA.
Through the review of the literature, it was observed that the incidence of involvement of both the carotid arteries and subclavian arteries was consistently high across five studies, including our study [5, 18, 19, 27]. The involved vessels in patients with TA varied by different geographic areas. The rate of vessel involvement in this study was similar to the results of Li’s study [18], which is also based on Chinese patients with TA and has the largest number of patients. Compared to the results of Li’s study [18], patients with TA undergoing operations had a higher rate of renal artery and abdominal aorta involvement.
In this study, bypass graft operations (58.4%) were the most common operation for patients with TA undergoing open or endovascular operations, followed by PTAs (24.7%) and stent placements (16.9%). The rates of surgery were higher in patients with renal artery (83.3%) and carotid artery (65.2%) involvement. We assume this is the result that renal artery and carotid artery involvement can cause obvious clinical symptoms in a relatively early stage and the consequences can be catastrophic. The leading causes for renal artery and carotid artery operations were hypertension not controlled by medical therapy and dizziness, respectively. In contrast, the subclavian (14.7%) and vertebral (10.2%) had much lower rates of operations. We speculate this is because symptoms from the involvement of these arteries are usually more insidious until the lesion is very severe because of better compensation and the consequences are usually milder. This result suggested that when dealing with TA patients with renal artery or carotid artery involvement, doctors should be more cautious and keep the option of operating in mind more. A higher level of surveillance is also needed for these patients because the involvement of these arteries has a much higher possibility of requiring an operation. In the meanwhile, subclavian and vertebral involvement seem less worrying, as they rarely needed operating on.
Our study has several limitations, including its single-centre retrospective design. Another weak point of this study is that in this real-world retrospective study, some important variables that are not routinely collected in usual care were not available, such as functional scores and quality-of-life indicators. Some imaging information was also not available as not all patients had all of the desired examinations.
In conclusion, the subclavian and carotid arteries, as well as the type V (40.5%) pattern exhibited the highest frequency of involvement among patients with Takayasu arteritis who underwent open or endovascular operations. In this article, patients with renal artery and carotid artery involvement had a much higher rate of undergoing an operation. Variations in angiographic features can result in differences in clinical manifestations and can significantly impact on the possibility and modalities of operating.
TA, Takayasu arteritis; PTA, percutaneous transluminal angioplasty.
All data points generated or analyzed during this study are included in this article and there are no further underlying data necessary to reproduce the results.
Conception and design: XZ, LG, YL; Data collection: LG, ZW, ZC, RL, YM, YD; Writing the article: XZ, LG, RL, YL; Final approval of the article: YL; Statistical analysis: XZ; Overall responsibility: YL. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The Ethics Committee of Beijing Hospital granted ethical approval for the study protocol (ethics approval number: 2018BJYYEC-030-01). All participants agreed to participate in this study and signed written informed consent forms.
Not applicable.
This work was supported by a grant from The Beijing Hospital Clinical Research 121, Project (No. BJ-2018-089).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.