





1 Department of Cardiology and Institute of Vascular Medicine, Peking University Third Hospital; NHC Key Laboratory of Cardiovascular Molecular Biology and Regulatory Peptides; Key Laboratory of Molecular Cardiovascular Science, Ministry of Education; Beijing Key Laboratory of Cardiovascular Receptors Research, 100191 Beijing, China
2 Research Unit of Medical Science Research Management/Basic and Clinical Research of Metabolic Cardiovascular Diseases, Chinese Academy of Medical Sciences, 100021 Beijing, China
3 State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, 100005 Beijing, China
4 School of Humanities and Social Sciences, Chinese Academy of Medical Science & Peking Union Medical College, 100005 Beijing, China
5 Faculty of Health and Medicine, Division of Health Research, Lancaster University, LA1 4YW Lancaster, UK
6 Department of Physiology and Pathophysiology, School of Basic Medical Sciences, Peking University; Key Laboratory of Molecular Cardiovascular Science, Ministry of Education, 100191 Beijing, China
†These authors contributed equally.
Abstract
Background: The high prevalence of chronic obstructive pulmonary
disease (COPD) in coronary artery disease (CAD) has been acknowledged over the
past decade, although the cause/s remain uncertain due to differences in
diagnoses. COPD has also become a leading CAD comorbidity, although again little
is known about its interactions. This meta-analysis explored COPD prevalence in
the global CAD population, as well as the influence of COPD on CAD.
Methods: PubMed, Web of Science, Embase, and grey literature were
searched until 26th November 2021. The prevalence of COPD was calculated, and
data were grouped according to COPD diagnostic methods, interventions, region,
economic status, etc. Outcomes including all-cause death, cardiac death,
myocardial infarction, revascularization, stroke, heart failure, and respiratory
failure were analyzed. This study was registered with PROSPERO (CRD
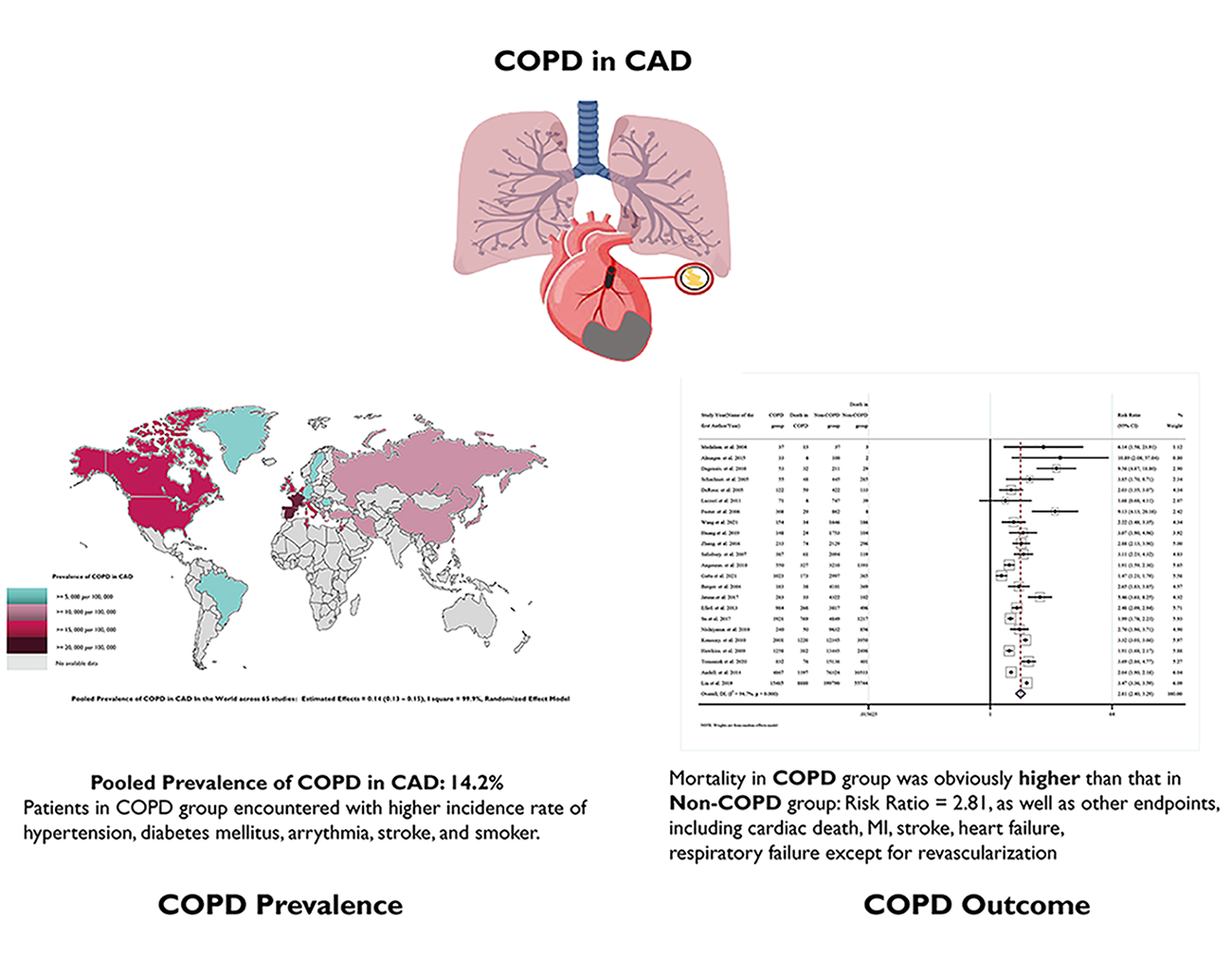
No.42021293270). Results: There was an average prevalence of 14.2% for
COPD in CAD patients (95% CI: 13.3–15.1), with diagnostics of COPD through
spirometry, International Classification of the Diseases (ICD codes), and self-reported methods. Comorbid COPD–CAD patients
were more likely to be smokers and suffer from cardiovascular and respiratory
complications (all odds ratios [OR]
Graphical Abstract
Keywords
- chronic obstructive pulmonary disease
- coronary artery disease
- meta-analysis
Chronic obstructive pulmonary disease (COPD) is a leading cause of death and incidence increases with age [1]. The number of people with chronic respiratory diseases is estimated to be approximately 544.9 million, with almost 55% experiencing COPD [2]. Likewise, coronary artery disease (CAD) is a leading cause of death and consists of common risk factors, including smoking, pollution, unhealthy diet, as well as genetic variances. The coexistence of COPD and CAD is thought to be common and has a hugely detrimental impact on comorbidity outcomes [3]. Indeed, COPD, as a comorbidity of CAD patients, is receiving increased attention, however, there is currently no systematic review or meta-analysis on this growing trend.
The occurrence of CAD with COPD can be understood from both a physiological perspective, including inflammation activation, hypoxia stress, etc., and by considering common risk factors, such as tobacco use, and aging. de Miguel-Díez et al. [4]. reported on the prevalence of COPD in participants who received a percutaneous coronary intervention (PCI) and found that it gradually increased from 6.2% in 2001 to 7.4% in 2011. This highlights a rising global trend of COPD occurring in CAD patients [4, 5]. We know that the prevalence of COPD in the CAD population varies according to diagnostic methods, ethnic differences, and according to socioeconomic differences. Furthermore, some COPD–CAD patients acquired severe dyspnea, hypoxia, and exercise intolerability, which are associated with increased mortality [6]; however, COPD–CAD outcomes vary substantially.
While we are aware that mortality increases with comorbid COPD–CAD and other related outcomes, such as major adverse cardiovascular events (MACEs), revascularization, myocardial infarction (MI), and stroke, there is conflicting evidence. This means that clinical choices related to revascularization for COPD patients have a direct impact and fuel the debate around the most effective intervention—coronary artery bypass graft (CABG) or PCI. Clearly, there is a need to systematically assess the available evidence to identify gaps in our knowledge and recommend further research. Therefore, we conducted this first systematic review and meta-analysis to investigate the prevalence of COPD in CAD patients, as well as to understand how COPD influences CAD.
Search strategies were developed after a discussion with two physicians and a clinical epidemiologist (YDT, CLS, and SS). PubMed, Embase, Web of Science, and grey literature sources were searched exhaustively. Two additional websites, e.g., Chest, and the European Heart Journal, were searched to ensure that all current research was included and because of their respective high impact in publishing circulatory and respiratory systems research. A detailed outline of our search strategy has been provided in the Supplementary Materials, as Supplementary Material 1.
Studies identified through the aforementioned databases from inception until 26
November 2021 were initially considered eligible. Eligibility criteria are
provided in Fig. 1. CAD was diagnosed and included: (1) existing myocardial
infarction; (2) those treated with PCI or a CABG;
(3)
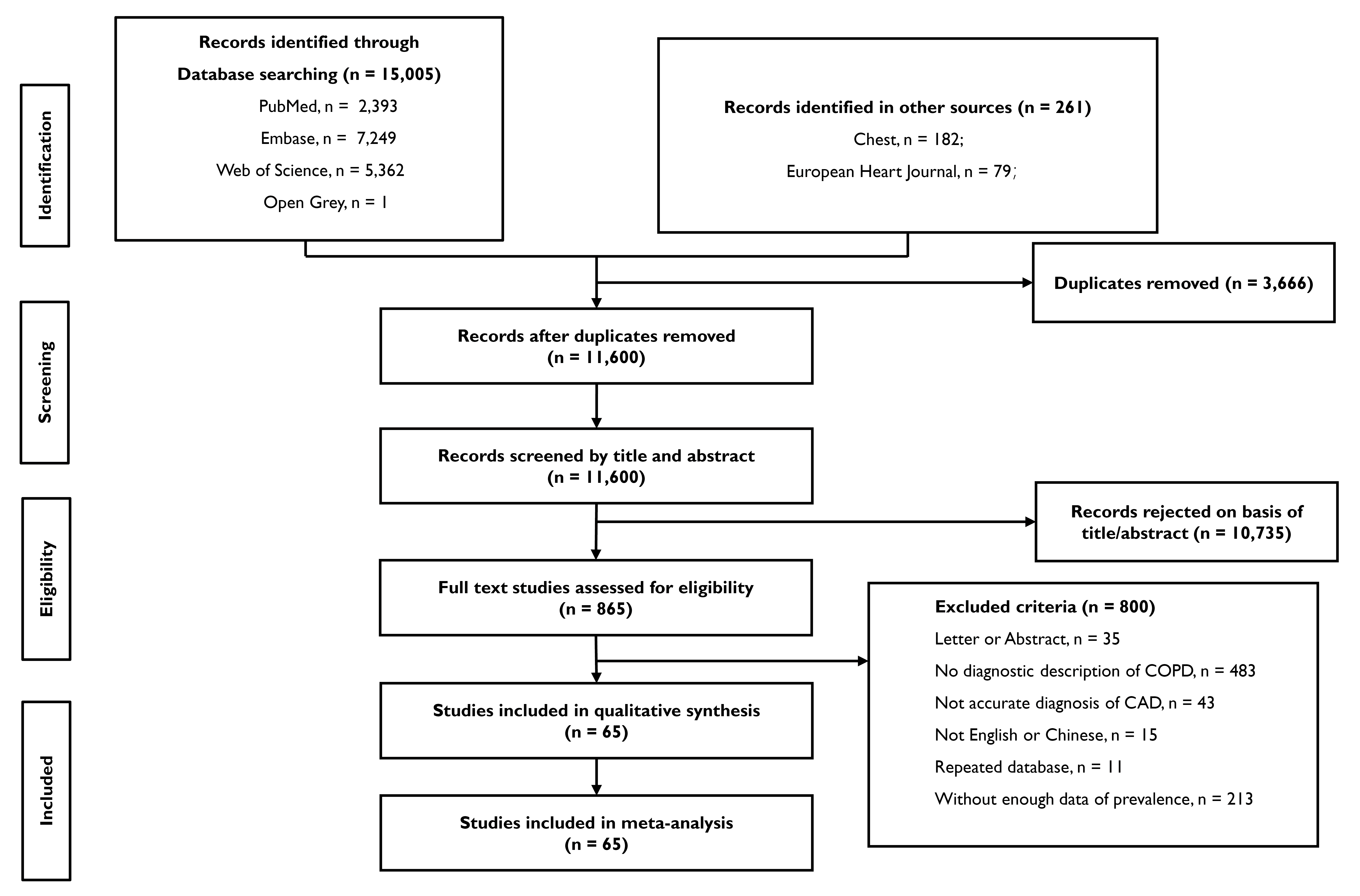 Fig. 1.
Fig. 1.Flowchart according to PRISMA statement. Flowchart of the study. COPD, chronic obstructive pulmonary disease; CAD, coronary artery disease.
COPD was diagnosed and classified according to the pulmonary function test (PFT), International Classification of the Diseases (ICD codes), or through self-reported methods. It is important to note that in most studies, the PFT criteria met the gold standard criteria, although a small number of studies involved various other PFT criteria, which were developed before the gold standard was established. ICD codes indicate that patients might have been diagnosed with COPD prior to admission and should not undergo the PFT. Various studies exhibited divergent self-reported methodologies–for instance, a combination of clinical symptoms and COPD medication usage. Studies that did not report diagnostic methods for either CAD or COPD were excluded. Two reviewers independently screened studies (YTZ and ZLH) and discrepancies were resolved by the third reviewer (SS).
Two reviewers (YTZ and ZLH) independently assessed the risk of bias using two
separate tools. For the prevalence of COPD–CAD, we used a customized
Newcastle–Ottawa Scale (NOS), to classify studies. Scores
Two reviewers (YTZ and ZLH) extracted and cross-checked data from studies, including demographics and study designs, such as country or region, study type, age, gender, etc. Detailed information has been provided in Table 1 (Ref. [4, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61,62, 63, 64, 65, 66, 67, 68, 69, 70, 71]) and Supplementary Table 1. Supplementary Material 3 including all supplemental figures and tables.
| Study year (name of the first author/year) | Research held country or region | Area | Economic status | Study type | Patients characteristics | Diagnosed method |
| Erdil et al. 2016 [13] | Turkey | Europe | Upper-middle income | Observational, single center | CAD patients underwent CABG | Pulmonary function test |
| Geçmen et al. 2016 [14] | Turkey | Europe | Upper-middle income | Observational, single center | CAD patients underwent CABG | Pulmonary function test |
| Barandon et al. 2008 [15] | France | Europe | High income | Observational, single center | CAD patients underwent CABG | Pulmonary function test |
| Yangui et al. 2021 [16] | Tunisia | Africa | Upper-middle income | Observational, single center | CAD patients | Pulmonary function test |
| Almagro et al. 2015 [17] | Spain | Europe | High income | Observational, single center | CAD patients underwent PCI | Pulmonary function test |
| Campo et al. 2016 [18] | Italy | Europe | High income | Observational, single center | MI patients with smoking | Pulmonary function test |
| Stelle et al. 2011 [19] | United States of America | North America | High income | Observational, single center | CAD patients underwent CABG | Pulmonary function test |
| Hamrah et al. 2015 [20] | Japan | Asia | High income | Observational, single center | CAD patients | Pulmonary function test |
| Dagenais et al. 2010 [21] | Canada | North America | High income | Observational, single center | CAD patients over 70 years old, who underwent CABG | Pulmonary function test |
| Komaru et al. 2017 [22] | Japan | Asia | High income | Observational, single center | CAD patients | Pulmonary function test |
| Khassawneh et al. 2018 [23] | Jordan | Asia | Upper-middle income | Observational, single center | CAD patients | Pulmonary function test |
| Ovalı et al. 2018 [24] | Turkey | Europe | Upper-middle income | Observational, single center | CAD patients underwent CABG | Pulmonary function test |
| Çağdaş et al. 2019 [25] | Turkey | Europe | Upper-middle income | Observational, single center | CAD patients underwent PCI | Self-reported method |
| Soliman Hamad et al. 2011 [26] | Netherlands | Europe | High income | Observational, single center | CAD patients underwent CABG with EF |
Self-reported method |
| Vlahou et al. 2016 [27] | Greece | Europe | High income | Observational, single center | CAD patients underwent CABG | Pulmonary function test |
| Ponomarev et al. 2017 [28] | Russia | Europe | High income | Observational, single center | CAD patients underwent CABG | Pulmonary function test |
| Ko et al. 2016 [29] | China | Asia | Upper-middle income | Observational, single center | CAD patients underwent PCI | Pulmonary function test |
| Kuo et al. 2016 [30] | Taiwan region | Asia | High income | Administrative database | MI patients | ICD codes |
| Schachner et al. 2005 [31] | Austria | Europe | High income | Observational, single center | CAD patients underwent CABG | Self-reported method |
| Sá et al. 2010 [32] | Brazil | South America | Upper-middle income | Observational, single center | CAD patients underwent CABG | Self-reported method |
| Topcu et al. 2017 [33] | Turkey | Europe | Upper-middle income | Observational, single center | CAD patients | Pulmonary function test |
| DeRose et al. 2005 [34] | United States of America | North America | High income | Observational, single center | CAD patients underwent CABG with EF |
Self-reported method |
| Najafi et al. 2015 [35] | Iran | Asia | Upper-middle income | Observational, single center | CAD patients underwent CABG | Pulmonary function test |
| Șerban et al. 2019 [36] | Romania | Europe | Upper-middle income | Observational, single center | MI patients | Self-reported method |
| Medalion et al. 2004 [37] | Israel | Asia | High income | Observational, single center | CAD patients underwent CABG | Self-reported method |
| Yokoyama et al. 2000 [38] | United States of America | North America | High income | Observational, single center | CAD patients underwent CABG | Self-reported method |
| Lazzeri et al. 2013 [39] | Italy | Europe | High income | Observational, single center | MI patients underwent PCI | Self-reported method |
| Canver et al. 1998 [40] | United States of America | North America | High income | Observational, single center | CAD patients underwent CABG | Pulmonary function test |
| Fuster et al. 2006 [41] | Spain | Europe | High income | Administrative database | CAD patients underwent CABG | Pulmonary function test |
| Cohen et al. 1997 [42] | Israel | Asia | High income | Observational, single center | CAD patients underwent CABG | Self-reported method |
| Oliveira et al. 2017 [43] | Brazil | South America | Upper-middle income | Observational, single center | CAD patients underwent CABG | Self-reported method |
| Prapas et al. 2007 [44] | Greece | Europe | High income | Observational, single center | CAD patients underwent CABG | Self-reported method |
| Wang et al. 2021 [9] | Multiple countries | N/A | N/A | Randomized clinical trial | CAD patients underwent revascularization | Self-reported method |
| Magnuson et al. 2013 [45] | Multiple countries | N/A | N/A | Randomized clinical trial | CAD patients with diabetes | ICD codes |
| Huang et al. 2019 [8] | Multiple countries | N/A | N/A | Randomized clinical trial | CAD patients underwent revascularization | Self-reported method |
| Zhang et al. 2016 [46] | China | Asia | Upper-middle income | Observational, single center | CAD patients underwent PCI | Self-reported method |
| Salisbury et al. 2007 [47] | United States of America | North America | High income | Observational, multicenter | MI patients | Self-reported method |
| Dai-Yin Lu et al. 2017 [48] | Taiwan region | Asia | High income | Administrative database | CAD patients underwent CABG | ICD codes |
| Macchia et al. 2008 [49] | Italy | Europe | High income | Administrative database | MI patients | ICD codes |
| Angouras et al. 2010 [50] | Greece | Europe | High income | Observational, single center | CAD patients underwent CABG | Pulmonary function test |
| Gatta et al. 2022 [51] | United Kingdom | Europe | High income | Observational, single center | CAD patients underwent CABG | Pulmonary function test |
| Çakalağaoğlu et al. 2020 [52] | Turkey | Europe | Upper-middle income | Observational, single center | CAD patients underwent CABG | Self-reported method |
| Berger et al. 2004 [53] | United States of America | North America | High income | Observational, multicenter | CAD patients underwent PCI | Pulmonary function test |
| Jatene et al. 2017 [11] | Multiple countries | N/A | N/A | Randomized clinical trial | CAD patients underwent PCI | Self-reported method |
| Efird et al. 2013 [54] | United States of America | North America | High income | Observational, single center | CAD patients underwent CABG | Pulmonary function test |
| Su et al. 2017 [55] | Taiwan region | Asia | High income | Administrative database | MI patients | ICD codes |
| Maynard et al. 2006 [56] | United States of America | North America | High income | Administrative database | MI patients | ICD codes |
| Clement et al. 2020 [57] | United States of America | North America | High income | Administrative database | CAD patients underwent CABG | ICD codes |
| Nishiyama et al. 2010 [58] | Japan | Asia | High income | Observational, multicenter | CAD patients underwent revascularization | Self-reported method |
| O’Boyle et al. 2013 [59] | United Kingdom | Europe | High income | Administrative database | CAD patients underwent CABG | Pulmonary function test |
| Konecny et al. 2010 [60] | United States of America | North America | High income | Observational, single center | CAD patients underwent PCI | ICD codes |
| Hawkins et al. 2009 [61] | Multiple countries | N/A | N/A | Randomized clinical trial | MI patients | Self-reported method |
| Tomaniak et al. 2020 [10] | Multiple countries | N/A | N/A | Randomized clinical trial | CAD patients underwent PCI | Self-reported method |
| Hong et al. 2019 [62] | Canada | North America | High income | Observational, single center | CAD patients | Self-reported method |
| Butt et al. 2019 [63] | Denmark | Europe | High income | Administrative database | CAD patients underwent CABG | ICD codes |
| Kostis et al. 1994 [64] | United States of America | North America | High income | Administrative database | MI patients | ICD codes |
| Andell et al. 2014 [65] | Sweden | Europe | High income | Observational, multicenter | MI patients | ICD codes |
| Elbaz-Greener et al. 2020 [66] | Israel | Asia | High income | Administrative database | MI patients underwent CABG | ICD codes |
| Deo et al. 2021 [67] | United States of America | North America | High income | Administrative database | CAD patients underwent CABG | ICD codes |
| Lin et al. 2019 [12] | Taiwan region | Asia | High income | Administrative database | CAD patients underwent PCI | ICD codes |
| Sundaram et al. 2020 [68] | United Kingdom | Europe | High income | Administrative database | MI patients | Self-reported method |
| de Miguel-Díez et al. 2015 [4] | Spain | Europe | High income | Administrative database | CAD patients underwent revascularization | ICD codes |
| Krittanawong et al. 2020 [69] | United States of America | North America | High income | Administrative database | MI patients |
ICD codes |
| Johnson-Sasso et al. 2018 [70] | United States of America | North America | High income | Administrative database | MI patients | ICD codes |
| Neumann et al. 2020 [71] | Germany | Europe | High income | Administrative database | MI patients | ICD codes |
CAD, coronary artery disease; MI, myocardial infarction; CABG, coronary artery bypass graft; PCI, percutaneous coronary intervention; ICD, International Classification of the Diseases; N/A, not applicable; EF, ejection fraction.
The random effects model (DerSimonian and Laird method) was implemented due to assumed differences within (and between) populations. Estimates with 95% confidence intervals (CI) have been provided. We adopted two types of proportional transformation, i.e., Logit transformation and Freeman–Tukey double arcsine transformation for sensitivity analysis. Leave-one-out analysis and exclusion analysis were conducted according to the number of participants in specific subgroups.
Subgroup analysis of COPD diagnostics, study type, location of study, economic status (according to World Bank), and risk of bias, were performed to identify potential sources of heterogeneity. Univariate meta-regression analyses were performed, with the prevalence of COPD in CAD as the dependent variable.
Independent variables included the COPD definition, economic status, study type,
risk of bias, area, age, male, hypertension, diabetes mellitus, dyslipidemia,
atrial fibrillation, stroke, and smoker status. Independent variables with
p
For comorbidities and risk factors in the COPD group, odds ratios (ORs) with corresponding 95% CIs were calculated according to COPD status. Values with 95% CIs that did not include one were accepted as statistically significant.
For outcomes related to COPD–CAD status, the primary endpoint was all-cause mortality. Secondary endpoints included cardiac death, stroke, revascularization, myocardial infarction (MI), heart failure, and respiratory failure. The random effect model was also implemented to pool a conservative risk ratio of COPD (compared to non-COPD) in CAD, according to various endpoints.
Subgroup analyses were performed to compare mortality in different groups, specifically the PFT versus ICD codes/self-reported method, and CABG vs. PCI. Leave-one-out analysis was again performed to assess the impact of single studies on pooled risk ratios.
Studies that reported comparisons in outcomes related to CABG and PCI in COPD patients were enlisted for meta-analysis. Outcomes related to revascularization methods, such as all-cause death, myocardial infarction, stroke, and revascularization were established as endpoints. Additionally, publication bias was assessed using Egger’s test, with results presented in the form of a funnel plot.
All statistical analyses were performed using Stata (version 13.0, StataCorporation, Austin, TX, USA) and R (version 4.0.5, R Foundation for Statistical Computing, Vienna, Austria). This study was registered with PROSPERO (CRD #42021293270) and in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Please see Supplementary Material 4 for further details.
We created a graphical abstract for ease (please see the structural graphical abstract appended). After searching databases and specific websites, we initially identified approximately 15,000 studies. Once duplicates had been excluded, 11,600 study titles were screened. A total of 10,735 studies were excluded at this screening stage, meaning 865 reports remained and the abstracts were read. Sixty-five studies were finally included for a full examination and data were extracted for pooling purposes (Fig. 2).
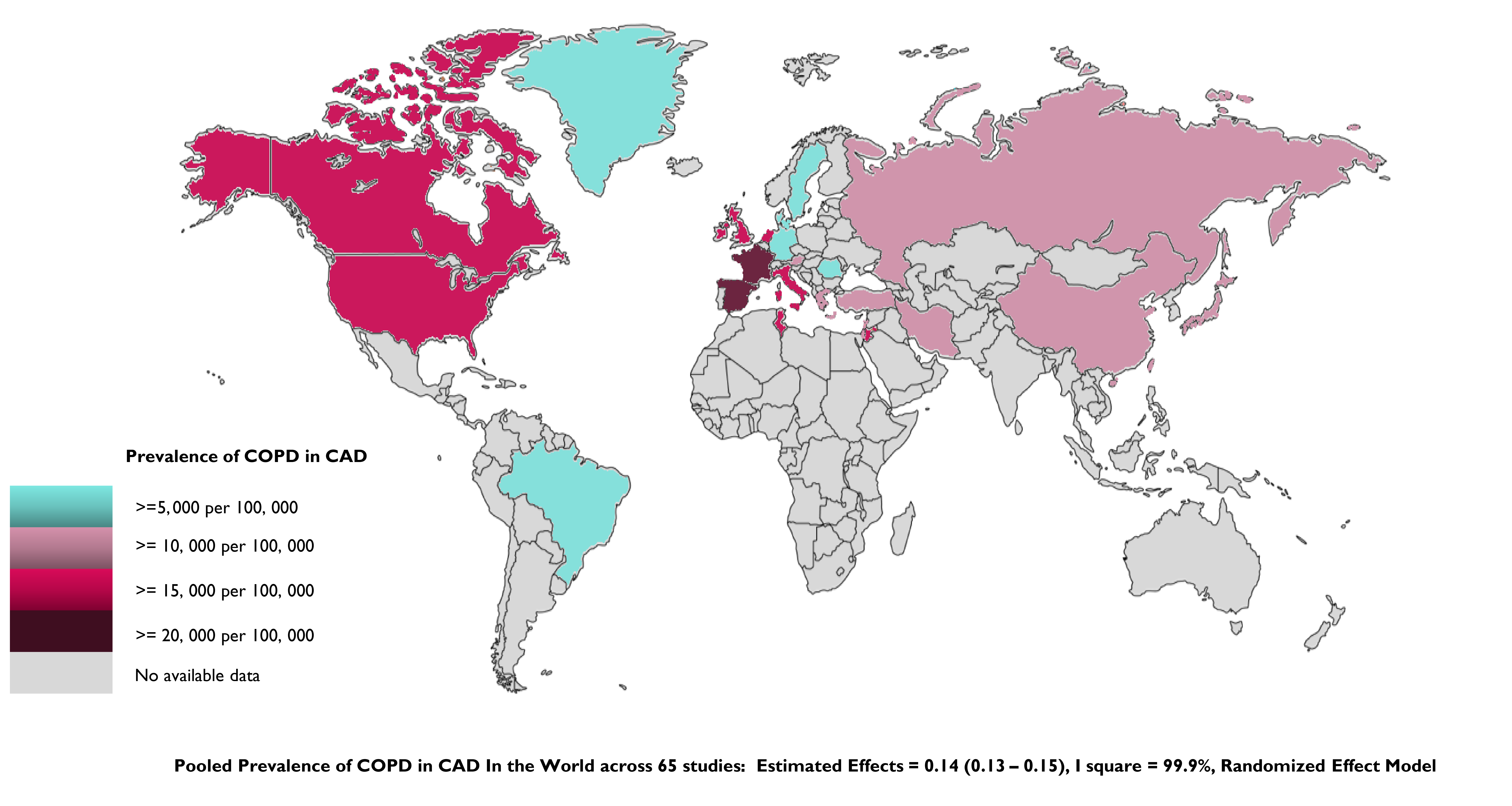 Fig. 2.
Fig. 2.Global prevalence of COPD in CAD by country. Countries for which data were unavailable are shown in grey. COPD, chronic obstructive pulmonary disease; CAD, coronary artery disease.
Study and participant characteristics, such as study type, research location, economic status, etc., are provided in Table 1 and Supplementary Table 1. Forest plots suggested that the pooled prevalence of COPD in CAD patients is 14.2% (95% CI: 13.3–15.1). Please see the Supplementary Materials, Supplementary Fig. 1, for further details. Supplementary Fig. 2 showed the publication bias of each study.
Sensitivity analysis was conducted using the inverse variance and Logit transformation methods and a similar prevalence was reported for each (Supplementary Table 2). Leave-one-out analysis suggested that there was no significant impact by a single study on the pooled COPD–CAD prevalence (Supplementary Fig. 3). However, during the sensitivity analysis, and by excluding studies according to sample size, some heterogeneity was found to exist. By initially excluding the smallest sample of studies, we found that heterogeneity was closely related to studies using the PFT as a diagnostic method (Supplementary Tables 3,4).
The pooled prevalence of COPD–CAD across different countries or regions was presented as a visualized version of the world map, with different colors indicating the extent of the COPD–CAD prevalence (Fig. 3). From the heat map, one can see that the prevalence appears highest in North America, followed by Asia, Europe, and South America. For countries in Africa and Oceania, evidence of COPD prevalence in CAD is lacking, with only one study from the African continent reporting on prevalence (Fig. 3).
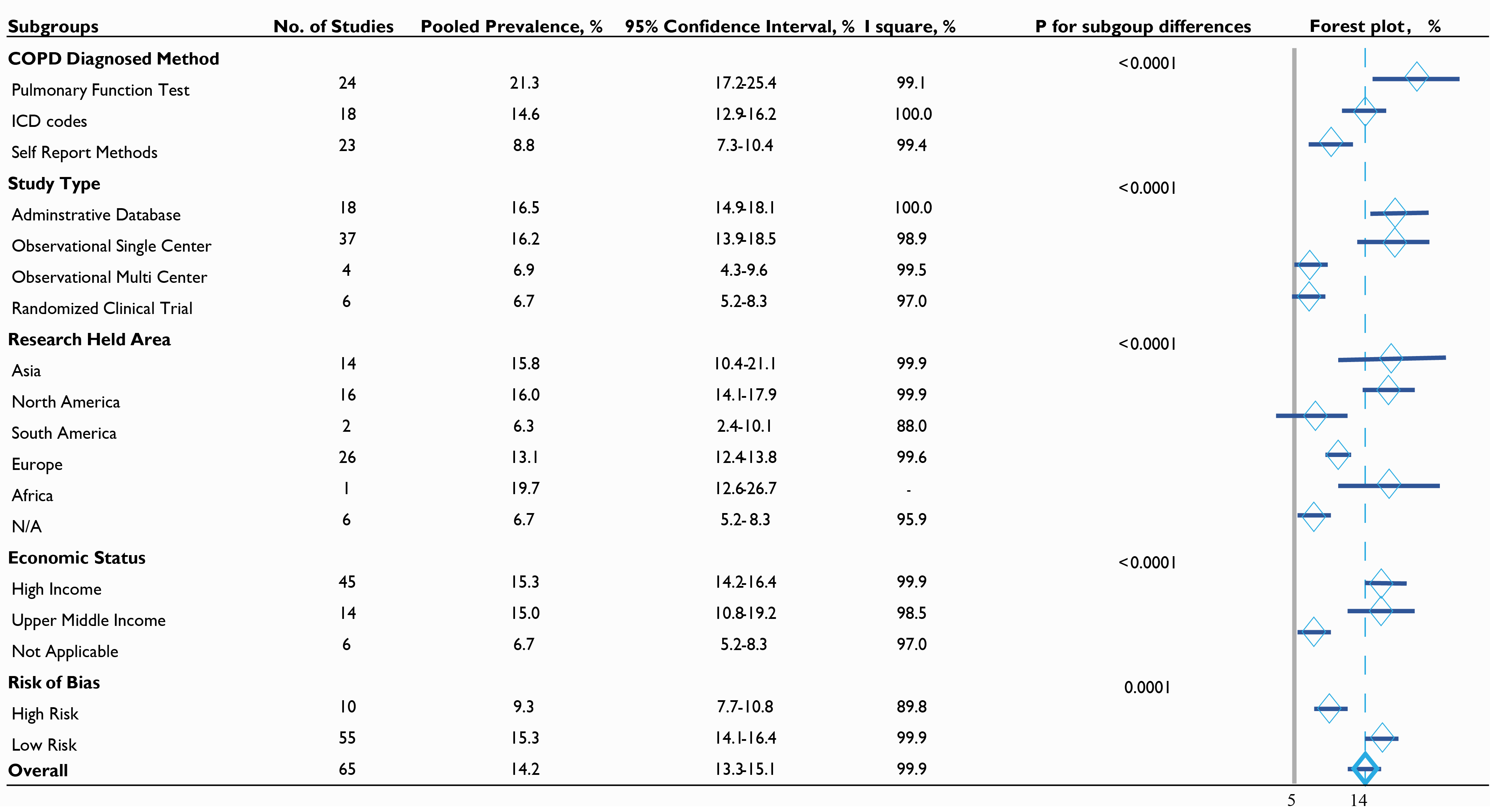 Fig. 3.
Fig. 3.Prevalence of COPD in CAD in various subgroups. COPD, chronic obstructive pulmonary disease; ICD, International Classification of the Diseases; N/A, not applicable.
The analysis of subgroups also helped to uncover potential factors that may
influence prevalence. For example, the prevalence in the PFT group was
significantly higher than the rate observed in the ICD codes group or in the
self-reported group (21.3% vs. 14.6% vs. 8.8%) and was also significant
(p
Univariate and multivariate meta-regression analyses were performed to identify
potential sources of heterogeneity. COPD diagnostics appears to be the main
source of heterogeneity, followed by study type, economic status, and diabetes
mellitus (all p
Information on OR related to patient characteristics, according to COPD status, is provided in Table 2. A total of 23 studies reported the number of men in the COPD group and non-COPD groups, with no obvious differences noted according to gender (OR = 1.001, 95% CI: 0.87–1.15). A total of 17 studies also reported dyslipidemia rates in the two groups, although, again, no statistically significant differences were observed (OR = 1.03, 95% CI: 0.89–1.19).
| Variables | No. of studies | OR | Tau square for OR | I square for OR, % | Pooled COPD prevalence in CAD (95% CI), % | |
| Smoker | 22 | 1.94 (1.57–2.40) | 0.211 | 96.0 | 17.0 (14.7–19.3) | |
| sub: non-smoker | - | - | - | 10.5 (9.0–11.9) | ||
| Hypertension | 25 | 1.36 (1.20–1.53) | 0.070 | 92.7 | 14.5 (12.4–16.6) | |
| sub: non-hypertension | - | - | - | 10.6 (9.4–11.8) | ||
| Diabetes mellitus | 25 | 1.18 (1.10–1.27) | 0.016 | 76.5 | 14.6 (12.6–16.7) | |
| sub: non-DM | - | - | - | 13.0 (11.5–14.5) | ||
| Dyslipidemia | 17 | 1.03 (0.89–1.19) | 0.068 | 93.0 | 14.3 (11.8–16.8) | |
| sub: non-dyslipidemia | - | - | - | 13.9 (11.6–16.3) | ||
| Atrial fibrillation | 8 | 1.64 (1.14–2.36) | 0.169 | 79.1 | 30.3 (17.3–43.3) | |
| sub: non-AF | - | - | - | 17.1 (11.1–23.1) | ||
| Stroke | 13 | 1.72 (1.35–2.18) | 0.143 | 95.3 | 18.8 (14.9–22.7) | |
| sub: non-Stroke | - | - | - | 12.5 (10.9–14.1) | ||
| Male | 23 | 1.00 (0.87–1.15) | 0.089 | 95.0 | 13.7 (12.0–15.3) | |
| sub: female | - | - | - | 12.7 (10.9–14.5) | ||
| Dyspnea | 4 | 4.11 (2.65–6.38) | 0.084 | 36.7 | 29.6 (18.7–40.5) | |
| sub: non-dyspnea | - | - | - | 5.9 (2.1–9.7) | ||
| Wheezes | 2 | 9.86 (1.08–90.20) | 2.021 | 75.7 | 69.7 (16.7–122.7) | |
| sub: non-wheezing | - | - | - | 11.7 (7.1–16.2) | ||
| Chronic bronchitis | 2 | 19.07 (5.14–70.81) | 0.505 | 43.8 | 67.3 (24.3–110.3) | |
| sub: non-chronic bronchitis | - | - | - | 9.3 (2.4–16.1) | ||
COPD, chronic obstructive pulmonary disease; CAD, coronary artery disease; OR, odds ratio; CI, confidence interval; AF, atrial fibrillation; DM, diabetes mellitus.
Further comorbidities and risk factors, including hypertension, diabetes
mellitus, atrial fibrillation, stroke, smoking, dyspnea, wheezes, and chronic
bronchitis were all reported to be significantly higher in the COPD–CAD group,
compared with the non-COPD–CAD group (all OR
The OR in the COPD group was nearly twice that in the non-COPD group (OR: 1.94, 95% CI: 1.57–2.4). Moreover, a higher incidence of atrial fibrillation and a history of stroke were both observed in the group with comorbid COPD. Atrial fibrillation provided an OR of 1.64 (95% CI: 1.14–2.36), while a history of stroke generated an OR of 1.72 (95% CI: 1.35–2.18). See Table 2 for further details.
A total of 23 studies reported all-cause mortality, 7 studies focused on cardiac death, 9 on myocardial infarction, and 6 focused on revascularization and stroke. Pooled all-cause mortality in the COPD group was triple that in the non-COPD group (risk ratio [RR] = 2.81, 95% CI: 2.40–3.29), see Fig. 4 and Supplementary Table 6.
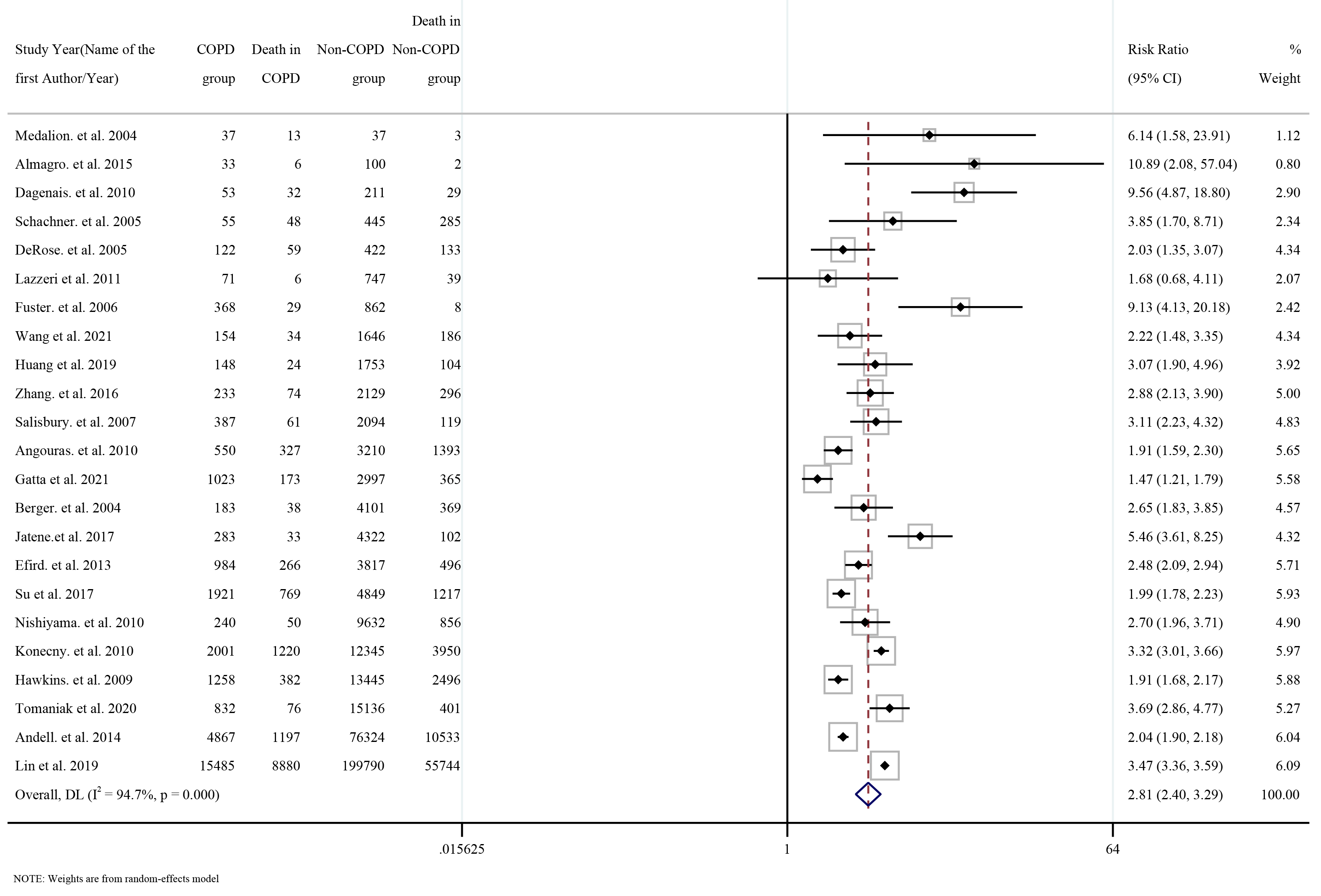 Fig. 4.
Fig. 4.Forest plot for risk of all-cause mortality according to COPD status. COPD, chronic obstructive pulmonary disease.
Pooled cardiac death, myocardial infarction, stroke, heart failure, and
respiratory failure were significantly higher in the COPD group than in the
non-COPD group (all RR
Sensitivity analyses, using the leave-one-out method, were conducted to determine whether any single study impacted the overall pooled RR (Supplementary Fig. 11). There was no obvious impact of a single study on all-cause death, cardiac death, myocardial infarction, stroke, heart failure, and respiratory failure. However, after excluding the study by Lin et al. [12] from the pooled RR for revascularization, the pooled RR increased, although, ultimately, remained lower than the null hypothesis, i.e., one (Supplementary Fig. 11).
A total of two studies directly compared the outcome of COPD–CAD patients who underwent CABG vs. PCI therapy. These two studies were both large, high-quality multicenter randomized clinical trials [8, 9]. However, they were also both post hoc, non-prespecified explorations. Therefore, we pooled the outcomes of these two studies, to compare the impact of the revascularization method on the COPD–CAD patients. As shown in Supplementary Fig. 12, an obvious reduction in revascularizations was observed after therapy (OR: 0.43, 95% CI: 0.20–0.94), along with a reduction in myocardial infarction (OR: 0.62, 95% CI: 0.18–2.11). However, no obvious benefit was observed from PCI for all-cause mortality (OR: 0.97, 95% CI: 0.54–1.74). The risk of stroke after revascularization increased in the CABG group (OR: 2.00, with 95% CI: 0.50–7.94).
Further subgroup analysis was conducted to investigate the differences in the RR between the PFT and ICD codes/self-reported method groups, and the CABG vs. PCI groups (Supplementary Figs. 13,14). Slightly higher mortality was observed in the PFT group compared with the ICD-codes/self-reported method group, although this was not considered significant (3.08 vs. 2.94, p value for subgroup differences = 0.833) (Supplementary Fig. 14). We also found no significant decrease in mortality in the CABG group compared to the PCI group (2.97 vs. 3.43, p for subgroup difference = 0.427) (Supplementary Fig. 13).
Studies reporting on revascularization in COPD–CAD patients were systematically reviewed. A total of seven studies reported the PCI rate for COPD–CAD patients. The pooled OR of the prescription rate in the COPD group was 0.68, with 95% CI: 0.56 to 0.83 when compared with the non-COPD group. A total of six studies reported the CABG rate for COPD–CAD patients and also indicated a reduced prescription rate for CABG in the COPD group, with a pooled OR equal to 0.93 and 95% CI: 0.75 to 1.15 (Supplementary Fig. 15). No significant difference was observed in strictly corrected COPD group according to GOLD criteria when compared with not strictly corrected COPD group (Supplementary Fig. 16).
Biases associated with the prevalence and outcomes were assessed separately,
including publication bias and quality assessment. Prevalence-based publication
bias was assessed using Begg’s and Egger’s tests; both at p
This systematic review and meta-analysis was designed to investigate global prevalence, comorbidities, and outcomes related to CAD patients with COPD. Additionally, we compared methods of revascularization and the outcomes for participants with COPD. We found a relatively high prevalence of COPD in CAD patients, which was higher than the previous estimate of 6% for the US adult population, provided in 2020 [74]. COPD-positive patients are more likely to be smokers, and hypertensive, with diabetes mellitus and atrial fibrillation, in addition to suffering from strokes. This supports the notion that there is a close relationship between COPD in CAD patients and other comorbidities. Additionally, we found that CAD patients with COPD are at high risk of all-cause death, cardiac death, myocardial infarction, stroke, heart failure, and respiratory failure. Further comparisons of CABG and PCI indicated that CABG may reduce the need for revascularization but that it did not lower the risk of death.
The prevalence of COPD in CAD patients is high, although there are also variations across different regions of the world. The highest rate of COPD in CAD is reported in North America, where the prevalence appears to be the same as the rate for COPD in atrial fibrillation [7]. One may assume that different diagnostic methods influence the prevalence, however, the diagnostics used for COPD are similar across North America, Europe, and Asia. Therefore, differences are more likely to be the result of culture, such as smoking and diet. Of course, there is a plethora of research on the link between diet and CAD, particularly around red meats, sugar, and salt [75, 76, 77], while the US, European nations, and Asia are distinct in terms of food cultures. Although, air pollution and other different epigenetic mechanisms can also create susceptibilities, as demonstrated by evidence that epigenetic mechanisms are involved in the development of COPD [78]; however, this does not account for differences in our genetic makeup. This study was not designed to explore genetic differences and we were only able to gain some insights into countries and cultures.
For example, we found one study that reported the prevalence of COPD–CAD in Africa. This study by Yangui et al. (2021) [16] was conducted in Tunisia, although it cannot be taken as representative since 98.3% of the sample participants were men, which suggests there are other issues that need to be overcome. For example, the high prevalence of COPD in CAD patients, at least in some Arab cultures in northern Africa, may relate to shisha culture, pollution, perhaps dry air, and socioeconomics. Cortes-Ramirez et al. [79] studied environmental risk factors associated with respiratory diseases in the region and found a potential link with Saharan dust. However, there is a paucity of evidence around the prevalence of COPD in African nations, generally [80]. Therefore, we have identified several issues that need to be studied to support health policymakers in African nations, not only related to smoking but in relation to the many other potential environmental and cultural factors involved.
We found a higher rate of smoking among those with comorbid COPD–CAD compared with CAD patients, without COPD. There is also strong evidence around the relationships between hypertension, diabetes mellitus, and COPD, with the accepted reason for this being tobacco smoking [81, 82]. COPD has also been identified as an independent factor that is involved in the development of atrial fibrillation [83, 84], while there is a higher incidence of stroke in those with COPD. According to several published studies, COPD influences stroke outcomes in two distinct ways, through COPD-related systemic inflammation and oxidative stress [85]. In the present study, all patients with CAD had similar risk ratios, which means the incidence of stroke may be due to cerebral vascular dysfunction or platelet hyperactivity related to COPD-related pathophysiologic mechanisms. Although, again, this is an area that demands further research.
Subgroup analysis highlighted differences among the included diagnostic methods. When the prevalence differences were compared, we found that PFT was associated with a 21.3% prevalence, ICD code diagnosis with 14.6%, and self-reported had 8.8%. One can assume this is related to the sensitivity and specificity of the diagnostic methods; however, perhaps more importantly, this highlights a potentially large clinical iceberg of CAD patients with COPD. This undiagnosed, and therefore untreated population is of particular concern because of the related outcomes and because many of these people may also be prediabetic or currently self-managing type II diabetes symptoms. Researchers have suggested that as much as 70% of the COPD population are undiagnosed, meaning they may be self-medicating or attempting to manage symptoms without knowing the exact cause [86]. This presents a number of problems and would certainly appear to support calls for more opportunistic testing while clinicians are treating patients for CAD.
We compared CABG to PCI and found that CABG had a similar risk ratio for mortality in the COPD group. This appears to contradict other studies that reported a beneficial effect on mortality from CABG for CAD patients. This result can be understood pathophysiologically since the occurrence of COPD and CAD is associated with systemic inflammation, oxygen depletion, and oxidative stress, which influence numerous coronary vessels. This, in turn, increases the probability of revascularization; however, this evidence was only generated from two randomized clinical trials, with small COPD patient samples. This of course affects the generalizability of the findings and the two clinical trials also did not categorize the COPD diagnostics as from either the pulmonary function test or any other test. This creates questions around the designs of studies and research quality and again highlights the need for further well-designed, clinical trials.
The incidence of revascularization in those with comorbid COPD–CAD did not increase above that observed in patients with CAD alone. Some studies have reported an increased incidence of MACEs in COPD patients after revascularization, which is mainly driven by mortality and not as a result of revascularization [10, 11]. This may explain why outcomes for COPD are so unsure, especially when choosing MACEs as the primary endpoint. Since revascularization is a MACE for COPD, MACEs are not the most suitable primary endpoint. Interestingly, there remains a substantial amount of publication bias with regard to revascularization outcomes. In a recent study, that adopted a leave-one-out approach, Lin et al. [12] found that revascularization had a substantial impact on pooled risk ratios. However, when we excluded the study by Lin et al. [12] from our analysis, the pooled risk ratio remained less than 1. This suggests that the impact of COPD on the outcome of CAD patients is limited, and therefore, revascularization may not influence outcomes as originally thought.
Several limitations ought to be discussed before we provide recommendations. First, we should acknowledge diagnostic biases, which will have occurred through different diagnostic methods. We must also acknowledge that more than half of the participants affected by COPD had not been diagnosed, which suggests the estimated prevalence of CAD–COPD is actually higher. Second, even though our study included numerous studies there are still some high-quality studies that were not included due to our inclusion criteria. However, this does not detract from the scientific merit of this study [87, 88]. Third, even though the goal was to assess global prevalence, we were not able to gain insights into African nations, most of the Middle East, South America, India, Central Asia, Southeast Asia, and Australia. One might assume this is related to income, although this was based on the heatmap rather than it being scientifically determined. Fourth, heterogeneity and bias appear particularly high and there are a number of reasons for this that should be further explored. Thus, additional research using a longitudinal approach and multinational databases is required, although this will require cooperation and collaboration at the highest levels. Finally, there appears to be an issue around polypharmacy reporting for those with COPD–CAD. This may be occurring because researchers feel it is unnecessary to report these interactions or because of publication parameters. We hope this will change; however, more sophisticated research designs are required for health policy development.
The global prevalence of COPD–CAD appears generally high, although there are clear geographical differences. COPD diagnostic methods undoubtedly cause a proportion of the variations observed, however, there is clearly a clinical iceberg of COPD among CAD patients. CAD patients with COPD also appear to have multiple related comorbidities, which influence prognoses. Physicians should opportunistically test for COPD to ensure their patients are not self-medicating and adding complications. More direct comparisons of revascularization versus anti-inflammation therapies, and beta-blockers for COPD–CAD patients may also prove useful.
Datasets generated and analyzed for this work are available in the main text.
YTZ, ZLH, SS, CL, JY, WYW, YQ, YF, and HX designed the study, and all authors oversaw its implementation. YTZ and ZLH coordinated and performed all review activities, including search screening, study selection, data extraction, and quality assessment. YTZ, ZLH, SS, and YDT did the data analyses. CLS and YDT improved the methods of this study. YTZ, ZLH, SS, CLS, and YDT wrote the initial draft of the manuscript. CL, JY, WYW, YQ, YF, and HX help revise this manuscript. All authors reviewed the study findings and read and approved the final version before submission. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Not applicable.
Not applicable.
This article was supported by CAMS Innovation Fund for Medical Sciences (2021-I2M-5-003), Beijing Natural Science Foundation (7232209), and National Natural Science Foundation of China (81825003).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.