




 , Xianhong Shu 1,2,3,*
, Xianhong Shu 1,2,3,*1 Department of Echocardiography, Zhongshan Hospital, Fudan University, 200032 Shanghai, China
2 Shanghai Institute of Cardiovascular Diseases, 200032 Shanghai, China
3 Shanghai Institute of Medical Imaging, 200032 Shanghai, China
†These authors contributed equally.
Abstract
Background: Predicting outcomes of surgical aortic valve replacement
(AVR) in patients with chronic severe aortic regurgitation (AR) and markedly
reduced left ventricular (LV) function remains a challenge. This study aimed to
explore the preoperative echocardiographic index that could predict the recovery
of LV systolic function after surgery in patients with chronic severe AR and
reduced left ventricular ejection fraction (LVEF). Methods: The study
group consisted of 50 patients diagnosed with chronic severe AR (
Keywords
- speckle tracking echocardiography
- stress echocardiography
- aortic regurgitation
- left ventricular systolic function
- LVEF
- longitudinal strain
Chronic severe aortic regurgitation (AR) has a poor prognosis and is associated with increased mortality and morbidity [1]. At its late stage, the markedly decreased left ventricular ejection fraction (LVEF) may incur excessive surgical mortality. However, previous studies found that surgical aortic valve replacement (AVR) could still be beneficial since volume overload is relieved [2, 3, 4]. Therefore, it is of great importance to identify those preoperative parameters which distinguish those patients that can have a better recovery, which is closely related to improvement of symptoms and long-term prognosis [5, 6, 7].
Stress echocardiography (SE) has been used to identify viable myocardium and contractile reserve (CR) in a variety of heart diseases with left ventricular (LV) contractile dysfunction [8, 9, 10]. In previous studies, LV CR estimated by low-dose dobutamine stress echocardiography (DSE) in patients with severe AR and mild-moderately reduced LVEF is highly predictive of postoperative LV contractile function and clinical outcomes after AVR [11, 12]. In patients with chronic severe AR with significantly decreased LVEF, however, it remains unclear whether low-dose DSE has the same predictive power in the recovery of LV contractile function after AVR.
Speckle tracking echocardiographic (STE) is a reliable and reproducible method to assess myocardial deformation with incremental value to subtle regional wall motion change than traditional echocardiography, and it had been shown to achieve high reproducibility during all stages of SE [13, 14, 15]. In the present study, by combining STE and low-dose DSE, we sought to determine novel predictors for early recovery of LV contractile function following surgical AVR in patients with chronic severe AR and significantly decreased LVEF.
From April 2014 to February 2018, 50 patients with chronic severe AR and a
significant reduction of LVEF (
Exclusion criteria included concomitant moderate or severe aortic stenosis and other moderate or severe valvular disease, coronary artery disease, atrial fibrillation, congenital heart disease, cardiomyopathy, severe hypertension, allergies to dobutamine, and other systemic diseases that cannot tolerate DSE. This study was conducted according to the principles stated in the Declaration of Helsinki. Ethics approval for the study was granted by the Ethics Committees of Zhongshan Hospital, Fudan University, and all patients provided written informed consent.
All patients underwent low-dose dobutamine stress echocardiography
(DSE) (peak dose 20
Examinations were performed with a GE E9 system equipped with a M5Sc probe
(1.7–3.4 Hz) (GE Vingmed Ultrasound AS, Horten, Norway). Image acquisition and
conventional measurements were performed according to the American Society of
Echocardiography Examination guidelines for adult transthoracic echocardiography
[17]. Dynamic images were acquired in cine loops with 3–5 cardiac cycles for
on-cart analysis during rest and peak stress stage. All echocardiographic images
were recorded in a digital raw-data format (native DICOM format) for further
analysis. During the comprehensive echocardiographic examination, LV
end-diastolic diameter (LVEDD) and LV end-systolic diameter (LVESD) were obtained
by M-mode in parasternal long axis view at rest (defined as baseline or
pre-surgery values, respectively). Standard two-dimensional (2D) apical views
(four-chamber, two-chamber, and three-chamber) were obtained in the triplane mode
using a three-dimensional (3D) matrix array transducer. LV end-diastolic volume,
LV end-systolic volume and stroke volume were analyzed using the triplane Simpson
method, with subsequent calculation of LVEF at rest and peak stress stage
(defined as baseline or pre-surgery LVEF value, peak LVEF value, respectively)
(Fig. 1). The above indicators are the average of 3 consecutive cardiac cycles.
Current guidelines recommend the LV CR definition in asymptomatic chronic AR
patients as an absolute increase in ejection fraction (
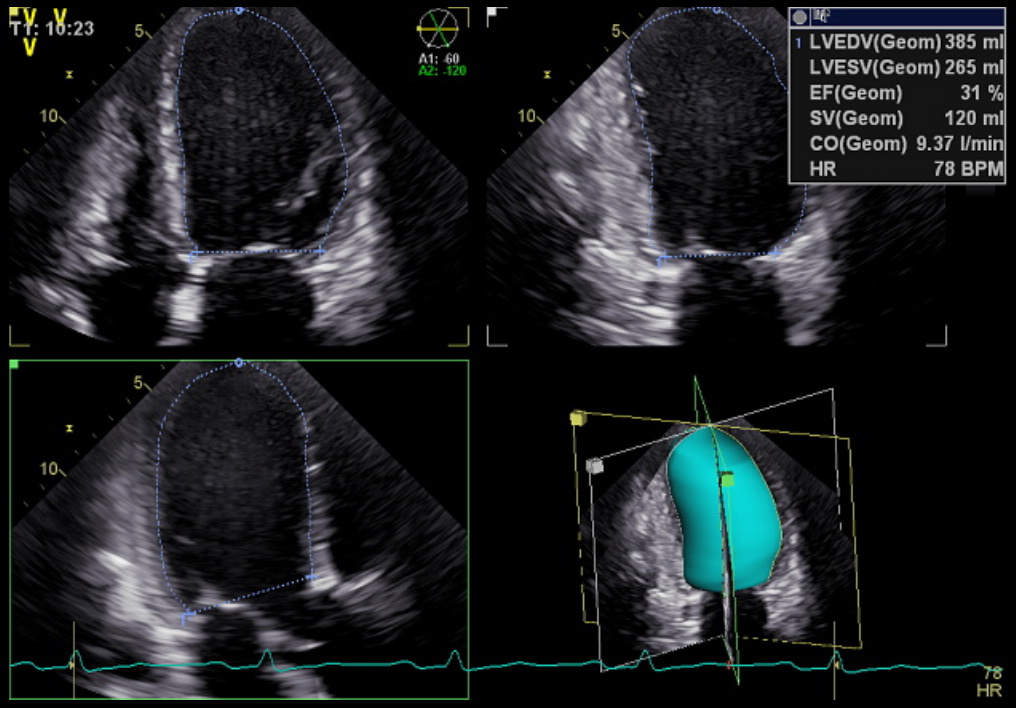 Fig. 1.
Fig. 1.Representative example of LV volume analyzed through triplane Simpson method, with subsequent calculation of LVEF. LV, left ventricular; LVEF, left ventricular ejection fraction.
The analysis was performed offline by a single observer without knowledge of hemodynamic data, using commercially available software (Echopac PC, Version 203, GE Vingmed Ultrasound AS, Horten, Norway). The LV global longitudinal strain (GLS) was analyzed in 2D images of three apical views (four-chamber, two-chamber, and three-chamber) at rest and peak stress stage during low-dose DSE (defined as baseline GLS and peak GLS values, respectively). The software could track the motion of speckles within the myocardium after the LV endocardial border was delineated in the end-systolic frame, and automatically analyze the longitudinal strain. If the tracking is suboptimal, the region of interest can be readjusted in real-time. After obtaining the corresponding curves and longitudinal strain values of the three apical views, the software could automatically calculate the LV GLS, which was the consecutive average of the peak systolic longitudinal strain (Fig. 2).
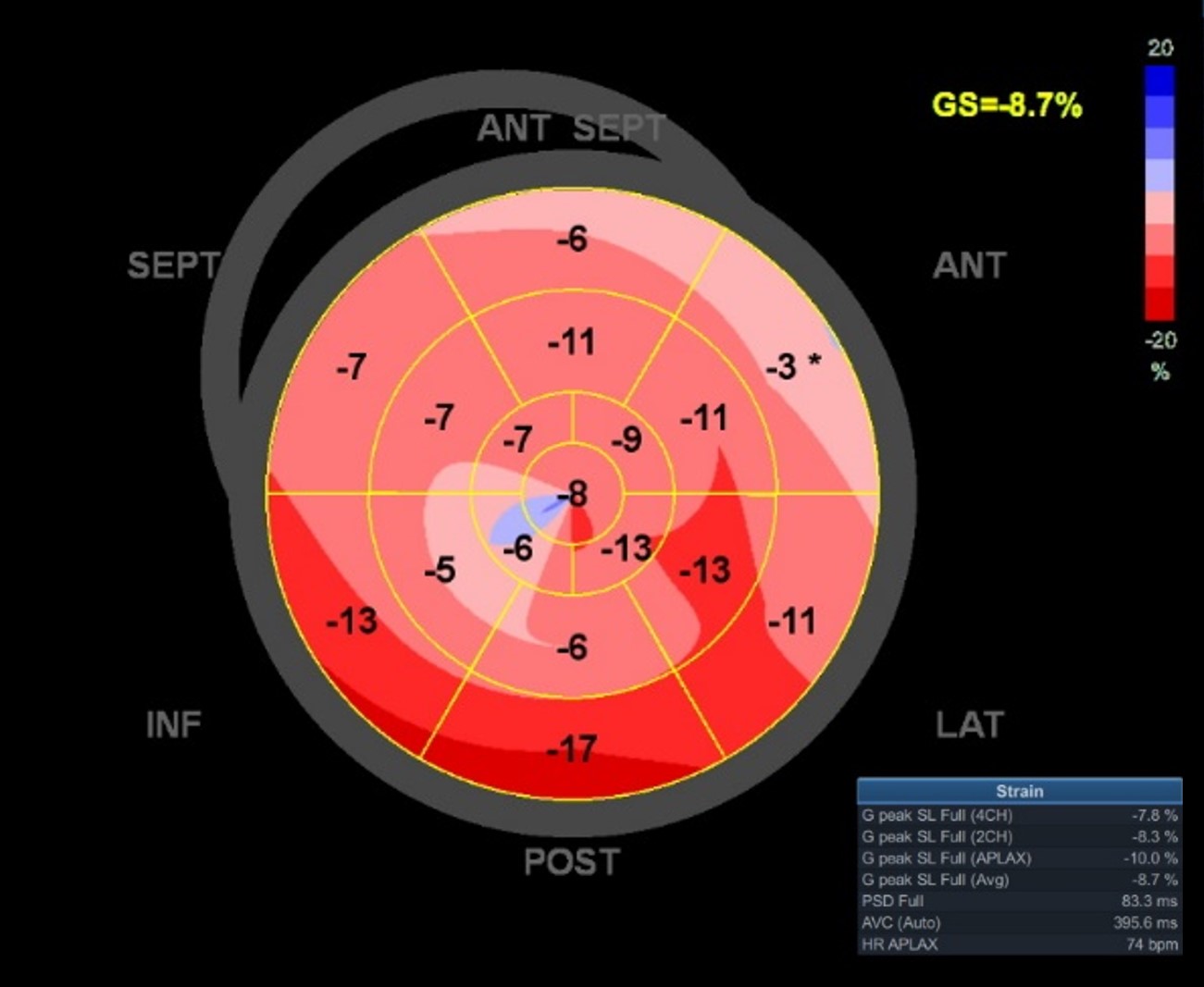 Fig. 2.
Fig. 2.Representative example of the LV GLS measurement based on 2D echocardiography by offline analysis software EchoPAC. LV, left ventricular; GLS, global longitudinal strain; 2D, two-dimensional.
All the patients with LV CR underwent standard surgical AVR. Perioperative events that were recorded included death, infection, heart failure, prolonged ventilation, and other cardiovascular and cerebrovascular events. Follow-up TTE was performed over six months to one year, and included LVEF, LVEDD and LVESD (defined as post-surgery values, respectively).
During the follow-up period, patients were divided into two groups according to
whether the post-surgery LVEF improved to the lower limit of heart failure with
mildly reduced LVEF (HFmrEF, which is defined as LVEF 41%–49% according to the
2022 AHA/ACC/HFSA guideline) [18]. The well-recovery group was defined as an LVEF
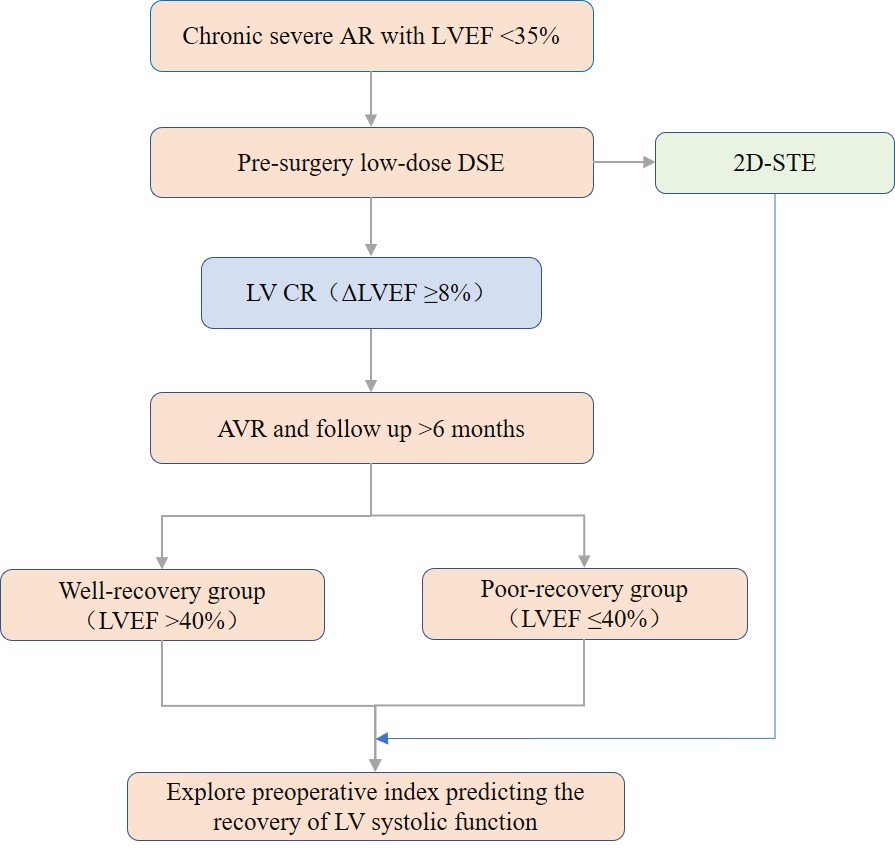 Fig. 3.
Fig. 3.The experimental flow chart. AR, aortic regurgitation; LVEF, left ventricular ejection fraction; DSE, Dobutamine stress echocardiography; 2D-STE, two-dimensional speckle tracking echocardiographic; LV, left ventricular; CR, contraction reserve; AVR, aortic valve replacement.
Statistical analysis was performed using SPSS version 22.0 (SPSS, Chicago, IL,
USA). All continuity variables were tested by normality test and presented as the
mean
A total of 50 patients were included in this retrospective study. All patients
achieved the peak stress (20
| Vriables | Patients (n = 37) | |
| Age (yrs) | 55 | |
| Male, n (%) | 32 (87) | |
| Hypertension, n (%) | 14 (38) | |
| Diabetes, n (%) | 5 (14) | |
| NYHA class ( |
30 (81) | |
| Heart rate (bpm) | 76 | |
| Etiology | ||
| Degenerative, n (%) | 13 (35) | |
| Bicuspid valve, n (%) | 6 (16) | |
| Endocarditis, n (%) | 1 (3) | |
| Rheumatic, n (%) | 6 (16) | |
| Aortic root ectasia, n (%) | 11 (30) | |
| Surgical method | ||
| AVR, n (%) | 29 (74) | |
| Bentall, n (%) | 8 (26) | |
| Valve type | ||
| Mechanical valve, n (%) | 28 (76) | |
| Biological valve, n (%) | 9 (24) | |
| Data are expressed as mean | ||
Table 2 shows the changes of LVEF and GLS at rest and peak stress stage during
DSE. Baseline LVEF and baseline GLS were all significantly lower than normal
levels. The peak values during DSE significantly increased compared with those at
rest (36.1
| Variables | Baseline | Peak | Addition (Δ) |
|---|---|---|---|
| LVEF (%) | 26.2 |
36.1 |
10.0 |
| GLS (%) | –7.5 |
–9.4 |
–1.9 |
| Data are expressed as mean *Significant difference (p | |||
Postoperative LVEF ranged between 20% and 64%. Changes in LV size (LVEDD,
LVESD) and LVEF evaluated by TTE are shown in Table 3. The postoperative LVEDD,
LVESD and LVEF were significantly improved from the
preoperative data (62.6
| Variables | Pre-surgery | Post-surgery | p value |
|---|---|---|---|
| LVEDD (mm) | 76.2 |
62.6 |
|
| LVESD (mm) | 65.1 |
49.7 |
|
| LVEF (%) | 26.2 |
42.4 |
|
| Data are expressed as mean | |||
All post-surgery cases were divided into a well-recovery group (post LVEF
| Variables | Well-recovery group (n = 18) | Poor-recovery group (n = 19) | p value | |
|---|---|---|---|---|
| Clinical data | ||||
| Age (yrs) | 53 |
57 |
0.262 | |
| Male, n (%) | 15 (83) | 17 (89) | 0.585 | |
| Hypertension, n (%) | 9 (50) | 5 (26) | 0.138 | |
| Diabetes, n (%) | 2 (11) | 3 (16) | 0.677 | |
| NYHA class ( |
16 (89) | 15 (79) | 0.412 | |
| Heart rate (bpm) | 74 |
77 |
0.405 | |
| AF, n (%) * | 1 (6) | 3 (16) | 0.604 | |
| Valve type * | ||||
| Mechanical valve, n (%) | 15 (83) | 13 (68) | 0.291 | |
| Biological valve, n (%) | 3 (17) | 6 (32) | ||
| Echocardiographic data | ||||
| Baseline LVEDD (mm) | 74.1 |
78.2 |
0.139 | |
| Baseline LVESD (mm) | 61.7 |
68.3 |
0.008 | |
| Baseline LVEF (%) | 27.6 |
24.8 |
0.122 | |
| Peak LVEF (%) | 38.0 |
34.3 |
0.070 | |
| ΔLVEF (%) | 10.4 |
9.5 |
0.318 | |
| Vmax (m/s) * | 2.5 |
2.6 |
0.563 | |
| Maximum PG (mmHg) * | 26.7 |
27.9 |
0.677 | |
| Mean PG (mmHg) * | 14.8 |
16.1 |
0.410 | |
| STE data | ||||
| Baseline GLS (%) | –8.6 |
–6.5 |
||
| Peak GLS (%) | –10.6 |
–8.2 |
||
| ΔGLS (%) | –1.9 |
–1.8 |
0.703 | |
| Data are expressed as mean * These data were postoperative results. | ||||
In simple linear regression analysis, baseline GLS and peak GLS correlated
better with post-surgery LVEF (R = –0.581 for baseline GLS, p
| Pre-surgery variables | Correlation coefficient | p value | |
|---|---|---|---|
| Echocardiographic data | |||
| Baseline LVEDD (mm) | –0.355 | 0.031 | |
| Baseline LVESD (mm) | –0.543 | ||
| Baseline LVEF (%) | 0.219 | 0.192 | |
| Peak LVEF (%) | 0.296 | 0.075 | |
| ΔLVEF (%) | 0.238 | 0.156 | |
| STE data | |||
| Baseline GLS (%) | –0.581 | ||
| Peak GLS (%) | –0.596 | ||
| ΔGLS (%) | –0.059 | 0.728 | |
| LVEDD, left ventricular end-diastolic diameter; LVESD, left ventricular end-systolic diameter; LVEF, left ventricular ejection fraction; STE, Speckle tracking Echocardiography; GLS, global longitudinal strain. | |||
The prediction performance of conventional echocardiographic parameters and STE
parameters for marked recovery of LV contractive function (follow-up LVEF
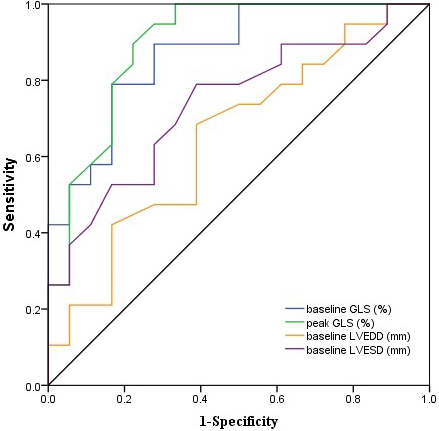 Fig. 4.
Fig. 4. The ROC curves for predicting marked recovery of LV contractive
function (follow-up LVEF
| Variables | AUC (95% CI) | Cutoff value | Sensitivity, % | Specificity, % | p value |
| Baseline LVEDD (mm) | 0.649 (0.471–0.828) | 75.5 | 68.4 | 61.1 | 0.121 |
| Baseline LVESD (mm) | 0.738 (0.577–0.899) | 64.5 | 63.2 | 72.2 | 0.013 |
| Baseline GLS (%) | 0.868 (0.755–0.982) | –7.8 | 89.5 | 72.2 | |
| Peak GLS (%) | 0.895 (0.789–1.000) | –9.4 | 89.5 | 77.8 | |
| Data are expressed as mean | |||||
AR occurs secondary to primary aortic valve lesions or geometric changes in the aortic root, commonly in degenerative diseases, rheumatic heart disease, and congenital abnormalities [19]. Chronic severe AR causes excessive LV volume overload and end-diastolic pressure which can lead to LV enlargement and LV contractile dysfunction [20]. According to the guidelines, it is necessary for patients with chronic severe AR and significantly decreased LVEF to undergo surgical AVR [16, 21]. This specific patient population has a higher perioperative mortality than those with normal or mild-moderately reduced LVEF. The short-term recovery of LV contractile function after AVR is closely related to long-term prognosis [3, 5, 22]. Therefore, it is important to be able to accurately predict the short-term recovery after AVR in patients with reduced LVEF to determine which patients will derive the greatest benefit from surgery.
Stress echocardiography (SE) is a commonly used, non-invasive, convenient and
reliable method for evaluating LV CR in clinical practice. Several studies have
shown that in patients with severe AR, LV CR based on conventional
echocardiographic parameters could predict the recovery of LV contractile
function after surgery [12, 22, 23]. In our study, all surgical patients were
assessed with LV CR based on conventional echocardiographic parameters for LVEF.
During short-term follow-up, LVEF and LV size markedly improved compared with
pre-surgery data in the entire group. This reverse remodeling of LV demonstrated
that some patients could benefit from surgery. Moreover, only one patient
experienced a perioperative death because of respiratory failure. This low
perioperative mortality may be related to our strict definition of LV CR
(
However, we also found that the recovery of LVEF varied significantly and only
half of these patients improved to an LVEF
Conventional echocardiographic parameters reflect the functional structure of the left ventricle as a whole, but cannot reflect the function of the local myocardium. The contraction of the LV myocardium involves multiple directions including longitudinal, radial, circumferential, and torsional one. They act simultaneously to constitute the overall contractile activity of the LV. STE can quantitatively analyze the myocardial strain in a specific direction, such as GLS, which is in the longitudinal direction [27]. Therefore, STE is currently a widely used tool for evaluating intrinsic contractility of the myocardium as it can track the movement of the myocardium and detect subtle changes at the myocardial level [27, 28]. Previous studies have shown that myocardial strain based on STE is more sensitive in evaluating LV systolic dysfunction in patients with chronic AR than volume-based LVEF [14, 29, 30, 31]. In addition, due to the high reproducibility and feasibility of GLS, it has been suggested as a diagnostic tool to evaluate LV CR [10, 32].
In our study, both the baseline GLS and peak GLS during low-dose DSE were
significantly lower than the normal value (
Both baseline GLS and peak GLS showed higher predictive value than conventional echocardiographic indices for predicting postoperative recovery in these patients. Furthermore, peak GLS had the highest predictive ability (AUC: 0.895; sensitivity: 89.5%; and specificity: 77.8%). This may be due to the fact that peak GLS reflects both the baseline and reserved contractility of the LV, which is revealed by the combination of DSE and STE. The preoperative peak GLS may better determine the level of recovery of LVEF after AVR in patients with chronic severe AR and severe LV contractile dysfunction.
Myocardial deformation could be assessed by speckle tracking technologies including 2D and 3D STE. 2D-STE has been shown to be able to effectively detect subtle systolic function impairment in a variety of diseases [33, 34]. One previous study [35] found that in asymptomatic chronic AR patients with preserved LVEF, strain parameters acquired by 3D-STE were basically consistent with 2D-STE and feature tracking magnetic resonance imaging. This confirms that 3D-STE is highly reliable in such patients. In addition, 3D-STE allows the quantification of complex ventricular mechanics including torsion, twist and area strain, which could not be reliably assessed by 2D-STE. 3D-STE is also free from the influence of out-of-plane motion in 2D echocardiography. However, 3D-STE is subject to technical limitations including very low temporal and spatial resolution, intervendor differences and non-standardization [36]. Future clinical studies investigating the added prognostic value of 3D-STE in the current patient population are promised.
It should be noted that this study has some limitations. First, due to the strict enrollment criteria of this study in a single center, the sample size was relatively small. With this relatively low number of patients involved, only limited consequences could come out. Thus, this study could be considered as a preliminary validation of the feasibility of STE combined with low-dose DSE in predicting the surgical outcome in patients with chronic severe AR and markedly reduced LV function. Future studies with larger sample size and more definite outcome events are guaranteed. Second, this is a trial with retrospective design and is thus subject to its innate limitations. Prospective studies are needed to verify the current findings. Third, TTE and STE were all 2D-based in this study. The influence of out-of-plane motion was especially prominent in significantly enlarged LV and may prevent accurate assessment of strain parameters. 3D TTE and STE is not subject to such influence and could be considered a promising research direction.
Patients with chronic severe AR and markedly reduced LV function who demonstrate LV CR could benefit from surgical AVR. STE combined with DSE could provide a more sensitive quantitative index for predicting the recovery of LV systolic function after AVR in this patient population. Due to the non-invasive, convenient and accurate characteristics of this combined method, it would be expected to become a new means for clinical application to evaluate LV contractile function and CR, and may be an important reference for clinical decision-making.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
LLD, XHS and QL participated in the study design; WXZ and YFW performed the research; QL, YL and BQC performed the statistical analysis and manuscript drafting. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was conducted according to the principles stated in the Declaration of Helsinki. Ethics approval for the study was granted by the Ethics Committees of Zhongshan Hospital, Fudan University (Y2020-458), and all subjects provided written informed consent.
Not applicable.
This research was funded by Name of Scientific Research Project of Shanghai Health Commission (20204Y0345).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.